
Renal and Red Marrow Dosimetry in Peptide Receptor Radionuclide Therapy: 20 Years of History and Ahead

Cliniques Universitaires Saint-Luc, 1200 Brussels, Belgium
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2021, 22(15), 8326; https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22158326
Submission received: 18 May 2021
/
Revised: 28 July 2021
/
Accepted: 31 July 2021
/
Published: 3 August 2021
(This article belongs to the Special Issue Somatostatin 2.0)
Abstract
:The development of dosimetry and studies in peptide receptor radionuclide therapy (PRRT) over the past two decades are reviewed. Differences in kidney and bone marrow toxicity reported between 90Y, 177Lu and external beam radiotherapy (EBRT) are discussed with regard to the physical properties of these beta emitter radionuclides. The impact of these properties on the response to small and large tumors is also considered. Capacities of the imaging modalities to assess the dosimetry to target tissues are evaluated. Studies published in the past two years that confirm a red marrow uptake in 177Lu-DOTATATE therapy, as already observed 20 years ago in 86Y-DOTATOC PET studies, are analyzed in light of the recent developments in the transferrin transport mechanism. The review enlightens the importance (i) of using state-of-the-art imaging modalities, (ii) of individualizing the activity to be injected with regard to the huge tissue uptake variability observed between patients, (iii) of challenging the currently used but inappropriate blood-based red marrow dosimetry and (iv) of considering individual tandem therapy. Last, a smart individually optimized tandem therapy taking benefit of the bi-orthogonal toxicity-response pattern of 177Lu-DOTATATE and of 90Y-DOTATOC is proposed.
1. Introduction
Peptide receptor radionuclide therapy (PRRT) is a well-established therapy for metastatic cancers expressing somatostatin receptors. A somatostatin analog peptide, such as octreotide or octreotate, is covalently bounded to a chelator, such as DTPA or DOTA. This chelator can be viewed as an empty basket. Before intravenous injection, a radionuclide (111In, 90Y, 177Lu) is mixed with the chelator–peptide in a solution at a low pH and at a temperature both optimized to promote the entrance of the radionuclide within the chelator cage. High labelling fractions are easily reached, i.e., less than 2% of residual free radionuclide. The labeled compound exhibits a rather high stability when the pH solution is increased above 6.
The quantity to be injected is expressed in becquerel (Bq), which corresponds to one decay per second, and is named activity. By analogy with pharmaceutical drug, this quantity is often named dose, which is incorrect—the term dose identifies the quantity of energy deposed in a tissue by the particles emitted during the decays. This dose is expressed in gray (Gy), corresponding to 1 joule (J) delivered in 1 kg of tissue.
The first PRRT trials used 111In-DTPA-octreotide [1], a tracer initially developed for diagnostic intent. Due to the cell internalization of the tracer, the short range 111In auger electrons were considered suitable for tumor therapy [2]. The observed tumor control appeared promising, but an escalating activity study quickly revealed hematological concerns [3]. Indeed, as most of the 111In decay energy is converted into gamma rays, the cross-irradiation of the red marrow from the remainder of the body was significant [4].
This issue was overcome using 90Y-DOTA-octreotide (90Y-DOTATOC) [5], which for therapy intent, can be considered as a pure beta emitter. This was confirmed by the 90Y-DOTATOC clinical phase I trial SMT-487 [6,7]. With this compound, the first organ at risk was no longer the red marrow, but the kidneys, which is less life threatening [8]. However, due to its long beta range, i.e., maximal 11 mm in water, the dose delivered to small tumors is limited. Thus, relapse of micro-metastases initially not visible on imaging modalities were observed, although all known metastases completely responded.
To improve small tumor control, 177Lu-DOTA-octreotate (177Lu-DOTATATE) was developed [9], the beta of which has a smaller range, i.e., 2 mm in water. Although the decay energy is mostly brought by the beta, the main tissue at risk identified in the phase III study was the red marrow, with about 10% of the patients undergoing grade 3 or 4 lymphopenia [10].
The aim of this paper is to provide a comprehensive review of the literature evidencing and explaining the different toxicity and response patterns observed between 90Y-DOTATOC and 177Lu-DOTATATE PRRT. Last, by combining therapy improvements reported in the literature, a smart optimized tandem therapy design is proposed.
2. Kidney Dosimetry and Toxicity
The 90Y-DOTATOC clinical phase I trial 86Y-SMT-487 [6,7,8] was designed following the FDA requirements. The total injected activity was computed to deliver a maximum dose of 27 Gy to the kidneys, based on a pre-therapy 86Y-DOTATOC PET using the MIRD pamphlet no. 11 [11], which assumed a standard kidney volume for the dosimetry calculation. The PET scan was reconstructed using a dedicated prompt single gamma ray correction [12].
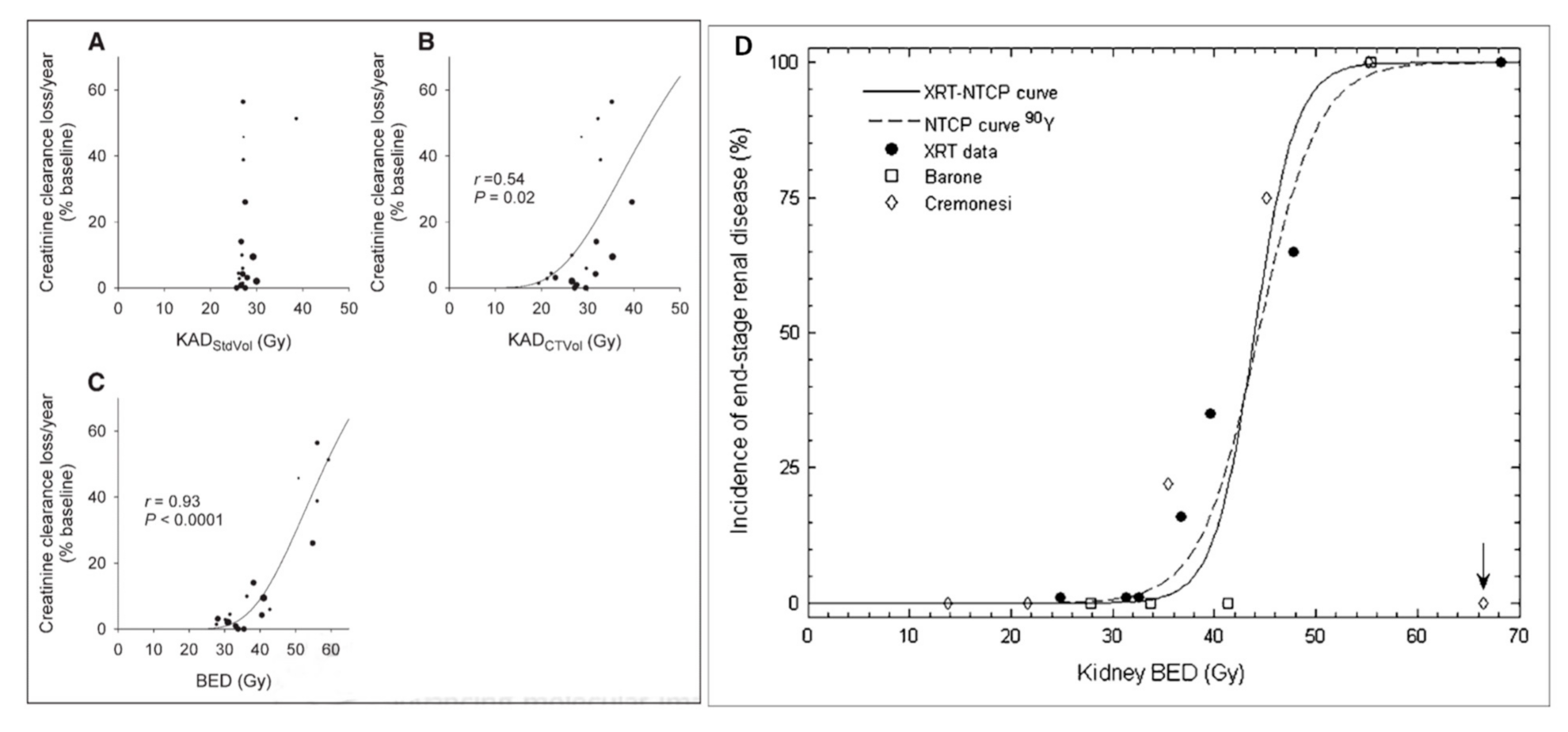
The trial included a cycle activity escalation, i.e., a reduction in the number of therapy cycles needed to reach 27 Gy to the kidneys, starting from five cycles to a single cycle. The patient kidney follow-up was set as 5 years, with patients exhibiting a creatinine clearance lost per year up to 60%. Figure 1A clearly shows that obviously no toxicity–dose correlation was observed, as all the patients, apart from one receiving an extra cycle for compassionate use, received the same kidney dose.
Rather than to conclude that dosimetry was useless, which sometimes happens in nuclear medicine, the patient CT analogic films were scanned and the renal volume measured. At this time, no hybrid SPECT-CT or PET-CT was available, and due to limited data storage capacity, most patient CT slices were only analogically archived. Figure 1B shows that by just rescaling the kidney dose with the standard to individual kidney volume ratio, a toxicity–dose relation became visible.
It was noted that globally, the patients receiving fewer cycles experienced higher creatinine clearance lost per year (Figure 1B). The absorbed doses were thus converted into a biological effective dose (BED) using the Lea–Catcheside formalism [14], and a clear toxicity–dose correlation appeared (Figure 1C). This toxicity–dose relation observed in nuclear medicine was the first one matching that observed in EBRT (Figure 1D): the dose calculation based on fractionation commonly used in EBRT was proved applicable in nuclear medicine.
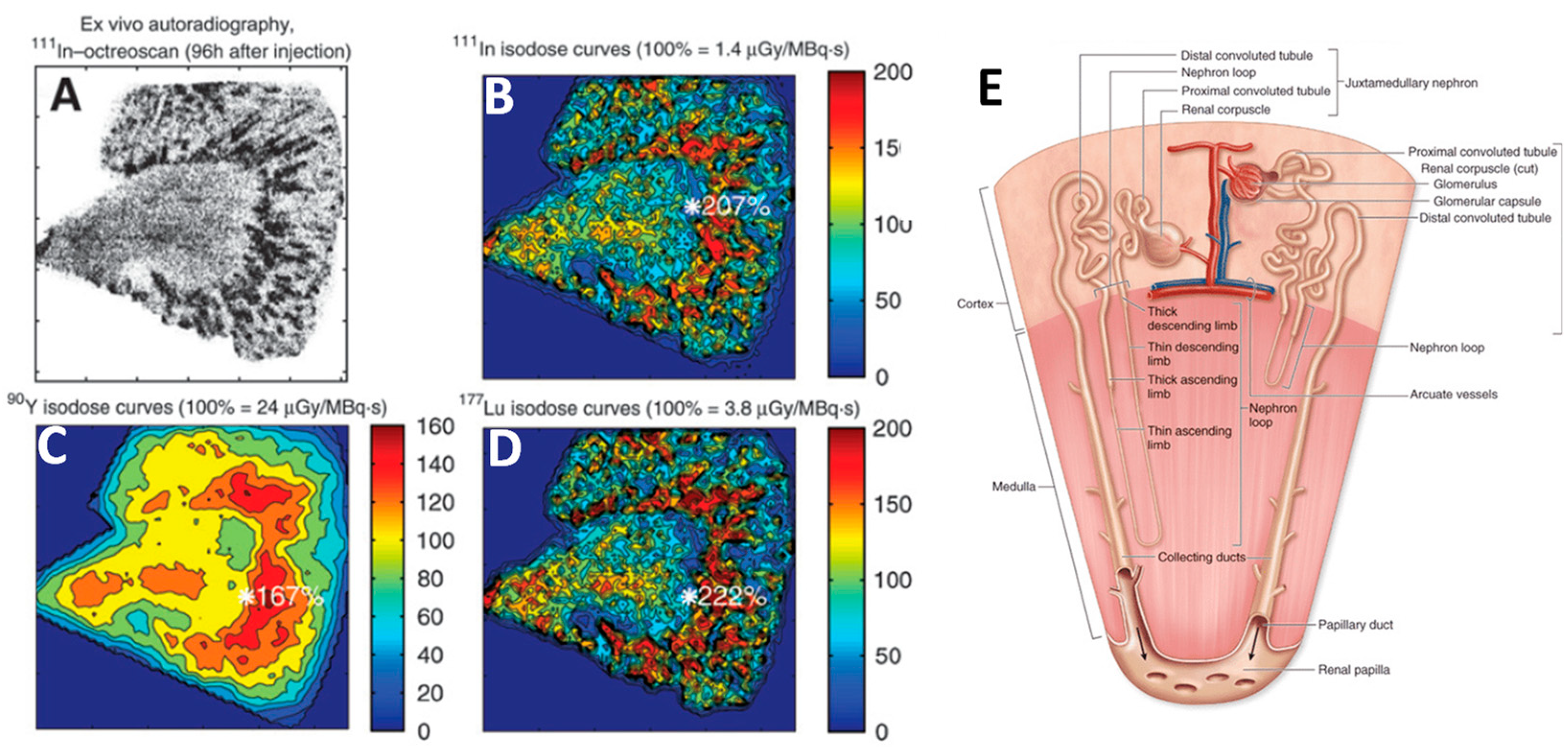
In all PRRT studies, i.e., 111In-DTPA-octreotide SPECT [15], 86Y-DOTATOC PET [12] and 177Lu-DOTATATE SPECT [16], showed that the kidney uptake is localized in the cortex such as initially observed by Hammond et al. in planar 111In-DTPA-octreotide scintigraphy [17]. Intra-patient 86Y-DOTATOC PET studies proved that amino acid infusion significantly reduced the renal reuptake [6]. By competing with the megalin/cubilin complex on the apical membrane of proximal tubular cells (PTCs), basic amino acids, such as L-lysine and L-arginine, can reduce by ≈50% the reuptake of the radiolabeled peptide. The other fraction is taken up by the PTCs by fluid-phase endocytosis, that is not influenced by the presence of high amounts of basic amino acids [18,19]. Studies in knock-out rat provided evidence that megalin is essential for renal tubule reabsorption of the peptide [20].
Ex vivo autoradiography of healthy kidney tissue, from patients who received 111In-DTPA-octreotide before nephrectomy (Figure 2A), showed an uptake gradient decreasing from the inner to the outer cortex boundary [21]. As the radiosensitive glomerulus is about 6 mm far from the inner boundary (Figure 2E), its crossfire irradiation by the activity taken up by the tubules will strongly depend on the radionuclide beta range, as clearly shown in the Monte Carlo (MC) isodose simulations (Figure 2B,C). These MC simulations explain why the first limiting tissue is the kidney with 90Y-DOTATOC and the red marrow in 177Lu-DOTATATE PRRT, respectively (see Section 3).
3. Red Marrow Dosimetry and Toxicity
A highly variable red marrow inter-patient uptake in PRRT was evidenced early in 2005 during the 86Y-DOTATOC phase I 86Y-SMT-487 trial, which used state-of-the-art PET imaging [23]. Furthermore, this red marrow uptake was intra-patient, correlated to that measured with 111In-DTPA-octreotide by SPECT [24]. This was overlooked by the nuclear medicine community, who argued that RM uptake was not visible in 90Y bremsstrahlung or 177Lu SPECT [25,26]. The case appeared to be solved in 2017 when the LutatheraTM insert package, which states that establishing red marrow dosimetry is useless in predicting observed toxicity, was agreed upon by the FDA and the EMA [27].
These past few years, several teams using state-of-the-art SPECT/CT demonstrated clear red marrow uptake of 177Lu in 177Lu-DOTATATE therapy [16], the dosimetry based on enabling some toxicity prediction [28,29,30]. The observed red marrow dosimetry was about fourfold that of the blood-based method used in the Netter study [10], explaining why about 10% Grade 3–4 hematological toxicity was observed in this study.
Such red marrow uptake could appear surprising, given the high DOTA affinity and stability for yttrium and for lutetium. However, in the transchelation competition with transferrin, DOTA is just a passive and naïve chelator stroke by an active and cunning thief. Iron is a vital compound for mammalians and evolution spent hundreds of millions of years to improve transferrin, versus a few decades for chemists.
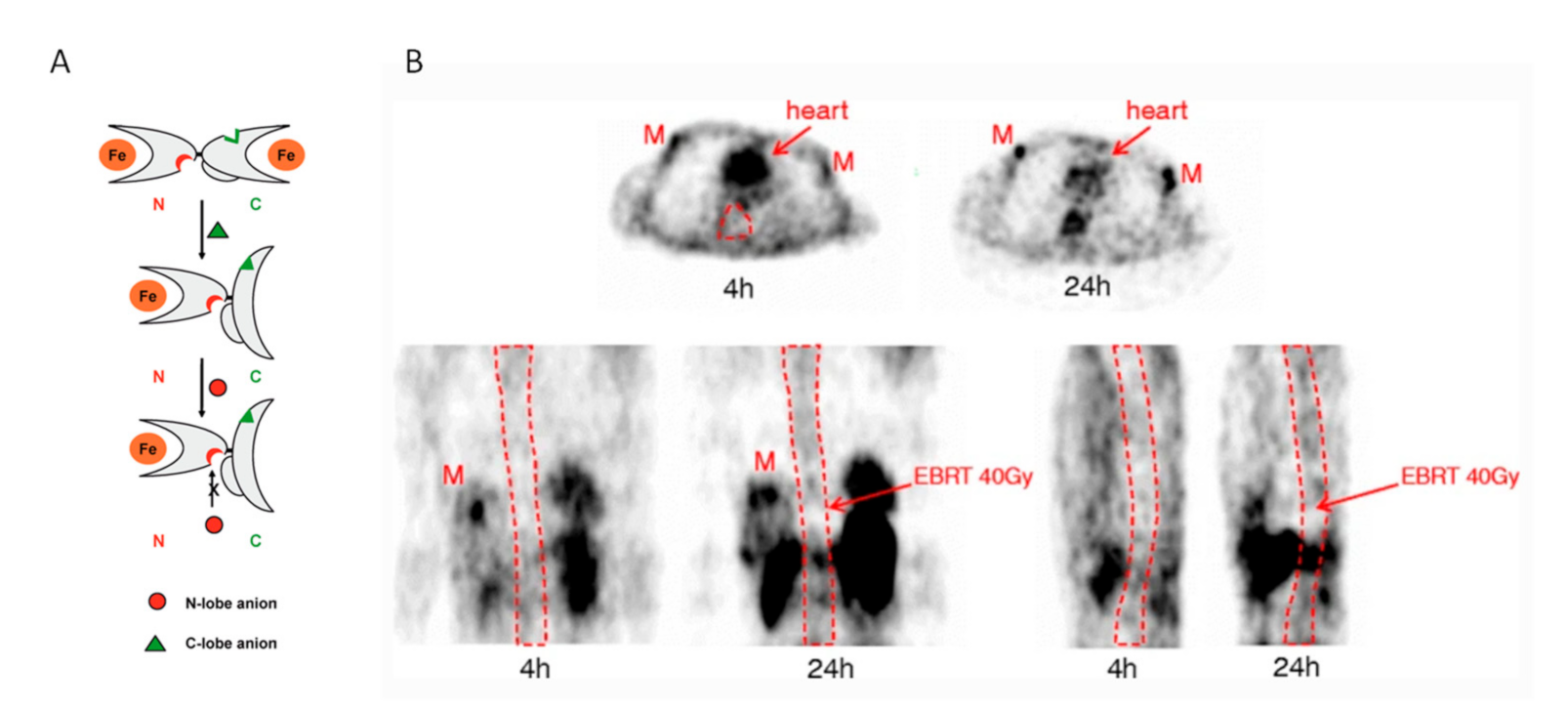
Transferrin is a protein having two active lobes (Figure 3A) [31]. In the iron-free state, i.e., apo-transferrin, the N-lobe and the C-lobe are open, ready to catch a metallic ion. When a metallic ion enters a lobe, the lobe closes and surrounds the ion as a result of the Van der Waals forces. In this state, no other external force can easily remove the ion from the locked lobe. When an appropriate anion binds to the corresponding active site, the lobe opens and releases the metallic ion. This key-padlock mechanism ensures that iron will be released to the appropriate cells and not elsewhere in the body.
The ion transferrin release is an active process, along with the ion catching one. Inorganic chelators, such as DOTA, have to wait for the release of a metal ion by another chelator in order to trap it, which is rare from a good competitor. In contrary, kinetics and spectrometry studies evidenced that transferrin can create a ternary (or mixed) complex with the initial metal–chelator complex [32]. During the life of this ternary complex, the metal ion is transferred from the chelator to the transferrin metal binding site, likely by the Van der Waals forces. Many in vitro competition studies between transferrin and DOTA evidenced the transferrin superiority [24,33]. In vitro data using plasma from subjects injected with 111In-pentetreotide demonstrated that after 7 days, the radioactive metal was effectively bound to transferrin [34].
A recent study in humans [35] showed that only 23% and 2% of 177Lu-DOTATATE remain intact after 24 h and 96 h post-injection, respectively. Figure 3B clearly illustrates the uptake difference between the tumor receptor-based mechanism and the transferrin transport to red marrow mechanism observed in the 86Y-SMT-487 study [24]. Directly during the first pass, the 86Y-DOTATATE binds to the tumor receptors, resulting in a strong uptake within 4 h pi, while it takes a much longer time for the transferrin to catch the metal and to deliver it to the red marrow cells. The 4 and 24 h images proved the red marrow activity behavior in the opposition phase versus the blood pool, which makes the blood-based red marrow dosimetry method unlikely to be physiologically adequate. Table 1 shows red marrow dosimetry assessments and dose–toxicity correlations reported in the recent literature.
Using 4 SPECT/CT performed after the first and second cycles, Santoro et al. [28] evaluated the organs at risk in 12 patients treated with 177Lu-DOTATATE. The mean dosimetry for kidney and red marrow was 0.43 ± 0.13 mGy/MBq and 0.04 ± 0.02 mGy/MBq, respectively. As the maximal tolerated dose for red marrow is about tenfold lower than that of kidney [24], this explains why hematological toxicity is the limiting factor in 26% of individually optimized 177Lu PRRT [36].
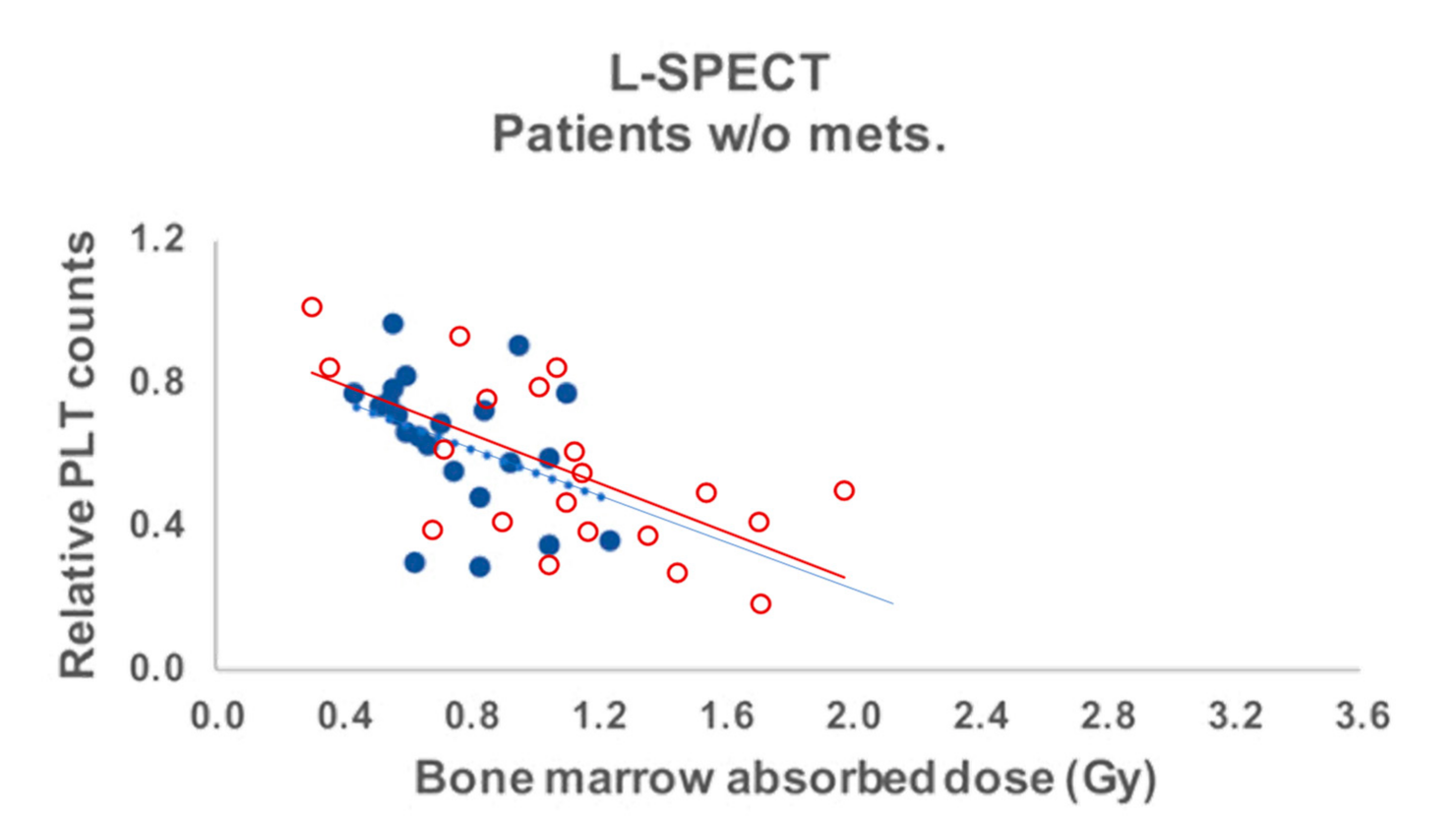
Using a SPECT/CT-planar hybrid method, Hagmarker et al. [29] in 177Lu-DOTATATE therapy found similar red marrow dosimetry, i.e., 0.06 (0.02–0.12) mGy/MBq in 22 patients without skeletal metastases. They observed a dose–platelet counts nadir relationship (Figure 4) perfectly in line with that observed in the 90Y-DOTATOC clinical phase I trial using 86Y-DOTATOC PET-based red marrow dosimetry [23,24].
In 200 patients treated with 177Lu-DOTATATE, Garsk et al. [36] observed fourfold lower mean blood-based red marrow dosimetry than that observed in the two reported SPECT studies, i.e., 0.016 mGy/MBq, which was unable to predict the hematological toxicity observed in 40 patients. Page et al. [37] compared blood-based and SPECT/CT-based red marrow dosimetry in 11 patients treated with 177Lu-DOTATATE and observed the same fourfold ratio.
The results of these six studies [28,29,30,35,36,37] urge for using post-cycles SPECT/CT-based red marrow dosimetry for all 177Lu therapies. With optimized imaging and reconstruction methods of SPECT/CT, these studies provide evidence that direct RM uptake-based dosimetry clearly outperforms the blood-based estimations, as advocated in the Luthatera package insert. One must keep in mind that the maximal red marrow tolerable dose is about tenfold lower than that of other tissues. Thus, a long duration, i.e., >30 min, dual-head SPECT is required to accurately assess the red marrow uptake at several timepoints. Red marrow activity should be measured on the thoracic vertebras: the region with the lowest attenuation and without surrounding tissues with high uptake, such as the liver, spleen or kidneys, that can produce long tail artefacts in reconstructed slices. Fortunately, nowadays, a single SPECT/CT scan encompass the thorax and the kidneys. Clearly, state-of-the-art imaging capacities as available now can help improve this paradigm of RM dosimetry based on imaging, rather than on blood activity.
4. 177Lu-90Y PRRT Tandem Therapy: A Bi-Orthogonal Synergy
Hobbs et al. [38] introduced the “orthogonal radionuclides” concept to promote tandem therapy with radionuclides taken up by different tissues and thus presenting different toxicities. Such tandem allows increasing the tumor dose by splitting the unwanted irradiation between different organs, as similarly performed in EBRT by rotating the beam source around the targeted tumor.
Comparing toxicities of 177Lu-DOTATATE and 90Y-DOTATOC therapies is very challenging considering the sparse information provided in the clinical trials publications. In the Netter phase III study [10], in 116 patients receiving four repeated injections of 7.4 GBq every 8 weeks, 0.4% and 11% underwent a renal and hematological toxicity of grade 3 or 4, respectively. In the phase II 90Y-DOTATOC study [39] in 1109 patients receiving in average 2.5 cycles of 3.7 GBq/m2, 9.2% and 12.8% experienced a renal and hematological toxicity of grade 3 or 4, respectively. However, the frequency of this hematological toxicity cannot be directly compared; indeed, assuming similar uptakes, the 90Y protocol delivered a much higher tissue dose than that of 177Lu (Table 2). The hematological to renal toxicity ratio is about twentyfold higher for the 177Lu-DOTATATE therapy.
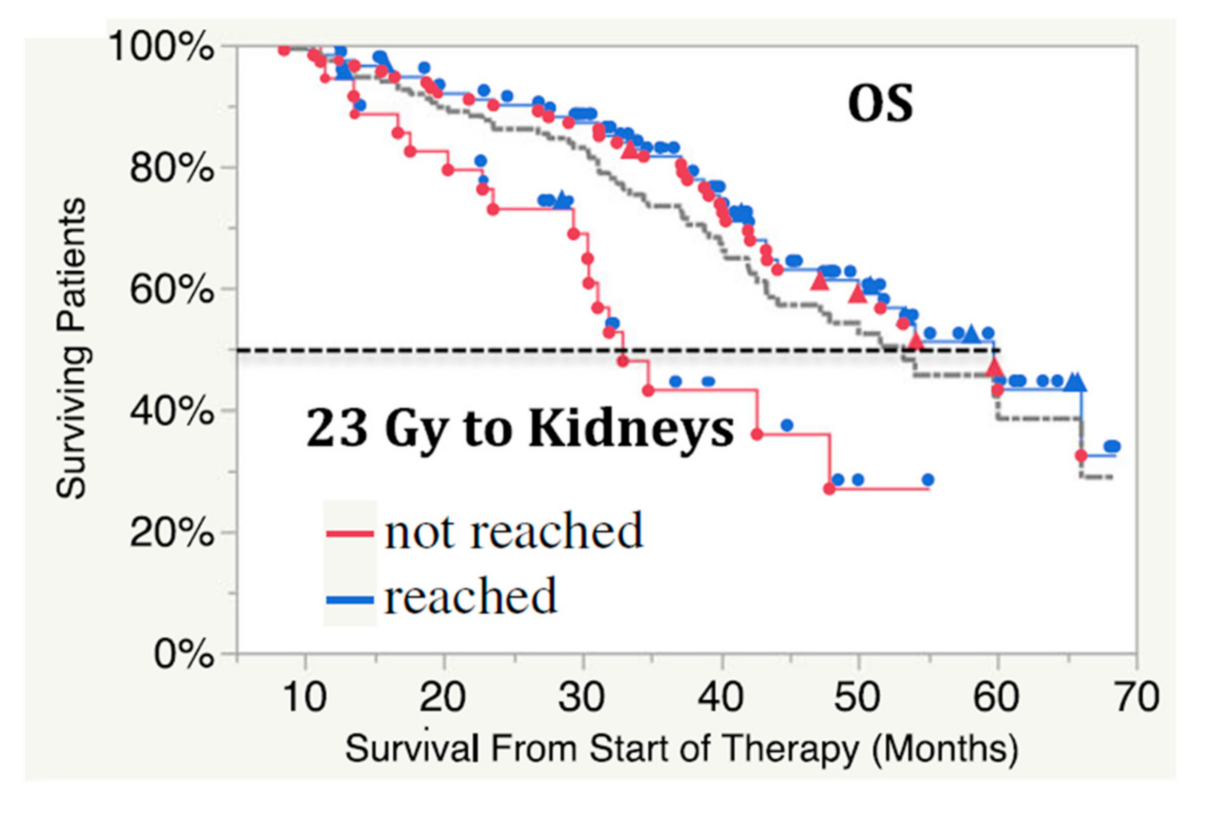
Regarding dosimetry-based studies, in individualized 177Lu-DOTATATE study aiming to deliver 23 Gy to the kidney in 154 patients, 26% presented a hematological toxicity, halting the therapy [36], while this event occurs only in 1 patient out of 60 in the individualized 90Y-DOTATOC study aiming to deliver 27 Gy to the kidney [7]. Again, a twentyfold higher prevalence of hematological toxicity is observed in 177Lu-DOTATATE therapy.
This much higher prevalence of hematological toxicity in 177Lu-DOTATATE therapy is in line with the low in vivo stability of this compound: only 23% and 2% of 177Lu-DOTATATE remain intact after 24 h and 96 h post-injection in patients [35], whereas 90% of 86Y-DOTATOC remains intact 5 h post-injection in primates [40]. Intuitively, it makes sense that the larger electron orbital of 177Lu makes it more sensitive to external Van der Waals forces coming from an open transferrin lobe. Note that, as transferrin is not excreted by the kidneys, radionuclide to protein binding analysis in urine is not appropriate to evaluate the in vivo compound stability. In vitro transchelation competition with apo-transferrin could also be biased, considering that in vivo, apo-transferrin is continuously renewed by the release of the metal ion in the red marrow. Such in vitro studies thus have to be performed with a huge apo-transferrin overload. Last, caution is also needed with in vivo rodent stability studies, considering that experiments proved different iron binding and release properties compared to humans [41]; this could also hold true for yttrium and lutetium.
All these facts clearly show that the orthogonal toxicity concept applies to the couple 177Lu-DOTATATE and 90Y-DOTATOC for which the prime tissue at risk is the red marrow and the kidney, respectively. This feature alone should be sufficient to promote the tandem approach as a new standard for PRRT therapy.
Last, but not least, this tandem is also orthogonal regarding the tumor response (justifying the bi-orthogonal appellation): by its short beta range, 177Lu is efficient to deliver high doses in sub-centimetric tumors, whereas the 90Y beta, with its one cm range, is more efficient to cross-irradiate low vascularized regions often present in larger tumors [42,43].
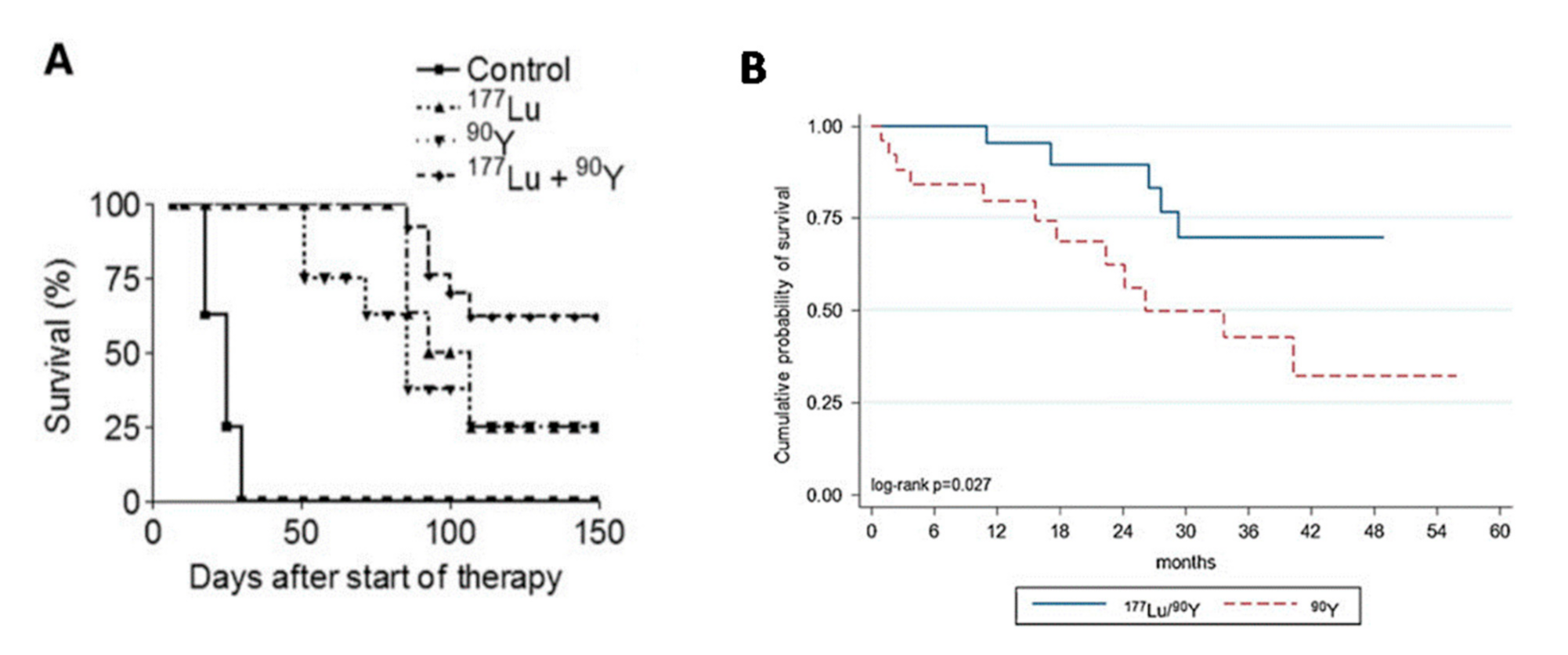
This dose–response synergy was already observed in 2005 in a preclinical model [44]. Pancreatic cancer cells were successively grafted, i.e., spaced by 3 weeks, in the two opposite flanks of rats, resulting in rats bearing a small (≈0.5 cm2) and a large (≈8 cm2) tumor. Rats were split into four groups of about 12 individuals. Survival was impressively higher in rats treated with the 177Lu-DOTATATE and 90Y-DOTATOC tandem than that of rats treated with only one radionuclide (Figure 5A).
Kunikowska et al. [45] compared overall survival (OS) between single 90Y-DOTATOC therapy and 90Y-177Lu tandem therapy. The patients were not randomly drawn: the first 25 consecutive patients were treated with 90Y alone (7.4 GBq/m2), and the following 25 consecutive patients were treated with the 90Y-177Lu tandem (3.7–3.7 GBq/m2). However, the same patient enrollment criteria were chosen for both groups. As in the rat study, the OS was impressively better in the tandem group, especially that, when assuming similar uptake, the tandem delivers absorbed doses 30% lower than that of the 90Y alone using this activity protocol.
In this study, the tandem was given together in two or three cycles, which is not the right strategy: the well-vascularized large tumor region takes fewer radionuclides in the following cycle due to the additional 177Lu irradiation eradicating cells which uptake the peptide. The best strategy is to first perform the 90Y cycles to benefit from the high uptake of vascularized regions to cross-irradiate the other tumor regions, then to end up with a 177Lu cycle to efficiently irradiate, and hopefully eradicate, small metastases [46].
5. Individual PRTT Optimization Planning
Multi-cycle PRRT is well adapted to individualized therapy planning as the first cycle delivered dose is safe for all patients. Afterwards, post-cycle dosimetry can be performed to optimize the activity to be injected in the following cycles. Note that if 98Ga-DOTATATE PET is of prime interest to select a candidate for the PRRT therapy, it is useless for dosimetry estimation given its too short half-life. In 90Y-DOTATOC therapy, phantom and patient studies proved 90Y PET imaging providing an accurate kidney dose estimation [47], while medium energy collimator SPECT/CT is well adapted for 177Lu-DOTATATE [16], provided that the acquisition time is long enough.
PRRT dosimetry requires at least two imaging time points, as tissue activity curves exhibit a bi-exponential asymmetric bell shape. This feature renders proposed single time-point estimates inaccurate [48], which is only for a single exponential starting from t = 0, the model used to propose it [49]. One time point after the maximal uptake is needed, e.g., 24 h post-injection, and another time point somewhere around one effective half-life, i.e., 48 or 72 h post 90Y injection and 5 to 8 days post 177Lu injection.
Only the two tissues at risk have to be imaged, i.e., the thoracic vertebrae and the kidneys, which can be performed with two PET/CT positions for 90Y and with one single SPECT/CT position for 177Lu. Planar imaging and combined planar and hybrid SPECT/CT should be avoided given the superimposition of the residual blood-pool activity for red marrow and of the liver and of the spleen activity for the kidneys. Many physicians think it is mandatory to use state-of-the-art TOF-PET/CT to perform tumor staging or follow-up! It is time to tackle claims that short-duration, whole-body planar scan is sufficient to perform dosimetry. By always trying to simplify dosimetry to satisfy this claim, medical physics experts (MPE) are left with poor quality data for accurate dosimetry, which reinforces the common belief that dosimetry is useless.
Menda et al. [50] conducted a prospective post-cycle renal dosimetry using 90Y-bremsstrahlung SPECT/CT in 25 patients with neuroendocrine tumors. A 90Y TOF-PET/CT [47] was used at the first time for bremsstrahlung SPECT/CT calibration purposes. The study confirmed the very high variability of inter-patient renal dosimetry, as already observed using 86Y-DOTATOC PET [8], advocating the interest to individually optimize the injected 90Y activity.
Almost twenty years after the individualized 90Y-SMT-487 trial [23], Del Petre et al. [51], Sundlov et al. [52] and Garske-Roman et al. [36] performed SPECT/CT-based individualized planning in 177Lu-DOTATATE therapy in 52, 51 and 200 patients aiming at a renal BED = 27 Gy, D = 23 Gy and D = 23 Gy, respectively. They demonstrated that applying the standard recommendation of four 7.4 GBq cycles results in undertreating 85%, 73% and 49% of the patients.
6. Smart Optimized Tandem Therapy Design: A Proposal
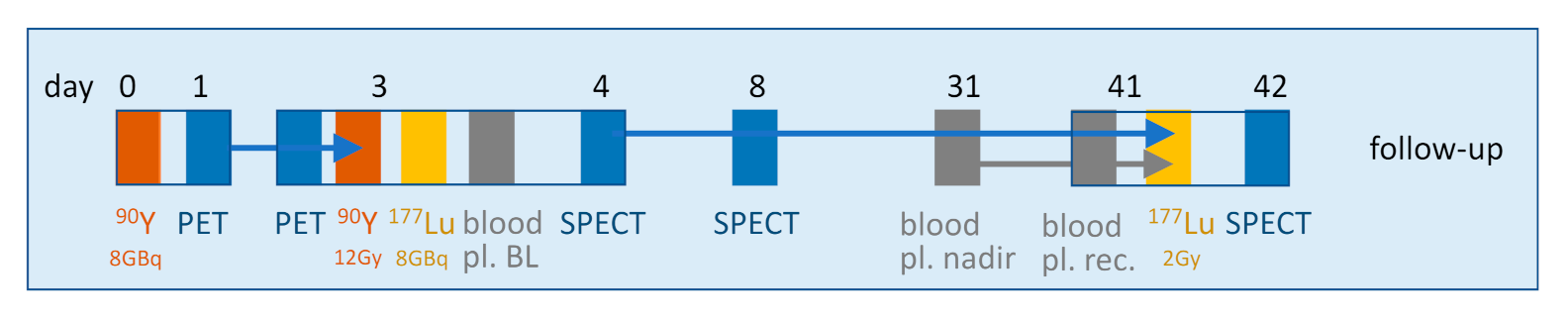
As in tandem therapy, the potential toxicity is split between two different tissues, and the activity fractionation can be reduced versus a single radionuclide therapy, which has the benefit to reduce aggressive tumors regrowth between cycles. As a result, a smart full optimized tandem therapy, fractionated in three cycles, can be proposed (Figure 7). It requires only four patient visits to the hospital, three amino acid infusions and five imaging sessions.
At day 0, a fixed activity of 90Y-DOTATOC/TATE is injected with amino acid infusion. The following day, before releasing the patient from the hospital, a 90Y kidney 30 min-PET/CT is performed.
At day 3, a 90Y kidneys 30 min-PET/CT is performed to compute the kidney dosimetry in order to assess the residual 90Y activity needed to reach a BED of 15 Gy to the kidneys. Afterwards, this 90Y-DOTATOC/TATE activity complement is injected to the patient together with a fixed 177Lu-DOTATATE activity along with amino acid infusion, and a blood sample is withdrawn to obtain the cell count base line. As this session corresponds to the last 90Y cycle, co-injection of 177Lu does not impact the 90Y cross irradiation. Note that with regard to the effective kidney half-life (≈30 h, [8]), the initial dose rate is already reduced by a factor ≈5, corresponding to an effective dose fractionation. The following day, before releasing the patient, a 177Lu thorax-abdomen 30 min dual-head SPECT/CT is performed. Additionally, for a highly valuable scientific point of view, a blood sample could be taken to assess the relative binding of 177Lu and 90Y to transferrin in the same patient at the same time using size-exclusion chromatography, with appropriate MW standards.
At day 8, a 177Lu thorax-abdomen SPECT/CT is performed, and the kidney and RM dosimetry is computed. The kidney dosimetry should be computed using the Sfactors taking into account the 90Y and 177Lu beta range for the cross irradiation of the glomerulus by the taking up tubules [21]. At day 31, a blood sample is taken by the treating team or by the general practitioner to estimate the blood cell count nadir.
At day 41, a blood sample is withdrawn to check the cell count recovery, and depending on the values at nadir and recovery, a 177Lu-DOTATATE activity complement is injected, satisfying, for the whole therapy, the two limits: D < 2 Gy to the red marrow and BED < 31 Gy to the kidneys. Note that the physician has the competence to modulate these limits according to the patient status and to his cell count recovery. The following day, before releasing the patient, a thorax-abdomen 177Lu SPECT/CT is performed.
Afterwards, the patient undergoes the normal follow-up.
7. Conclusions
In recent years, many studies provided evidence of the huge benefit for the patient outcome to individually optimize the activity to be injected. Furthermore, although not performed along an optimized planning, recent studies have also established the importance to profit of the bi-orthogonal toxicity-response patterns of the tandem 90Y-DOTATOC-177Lu-DOTATATE. There is no doubt that the combination of these two approaches, as proposed in Figure 7, will still improve the patient outcome and will push PRRT to a real curative intent.
However, last year, the EANM published a position paper [53] on article 56 of the Council Directive 2013/95 Euratom, which required an individualized optimization planning in all radiotherapies. This position paper aims to provide guidance on how to interpret the Directive and states that 177Lu-DOTATATE, used according to the package insert, is a standard therapy not requiring any individualized planning, which is scientifically questionable considering the present review.
However, let us recall that legally, the MPE responsibility is framed by the corresponding national transposition of the directive. However, the MPE or practitioner cannot be prosecuted for having followed Directive 2013/95 rather than the national implementation. Indeed, as the Directive 2013/95 provisions are unconditional and sufficiently clear and precise, the directive has direct effects, and any individual can invoke its provisions in front of any national court [54]. The European Court of Justice’s jurisprudence has extended this principle to cases with incorrect implementation of a directive [55].
Author Contributions
Conceptualization, S.W. and F.J.; methodology, S.W. and F.J.; formal analysis, S.W. and F.J.; investigation, S.W. and F.J.; resources, S.W. and F.J.; writing—original draft preparation, S.W. and F.J.; writing—review and editing, S.W. and F.J.; supervision, S.W. and F.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data came from published articles.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Krenning, E.P.; De Jong, M.; Kooij, P.P.; Breeman, W.A.; Bakker, W.H.; De Herder, W.W.; Van Eijck, C.H.; Kwekkeboom, D.J.; Jamar, F.; Pauwels, S.; et al. Radiolabelled somatostatin analogue(s) for peptide receptor scintigraphy and radionuclide therapy. Ann. Oncol. 1999, 10, S23–S30. [Google Scholar] [CrossRef]
- Laster, B.H.; Shani, G.; Kahl, S.B.; Warkentien, L. The biological effects of Auger electrons compared to α-particles and Li ions. Acta Oncol. 1996, 35, 917–923. [Google Scholar] [CrossRef]
- De Jong, M.; Valkema, R.; Jamar, F.; Kvols, L.K.; Kwekkeboom, D.J.; Breeman, W.A.; Bakker, W.H.; Smith, C.; Pauwels, S.; Krenning, E.P. Somatostatin receptor-targeted radionuclide therapy of tumors: Preclinical and clinical findings. SEM Nucl. Med. 2002, 32, 133–140. [Google Scholar] [CrossRef]
- Barone, R.; Walrand, S.; Konijnenberg, M.; Valkema, R.; Kvols, L.K.; Krenning, E.P.; Pauwels, S.; Jamar, F. Therapy using labelled somatostatin analogues: Comparison of the absorbed doses with 111In-DTPA-D-Phe1-octreotide and yttrium-labelled DOTA-D-Phe1-Tyr3-octreotide. Nucl. Med. Com. 2008, 29, 283–290. [Google Scholar] [CrossRef]
- Otte, A.; Herrmann, R.; Heppeler, A.; Behe, M.; Jermann, E.; Powell, P.; Maecke, H.R.; Muller, J. Yttrium-90 DOTATOC: First clinical results. Eur. J. Nucl. Med. 1999, 26, 1439–1447. [Google Scholar] [CrossRef]
- Jamar, F.; Barone, R.; Mathieu, I.; Walrand, S.; Labar, D.; Carlier, P.; De Camps, J.; Schran, H.; Chen, T.; Smith, M.C.; et al. 86 Y-DOTA 0-d-Phe 1-Tyr 3-octreotide (SMT487)—A phase 1 clinical study: Pharmacokinetics, biodistribution and renal protective effect of different regimens of amino acid co-infusion. Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Valkema, R.; Pauwels, S.A.; Kvols, L.K.; Kwekkeboom, D.J.; Jamar, F.; de Jong, M.; Barone, R.; Walrand, S.; Kooij, P.P.; Bakker, W.H.; et al. Long-term follow-up of renal function after peptide receptor radiation therapy with 90Y-DOTA0, Tyr3-octreotide and 177Lu-DOTA0, Tyr3-octreotate. J. Nucl. Med. 2005, 46, 83S–91S. [Google Scholar]
- Barone, R.; Borson-Chazot, F.; Valkema, R.; Walrand, S.; Chauvin, F.; Gogou, L.; Kvols, L.K.; Krenning, E.P.; Jamar, F.; Pauwels, S. Patient-specific dosimetry in predicting renal toxicity with 90Y-DOTATOC: Relevance of kidney volume and dose rate in finding a dose–effect relationship. J. Nucl. Med. 2005, 46, 99S–106S. [Google Scholar]
- Kwekkeboom, D.J.; Bakker, W.H.; Kam, B.L.; Teunissen, J.J.; Kooij, P.P.; De Herder, W.W.; Feelders, R.A.; Van Eijck, C.H.; De Jong, M.; Srinivasan, A.; et al. Treatment of patients with gastro-enteropancreatic (GEP) tumours with the novel radiolabelled somatostatin analogue [177Lu-DOTA(0),Tyr(3)]octreotate. Eur. J. Nucl. Med. 2003, 30, 417–422. [Google Scholar] [CrossRef] [Green Version]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 trial of 177Lu-Dotatate for midgut neuroendocrine tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef]
- Snyder, W.S.; Ford, M.R.; Warner, G.G.; Watson, S. MIRD Pamphlet no. 11: S, Absorbed Dose per unit Cumulated Activity for Selected Radionuclides and Organs; Society of Nuclear Medicine: New York, NY, USA, 1975. [Google Scholar]
- Walrand, S.; Jamar, F.; Mathieu, I.; De Camps, J.; Lonneux, M.; Sibomana, M.; Labar, D.; Michel, C.; Pauwels, S. Quantitation in PET using isotopes emitting prompt single gammas: Application to yttrium-86. Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 354–361. [Google Scholar] [CrossRef]
- Wessels, B.W.; Konijnenberg, M.W.; Dale, R.G.; Breitz, H.B.; Cremonesi, M.; Meredith, R.F.; Green, A.J.; Bouchet, L.G.; Brill, A.B.; Bolch, W.E.; et al. MIRD pamphlet no. 20: The effect of model assumptions on kidney dosimetry and response—Implications for radionuclide therapy. J. Nucl. Med. 2008, 49, 1884–1899. [Google Scholar] [CrossRef] [Green Version]
- McParland, B.J. Nuclear Medicine Radiation Dosimetry: Advanced Theoretical Principles; Springer: Lodon, UK, 2010; pp. 427–430. [Google Scholar]
- Helisch, A.; Förster, G.J.; Reber, H.; Buchholz, H.G.; Arnold, R.; Göke, B.; Weber, M.M.; Wiedenmann, B.; Pauwels, S.; Haus, U.; et al. Pre-therapeutic dosimetry and biodistribution of 86 Y-DOTA-Phe 1-Tyr 3-octreotide versus 111 In-pentetreotide in patients with advanced neuroendocrine tumours. Eur. J. Nucl. Med. Mol. Imaging 2004, 31, 1386–1392. [Google Scholar] [CrossRef]
- Rydén, T.; Lagerlöf, J.H.; Hemmingsson, J.; Marin, I.; Svensson, J.; Båth, M.; Gjertsson, P.; Bernhardt, P. Fast GPU-based Monte Carlo code for SPECT/CT reconstructions generates improved 177 Lu images. Ejnmmi Phys. 2018, 5, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammond, P.J.; Wade, A.F.; Gwilliam, M.E.; Peters, A.M.; Myers, M.J.; Gilbey, S.G.; Bloom, S.R.; Calam, J. Amino acid infusion blocks renal tubular uptake of an indium-labelled somatostatin analogue. Brit. J. Cancer. 1993, 67, 1437–1439. [Google Scholar] [CrossRef] [Green Version]
- Barone, R.; Pauwels, S.; De Camps, J.; Krenning, E.P.; Kvols, L.K.; Smith, M.C.; Bouterfa, H.; Devuyst, O.; Jamar, F. Metabolic effects of amino acid solutions infused for renal protection during therapy with radiolabelled somatostatin analogues. Nephr Dial. Transp. 2004, 19, 2275–2281. [Google Scholar] [CrossRef] [PubMed]
- Barone, R.; Van Der Smissen, P.; Devuyst, O.; Beaujean, V.; Pauwels, S.; Courtoy, P.J.; Jamar, F. Endocytosis of the somatostatin analogue, octreotide, by the proximal tubule-derived opossum kidney (OK) cell line. Kidney Int. 2005, 67, 969–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Jong, M.; Barone, R.; Krenning, E.; Bernard, B.; Melis, M.; Visser, T.; Gekle, M.; Willnow, T.E.; Walrand, S.; Jamar, F.; et al. Megalin is essential for renal proximal tubule reabsorption of 111In-DTPA-octreotide. J. Nucl. Med. 2005, 46, 1696–1700. [Google Scholar] [PubMed]
- Konijnenberg, M.; Melis, M.; Valkema, R.; Krenning, E.; De Jong, M. Radiation dose distribution in human kidneys by octreotides in peptide receptor radionuclide therapy. J. Nucl. Med. 2007, 48, 134–142. [Google Scholar]
- Available online: https://www.pinterest.com/pinklb/urology-nursing/ (accessed on 1 August 2021).
- Pauwels, S.; Barone, R.; Walrand, S.; Borson-Chazot, F.; Valkema, R.; Kvols, L.K.; Krenning, E.P.; Jamar, F. Practical dosimetry of peptide receptor radionuclide therapy with 90Y-labeled somatostatin analogs. J. Nucl. Med. 2005, 46, 92S–98S. [Google Scholar]
- Walrand, S.; Barone, R.; Pauwels, S.; Jamar, F. Experimental facts supporting a red marrow uptake due to radiometal transchelation in 90 Y-DOTATOC therapy and relationship to the decrease of platelet counts. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 1270–1280. [Google Scholar] [CrossRef]
- Hartmann, H.; Oehme, L.; Kotzerke, J. 86 Y-DOTATOC uptake in red marrow is not routinely visible. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 1384. [Google Scholar] [CrossRef] [PubMed]
- Forrer, F.; Krenning, E.P.; Kooij, P.P.; Bernard, B.F.; Konijnenberg, M.; Bakker, W.H.; Teunissen, J.J.; de Jong, M.; van Lom, K.; de Herder, W.W.; et al. Bone marrow dosimetry in peptide receptor radionuclide therapy with [177 Lu-DOTA 0, Tyr 3] octreotate. Eur. J. Nucl. Med. Mol. Imaging 2009, 36, 1138–1146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Available online: https://www.ema.europa.eu/en/documents/product-information/lutathera-epar-product-information_en.pdf (accessed on 1 August 2021).
- Santoro, L.; Mora-Ramirez, E.; Trauchessec, D.; Chouaf, S.; Eustache, P.; Pouget, J.P.; Kotzki, P.O.; Bardiès, M.; Deshayes, E. Implementation of patient dosimetry in the clinical practice after targeted radiotherapy using [177 Lu-[DOTA0, Tyr3]-octreotate. Eur. J. Nucl. Med. Mol. Imaging 2018, 8, 103. [Google Scholar]
- Hagmarker, L.; Svensson, J.; Rydén, T.; van Essen, M.; Sundlöv, A.; Gleisner, K.S.; Gjertsson, P.; Bernhardt, P. Bone Marrow Absorbed Doses and Correlations with Hematologic Response During 177Lu-DOTATATE Treatments Are Influenced by Image-Based Dosimetry Method and Presence of Skeletal Metastases. J. Nucl. Med. 2019, 60, 1406–1413. [Google Scholar] [CrossRef] [Green Version]
- Tipping, J.; Page, E.; Calvert, N.; Hamilton, D.; Cullen, D.; Price, E.; Pells, S.; Needham, G.; Manoharan, P. Improved prediction of haematological toxicity during 177Lu Lu-DOTA-TATE therapy by optimising serial SPECT-CT red marrow dosimetry. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, S239. [Google Scholar]
- Hamilton, D.H.; Turcot, I.; Stintzi, A.; Raymond, K.N. Large cooperativity in the removal of iron from transferrin at physiological temperature and chloride ion concentration. J. Biol. Inorg. Chem. 2004, 9, 936–944. [Google Scholar] [CrossRef]
- Bates, G.W.; Billups, C.; Saltman, P. The Kinetics and Mechanism of Iron (III) Exchange between Chelates and Transferrin II. The presentation and removal with ethylenediaminetetraacetate. J. Biol. Chem. 1967, 242, 2816–2821. [Google Scholar] [CrossRef]
- EW Price. Synthesis, Evaluation, and Application of New Ligands for Radiometal Based Radiopharmaceuticals. Ph.D. Thesis, University British Columbia, Vancouver, BC, Canada, 2014. Available online: https://open.library.ubc.ca/cIRcle/collections/ubctheses/24/items/1.0103411 (accessed on 1 August 2021).
- Barone, R.; Walrand, S.; Leveque, P.; Pauwels, S.; Jamar, F. Red marrow toxicity after therapy with radiolabelled somatostatin analogues: A possible role of plasma protein binding. Eur. J. Nucl. Med. 2003, 30, 232. [Google Scholar]
- Lubberink, M.; Wilking, H.; Öst, A.; Ilan, E.; Sandström, M.; Andersson, C.; Fröss-Baron, K.; Velikyan, I.; Sundin, A. In vivo instability of 177Lu-DOTATATE during peptide receptor radionuclide therapy. J Nucl. Med. 2020, 61, 1337–1340. [Google Scholar] [CrossRef]
- Garske-Roman, U.; Sandström, M.; Fröss Baron, K.; Lundin, L.; Hellman, P.; Welin, S.; Johansson, S.; Khan, T.; Lundqvist, H.; Eriksson, B.; et al. Prospective observational study of 177Lu-DOTA-octreotate therapy in 200 patients with advanced metastasized neuroendocrine tumours (NETs): Feasibility and impact of a dosimetry-guided study protocol on outcome and toxicity. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 970–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, E.; Tipping, J.; Hamilton, D.; Cullen, D.; Calvert, N.; Pietras, B.; Pells, S.; Price, E. Red marrow dosimetry for PRRT: Blood versus 3D image based methods of activity measurement.
- Hobbs, R.F.; Wahl, R.L.; Frey, E.C.; Kasamon, Y.; Song, H.; Huang, P.; Jones, R.J.; Sgouros, G. Radiobiologic optimization of combination radiopharmaceutical therapy applied to myeloablative treatment of non-Hodgkin lymphoma. J. Nucl. Med. 2013, 54, 1535–1542. [Google Scholar] [CrossRef] [Green Version]
- Imhof, A.; Brunner, P.; Marincek, N.; Briel, M.; Schindler, C.; Rasch, H.; Mäcke, H.R.; Rochlitz, C.; Müller-Brand, J.; Walter, M.A. Response, survival, and long-term toxicity after therapy with the radiolabeled somatostatin analogue [90Y-DOTA]-TOC in metastasized neuroendocrine cancers. J. Clin. Oncol. 2011, 29, 2416–2423. [Google Scholar] [CrossRef]
- Rösch, F.; Herzog, H.; Stolz, B.; Brockmann, J.; Köhle, M.; Mühlensiepen, H.; Marbach, P.; Müller-Gärtner, H.W. Uptake kinetics of the somatostatin receptor ligand [86 Y] DOTA-d Phe 1-Tyr 3-octreotide ([86 Y] SMT487) using positron emission tomography in non-human primates and calculation of radiation doses of the 90 Y-labelled analogue. Eur. J. Nucl. Med. 1999, 26, 358–366. [Google Scholar] [CrossRef]
- Welch, S.; Skinner, A. A comparison of the structure and properties of human, rat and rabbit serum transferrin. Comparative biochemistry and physiology. B Comp. Biochem. 1989, 93, 417–424. [Google Scholar]
- Konijnenberg, M.W.; de Jong, M. Preclinical animal research on therapy dosimetry with dual isotopes. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 19–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walrand, S.; Hanin, F.X.; Pauwels, S.; Jamar, F. Tumour control probability derived from dose distribution in homogeneous and heterogeneous models: Assuming similar pharmacokinetics, 125Sn–177Lu is superior to 90Y–177Lu in peptide receptor radiotherapy. Phys. Med. Biol. 2012, 57, 4263. [Google Scholar] [CrossRef] [Green Version]
- De Jong, M.; Breeman, W.A.; Valkema, R.; Bernard, B.F.; Krenning, E.P. Combination radionuclide therapy using 177Lu-and 90Y-labeled somatostatin analogs. J. Nucl. Med. 2005, 46, 13S–17S. [Google Scholar] [PubMed]
- Kunikowska, J.; Królicki, L.; Hubalewska-Dydejczyk, A.; Mikołajczak, R.; Sowa-Staszczak, A.; Pawlak, D. Clinical results of radionuclide therapy of neuroendocrine tumours with 90 Y-DOTATATE and tandem 90 Y/177 Lu-DOTATATE: Which is a better therapy option? Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 1788–1797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, G.; Callahan, J.; Hofman, M.S.; Pattison, D.A.; Akhurst, T.; Michael, M.; Eu, P.; Hicks, R.J. High clinical and morphologic response using 90 Y-DOTA-octreotate sequenced with 177 Lu-DOTA-octreotate induction peptide receptor chemoradionuclide therapy (PRCRT) for bulky neuroendocrine tumours. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 476–489. [Google Scholar] [CrossRef] [PubMed]
- Walrand, S.; Jamar, F.; van Elmbt, L.; Lhommel, R.; Bekonde, E.B.; Pauwels, S. 4-Step renal dosimetry dependent on cortex geometry applied to 90Y peptide receptor radiotherapy: Evaluation using a fillable kidney phantom imaged by 90Y PET. J. Nucl. Med. 2010, 51, 1969–1973. [Google Scholar] [CrossRef] [Green Version]
- Hou, X.; Brosch, J.; Uribe, C.; Desy, A.; Boning, G.; Beauregard, J.M.; Celler, A.; Rahmim, A. Feasibility of single-time-point dosimetry for radiopharmaceutical therapies. J. Nucl. Med. 2020, 30, 1006–1011. [Google Scholar] [CrossRef]
- Sundlöv, A.; Gustafsson, J.; Brolin, G.; Mortensen, N.; Hermann, R.; Bernhardt, P.; Svensson, J.; Ljungberg, M.; Tennvall, J.; Gleisner, K.S. Feasibility of simplifying renal dosimetry in 177 Lu peptide receptor radionuclide therapy. Ejnmmi Phys. 2018, 5, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Menda, Y.; Madsen, M.T.; O’Dorisio, T.M.; Sunderland, J.J.; Watkins, G.L.; Dillon, J.S.; Mott, S.L.; Schultz, M.K.; Zamba, G.K.; Bushnell, D.L.; et al. 90Y-DOTATOC Dosimetry–Based Personalized Peptide Receptor Radionuclide Therapy. J. Nucl. Med. 2018, 59, 1692–1698. [Google Scholar] [CrossRef] [Green Version]
- Del Prete, M.; Buteau, F.A.; Arsenault, F.; Saighi, N.; Bouchard, L.O.; Beaulieu, A.; Beauregard, J.M. Personalized 177 Lu-octreotate peptide receptor radionuclide therapy of neuroendocrine tumours: Initial results from the P-PRRT trial. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 728–742. [Google Scholar] [CrossRef] [PubMed]
- Sundlöv, A.; Sjögreen-Gleisner, K.; Svensson, J.; Ljungberg, M.; Olsson, T.; Bernhardt, P.; Tennvall, J. Individualised 177 Lu-DOTATATE treatment of neuroendocrine tumours based on kidney dosimetry. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1480–1489. [Google Scholar] [CrossRef] [Green Version]
- Konijnenberg, M.; Herrmann, K.; Kobe, C.; Verburg, F.; Hindorf, C.; Hustinx, R.; Lassmann, M. EANM position paper on article 56 of the Council Directive 2013/59/Euratom (basic safety standards) for nuclear medicine therapy. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/HTML/?uri=LEGISSUM:l14547&from=HR (accessed on 1 August 2021).
- Available online: https://curia.europa.eu/juris/showPdf.jsf?text=&docid=85945&pageIndex=0&doclang=EN&mode=req&dir=&occ=first&part=1&cid=771955para.2 (accessed on 1 August 2021).
Figure 1.
(A) Toxicity observed in the 86Y-SMT-487 phase I trial as a function of the absorbed dose computed with the MIRD pamphlet no. 11 formalism [11], (B) after rescaling with the individual kidney volume and (C) converted into BED. The dots diameter corresponds to the number of cycles. Reprinted with permission from Ref. [8]. Copyright 2021 SNM. (D) Matching of the NTCPs observed in 90Y-DOTATOC with that of EBRT. Reprinted with permission from Ref. [13]. Copyright 2021 SNM.
Figure 1.
(A) Toxicity observed in the 86Y-SMT-487 phase I trial as a function of the absorbed dose computed with the MIRD pamphlet no. 11 formalism [11], (B) after rescaling with the individual kidney volume and (C) converted into BED. The dots diameter corresponds to the number of cycles. Reprinted with permission from Ref. [8]. Copyright 2021 SNM. (D) Matching of the NTCPs observed in 90Y-DOTATOC with that of EBRT. Reprinted with permission from Ref. [13]. Copyright 2021 SNM.

Figure 2.
(A) 111In autoradiography. (B–D) corresponding isodoses simulated by Monte Carlo for 111In, 90Y and 177Lu, respectively. Reprinted with permission [21] 2021 SNM. (E) nephron anatomy showing the glomerulus and tubule location. Reprinted from [22].

Figure 3.
(A) Transferrin release mechanism (Reprinted from Ref. [31]) (B) 24 h post 86Y-DOTATOC injection from the 86Y-SMT-487 clinical trial. Metastases (M) already exhibit a strong uptake 4 h pi, while red marrow activity behaves in phase opposition to the blood pool visible in the heart. Previously irradiated vertebra by EBRT, which has eradicated active marrow, have a similar behavior as the blood pool. Reprinted with permission from Ref. [24]. Copyright 2021 Springer.
Figure 3.
(A) Transferrin release mechanism (Reprinted from Ref. [31]) (B) 24 h post 86Y-DOTATOC injection from the 86Y-SMT-487 clinical trial. Metastases (M) already exhibit a strong uptake 4 h pi, while red marrow activity behaves in phase opposition to the blood pool visible in the heart. Previously irradiated vertebra by EBRT, which has eradicated active marrow, have a similar behavior as the blood pool. Reprinted with permission from Ref. [24]. Copyright 2021 Springer.

Figure 4.
Blue solid circles: relative platelet counts decrease at nadir as a function of the red marrow in 177Lu-DOTATATE therapy (Reprinted with permission from Ref. [29]. Copyright 2019 P Bernhardt). Red empty circles: decrease observed in the 90Y-DOTATOC trial using 86Y-DOTATOC PET-based dosimetry added by the authors [24]. Both trendlines are very similar.
Figure 4.
Blue solid circles: relative platelet counts decrease at nadir as a function of the red marrow in 177Lu-DOTATATE therapy (Reprinted with permission from Ref. [29]. Copyright 2019 P Bernhardt). Red empty circles: decrease observed in the 90Y-DOTATOC trial using 86Y-DOTATOC PET-based dosimetry added by the authors [24]. Both trendlines are very similar.

Figure 5.
(A) Survival in rats bearing a small and large tumor treated with single or tandem PRRT. Reprinted with permission from Ref. [44]. Copyright 2021 SNM. (B) Survival in patients treated with 7.4 GBq/m2 of 90Y-DOTATOC or with 3.7 GBq/m2 of 90Y-DOTATOC + 3.7 GBq/m2 of 177Lu-DOTATATE. Note that assuming similar uptake, the tandem delivers absorbed doses 30% lower than those of 90Y alone. Reprinted with permission from Ref. [45]. Copyright 2021 Springer.
Figure 5.
(A) Survival in rats bearing a small and large tumor treated with single or tandem PRRT. Reprinted with permission from Ref. [44]. Copyright 2021 SNM. (B) Survival in patients treated with 7.4 GBq/m2 of 90Y-DOTATOC or with 3.7 GBq/m2 of 90Y-DOTATOC + 3.7 GBq/m2 of 177Lu-DOTATATE. Note that assuming similar uptake, the tandem delivers absorbed doses 30% lower than those of 90Y alone. Reprinted with permission from Ref. [45]. Copyright 2021 Springer.

Figure 6.
Overall survival in 177Lu-DOTA-octreotate therapy in relation to 23 Gy achieved to the kidney (blue curve), or not due to hematological toxicity (red curve). Gray curve: all patients OS. Red symbol: patients died. Blue symbol: patients alive (Reprinted with permission from Ref. [36]. Copyright 2021 Sundin).
Figure 6.
Overall survival in 177Lu-DOTA-octreotate therapy in relation to 23 Gy achieved to the kidney (blue curve), or not due to hematological toxicity (red curve). Gray curve: all patients OS. Red symbol: patients died. Blue symbol: patients alive (Reprinted with permission from Ref. [36]. Copyright 2021 Sundin).

Figure 7.
Proposed smart optimized tandem therapy work flow including 4 patient visits to the hospital, with one or two imagings at each visit.
Figure 7.
Proposed smart optimized tandem therapy work flow including 4 patient visits to the hospital, with one or two imagings at each visit.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Blood and image-based RM dose comparisons.
| 177Lu-DOTATATE Study | Blood-Based RM Dosi. (mGy/MBq) | Image-Based RM Dosi. (mGy/MBq) | Toxicity–Dose Correlation |
|---|---|---|---|
| Santoro et al. [28] | n.a. | 0.04 [0.01–0.09] | Yes |
| Hagmarker et al. [29] | n.a. | 0.06 [0.02–0.12] | Yes |
| Garsk et al. [36] | 0.016 | n.a. | No |
| Page et al. [37] | 0.02 [0.01–0.03] | 0.06 [0.03–0.11] | Yes for imaging |
n.a. = not assessed.
Table 2.
Comparison of grade 3–4 toxicities between 177Lu-DOTATATE and 90Y-DODTATOC therapies.
| 177Lu-DOTATATE Phase III [10] | 90Y-DOTATOC Phase II [39] | 177Lu-DOTATATE Indiv. Optim. [36] | 90Y-DOTATOC Indiv. Optim. [7] | |
|---|---|---|---|---|
| inj. activity | 4 × 7.4 GBq | 2.5 × 10.4 GBq/m2 | 23 Gy to kidneys | 27 Gy to kidneys |
| inj. decay energy | 511 J | 2193 * J | n.a. | n.a. |
| renal toxicity | 0.4% | 9.2% | n.a. | n.a. |
| hematotoxicity | 11.0% | 12.8% | 26.0% | 1.6% |
| hemato/renal tox | 27.5 | 1.4 | n.a. | n.a. |
*: Assuming a body surface area of 1.7 m2; n.a.: not applicable; indiv. optim.: individualized optimization. Bold numbers show the hematotoxicity risk comparison.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Walrand, S.; Jamar, F. Renal and Red Marrow Dosimetry in Peptide Receptor Radionuclide Therapy: 20 Years of History and Ahead. Int. J. Mol. Sci. 2021, 22, 8326. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22158326
AMA Style
Walrand S, Jamar F. Renal and Red Marrow Dosimetry in Peptide Receptor Radionuclide Therapy: 20 Years of History and Ahead. International Journal of Molecular Sciences. 2021; 22(15):8326. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22158326
Chicago/Turabian StyleWalrand, Stephan, and François Jamar. 2021. "Renal and Red Marrow Dosimetry in Peptide Receptor Radionuclide Therapy: 20 Years of History and Ahead" International Journal of Molecular Sciences 22, no. 15: 8326. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22158326
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.