
Multiplex Screening for Interacting Compounds in Paediatric Acute Myeloid Leukaemia


Abstract
:1. Introduction
2. Results
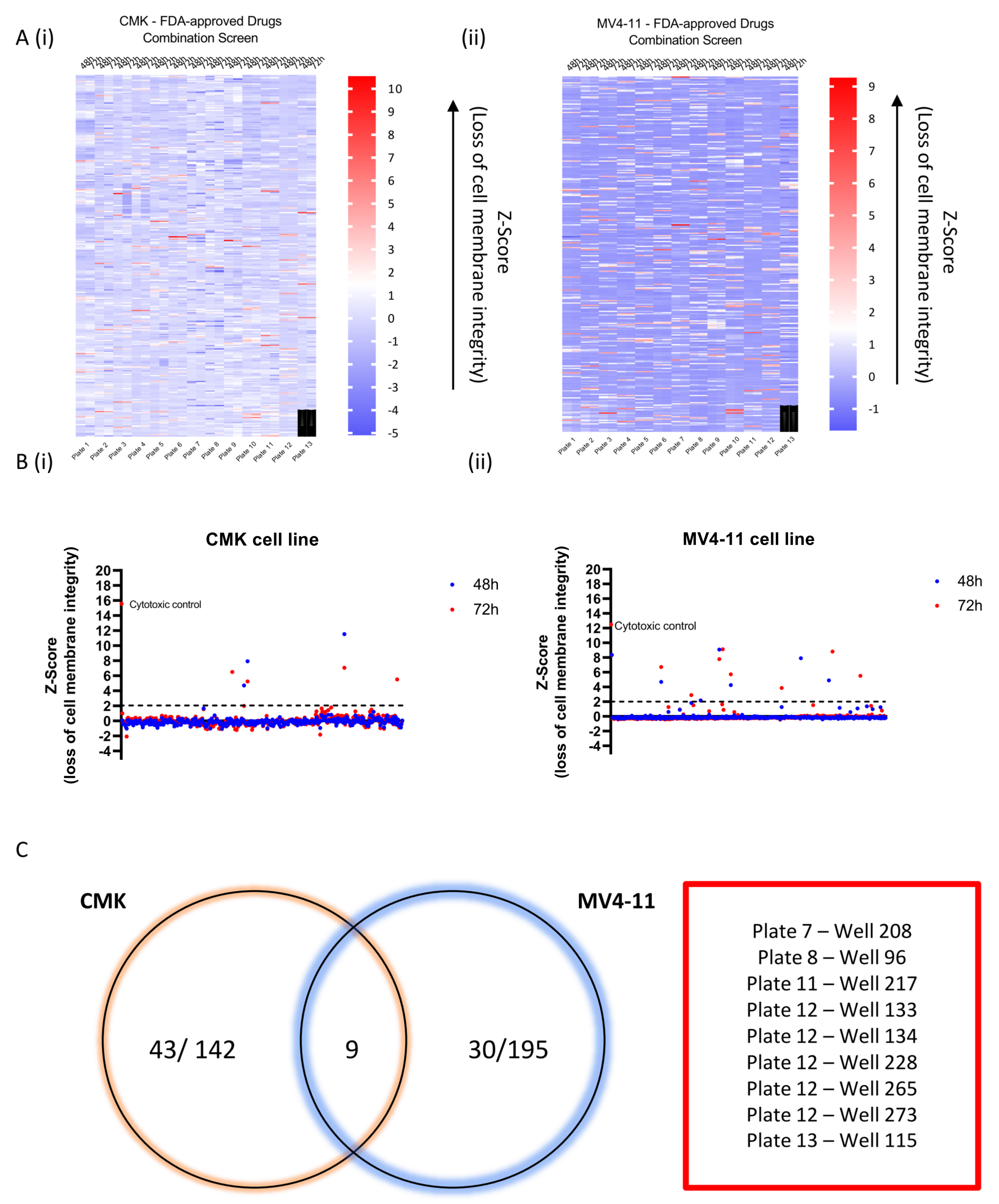
2.1. Multiplex Screening Using an All-Pairs Testing Algorithm to Identify Combination Therapies In Vitro
2.2. Deconvolution of ‘Hit’ Wells to Investigate Double and Triple Combinations as Potential Therapies for the Treatment of Paediatric AML
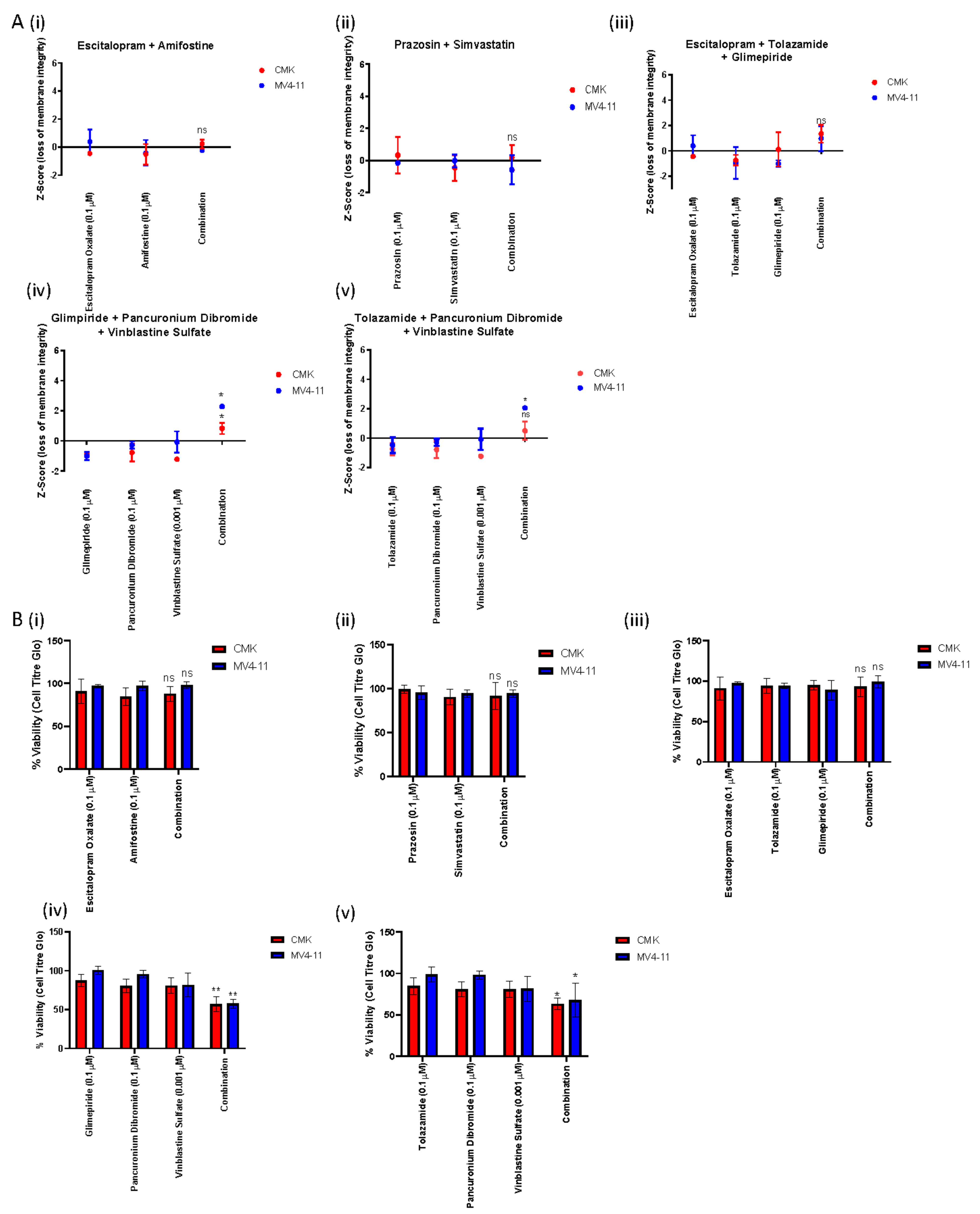
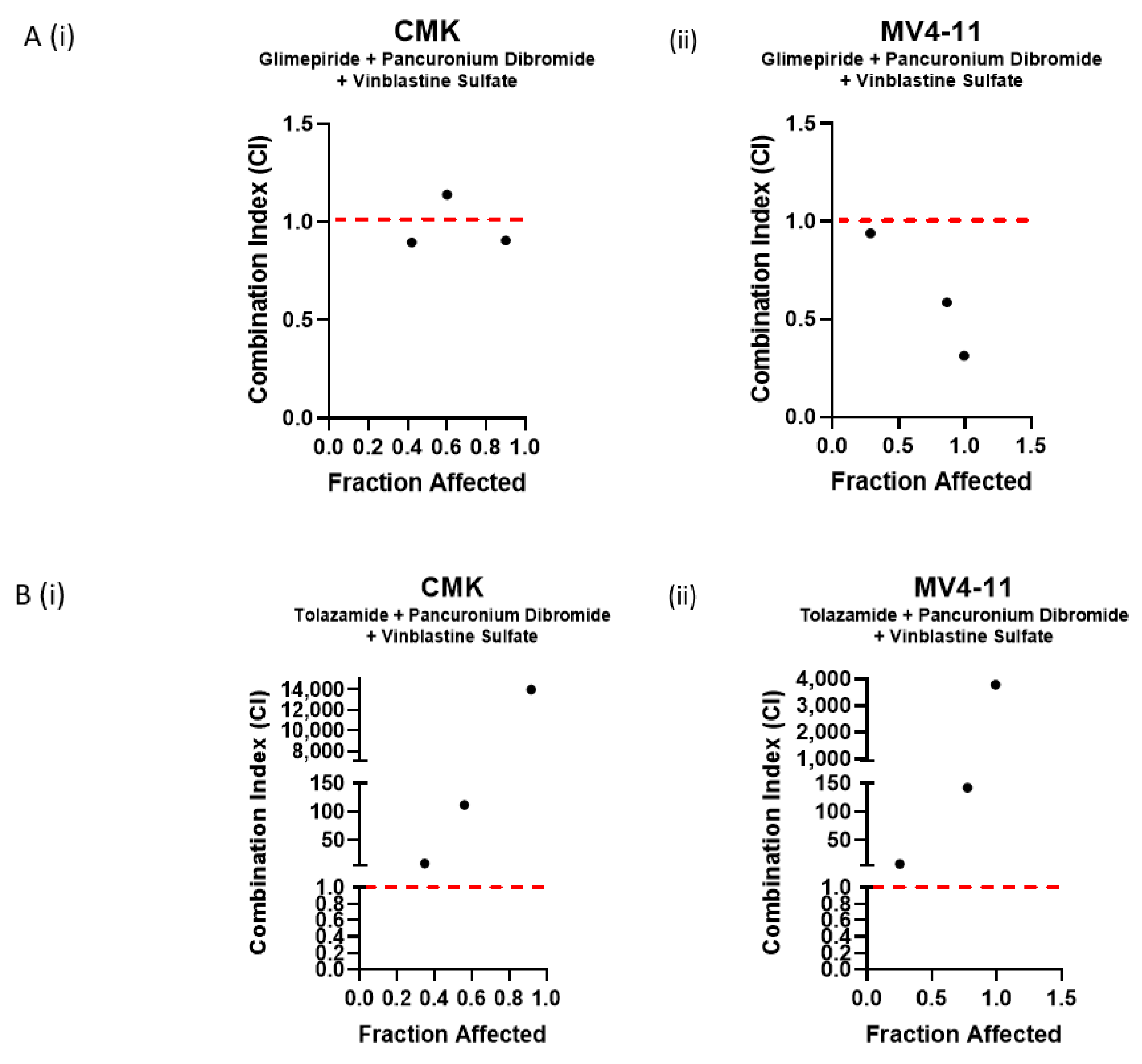
2.3. Validation of Double and Triple Combinations Identified in the Deconvolution of Plate 13 Well 115
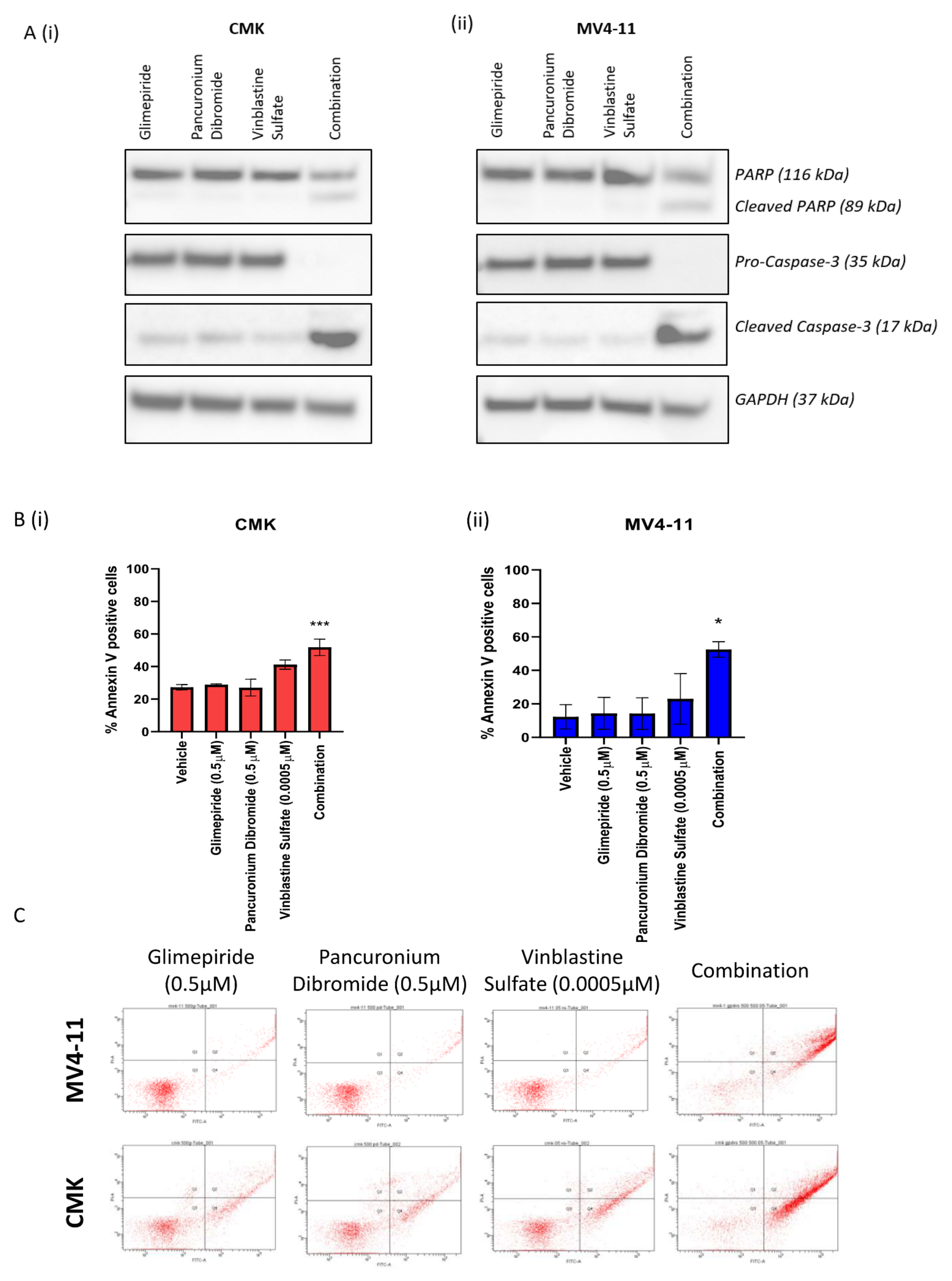
2.4. The Combination of Glimepiride, Pancuronium Dibromide and Vinblastine Sulfate Induces Apoptotic Cell Death in Paediatric AML
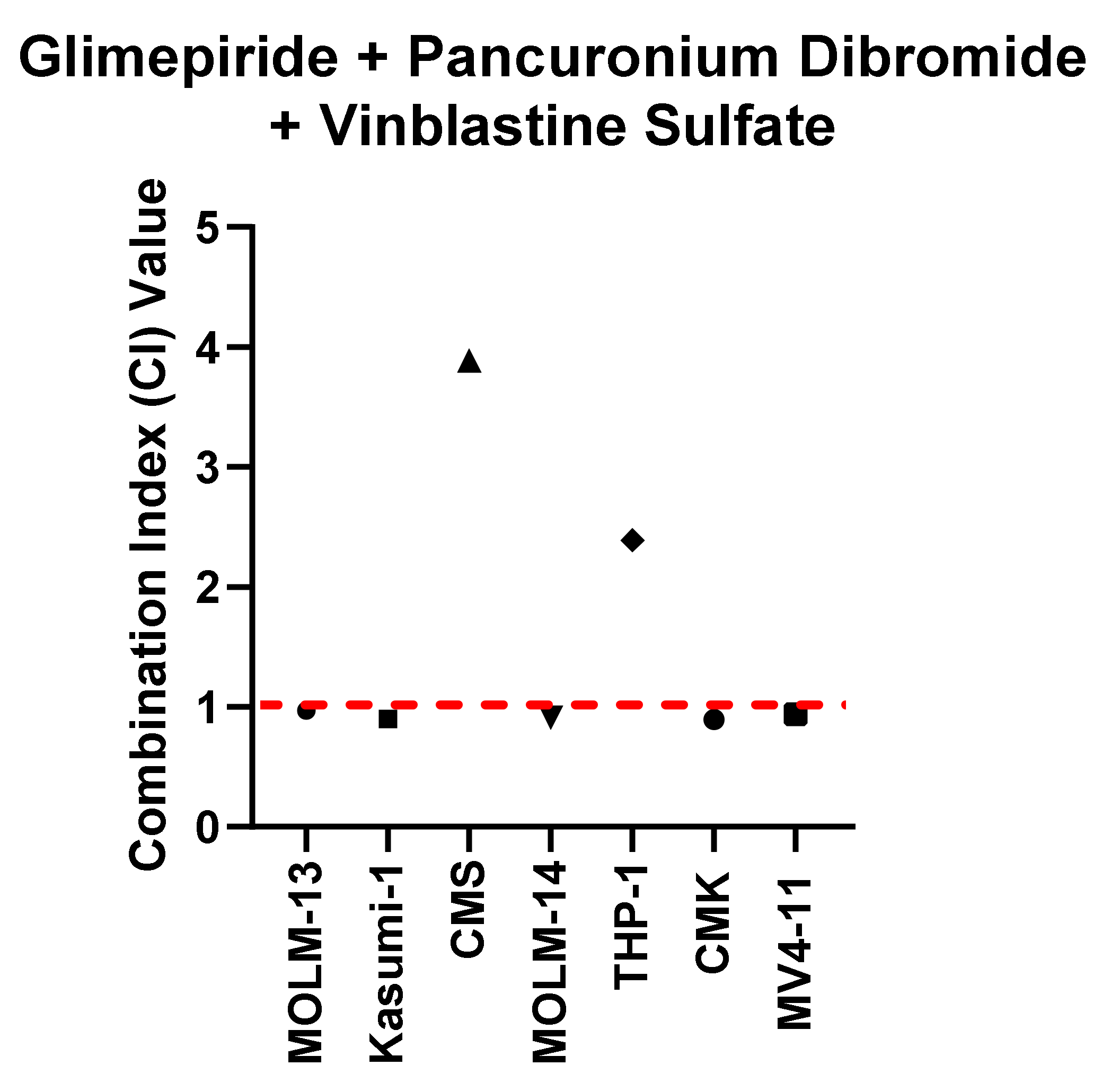
2.5. The Combination of Glimepiride, Pancuronium Dibromide and Vinblastine Sulfate Demonstrates Reduced Cell Viability across Multiple Paediatric Cell Lines
3. Discussion
4. Materials and Methods
4.1. Cell Lines
4.2. Combination Screen Algorithm
4.3. Compound Screening
4.4. Z-Score Calculation
4.5. Deconvolution
4.6. Cell Viability Assay
4.7. Combination Index Values
4.8. Western Blot Analysis
4.9. Annexin V Flow Cytometry
4.10. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kellaway, S.; Chin, P.S.; Barneh, F.; Bonifer, C.; Heidenreich, O. t(8;21) Acute Myeloid Leukemia as a Paradigm for the Understanding of Leukemogenesis at the Level of Gene Regulation and Chromatin Programming. Cells 2020, 9, 2681. [Google Scholar] [CrossRef]
- Carter, J.L.; Hege, K.; Yang, J.; Kalpage, H.A.; Su, Y.; Edwards, H.; Hüttemann, M.; Taub, J.W.; Ge, Y. Targeting multiple signaling pathways: The new approach to acute myeloid leukemia therapy. Signal Transduct. Target. Ther. 2020, 5, 1–29. [Google Scholar] [CrossRef]
- Heuser, M.; Ofran, Y.; Boissel, N.; Brunet Mauri, S.; Craddock, C.; Janssen, J.; Wierzbowska, A.; Buske, C. Acute myeloid leukaemia in adult patients: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 697–712. [Google Scholar] [CrossRef] [PubMed]
- Cooper, S.L.; Brown, P.A. Treatment of Pediatric Acute Lymphoblastic Leukemia Stacy. Paediatr. Clin. N. Am. 2015, 62, 61–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hao, T.K.; Ha, C.V.; Son, N.H.; Hiep, P.N. Long-term outcome of childhood acute myeloid leukemia: A 10-year retrospective cohort study. Pediatr. Rep. 2020, 12, 22–25. [Google Scholar]
- Creutzig, U.; Heuvel-Eibrink, M.M.V.D.; Gibson, B.; Dworzak, M.N.; Adachi, S.; Bont, E.D.; Harbott, J.; Hasle, H.; Johnston, D.; Kinoshita, A.; et al. Diagnosis and management of acute myeloid leukemia in children and adolescents: Recommendations from an international expert panel. Blood 2012, 120, 3167–3205. [Google Scholar] [CrossRef]
- Davila, J.; Slotkin, E.; Renaud, T. Relapsed and refractory pediatric acute myeloid leukemia: Current and emerging treatments. Pediatr. Drugs 2014, 16, 151–168. [Google Scholar] [CrossRef]
- Lappin, K.M.; Davis, L.; Matchett, K.B.; Ge, Y.; Mills, K.I.; Blayney, J.K. A compound combination screening approach with potential to identify new treatment options for paediatric acute myeloid leukaemia. Sci. Rep. 2020, 10, 1–13. [Google Scholar] [CrossRef]
- Chaudhury, S.; O’Connor, C.; Cañete, A.; Bittencourt-Silvestre, J.; Sarrou, E.; Prendergast, Á.; Choi, J.; Johnston, P.; Wells, C.A.; Gibson, B.; et al. Age-specific biological and molecular profiling distinguishes paediatric from adult acute myeloid leukaemias. Nat. Commun. 2018, 9, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Bolouri, H.; Farrar, J.E.; Triche, T.J.; Ries, R.E.; Lim, E.L.; Alonzo, T.A.; Ma, Y.; Moore, R.; Mungall, A.J.; Marra, M.A.; et al. The molecular landscape of pediatric acute myeloid leukemia reveals recurrent structural alterations and age-specific mutational interactions. Nat. Med. 2018, 24, 103–112. [Google Scholar] [CrossRef] [Green Version]
- Brown, F.C.; Cifani, P.; Drill, E.; He, J.; Still, E.; Zhong, S.; Balasubramanian, S.; Pavlick, D.; Yilmazel, B.; Knapp, K.M.; et al. Genomics of primary chemoresistance and remission induction failure in paediatric and adult acute myeloid leukaemia. Br. J. Haematol. 2017, 176, 86–91. [Google Scholar] [CrossRef]
- Banck, J.C.; Görlich, D. In-silico comparison of two induction regimens (7 + 3 vs 7 + 3 plus additional bone marrow evaluation) in acute myeloid leukemia treatment. BMC Syst. Biol. 2019, 13, 18. [Google Scholar] [CrossRef] [PubMed]
- Lichtman, M.A. A historical perspective on the development of the cytarabine (7days) and daunorubicin (3days) treatment regimen for acute myelogenous leukemia: 2013 the 40th anniversary of 7+3. Blood Cells Mol. Dis. 2013, 50, 119–130. [Google Scholar] [CrossRef]
- Leahey, A.M.; Teunissen, H.; Friedman, D.L.; Moshang, T.; Lange, B.J.; Meadows, A.T. Late effects of chemotherapy compared to bone marrow transplantation in the treatment of pediatric acute myeloid leukemia and myelodysplasia. Med. Pediatr. Oncol. 1999, 32, 163–169. [Google Scholar] [CrossRef]
- Specialist, I. Long-Term and Late Effects of Treatment for Childhood Leukemia or Lymphoma Facts. Leuk. Lymphoma Soc. 2013, 15, 1–8. [Google Scholar]
- Frei, E.; Karon, M.; Levin, R.H.; Freireich, E.J.; Taylor, R.J.; Hananian, J.; Selawry, O.; Holland, J.F.; Hoogstraten, B.; Wolman, I.J.; et al. The Effectivness of Combinations of Antileukemic Agents in Inducing and Maintaing Remission in Children with Acute Leukemia. Blood 1965, 26, 645–656. [Google Scholar] [CrossRef] [Green Version]
- Mokhtari, R.B.; Homayouni, T.S.; Baluch, N.; Morgatskaya, E.; Kumar, S.; Das, B.; Yeger, H. Combination therapy in combating cancer Systematic Review: Combination Therapy in Combating Cancer Background. Oncotarget 2017, 8, 38022–38043. [Google Scholar] [CrossRef] [Green Version]
- Gumusay, O.; Vitiello, P.P.; Wabl, C.; Corcoran, R.B.; Bardelli, A.; Rugo, H.S. Strategic Combinations to Prevent and Overcome Resistance to Targeted Therapies in Oncology. Am. Soc. Clin. Oncol. Educ. B. 2020, 40, e292–e308. [Google Scholar] [CrossRef]
- Wojcicki, A.V.; Kadapakkam, M.; Frymoyer, A.; Lacayo, N.; Chae, H.D.; Sakamoto, K.M. Repurposing drugs for acute myeloid leukemia: A worthy cause or a futile pursuit? Cancers 2020, 12, 441. [Google Scholar] [CrossRef] [Green Version]
- McCabe, B.; Liberante, F.; Mills, K.I. Repurposing medicinal compounds for blood cancer treatment. Ann. Hematol. 2015, 94, 1267–1276. [Google Scholar] [CrossRef] [Green Version]
- Jin, Y.; Lu, Z.; Ding, K.; Li, J.; Du, X.; Chen, C.; Sun, X.; Wu, Y.; Zhou, J.; Pan, J. Antineoplastic mechanisms of niclosamide in acute myelogenous leukemia stem cells: Inactivation of the NF-κB pathway and generation of reactive oxygen species. Cancer Res. 2010, 70, 2516–2527. [Google Scholar] [CrossRef] [Green Version]
- Škrtić, M.; Sriskanthadevan, S.; Jhas, B.; Gebbia, M.; Wang, Z.; Hurren, R.; Jitkova, Y.; Gronda, M.; Maclean, N.; Lai, C.K.; et al. Inhibition of Mitochondrial Translation as a Therapeutic Strategy for Human Acute Myeloid Leukemia. Cancer Cell 2011, 20, 674–688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, D.; Zhang, Y.T.; Xu, G.P.; Yan, W.W.; Pan, X.R.; Tong, J.H. Sertraline exerts its antitumor functions through both apoptosis and autophagy pathways in acute myeloid leukemia cells. Leuk. Lymphoma 2017, 58, 2208–2217. [Google Scholar] [CrossRef]
- Singhal, S.; Mehta, J.; Desikan, R.; Ayers, D.; Roberson, P.; Eddlemon, P.; Munshi, N.; Anaissie, E.; Wilson, C.; Dhodapkar, M.; et al. Antitumor Activity of Thalidomide in Refractory Multiple Myeloma. N. Engl. J. Med. 1999, 341, 1565–1571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, R.K. Glimepiride: Role of a new sulfonylurea in the treatment of type 2 diabetes mellitus. Ann. Pharmacother. 1998, 32, 1044–1052. [Google Scholar] [CrossRef] [PubMed]
- Docherty, J.R.; Mcgrath, J.C. a Comparison of the Effects of Pancuronium Bromide and Its Monoquaternary Analogue, Org Nc 45, on Autonomic and Somatic Neurotransmission in the Rat. Br. J. Pharmacol. 1980, 71, 225–233. [Google Scholar] [CrossRef] [Green Version]
- Rtibi, K.; Grami, D.; Selmi, S.; Amri, M.; Sebai, H.; Marzouki, L. Vinblastine, an anticancer drug, causes constipation and oxidative stress as well as others disruptions in intestinal tract in rat. Toxicol. Rep. 2017, 4, 221–225. [Google Scholar] [CrossRef]
- Allison, A.C.; Eugui, E.M. Mycophenolate mofetil and its mechanisms of action. Immunopharmacology 2000, 47, 85–118. [Google Scholar] [CrossRef]
- Chen, V.C.H.; Hsieh, Y.H.; Chen, L.J.; Hsu, T.C.; Tzang, B.S. Escitalopram oxalate induces apoptosis in U-87MG cells and autophagy in GBM8401 cells. J. Cell. Mol. Med. 2018, 22, 1167–1178. [Google Scholar] [CrossRef]
- Wang, H.T.; Yang, B.; Hu, B.; Chi, X.H.; Luo, L.L.; Yang, H.Q.; Lang, X.L.; Geng, J.; Qiao, C.X.; Li, Y.; et al. The effect of amifostine on differentiation of the human megakaryoblastic Dami cell line. Cancer Med. 2016, 5, 2012–2021. [Google Scholar] [CrossRef] [PubMed]
- Assad Kahn, S.; Costa, S.L.; Gholamin, S.; Nitta, R.T.; Dubois, L.G.; Fève, M.; Zeniou, M.; Coelho, P.L.C.; El-Habr, E.; Cadusseau, J.; et al. The anti-hypertensive drug prazosin inhibits glioblastoma growth via the PKC δ-dependent inhibition of the AKT pathway. EMBO Mol. Med. 2016, 8, 511–526. [Google Scholar] [CrossRef] [PubMed]
- Yaluri, N.; Modi, S.; Rodríguez, M.L.; Stancáková, A.; Kuusisto, J.; Kokkola, T.; Laakso, M. Simvastatin impairs insulin secretion by multiple mechanisms in MIN6 cells. PLoS ONE 2015, 10, e0142902. [Google Scholar] [CrossRef] [PubMed]
- Tao, P.; Li, Z.; Woofork, A.G.; Hage, D.S. Characterization of Tolazamide Binding with Glycated and Normal Human Serum Albumin by Using High-Performance Affinity Chromatography. J. Pharm. Biomed. Anal. 2019, 166, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Ingham, V.; Williams, A.; Bate, C. Glimepiride reduces CD14 expression and cytokine secretion from macrophages. J. Neuroinflammation 2014, 11, 115. [Google Scholar] [CrossRef] [Green Version]
- Chou, T.-C.; Talalay, P. Analysis of combined drug effects: A new look at a very old problem. Trends Pharmacol. Sci. 1983, 4, 450–454. [Google Scholar] [CrossRef]
- Hu, Y.; Chen, A.; Zheng, X.; Lu, J.; He, H.; Yang, J.; Zhang, Y.; Sui, P.; Yang, J.; He, F.; et al. Ecological principle meets cancer treatment: Treating children with acute myeloid leukemia with low-dose chemotherapy. Natl. Sci. Rev. 2019, 6, 469–479. [Google Scholar] [CrossRef]
- Rooij, J.D.; Zwaan, C.; Heuvel-Eibrink, M.V.D. Pediatric AML: From Biology to Clinical Management. J. Clin. Med. 2015, 4, 127–149. [Google Scholar] [CrossRef] [PubMed]
- Lonetti, A.; Pession, A.; Masetti, R. Targeted Therapies for Pediatric AML: Gaps and Perspective. Front. Pediatr. 2019, 7, 1–11. [Google Scholar] [CrossRef]
- Balgobind, B.V.; Zwaan, C.M.; Pieters, R.; Heuvel-Eibrink, M.M.V.D. The heterogeneity of pediatric MLL -rearranged acute myeloid leukemia. Leukemia 2011, 25, 1239–1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Smith, K.S.; Murphy, M.; Piloto, O.; Somervaille, T.C.P.; Cleary, M.L. Glycogen synthase kinase 3 in MLL leukaemia maintenance and targeted therapy. Nature 2008, 455, 1205–1210. [Google Scholar] [CrossRef] [Green Version]
- Estey, E.; Karp, J.E.; Emadi, A.; Othus, M.; Gale, R.P. Recent drug approvals for newly diagnosed acute myeloid leukemia: Gifts or a Trojan horse? Leukemia 2020, 34, 671–681. [Google Scholar] [CrossRef] [PubMed]
- Valli, D.; Gruszka, A.M.; Alcalay, M. Has Drug Repurposing Fulfilled Its Promise in Acute Myeloid Leukaemia? J. Clin. Med. 2020, 9, 1892. [Google Scholar] [CrossRef] [PubMed]
- Roulston, G.D.R.; Burt, C.L.; Kettyle, L.M.J.; Matchett, K.B.; Keenan, H.L.; Mulgrew, N.M.; Ramsey, J.M.; Dougan, C.; Grishagin, I.V.; Mills, K.I.; et al. Low-dose salinomycin induces anti-leukemic responses in AML and MLL. Oncotarget 2016, 7, 73448. [Google Scholar] [CrossRef] [Green Version]
- Zhou, A.; Han, Q.; Song, H.; Zi, J.; Ma, J.; Ge, Z. Efficacy and toxicity of cladribine for the treatment of refractory acute myeloid leukemia: A meta-analysis. Drug Des. Dev. Ther. 2019, 13, 1867–1878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drenberg, C.D.; Shelat, A.; Dang, J.; Cotton, A.; Orwick, S.J.; Li, M.; Jeon, J.Y.; Fu, Q.; Buelow, D.R.; Pioso, M.; et al. A high-throughput screen indicates gemcitabine and JAK inhibitors may be useful for treating pediatric AML. Nat. Commun. 2019, 10, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Depreter, B.; Moerloose, B.D.; Vandepoele, K.; Uyttebroeck, A.; Damme, A.V.; Terras, E.; Denys, B.; Dedeken, L.; Dresse, M.-F.; Van der Werff Ten Bosch, J.; et al. Deciphering molecular heterogeneity in pediatric AML using a cancer vs. normal transcriptomic approach. Pediatr. Res. 2020, 89, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Illangeswaran, R.S.S.; Das, S.; Paul, D.Z.; Mathews, V.; Balasubramanian, P. A personalized approach to acute myeloid leukemia therapy: Current options. Pharmacogenomics Pers. Med. 2019, 12, 167–179. [Google Scholar] [CrossRef] [Green Version]
- Pasello, G.; Urso, L.; Conte, P.; Favaretto, A. Effects of Sulfonylureas on Tumor Growth: A Review of the Literature. Oncologist 2013, 18, 1118–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, C.H.; Lin, J.W.; Wu, L.C.; Lai, M.S.; Chuang, L.M. Oral insulin secretagogues, insulin, and cancer risk in type 2 diabetes mellitus. J. Clin. Endocrinol. Metab. 2012, 97, 1170–1175. [Google Scholar] [CrossRef]
- Barbieri, M.; Grella, R.; Passariello, N.; Barone, M.; Paolisso, G. Le repaglinide est plus efficace que le glimépiride sur la sécrétion d’insuline et sur les excursions glycémiques post-prandiales chez les diabétiques de type 2. Une étude à court terme. Diabetes Metab. 2003, 30, 81–89. [Google Scholar]
- Hendriks, A.M.; Schrijnders, D.; Kleefstra, N.; Vries, E.G.E.D.; Bilo, H.J.G.; Jalving, M.; Landman, G.W.D. Sulfonylurea derivatives and cancer, friend or foe? Eur. J. Pharmacol. 2019, 861, 172598. [Google Scholar] [CrossRef] [PubMed]
- Xue, Q.S.; Yu, B.W. The role of neuronal nicotinic acetylcholine receptors in the mechanisms of general anesthesia. Sheng Li Ke Xue Jin Zhan 2003, 34, 37–41. [Google Scholar] [PubMed]
- Di Cesare, E.; Verrico, A.; Miele, A.; Giubettini, M.; Rovella, P.; Coluccia, A.; Famiglini, V.; La Regina, G.; Cundari, E.; Silvestri, R.; et al. Mitotic cell death induction by targeting the mitotic spindle with tubulin-inhibitory indole derivative molecules. Oncotarget 2017, 8, 19738–19759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cutts, J.H.; Beer, C.T.; Noble, R.L. Biological Properties of Vincaleukoblastine, an Alkaloid in Vinca rosea Linn, with Reference to Its Antitumor Action. Cancer Res. 1960, 20, 1023–1031. [Google Scholar]
- Lucas, D.M.; Still, P.; Bueno Perez, L.; Grever, M.R.; Kinghorn, A.D. Potential of Plant-Derived Natural Products in the Treatment of Leukemia and Lymphoma. Curr. Drug Targets 2010, 11, 812–822. [Google Scholar] [CrossRef]
- Johnson, I.S.; Armstrong, J.G.; Gorman, M.; Burnett, J.P. The Vinca Alkaloids: A New Class of Oncolytic Agents. Cancer Res. 1963, 23, 1390–1427. [Google Scholar]
- Stadheim, T.A.; Xiao, H.; Eastman, A. Inhibition of extracellular signal-regulated kinase (ERK) mediates cell cycle phase independent apoptosis in vinblastine-treated ML-1 cells. Cancer Res. 2001, 61, 1533–1540. [Google Scholar] [PubMed]
- Bates, D.J.P.; Salerni, B.L.; Lowrey, C.H.; Eastman, A. Vinblastine sensitizes leukemia cells to cyclin-dependent kinase inhibitors, inducing acute cell cycle phase-independent apoptosis. Cancer Biol. Ther. 2011, 12, 314–325. [Google Scholar] [CrossRef] [PubMed]
- Lange, B.; Valtieri, M.; Santoli, D.; Caracciolo, D.; Mavilio, F.; Gemperlein, I.; Griffin, C.; Emanuel, B.; Finan, J.; Nowell, P.; et al. Growth Factor Requirements of Childhood Acute Leukemia: Establishment of GM-CSF-Dependent Cell Lines. Blood 1987, 70, 192–199. [Google Scholar] [CrossRef] [Green Version]
- Niu, X.; Wang, G.; Wang, Y.; Caldwell, J.T.; Edwards, H.; Xie, C.; Taub, J.W.; Li, C.; Lin, H.; Ge, Y. Acute Myeloid Leukemia Cells Harboring MLL Fusion Genes or with the Acute Promyelocytic Leukemia Phenotype Are Sensitive to the Bcl-2-selective Inhibitor ABT-199. Leukemia 2015, 28, 1557–1560. [Google Scholar] [CrossRef] [PubMed]
- Ayyagari, V.N.; Brard, L. Bithionol inhibits ovarian cancer cell growth In Vitro–studies on mechanism (s) of action. BMC cancer 2014, 14, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CMK | MV4-11 | ||
|---|---|---|---|
| Pairwise Combinations | Triple Combinations | Pairwise Combinations | Triple Combinations |
| Escitalopram oxalate + Amifostine | Combo 107 − Escitalopram oxalate + Tolazamide + Glimepiride | Prazosin + Simvastatin | Combo 14 − Glimepiride + Pancuronium Dibromide + Vinblastine Sulfate |
| Combo 99 − Tolazamide + Pancuronium Dibromide + Vinblastine Sulfate | |||
| Glimepiride (µM) | Pancuronium Dibromide (µM) | Vinblastine Sulfate (µM) |
CI Value CMK |
CI Value MV4-11 |
|---|---|---|---|---|
| 0.5 | 0.5 | 0.0005 | 0.89551 | 0.93907 |
| 1 | 1 | 0.001 | 1.14521 | 0.58593 |
| 1 | 1 | 0.002 | 0.90606 | 0.31275 |
| Tolazamide (µM) | Pancuronium Dibromide (µM) | Vinblastine Sulfate (µM) |
CI Value CMK |
CI Value MV4-11 |
|---|---|---|---|---|
| 0.5 | 0.5 | 0.0005 | 9.22723 | 8.51182 |
| 1 | 1 | 0.001 | 119.937 | 142.212 |
| 1 | 1 | 0.002 | 140,007.0 | 3796.52 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cairns, L.V.; Lappin, K.M.; Mutch, A.; Ali, A.; Matchett, K.B.; Mills, K.I. Multiplex Screening for Interacting Compounds in Paediatric Acute Myeloid Leukaemia. Int. J. Mol. Sci. 2021, 22, 10163. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms221810163
Cairns LV, Lappin KM, Mutch A, Ali A, Matchett KB, Mills KI. Multiplex Screening for Interacting Compounds in Paediatric Acute Myeloid Leukaemia. International Journal of Molecular Sciences. 2021; 22(18):10163. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms221810163
Chicago/Turabian StyleCairns, Lauren V., Katrina M. Lappin, Alexander Mutch, Ahlam Ali, Kyle B. Matchett, and Ken I. Mills. 2021. "Multiplex Screening for Interacting Compounds in Paediatric Acute Myeloid Leukaemia" International Journal of Molecular Sciences 22, no. 18: 10163. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms221810163