
Chronic Kidney Disease: Strategies to Retard Progression


1
Department of Medicine, Division of Nephrology, Cathay General Hospital, School of Medicine, Fu-Jen Catholic University, Taipei 106, Taiwan
2
National Defense Medical Center, Graduate Institute of Medical Sciences, Taipei 114, Taiwan
3
Department of Internal Medicine, Nephrology Division, National Taiwan University Hospital, Taipei 104, Taiwan
4
Graduate Institute of Toxicology, National Taiwan University College of Medicine, Taipei 104, Taiwan
5
Department of Internal Medicine, Nephrology Division, National Taiwan University College of Medicine, Taipei 104, Taiwan
6
Department of Internal Medicine, Nephrology Division, National Defense Medical Center, Taipei 104, Taiwan
*
Author to whom correspondence should be addressed.
†
Current address: Division of Nephrology, Department of Medicine, National Defense Medical Center, Tri-Service General Hospital, Taipei 104, Taiwan.
Int. J. Mol. Sci. 2021, 22(18), 10084; https://0-doi-org.brum.beds.ac.uk/10.3390/ijms221810084
Submission received: 31 August 2021
/
Revised: 12 September 2021
/
Accepted: 13 September 2021
/
Published: 18 September 2021
(This article belongs to the Special Issue Acute Kidney Injury and Chronic Kidney Diseases)
Abstract
:Chronic kidney disease (CKD), defined as the presence of irreversible structural or functional kidney damages, increases the risk of poor outcomes due to its association with multiple complications, including altered mineral metabolism, anemia, metabolic acidosis, and increased cardiovascular events. The mainstay of treatments for CKD lies in the prevention of the development and progression of CKD as well as its complications. Due to the heterogeneous origins and the uncertainty in the pathogenesis of CKD, efficacious therapies for CKD remain challenging. In this review, we focus on the following four themes: first, a summary of the known factors that contribute to CKD development and progression, with an emphasis on avoiding acute kidney injury (AKI); second, an etiology-based treatment strategy for retarding CKD, including the approaches for the common and under-recognized ones; and third, the recommended approaches for ameliorating CKD complications, and the final section discusses the novel agents for counteracting CKD progression.
1. Introduction
Chronic kidney disease (CKD) is defined as a progressive and irreversible loss of renal function evidenced by an estimated glomerular filtration rate (eGFR) of <60 mL/min per 1.73m2, the persistent presence of manifestations that are suggestive of kidney damage (proteinuria, active urine sediments, histological damages, structural abnormalities or a history of kidney transplantation), or both, lasting for more than 3 months [1]. CKD has long been a worldwide public health concern and constitutes a heavy healthcare and economic burden, as a reduced GFR is widely known to increase the risk of cardiovascular events, hospitalization, cognitive dysfunction, and overall mortality [2]. The prevalence of CKD varies according to geographic areas, mostly ranging from 10 to 20%, but rises gradually, particularly in developed countries [3,4,5]. This trend can be partially attributed to the expanding aging population globally [6]. In addition, the increased prevalence of risk factors such as diabetes mellitus (DM), hypertension, and obesity in patients with CKD is also notable [7,8].
Having a diagnosis of CKD means that an individual’s renal function has entered into a “point of no return,” indicating that the deterioration of renal function over time is inevitable and frequently irreversible. However, there can still be different patterns of renal function decline in patients with CKD. These patterns can be classified intuitively into very fast, fast, moderate, or slow, depending on the threshold required for defining the renal function decline rate, using mL/min/year or mL/min/month (Figure 1A). These differences in patterns largely reflect the heterogeneity of CKD origins and the subsequent pathologies, adjunct comorbidities, interventions that patients receive, and other harsh environmental exposures [9]. From this perspective, finding how to retard renal progression in patients with CKD is still fraught with challenges. In this review, we will focus on established and potential management strategies that aim to slow down the deterioration of renal function and treat the relevant complications in patients with CKD.
2. Risks of CKD Progression
Estimated GFR trajectories are highly variable in CKD. This phenomenon implies that a wide array of heterogeneous risk factors may contribute to CKD progression and that these risk factors may be potential therapeutic targets if we wish to achieve renoprotection. Socioeconomic factors and lifestyle factors (e.g., diet, sleep deprivation, smoking, and lack of exercise) are well-known risk factors that are associated with CKD progression. Systemic and metabolic disorders, including DM, hypertension, gout, and cardiovascular diseases, can also precipitate the development of CKD and aggravate eGFR decline (Figure 2) [10]. Recently, atrial fibrillation (AF) has also been shown to be a contributor to rapid eGFR decline, and the CHA2DS2-VASc score, a stroke-risk stratification model for patients with AF, can predict renal progression [11].
The intrinsic factors that are related to kidneys per se also play an important role in influencing renal function decline, such as GFR, proteinuria, glomerulopathy, interstitial lesions, and renal outlet obstruction (obstructive nephropathy). Each glomerulopathy distinctly influences the pace of renal function deterioration; for example, focal segmental glomerulosclerosis (FSGS) is more likely to result in a faster GFR decline, while the rate is lower for patients with IgA nephropathy (IgAN), membranous nephropathy (MN), and diabetic kidney disease (DKD) [12]. Polymorphisms in the genes involved in pathways such as those associated with inflammatory reactions (e.g., tumor necrosis factor (TNF)-α and interleukin (IL)-4), fibrosis (e.g., TGFB1), phase-II metabolism (e.g., GSTP1 and GSTO1), CKD worsening (e.g., UMOD) and the renin–angiotensin–aldosterone system (RAAS) (e.g., AGT and RENBP) have been suggested to affect the progression rate of patients with CKD [13].
3. Epithelial–Mesenchymal Transition (EMT)
Renal fibrosis, including nephrosclerosis and tubulointerstitial fibrosis, constitutes the final common pathway of renal injuries, regardless of etiologies. EMT is the major mechanism promoting renal fibrosis, and myofibroblasts are the main cell type that produces the extracellular matrix [14]. The origin of myofibroblasts in the kidney remains uncertain, but several candidates have been suggested, including resident fibroblasts, bone marrow-derived fibroblasts, or transition from pericytes or endothelial cells [15]. Recent research has revealed that EMT is fairly uncommon, as fibroblasts derived from EMT are rarely found in renal interstitium. A novel concept of partial EMT, indicating that tubular epithelial cells gain mesenchymal characteristics but retain their attachment to the basement membrane, may explain the pathogenic role of renal tubular epithelia in renal fibrosis [16].
After acute kidney injury (AKI) attacks, the c-Jun NH2-terminal kinase (JNK) signal is activated in tubular epithelial cells to enhance the expression of typical mesenchymal markers (e.g., e-cadherin, α-smooth muscle actin) and to upregulate profibrogenic factors (mainly transforming growth factor (TGF)-β and connective tissue growth factor (CTGF)) [17]. The persistent activation of the TGF-β pathway leading to an increased expression of SNAI1 and TWIST1 further promotes G2/M arrest. Cell cycle arrest in the G2/M phase in injured tubular cells, through JNK activation, amplifies the profibrogenic factors, such as TGF-β and CTGF, constituting a vicious cycle culminating in the fibrosis progression [18]. Fatty acid oxidation (FAO) is the main energy source of the proximal tubule (PCT). SMAD3 activated by TGF-β will suppress PPARGC1a expression to cause dysregulated FAO with lipid accumulation in the PCT, one of the characteristic features of EMT [19]. The PCT cells with lipid accumulation will enhance inflammation, innate immunity, and apoptosis to worsen renal fibrosis. Tubular cells with partial EMT can also activate fibroblasts and recruit inflammatory cells via the secretome composed of growth factors, chemokines, and cytokines, subsequently aggravating fibrosis [20]. Blocking EMT with approaches targeting the cell cycle or the inhibition of SNAI1 or TWIST1 expressions has been found to repress inflammation and fibrosis, pointing to the fact that EMT may be a good target mechanism to reverse renal fibrosis [15,18]. Bone morphogenetic protein-7 (BMP-7) can reverse EMT by counteracting the TGF-β/SMAD2/3 pathway and serves as another potential therapeutic target for improving renal injury [21]. However, the results in clinical studies of BMP-7 analogs involving patients with CKD are heterogeneous, suggesting a complex interaction between BMP-7 and other EMT-related pathways, as well as the necessity of determining the optimal serum BMP-7 concentration [22].
Epigenetic modifications, including DNA methylation and histone modification, also participate heavily in the regulation of partial EMT. The inhibition of DNA methylation was reported to ameliorate renal fibrosis. For example, low-dose hydralazine causing the de-methylation of the NASAL1 promotor and 5′-azacytidine, resulting in an inhibition of DNA methyltransferase 1 (DNMT1) [23,24,25]. Furthermore, agents targeting histone modification also confer renal benefits in CKD or AKI-to-CKD transition through the inhibition of histone methyltransferase (e.g., enhancer of zeste homolog 2) or the inhibition of histone deacetylases by directly inhibiting deacetylase (e.g., valproic acid) or indirectly interfering with histone modification readers (e.g., bromodomain and extra-terminal (BET) protein inhibitors) [26,27,28]. Epigenetics may be a novel therapeutic target for renal diseases.
4. Avoidance of Acute Kidney Injury (AKI) in Patients with CKD
AKI is associated with significant morbidity and mortality, including an increase in adverse renal outcomes. Cumulative evidence suggests that AKI is never self-limited, as it serves as a gateway to subsequent AKI episodes and, potentially, incident CKD, regardless of whether patients show recovery from AKI episodes or not [29]. Moreover, a single episode of severe AKI superimposed on patients with pre-existing CKD can cause further renal deterioration to end-stage kidney disease (ESKD) rapidly at a non-linear pace (Figure 1B). The risk factors associated with the AKI-related acceleration of renal progression were identified previously, and include older age, delayed renal function recovery from AKI, severe AKI episodes, the presence of proteinuria, and comorbidities such as DM, hypertension, and heart failure [30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132]. Long-term renal sequelae become very serious if patients have acute tubular necrosis (ATN) or ischemic AKI compared with those who have other forms of AKI, suggesting that the etiology of the AKI may also be a very important risk factor [33].
Biomarkers such as kidney injury molecule (KIM)-1 and neutrophil gelatinase-associated lipocalin (NGAL) are able to detect AKI earlier than conventional indicators [34,35]. Moreover, a combination of biomarkers such as insulin-like growth factor-binding protein 7 (IGFBP7) and tissue inhibitor of metalloproteinases-2 (TIMP-2) was shown to successfully predict the development of AKI during the 12 h following blood tests and can guide the selection of interventions to prevent AKI [36,37].
The mechanisms that are responsible for the transition from AKI to CKD remain under active investigation, and a maladaptive repair response with partial epithelial–mesenchymal transition (EMT), especially at the proximal tubule (PCT), has an important role. Cell cycle arrest in the G2/M phase, the dysregulated regeneration of injured PCT due to mitochondrial dysfunction, and the aberrant activation of developmental pathways (such as the Wnt, Hedgehog, and Notch pathways) also contribute to AKI-to-CKD transition. Phenotypic changes of fibroblasts to myofibroblasts or the formation of tertiary lymphoid tissue, as well as defective switches of recruited T cells and M1 macrophages to regulatory T cells and M2 macrophages, respectively, will perpetuate inflammation and fibrosis, leading to capillary rarefaction, hypoxia, and tubule cell damage, constituting a vicious cycle [38,39,40]. Furthermore, the persistent expression of either transforming growth factor (TGF)-β or kidney injury molecule-1 (KIM-1) has also been held responsible [41,42]. Notably, several pathogenic processes contributing to AKI-to-CKD transition are also physiological repair processes within kidneys. Additional insults, including high salt and high protein intake and nephrotoxic agents, during or after AKI episodes, as well as the underlying diseased kidney (e.g., diabetic nephropathy), may turn physiological renal responses into disordered regeneration.
Identification of Factors Causing AKI
The fundamental management of AKI in patients with CKD involves preventing the occurrence of AKI, and the success of this approach largely depends on the identification of the etiologies contributing to AKI (Table 1). Furthermore, treating the underlying etiologies of AKI, the optimization of volume and hemodynamic status, the withdrawal of nephrotoxic agents, the adjustment of medication doses according to renal function, adopting a conservative (<180 mg/dL), rather than an intensive glycemic control goal, and maintaining higher mean arterial pressure in patients with underlying hypertension can be crucial strategies for AKI management [43,44]. Drug regimens should be reviewed carefully to prevent drug–drug interactions. For example, adding piperacillin/tazobactam should be avoided, as it potentiates the nephrotoxicity of vancomycin. Several agents and strategies have been tested for treating AKI, including recombinant alkaline phosphatase and L-carnitine for sepsis-related AKI, as well as p53-targeted small interfering RNA (siRNA) and remote ischemic preconditioning for surgery-associated AKI [45,46].
5. An Etiology-Based Treatment Strategy for CKD
As mentioned above, the different etiologies of CKD themselves have various impacts on renal progression. As an etiology-based treatment strategy for CKD has not been well addressed, we touch on this management issue for both the common and less-appreciated causes of CKD.
5.1. Glomerulopathy
Glomerulopathy is a heterogeneous group of diseases and accounts for a significant number of CKDs. It occurs more commonly in young people with non-specific presentations. Although novel diagnostic tools are under investigation, renal biopsy is still the gold standard for achieving a definite diagnosis. A slow deterioration of renal function occurs in a proportion of patients. The risk factors for a faster GFR reduction include obesity, smoking, hypertension, significant proteinuria (usually >1 g/day), CKD at the diagnosis of glomerulopathy, and pathologically chronic renal lesions (glomerulosclerosis, tubular atrophy, and interstitial fibrosis) [47]. Genetic factors contribute to a rapid GFR loss, such as APOL1 in those with FSGS [48]. Fabry disease is a frequently ignored X-link inherited disease caused by a pathogenic mutation involving GLA-encoding lysosome enzyme α-galactosidase A [49]. The deficient enzyme function results in the intracellular accumulation of globotriaosylceramide, which impairs cell metabolism. Apart from neurological and cardiovascular associations, the kidneys may also be affected by presentations of proteinuria and renal failure. Enzyme replacement therapy is the cornerstone of renal progression reduction or prevention. A brief summary of the preferred treatment for different underlying glomerulonephritis is shown in Table 2.
5.2. DM-Related CKD
DM is the most common etiology of CKD and ESKD worldwide [50]. DKD usually occurs in patients with poor glycemic control, but also arises in 30–40% of patients with intensive glycemic control, suggesting a complex and multifactorial pathogenesis of DKD [51,52,53]. Clinical manifestations of DKD include impaired renal function with proteinuria. Several risk factors have been discovered, including early onset of DM, hypertension, ethnicity, obesity, the severity of proteinuria, and smoking [54,55,56,57]. In addition to adequate glycemic control, RAAS blockade is the centerpiece of DKD management. Pentoxiphylline can delay the initiation of dialysis and exert a significant antiproteinuric effect in DM patients already receiving RAAS blockades [57]. Although most statins exhibit minimal renoprotective effects [58,59,60], fenofibrate, a peroxisome proliferator-activated receptor (PPAR) α-agonist, has been shown to have an antiproteinuric effect in DKD [61]. Thiazolidinediones, a PPARγ agonist, can be beneficial for DKD, with salt and fluid retention side effects [62,63] that should be considered.
Sodium-glucose cotransporter-2 (SGLT2) inhibitors are the latest anti-hyperglycemic agent capable of decreasing blood glucose effectively by blocking glucose reabsorption in the PCT. In addition to cardiovascular benefits, SGLT2 inhibitors also postpone renal deterioration and reduce the severity of proteinuria in patients with DM (Figure 3) [64,65,66]. It is proposed that SGLT2 inhibitors protect the kidney by enhancing glycemic control, improving cardiovascular function, and decreasing body weight, as well as restoring intra and extrarenal hemodynamics, including lowering blood pressure (BP), promoting natriuresis, and re-activating tubuloglomerular feedback [67]. Structurally, SGLT2 inhibitors also are known to reverse PCT hypertrophy, which is induced by insulin resistance and hyperglycemia-related increasing sodium and glucose reabsorption through SGLT2 [68]. With the reversal of PCT hypertrophy and decreased Na+-glucose reabsorption, the kidney will be protected due to reduced energy demand and subsequently less oxidative stress, inflammation, fibrosis, and growth factor expression. Furthermore, AMPK/SIRT1 signaling, which is suppressed by hyperglycemia, could be re-activated by SGLT2 inhibitors to promote anti-inflammatory hypoxia-inducible factor (HIF)-2α and to suppress the expression of pro-inflammatory HIF-1α [69,70,71]. Hyperglycemia increases the production of reactive oxygen species (ROS), diacylglycerol (DAG), and advanced glycation end products (AGEs), all contributing to the impaired autophagic clearance of SNAI1 and activated p21 and p27. Accumulated SNAI1 and the activation of p21 and p27 result in G2/M cell cycle arrest, the hallmark of EMT, and maladaptive renal tubular regeneration. The use of SGLT2 inhibitors can restore normal autophagic clearance and inhibit pathways due to the products of hyperglycemia, attenuating cell cycle arrest-related kidney damage. Notably, it is found that the renoprotective effect may be extended to non-diabetic patients with kidney diseases [72].
O-GlcNAcylation is a post-translational modification of proteins and can regulate various physiological or pathological processes. In DM, O-GlcNAcylation has a role in insulin resistance and can mediate glucose toxicity, and subsequently, DM complications, including DKD. Recent research has demonstrated that the O-GlcNAcylation of cellular proteins such as ICln impairs cell volume regulation in diverse cell types, a common phenomenon in DM [73]. A hypertrophic PCT is a typical feature of DKD as increased filtrated glucose promotes the reabsorption of glucose and sodium in PCT. O-GlcNAcylation may result in the cell death of PCT and contribute to the development or progression of DKD by impairing the volume regulation, which could be reversed by reducing the O-GlcNAcylation of ICln [74]. Moreover, O-GlcNAcylation in PCT was found to correlate with fatty acid oxidation [75]. These findings suggest that the manipulation of O-GlcNAcylation may be a potential target for the treatment DKD [76].
6. Hypertension-Related CKD
BP lowering is one of the most important managing strategies for hypertensive patients with CKD [77]. The previous consensus suggested that a systolic BP (SBP) goal of <140 mmHg in patients with CKD and <130 mmHg in patients with CKD and proteinuria [78] would be reasonable. In proteinuric CKD patients, intensive BP control is associated with a lower occurrence of serum creatinine doubling or ESKD. Of note, Kidney Disease Improving Global Outcomes (KDIGO) updated the treatment target of SBP control to <120 mmHg in patients with hypertensive CKD [79].
Besides lifestyle modifications, including salt restriction, smoking cessation, weight loss, and adequate exercise, pharmacotherapy can be beneficial with the use of renoprotective agents, including RAAS blockades and carvedilol [80,81,82]. Mineralocorticoid receptor antagonists (MRAs), such as spironolactone, are able to reduce proteinuria and BP, but are limited in the treatment of CKD due to their association with GFR decline and hyperkalemia [83,84,85]. Novel nonsteroidal MRAs, such as esaxerenone and finerenone have been developed with better anti-fibrotic and anti-inflammatory effects (Figure 4) [86,87]. Compared with steroidal MRAs, both finerenone and esaxerenone exhibit similar proteinuria-lowering effects in patients with CKD, and a lower incidence of hyperkalemia [88,89,90]. Moreover, a combination of one RAAS blockade with nonsteroidal MRAs showed a similar AKI occurrence with finerenone but steadily decreased GFR in esaxerenone trials [91,92]. Whether the combination of nonsteroidal MRAs with other RAAS blockades will confer further renoprotection merits further investigation.
6.1. Heart Failure (HF)-Related CKD
In addition to traditional medications to control HF, sacubitril, an angiotensin receptor–neprilysin inhibitor (ARNI), is currently recommended for patients with HF due to its significant benefits in reducing cardiovascular mortality and hospitalization [93]. In view of the frequent occurrence of impaired renal function in patients with heart failure, the potential renal advantages of sacubitril/valsartan are being investigated. Sacubitril/valsartan was recently found to help reserve renal function and to reduce the severity of proteinuria in HF patients with a reduced ejection fraction [94].
6.2. Nephrolithiasis and Urothithiasis
Nephrolithiasis significantly increases the risk of incident CKD and accounts for about 2–3% of cases with ESKD [95]. Stone formers have a lower estimated GFR compared with those without renal stones [96]. This phenomenon likely results from the fact that nephrolithiasis shares many risk factors with CKD, including nephrotoxic analgesic use for pain control during obstructive uropathy, a decreased water intake leading to volume depletion, an increased dietary protein intake, recurrent sepsis, urinary tract structural abnormalities, and exposure to contrast media for imaging purposes [97,98]. Notably, both operations and shock wave lithotomy induce renal parenchymal injury, inflammation, and fibrosis. Furthermore, different stone types correlate with different CKD risk. For example, cystine stones carry the highest risk of CKD progression, followed by uric acid and struvite stones [99]. Given the higher rate of recurrence, nephrolithiasis and urothithiasis in CKD should be well managed.
Pathways leading to CKD may be stone-specific. Brushite stones frequently generate plugs at the ducts of Bellini and cause duct obstruction. The deposition of uric acid crystals may lead to inflammation and fibrosis. Chronic pyelonephritis, high urine pH due to urease action, and staghorn stones in the struvite stone formers may cause papillary necrosis and renal parenchymal injury [100]. Uncommon hereditary diseases can also present with nephrolithiasis, such as primary hyperoxaluria, cystinuria, Dent’s disease, and adenine phosphoribosyltransferase (APRT) deficiency [101,102]. The prevention of stone formation may be a key step to improve outcomes (Figure 5). Patients with uric acid stones have also been found to have better renal outcomes when they receive xanthine oxidase inhibitors, especially febuxostat and maintain alkaline urine [103]. Stone-specific agents can be utilized. Lumasiran, an RNAi therapy for type 1 primary hyperoxaluria, was recently approved for clinical use [104].
6.3. Autosomal Dominant Polycystic Kidney Disease (ADPKD)
ADPKD is the most common genetic cause of ESKD [105,106] and the majority of cases carry mutations in either PKD1 or PKD2. Recently, GANAB encoding glucosidase II subunit α was identified as another pathogenic gene [107]. Clinical manifestations of ADPKD include renal (flank pain, hematuria, calculi, urinary tract infection, polyuria, nocturia, and hypertension) and extrarenal (cerebral aneurysm, cysts in the liver or other organs, and valvular heart disease) presentations [108]. Multiple signaling pathways have been suggested to cause metabolic disturbance during the course of ADPKD, especially the cAMP pathway, which serves as the central player in cystogenesis [109] Transplantation is the best therapeutic strategy since treatments such as angiotensin-converting enzyme inhibitor (ACEi) or angiotensin receptor blocker (ARB) provide a limited effect on GFR decline [110]. However, encouraging results suggest that the use of the V2 receptor antagonist tolvaptan in patients aged <55 years with an estimated GFR >25 mL/min/1.73 m2 can delay the worsening of kidney function and decrease the volume in a dose-dependent manner with adequate safety and tolerance [111,112].
6.4. Autosomal Dominant Tubulointerstitial Kidney Disease (ADTKD)
Autosomal dominant tubulointerstitial kidney disease (ADTKD) is characterized by tubular damage and interstitial fibrosis with intact glomeruli and positive family history [113]. It inevitably causes CKD progression to ESKD but is usually un-recognized even though it accounts for about 5% of monogenic disorders resulting in ESKD [114]. The introduction of genetic tests improves the sensitivity of the diagnosis. The causative mutations mainly involve five genes, including UMOD, MUC1, REN, HNF1B, and SEC61A1. Although there is no specific therapy available for ADTKD currently, a low-salt diet is not suggested and diuretics should be used with caution to prevent the aggravation of salt and volume depletion as well as hyperuricemia and gout [115]
6.5. Patients with Graft Kidney
Compared with dialysis, patients receiving kidney transplantation have better outcomes and quality of life. After induction therapy with T cell depleting agents, maintenance immunosuppressants targeting three signals for T cell activation and proliferation should be continued to avoid rejection [116]. Glucocorticoids are commonly used for the induction and maintenance of immunosuppression by inhibiting nuclear factor κB (NF-κB) and its downstream cytokine expression. Early withdrawal can be considered in patients without direct immune-mediated renal diseases and with low immunologic risk [117]. Antimetabolites are also commonly used, including azathioprine, mycophenolate/mizoribine, and its active metabolite [118].
Calcineurin inhibitors (CNIs) are the major medications blocking signal 1 via binding to the FK506 binding protein (FKBP). Although CNIs improve graft outcomes significantly, 12 h trough or 2 h peak (for neoral only) serum levels should be measured to prevent excessive nephrotoxicity [119]. The complex drug interactions of CNIs with those capable of inducing or inhibiting cytochrome P450 need more attention. mTOR inhibitors (mTORi) also bind to FKBP but inhibit mTOR from blocking signal 3 [120]. Proteinuria should be measured during the use of mTORi to monitor side effects such as de novo proteinuria [121]. Belatacept binding to CD80/CD86 on antigen-presenting cells can interrupt the interaction with CD28 on T cells to block signal 2 [122].
Triple therapy is usually maintained in patients with higher immunologic risk, such as those with underlying glomerulonephritis, receiving re-transplantation, and those with high panel-reactive antibody titers [123]. With a lower estimated GFR after transplantation, a mTORi-based regimen is considered more often than a CNI-based regimen [124]. mTORi can replace CNIs or antimetabolites with similar allograft survival, better post-transplant renal function reserve, but a decreased occurrence of non-melanoma skin cancers [125]. Except for de novo proteinuria, mTORi may contribute to hyperlipidemia, bone marrow suppression, and infection. Other than pharmacotherapy, the frequent monitoring of kidney graft function is crucial. While serum creatinine increases, it is important to identify reversible factors such as sepsis, volume depletion, and drug toxicity. BK virus infection also needs to be excluded. Ultrasound is helpful in evaluating structural problems and vascular inflows. Kidney allograft biopsy may be indicated if recurrent/de novo kidney diseases or rejection are suspected, or incident proteinuria occurs.
7. Management of CKD Complications
The clinical manifestations of CKD are different according to the etiologies, staging, and comorbidities. Kidneys not only handle solute excretion and water balance but also maintain endocrine homeostasis. As CKD progresses, uremic toxins will accumulate. The appropriate management of CKD complications may also attenuate the renal progression rate.
7.1. Metabolic Acidosis
With the progressive loss of renal function, the declined renal capacity of acid excretion and ammonia synthesis, along with increased non-volatile acid production, leads to metabolic acidosis. The prevalence of metabolic acidosis was shown to increase linearly with GFR decline [126]. Metabolic acidosis can contribute to renal progression, and using alkali therapy was shown to slow renal progression [127]. The mechanism of metabolic acidosis-induced kidney progression is multi-faceted (Figure 6). Enhanced ammonia production in surviving nephrons secondary to metabolic acidosis in surviving nephrons may result in complement activation with tubulointerstitial damages [128,129]. Increased endothelin production related to metabolic acidosis is found to reduce GFR and tubulointerstitial injury [130]. Beyond renal adverse effects, metabolic acidosis negatively influences cardiovascular outcomes by aggravating inflammatory responses, increasing aldosterone secretion, enhancing endothelin synthesis, and impairing endothelial function, as well as reducing Na+/K+-ATPase activity and subsequently impaired heart contractility [131,132]. Metabolic acidosis is also associated with impaired bone mineralization, insulin resistance, and higher all-cause mortality [133,134].
Alkali therapy can be initiated early to achieve a serum HCO3− level between 22 and 26 mEq/L [135], since a HCO3− concentration >26 mEq/L is associated with higher mortality and cardiac events [136]. NaHCO3− and Na citrate are two commonly used alkali supplements; the former is cheaper but may result in bloating, while the latter is costly and enhances gastrointestinal absorption of aluminum. The concern about sodium/volume retention and hypertension being exacerbated by alkali therapy may be relieved with diuretics. Fruits and vegetables have also been shown to significantly increase serum HCO3− levels and to help preserve GFR in patients with stage 3 to 4 CKD without producing hyperkalemia, despite their lower effectiveness compared to medications [137].
7.2. Low Protein Diet with Ketoanalogues
A high protein intake causes hyperfiltration and increased intraglomerular pressure, resulting in the onset or progression of CKD. Therefore, dietary protein restriction has long been thought as the mainstay of nutritional therapies for CKD. In general, dietary protein of 0.55–0.6 g/kg/day is suggested for stage 3 to 5 CKD patients without DM, and 0.6–0.8 g/kg/day for those with DM. Compared with animal proteins, plant proteins have less influence on glomerular hemodynamics and a lower net acid production. Phosphate in plant origin proteins has relatively low bioavailability and results in a smaller phosphate accumulation [138]. Clinically, plant proteins are associated with a reduced rate of GFR decline and better outcomes and may be preferred as the major protein source in patients with CKD [139,140].
As a very low protein diet (0.3–0.4 g/kg/day protein) was reported to reduce the risks of incident dialysis compared with a low or normal protein diet, the means of preventing protein-energy wasting during a restriction of dietary protein becomes a critical issue [141]. Ketoanalogues are the precursors of essential amino acids, and their use with concomitant dietary protein restriction has been found to significantly delay the progression of CKD and to reduce the risks of dialysis initiation in patients with (estimated GFR >18 mL/min/1.73 m2) or without advanced CKD [142].
Regular physical exercise is recommended for patients regardless of CKD stage and may benefit kidney outcomes. However, there is still doubt about the relationship between the restriction of dietary protein and uremic sarcopenia in CKD patients. Indeed, regular physical activity during a low protein diet or a very low protein diet with ketoanalogues will not cause net protein catabolism but will help with an improvement in muscle strength, inflammation, and nutrition status if the energy supply is adequate [143,144]. Therefore, an increased intake of protein-free nutrition provides adequate energy needs without the trade-off of a high phosphate intake. Notably, the use of ketoanalogues can effectively prevent the occurrence of protein-energy wasting and may be considered as an important part of CKD nutritional therapy.
7.3. Anemia
Anemia is a frequent complication of CKD and is associated with a poor prognosis. The correction of anemia in CKD may enhance the quality of life for patients and reduce their renal function deterioration. Presently, mechanisms that are responsible for the development of renal anemia are only partially known [145]. Insufficient erythropoietin (EPO) production has been suggested as the major cause of renal anemia. Although the introduction of erythropoiesis-stimulating agents (ESAs) reduces transfusion-related complications and improves the symptoms of anemia [146], no significant improvement in anemia-related mortality and morbidity is observed, which is probably related to their adverse effects, such as worsening hypertension, malignancy progression, higher cardiovascular complications, and thrombosis [147]. These findings suggest that EPO deficiency is not the sole cause of renal anemia.
Hepcidin, a 25-amino acid peptide encoded by HAMP, serves as a key molecule in iron homeostasis by reducing gastrointestinal iron absorption and compromising iron distribution [148]. Inflammatory cytokines, such as interleukin-6, enhance hepcidin production, while EPO increases erythroferrone expression to suppress hepcidin production [149,150]. Hepcidin also plays a central role in iron regulation in patients with CKD; either chronic inflammation or EPO deficiency related to CKD enhances hepcidin production, resulting in impaired intestinal iron absorption and the mobilization of iron from its storage site [151,152].
Recently, hypoxia-inducible factor (HIF) stabilizers, such as roxadustat and vadadustat, have been developed for the treatment of renal anemia [153]. HIF, unlike ESAs, can bind to specific sequences called hypoxia response elements (HREs) to increase the production of endogenous EPO and to improve iron utility under hypoxia. With normoxia, the hydroxylation of HIF by prolyl hydroxylase domain (PHD) enzymes will cause the degradation of HIF for the purpose of regulating HIF activities [154]. HIF stabilizers have been shown to be non-inferiority to ESAs, especially in non-dialysis CKD, with regards to anemia-treatment efficacy [155,156]. However, their pleiotropic effects and long-term complications still require further investigation.
7.4. Hyperkalemia
Hyperkalemia is a potentially life-threatening condition and correlates with a rapid decline in renal function in patients with CKD. To educate patients with CKD about the restriction of dietary potassium (K+) is the cornerstone of management. Although cationic exchange resins, including sodium or calcium polystyrene sulfonate have been widely used in patients with CKD, the associated sodium load, gastrointestinal irritation, inadequate selectivity for certain cations, and their limited therapeutic efficacy reduce the utility of these resins. Recently, novel agents, including sodium zirconium cyclosilicate (ZS-9) and patiromer have been shown to have a higher selectivity for potassium with milder GI adverse effects. ZS-9 may play an important role in the management of acute hyperkalemia, due to its rapid onset of action (within 1 h), while patiromer shows a persistent K+-lowering effect lasting for 48 h [157,158,159]. Importantly, the high efficacy of both ZS-9 and patiromer to lower K+ may improve the prognosis of patients with CKD by reducing the probability of discontinuing RAAS blockades resulting in better heart and renal outcomes.
8. Specific Issues of CKD
8.1. Novel Therapeutic Approaches
The limited effects of the current therapy for CKD drives the need for the development of novel therapeutic agents. Regardless of the etiologies, several processes, including fibrosis, inflammation, and oxidative stress, as well as impaired cell regeneration, are ongoing in the kidney. Some novel agents targeting these pathways were investigated in preclinical studies and clinical trials. For example, atrasentan targeting the endothelin-1 receptor ETA, successfully delays the progression of DKD in clinical trials [160]. Given the critical role of transforming growth factor (TGF)-β in not only fibrosis but also inflammation, oxidation, and apoptosis, pirfenidone (with the ability to reduce TGF-β production) was shown to retard the progression of estimated GFR in FSGS clinical trials [161]. MicroRNAs can regulate numerous biological processes by repressing translationally or mediating the degradation of mRNA. MiR-21 can be induced by TGF-β in kidneys and is associated with fibrosis and podocyte injury. Lademirsen, as a blocker of miR-21, was found to prevent the progression of Alport syndrome in preclinical studies [162]. Bromodomain and extraterminal (BET) proteins are epigenetic regulators involved in cell proliferation, differentiation, and inflammation. A BET protein inhibitor, apabetalone, showed favorable renal outcomes in patients with coronary artery disease and DKD [163,164]. Furthermore, clinical trials using inhibitors of Nrf2 and p53 are ongoing [165].
Considering the complexity of CKD pathogenesis involving different cell types and changes of multiple signal pathways, multi-target drugs (MTD) emerge as a useful tool; for example, soluble epoxide hydrolase (SHE)-based PTUPB (with cyclo-oxygenase 2 (COX2) inhibitor), PB394 (with PPARγ agonist), and DM509 (with farnesoid X receptor agonist) to alleviate fibrosis, inflammatory response, and oxidative stress from CKD related to DM, hypertension, hyperlipidemia, or other etiologies [166,167,168].
8.2. Mesenchymal Stem Cells and Their Conditioned Media
Mesenchymal stem cells (MSCs) characterized by the ability to self-renew and differentiate to different cells can be isolated from different tissues such as adipose tissue and bone marrow [169]. Due to the low immunogenicity of MSCs, their transplantation is a safe therapy and has been used in the treatment of numerous diseases, including kidney diseases. Transplanted MSCs can migrate into injured tissue, so-called MSC homing, and exert their immune modulation, anti-apoptosis, anti-inflammation, and anti-oxidation abilities to enhance tissue repair in the manner of direct cell–cell interaction or paracrine [170]. Moreover, extracellular vesicles (EVs) secreted by MSCs and the conditioned medium (CM) of MSCs are both shown to help heal injured tissues [171]. In diverse models of AKI and CKD, the systemic or local injection of MSC, MSC-EV, or MSC-CM has been demonstrated to enhance tubular repair, ameliorate inflammation, alleviate fibrosis, and preserve kidney function. In clinical trials of AKI and CKD (Table 3), MSC therapy evinced safety and tolerability, but the small case number and short duration of follow-up meant that the efficacy of MSC therapy on kidney protection was inconclusive [172]. For DKD, MSC administration tended to stabilize or improve the GFR in patients with type 2 DM, but hyperglycemia may diminish the renoprotective effect by causing damage to MSCs, which could be resolved by a co-culture of macrophage with MSCs or a modification of MSCs by angiotensin-converting enzyme 2 [173]. Similarly, uremic toxins such as p-cresol can impair the function of MSCs, and the concomitant use of pioglitazone helps to restore the MSC function [174].
9. Conclusions
The management of patients with CKD is complex and challenging because of the heterogeneous nature of CKD and an inadequate awareness of its adverse impact. Besides lifestyle modifications and the correction of CKD risk factors, the prompt identification of AKI and early medical interventions for complications including anemia, metabolic acidosis, low protein diet with ketoanalogues, hyperkalemia, and CKD-mineral bone disorder (CKD-MBD) are crucial for retarding renal progression and lowering the morbidity and mortality of patients with CKD. With the advancements that have been made in understanding the molecular mechanisms of CKD, novel therapeutic agents being continuously identified, and the translation of these findings from bench to bedside will likely improve the efficacy of treatments for CKD.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors have no relevant financial or non-financial competing interests to declare in relation to this manuscript.
References
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Tonelli, M.; Wiebe, N.; Culleton, B.; House, A.; Rabbat, C.; Fok, M.; McAlister, F.; Garg, A.X. Chronic Kidney Disease and Mortality Risk: A Systematic Review. J. Am. Soc. Nephrol. 2006, 17, 2034–2047. [Google Scholar] [CrossRef] [Green Version]
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.; O’Callaghan, C.A.; Lasserson, D.; Hobbs, R. Global Prevalence of Chronic Kidney Disease—A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef]
- Ruiz-Ortega, M.; Rayego-Mateos, S.; Lamas, S.; Ortiz, A.; Rodrigues-Diez, R.R. Targeting the progression of chronic kidney disease. Nat. Rev. Nephrol. 2020, 16, 269–288. [Google Scholar] [CrossRef]
- Murton, M.; Goff-Leggett, D.; Bobrowska, A.; Garcia Sanchez, J.J.; James, G.; Wittbrodt, E.; Nolan, S.; Sörstadius, E.; Pecoits-Filho, R.; Tuttle, K. Burden of Chronic Kidney Disease by KDIGO Categories of Glomerular Filtration Rate and Albuminuria: A Systematic Review. Adv. Ther. 2021, 38, 180–200. [Google Scholar] [CrossRef]
- Stevens, L.A.; Viswanathan, G.; Weiner, G.E. Chronic kidney disease and end-stage renal disease in the elderly population: Current prevalence, future projections, and clinical significance. Adv. Chronic Kidney Dis. 2010, 17, 293–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, M.; Liu, S.-W.; Wang, L.-J.; Bai, Y.-M.; Zeng, X.-Y.; Guo, H.-B.; Liu, Y.-N.; Jiang, Y.-Y.; Dong, W.-L.; He, G.-X.; et al. Burden of diabetes, hyperglycaemia in China from to 2016: Findings from the 1990 to 2016, global burden of disease study. Diabetes Metab. 2018, 45, 286–293. [Google Scholar] [CrossRef]
- Duan, J.; Wang, C.; Liu, D.; Qiao, Y.; Pan, S.; Jiang, D.; Zhao, Z.; Liang, L.; Tian, F.; Yu, P.; et al. Prevalence and risk factors of chronic kidney disease and diabetic kidney disease in Chinese rural residents: A cross-sectional survey. Sci. Rep. 2019, 9, 10408. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Astor, B.C.; Lewis, J.; Hu, B.; Appel, L.J.; Lipkowitz, M.S.; Toto, R.D.; Wang, X.; Wright, J.T.; Greene, T.H. Longitudinal Progression Trajectory of GFR Among Patients With CKD. Am. J. Kidney Dis. 2012, 59, 504–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.E.; Qamar, M.; Wilke, R.A. Relative Contribution of Genetic and Environmental Factors in CKD. S. Dak. Med. 2021, 74, 306–309. [Google Scholar]
- Beyer-Westendorf, J.; Kreutz, R.; Posch, F.; Ay, C. The CHA2DS2-VASc score strongly correlates with glomerular filtration rate and predicts renal function decline over time in elderly patients with atrial fibrillation and chronic kidney disease. Int. J. Cardiol. 2018, 253, 71–77. [Google Scholar] [CrossRef]
- Remuzzi, G.; Benigni, A.; Remuzzi, A. Mechanisms of progression and regression of renal lesions of chronic nephropathies and diabetes. J. Clin. Investig. 2006, 116, 288–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cañadas-Garre, M.; Anderson, K.; Cappa, R.; Skelly, R.; Smyth, L.J.; McKnight, A.J.; Maxwell, A.P. Genetic Susceptibility to Chronic Kidney Disease—Some More Pieces for the Heritability Puzzle. Front. Genet. 2019, 10, 453. [Google Scholar] [CrossRef] [PubMed]
- Djudjaj, S.; Boor, P. Cellular and molecular mechanisms of kidney fibrosis. Mol. Asp. Med. 2019, 65, 16–36. [Google Scholar] [CrossRef]
- Grande, M.T.; Sanchez-Laorden, B.; Lopez-Blau, C.; De Frutos, C.A.; Boutet, A.; Arevalo, M.; Rowe, R.G.; Weiss, S.J.; Lopez-Novoa, J.M.; Nieto, M.A. Snail1-induced partial epithelial-to-mesenchymal transition drives renal fibrosis in mice and can be targeted to re-verse established disease. Nat. Med. 2015, 21, 989–997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajarnis, S.; Yheskel, M.; Williams, D.; Brefort, T.; Glaudemans, B.; Debaix, H.; Baum, M.; Devuyst, O.; Patel, V. Suppression of microRNA Activity in Kidney Collecting Ducts Induces Partial Loss of Epithelial Phenotype and Renal Fibrosis. J. Am. Soc. Nephrol. 2018, 29, 518–531. [Google Scholar] [CrossRef] [PubMed]
- Canaud, G.; Bonventre, V. Cell cycle arrest and the evolution of chronic kidney disease from acute kidney injury. Nephrol. Dial. Transpl. 2015, 30, 575–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lovisa, S.; LeBleu, V.S.; Tampe, B.; Sugimoto, H.; Vadnagara, K.; Carstens, J.L.; Wu, C.-C.; Hagos, Y.; Burckhardt, B.C.; Pentcheva-Hoang, T.; et al. Epithelial-to-mesenchymal transition induces cell cycle arrest and parenchymal damage in renal fibrosis. Nat. Med. 2015, 21, 998–1009. [Google Scholar] [CrossRef]
- Chung, K.W.; Lee, E.K.; Lee, M.K.; Oh, G.T.; Yu, B.P.; Chung, H.Y. Impairment of PPAR α and the Fatty Acid Oxidation Pathway Ag-gravates Renal Fibrosis during Aging. J. Am. Soc. Nephrol. 2018, 29, 1223–1237. [Google Scholar] [CrossRef] [Green Version]
- Liu, B.-C.; Tang, T.-T.; Lv, L.-L.; Lan, H.-Y. Renal tubule injury: A driving force toward chronic kidney disease. Kidney Int. 2018, 93, 568–579. [Google Scholar] [CrossRef]
- Song, Y.; Lv, S.; Wang, F.; Liu, X.; Cheng, J.; Liu, S.; Wang, X.; Chen, W.; Guan, G.; Liu, G.; et al. Overexpression of BMP-7 reverses TGF-β1-induced epithelial-mesenchymal transition. Mol. Med. Rep. 2020, 21, 833–841. [Google Scholar] [PubMed] [Green Version]
- Tampe, B.; Tampe, D.; Nyamsuren, G.; Klöpper, F.; Rapp, G.; Kauffels, A.; Lorf, T.; Zeisberg, E.M.; Müller, G.A.; Kalluri, R.; et al. Pharmacological induction of hypoxia-inducible transcription factor ARNT attenuates chronic kidney failure. J. Clin. Investig. 2018, 128, 3053–3070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tampe, B.; Tampe, D.; Zeisberg, E.M.; Müller, G.A.; Bechtel-Walz, W.; Koziolek, M.; Kalluri, R.; Zeisberg, M. Induction of Tet3-dependent Epigenetic Remodeling by Low-dose Hydralazine Attenuates Progression of Chronic Kidney Disease. EBioMedicine 2014, 2, 19–36. [Google Scholar] [CrossRef] [Green Version]
- Tampe, B.; Steinle, U.; Tampe, D.; Carstens, J.; Korsten, P.; Zeisberg, E.M.; Müller, G.A.; Kalluri, R.; Zeisberg, M. Low-dose hydralazine prevents fibrosis in a murine model of acute kidney injury–to–chronic kidney disease progression. Kidney Int. 2016, 91, 157–176. [Google Scholar] [CrossRef] [PubMed]
- Larkin, B.P.; Saad, S.; Glastras, S.J.; Nguyen, L.T.; Hou, M.; Chen, H.; Wang, R.; Pollock, C.A. Low-dose hydralazine during gestation reduces renal fibrosis in rodent offspring exposed to maternal high fat diet. PLoS ONE 2021, 16, e0248854. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Zang, X.; Ponnusamy, M.; Masucci, M.V.; Tolbert, E.; Gong, R.; Zhao, T.C.; Liu, N.; Bayliss, G.; Dworkin, L.D.; et al. Enhancer of Zeste Homolog 2 Inhibition Attenuates Renal Fibrosis by Maintaining Smad7 and Phosphatase and Tensin Homolog Ex-pression. J. Am. Soc. Nephrol. 2016, 27, 2092–2108. [Google Scholar] [CrossRef] [Green Version]
- Morgado-Pascual, J.L.; Rayego-Mateos, S.; Tejedor, L.; Suarez-Alvarez, B.; Ruiz-Ortega, M. Bromodomain and Extraterminal Pro-teins as Novel Epigenetic Targets for Renal Diseases. Front. Pharmacol. 2019, 10, 1315. [Google Scholar] [CrossRef]
- Mello, M.L.S. Sodium Valproate-Induced Chromatin Remodeling. Front. Cell Dev. Biol. 2021, 9, 645518. [Google Scholar] [CrossRef]
- Heung, M.; Steffick, D.E.; Zivin, K.; Gillespie, B.W.; Banerjee, T.; Hsu, C.-Y.; Powe, N.R.; Pavkov, M.E.; Williams, D.E.; Saran, R.; et al. Acute Kidney Injury Recovery Pattern and Subsequent Risk of CKD: An Analysis of Veterans Health Administration Data. Am. J. Kidney Dis. 2016, 67, 742–752. [Google Scholar] [CrossRef]
- Ishani, A.; Xue, J.L.; Himmelfarb, J.; Eggers, P.W.; Kimmel, P.L.; Molitoris, B.A.; Collins, A.J. Acute Kidney Injury Increases Risk of ESRD among Elderly. J. Am. Soc. Nephrol. 2008, 20, 223–228. [Google Scholar] [CrossRef] [Green Version]
- Liu, K.D.; Yang, J.; Tan, T.C.; Glidden, D.V.; Zheng, S.; Pravoverov, L.; Hsu, C.Y.; Go, A.S. Risk Factors for Recurrent Acute Kidney Injury in a Large Population-Based Cohort. Am. J. Kidney Dis. 2019, 73, 163–173. [Google Scholar] [CrossRef] [Green Version]
- Coca, S.; Singanamala, S.; Parikh, C.R. Chronic kidney disease after acute kidney injury: A systematic review and meta-analysis. Kidney Int. 2012, 81, 442–448. [Google Scholar] [CrossRef] [Green Version]
- Amdur, R.L.; Chawla, L.S.; Amodeo, S.; Kimmel, P.L.; Palant, C.E. Outcomes following diagnosis of acute renal failure in U.S. veterans: Focus on acute tubular necrosis. Kidney Int. 2009, 76, 1089–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kashani, K.; Kellum, J.A. Novel biomarkers indicating repair or progression after acute kidney injury. Curr. Opin. Nephrol. Hypertens. 2015, 24, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Sabbisetti, V.S.; Waikar, S.S.; Antoine, D.J.; Smiles, A.; Wang, C.; Ravisankar, A.; Ito, K.; Sharma, S.; Ramadesikan, S.; Lee, M.; et al. Blood Kidney Injury Molecule-1 Is a Biomarker of Acute and Chronic Kidney Injury and Predicts Progression to ESRD in Type I Diabetes. J. Am. Soc. Nephrol. 2014, 25, 2177–2186. [Google Scholar] [CrossRef]
- Teo, S.H.; Endre, Z.H. Biomarkers in acute kidney injury (AKI). Best Pract. Res. Clin. Anaesthesiol. 2017, 31, 331–344. [Google Scholar] [CrossRef] [PubMed]
- Göcze, I.; Jauch, D.; Götz, M.; Kennedy, P.; Jung, B.; Zeman, F.; Gnewuch, C.; Graf, B.M.; Gnann, W.; Banas, B.; et al. Biomarker-guided Intervention to Prevent Acute Kidney Injury After Major Surgery: The Prospective Randomized BigpAK Study. Ann. Surg. 2018, 267, 1013–1020. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Besschetnova, T.Y.; Brooks, C.R.; Shah, J.V.; Bonventre, J.V. Epithelial cell cycle arrest in G2/M mediates kidney fibrosis after injury. Nat. Med. 2010, 16, 535–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basile, D. The endothelial cell in ischemic acute kidney injury: Implications for acute and chronic function. Kidney Int. 2007, 72, 151–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Little, M.H.; Kairath, P. Does Renal Repair Recapitulate Kidney Development? J. Am. Soc. Nephrol. 2017, 28, 34–46. [Google Scholar] [CrossRef] [Green Version]
- Kramann, R.; Wongboonsin, J.; Chang-Panesso, M.; Machado, F.G.; Humphreys, B.D. Gli1 + Pericyte Loss Induces Capillary Rare-faction and Proximal Tubular Injury. J. Am. Soc. Nephrol. 2017, 28, 776–784. [Google Scholar] [CrossRef] [Green Version]
- Sato, Y.; Yanagita, M. Immune cells and inflammation in AKI to CKD progression. Am. J. Physiol. Physiol. 2018, 315, F1501–F1512. [Google Scholar] [CrossRef]
- NICE-SUGAR Study Investigators; Finfer, S.; Chittock, D.R.; Su, S.Y.; Blair, D.; Foster, D.; Dhingra, V.; Bellomo, R.; Cook, D.; Dodek, P.; et al. Intensive versus conventional glucose control in critically ill patients. N. Engl. J. Med. 2009, 360, 1283–1297. [Google Scholar]
- Asfar, P.; Meziani, F.; Hamel, J.-F.; Grelon, F.; Mégarbane, B.; Anguel, N.; Mira, J.-P.; Dequin, P.-F.; Gergaud, S.; Weiss, N.; et al. High versus Low Blood-Pressure Target in Patients with Septic Shock. N. Engl. J. Med. 2014, 370, 1583–1593. [Google Scholar] [CrossRef] [Green Version]
- Kaushal, G.P.; Shah, S.V. Challenges and Advances in the Treatment of AKI. J. Am. Soc. Nephrol. 2014, 25, 877–883. [Google Scholar] [CrossRef] [PubMed]
- Hausenloy, D.J.; Candilio, L.; Evans, R.; Ariti, C.; Jenkins, D.P.; Kolvekar, S.; Knight, R.; Kunst, G.; Laing, C.; Nicholas, J.; et al. Remote Ischemic Preconditioning and Outcomes of Cardiac Surgery. N. Engl. J. Med. 2015, 373, 1408–1417. [Google Scholar] [CrossRef] [PubMed]
- Floege, J.; Amann, K. Primary glomerulonephritides. Lancet 2016, 387, 2036–2048. [Google Scholar] [CrossRef]
- Friedman, D.; Pollak, M.R. APOL1and Kidney Disease: From Genetics to Biology. Annu. Rev. Physiol. 2020, 82, 323–342. [Google Scholar] [CrossRef] [Green Version]
- Turkmen, K.; Baloglu, I. Fabry disease: Where are we now? Int. Urol. Nephrol. 2020, 52, 2113–2122. [Google Scholar] [CrossRef] [PubMed]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic Kidney Disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Gnudi, L.; Coward, R.M.; Long, D.A. Diabetic Nephropathy: Perspective on Novel Molecular Mechanisms. Trends Endocrinol. Metab. 2016, 27, 820–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallon, V.; Gerasimova, M.; Rose, M.A.; Masuda, T.; Satriano, J.; Mayoux, E.; Koepsell, H.; Thomson, S.C.; Rieg, T. SGLT2 inhibitor em-pagliflozin reduces renal growth and albuminuria in proportion to hyperglycemia and prevents glomerular hyperfiltration in diabetic Akita mice. Am. J. Physiol. Renal. Physiol. 2014, 306, F194–F204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonneijck, L.; Muskiet, M.H.A.; Smits, M.M.; van Bommel, E.J.; Heerspink, H.J.L.; van Raalte, D.H.; Joles, J.A. Glomerular Hyperfiltration in Diabetes: Mechanisms, Clinical Significance, and Treatment. J. Am. Soc. Nephrol. 2017, 28, 1023–1039. [Google Scholar] [CrossRef] [Green Version]
- Thomas, M.C.; Brownlee, M.; Susztak, K.; Sharma, K.; Jandeleit-Dahm, K.A.; Zoungas, S.; Rossing, P.; Groop, P.H.; Cooper, M.E. Diabetic kidney disease. Nat. Rev. Dis. Primers 2015, 1, 15018. [Google Scholar] [CrossRef]
- Ravid, M.; Brosh, D.; Ravid-Safran, D.; Levy, Z.; Rachmani, R. Main Risk Factors for Nephropathy in Type 2 Diabetes Mellitus Are Plasma Cholesterol Levels, Mean Blood Pressure, and Hyperglycemia. Arch. Intern. Med. 1998, 158, 998–1004. [Google Scholar] [CrossRef]
- Alicic, R.Z.; Rooney, M.T.; Tuttle, K.R. Diabetic Kidney Disease: Challenges, Progress, and Possibilities. Clin. J. Am. Soc. Nephrol. 2017, 12, 2032–2045. [Google Scholar] [CrossRef]
- Navarro-González, J.F.; Mora-Fernández, C.; Muros de Fuentes, M.; Chahin, J.; Méndez, M.L.; Gallego, E.; Macía, M.; del Castillo, N.; Rivero, A.; Getino, M.A.; et al. Effect of Pentoxifylline on Renal Function and Urinary Albumin Excretion in Patients with Diabetic Kidney Disease: The PREDIAN Trial. J. Am. Soc. Nephrol. 2015, 26, 220–229. [Google Scholar] [CrossRef] [Green Version]
- Vogt, L.; Bangalore, S.; Fayyad, R.; Melamed, S.; Hovingh, G.K.; DeMicco, D.A.; Waters, D.D. Atorvastatin Has a Dose-Dependent Beneficial Effect on Kidney Function and Associated Cardiovascular Outcomes: Post Hoc Analysis of 6 Double-Blind Ran-domized Controlled Trials. J. Am. Heart Assoc. 2019, 8, e010827. [Google Scholar] [CrossRef] [Green Version]
- De Zeeuw, D.; Anzalone, D.A.; Cain, V.A.; Cressman, M.D.; Heerspink, H.J.; Molitoris, B.A.; Monyak, J.T.; Parving, H.H.; Remuzzi, G.; Sowers, J.R.; et al. Renal effects of atorvastatin and rosuvastatin in patients with diabetes who have progressive renal disease (PLANET I): A randomised clinical trial. Lancet Diabetes Endocrinol. 2015, 3, 181–190. [Google Scholar] [CrossRef]
- Rutter, M.; Prais, H.R.; Charlton-Menys, V.; Gittins, M.; Roberts, C.; Davies, R.R.; Moorhouse, A.; Jinadev, P.; France, M.; Wiles, P.G.; et al. Protection Against Nephropathy in Diabetes with Atorvastatin (PANDA): A randomized double-blind placebo-controlled trial of high- vs. low-dose atorvastatin1. Diabet. Med. 2010, 28, 100–108. [Google Scholar] [CrossRef]
- Ansquer, J.C.; Foucher, C.; Rattier, S.; Taskinen, M.R.; Steiner, G.; DAIS Investigators. Fenofibrate reduces progression to microalbu-minuria over 3 years in a placebo-controlled study in type 2 diabetes: Results from the Diabetes Atherosclerosis Intervention Study (DAIS). Am. J. Kidney Dis. 2005, 45, 485–493. [Google Scholar] [CrossRef]
- Miyazaki, Y.; Cersosimo, E.; Triplitt, C.; DeFronzo, R. Rosiglitazone decreases albuminuria in type 2 diabetic patients. Kidney Int. 2007, 72, 1367–1373. [Google Scholar] [CrossRef] [Green Version]
- Sarafidis, P.A. Thiazolidinediones and diabetic nephropathy: Need for a closer examination? J. Cardiometab. Syndr. Fall 2007, 2, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; De Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef] [PubMed]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.; Cahn, A.; Trimarco, B.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef]
- Alicic, R.Z.; Neumiller, J.J.; Johnson, E.J.; Dieter, B.; Tuttle, K. Sodium–Glucose Cotransporter 2 Inhibition and Diabetic Kidney Disease. Diabetes 2019, 68, 248–257. [Google Scholar] [CrossRef] [Green Version]
- Tejedor Jorge, A. Hemodynamic and renal implications of sodium-glucose cotransporter- 2 inhibitors in type 2 diabetes mellitus. Med. Clin. 2016, 147, 35–43. [Google Scholar] [CrossRef]
- Chilton, R.; Tikkanen, I.; Cannon, C.P.; Crowe, S.; Woerle, H.J.; Broedl, U.C.; Johansen, O.E. Effects of empagliflozin on blood pressure and markers of arterial stiffness and vascular resistance in patients with type 2 diabetes. Diabetes Obes. Metab. 2015, 17, 1180–1193. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.; Perkins, B.A.; Fitchett, D.H.; Husain, M.; Cherney, D.Z. Sodium Glucose Cotransporter 2 Inhibitors in the Treatment of Diabetes Mellitus: Cardiovascular and Kidney Effects, Potential Mechanisms, and Clinical Applications. Circulation 2016, 134, 752–772. [Google Scholar] [CrossRef]
- Kalra, S. Sodium Glucose Co-Transporter-2 (SGLT2) Inhibitors: A Review of Their Basic and Clinical Pharmacology. Diabetes Ther. 2014, 5, 355–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez-Fernandez, B.; Sarafidis, P.; Kanbay, M.; Navarro-González, J.F.; Soler, M.J.; Górriz, J.L.; Ortiz, A. SGLT2 inhibitors for non-diabetic kidney disease: Drugs to treat CKD that also improve glycaemia. Clin. Kidney J. 2020, 13, 728–733. [Google Scholar] [CrossRef]
- Costa, R.; Remigante, A.; Civello, D.A.; Bernardinelli, E.; Szabó, Z.; Morabito, R.; Marino, A.; Sarikas, A.; Patsch, W.; Paulmichl, M.; et al. O-GlcNAcylation Suppresses the Ion Current IClswell by Preventing the Binding of the Protein ICln to α-Integrin. Front. Cell Dev. Biol. 2020, 8, 607080. [Google Scholar] [CrossRef] [PubMed]
- Okada, Y.; Numata, T.; Sato-Numata, K.; Sabirov, R.Z.; Liu, H.; Mori, S.I.; Morishima, S. Roles of volume-regulatory anion channels, VSOR and Maxi-Cl, in apoptosis, cisplatin resistance, necrosis, ischemic cell death, stroke and myocardial infarction. Curr. Top. Membr. 2019, 83, 205–283. [Google Scholar] [PubMed]
- Sugahara, S.; Kume, S.; Chin-Kanasaki, M.; Tomita, I.; Yasuda-Yamahara, M.; Yamahara, K.; Takeda, N.; Osawa, N.; Yanagita, M.; Araki, S.I.; et al. Protein O-GlcNAcylation Is Essential for the Maintenance of Renal Energy Homeostasis and Function via Lipolysis during Fasting and Diabetes. J. Am. Soc. Nephrol. 2019, 30, 962–978. [Google Scholar] [CrossRef]
- Furst, J.; Gschwentner, M.; Ritter, M.; Botta, G.; Jakab, M.; Mayer, M.; Garavaglia, L.; Bazzini, C.; Rodighiero, S.; Meyer, G.; et al. Molecular and functional aspects of anionic channels activated during regulatory volume decrease in mammalian cells. Pflugers Arch. 2002, 444, 1–25. [Google Scholar] [CrossRef]
- Ku, E.; Lee, B.J.; Wei, J.; Weir, M.R. Hypertension in CKD: Core Curriculum 2019. Am. J. Kidney Dis. 2019, 74, 120–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taler, S.J.; Agarwal, R.; Bakris, G.L.; Flynn, J.T.; Nilsson, P.M.; Rahman, M.; Sanders, P.; Textor, S.C.; Weir, M.R.; Townsend, R.R. KDOQI US Commentary on the 2012 KDIGO Clinical Practice Guideline for Management of Blood Pressure in CKD. Am. J. Kidney Dis. 2013, 62, 201–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kidney Disease: Improving Global Outcomes (KDIGO) Blood Pressure Work Group. KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney Int 2021, 99, S1–S87. [Google Scholar] [CrossRef]
- Hsu, C.-N.; Tain, Y.-L. Gasotransmitters for the Therapeutic Prevention of Hypertension and Kidney Disease. Int. J. Mol. Sci. 2021, 22, 7808. [Google Scholar] [CrossRef] [PubMed]
- Bakris, G.; Hart, P.; Ritz, E. Beta blockers in the management of chronic kidney disease. Kidney Int. 2006, 70, 1905–1913. [Google Scholar] [CrossRef] [Green Version]
- Pugh, D.; Gallacher, P.J.; Dhaun, N. Management of Hypertension in Chronic Kidney Disease. Drugs 2019, 79, 365–379. [Google Scholar] [CrossRef] [Green Version]
- Chung, E.Y.; Ruospo, M.; Natale, P.; Bolignano, D.; Navaneethan, S.D.; Palmer, S.C.; Strippoli, G.F. Aldosterone antagonists in addition to renin angiotensin system antagonists for preventing the progression of chronic kidney disease. Cochrane Database Syst. Rev. 2020, 10, CD007004. [Google Scholar] [CrossRef] [PubMed]
- Bolignano, D.; Palmer, S.C.; Navaneethan, S.D.; Strippoli, G.F. Aldosterone antagonists for preventing the progression of chronic kidney disease. Cochrane Database Syst. Rev. 2014, 29, CD007004. [Google Scholar] [CrossRef]
- Takahashi, S.; Katada, J.; Daida, H.; Kitamura, F.; Yokoyama, K. Effects of mineralocorticoid receptor antagonists in proteinuric kidney disease: A systematic review and meta-analysis of randomized controlled trials. J. Hypertens. 2019, 37, 2307–2324. [Google Scholar]
- Grune, J.; Beyhoff, N.; Smeir, E.; Chudek, R.; Blumrich, A.; Bán, Z.; Brix, S.; Betz, I.R.; Schupp, M.; Foryst-Ludwig, A.; et al. Selective Mineralocorticoid Receptor Cofactor Modulation as Molecular Basis for Finerenone’s Antifibrotic Activity. Hypertension 2018, 71, 599–608. [Google Scholar] [CrossRef]
- Agarwal, R.; Kolkhof, P.; Bakris, G.; Bauersachs, J.; Haller, H.; Wada, T.; Zannad, F. Steroidal and non-steroidal mineralocorticoid receptor antagonists in cardiorenal medicine. Eur Heart J. 2021, 42, 152–161. [Google Scholar] [CrossRef]
- Pitt, B.; Kober, L.; Ponikowski, P.; Gheorghiade, M.; Filippatos, G.; Krum, H.; Nowack, C.; Kolkhof, P.; Kim, S.-Y.; Zannad, F. Safety and tolerability of the novel non-steroidal mineralocorticoid receptor antagonist BAY 94-8862 in patients with chronic heart failure and mild or moderate chronic kidney disease: A randomized, double-blind trial. Eur. Hear. J. 2013, 34, 2453–2463. [Google Scholar] [CrossRef]
- Bakris, G.L.; Agarwal, R.; Anker, S.D.; Pitt, B.; Ruilope, L.M.; Rossing, P.; Kolkhof, P.; Nowack, C.; Schloemer, P.; Joseph, A.; et al. Effect of Finerenone on Chronic Kidney Disease Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2020, 383, 2219–2229. [Google Scholar] [CrossRef]
- Ito, S.; Kashihara, N.; Shikata, K.; Nangaku, M.; Wada, T.; Okuda, Y.; Sawanobori, T. Esaxerenone (CS-3150) in Patients with Type 2 Diabetes and Microalbuminuria (ESAX-DN): Phase 3 Randomized Controlled Clinical Trial. Clin. J. Am. Soc. Nephrol. 2020, 15, 1715–1727. [Google Scholar] [CrossRef] [PubMed]
- Itoh, H.; Ito, S.; Rakugi, H.; Okuda, Y.; Nishioka, S. Efficacy and safety of dosage-escalation of low-dosage esaxerenone added to a RAS inhibitor in hypertensive patients with type 2 diabetes and albuminuria: A single-arm, open-label study. Hypertens. Res. 2019, 42, 1572–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rico-Mesa, J.S.; White, A.; Ahmadian-Tehrani, A.; Anderson, A.S. Mineralocorticoid Receptor Antagonists: A Comprehensive Re-view of Finerenone. Curr. Cardiol. Rep. 2020, 22, 140. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.D.; Vaduganathan, M.; Claggett, B.L.; Packer, M.; Zile, M.; Swedberg, K.; Rouleau, J.; Pfeffer, M.A.; Desai, A.; Lund, L.H.; et al. Sacubitril/Valsartan Across the Spectrum of Ejection Fraction in Heart Failure. Circulation 2020, 141, 352–361. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Claggett, B.; Lefkowitz, M.P.; McMurray, J.J.V.; Rouleau, J.L.; Solomon, S.D.; Zile, M.R. Effect of neprilysin inhibition on renal function in patients with type 2 diabetes and chronic heart failure who are receiving target doses of inhibitors of the ren-in-angiotensin system: A secondary analysis of the PARADIGM-HF trial. Lancet Diab. Endocrinol. 2018, 6, 547–554. [Google Scholar] [CrossRef]
- Collins, A.J.; Foley, R.N.; Herzog, C.; Chavers, B.; Gilbertson, D.; Ishani, A.; Kasiske, B.; Liu, J.; Mau, L.W.; McBean, M.; et al. US Renal Data System 2010 Annual Data Report. Am. J. Kidney Dis. 2011, 57, A8. [Google Scholar] [CrossRef]
- Gillen, D.L.; Worcester, E.M.; Coe, F.L. Decreased renal function among adults with a history of nephrolithiasis: A study of NHANES III. Kidney Int. 2005, 67, 685–690. [Google Scholar] [CrossRef] [Green Version]
- Uribarri, J. Chronic kidney disease and kidney stones. Curr. Opin. Nephrol. Hypertens. 2020, 29, 237–242. [Google Scholar] [CrossRef]
- Tang, X.; Lieske, J.C. Acute and chronic kidney injury in nephrolithiasis. Curr. Opin. Nephrol. Hypertens. 2014, 23, 385–390. [Google Scholar] [CrossRef] [Green Version]
- Rule, A.D.; Krambeck, A.E.; Lieske, J.C. Chronic Kidney Disease in Kidney Stone Formers. Clin. J. Am. Soc. Nephrol. 2011, 6, 2069–2075. [Google Scholar] [CrossRef] [Green Version]
- Gambaro, G.; Favaro, S.; D’Angelo, A. Risk for Renal Failure in Nephrolithiasis. Am. J. Kidney Dis. 2001, 37, 233–243. [Google Scholar] [CrossRef]
- Hoppe, B.; Martin-Higueras, C. Inherited conditions resulting in nephrolithiasis. Curr. Opin. Pediatr. 2020, 32, 273–283. [Google Scholar] [CrossRef]
- Edvardsson, V.O.; Goldfarb, D.; Lieske, J.C.; Lasic, L.B.; Anglani, F.; Milliner, D.S.; Palsson, R. Hereditary causes of kidney stones and chronic kidney disease. Pediatr. Nephrol. 2013, 28, 1923–1942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, T.V.M.; Maalouf, N.M. Uric acid stone disease: Lessons from recent human physiologic studies. Curr. Opin. Nephrol. Hypertens. 2020, 29, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Garrelfs, S.F.; Frishberg, Y.; Hulton, S.A.; Koren, M.J.; O’Riordan, W.D.; Cochat, P.; Deschênes, G.; Shasha-Lavsky, H.; Saland, J.M.; Hoff, W.G.V.; et al. Lumasiran, an RNAi Therapeutic for Primary Hyperoxaluria Type 1. N. Engl. J. Med. 2021, 384, 1216–1226. [Google Scholar] [CrossRef] [PubMed]
- Chapman, A.B.; Devuyst, O.; Eckardt, K.-U.; Gansevoort, R.T.; Harris, T.; Horie, S.; Kasiske, B.L.; Odland, D.; Pei, Y.; Perrone, R.D.; et al. Autosomal-dominant polycystic kidney disease (ADPKD): Executive summary from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2015, 88, 17–27. [Google Scholar] [CrossRef] [Green Version]
- Levy, M.; Feingold, J. Estimating prevalence in single-gene kidney diseases progressing to renal failure. Kidney Int. 2000, 58, 925–943. [Google Scholar] [CrossRef] [Green Version]
- Porath, B.; Gainullin, V.G.; Cornec-Le Gall, E.; Dillinger, E.K.; Heyer, C.M.; Hopp, K.; Edwards, M.E.; Madsen, C.D.; Mauritz, S.R.; Banks, C.J.; et al. Mutations in GANAB, Encoding the Glucosidase IIα Subunit, Cause Autosomal-Dominant Polycystic Kidney and Liver Disease. Am. J. Hum. Genet. 2016, 98, 1193–1207. [Google Scholar] [CrossRef] [Green Version]
- Cornec-Le Gall, E.; Alam, A.; Perrone, R.D. Autosomal dominant polycystic kidney disease. Lancet 2019, 393, 919–935. [Google Scholar] [CrossRef]
- Kim, D.Y.; Park, J.H. Genetic Mechanisms of ADPKD. Cystogenesis 2016, 933, 13–22. [Google Scholar] [CrossRef]
- Lanktree, M.; Chapman, A.B. New treatment paradigms for ADPKD: Moving towards precision medicine. Nat. Rev. Nephrol. 2017, 13, 750–768. [Google Scholar] [CrossRef]
- Torres, V.E.; Chapman, A.B.; Devuyst, O.; Gansevoort, R.T.; Perrone, R.D.; Dandurand, A.; Ouyang, J.; Czerwiec, F.S.; Blais, J.D.; for the TEMPO 4:4 Trial Investigators. Multicenter, open-label, extension trial to evaluate the long-term efficacy and safety of early versus delayed treatment with tolvaptan in autosomal dominant polycystic kidney disease: The TEMPO 4:4 Trial. Nephrol. Dial. Transplant. 2017, 33, 477–489. [Google Scholar] [CrossRef] [Green Version]
- Torres, V.E.; Chapman, A.B.; Devuyst, O.; Gansevoort, R.T.; Grantham, J.J.; Higashihara, E.; Perrone, R.D.; Krasa, H.B.; Ouyang, J.; Czerwiec, F.S. Tolvaptan in Patients with Autosomal Dominant Polycystic Kidney Disease. N. Engl. J. Med. 2012, 367, 2407–2418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bleyer, A.J.; Kidd, K.; Živná, M.; Kmoch, S. Autosomal Dominant Tubulointerstitial Kidney Disease. Adv. Chronic Kidney Dis. 2017, 24, 86–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devuyst, O.; Olinger, E.; Weber, S.; Eckardt, K.U.; Kmoch, S.; Rampoldi, L.; Bleyer, A.J. Autosomal dominant tubulointerstitial kidney disease. Nat. Rev. Dis. Primers 2019, 5, 60. [Google Scholar] [CrossRef] [Green Version]
- Eckardt, K.-U.; Alper, S.L.; Antignac, C.; Bleyer, A.J.; Chauveau, D.; Dahan, K.; Deltas, C.; Hosking, A.; Kmoch, S.; Rampoldi, L.; et al. Autosomal dominant tubulointerstitial kidney disease: Diagnosis, classification, and management—A KDIGO consensus report. Kidney Int. 2015, 88, 676–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, M.A.; Kohli, J.; Bloom, R.D. Immunosuppression for kidney transplantation: Where are we now and where are we going? Transplant. Rev. 2017, 31, 10–17. [Google Scholar] [CrossRef]
- De Lucena, D.D.; Rangel, É.B. Glucocorticoids use in kidney transplant setting. Expert Opin. Drug Metab. Toxicol. 2018, 14, 1023–1041. [Google Scholar] [CrossRef] [PubMed]
- Clayton, P.A.; McDonald, S.P.; Chapman, J.R.; Chadban, S.J. Mycophenolate versus azathioprine for kidney transplantation: A 15-year follow-up of a randomized trial. Transplantation 2012, 94, 152–158. [Google Scholar] [CrossRef]
- Casey, M.J.; Meier-Kriesche, H.U. Calcineurin inhibitors in kidney transplantation: Friend or foe? Curr. Opin. Nephrol. Hypertens. 2011, 20, 610–615. [Google Scholar] [CrossRef] [PubMed]
- Vanhove, T.; Annaert, P.; Kuypers, D.R. Clinical determinants of calcineurin inhibitor disposition: A mechanistic review. Drug Metab. Rev. 2016, 48, 88–112. [Google Scholar] [CrossRef]
- Fantus, D.; Rogers, N.M.; Grahammer, F.; Huber, T.B.; Thomson, A.W. Roles of mTOR complexes in the kidney: Implications for renal disease and transplantation. Nat. Rev. Nephrol. 2016, 12, 587–609. [Google Scholar] [CrossRef] [PubMed]
- Noble, J.; Jouve, T.; Janbon, B.; Rostaing, L.; Malvezzi, P. Belatacept in kidney transplantation and its limitations. Expert Rev. Clin. Immunol. 2019, 15, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.; Venetz, J.-P.; Tolkoff-Rubin, N.; Pascual, M. 2005 Immunosuppressive Strategies in Kidney Transplantation: Which Role for the Calcineurin Inhibitors? Transplantation 2005, 80, 289–296. [Google Scholar] [CrossRef]
- Tedesco-Silva, H.; Rial, M.D.C.; Santiago, J.C.; Mazzali, M.; Pacheco-Silva, A.; Torres, R. Optimizing the Clinical Utility of Sirolimus-Based Immunosuppression for Kidney Transplantation. Clin. Transplant. 2018, 33, e13464. [Google Scholar] [CrossRef] [PubMed]
- Préterre, J.; Visentin, J.; Saint Cricq, M.; Kaminski, H.; Del Bello, A.; Prezelin-Reydit, M.; Merville, P.; Kamar, N.; Couzi, L. Comparison of two strategies based on mammalian target of rapamycin inhibitors in secondary prevention of non-melanoma skin cancer after kidney transplantation, a pilot study. Clin. Transplant. 2021, 35, e14207. [Google Scholar] [CrossRef] [PubMed]
- Kuczera, P.; Ciaston-Mogilska, D.; Oslizlo, B.; Hycki, A.; Wiecek, A.; Adamczak, M. The Prevalence of Metabolic Acidosis in Patients with Different Stages of Chronic Kidney Disease: Single-Centre Study Kidney. Blood Press Res. 2020, 45, 863–872. [Google Scholar] [CrossRef] [PubMed]
- Di Iorio, B.R.; Bellasi, A.; Raphael, K.L.; Santoro, D.; Aucella, F.; Garofano, L.; Ceccarelli, M.; Di Lullo, L.; Capolongo, G.; Di Iorio, M.; et al. Treatment of metabolic acidosis with sodium bicarbonate delays progression of chronic kidney disease: The UBI Study. J. Nephrol. 2019, 32, 989–1001. [Google Scholar] [CrossRef] [Green Version]
- Nagami, G.T. Role of angiotensin II in the enhancement of ammonia production and secretion by the proximal tubule in met-abolic acidosis. Am. J. Physiol. Renal Physiol. 2008, 294, 874–880. [Google Scholar] [CrossRef] [Green Version]
- Wesson, D.E.; Simoni, J. Acid retention during kidney failure induces endothelin and aldosterone production which lead to pro-gressive GFR decline, a situation ameliorated by alkali diet. Kidney Int. 2010, 78, 1128–1135. [Google Scholar] [CrossRef] [Green Version]
- Wesson, D.E.; Nathan, T.; Rose, T.; Simoni, J.; Tran, R.M. Dietary protein induces endothelin-mediated kidney injury through en-hanced intrinsic acid production. Kidney Int. 2007, 71, 210–217. [Google Scholar] [CrossRef] [Green Version]
- Kovesdy, C.P.; Anderson, J.E.; Kalantar-Zadeh, K. Association of serum bicarbonate levels with mortality in patients with non-dialysis-dependent CKD. Nephrol. Dial. Transplant. 2008, 24, 1232–1237. [Google Scholar] [CrossRef] [Green Version]
- Levy, B.; Collin, S.; Sennoun, N.; Ducrocq, N.; Kimmoun, A.; Asfar, P.; Perez, P.; Meziani, F. Vascular hyporesponsiveness to vaso-pressors in septic shock: From bench to bedside. Intensive Care Med. 2010, 36, 2019–2029. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Mehrotra, R.; Fouque, D.; Kopple, J.D. Poor Nutritional Status and Inflammation: Metabolic Acidosis and Malnutrition-Inflammation Complex Syndrome in Chronic Renal Failure. Semin. Dial. 2004, 17, 455–465. [Google Scholar] [CrossRef]
- Kraut, J.A.; Madias, N.E. Metabolic acidosis is associated with increased risk of adverse kidney outcomes and mortality in patients with non-dialysis dependent chronic kidney disease: An observational cohort study. BMC Nephrol. 2021, 22, 185. [Google Scholar]
- De Brito-Ashurst, I.; Varagunam, M.; Raftery, M.J.; Yaqoob, M.M. Bicarbonate supplementation slows progression of CKD and im-proves nutritional status. J. Am. Soc. Nephrol. 2009, 20, 2075–2084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobre, M.; Yang, W.; Pan, Q.; Appel, L.; Bellovich, K.; Chen, J.; Feldman, H.; Fischer, M.J.; Ham, L.L.; Hostetter, T.; et al. Persistent High Serum Bicarbonate and the Risk of Heart Failure in Patients with Chronic Kidney Disease (CKD): A Report From the Chronic Renal Insufficiency Cohort (CRIC) Study. J. Am. Hear. Assoc. 2015, 4, e001599. [Google Scholar] [CrossRef] [Green Version]
- Goraya, N.; Simoni, J.; Jo, C.-H.; Wesson, D.E. Treatment of metabolic acidosis in patients with stage 3 chronic kidney disease with fruits and vegetables or oral bicarbonate reduces urine angiotensinogen and preserves glomerular filtration rate. Kidney Int. 2014, 86, 1031–1038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cupisti, A.; Kalantar-Zadeh, K. Management of natural and added dietary phosphorus burden in kidney disease. Semin. Nephrol. 2013, 33, 180–190. [Google Scholar] [CrossRef] [Green Version]
- Alvirdizadeh, S.; Yuzbashian, E.; Mirmiran, P.; Eghtesadi, S.; Azizi, F. A prospective study on total protein, plant protein and animal protein in relation to the risk of incident chronic kidney disease. BMC Nephrol. 2020, 21, 489. [Google Scholar] [CrossRef] [PubMed]
- Kontessis, P.; Jones, S.; Dodds, R.; Trevisan, R.; Nosadini, R.; Fioretto, P.; Borsato, M.; Sacerdoti, D.; Viberti, G. Renal, metabolic and hormonal responses to ingestion of animal and vegetable proteins. Kidney Int. 1990, 38, 136–144. [Google Scholar] [CrossRef] [Green Version]
- Hahn, D.; Hodson, E.M.; Fouque, D. Low protein diets for non-diabetic adults with chronic kidney disease. Cochrane Database Syst. Rev. 2018, 10, CD001892. [Google Scholar] [CrossRef] [PubMed]
- Yen, C.L.; Fan, P.C.; Lee, C.C.; Kuo, G.; Tu, K.H.; Chen, J.J.; Lee, T.H.; Hsu, H.H.; Tian, Y.C.; Chang, C.H. Advanced Chronic Kidney Disease with Low and Very Low GFR: Can a Low-Protein Diet Supplemented with Ketoanalogues Delay Dialysis? Nutrients 2020, 12, 3358. [Google Scholar] [CrossRef] [PubMed]
- Castaneda, C.; Gordon, P.L.; Uhlin, K.L.; Levey, A.S.; Kehayias, J.J.; Dwyer, J.T.; Fielding, R.A.; Roubenoff, R.; Singh, M.F. Resistance training to counteract the catabolism of a low protein diet in chronic renal insufficiency: A randomized, controlled trial. Ann. Intern. Med. 2001, 135, 965–976. [Google Scholar] [CrossRef]
- Cupisti, A.; Licitra, R.; Chisari, C.; Stampacchia, G.; D’Alessandro, C.; Galetta, F.; Rossi, B.; Barsotti, G. Skeletal muscle and nutritional status in chronic renal failure on a protein restricted diet. J. Int. Med. 2004, 255, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Nangaku, M.; Eckardt, K.-U. Pathogenesis of Renal Anemia. Semin. Nephrol. 2006, 26, 261–268. [Google Scholar] [CrossRef] [PubMed]
- MacDougall, I.C. Novel Erythropoiesis-Stimulating Agents: A New Era in Anemia Management. Clin. J. Am. Soc. Nephrol. 2007, 3, 200–207. [Google Scholar] [CrossRef]
- Salamin, O.; Kuuranne, T.; Saugy, M.; Leuenberger, N. Erythropoietin as a performance-enhancing drug: Its mechanistic basis, detection, and potential adverse effects. Mol. Cell. Endocrinol. 2018, 464, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Pagani, A.; Nai, A.; Silvestri, L.; Camaschella, C. Hepcidin and Anemia: A Tight Relationship. Front. Physiol. 2019, 10, 1294. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-Y.; Babitt, J.L. Hepcidin regulation in the anemia of inflammation. Curr. Opin. Hematol. 2016, 23, 189–197. [Google Scholar] [CrossRef]
- Akchurin, O.; Patino, E.; Dalal, V.; Meza, K.; Bhatia, D.; Brovender, S.; Zhu, Y.-S.; Cunningham-Rundles, S.; Perelstein, E.; Kumar, J.; et al. Interleukin-6 Contributes to the Development of Anemia in Juvenile CKD. Kidney Int. Rep. 2018, 4, 470–483. [Google Scholar] [CrossRef] [Green Version]
- Babitt, J.L.; Lin, H.Y. Mechanisms of Anemia in CKD. J. Am. Soc. Nephrol. 2012, 23, 1631–1634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gossmann, J.; Thürmann, P.; Bachmann, T.; Weller, S.; Kachel, H.-G.; Schoeppe, W.; Scheuermann, E.-H. Mechanism of angiotensin converting enzyme inhibitor-related anemia in renal transplant recipients. Kidney Int. 1996, 50, 973–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, N.; Wish, J.B. Hypoxia-Inducible Factor Prolyl Hydroxylase Inhibitors: A Potential New Treatment for Anemia in Patients with CKD. Am. J. Kidney Dis. 2017, 69, 815–826. [Google Scholar] [CrossRef] [Green Version]
- Epstein, A.C.; Gleadle, J.M.; McNeill, L.A.; Hewitson, K.S.; O’Rourke, J.; Mole, D.R.; Mukherji, M.; Metzen, E.; Wilson, M.I.; Dhanda, A.; et al. C. elegans EGL-9 and Mammalian Homologs Define a Family of Dioxygenases that Regulate HIF by Prolyl Hydroxylation. Cell 2001, 107, 43–54. [Google Scholar] [CrossRef] [Green Version]
- Chertow, G.M.; Pergola, P.E.; Farag, Y.M.; Agarwal, R.; Arnold, S.; Bako, G.; Block, G.A.; Burke, S.; Castillo, F.P.; Jardine, A.G.; et al. Vadadustat in Patients with Anemia and Non–Dialysis-Dependent CKD. N. Engl. J. Med. 2021, 384, 1589–1600. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Qian, J.; Chen, J.; Yu, X.; Mei, C.; Hao, C.; Jiang, G.; Lin, H.; Zhang, X.; Zuo, L.; et al. Phase 2 studies of oral hypoxia-inducible factor prolyl hydroxylase inhibitor FG-4592 for treatment of anemia in China. Nephrol. Dial. Transplant. 2017, 32, 1373–1386. [Google Scholar] [CrossRef] [PubMed]
- Linder, K.E.; Krawczynski, M.A.; Laskey, D. Sodium Zirconium Cyclosilicate (ZS-9): A Novel Agent for the Treatment of Hyper-kalemia. Pharmacotherapy 2016, 36, 923–933. [Google Scholar] [CrossRef]
- Colbert, G.B.; Patel, D.; Lerma, E.V. Patiromer for the treatment of hyperkalemia. Expert Rev. Clin. Pharmacol. 2020, 13, 563–570. [Google Scholar] [CrossRef]
- Leon, S.J.; Harasemiw, O.; Tangri, N. New therapies for hyperkalemia. Curr. Opin. Nephrol. Hypertens. 2019, 28, 238–244. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Andress, D.L.; Bakris, G.; Brennan, J.J.; Correa-Rotter, R.; Dey, J.; Hou, F.F.; Kitzman, D.W.; Kohan, D.; Makino, H.; et al. Rationale and protocol of the Study Of diabetic Nephropathy with AtRasentan (SONAR) trial: A clinical trial design novel to diabetic nephropathy. Diabetes Obes. Metab. 2018, 20, 1369–1376. [Google Scholar] [CrossRef] [Green Version]
- Cho, M.E.; Smith, D.C.; Branton, M.H.; Penzak, S.R.; Kopp, J. Pirfenidone Slows Renal Function Decline in Patients with Focal Segmental Glomerulosclerosis. Clin. J. Am. Soc. Nephrol. 2007, 2, 906–913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kashtan, C. Multidisciplinary Management of Alport Syndrome: Current Perspectives. J. Multidiscip. Healthc. 2021, 2021, 1169–1180. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Moreno, J.M.; Fontecha-Barriuso, M.; Martin-Sanchez, D.; Guerrero-Mauvecin, J.; Goma-Garces, E.; Fernandez-Fernandez, B.; Carriazo, S.; Sanchez-Niño, M.D.; Ramos, A.M.; Ruiz-Ortega, M.; et al. Epigenetic Modifiers as Potential Therapeutic Targets in Diabetic Kidney Disease. Int. J. Mol. Sci. 2020, 21, 4113. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Schwartz, G.G.; Nicholls, S.J.; Buhr, K.A.; Ginsberg, H.N.; Johansson, J.O.; Kulikowski, E.; Lebioda, K.; Toth, P.P.; Wong, N.; et al. Effect of Apabetalone on Cardiovascular Events in Diabetes, CKD, and Recent Acute Coronary Syndrome. Clin. J. Am. Soc. Nephrol. 2021, 16, 705–716. [Google Scholar] [CrossRef] [PubMed]
- Nezu, M.; Suzuki, N.; Yamamoto, M. Targeting the KEAP1-NRF2 System to Prevent Kidney Disease Progression. Am. J. Nephrol. 2017, 45, 473–483. [Google Scholar] [CrossRef]
- Hye Khan, M.A.; Hwang, S.H.; Sharma, A.; Corbett, J.A.; Hammock, B.D.; Imig, J.D. A dual COX-2/sEH inhibitor improves the metabolic profile and reduces kidney injury in Zucker diabetic fatty rat. Prostaglandins Other Lipid Mediat. 2016, 125, 40–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imig, J.D. Prospective for cytochrome P450 epoxygenase cardiovascular and renal therapeutics. Pharmacol. Ther. 2018, 192, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Stavniichuk, A.; Savchuk, O.; Khan, A.H.; Jankiewicz, W.K.; Imig, J.D.; Merk, D. The effect of compound DM509 on kidney fibrosis in the conditions of the experimental mode. Visnyk Kyivskoho Natsionalnoho Universytetu Im. Tarasa Shevchenka Biol. 2020, 80, 10–15. [Google Scholar]
- Ding, D.C.; Shyu, W.C.; Lin, S.Z. Mesenchymal stem cells. Cell Transplant. 2011, 20, 5–14. [Google Scholar] [CrossRef] [Green Version]
- Kuppe, C.; Kramann, R. Role of mesenchymal stem cells in kidney injury and fibrosis. Curr. Opin. Nephrol. Hypertens. 2016, 25, 372–377. [Google Scholar] [CrossRef]
- Aghajani Nargesi, A.; Lerman, L.O.; Eirin, A. Mesenchymal stem cell-derived extracellular vesicles for kidney repair: Current status and looming challenges. Stem Cell Res. Ther. 2017, 8, 273. [Google Scholar] [CrossRef] [PubMed]
- Squillaro, T.; Peluso, G.; Galderisi, U. Clinical Trials with Mesenchymal Stem Cells: An Update. Cell Transplant. 2016, 25, 829–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.E.; Jang, J.E.; Kim, H.S.; Jung, M.K.; Ko, M.S.; Kim, M.O.; Park, H.S.; Oh, W.; Choi, S.J.; Jin, H.J.; et al. Mesenchymal stem cells prevent the progression of diabetic nephropathy by improving mi-tochondrial function in tubular epithelial cells. Exp. Mol. Med. 2019, 51, 1–14. [Google Scholar] [PubMed] [Green Version]
- Yoon, Y.M.; Lee, J.H.; Yun, C.W.; Lee, S.H. Pioglitazone Improves the Function of Human Mesenchymal Stem Cells in Chronic Kidney Disease Patients. Int. J. Mol. Sci. 2019, 20, 2314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
(A) The different declined rates of renal function in CKD with the target switch from superfast to slow rate. (B) The consequence of AKI on CKD progression, depending on the severity and frequency of episodes.
Figure 1.
(A) The different declined rates of renal function in CKD with the target switch from superfast to slow rate. (B) The consequence of AKI on CKD progression, depending on the severity and frequency of episodes.

Figure 2.
The risk factors and management strategies of CKD development and progression.

Figure 3.
The pathogenesis of diabetic nephropathy and mechanism of sodium-glucose cotransporter inhibitors-associated renoprotection.
Figure 3.
The pathogenesis of diabetic nephropathy and mechanism of sodium-glucose cotransporter inhibitors-associated renoprotection.

Figure 4.
The structure and action mechanisms of different MRAs generations such as spironolactone, eplerenone, and novel nonsteroidal MRAs (esaxerenone and finerenone). Novel nonsteroidal MRAs exert better anti-fibrotic and anti-inflammatory effects with renal tubular sparing effects on hyperkalemia.
Figure 4.
The structure and action mechanisms of different MRAs generations such as spironolactone, eplerenone, and novel nonsteroidal MRAs (esaxerenone and finerenone). Novel nonsteroidal MRAs exert better anti-fibrotic and anti-inflammatory effects with renal tubular sparing effects on hyperkalemia.

Figure 5.
Different causes of nephrolithiasis and urothithiasis with the recommended management strategies to avoid recurrence.
Figure 5.
Different causes of nephrolithiasis and urothithiasis with the recommended management strategies to avoid recurrence.

Figure 6.
The multiple-faceted mechanisms of metabolic acidosis on renal progression such as enhanced ammonia production in surviving nephrons with complement activation and increased endothelin production, leading to reduced GFR and augmented tubulointerstitial injury.
Figure 6.
The multiple-faceted mechanisms of metabolic acidosis on renal progression such as enhanced ammonia production in surviving nephrons with complement activation and increased endothelin production, leading to reduced GFR and augmented tubulointerstitial injury.


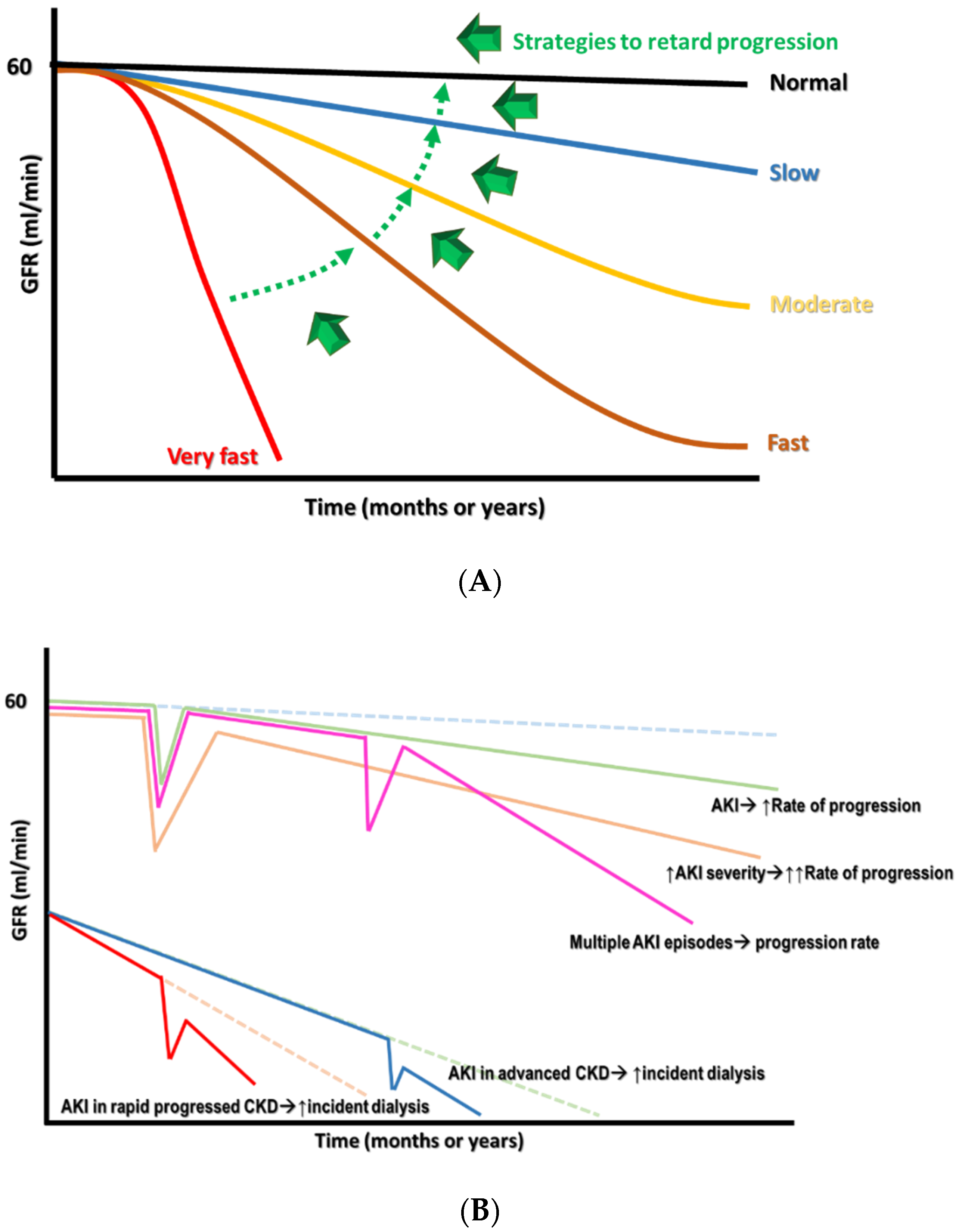{kind=link}
{kind=link}
{kind=link}
{kind=link}
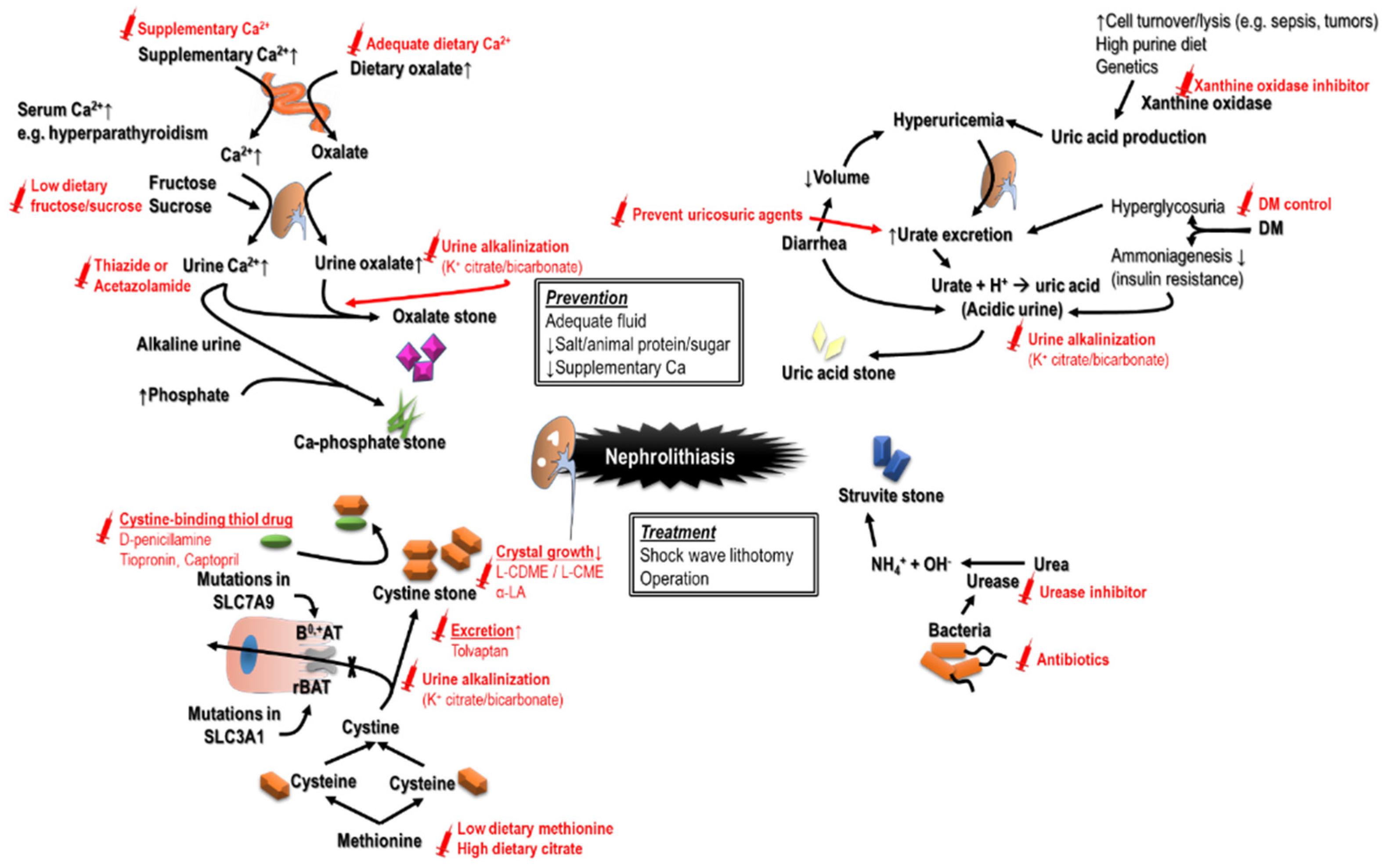{kind=link}
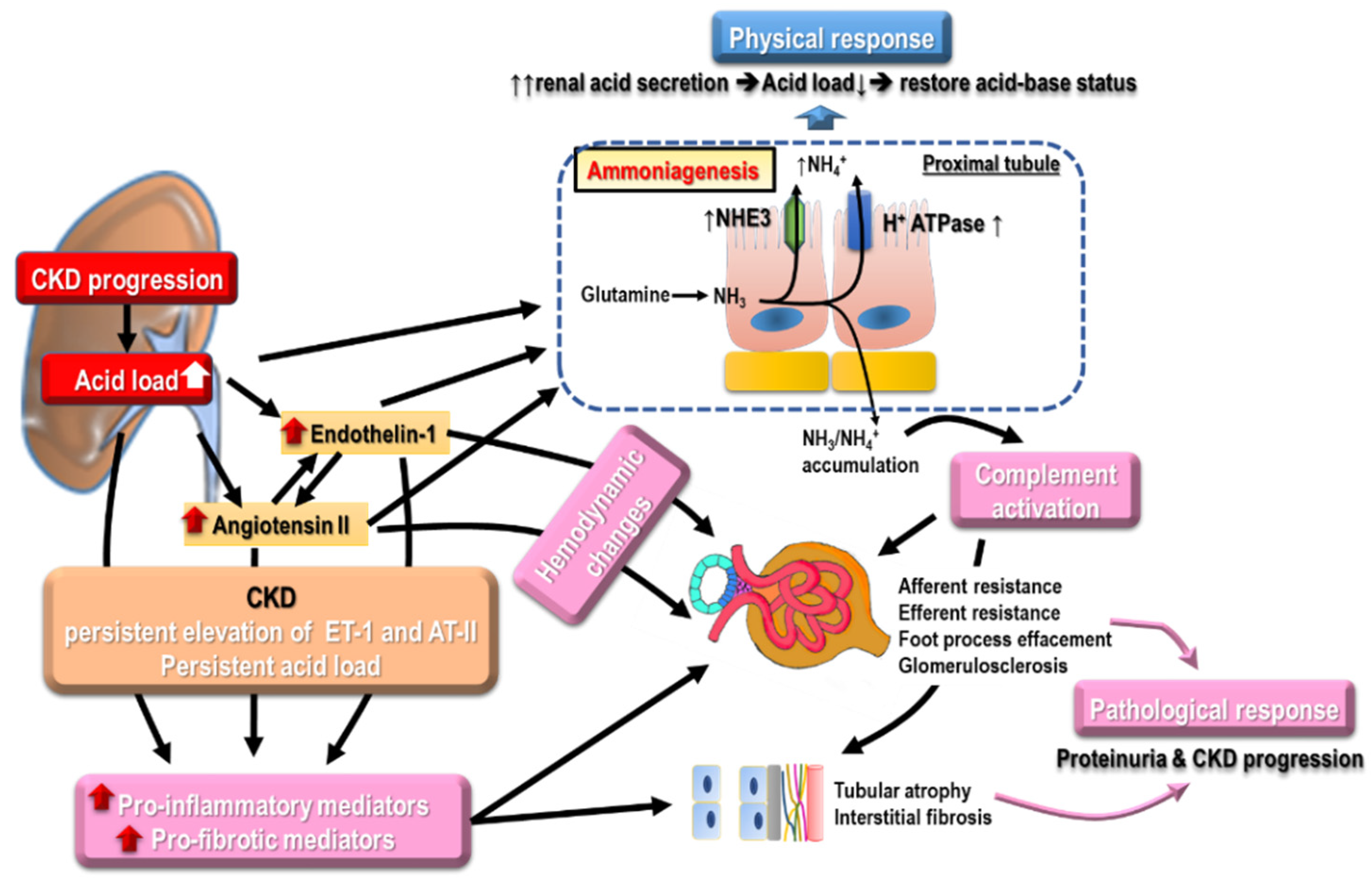{kind=link}
Table 1.
Common etiologies of acute kidney injury.
| Categories | Mechanism | Examples | Evaluation |
|---|---|---|---|
| Prerenal | Cardiac output↓ | Acute myocardial infarction, valve rupture, acute pericarditis, acute myocarditis Drugs exacerbate heart failure (COX inhibitors, CCB, TZD, DPP-4i) Drugs cause direct heart injury (rheumatologic agents (e.g., TNF-α inhibitors), anthracyclines, taxanes, targeted therapy (e.g., bevacizumab, sorafenib), anti-Parkinson (Pergolide, Pramipexole) | History: fever, vomiting, diarrhea, chest pain, orthopnea, palpitation, urine output↓, liver/CV diseases Drug: diuretics, NSAID Physical exam: BP↓/HR↑, skin turgor/mucosa, edema |
| True hypovolemia | Renal loss (diuretics, osmotic diuresis); Extrarenal loss (diarrhea, hemorrhage, burn, third spacing) | ||
| Effective volume↓ | Sepsis, neurogenic shock, anaphylaxis | ||
| Intrarenal vasoconstriction | Hypercalcemia, hepatorenal syndrome, drugs (CNIs, NSAID, vasoconstrictors.) | ||
| Intrinsic | Glomerular injury | Nephrotic (MCD, MPGN, drugs (NSAID, gold, penicillamine))213607Nephritic (IRGN, lupus nephritis, AAV, anti-GBM disease, IgAN, drugs (e.g., hydralazine)) | History: Fever, cellulitis, URI, flank pain, foamy urine, urine output↓, myalgia, hemoptysis Drug: antibiotics, NSAID, statin, contrast Physical exam: BP, Skin rash, arthritis |
| Tubular injury | Severe prerenal causes, toxins (endogenous: hemolysis, rhabdomyolysis, tumor lysis syndrome) or exogenous (aminoglycoside, contrast, CNIs, acyclovir, lithium, vancomycin)) | ||
| Interstitial injury | Allergy (drug: cephalosporin, penicillin, PPI, NSAID, herbs); Infection (bacteria, fungus, virus, leptospirosis); Autoimmune (Lupus, anti-TBM disease, AAV) | ||
| Vascular injury | Small caliber (TMA (malignant hypertension, HUS/TTP, DIC), scleroderma renal crisis) Large caliber (renal infarction, renal vein thrombosis) | ||
| Postrenal | Urinary tract | Benign prostatic hyperplasia; neurogenic bladder; Intra-ureter (stones, tumors); Extraureter (retroperitoneal fibrosis, intra-abdominal tumors) lesions | History: low urinary tract symptoms, gross hematuria Physical exam: suprapubic tenderness, abdomen mass Image: e.g., ultrasound |
| Intrarenal | Crystals (acyclovir, indinavir), stones, tumors, paraproteins (myeloma) |
Denote: AAV: ANCA associated vasculitis, COX: cyclooxygenase, CNIs: calcineurin inhibitors, DPP-4i: Dipeptidyl peptidase 4 inhibitors, DIC: disseminated intravascular coagulation, HUS: hemolytic uremic syndrome, IgAN: IgA nephropathy, MCD: minimal change disease, MPGN: membranoproliferative glomerulonephritis, NSAID: nonsteroidal anti-inflammatory drug, PPI: proton pump inhibitor, TBM: tubule basement membrane, TMA:thrombotic micrangiopathy, TNF: tumor necrosis factor, TTP: thrombotic thrombocytopenic purpura, TZD: Thiazolidinedione.
Table 2.
The therapy of glomerulopathy and the common side effects of the pharmacotherapy.
| Non-Immune Therapy | Immunosuppressant Therapy | Denote | |||||||
|---|---|---|---|---|---|---|---|---|---|
| ↓Dietary salt/protein SGLT2 inhibitors RAAS blockades Blood pressure Infection prophylaxis (vaccine, antibioticsantiviral agents) Vitamin D + calcium | Diuretics ↑Oncotic pressure (albumin infusion) Lipid lowering Anticoagulation (prevent or treat thromboembolism) | Steroids | Calcineurin inhibitors | Antimetabolite | Alkalizing agents | Anti-CD20 | PP | ||
| Prednisolone ACTH | Cyclosporine Tacrolimus | Mycophenolate Azathioprine | CYC Chlorambucil | Rituximab | |||||
| MCD | ν | ν | ν | ν | ν | ν | ν | ||
| FSGS | ν | ν | ν | ν | ν | Genetic test: Congenital/infantile type, APOL1 (adult) | |||
| MN | ν | ν | ν | ν | ν | ν | ν | Serum anti-PLA2R: diagnosis, follow-up and outcomes | |
| MPGN | ν | ν | ν | ν | Treat underlying diseases (e.g., MM, lymphoma or HCV) | ||||
| IgAN | ν | ν (IgAN+MCD) | ν | ν (some RTCs) | Adjuvant antimalarial Ongoing trial: Fostamatinib, Atacicept, Bortezomib | ||||
| LN | ν | ν (class V) | ν | ν | ν | ν | Antimalarial agents AZA for maintenance | ||
| AAV | ν | ν | ν | ν | ν severe AKI PH | Disease activity: chemokine C-X-C motif chemokine ligand 13, matrix metalloproteinase-3, tissue inhibitor of metalloproteinases-1 | |||
| Ani-GBM | ν | ν | ν | ν till anti-GBM (-) | Overlap syndrome (ANA, ANCA) | ||||
| Common S/E | Rare | Rare | ↑Glucose Cushing ↑BP | Nephrotoxic | GI upset Leukopenia | Bone marrow suppression Infertility | Infusion reaction, Infection Cytopenia | Fever Urticaria | |
Denote: AAV: ANCA associated vasculitis, BP: blood pressure, CYC: cyclophosphamide, FSGS: focal segmental glomerulonephropathy, GI: gastrointestinal, GBM: glomerular basement membrane, IgAN: IgA nephropathy, LN: lupus nephritis, MCD: minimal change disease, MM: multiple myeloma, MN: membranous nephropathy, MPGN: membranoproliferative glomerulonephritis, PH: pulmonary hemorrhage, PP: plasmapheresis, RAAS: renin-agiotensin-aldosterone system, SGLT2: sodium glucose cotransporter 2, S/E: side effect.
Table 3.
Potential novel agents targeting CKD progression.
| Categories | Agents | Mechanism |
|---|---|---|
| Anti-fibrotic | Pirfenidone | TGF-β inhibitor |
| Fresolimumab | Anti-TGF-β monoclonal antibody | |
| FG3019 | Anti-CTGF monoclonal antibody | |
| Anti-oxidative stress | Bardoxolone methyl | Activating Nrf-2 and inhibiting NF-κB pathway |
| Probucol | Phenolic antioxidant | |
| Anti-inflammatory | Adalimumab | Anti-TNF-α monoclonal antibody |
| Infliximab | Anti-TNF-α monoclonal antibody | |
| Etanercept | soluble recombinant receptor targeting TNF-α | |
| Rilonacept | Anti-IL-1 monoclonal antibody | |
| Signal transduction pathway | Ruboxistaurin | PKCβ inhibitor |
| Selonsertib | ASK1 inhibitor | |
| Fasudil | Rho kinase inhibitor | |
| Vasoactive agents | Avosentan | ET type A receptor antagonist |
| Atrasentan | ET type A receptor antagonist | |
| Sitaxsentan | ET type A receptor antagonist | |
| Bosentan | Dual ET type A and B antagonist | |
| Sparsentan | Selective dual antagonist of AT1 receptor and the ET type A receptor. | |
| Phosphodiesterase inhibitor | PF-00489791 | Phosphodiesterase V inhibitor |
| Cell-cell/cell-matrix interaction | GCS-100 | Galectin-3 inhibitor |
AT1: angiotensin II type I, CTGF: connective tissue growth factor, ET: Endothelin, IL-1: interleukin-1, TGF-β: transforming growth factor-β, TNF-α: tumor necrosis factor-α.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Yan, M.-T.; Chao, C.-T.; Lin, S.-H. Chronic Kidney Disease: Strategies to Retard Progression. Int. J. Mol. Sci. 2021, 22, 10084. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms221810084
AMA Style
Yan M-T, Chao C-T, Lin S-H. Chronic Kidney Disease: Strategies to Retard Progression. International Journal of Molecular Sciences. 2021; 22(18):10084. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms221810084
Chicago/Turabian StyleYan, Ming-Tso, Chia-Ter Chao, and Shih-Hua Lin. 2021. "Chronic Kidney Disease: Strategies to Retard Progression" International Journal of Molecular Sciences 22, no. 18: 10084. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms221810084
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.