
Clostridium Collagenase Impact on Zone of Stasis Stabilization and Transition to Healthy Tissue in Burns


Abstract
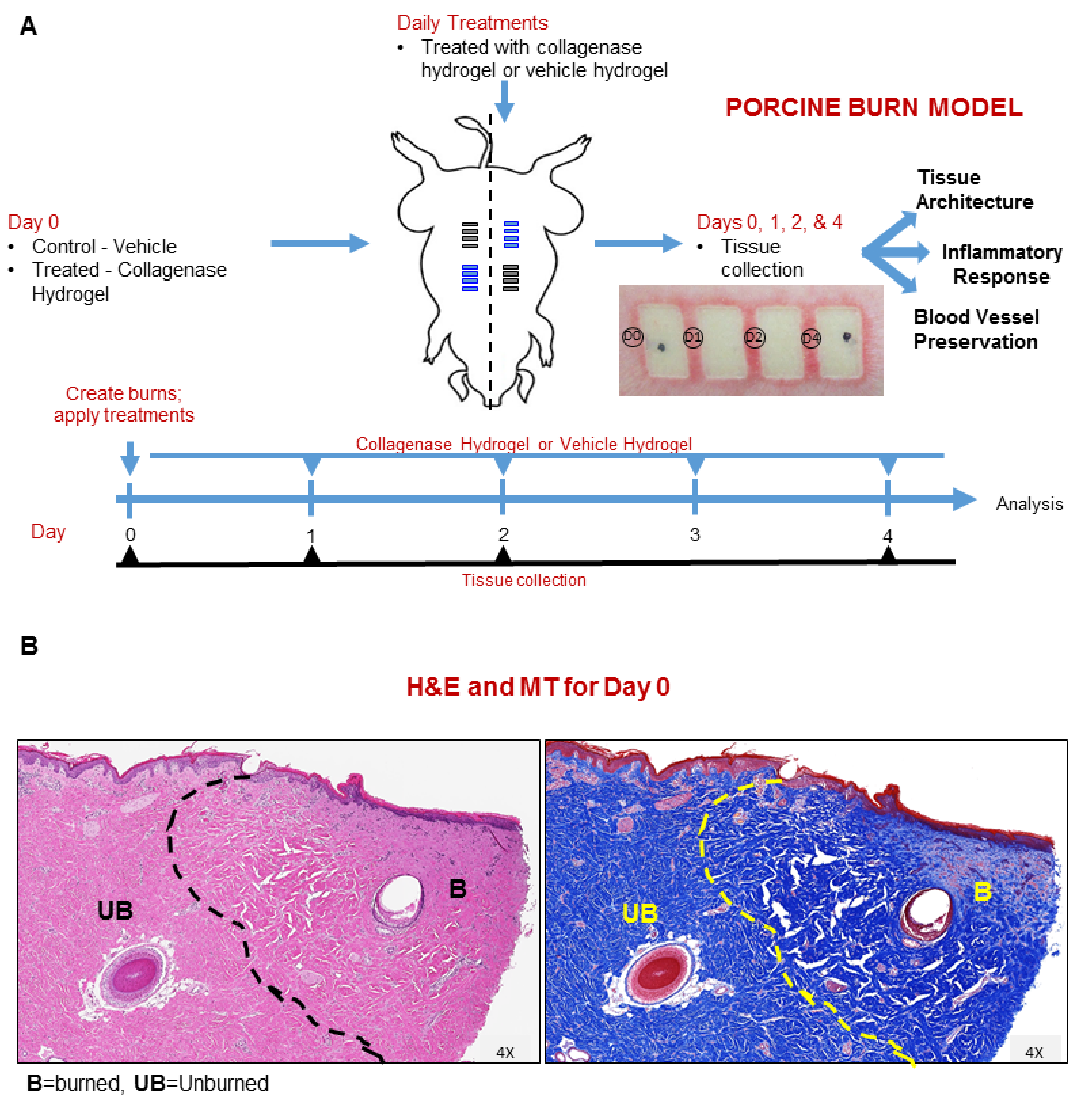
:1. Introduction
2. Results
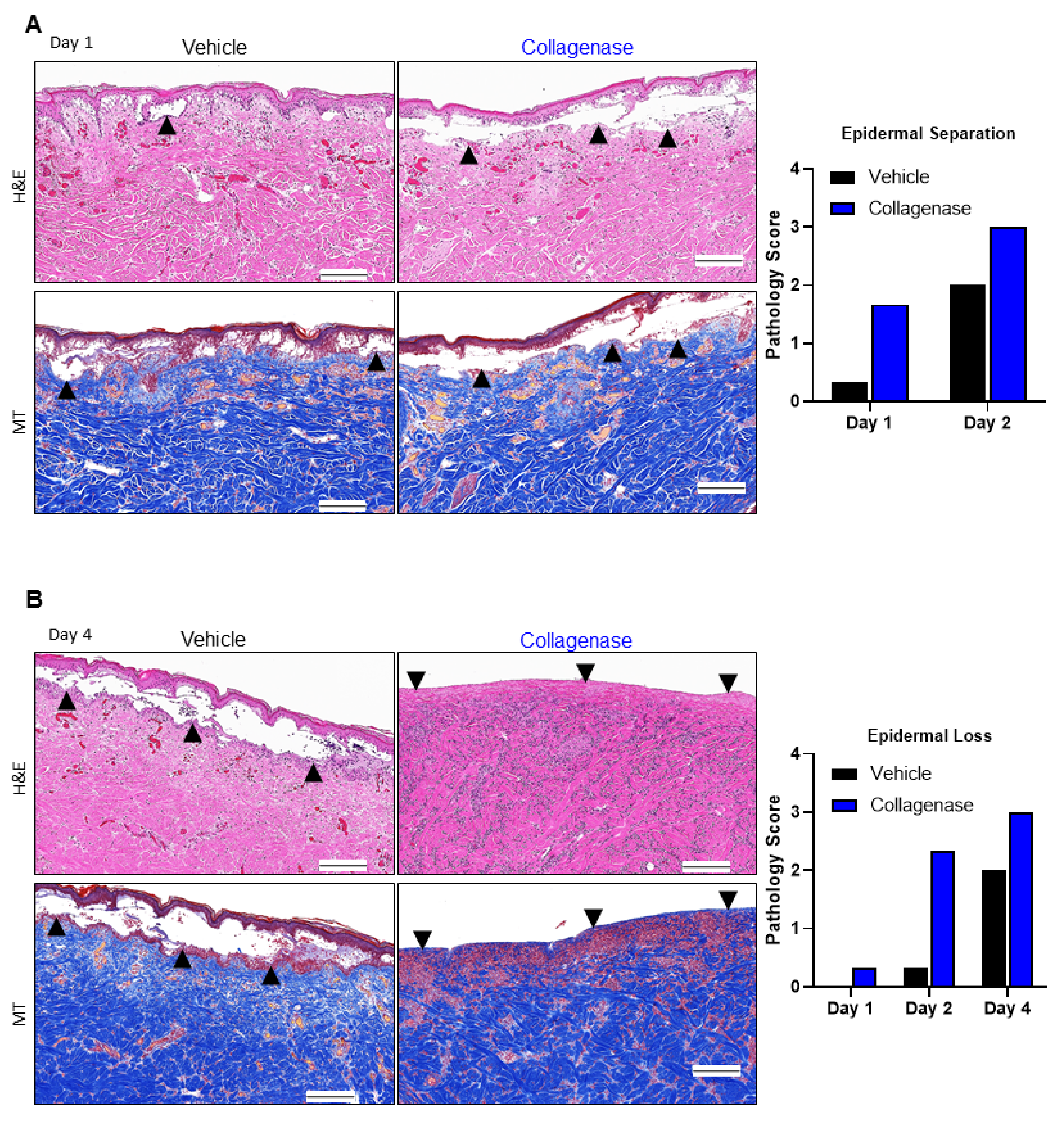
2.1. Clostridium Collagenase Facilitates Early Epidermal Separation and Loss
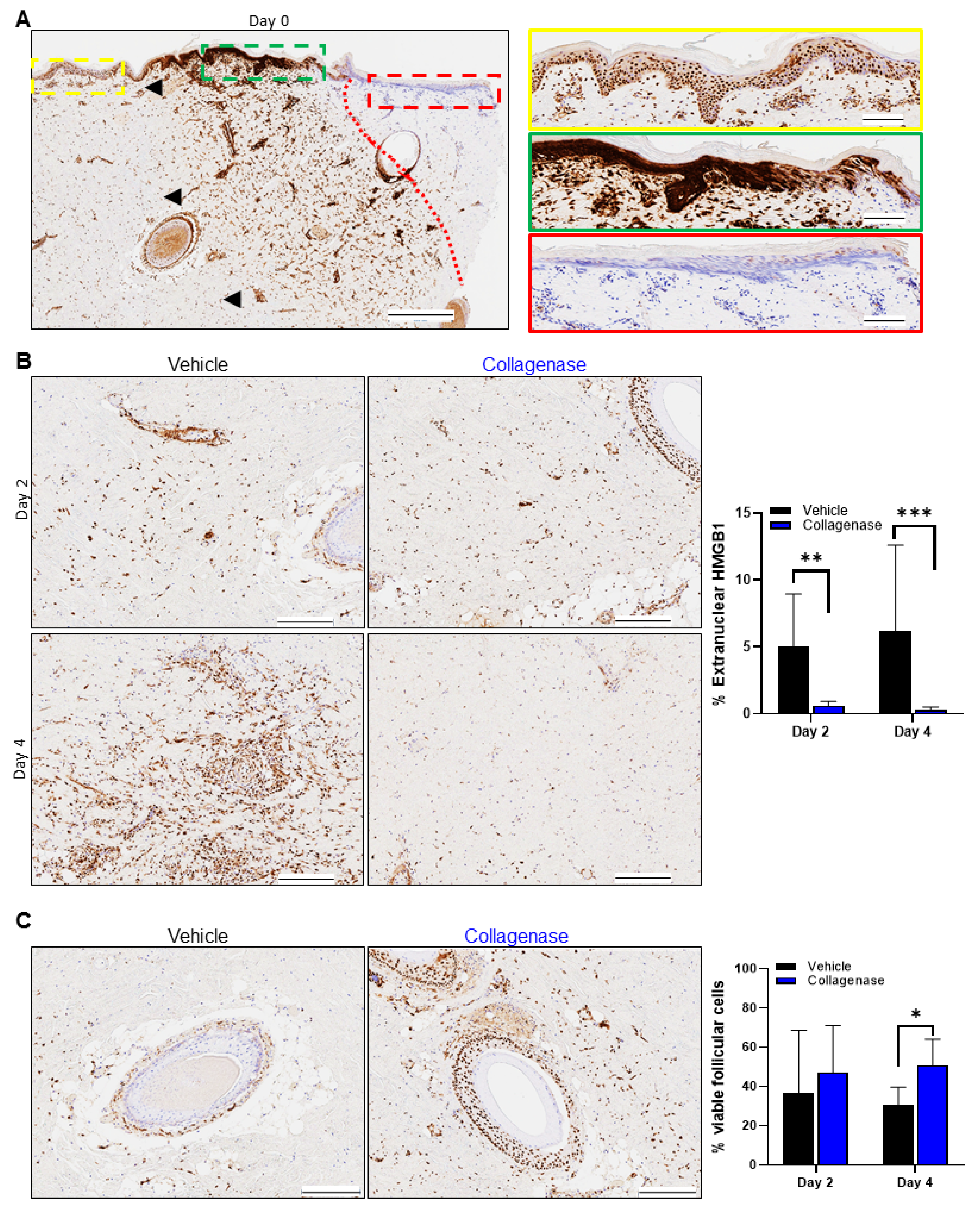
2.2. Clostridium Collagenase Reduces Necrosis
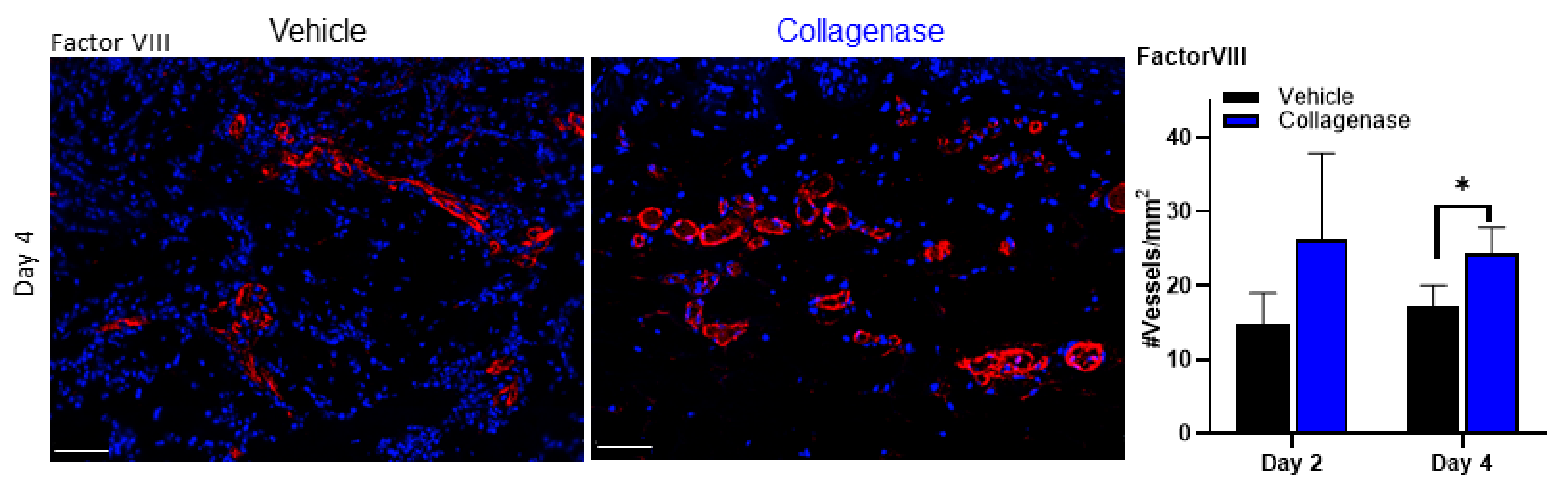
2.3. Clostridium Collagenase Preserves and Facilitates Blood Vessel Recovery and Formation
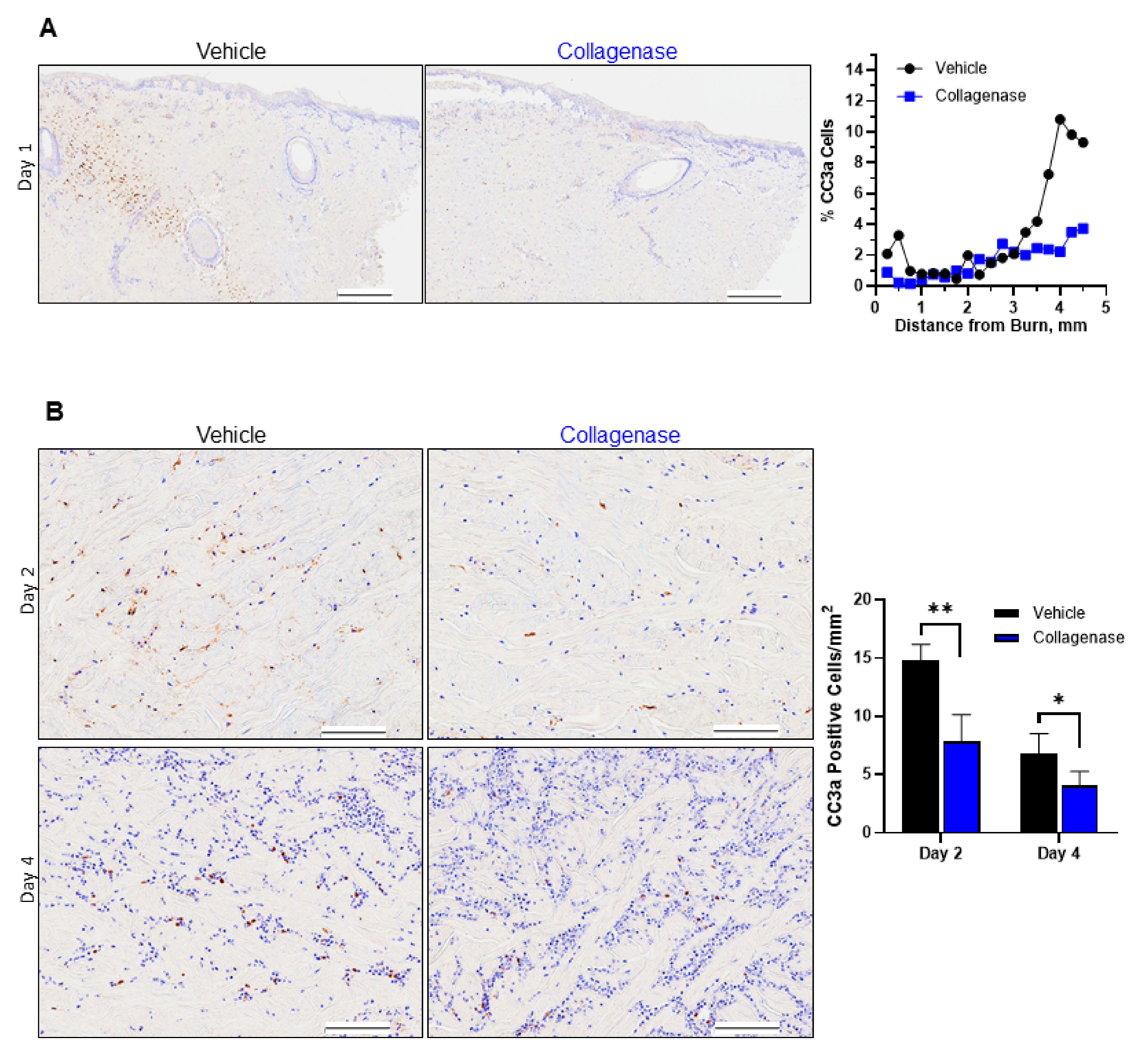
2.4. Treatment with Clostridium Collagenase Limits Apoptosis
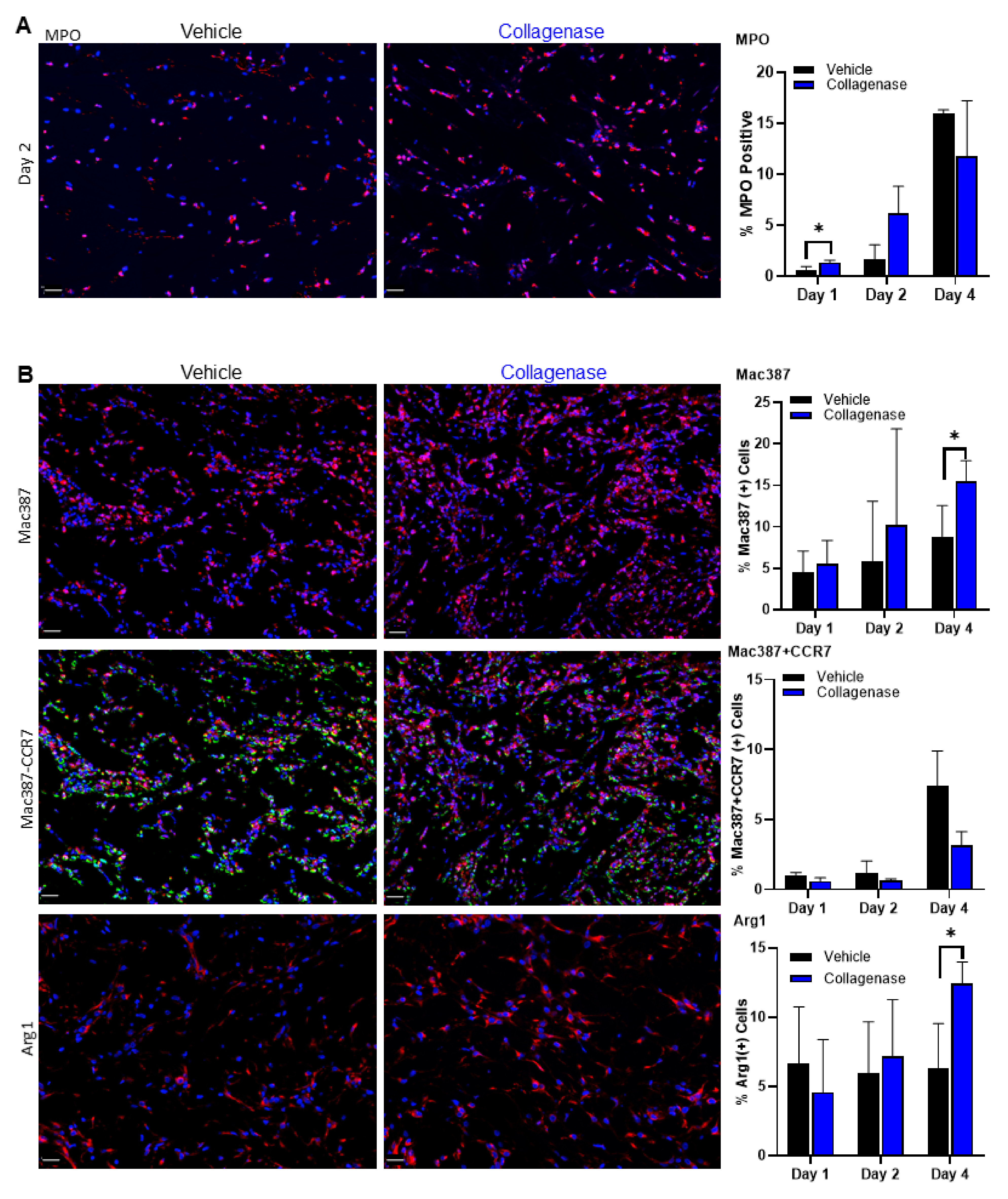
2.5. Clostridium Collagenase Leads to Early Neutrophil Recruitment
2.6. Infiltration of Inflammatory Cells Is Diminished with Clostridium Collagenase Treatment
3. Discussion
4. Materials and Methods
4.1. Materials and Reagents
4.1.1. Test Articles
4.1.2. In Vivo Testing
4.1.3. Immunohistochemistry
4.2. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jackson, D.M. The diagnosis of the depth of burning. Br. J. Surg 1953, 40, 588–596. [Google Scholar] [CrossRef] [Green Version]
- Arno, A.; Smith, A.H.; Blit, P.H.; Shehab, M.A.; Gauglitz, G.G.; Jeschke, M.G. Stem Cell Therapy: A New Treatment for Burns? Pharmaceuticals (Basel). 2011, 4, 1355–1380. [Google Scholar] [CrossRef] [PubMed]
- Giles, N.; Rea, S.; Beer, T.; Wood, F.M.; Fear, M.W. A peptide inhibitor of c-Jun promotes wound healing in a mouse full-thickness burn model. Wound Repair Regen. 2008, 16, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Bohr, S.; Patel, S.J.; Sarin, D.; Irimia, D.; Yarmush, M.L.; Berthiaume, F. Resolvin D2 prevents secondary thrombosis and necrosis in a mouse burn wound model. Wound Repair Regen. 2013, 21, 35–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gravante, G.; Delogu, D.; Palmieri, M.B.; Santeusanio, G.; Montone, A.; Esposito, G. Inverse relationship between the apoptotic rate and the time elapsed from thermal injuries in deep partial thickness burns. Burns 2008, 34, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Lanier, S.T.; McClain, S.A.; Lin, F.; Singer, A.J.; Clark, R.A. Spatiotemporal progression of cell death in the zone of ischemia surrounding burns. Wound Repair Regen. 2011, 19, 622–632. [Google Scholar] [CrossRef] [Green Version]
- Singer, A.J.; McClain, S.A.; Taira, B.R.; Guerriero, J.L.; Zong, W. Apoptosis and necrosis in the ischemic zone adjacent to third degree burns. Acad. Emerg. Med. 2008, 15, 549–554. [Google Scholar] [CrossRef]
- Bucky, L.P.; Vedder, N.B.; Hong, H.Z.; Ehrlich, H.P.; Winn, R.K.; Harlan, J.M.; May, J.W., Jr. Reduction of burn injury by inhibiting CD18-mediated leukocyte adherence in rabbits. Plast Reconstr. Surg. 1994, 93, 1473–1480. [Google Scholar] [CrossRef]
- Cetinkale, O.; Demir, M.; Sayman, H.B.; Ayan, F.; Onsel, C. Effects of allopurinol, ibuprofen and cyclosporin A on local microcirculatory disturbance due to burn injuries. Burns 1997, 23, 43–49. [Google Scholar] [CrossRef]
- Han, Y.P.; Tuan, T.L.; Wu, H.; Hughes, M.; Garner, W.L. TNF-alpha stimulates activation of pro-MMP2 in human skin through NF-(kappa)B mediated induction of MT1-MMP. J. Cell Sci. 2001, 114, 131–139. [Google Scholar] [CrossRef]
- Henze, U.; Lennartz, A.; Hafemann, B.; Goldmann, C.; Kirkpatrick, C.J.; Klosterhalfen, B. The influence of the C1-inhibitor BERINERT and the protein-free haemodialysate ACTIHAEMYL20% on the evolution of the depth of scald burns in a porcine model. Burns 1997, 23, 473–477. [Google Scholar] [CrossRef]
- Mileski, W.; Borgstrom, D.; Lightfoot, E.; Rothlein, R.; Faanes, R.; Lipsky, P.; Baxter, C. Inhibition of leukocyte-endothelial adherence following thermal injury. J. Surg. Res. 1992, 52, 334–339. [Google Scholar] [CrossRef]
- Moore, F.D., Jr.; Davis, C.; Rodrick, M.; Mannick, J.A.; Fearon, D.T. Neutrophil activation in thermal injury as assessed by increased expression of complement receptors. N. Engl. J. Med. 1986, 314, 948–953. [Google Scholar] [CrossRef] [PubMed]
- Nagane, N.S.; Bhagwat, V.R.; Subramanium, M. Increased free radical activity in burns. Indian J. Med. Sci. 2003, 57, 7–11. [Google Scholar] [PubMed]
- Parihar, A.; Parihar, M.S.; Milner, S.; Bhat, S. Oxidative stress and anti-oxidative mobilization in burn injury. Burns 2008, 34, 6–17. [Google Scholar] [CrossRef]
- Singh, V.; Devgan, L.; Bhat, S.; Milner, S.M. The pathogenesis of burn wound conversion. Ann. Plast Surg. 2007, 59, 109–115. [Google Scholar] [CrossRef]
- Cotran, R.S.; Majno, G. The Delayed and Prolonged Vascular Leakage in Inflammation. I. Topography of the Leaking Vessels after Thermal Injury. Am. J. Pathol. 1964, 45, 261–281. [Google Scholar]
- Hesketh, M.; Sahin, K.B.; West, Z.E.; Murray, R.Z. Macrophage Phenotypes Regulate Scar Formation and Chronic Wound Healing. Int. J. Mol. Sci. 2017, 18, 1545. [Google Scholar] [CrossRef] [Green Version]
- Elliott, M.R.; Koster, K.M.; Murphy, P.S. Efferocytosis Signaling in the Regulation of Macrophage Inflammatory Responses. J. Immunol. 2017, 198, 1387–1394. [Google Scholar] [CrossRef]
- Orgill, D.P. Excision and skin grafting of thermal burns. N. Engl. J. Med. 2009, 360, 893–901. [Google Scholar] [CrossRef] [Green Version]
- Dhaliwal, K.; Lopez, N. Hydrogel dressings and their application in burn wound care. Br. J. Community Nurs. 2018, 23, S24–S27. [Google Scholar] [CrossRef]
- Rowan, M.P.; Cancio, L.C.; Elster, E.A.; Burmeister, D.M.; Rose, L.F.; Natesan, S.; Chan, R.K.; Christy, R.J.; Chung, K.K. Burn wound healing and treatment: Review and advancements. Crit. Care 2015, 19, 243. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.; Hamilton, S.E.; Guddat, L.W.; Overall, C.M. Plant collagenase: Unique collagenolytic activity of cysteine proteases from ginger. Biochim. Biophys. Acta 2007, 1770, 1627–1635. [Google Scholar] [CrossRef]
- French, M.F.; Bhown, A.; Van Wart, H.E. Identification of Clostridium histolyticum collagenase hyperreactive sites in type I, II, and III collagens: Lack of correlation with local triple helical stability. J. Protein Chem. 1992, 11, 83–97. [Google Scholar] [CrossRef]
- Hansbrough, J.F.; Achauer, B.; Dawson, J.; Himel, H.; Luterman, A.; Slater, H.; Levenson, S.; Salzberg, C.A.; Hansbrough, W.B.; Doré, C. Wound healing in partial-thickness burn wounds treated with collagenase ointment versus silver sulfadiazine cream. J. Burn Care Rehabil. 1995, 16, 241–247. [Google Scholar] [CrossRef]
- Jimenez, J.C.; Agnew, P.S.; Mayer, P.; Clements, J.R.; Caporusso, J.M.; Lange, D.L.; Dickerson, J.E., Jr.; Slade, H.B. Enzymatic Debridement of Chronic Nonischemic Diabetic Foot Ulcers: Results of a Randomized, Controlled Trial. Wounds 2017, 29, 133–139. [Google Scholar] [PubMed]
- Motley, T.A.; Lange, D.L.; Dickerson, J.E., Jr.; Slade, H.B. Clinical outcomes associated with serial sharp debridement of diabetic foot ulcers with and without clostridial collagenase ointment. Wounds 2014, 26, 57–64. [Google Scholar] [PubMed]
- Das, A.; Sinha, M.; Datta, S.; Abas, M.; Chaffee, S.; Sen, C.K.; Roy, S. Monocyte and macrophage plasticity in tissue repair and regeneration. Am. J. Pathol. 2015, 185, 2596–2606. [Google Scholar] [CrossRef] [Green Version]
- Das, A.; Datta, S.; Roche, E.; Chaffee, S.; Jose, E.; Shi, L.; Grover, K.; Khanna, S.; Sen, C.K.; Roy, S. Novel mechanisms of Collagenase Santyl Ointment (CSO) in wound macrophage polarization and resolution of wound inflammation. Sci. Rep. 2018, 8, 1696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riley, K.N.; Herman, I.M. Collagenase promotes the cellular responses to injury and wound healing in vivo. J. Burns Wounds. 2005, 4, e8. [Google Scholar] [PubMed]
- Sheets, A.R.; Demidova-Rice, T.N.; Shi, L.; Ronfard, V.; Grover, K.V.; Herman, I.M. Identification and Characterization of Novel Matrix-Derived Bioactive Peptides: A Role for Collagenase from Santyl®®®® Ointment in Post-Debridement Wound Healing? PLoS ONE 2016, 11, e0159598. [Google Scholar]
- Shi, L.; Ermis, R.; Garcia, A.; Telgenhoff, D.; Aust, D. Degradation of human collagen isoforms by Clostridium collagenase and the effects of degradation products on cell migration. Int. Wound J. 2010, 7, 87–95. [Google Scholar] [CrossRef]
- Babakhani, A.; Nobakht, M.; Pazoki Torodi, H.; Dahmardehei, M.; Hashemi, P.; Mohajer Ansari, J.; Ramhormozi, P.; Yari, A.; Heidari, F. Effects of Hair Follicle Stem Cells on Partial-Thickness Burn Wound Healing and Tensile Strength. Iran. Biomed. J. 2020, 24, 99–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shpichka, A.; Butnaru, D.; Bezrukov, E.A.; Sukhanov, R.B.; Atala, A.; Burdukovskii, V.; Zhang, Y.; Timashev, P. Skin tissue regeneration for burn injury. Stem Cell Res. Ther. 2019, 10, 94. [Google Scholar] [CrossRef] [Green Version]
- Korkmaz, H.I.; Ulrich, M.M.W.; Vogels, S.; de Wit, T.; van Zuijlen, P.P.M.; Krijnen, P.A.J.; Niessen, H.W.M. Neutrophil extracellular traps coincide with a pro-coagulant status of microcirculatory endothelium in burn wounds. Wound Repair Regener. 2017, 25, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Stadelmann, C.; Lassmann, H. Detection of apoptosis in tissue sections. Cell Tissue Res. 2000, 301, 19–31. [Google Scholar] [CrossRef]
- Singer, A.J.; McClain, S.A.; Taira, B.R.; Romanov, A.; Rooney, J.; Zimmerman, T. Validation of a porcine comb burn model. Am. J. Emerg. Med. 2009, 27, 285–288. [Google Scholar] [CrossRef]
- Van Eycke, Y.R.; Allard, J.; Salmon, I.; Debeir, O.; Decaestecker, C. Image processing in digital pathology: An opportunity to solve inter-batch variability of immunohistochemical staining. Sci. Rep. 2017, 7, 42964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chlipala, E.A.; Bendzinski, C.M.; Dorner, C.; Sartan, R.; Copeland, K.; Pearce, R.; Doherty, F.; Bolon, B. An Image Analysis Solution for Quantification and Determination of Immunohistochemistry Staining Reproducibility. Appl. Immunohistochem. Mol. Morphol. 2020, 28, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Chlipala, E.A.; Butters, M.; Brous, M.; Fortin, J.S.; Archuletta, R.; Copeland, K.; Bolon, B. Impact of Preanalytical Factors During Histology Processing on Section Suitability for Digital Image Analysis. Toxicol. Pathol. 2020, 49, 755–772. [Google Scholar] [CrossRef]
- Schiraldi, M.; Raucci, A.; Muñoz, L.M.; Livoti, E.; Celona, B.; Venereau, E.; Apuzzo, T.; De Marchis, F.; Pedotti, M.; Bachi, A.; et al. HMGB1 promotes recruitment of inflammatory cells to damaged tissues by forming a complex with CXCL12 and signaling via CXCR. J. Exp. Med. 2012, 209, 551–563. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Liao, H.; Ochani, M.; Justiniani, M.; Lin, X.; Yang, L.; Al-Abed, Y.; Wang, H.; Metz, C.; Miller, E.J.; et al. Cholinergic agonists inhibit HMGB1 release and improve survival in experimental sepsis. Nat. Med. 2004, 10, 1216–1221. [Google Scholar] [CrossRef] [PubMed]
- Holmes, C.J.; Plichta, J.K.; Gamelli, R.L.; Radek, K.A. Burn Injury Alters Epidermal Cholinergic Mediators and Increases HMGB1 and Caspase 3 in Autologous Donor Skin and Burn Margin. Shock 2017, 47, 175–183. [Google Scholar] [CrossRef] [Green Version]
- Tan, J.Q.; Zhang, H.H.; Lei, Z.J.; Ren, P.; Deng, C.; Li, X.Y.; Chen, S.Z. The roles of autophagy and apoptosis in burn wound progression in rats. Burns 2013, 39, 1551–1556. [Google Scholar] [CrossRef]
- Jones, T.R.; Kao, K.J.; Pizzo, S.V.; Bigner, D.D. Endothelial cell surface expression and binding of factor VIII/von Willebrand factor. Am. J. Pathol. 1981, 103, 304–308. [Google Scholar]
- Fischer, D.; Kissel, T. Histochemical characterization of primary capillary endothelial cells from porcine brains using monoclonal antibodies and fluorescein isothiocyanate-labelled lectins: Implications for drug delivery. Eur. J. Pharm. Biopharm. 2001, 52, 1–11. [Google Scholar] [CrossRef]
- Xie, Y.; Zhu, K.Q.; Deubner, H.; Emerson, D.A.; Carrougher, G.J.; Gibran, N.S.; Engrav, L.H. The microvasculature in cutaneous wound healing in the female red Duroc pig is similar to that in human hypertrophic scars and different from that in the female Yorkshire pig. J. Burn Care Res. 2007, 28, 500–506. [Google Scholar] [CrossRef]
- Uzzan, B.; Nicolas, P.; Cucherat, M.; Perret, G.Y. Microvessel density as a prognostic factor in women with breast cancer: A systematic review of the literature and meta-analysis. Cancer Res. 2004, 64, 2941–2955. [Google Scholar] [CrossRef] [Green Version]
- DiPietro, L.A. Angiogenesis and wound repair: When enough is enough. J. Leukoc Biol. 2016, 100, 979–984. [Google Scholar] [CrossRef]
- Dhall, S.; Silva, J.P.; Liu, Y.; Hrynyk, M.; Garcia, M.; Chan, A.; Lyubovitsky, J.; Neufeld, R.J.; Martins-Green, M. Release of insulin from PLGA-alginate dressing stimulates regenerative healing of burn wounds in rats. Clin. Sci. (Lond.) 2015, 129, 1115–1129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teixeira, C.F.P.; Zamunér, S.R.; Zuliani, J.P.; Fernandes, C.M.; Cruz-Hofling, M.A.; Fernandes, I.; Chaves, F.; Gutiérrez, J.M. Neutrophils do not contribute to local tissue damage, but play a key role in skeletal muscle regeneration, in mice injected with Bothrops asper snake venom. Muscle Nerve 2003, 28, 449–459. [Google Scholar] [CrossRef]
- Gordon, S. Alternative activation of macrophages. Nat. Rev. Immunol. 2003, 3, 23–35. [Google Scholar] [CrossRef]
- Jetten, N.; Verbruggen, S.; Gijbels, M.J.; Post, M.J.; De Winther, M.P.; Donners, M.M. Anti-inflammatory M2, but not pro-inflammatory M1 macrophages promote angiogenesis in vivo. Angiogenesis 2014, 17, 109–118. [Google Scholar] [CrossRef]
- Watanabe, S.; Alexander, M.; Misharin, A.V.; Budinger, G.R.S. The role of macrophages in the resolution of inflammation. J. Clin. Invest. 2019, 129, 2619–2628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Funes, S.C.; Rios, M.; Escobar-Vera, J.; Kalergis, A.M. Implications of macrophage polarization in autoimmunity. Immunology 2018, 154, 186–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strudwick, X.L.; Cowin, A.J. The Role of the Inflammatory Response in Burn Injury. In Hot Topics in Burn Injuries; Kartal, S.P., Bayramgürler, D., Eds.; IntechOpen; University of South Australia: Adelaide, South Australia, Australia, 2018. [Google Scholar]
- Frye, K.E.; Luterman, A. Decreased Incidence of Hypertrophic Burn Scar Formation with the Use of Collagenase, an Enzymatic Debriding Agent. Wounds 2005, 17, 332–336. [Google Scholar]
- Ozcan, C.; Ergün, O.; Celik, A.; Cördük, N.; Ozok, G. Enzymatic debridement of burn wound with collagenase in children with partial-thickness burns. Burns 2002, 28, 791–794. [Google Scholar] [CrossRef]
- Pham, C.H.; Collier, Z.J.; Fang, M.; Howell, A.; Gillenwater, T.J. The role of collagenase ointment in acute burns: A systematic review and meta-analysis. J. Wound Care 2019, 28, S9–S15. [Google Scholar] [CrossRef]
- Soroff, H.S.; Sasvary, D.H. Collagenase ointment and polymyxin B sulfate/bacitracin spray versus silver sulfadiazine cream in partial-thickness burns: A pilot study. J. Burn Care Rehabil. 1994, 15, 13–17. [Google Scholar] [CrossRef]
- Shi, L.; Ramsay, S.; Ermis, R.; Carson, D. pH in the bacteria-contaminated wound and its impact on clostridium histolyticum collagenase activity: Implications for the use of collagenase wound debridement agents. J. Wound Ostomy Cont. Nurs. 2011, 38, 514–521. [Google Scholar] [CrossRef]
- Shi, L.; Carson, D. Collagenase Santyl ointment: A selective agent for wound debridement. J. Wound Ostomy Cont. Nurs. 2009, 36, S12–S16. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Epidermal Separation: Cleft between Dermis and Epidermis | |
|---|---|
| Grade | Description |
| 0 | Intact epidermis on entire section |
| 1 | Small area of epidermis separated from dermis (approximately less than 10% of section) |
| 2 | Mild, larger area of separation (approximately 10- 25% of section) |
| 3 | Moderate (approximately 25–75% of section) |
| Epidermal loss: area of complete loss of epidermis | |
| 0 | No epidermal loss |
| 1 | Small area (approximately less than 10%) |
| 2 | Larger area (approximately 10–25%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frederick, R.E.; Bearden, R.; Jovanovic, A.; Jacobson, N.; Sood, R.; Dhall, S. Clostridium Collagenase Impact on Zone of Stasis Stabilization and Transition to Healthy Tissue in Burns. Int. J. Mol. Sci. 2021, 22, 8643. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22168643
Frederick RE, Bearden R, Jovanovic A, Jacobson N, Sood R, Dhall S. Clostridium Collagenase Impact on Zone of Stasis Stabilization and Transition to Healthy Tissue in Burns. International Journal of Molecular Sciences. 2021; 22(16):8643. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22168643
Chicago/Turabian StyleFrederick, Rosanne E., Robert Bearden, Aleksa Jovanovic, Nasreen Jacobson, Rajiv Sood, and Sandeep Dhall. 2021. "Clostridium Collagenase Impact on Zone of Stasis Stabilization and Transition to Healthy Tissue in Burns" International Journal of Molecular Sciences 22, no. 16: 8643. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22168643