
Blood Plasma’s Protective Ability against the Degradation of S-Nitrosoglutathione under the Influence of Air-Pollution-Derived Metal Ions in Patients with Exacerbation of Heart Failure and Coronary Artery Disease

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results and Discussion
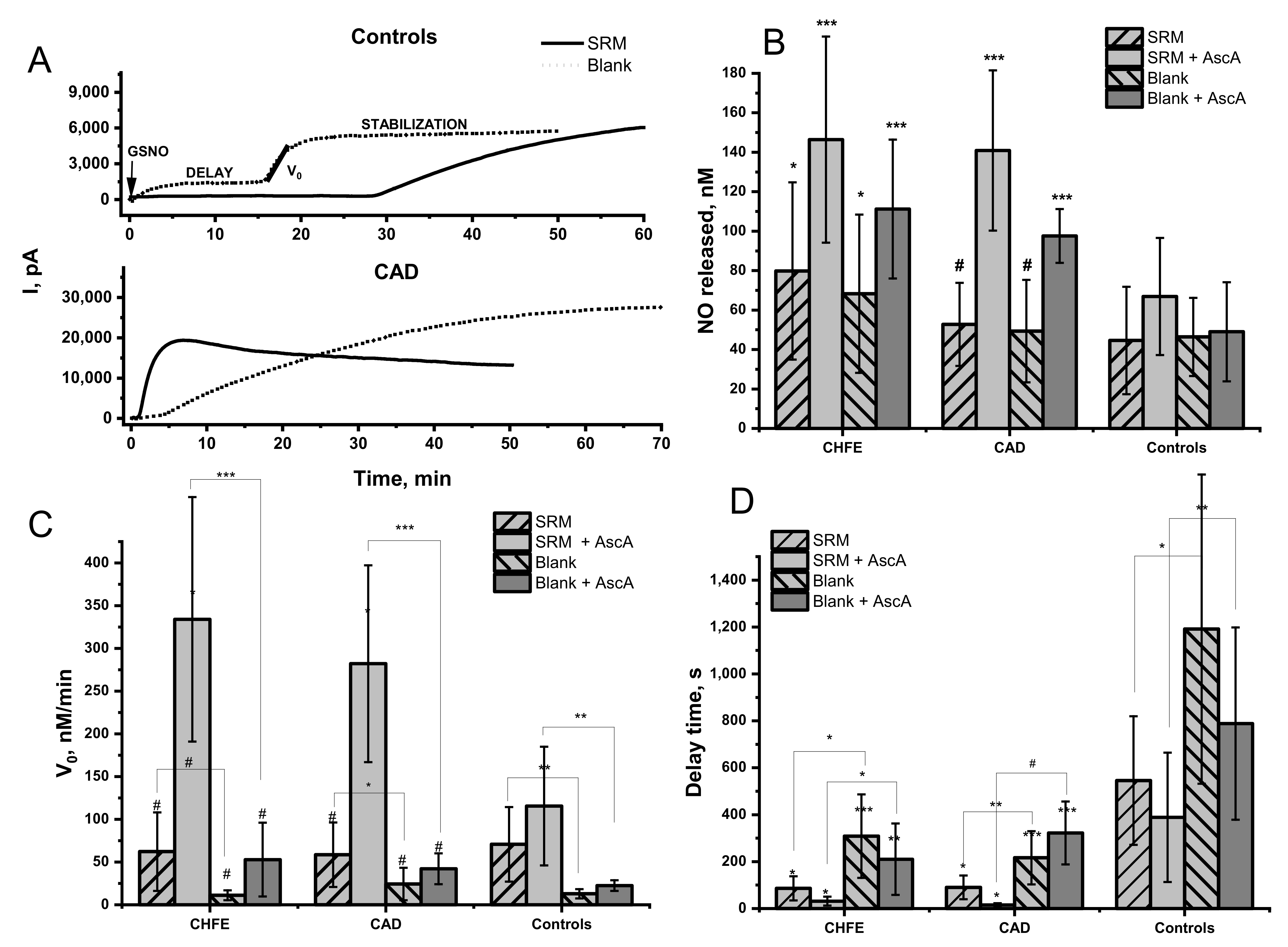
2.1. Influence of Urban PM Extracts on the GSNO Decomposition in the Blood Plasma Environment
2.2. Effect of Ascorbic Acid on the GSNO Decomposition by Urban PM Extracts in the Blood Plasma Environment
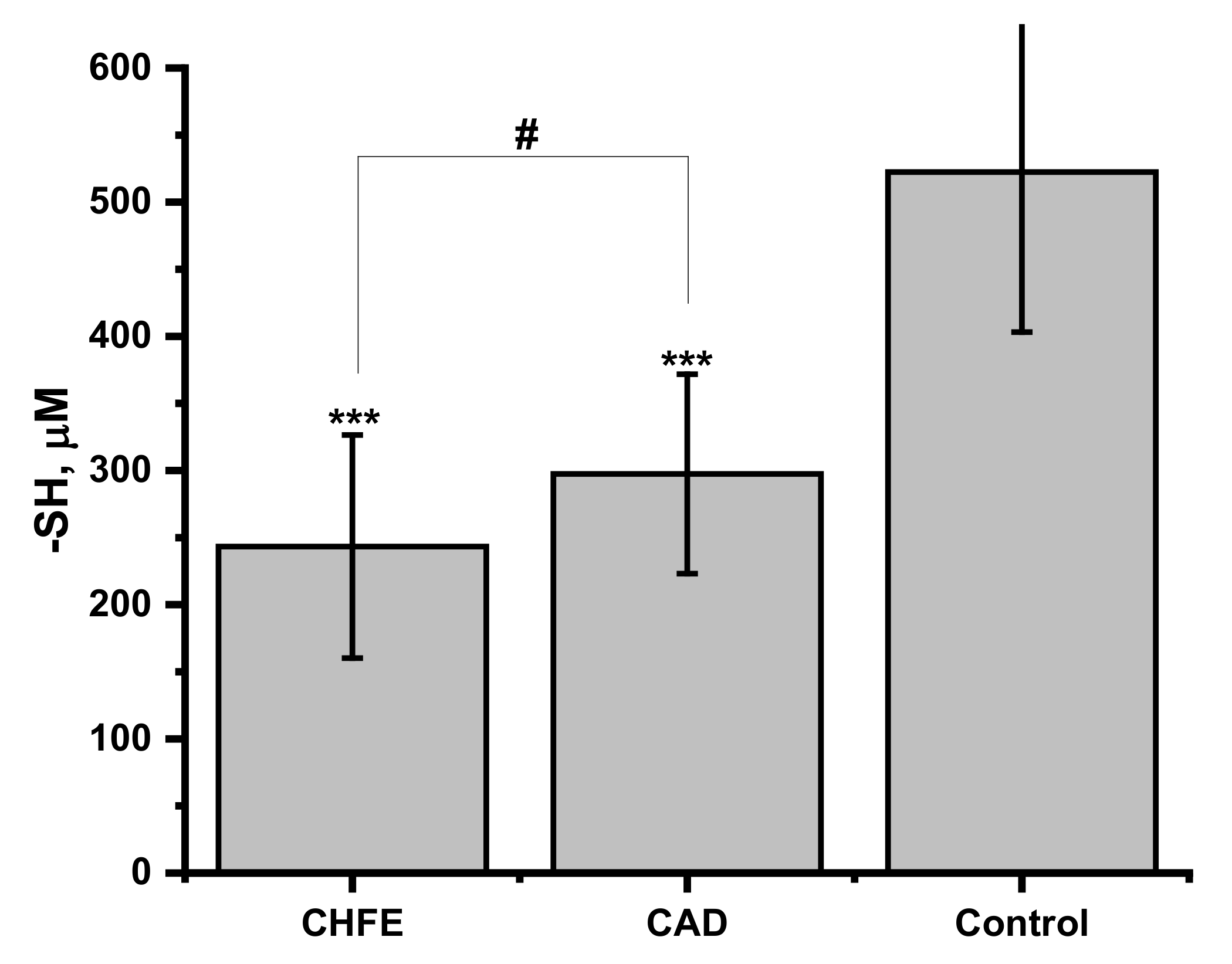
2.3. Free Thiol Content in Human Plasma and Its Influence on NO Release from GSNO
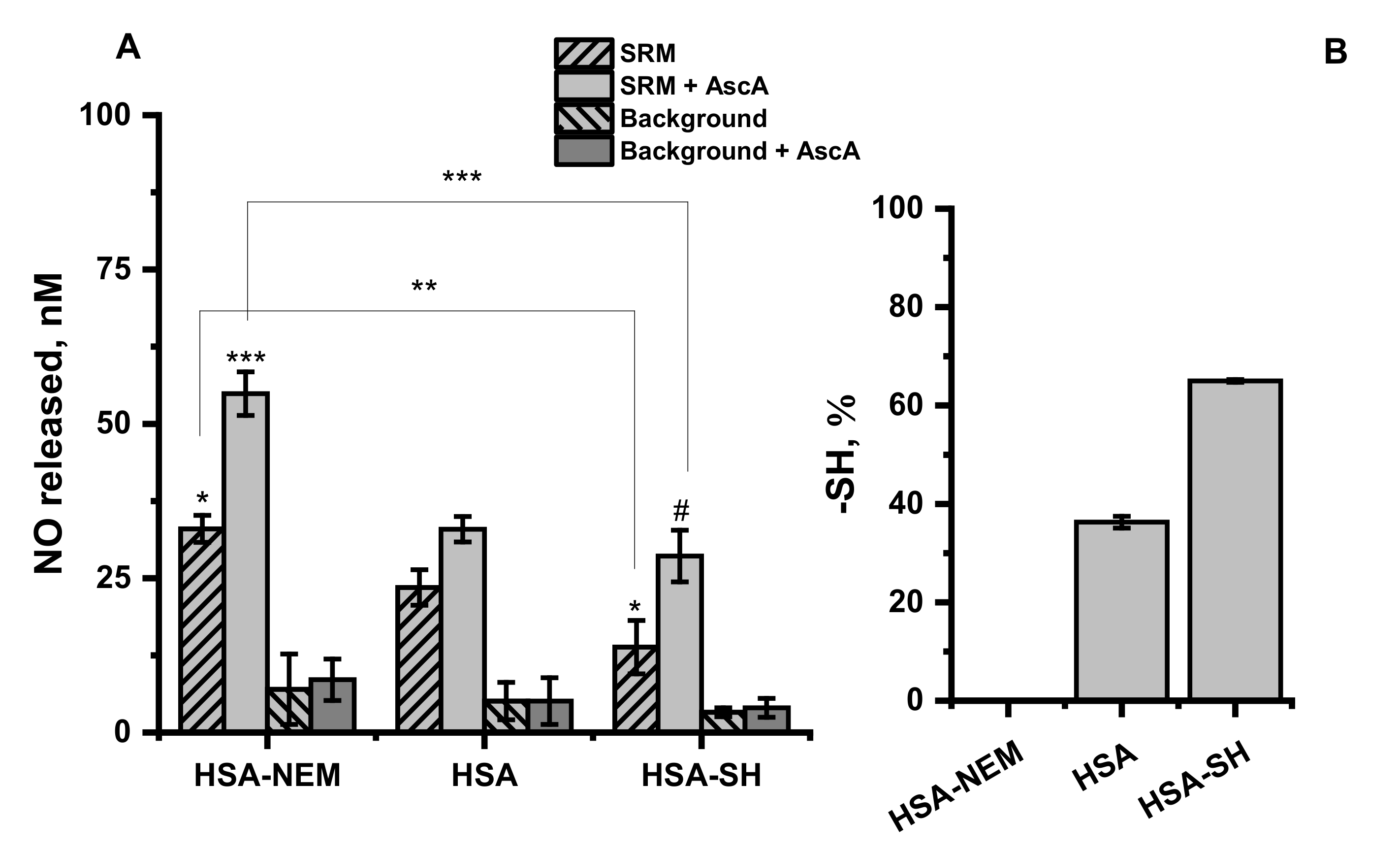
2.4. Effect of Free Thiol Groups in Albumin on GSNO Decomposition by Urban PM Extracts—Model Studies
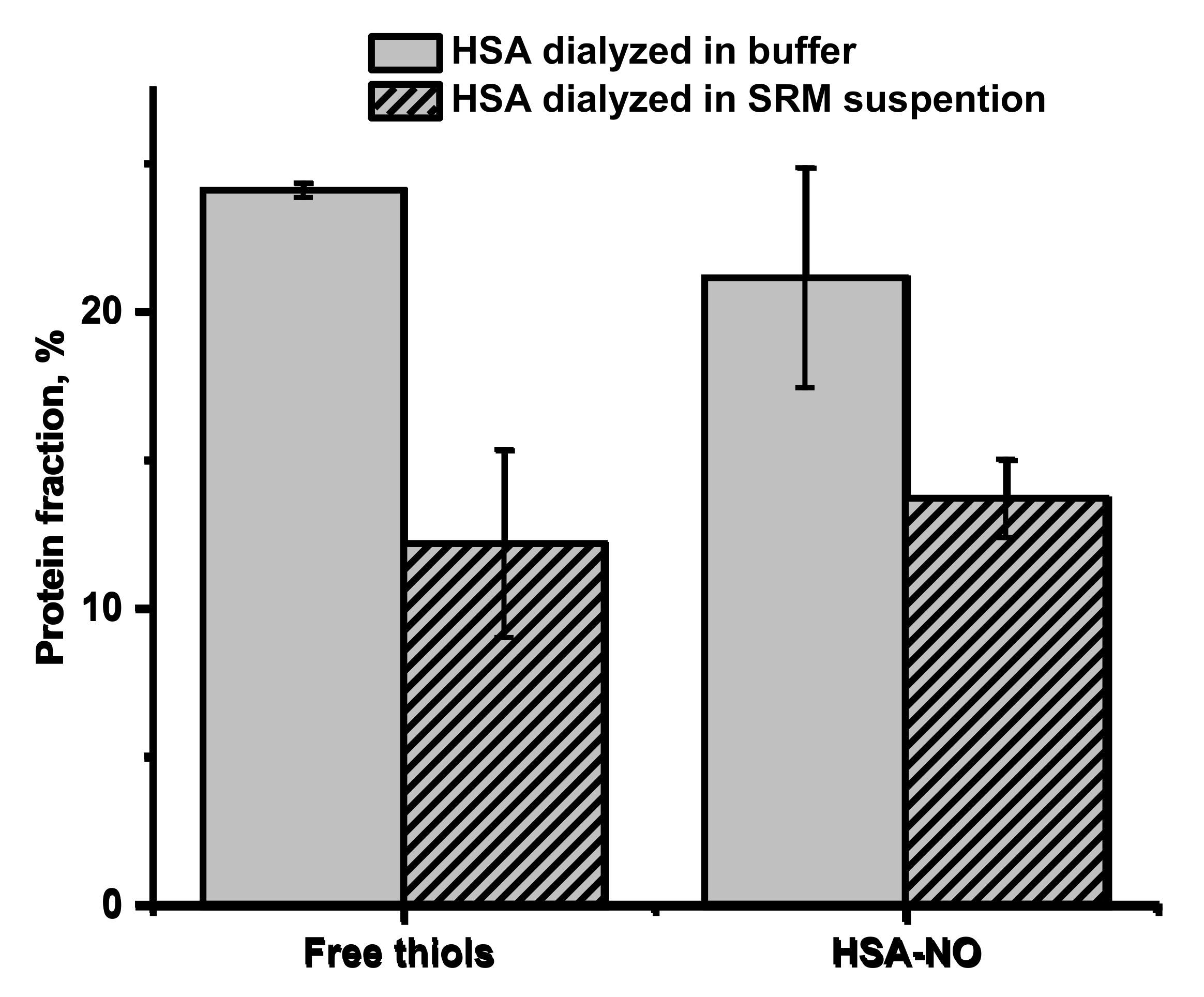
2.5. Effect of Urban PM Extracts on Free Thiol Groups in Albumin and S-Transnitrosation Process—Model Studies
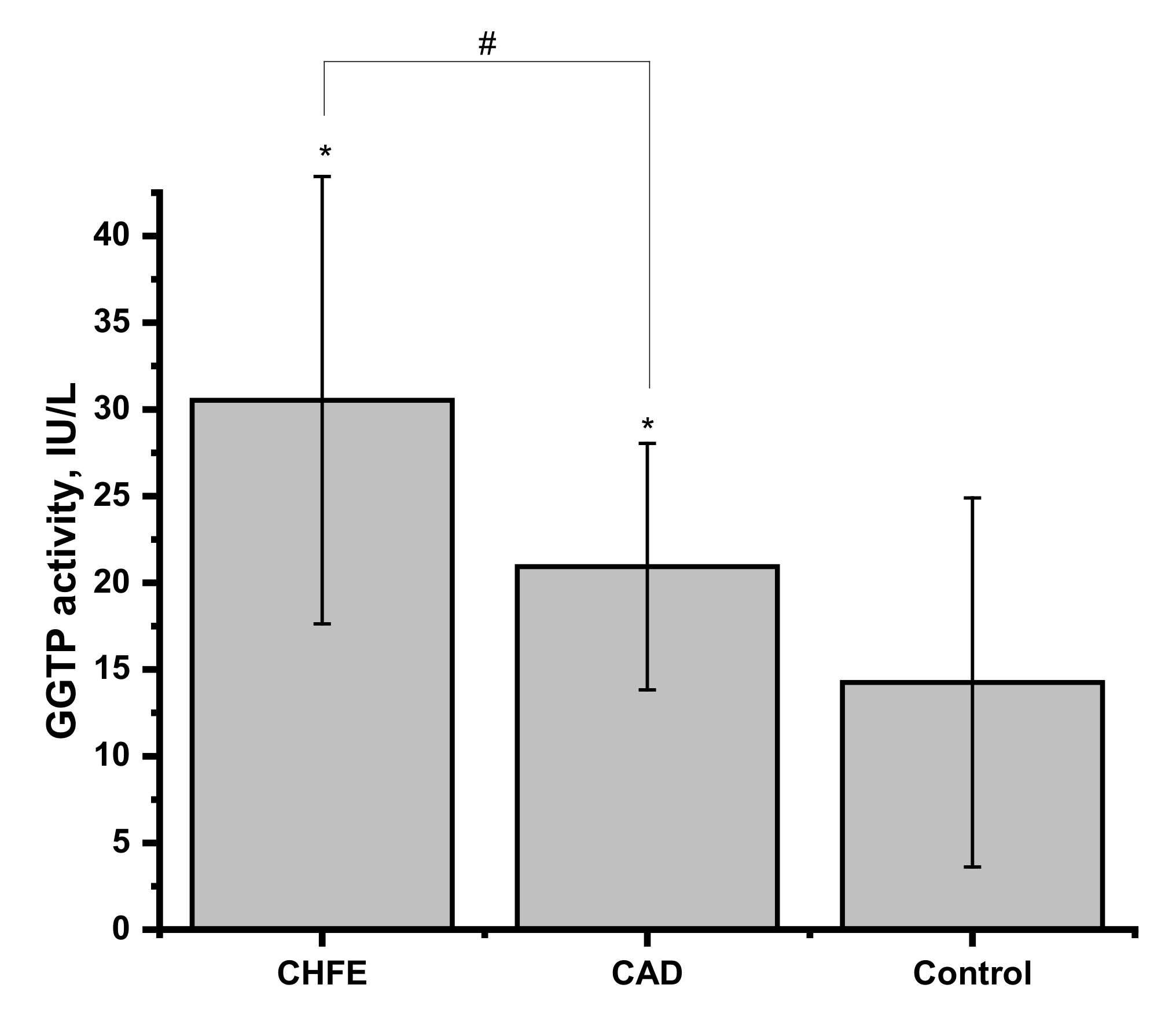
2.6. γ-Glutamyl Transpeptidase Activity in Human Blood Plasma and Its Influence on NO Release from GSNO
2.7. Metal Ions Content of Plasma Samples
3. Materials and Methods
3.1. Materials
3.2. Patients and Sample Collection
3.3. Ethics
3.4. GSNO Preparation
3.5. Particulate Matter’s Extract Preparation
3.6. Human Serum Albumin Modification
3.7. Determination of NO Release from GSNO
3.8. Determination of Free -SH Groups
3.9. Transnitrosation of HSA
3.10. Determination of HSA-NO Concentration
3.11. γ-Glutamyltranspeptidase (GGTP) Activity
3.12. ICP-MS Analysis of Plasma Samples
3.13. Statistics
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Burden of Disease from Household Air Pollution for 2012. In World Health Organization Global Health Risks; World Health Organization: Geneva, Switzerland, 2014; Volume 1, pp. 1–17. [Google Scholar]
- Neira, M.; Prüss-Ustün, A. Preventing Disease through Healthy Environments: A Global Assessment of the Environmental Burden of Disease. Toxicol. Lett. 2018, 259, S1. [Google Scholar] [CrossRef]
- Konduracka, E. A Link between Environmental Pollution and Civilization Disorders: A Mini Review. Rev. Environ. Health 2019, 34, 227–233. [Google Scholar] [CrossRef]
- Farah, C.; Michel, L.Y.M.; Balligand, J.L. Nitric Oxide Signalling in Cardiovascular Health and Disease. Nat. Rev. Cardiol. 2018, 15, 292–316. [Google Scholar] [CrossRef]
- Ahmad, A.; Dempsey, S.K.; Daneva, Z.; Azam, M.; Li, N.; Li, P.L.; Ritter, J.K. Role of Nitric Oxide in the Cardiovascular and Renal Systems. Int. J. Mol. Sci. 2018, 19, 2605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimmeler, S.; Zeiher, A.M. Nitric Oxide—An Endothelial Cell Survival Factor. Cell Death Differ. 1999, 6, 964–968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pacher, P.; Beckman, J.S.; Liaudet, L. Nitric Oxide and Peroxynitrite in Health and Disease. Physiol. Rev. 2007, 87, 315–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcinkiewicz, E.; Chłopicki, S.; Marcinkiewicz, J. Nitric Oxide—A pro-Inflammatory and Anti-Inflammatory Mediator. Cent. J. Immunol. 2003, 28, 74–78. [Google Scholar]
- Zhang, C.; Biggs, T.D.; Devarie-Baez, N.O.; Shuang, S.; Dong, C.; Xian, M. S-Nitrosothiols: Chemistry and Reactions. Chem. Commun. 2017, 53, 11266–11277. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.C.; Marletta, M.A. Mechanisms of S-Nitrosothiol Formation and Selectivity in Nitric Oxide Signaling. Curr. Opin. Chem. Biol. 2012, 16, 498–506. [Google Scholar] [CrossRef] [Green Version]
- Gaston, B.; Singel, D.; Doctor, A.; Stamler, J.S. S-Nitrosothiol Signaling in Respiratory Biology. Am. J. Respir. Crit. Care Med. 2006, 173, 1186–1193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, M.W.; Stamler, J.S. New Insights into Protein S-Nitrosylation: Mitochondria as a Model System. J. Biol. Chem. 2004, 279, 25891–25897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benhar, M.; Forrester, M.T.; Stamler, J.S. Protein Denitrosylation: Enzymatic Mechanisms and Cellular Functions. Nat. Rev. Mol. Cell Biol. 2009, 10, 721–732. [Google Scholar] [CrossRef] [PubMed]
- Opsha, Y.; Brophy, A. Blood, Blood Components, Plasma, and Plasma Products. Side Eff. Drugs Annu. 2015, 37, 403–418. [Google Scholar] [CrossRef]
- Phillips, A.; Gerald Shaper, A.; Whincup, P.H. Association Between Serum Albumin and Mortality From Cardiovascular Disease, Cancer, and Other Causes. Lancet 1989, 334, 1434–1436. [Google Scholar] [CrossRef]
- Oduncu, V.; Erkol, A.; Karabay, C.Y.; Kurt, M.; Akgün, T.; Bulut, M.; Pala, S.; Kirma, C. The Prognostic Value of Serum Albumin Levels on Admission in Patients with Acute ST-Segment Elevation Myocardial Infarction Undergoing a Primary Percutaneous Coronary Intervention. Coron. Artery Dis. 2013, 24, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Sujino, Y.; Tanno, J.; Nakano, S.; Funada, S.; Hosoi, Y.; Senbonmatsu, T.; Nishimura, S. Impact of Hypoalbuminemia, Frailty, and Body Mass Index on Early Prognosis in Older Patients (≥85 Years) with ST-Elevation Myocardial Infarction. J. Cardiol. 2015, 66, 263–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plakht, Y.; Gilutz, H.; Shiyovich, A. Decreased Admission Serum Albumin Level Is an Independent Predictor of Long-Term Mortality in Hospital Survivors of Acute Myocardial Infarction. Soroka Acute Myocardial Infarction II (SAMI-II) Project. Int. J. Cardiol. 2016, 219, 20–24. [Google Scholar] [CrossRef]
- Dziedzic, T.; Slowik, A.; Szczudlik, A. Serum Albumin Level as a Predictor of Ischemic Stroke Outcome. Stroke 2004, 35, 10–12. [Google Scholar] [CrossRef] [Green Version]
- Gryzunov, Y.A.; Arroyo, A.; Vigne, J.L.; Zhao, Q.; Tyurin, V.A.; Hubel, C.A.; Gandley, R.E.; Vladimirov, Y.A.; Taylor, R.N.; Kagan, V.E. Binding of Fatty Acids Facilitates Oxidation of Cysteine-34 and Converts Copper-Albumin Complexes from Antioxidants to Prooxidants. Arch. Biochem. Biophys. 2003, 413, 53–66. [Google Scholar] [CrossRef]
- Bourgonje, M.F.; Bourgonje, A.R.; Abdulle, A.E.; Kieneker, L.M.; la Bastide-van Gemert, S.; Gansevoort, R.T.; Bakker, S.J.L.; Mulder, D.J.; Pasch, A.; Saleh, J.; et al. Systemic Oxidative Stress, Aging and the Risk of Cardiovascular Events in the General Female Population. Front. Cardiovasc. Med. 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Bourgonje, A.R.; Abdulle, A.E.; Al-Rawas, A.M.; Al-Maqbali, M.; Al-Saleh, M.; Enriquez, M.B.; Al-Siyabi, S.; Al-Hashmi, K.; Al-Lawati, I.; Bulthuis, M.L.C.; et al. Systemic Oxidative Stress Is Increased in Postmenopausal Women and Independently Associates with Homocysteine Levels. Int. J. Mol. Sci. 2020, 21, 314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdulle, A.E.; Bourgonje, A.R.; Kieneker, L.M.; Koning, A.M.; La Bastide-Van Gemert, S.; Bulthuis, M.L.C.; Dijkstra, G.; Faber, K.N.; Dullaart, R.P.F.; Bakker, S.J.L.; et al. Serum Free Thiols Predict Cardiovascular Events and All-Cause Mortality in the General Population: A Prospective Cohort Study. BMC Med. 2020, 18, 130. [Google Scholar] [CrossRef] [PubMed]
- Ronit, A.; Kirkegaard-Klitbo, D.M.; Dohlmann, T.L.; Lundgren, J.; Sabin, C.A.; Phillips, A.N.; Nordestgaard, B.G.; Afzal, S. Plasma Albumin and Incident Cardiovascular Disease Results from the CGPS and an Updated Meta-Analysis. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 473–482. [Google Scholar] [CrossRef] [Green Version]
- Demircan, S.; Yazici, M.; Durna, K.; Kilicaslan, F.; Demir, S.; Pinar, M.; Gulel, O. The Importance of Gamma-Glutamyltransferase Activity in Patients with Coronary Artery Disease. Clin. Cardiol. 2009, 32, 220–225. [Google Scholar] [CrossRef]
- Poelzl, G.; Eberl, C.; Achrainer, H.; Doerler, J.; Pachinger, O.; Frick, M.; Ulmer, H. Prevalence and Prognostic Significance of Elevated γ- Glutamyltransferase in Chronic Heart Failure. Circ. Heart Fail. 2009, 2, 294–302. [Google Scholar] [CrossRef] [Green Version]
- Dalos, D.; Binder, C.; Duca, F.; Aschauer, S.; Kammerlander, A.; Hengstenberg, C.; Mascherbauer, J.; Reiberger, T.; Bonderman, D. Serum Levels of Gamma-Glutamyltransferase Predict Outcome in Heart Failure with Preserved Ejection Fraction. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef]
- Li, D.D.; Xu, T.; Cheng, X.Q.; Wu, W.; Ye, Y.C.; Guo, X.Z.; Cheng, Q.; Liu, Q.; Liu, L.; Zhu, G.J.; et al. Serum Gamma-Glutamyltransferase Levels Are Associated with Cardiovascular Risk Factors in China: A Nationwide Population-Based Study. Sci. Rep. 2018, 8, 16533. [Google Scholar] [CrossRef] [Green Version]
- Bonnet, F.; Gastaldelli, A.; Pihan-Le Bars, F.; Natali, A.; Roussel, R.; Petrie, J.; Tichet, J.; Marre, M.; Fromenty, B.; Balkau, B. Gamma-Glutamyltransferase, Fatty Liver Index and Hepatic Insulin Resistance Are Associated with Incident Hypertension in Two Longitudinal Studies. J. Hypertens. 2017, 35, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Brookes, M.J.; Cooper, B.T. Hypertension and Fatty Liver: Guilty by Association? J. Hum. Hypertens. 2007, 21, 264–270. [Google Scholar] [CrossRef]
- Matsushita, M.; Shirakabe, A.; Okazaki, H.; Shibata, Y.; Goda, H.; Shigihara, S.; Asano, K.; Tani, K.; Kiuchi, K.; Murase, T.; et al. Plasma Xanthine Oxidoreductase (XOR) Activity in Cardiovascular Disease Outpatients. Circ. Rep. 2020, 2, 104–112. [Google Scholar] [CrossRef] [Green Version]
- Trujillo, M.; Alvarez, M.N.; Peluffo, G.; Freeman, B.A.; Radi, R. Xanthine Oxidase-Mediated Decomposition of S-Nitrosothiols. J. Biol. Chem. 1998, 273, 7828–7834. [Google Scholar] [CrossRef] [Green Version]
- Yilmaz, N.; Demir, C.; Eren, E. Increased Levels of Thioredoxin and Thioredoxin Reductase in Diabetic Patients with Coronary Artery Disease. Med. Sci. Int. Med. J. 2021, 10, 391. [Google Scholar] [CrossRef]
- Hayashida, K.; Bagchi, A.; Miyazaki, Y.; Hirai, S.; Seth, D.; Silverman, M.G.; Rezoagli, E.; Marutani, E.; Mori, N.; Magliocca, A.; et al. Improvement in Outcomes after Cardiac Arrest and Resuscitation by Inhibition of S-Nitrosoglutathione Reductase. Circulation 2019, 139, 815–827. [Google Scholar] [CrossRef]
- Shen, J.; Griffiths, P.T.; Campbell, S.J.; Utinger, B.; Kalberer, M.; Paulson, S.E. Ascorbate Oxidation by Iron, Copper and Reactive Oxygen Species: Review, Model Development, and Derivation of Key Rate Constants. Sci. Rep. 2021, 11, 1–14. [Google Scholar] [CrossRef]
- Block, M.L.; Calderón-Garcidueñas, L. Air Pollution: Mechanisms of Neuroinflammation and CNS Disease. Trends Neurosci. 2009, 32, 506–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bal, W.; Sokołowska, M.; Kurowska, E.; Faller, P. Binding of Transition Metal Ions to Albumin: Sites, Affinities and Rates. Biochim. Biophys. Acta Gen. Subj. 2013, 1830, 5444–5455. [Google Scholar] [CrossRef] [PubMed]
- Blindauer, C.A.; Khazaipoul, S.; Yu, R.; Stewart, A.J. Fatty Acid-Mediated Inhibition of Metal Binding to the Multi-Metal Site on Serum Albumin: Implications for Cardiovascular Disease. Curr. Top. Med. Chem. 2016, 16, 3021–3032. [Google Scholar] [CrossRef] [Green Version]
- Mazuryk, O.; Gajda-Morszewski, P.; Flejszar, M.; Łabuz, P.; van Eldik, R.; Stochel, G.; Brindell, M. Influence of Aqueous Extracts of Urban Airborne Particulate Matter on the Structure and Function of Human Serum Albumin. Environ. Pollut. 2020, 263, 114667. [Google Scholar] [CrossRef]
- Wądołek, A.; Oszajca, M.; Pęcak, W.; Brindell, M.; Stochel, G. Enhancement of NO Release from S-Nitrosoalbumin by Pollution Derived Metal Ions. Dalt. Trans. 2021. [Google Scholar] [CrossRef]
- Oszajca, M.; Wądołek, A.; Hooper, J.; Brindell, M.; van Eldik, R.; Stochel, G. Urban Particulate Matter-Induced Decomposition of S-Nitrosoglutathione Relevant to Aberrant Nitric Oxide Biological Signaling. ChemSusChem 2019, 12, 661–671. [Google Scholar] [CrossRef]
- Xu, A.; Vita, J.A.; Keaney, J.F. Ascorbic Acid and Glutathione Modulate the Biological Activity of S-Nitrosoglutathione. Hypertension 2000, 36, 291–295. [Google Scholar] [CrossRef] [Green Version]
- Zhou, P.; Zhang, J.; Zhang, Y.; Liu, Y.; Liang, J.; Liu, B.; Zhang, W. Generation of Hydrogen Peroxide and Hydroxyl Radical Resulting from Oxygen-Dependent Oxidation of l-Ascorbic Acid via Copper Redox-Catalyzed Reactions. RSC Adv. 2016, 6, 38541–38547. [Google Scholar] [CrossRef]
- Araujo, F.B.; Barbosa, D.S.; Hsin, C.Y.; Maranhão, R.C.; Abdalla, D.S.P. Evaluation of Oxidative Stress in Patients with Hyperlipidemia. Atherosclerosis 1995, 117, 61–71. [Google Scholar] [CrossRef]
- Cervantes Gracia, K.; Llanas-Cornejo, D.; Husi, H. CVD and Oxidative Stress. J. Clin. Med. 2017, 6, 22. [Google Scholar] [CrossRef] [Green Version]
- Martín-Calvo, N.; Martínez-Gonzàlez, M.Á. Vitamin C Intake Is Inversely Associated with Cardiovascular Mortality in a Cohort of Spanish Graduates: The SUN Project. Nutrients 2017, 9, 954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gokce, N.; Keaney, J.F.; Frei, B.; Holbrook, M.; Olesiak, M.; Zachariah, B.J.; Leeuwenburgh, C.; Heinecke, J.W.; Vita, J.A. Long-Term Ascorbic Acid Administration Reverses Endothelial Vasomotor Dysfunction in Patients with Coronary Artery Disease. Circulation 1999, 99, 3234–3240. [Google Scholar] [CrossRef] [Green Version]
- Morelli, M.B.; Gambardella, J.; Castellanos, V.; Trimarco, V.; Santulli, G. Vitamin C and Cardiovascular Disease: An Update. Antioxidants 2020, 9, 1227. [Google Scholar] [CrossRef]
- Dewhirst, R.A.; Fry, S.C. The Oxidation of Dehydroascorbic Acid and 2,3-Diketogulonate by Distinct Reactive Oxygen Species. Biochem. J. 2018, 475, 3451–3470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandley, R.E.; Tyurin, V.A.; Huang, W.; Arroyo, A.; Daftary, A.; Harger, G.; Jiang, J.; Pitt, B.; Taylor, R.N.; Hubel, C.A.; et al. S-Nitrosoalbumin-Mediated Relaxation Is Enhanced by Ascorbate and Copper: Effects in Pregnancy and Preeclampsia Plasma. Hypertension 2005, 45, 21–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yordanova, M.G. Research of Oxidative Stress and Serum Thiols as a Criterion for the Antioxidant Barrier in Patients with Heart Failure (NYHA FC III-IV). Online J. Cardiol. Res. Rep. 2020, 4, 2–7. [Google Scholar] [CrossRef]
- Koning, A.M.; Meijers, W.C.; Pasch, A.; Leuvenink, H.G.D.; Frenay, A.R.S.; Dekker, M.M.; Feelisch, M.; de Boer, R.A.; van Goor, H. Serum Free Thiols in Chronic Heart Failure. Pharmacol. Res. 2016, 111, 452–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altiparmak, I.H.; Erkuş, M.E.; Sezen, H.; Demirbag, R.; Gunebakmaz, O.; Kaya, Z.; Sezen, Y.; Asoglu, R.; Dedeoglu, I.H.; Neselioglu, S.; et al. The Relation of Serum Thiol Levels and Thiol/Disulphide Homeostasis with the Severity of Coronary Artery Disease. Kardiol. Pol. 2016, 74, 1346–1353. [Google Scholar] [CrossRef] [PubMed]
- Kirsch, M.; Büscher, A.M.; Aker, S.; Schulz, R.; De Groot, H. New Insights into the S-Nitrosothiol-Ascorbate Reaction. The Formation of Nitroxyl. Org. Biomol. Chem. 2009, 7, 1954–1962. [Google Scholar] [CrossRef] [PubMed]
- Maksimenko, A.V.; Vavaev, A.V. Antioxidant Enzymes as Potential Targets in Cardioprotection and Treatment of Cardiovascular Diseases. Enzyme Antioxidants: The next Stage of Pharmacological Counterwork to the Oxidative Stress. Heart Int. 2012, 7, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Turell, L.; Radi, R.; Alvarez, B. The Thiol Pool in Human Plasma: The Central Contribution of Albumin to Redox Processes. Free Radic. Biol. Med. 2013, 65, 244–253. [Google Scholar] [CrossRef] [Green Version]
- Quinlan, G.J.; Martin, G.S.; Evans, T.W. Albumin: Biochemical Properties and Therapeutic Potential. Hepatology 2005, 41, 1211–1219. [Google Scholar] [CrossRef]
- Altomare, A.; Baron, G.; Brioschi, M.; Longoni, M.; Butti, R.; Valvassori, E.; Tremoli, E.; Carini, M.; Agostoni, P.; Vistoli, G.; et al. N-Acetyl-Cysteine Regenerates Albumin Cys34 by a Thiol-Disulfide Breaking Mechanism: An Explanation of Its Extracellular Antioxidant Activity. Antioxidants 2020, 9, 367. [Google Scholar] [CrossRef]
- Lovstad, R.A. Copper catalyzed oxidation of ascorbate (vitamin C). Inhibitory effect of catalase, superoxide dismutase, serum proteins (ceruloplasmin, albumin, apotransferrin) and amino acids. Int. J. Biochem. 1987, 19, 309–313. [Google Scholar] [CrossRef]
- Manoj, V.M.; Aravindakumar, C.T. Hydroxyl Radical Induced Decomposition of S-Nitrosoglutathione. Chem. Commun. 2000, 2361–2362. [Google Scholar] [CrossRef]
- Liu, S.; Grigoryan, H.; Edmands, W.M.B.; Dagnino, S.; Sinharay, R.; Cullinan, P.; Collins, P.; Chung, K.F.; Barratt, B.; Kelly, F.J.; et al. Cys34 Adductomes Differ between Patients with Chronic Lung or Heart Disease and Healthy Controls in Central London. Environ. Sci. Technol. 2018, 52, 2307–2313. [Google Scholar] [CrossRef]
- Tsikas, D.; Sandmann, J.; Lueßen, P.; Savva, A.; Rossa, S.; Stichtenoth, D.O.; Frölich, J.C. S-Transnitrosylation of Albumin in Human Plasma and Blood in Vitro and in Vivo in the Rat. Biochim. Biophys. Acta Protein Struct. Mol. Enzymol. 2001, 1546, 422–434. [Google Scholar] [CrossRef]
- Hogg, N.; Singh, R.J.; Konorev, E.; Joseph, J.; Kalyanaraman, B. S-Nitrosoglutathione as a Substrate for γ-Glutamyl Transpeptidase. Biochem. J. 1997, 323, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Dahboul, F.; Leroy, P.; Maguin Gate, K.; Boudier, A.; Gaucher, C.; Liminana, P.; Lartaud, I.; Pompella, A.; Perrin-Sarrado, C. Endothelial γ-Glutamyltransferase Contributes to the Vasorelaxant Effect of S-Nitrosoglutathione in Rat Aorta. PLoS ONE 2012, 7, e43190. [Google Scholar] [CrossRef] [PubMed]
- Angeli, V.; Tacito, A.; Paolicchi, A.; Barsacchi, R.; Franzini, M.; Baldassini, R.; Vecoli, C.; Pompella, A.; Bramanti, E. A Kinetic Study of Gamma-Glutamyltransferase (GGT)-Mediated S-Nitrosoglutathione Catabolism. Arch. Biochem. Biophys. 2009, 481, 191–196. [Google Scholar] [CrossRef]
- Giral, P.; Jacob, N.; Dourmap, C.; Hansel, B.; Carrié, A.; Bruckert, E.; Girerd, X.; Chapman, M.J. Elevated Gamma-Glutamyltransferase Activity and Perturbed Thiol Profile Are Associated with Features of Metabolic Syndrome. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 587–593. [Google Scholar] [CrossRef] [Green Version]
- Hart, T.W. Some Observations Concerning the S-Nitroso and S-Phenylsulphonyl Derivatives of L-Cysteine and Glutathione. Tetrahedron Lett. 1985, 26, 2013–2016. [Google Scholar] [CrossRef]
- Saville, B. A Scheme for the Colorimetric Determination of Microgram Amounts of Thiols. Analyst 1958, 83, 670–672. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| R | p | |
|---|---|---|
| SRM | −0.3871 | 0.035 |
| SRM + AscA | −0.7477 | <0.001 |
| Blank | −0.3005 | 0.107 |
| Blank + AscA | −0.7070 | <0.001 |
| R | p | |
|---|---|---|
| SRM | 0.66961 | <0.001 |
| SRM + AscA | 0.40602 | 0.029 |
| Blank | 0.61778 | <0.001 |
| Blank + AscA | 0.72515 | <0.001 |
| Free -SH | −0.45181 | 0.014 |
| Element | CHFE Patients (n = 7) | CAD Patients (n = 8) | Controls (n = 13) | Range |
|---|---|---|---|---|
| Mean ± Std Dev. | Mean ± Std Dev. | Mean ± Std Dev. | ||
| Be (μg/L) | 1.09 ± 0.43 | 0.87 ± 0.24 | 0.94 ± 0.08 | 0.69–1.38 |
| Mn (μg/L) | 3.82 ± 2.16 | 4.32 ± 3.17 | 3.73 ± 2.25 | 1.46–7.75 |
| Co (μg/L) | 1.22 ± 0.61 | 1.16 ± 0.62 | 1.23 ± 0.56 | 0.59–1.85 |
| Se (μg/L) | 58.52 ± 3.77 ** | 69.13 ± 1.05 | 74.35 ± 1.62 | 55.40–75.88 |
| Ag (μg/L) | 1.41 ± 0.39 | 1.3 ± 0.27 | 1.12 ± 0.37 | 0.98–1.74 |
| Cd (μg/L) | 0.84 ± 0.19 ** | 0.54 ± 0.08 | 0.52 ± 0.08 | 0.43–1.04 |
| Cs (μg/L) | 0.88 ± 0.03 | 0.58 ± 0.03 | 0.68 ± 0.02 | 0.55–0.91 |
| Ba (μg/L) | 8.01 ± 3.14 | 5.56 ± 1.59 | 10.22 ± 5.82 | 4.44–14.33 |
| Tl (μg/L) | 0.07 ± 0.04 | 0.04 ± 0.01 | 0.03 ± 0.01 | 0.02–0.11 |
| Pb (μg/L) | 9.98 ± 0.04 * | 9.70 ± 0.49 *** | 7.97 ± 0.12 | 7.88–11.24 |
| Bi (μg/L) | 1.94 ± 0.87 | 1.68 ± 1.33 | 2.18 ± 1.45 | 0.98–3.85 |
| Ni (μg/L) | 4.83 ± 3.57 | 4.13 ± 2.64 | 4.64 ± 3.34 | 0.78–8.15 |
| Fe (mg/L) | 1.16 ± 0.15* | 1.12 ± 0.03 ** | 1.78 ± 0.20 | 1.01–2.00 |
| Cu (mg/L) | 1.16 ± 0.16 | 1.01 ± 0.19 | 1.02 ± 0.19 | 0.80–1.21 |
| Zn (mg/L) | 0.65 ± 0.12 | 0.73 ± 0.08 | 0.70 ± 0.12 | 0.51–0.822 |
| Subjects | n = 30 | Age Range (years) | Mean Age (mean ± SD) | Males/Females |
|---|---|---|---|---|
| Healthy Controls | 15 | 44–59 | 49 ± 5 | 11/4 |
| Patients | ||||
| CHFE | 7 | 53–76 | 68 ± 9 | 5/2 |
| CAD | 8 | 61–79 | 73 ± 6 | 7/1 |
| CHFE | CAD | p Value | |
|---|---|---|---|
| Laboratory Investigaitons | Mean ± SD | ||
| HGB (g/dL) | 13.20 ± 1.66 | 13.40 ± 1.42 | >0.05 |
| CREA (µmol/L) | 99.86 ± 20.67 | 91.75 ± 10.95 | >0.05 |
| eGFR (mL/min/1.73 m2) | 65.86 ± 23.38 | 69.75 ± 7.43 | >0.05 |
| LDL-C (mmol/L) | 2.68 ± 0.98 | 2.68 ± 0.82 | >0.05 |
| HDL-C (mmol/L) | 1.06 ± 0.25 | 1.19 ± 0.22 | >0.05 |
| Non-HDL (mmol/L) | 2.77 ± 0.95 | 2.90 ± 0.81 | >0.05 |
| TC (mmol/L) | 3.83 ± 1.13 | 4.13 ± 0.67 | >0.05 |
| TG (mmol/L) | 1.02 ± 0.37 | 1.68 ± 0.76 | >0.05 |
| EF (%) | 21 ± 0.05 | 60 ± 0.05 | <0.001 |
| AIP | −0.03 ± 0.18 | 0.11 ± 0.25 | =0.02 |
| CRI-I | 3.59 ± 0.61 | 3.63 ± 1.05 | >0.05 |
| Pharmacological Treatment | CHFE | CAD | |
| Statins (%) | 57.14 | 87.50 | |
| ACEIs or ARB (%) | 57.14 | 100 | |
| β -Blockers (%) | 100 | 87.50 | |
| CCBs (%) | 0 | 37.50 | |
| Diuretics (%) | 100 | 75.00 | |
| Antiplatelet agents (%) | 100 | 100 | |
| Element | Calibration Range [μg/L] | ICP-MS Mode |
|---|---|---|
| Be | 0.01–10 | He |
| Mn | 0.01–10 | He |
| Co | 0.01–10 | He |
| Se | 0.01–10 | CH4 |
| Ag | 0.01–10 | No Gas |
| Cd | 0.01–10 | No Gas |
| Cs | 0.01–10 | No Gas |
| Ba | 0.01–10 | No Gas |
| Tl | 0.01–10 | No Gas |
| Pb | 0.01–10 | He |
| Bi | 0.01–10 | He |
| Fe | 0.5–100 | He |
| Ni | 0.01–10 | He |
| Cu | 0.01–10 | He |
| Zn | 0.01–10 | He |
| Element | Unit | Range of Measured Concentrations | Reference Range of Concentrations |
|---|---|---|---|
| Be | µg/L | 1.52–1.93 | 1.61–2.42 |
| Mn | µg/L | 1.16–1.66 | 1.81–2.72 |
| Co | µg/L | 2.25–2.75 | 1.74–2.61 |
| Se | µg/L | 96.44–129.4 | 98.1–147 |
| Ag | µg/L | 4.43–4.84 | 3.98–5.97 |
| Cd | µg/L | 1.26–1.85 | 1.50–2.25 |
| Ba | µg/L | 390.25–457.61 | 364–492 |
| Tl | µg/L | 1.74–1.90 | 1.49–2.23 |
| Bi | µg/L | 0.77–1.10 | 0.79–1.20 |
| Fe | mg/L | 1.15–1.49 | 0.874–1.31 |
| Ni | µg/L | 1.08–2.24 | 1.54–2.86 |
| Cu | mg/L | 0.83–1.3 | 0.902–1.22 |
| Zn | mg/L | 0.53–0.85 | 0.626–0.85 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wądołek, A.; Drwiła, D.; Oszajca, M.; Stochel, G.; Konduracka, E.; Brindell, M. Blood Plasma’s Protective Ability against the Degradation of S-Nitrosoglutathione under the Influence of Air-Pollution-Derived Metal Ions in Patients with Exacerbation of Heart Failure and Coronary Artery Disease. Int. J. Mol. Sci. 2021, 22, 10500. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms221910500
Wądołek A, Drwiła D, Oszajca M, Stochel G, Konduracka E, Brindell M. Blood Plasma’s Protective Ability against the Degradation of S-Nitrosoglutathione under the Influence of Air-Pollution-Derived Metal Ions in Patients with Exacerbation of Heart Failure and Coronary Artery Disease. International Journal of Molecular Sciences. 2021; 22(19):10500. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms221910500
Chicago/Turabian StyleWądołek, Anna, Dominika Drwiła, Maria Oszajca, Grażyna Stochel, Ewa Konduracka, and Małgorzata Brindell. 2021. "Blood Plasma’s Protective Ability against the Degradation of S-Nitrosoglutathione under the Influence of Air-Pollution-Derived Metal Ions in Patients with Exacerbation of Heart Failure and Coronary Artery Disease" International Journal of Molecular Sciences 22, no. 19: 10500. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms221910500