
Recurrence of a Mediastinal Germ-Cell Tumor as a Somatic-Type Malignancy: A Complex Case Report

 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Background
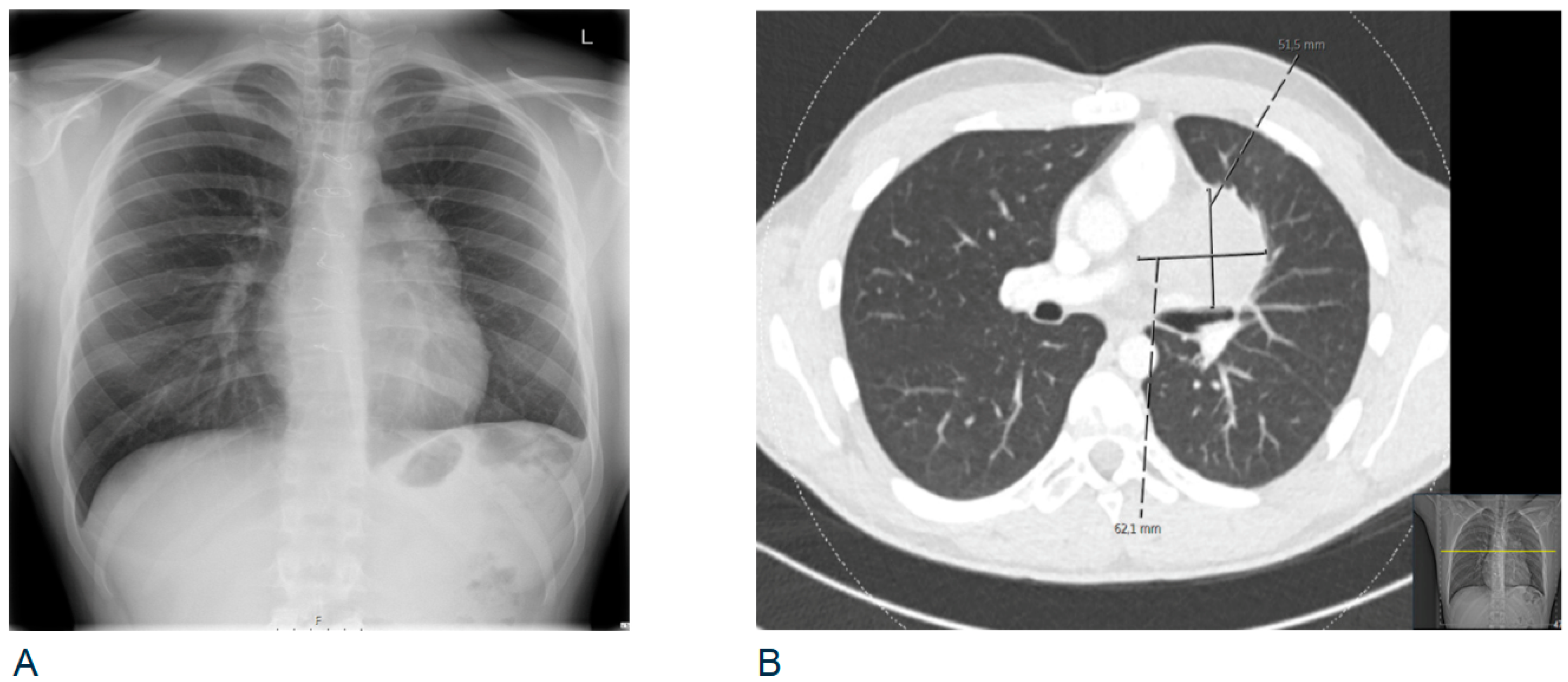
2. Case
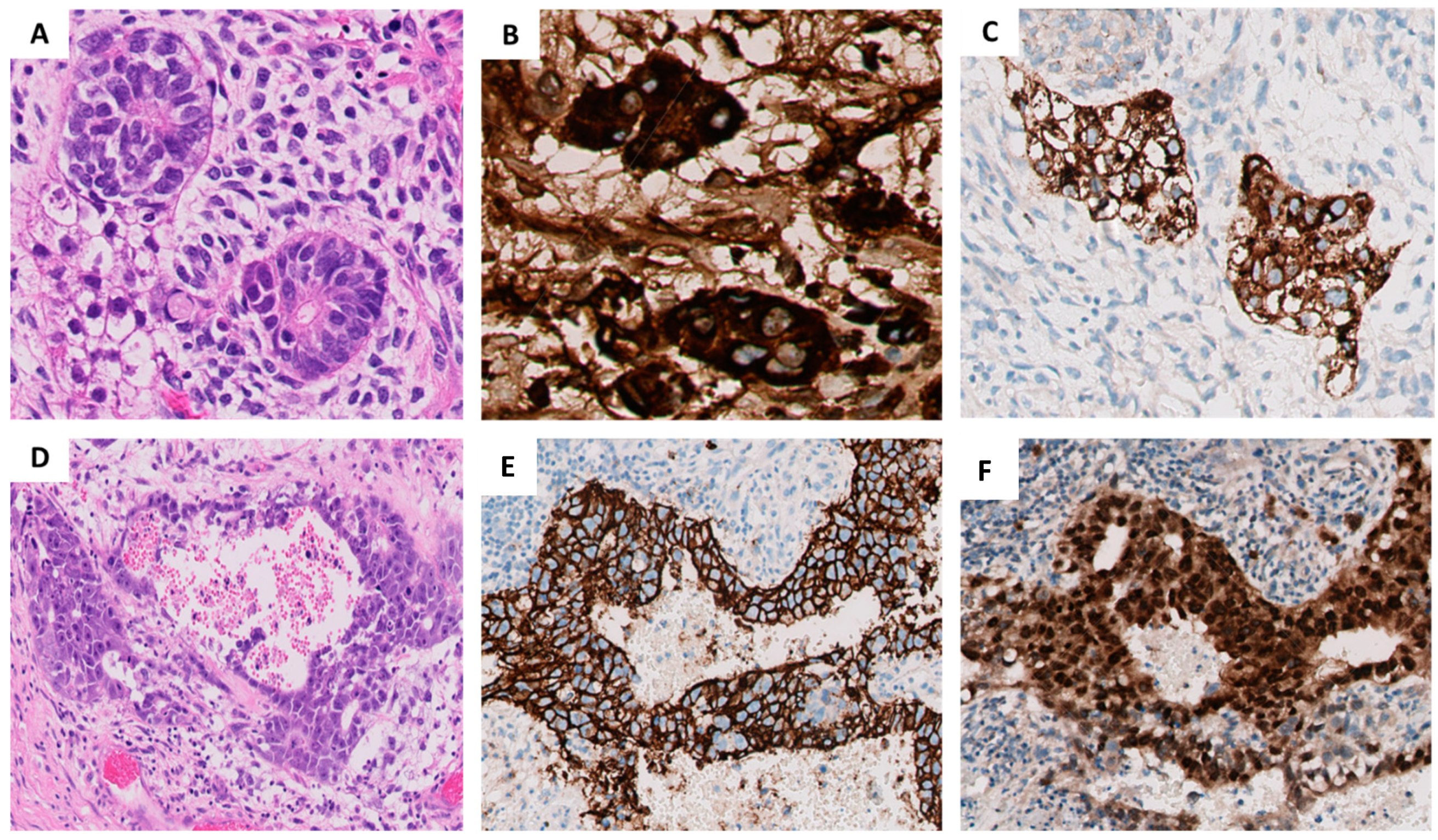
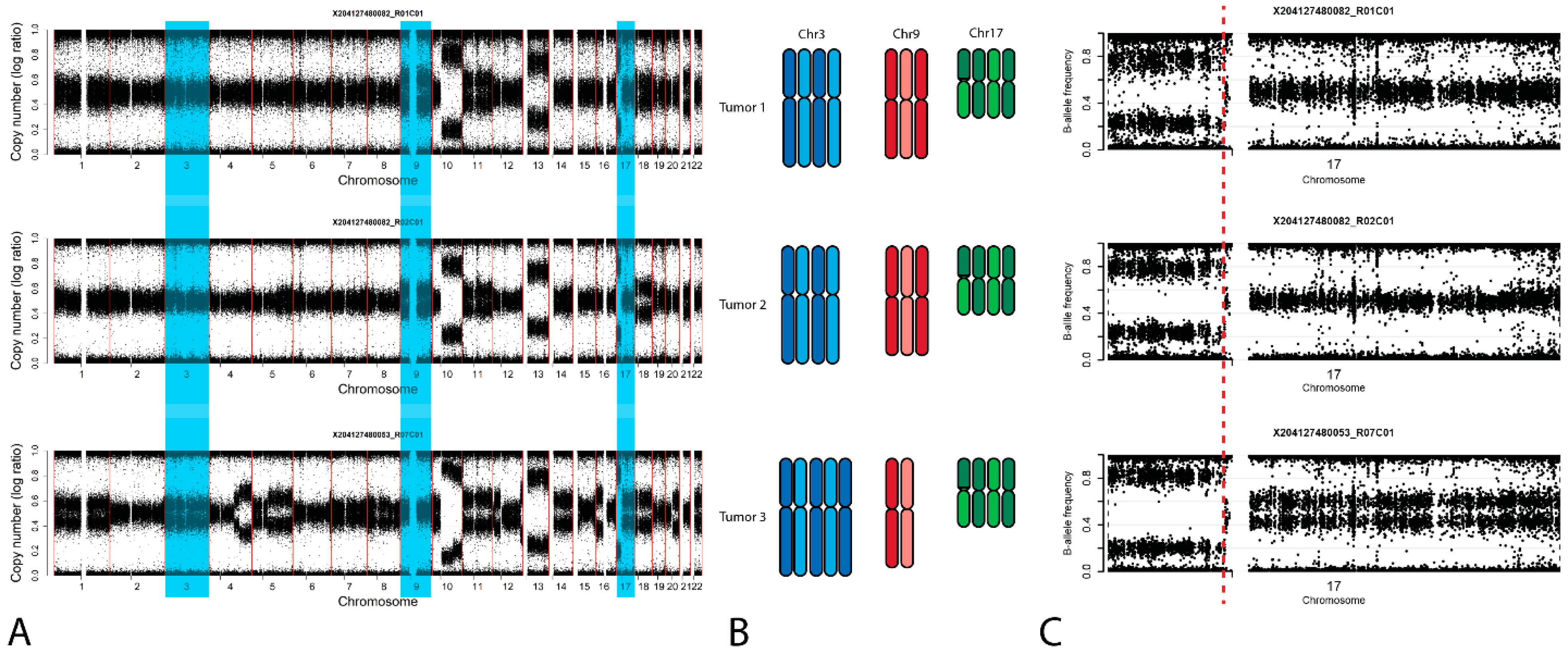
2.1. Clinical Description and Histological Findings
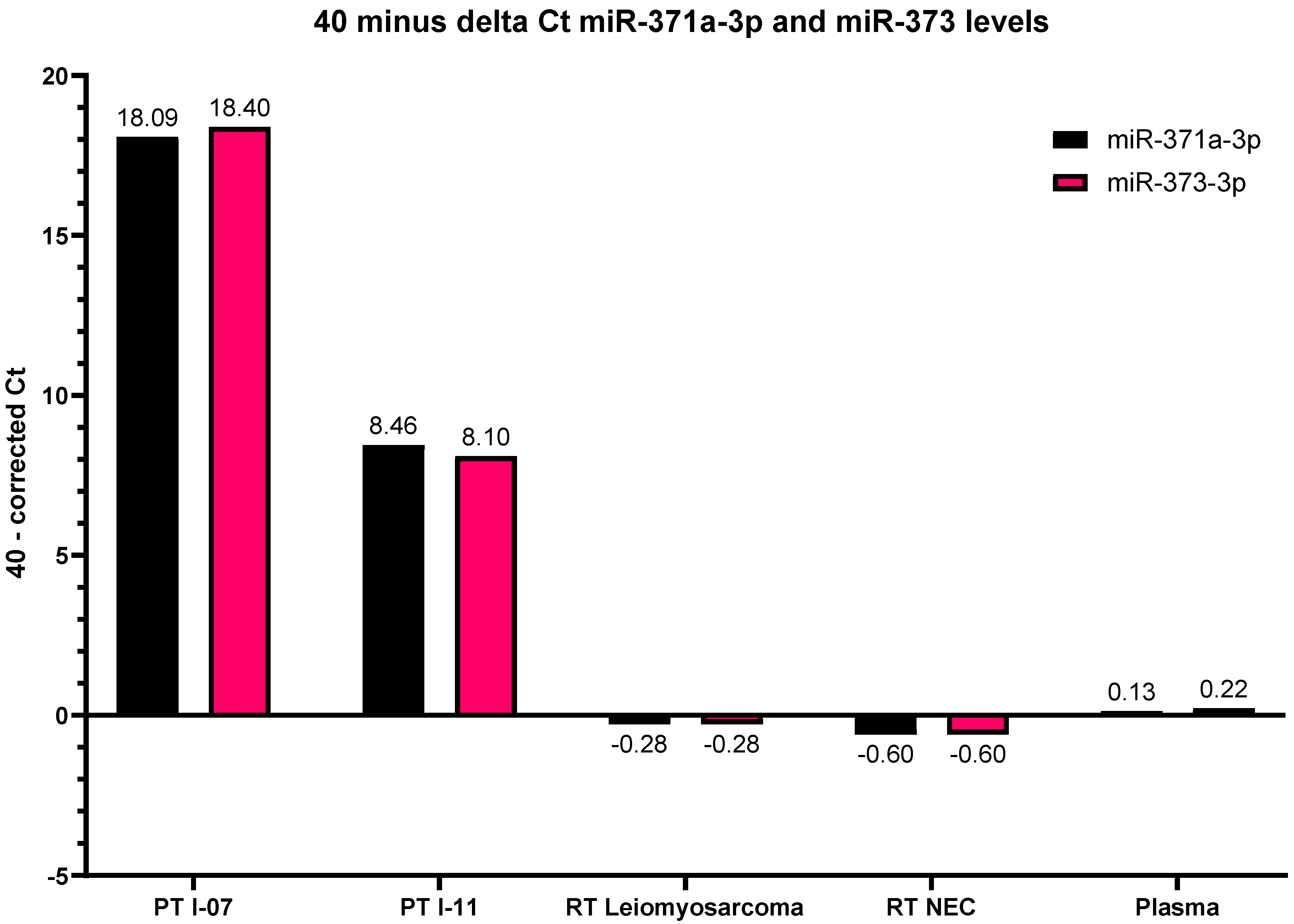
2.2. miRNA
3. Discussion
4. Materials & Methods
4.1. Immunohistochemistry
4.2. microRNA Profiling of Plasma and Tumors
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Murray, M.J.; Nicholson, J.C. Germ cell tumours in children and adolescents. Paediatr. Child Health 2010, 20, 109–116. [Google Scholar] [CrossRef]
- Oosterhuis, J.W.; Looijenga, L.H.J. Human germ cell tumours from a developmental perspective. Nat. Rev. Cancer 2019, 19, 522–537. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.J.; Bell, E.; Raby, K.L.; Rijlaarsdam, M.A.; Gillis, A.J.M.; Looijenga, L.H.J.; Brown, H.; Destenaves, B.; Nicholson, J.C.; Coleman, N. A pipeline to quantify serum and cerebrospinal fluid microRNAs for diagnosis and detection of relapse in paediatric malignant germ-cell tumours. Br. J. Cancer 2016, 114, 151–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oosterhuis, J.W.; Stoop, J.A.; Rijlaarsdam, M.A.; Biermann, K.; Smit, V.T.H.B.M.; Hersmus, R.; Looijenga, L.H.J. Pediatric germ cell tumors presenting beyond childhood? Andrology 2015, 3, 70–77. [Google Scholar] [CrossRef]
- Murray, M.J.; Smith, S.; Ward, D.; Verduci, L.; Nicholson, J.C.; Scarpini, C.G.; Coleman, N. Circulating microRNAs as biomarkers to assist the management of the malignant germ-cell-tumour subtype choriocarcinoma. Transl. Oncol. 2021, 14, 100904. [Google Scholar] [CrossRef]
- Murray, M.J.; Coleman, N. Testicular cancer: A new generation of biomarkers for malignant germ cell tumours. Nat. Rev. Urol. 2012, 9, 298–300. [Google Scholar] [CrossRef] [PubMed]
- Singla, N.; Lafin, J.T.; Bagrodia, A. MicroRNAs: Turning the Tide in Testicular Cancer. Eur. Urol. 2019, 76, 541–542. [Google Scholar] [CrossRef] [PubMed]
- Leao, R.; Albersen, M.; Looijenga, L.H.J.; Tandstad, T.; Kollmannsberger, C.; Murray, M.J.; Culine, S.; Coleman, N.; Belge, G.; Hamilton, R.J.; et al. Circulating MicroRNAs, the Next-Generation Serum Biomarkers in Testicular Germ Cell Tumours: A Systematic Review. Eur. Urol. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Almstrup, K.; Lobo, J.; Mørup, N.; Belge, G.; Rajpert-De Meyts, E.; Looijenga, L.H.J.; Dieckmann, K.-P. Application of miRNAs in the diagnosis and monitoring of testicular germ cell tumours. Nat. Rev. Urol. 2020, 17, 201–213. [Google Scholar] [CrossRef] [PubMed]
- Billmire, D.; Vinocur, C.; Rescorla, F.; Colombani, P.; Cushing, B.; Hawkins, E.; London, W.B.; Giller, R.; Lauer, S. Malignant mediastinal germ cell tumors: An intergroup study. J. Pediatr. Surg. 2001, 36, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Grabski, D.F.; Pappo, A.S.; Krasin, M.J.; Davidoff, A.M.; Rao, B.N.; Fernandez-Pineda, I. Long-term outcomes of pediatric and adolescent mediastinal germ cell tumors: A single pediatric oncology institutional experience. Pediatr. Surg. Int. 2017, 33, 235–244. [Google Scholar] [CrossRef]
- Schneider, D.T.; Calaminus, G.; Koch, S.; Teske, C.; Schmidt, P.; Haas, R.J.; Harms, D.; Göbel, U. Epidemiologic Analysis of 1,442 Children and Adolescents Registered in the German Germ Cell Tumor Protocols. Pediatr. Blood Cancer 2004, 42, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Ablin, A.R.; Krailo, M.D.; Ramsay, N.K.C.; Malogolowkin, M.H.; Isaacs, H.; Raney, R.B.; Adkins, J.; Hays, D.M.; Benjamin, D.R.; Grosfeld, J.L.; et al. Results of treatment of malignant germ cell tumors in 93 children: A report from the Childrens Cancer Study Group. J. Clin. Oncol. 1991, 9, 1782–1792. [Google Scholar] [CrossRef] [PubMed]
- Mann, J.R.; Raafat, F.; Robinson, K.; Imeson, J.; Gornall, P.; Phillips, M.; Sokal, M.; Gray, E.; McKeever, P.; Oakhill, A. UKCCSG’S germ cell tumour (GCT) studies: Improving outcome for children with malignant extracranial non-gonadal tumours—Carboplatin, etoposide, and bleomycin are effective and less toxic than previous regimens. Med. Pediatr. Oncol. 1998, 30, 217–227. [Google Scholar] [CrossRef]
- Baranzelli, M.C.; Kramar, A.; Bouffet, E.; Quintana, E.; Rubie, H.; Edan, C. Prognostic Factors in Children With Localized Malignant Nonseminomatous Germ Cell Tumors. J. Clin. Oncol. 1999, 17, 1212–1218. [Google Scholar] [CrossRef] [PubMed]
- Schneider, D.T.; Calaminus, G.; Reinhard, H.; Gutjahr, P.; Kremens, B.; Harms, D.; Göbel, U. Primary Mediastinal Germ Cell Tumors in Children and Adolescents: Results of the German Cooperative Protocols MAKEI 83/86, 89, and 96. J. Clin. Oncol. 2000, 18, 832–839. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc. Natl. Acad. Sci. USA 2008, 105, 10513–10518. [Google Scholar] [CrossRef] [Green Version]
- Lobo, J.; Gillis, A.J.M.; van den Berg, A.; Dorssers, L.C.J.; Belge, G.; Dieckmann, K.P.; Roest, H.P.; van der Laan, L.J.W.; Gietema, J.; Hamilton, R.J.; et al. Identification and Validation Model for Informative Liquid Biopsy-Based microRNA Biomarkers: Insights from Germ Cell Tumor In Vitro, In Vivo and Patient-Derived Data. Cells 2019, 8, 1637. [Google Scholar] [CrossRef] [Green Version]
- Looijenga, L.H.J.; Van Der Kwast, T.H.; Grignon, D.; Egevad, L.; Kristiansen, G.; Kao, C.-S.; Idrees, M.T. Report From the International Society of Urological Pathology (ISUP) Consultation Conference on Molecular Pathology of Urogenital Cancers IV: Current and Future Utilization of Molecular-Genetic Tests for Testicular Germ Cell Tumors. Am. J. Surg. Pathol. 2020, 44, e66. [Google Scholar] [CrossRef]
- Agthoven, T.T.; Looijenga, L.H.J. Accurate primary germ cell cancer diagnosis using serum based microRNA detection (ampTSmiR test). Oncotarget 2016, 8, 58037–58049. [Google Scholar] [CrossRef] [PubMed] [Green Version]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hulsker, C.C.C.; Kranendonk, M.E.G.; Eleveld, T.F.; Gillis, A.J.M.; van de Ven, C.P.; van Eijkelenburg, N.K.A.; van der Kaaij, N.P.; van der Steeg, A.F.W.; Looijenga, L.H.J. Recurrence of a Mediastinal Germ-Cell Tumor as a Somatic-Type Malignancy: A Complex Case Report. Int. J. Mol. Sci. 2021, 22, 9310. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22179310
Hulsker CCC, Kranendonk MEG, Eleveld TF, Gillis AJM, van de Ven CP, van Eijkelenburg NKA, van der Kaaij NP, van der Steeg AFW, Looijenga LHJ. Recurrence of a Mediastinal Germ-Cell Tumor as a Somatic-Type Malignancy: A Complex Case Report. International Journal of Molecular Sciences. 2021; 22(17):9310. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22179310
Chicago/Turabian StyleHulsker, Caroline C. C., Mariëtte E. G. Kranendonk, Thomas F. Eleveld, Ad J. M. Gillis, Cornelis P. van de Ven, Natasha K. A. van Eijkelenburg, Niels P. van der Kaaij, Alida F. W. van der Steeg, and Leendert H. J. Looijenga. 2021. "Recurrence of a Mediastinal Germ-Cell Tumor as a Somatic-Type Malignancy: A Complex Case Report" International Journal of Molecular Sciences 22, no. 17: 9310. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22179310