
Comparative Analysis of Chromatin-Delivered Biomarkers in the Monitoring of Sepsis and Septic Shock: A Pilot Study


 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Results
2.1. Development of a Home-Made Immunoassay for Detection of Nucleoproteins in Plasma
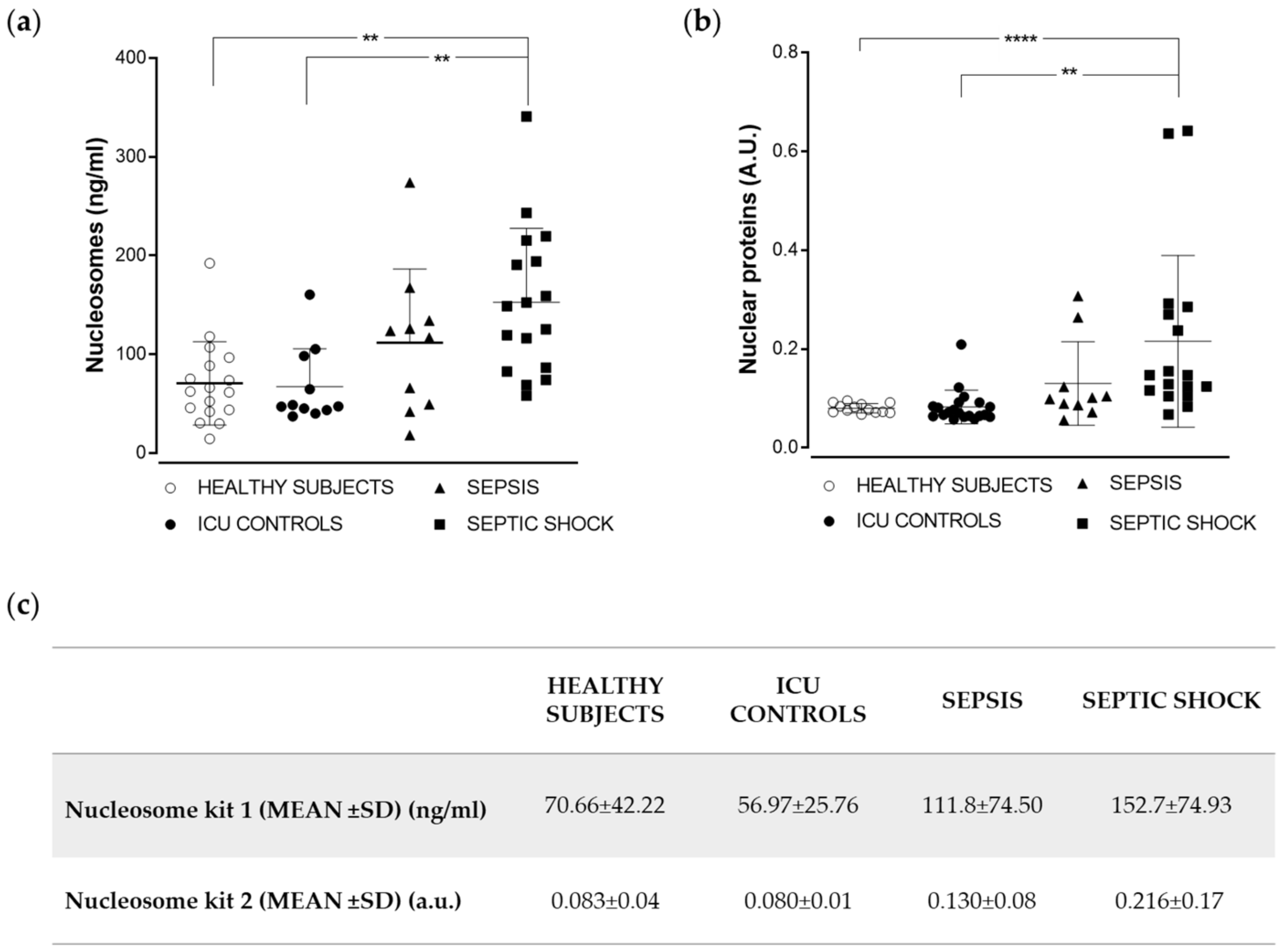
2.2. Analysis of Nucleoprotein Levels in a Cohort of Sepsis and Septic Shock Patients
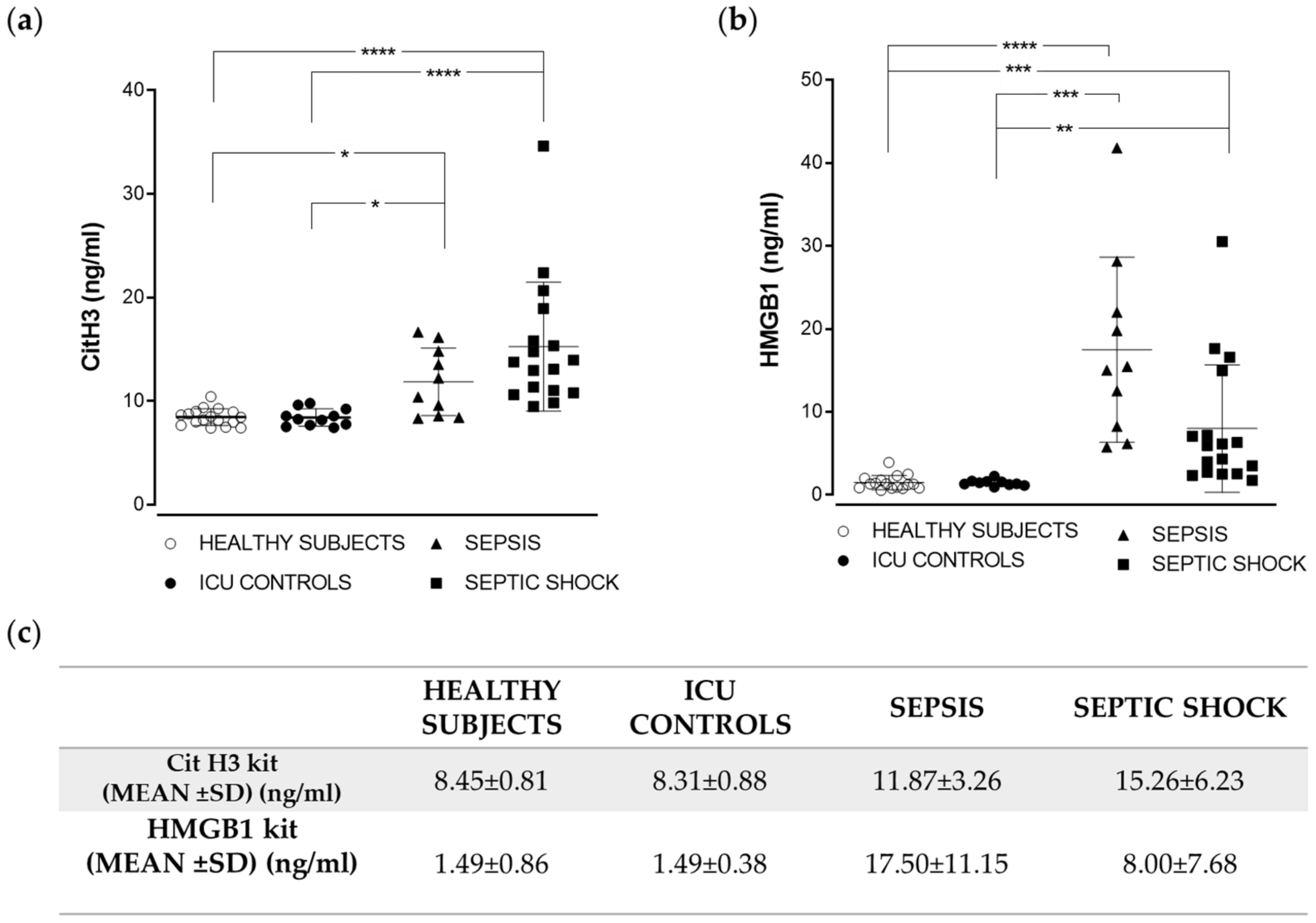
2.3. Citrullinated Histone H3 and HMGB1 Levels in Sepsis and Septic Shock Patients
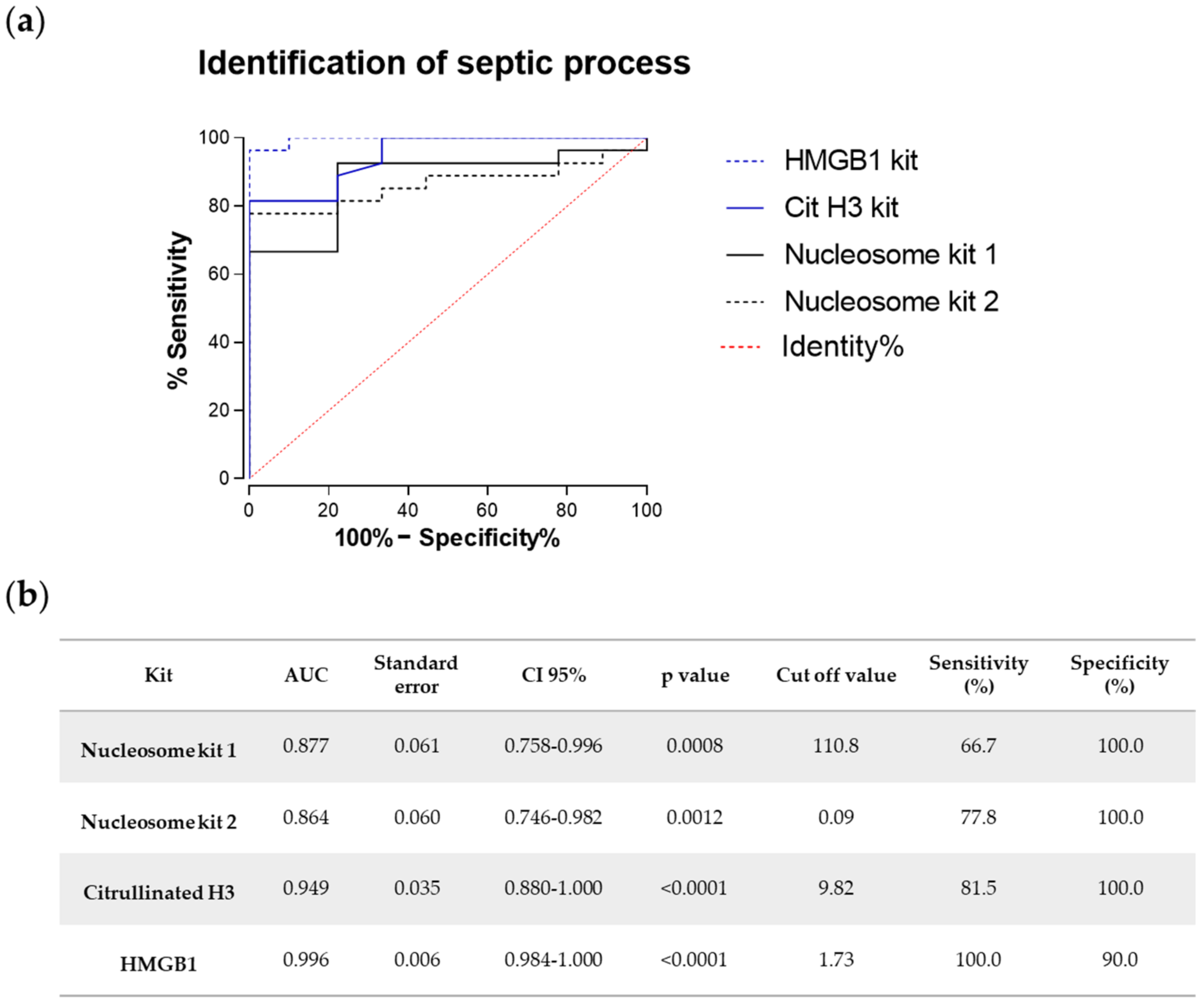
2.4. Comparative Analysis of the Diagnostic Potential of Chromatin-Delivered Biomarkers
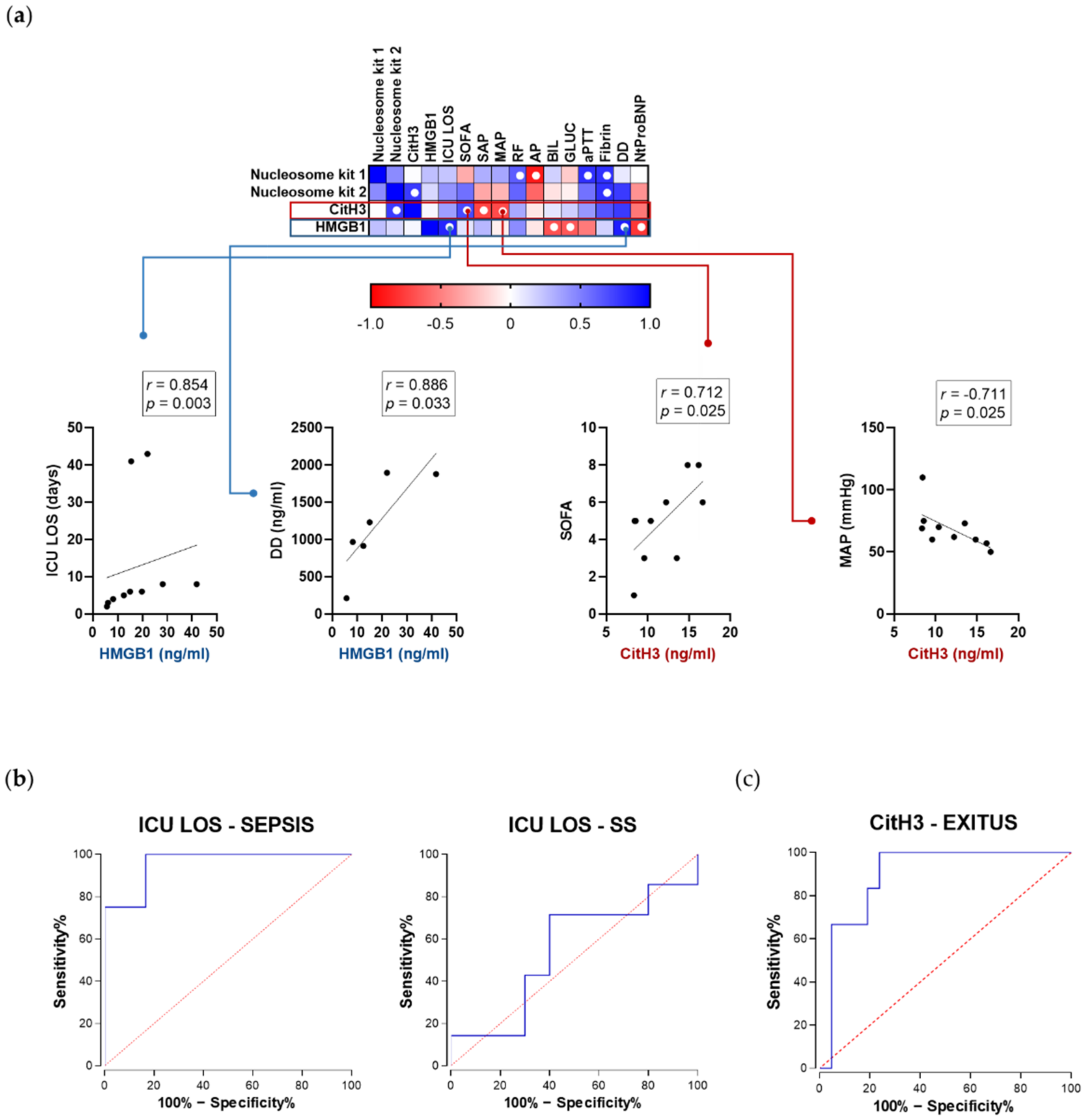
2.5. Correlation with Clinical Parameters in Sepsis Patients Varies between Nucleosomes, Citrullinated Histone H3, and HMGB1
3. Discussion
4. Materials and Methods
4.1. Production of Monoclonal Antinucleoprotein Antibodies
4.2. Home-Made Nucleosome ELISA
4.3. Commercial ELISA Kits
4.4. Selection of the Cohorts and Blood Collection
4.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Purification and Isolation of Monoclonal Antibodies
Appendix A.2. Purification of Histones
Appendix A.3. Analytes Used in the Specificity Tests for Home-Made ELISA and Standard Curve

Appendix A.4. Exclusion Criteria for the Cohorts and Results for Hemoculture
Appendix A.5. References
- Shechter, D., Dormann, H. L., Allis, C. D. & Hake, S. B. Extraction, purification and analysis of histones. Nature protocols 2, 1445–1457, doi:10.1038/nprot.2007.202 (2007).
- Bradford, M. M. A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Analytical Biochemistry 72, 248–254, doi:10.1016/0003-2697(76)90527-3 (1976).
References
- Singer, M.; Deutschman, C.S.; Seymour, C.C.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.C.; et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Joffre, J.; Hellman, J. Oxidative stress and endothelial dysfunction in sepsis and acute inflammation. Antioxid. Redox Signal 2021. [Google Scholar] [CrossRef] [PubMed]
- Beraha, E.M.; Salemink, E.; Goudriaan, A.E.; Bakker, A.; de Jong, D.; Smits, N.; Zwart, J.W.; van Geest, D.; Bodewits, P.; Schiphof, T.; et al. Efficacy and safety of high-dose baclofen for the treatment of alcohol dependence: A multicentre, randomised, double-blind controlled trial. Eur. Neuropsychopharmacol. 2016, 26, 1950–1959. [Google Scholar] [CrossRef]
- Westwood, M.; Ramaekers, B.; Whiting, P.; Tomini, F.; Joore, M.; Armstrong, N.; Ryder, S.; Stirk, L.; Severens, J.; Kleijnen, J. Procalcitonin testing to guide antibiotic therapy for the treatment of sepsis in intensive care settings and for suspected bacterial infection in emergency department settings: A systematic review and cost-effectiveness analysis. Health Technol. Assess. 2015, 19, 1–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Jong, E.; van Oers, J.A.; Beishuizen, A.; Vos, P.; Vermeijden, W.J.; Haas, L.E.; Loef, B.G.; Dormans, T.; van Melsen, G.C.; Kluiters, Y.C.; et al. Efficacy and safety of procalcitonin guidance in reducing the duration of antibiotic treatment in critically ill patients: A randomised, controlled, open-label trial. Lancet Infect. Dis. 2016, 16, 819–827. [Google Scholar] [CrossRef]
- Struck, J.; Tao, C.; Morgenthaler, N.G.; Bergmann, A. Identification of an Adrenomedullin precursor fragment in plasma of sepsis patients. Peptides 2004, 25, 1369–1372. [Google Scholar] [CrossRef]
- Suberviola, B.; Castellanos-Ortega, A.; Llorca, J.; Ortiz, F.; Iglesias-Posadilla, D.; Prieto, B. Prognostic value of proadrenomedullin in severe sepsis and septic shock patients with community-acquired pneumonia. Swiss Med. Wkly. 2012, 142, w13542. [Google Scholar] [CrossRef]
- Schuetz, P.; Christ-Crain, M.; Müller, B. Biomarkers to improve diagnostic and prognostic accuracy in systemic infections. Curr. Opin. Crit. Care 2007, 13, 578–585. [Google Scholar] [CrossRef]
- Silvestre, J.; Coelho, L.; Póvoa, P. Should C-reactive protein concentration at ICU discharge be used as a prognostic marker? BMC Anesthesiol. 2010, 10, 17. [Google Scholar] [CrossRef] [Green Version]
- Pierrakos, C.; Vincent, J.-L. Sepsis biomarkers: A review. Crit. Care 2010, 14, R15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silk, E.; Zhao, H.; Weng, H.; Ma, D. The role of extracellular histone in organ injury. Cell Death Dis. 2017, 8, e2812. [Google Scholar] [CrossRef] [Green Version]
- Mena, H.A.; Carestia, A.; Scotti, L.; Parborell, F.; Schattner, M.; Negrotto, S. Extracellular histones reduce survival and angiogenic responses of late outgrowth progenitor and mature endothelial cells. J. Thromb. Haemost. 2016, 14, 397–410. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Cremades, D.; Bueno-Beti, C.; García-Giménez, J.L.; Ibañez-Cabellos, J.S.; Hermenegildo, C.; Pallardó, F.V.; Novella, S. Extracellular histones disarrange vasoactive mediators release through a COX-NOS interaction in human endothelial cells. J. Cell. Mol. Med. 2017, 21, 1584–1592. [Google Scholar] [CrossRef] [Green Version]
- Raffray, L.; Douchet, I.; Augusto, J.-F.; Youssef, J.; Contin-Bordes, C.; Richez, C.; Duffau, P.; Truchetet, M.-E.; Moreau, J.-F.; Cazanave, C.; et al. Septic shock sera containing circulating histones induce dendritic cell–regulated necrosis in fatal septic shock patients. Crit. Care Med. 2015, 43, e107–e116. [Google Scholar] [CrossRef]
- Xu, J.; Zhang, X.; Pelayo, R.; Monestier, M.; Ammollo, C.T.; Semeraro, F.; Taylor, F.B.; Esmon, N.L.; Lupu, F.; Esmon, C.T. Extracellular histones are major mediators of death in sepsis. Nat. Med. 2009, 15, 1318–1321. [Google Scholar] [CrossRef] [Green Version]
- Cabellos, J.S.I.; Aguado, C.; Pérez-Cremades, D.; García-Giménez, J.L.; Bueno-Beti, C.; García-López, E.M.; Romá-Mateo, C.; Novella, S.; Hermenegildo, C.; Pallardó, F.V. Extracellular histones activate autophagy and apoptosis via mTOR signaling in human endothelial cells. Biochim. Biophys. Acta Mol. Basis Dis. 2018, 1864, 3234–3246. [Google Scholar] [CrossRef] [PubMed]
- García Giménez, J.L.; Romá Mateo, C.; Seco Cervera, M.; Ibañez Cabellos, J.S.; Pallardó, F.V. Chapter 25—Circulating histones and nucleosomes as biomarkers in sepsis and septic shock A2—García-Giménez, José Luis. In Epigenetic Biomarkers and Diagnostics; Academic Press: Boston, MA, USA, 2016; pp. 497–517. [Google Scholar] [CrossRef]
- Wildhagen, K.C.; Wiewel, M.A.; Schultz, M.J.; Horn, J.; Schrijver, R.; Reutelingsperger, C.P.; van der Poll, T.; Nicolaes, G.A. Extracellular histone H3 levels are inversely correlated with antithrombin levels and platelet counts and are associated with mortality in sepsis patients. Thromb. Res. 2015, 136, 542–547. [Google Scholar] [CrossRef]
- Yang, H.; Wang, H.; Chavan, S.S.; Andersson, U. High Mobility Group Box Protein 1 (HMGB1): The Prototypical Endogenous Danger Molecule. Mol. Med. 2015, 21, S6–S12. [Google Scholar] [CrossRef]
- Deng, M.; Tang, Y.; Li, W.; Wang, X.; Zhang, R.; Zhang, X.; Zhao, X.; Liu, J.; Tang, C.; Liu, Z.; et al. The Endotoxin delivery protein HMGB1 mediates caspase-11-dependent lethality in sepsis. Immunity 2018, 49, 740–753.e7. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Q.; Tu, T.; Tai, S.; Tang, L.; Yang, H.; Zhu, Z. Endothelial specific deletion of HMGB1 increases blood pressure and retards ischemia recovery through eNOS and ROS pathway in mice. Redox Biol. 2021, 41, 101890. [Google Scholar] [CrossRef] [PubMed]
- García-Giménez, J.L.; Romá-Mateo, C.; Carbonell, N.; Palacios, L.; Peiró-Chova, L.; García-López, E.; García-Simón, M.; Lahuerta, R.; Gimenez-Garzó, C.; Berenguer-Pascual, E.; et al. A new mass spectrometry-based method for the quantification of histones in plasma from septic shock patients. Sci. Rep. 2017, 7, 1–10. [Google Scholar] [CrossRef]
- Zeerleder, S.; Stephan, F.; Emonts, M.; De Kleijn, E.D.; Esmon, C.T.; Varadi, K.; Hack, C.E.; Hazelzet, J. Circulating nucleosomes and severity of illness in children suffering from meningococcal sepsis treated with protein C. Crit. Care Med. 2012, 40, 3224–3229. [Google Scholar] [CrossRef]
- Li, Y.; Liu, Z.; Liu, B.; Zhao, T.; Chong, W.; Wang, Y.; Alam, H.B. Citrullinated histone H3: A novel target for the treatment of sepsis. Surgery 2014, 156, 229–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alhamdi, Y.; Abrams, S.T.; Cheng, Z.; Jing, S.; Su, D.; Liu, Z.; Lane, S.M.; Welters, I.D.; Wang, G.; Toh, C.-H. Circulating histones are major mediators of cardiac injury in patients with sepsis. Crit. Care Med. 2015, 43, 2094–2103. [Google Scholar] [CrossRef] [PubMed]
- Allam, R.; Kumar, S.V.; Darisipudi, M.N.; Anders, H.-J. Extracellular histones in tissue injury and inflammation. J. Mol. Med. 2014, 92, 465–472. [Google Scholar] [CrossRef]
- Szatmary, P.; Huang, W.; Criddle, D.; Tepikin, A.; Sutton, R. Biology, role and therapeutic potential of circulating histones in acute inflammatory disorders. J. Cell. Mol. Med. 2018, 22, 4617–4629. [Google Scholar] [CrossRef]
- Deng, M.; Scott, M.J.; Fan, J.; Billiar, T.R. Location is the key to function: HMGB1 in sepsis and trauma-induced inflammation. J. Leukoc. Biol. 2019, 106, 161–169. [Google Scholar] [CrossRef]
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelford, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.; Kissoon, N.; Finfer, S.; et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet 2020, 395, 200–211. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.; Ye, L.; Jin, Y.; Zhang, N.; Lou, T.; Qiu, Z.; Jin, Y.; Cheng, B.; Fang, X. Circulating nucleosomes as a predictor of sepsis and organ dysfunction in critically ill patients. Int. J. Infect. Dis. 2012, 16, e558–e564. [Google Scholar] [CrossRef] [Green Version]
- Beltrán-García, J.; Osca-Verdegal, R.; Romá-Mateo, C.; Carbonell, N.; Ferreres, J.; Rodríguez, M.; Mulet, S.; García-López, E.; Pallardó, F.V.; García-Giménez, J.L. Epigenetic biomarkers for human sepsis and septic shock: Insights from immunosuppression. Epigenomics 2020, 12, 617–646. [Google Scholar] [CrossRef]
- Basso, D.; Padoan, A.; Laufer, T.; Aneloni, V.; Moz, S.; Schroers, H.; Pelloso, M.; Saiz, A.; Krapp, M.; Fogar, P.; et al. Relevance of pre-analytical blood management on the emerging cardiovascular protein biomarkers TWEAK and HMGB1 and on miRNA serum and plasma profiling. Clin. Biochem. 2016, 50, 186–193. [Google Scholar] [CrossRef]
- Le, K.; Mo, S.; Lu, X.; Ali, A.I.; Yu, D.; Guo, Y. Association of circulating blood HMGB1 levels with ischemic stroke: A systematic review and meta-analysis. Neurol. Res. 2018, 40, 907–916. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhou, C.; Jiang, J.; Su, Q.; Ding, X. Blockade of HMGB1 preserves vascular homeostasis and improves blood perfusion in rats of acute limb ischemia/reperfusion. Microvasc. Res. 2017, 112, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, S.; Pettilä, V.; Tenhunen, J.; Laru-Sompa, R.; Hynninen, M.; Ruokonen, E. HMGB1 as a predictor of organ dysfunction and outcome in patients with severe sepsis. Intensive Care Med. 2008, 34, 1046–1053. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Nonseptic ICU (n = 9) | Septic ICU (n = 10) | Septic Shock ICU (n = 17) | p Value | |
|---|---|---|---|---|
| Demographics and clinical indexes | ||||
| Age (years) (mean ± SD) | 64.38 ± 8.31 | 65.10 ± 13.10 | 66.18 ± 11.60 | ns |
| Male gender (%) | 6 (66.7) | 7 (70.8) | 10 (58.8) | ns |
| APACHE II score (mean ± SD) | 15.11 ± 4.80 | 15.80 ± 4.90 | 22.12 ± 9.07 | 0.03 |
| SOFA (mean ± SD) | 3.44 ± 3.09 | 5.00 ± 2.21 | 9.65 ± 3.43 | <0.0001 |
| Organ support therapy (1st day) | ||||
| Vasopressor therapy (%) | 1 (11.1) | 2 (20.0) | 16 (94.1) | <0.0001 |
| CRRT (%) | 0 | 0 | 2 (11.76) | ns |
| Mechanical ventilation (%) | 3 (33.3) | 0 | 3 (21.4) | ns |
| Inflammatory parameters | ||||
| White blood cells (mean ± SD) | 10,603 ± 4939 | 12,977 ± 11,589 | 16,395 ± 9612 | ns |
| CRP (mg/L) (mean ± SD) | 25.14 ± 26.31 | 250.20 ± 133.46 | 339.35 ± 189.72 | <0.0001 |
| PCT (ng/mL) (mean ± SD | 0.06 ± 0.07 | 2.21 ± 3.08 | 1.52 ± 2.29 | ns |
| Lactate | ||||
| Lactate 1st hour (mmol/L) (mean ± SD) | 1.61 ± 6.98 | 1.91 ± 1.25 | 1.81 ± 1.99 | ns |
| Coagulopathy parameters | ||||
| Platelets count/L (mean ± SD) | 240.4 × 103 ± 89.3 × 103 | 229.6 × 103 ± 147.36 × 103 | 169.4 × 103 ± 122.8 × 103 | n.s |
| APTT (seconds) (mean ± SD) | 29.67 ± 2.88 | 99.833 ± 118.82 | 117.43 ± 154.83 | 0.014 |
| Outcome | ||||
| ICU LOS (days) (mean ± SD) | 5.9 ± 6.6 | 12.6 ± 15.62 | 9.47 ± 8.61 | ns |
| Hospital LOS (days) (mean ± SD) | 15.4 ± 14.6 | 20.6 ± 13.1 | 19.88 ± 17.8 | ns |
| ICU Mortality (%) | 2 (22.2) | 2 (20.0) | 4 (23.5) | ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beltrán-García, J.; Manclús, J.J.; García-López, E.M.; Carbonell, N.; Ferreres, J.; Rodríguez-Gimillo, M.; Garcés, C.; Pallardó, F.V.; García-Giménez, J.L.; Montoya, Á.; et al. Comparative Analysis of Chromatin-Delivered Biomarkers in the Monitoring of Sepsis and Septic Shock: A Pilot Study. Int. J. Mol. Sci. 2021, 22, 9935. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22189935
Beltrán-García J, Manclús JJ, García-López EM, Carbonell N, Ferreres J, Rodríguez-Gimillo M, Garcés C, Pallardó FV, García-Giménez JL, Montoya Á, et al. Comparative Analysis of Chromatin-Delivered Biomarkers in the Monitoring of Sepsis and Septic Shock: A Pilot Study. International Journal of Molecular Sciences. 2021; 22(18):9935. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22189935
Chicago/Turabian StyleBeltrán-García, Jesús, Juan J. Manclús, Eva M. García-López, Nieves Carbonell, José Ferreres, María Rodríguez-Gimillo, Concepción Garcés, Federico V. Pallardó, José L. García-Giménez, Ángel Montoya, and et al. 2021. "Comparative Analysis of Chromatin-Delivered Biomarkers in the Monitoring of Sepsis and Septic Shock: A Pilot Study" International Journal of Molecular Sciences 22, no. 18: 9935. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22189935