A Micellar Formulation of Quercetin Prevents Cisplatin Nephrotoxicity

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Results
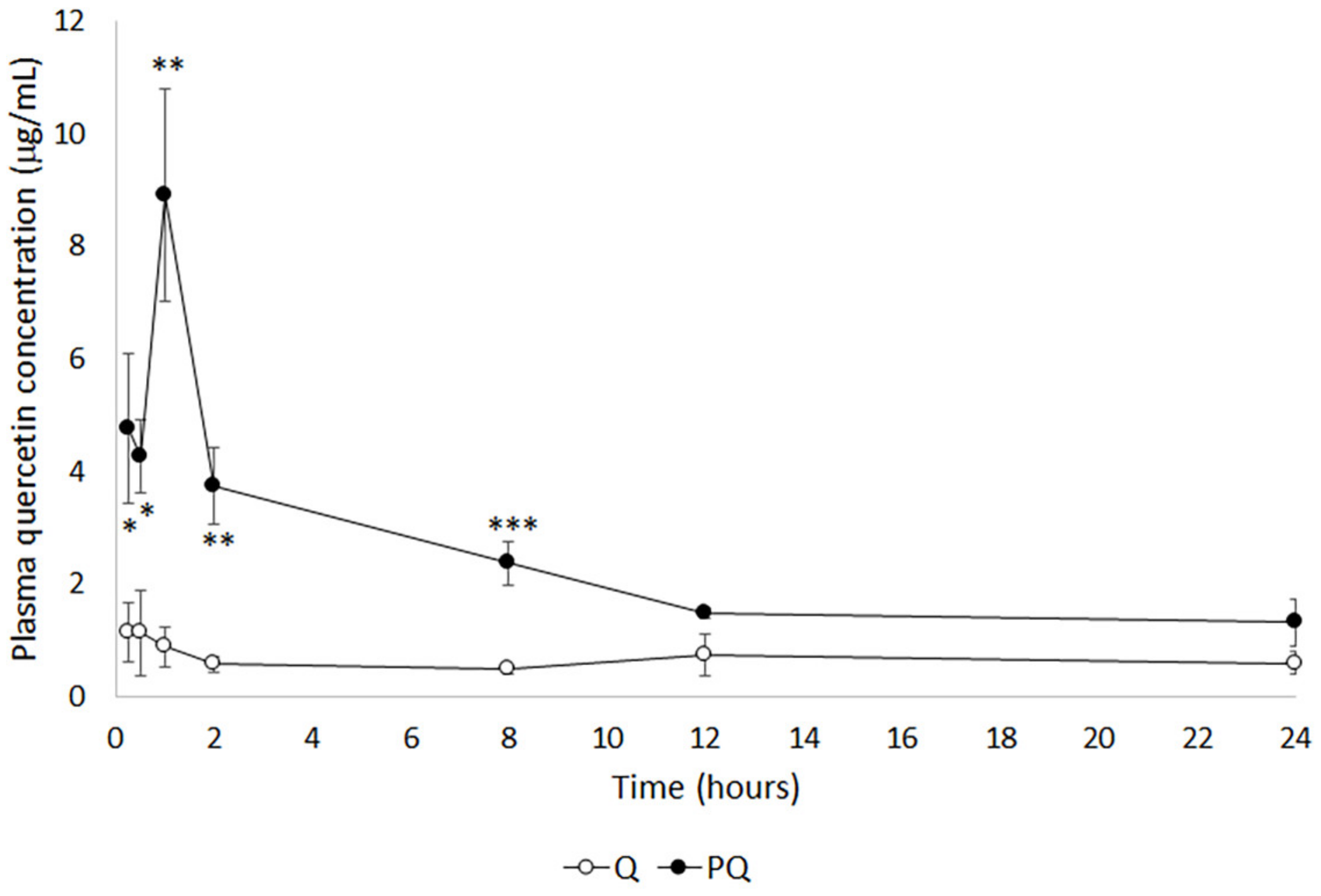
2.1. Bioavailability Study
2.2. Nephroprotective Efficacy Study
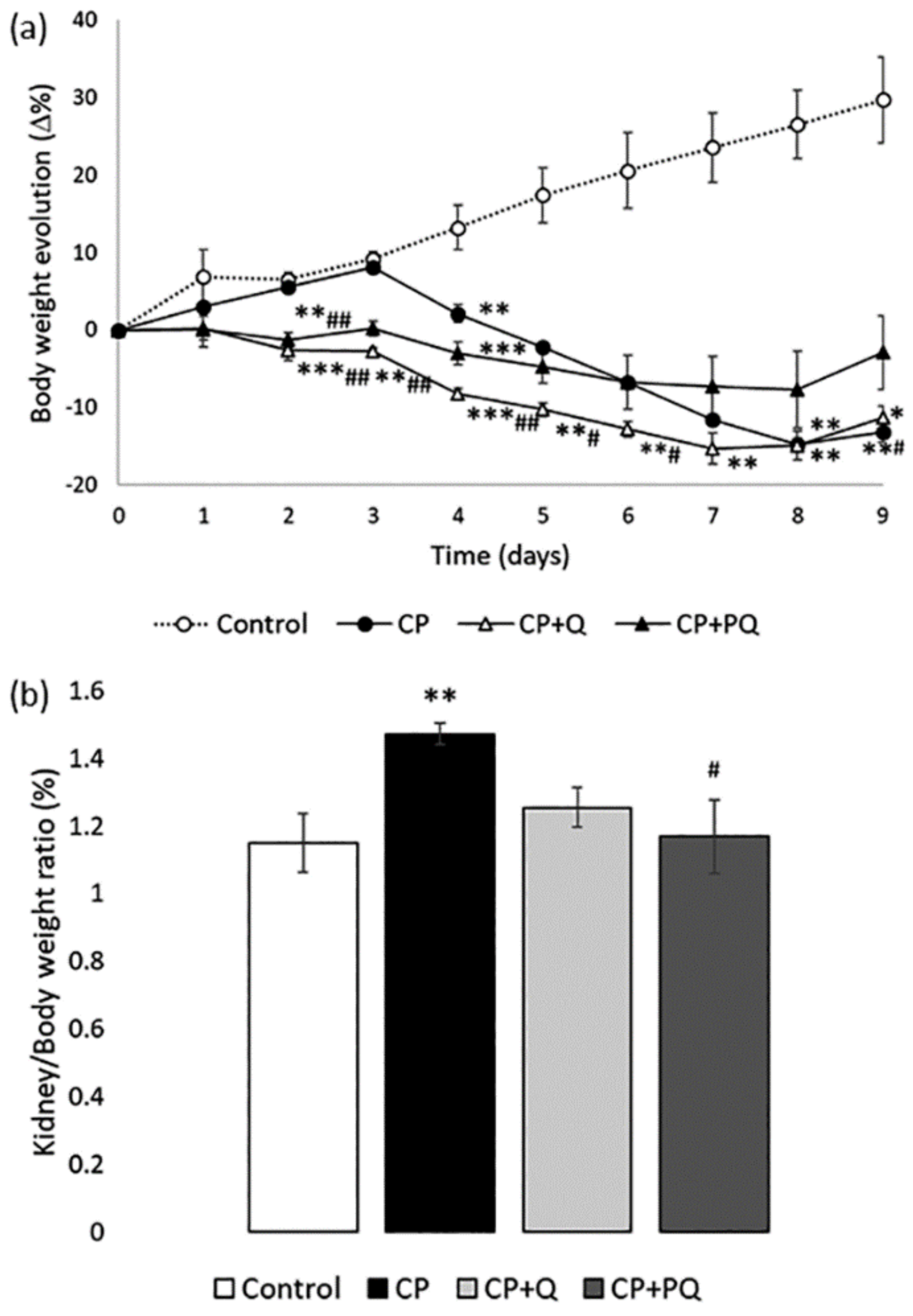
2.2.1. Physiological State
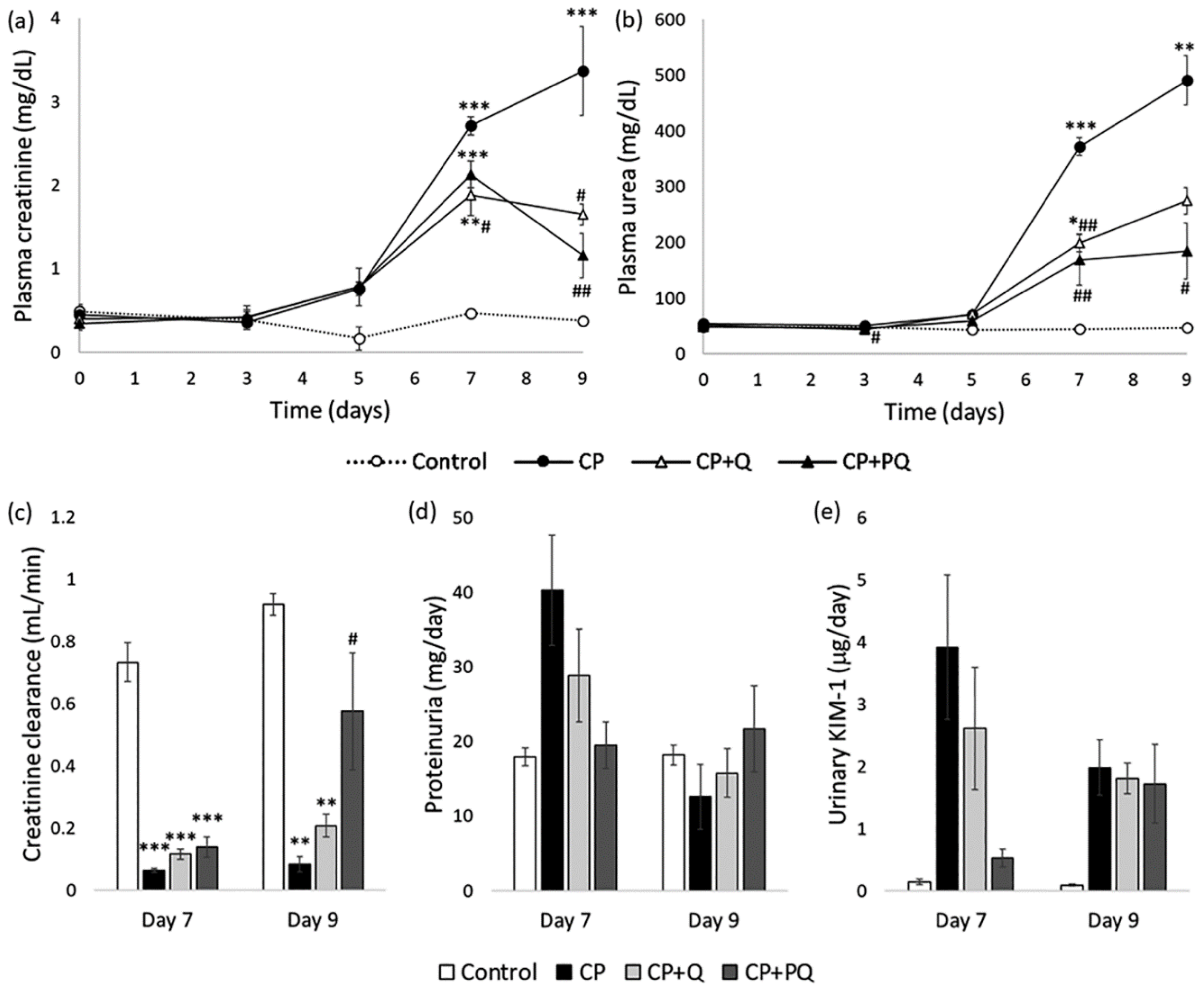
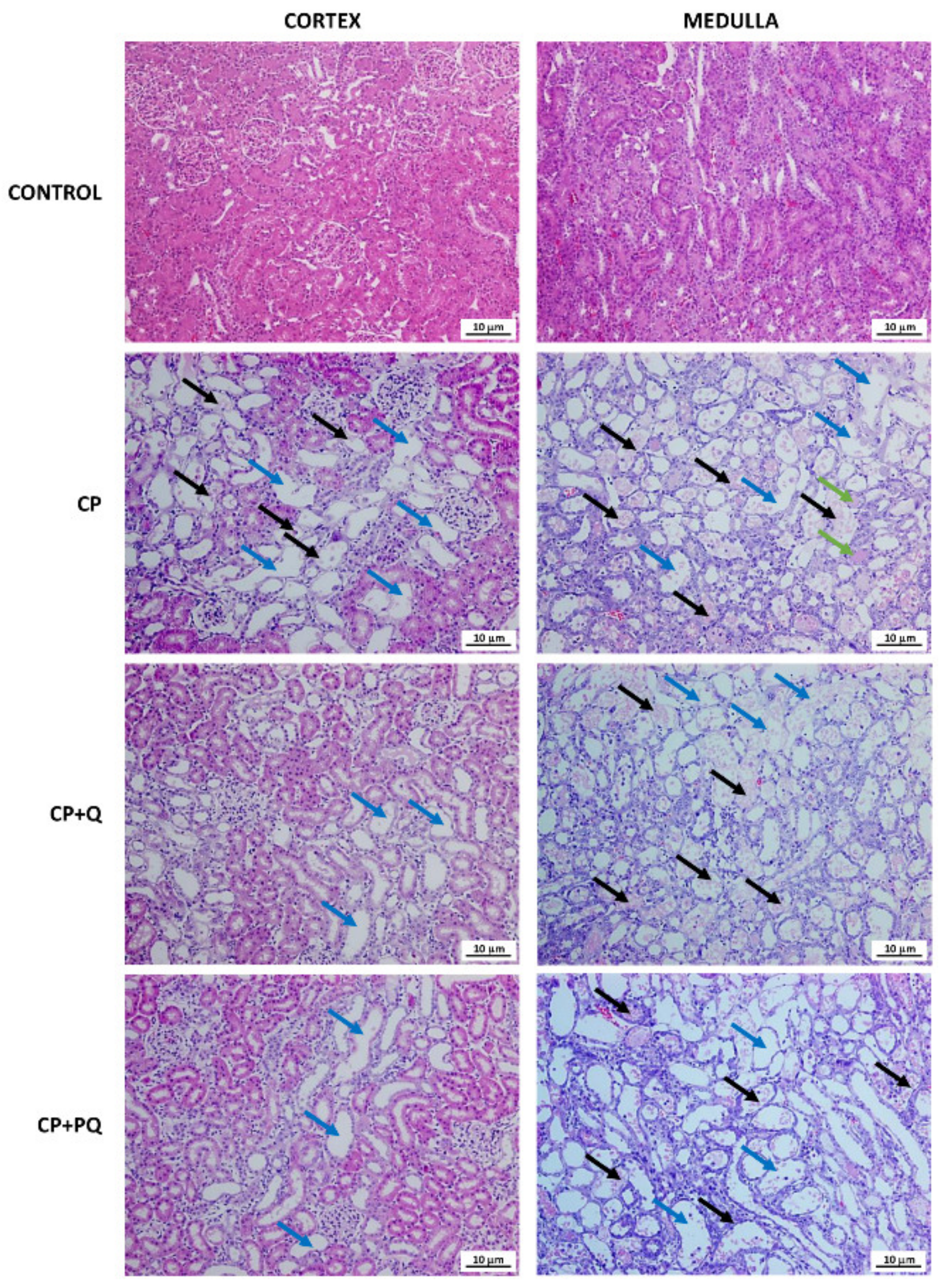
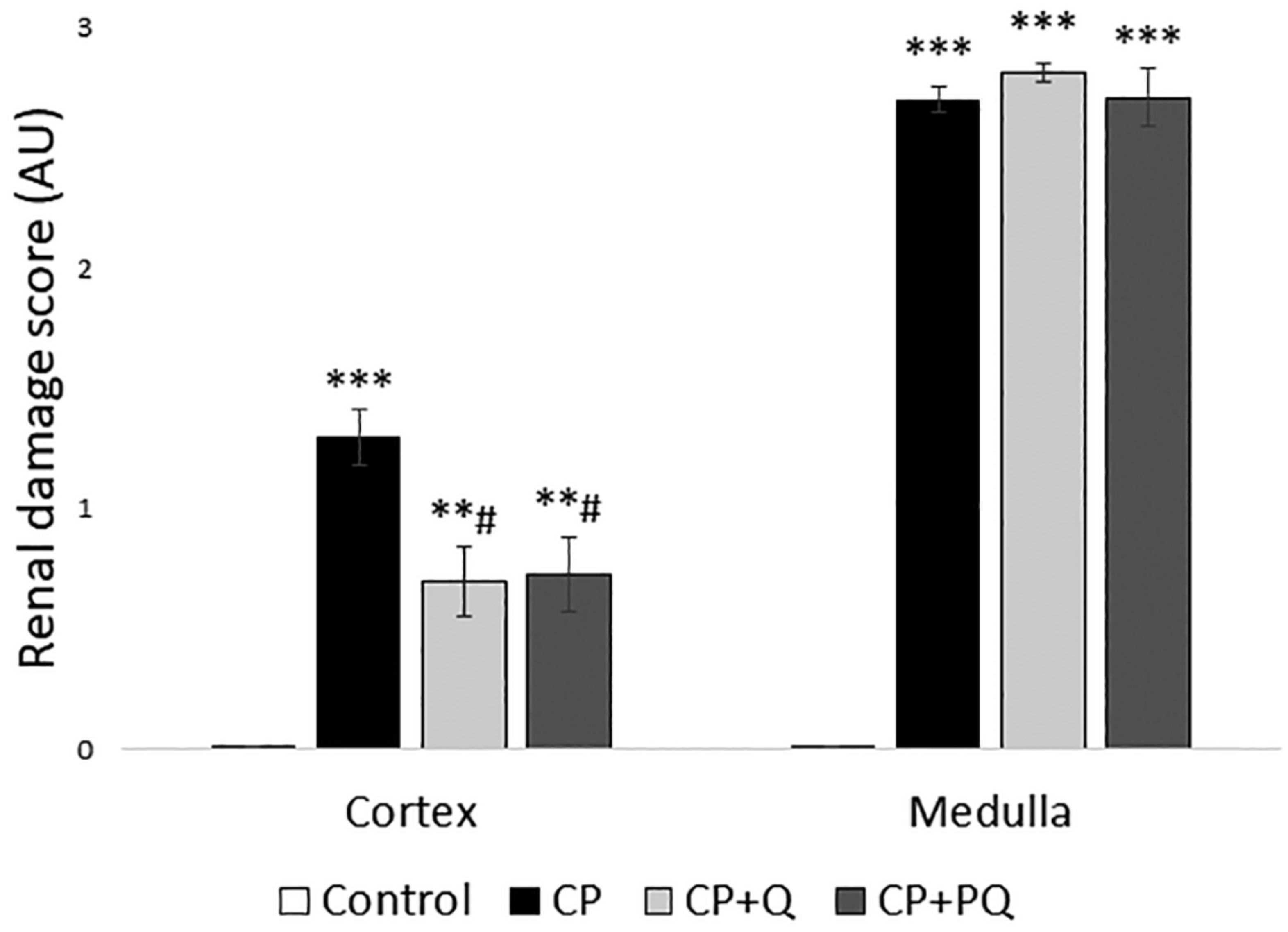
2.2.2. Renal Function and Renal Tissue Assessment
3. Discussion
4. Materials and Methods
4.1. Preparation of the Micellar Formulation (P-quercetin) and the Natural Quercetin Formulation
4.2. Animals and Bioethics
4.3. Bioavailability Study
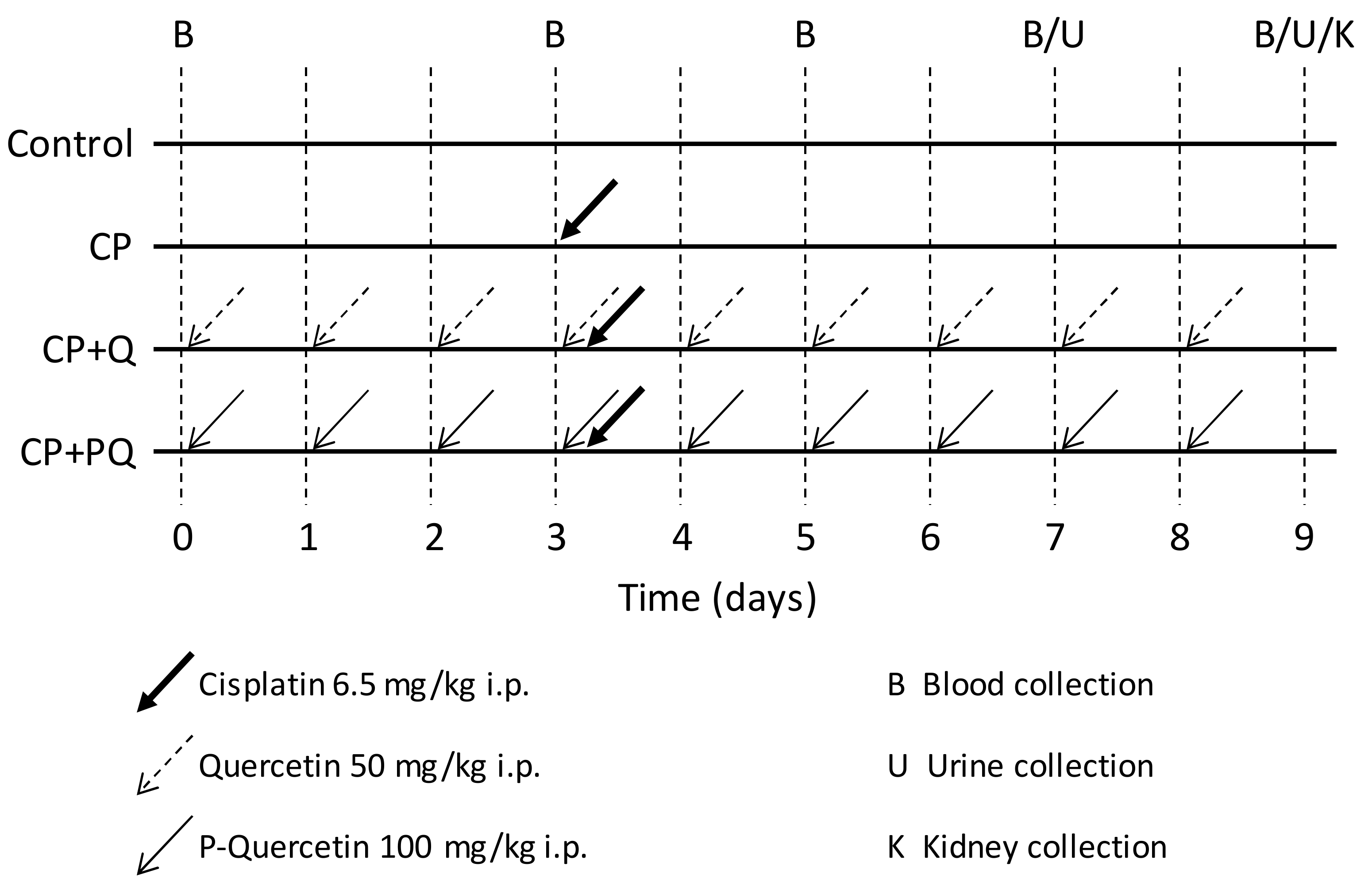
4.4. Nephroprotection Study
4.5. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AKI | Acute kidney injury |
| ANOVA | Analysis of variance |
| AUC | Area under the curve |
| AUC024 | Area under the partial curve |
| AUC0∞ | Area under the total curve |
| 𝐶max | Maximum drug concentration |
| ClCr | Creatinine clearance |
| Crpl Crur | Plasma creatinine Urinary creatinine |
| GFR | Glomerular filtration rate |
| i.p. | Intraperitoneal/intraperitoneally |
| KIM-1 | Kidney injury molecule 1 |
| MRT | Mean residence time |
| SEM | Standard error of the mean |
| t1/2 | Elimination half-life |
References
- Awdishu, L.; Mehta, R.L. The 6R’s of Drug Induced Nephrotoxicity. BMC Nephrol. 2017, 18, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perazella, M.A. Drug Use and Nephrotoxicity in the Intensive Care Unit. Kidney Int. 2012, 81, 1172–1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taber, S.S.; Mueller, B.A. Drug-Associated Renal Dysfunction. Crit. Care Clin. 2006, 22, 357–374, viii. [Google Scholar] [CrossRef]
- Huang, J.X.; Blaskovich, M.A.; Cooper, M.A. Cell- and Biomarker-Based Assays for Predicting Nephrotoxicity. Expert Opin. Drug Metab. Toxicol. 2014, 10, 1621–1635. [Google Scholar] [CrossRef] [PubMed]
- Volarevic, V.; Djokovic, B.; Jankovic, M.G.; Harrell, C.R.; Fellabaum, C.; Djonov, V.; Arsenijevic, N. Molecular Mechanisms of Cisplatin-Induced Nephrotoxicity: A Balance on the Knife Edge between Renoprotection and Tumor Toxicity. J. Biomed. Sci. 2019, 26, 25. [Google Scholar] [CrossRef] [Green Version]
- Hamroun, A.; Lenain, R.; Bigna, J.J.; Speyer, E.; Bui, L.; Chamley, P.; Pottier, N.; Cauffiez, C.; Dewaeles, E.; Dhalluin, X.; et al. Prevention of Cisplatin-Induced Acute Kidney Injury: A Systematic Review and Meta-Analysis. Drugs 2019, 79, 1567–1582. [Google Scholar] [CrossRef] [PubMed]
- Holditch, S.J.; Brown, C.N.; Lombardi, A.M.; Nguyen, K.N.; Edelstein, C.L. Recent Advances in Models, Mechanisms, Biomarkers, and Interventions in Cisplatin-Induced Acute Kidney Injury. Int. J. Mol. Sci. 2019, 20, 3011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.-Q.; Cai, G.-Y.; Wang, S.-Y.; Song, Y.-H.; Xia, Y.-Y.; Liang, S.; Wang, W.-L.; Nie, S.-S.; Feng, Z.; Chen, X.-M. The Characteristics and Risk Factors for Cisplatin-Induced Acute Kidney Injury in the Elderly. Clin. Risk Manag. 2018, 14, 1279–1285. [Google Scholar] [CrossRef] [Green Version]
- Ozkok, A.; Edelstein, C.L. Pathophysiology of Cisplatin-Induced Acute Kidney Injury. Biomed. Res. Int. 2014, 2014, 967826. [Google Scholar] [CrossRef]
- Kuhlmann, M.K.; Burkhardt, G.; Köhler, H. Insights into Potential Cellular Mechanisms of Cisplatin Nephrotoxicity and Their Clinical Application. Nephrol. Dial. Transpl. 1997, 12, 2478–2480. [Google Scholar] [CrossRef]
- Price, P.M.; Safirstein, R.L.; Megyesi, J. Protection of Renal Cells from Cisplatin Toxicity by Cell Cycle Inhibitors. Am. J. Physiol. Ren. Physiol. 2004, 286, F378–F384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karasawa, T.; Steyger, P.S. An Integrated View of Cisplatin-Induced Nephrotoxicity and Ototoxicity. Toxicol. Lett. 2015, 237, 219–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-González, P.D.; López-Hernández, F.J.; López-Novoa, J.M.; Morales, A.I. An Integrative View of the Pathophysiological Events Leading to Cisplatin Nephrotoxicity. Crit. Rev. Toxicol. 2011, 41, 803–821. [Google Scholar] [CrossRef] [PubMed]
- Gameiro, J.; Fonseca, J.A.; Marques, F.; Lopes, J.A. Management of Acute Kidney Injury Following Major Abdominal Surgery: A Contemporary Review. J. Clin. Med. 2020, 9, 2679. [Google Scholar] [CrossRef]
- Sancho-Martínez, S.M.; Prieto-García, L.; Prieto, M.; López-Novoa, J.M.; López-Hernández, F.J. Subcellular Targets of Cisplatin Cytotoxicity: An Integrated View. Pharmacol. Ther. 2012, 136, 35–55. [Google Scholar] [CrossRef]
- Sancho-Martínez, S.M.; Prieto-García, L.; Prieto, M.; Fuentes-Calvo, I.; López-Novoa, J.M.; Morales, A.I.; Martínez-Salgado, C.; López-Hernández, F.J. N-Acetylcysteine Transforms Necrosis into Apoptosis and Affords Tailored Protection from Cisplatin Cytotoxicity. Toxicol. Appl. Pharm. 2018, 349, 83–93. [Google Scholar] [CrossRef]
- Chirino, Y.I.; Pedraza-Chaverri, J. Role of Oxidative and Nitrosative Stress in Cisplatin-Induced Nephrotoxicity. Exp. Toxicol. Pathol. 2009, 61, 223–242. [Google Scholar] [CrossRef]
- McMahon, K.R.; Rassekh, S.R.; Schultz, K.R.; Blydt-Hansen, T.; Cuvelier, G.D.E.; Mammen, C.; Pinsk, M.; Carleton, B.C.; Tsuyuki, R.T.; Ross, C.J.D.; et al. Epidemiologic Characteristics of Acute Kidney Injury During Cisplatin Infusions in Children Treated for Cancer. JAMA Netw. Open 2020, 3, e203639. [Google Scholar] [CrossRef]
- Crona, D.J.; Faso, A.; Nishijima, T.F.; McGraw, K.A.; Galsky, M.D.; Milowsky, M.I. A Systematic Review of Strategies to Prevent Cisplatin-Induced Nephrotoxicity. Oncologist 2017, 22, 609–619. [Google Scholar] [CrossRef] [Green Version]
- Casanova, A.G.; Hernández-Sánchez, M.T.; López-Hernández, F.J.; Martínez-Salgado, C.; Prieto, M.; Vicente-Vicente, L.; Morales, A.I. Systematic Review and Meta-Analysis of the Efficacy of Clinically Tested Protectants of Cisplatin Nephrotoxicity. Eur. J. Clin. Pharm. 2020, 76, 23–33. [Google Scholar] [CrossRef]
- Casanova, A.G.; Hernández-Sánchez, M.T.; Martínez-Salgado, C.; Morales, A.I.; Vicente-Vicente, L.; López-Hernández, F.J. A Meta-Analysis of Preclinical Studies Using Antioxidants for the Prevention of Cisplatin Nephrotoxicity: Implications for Clinical Application. Crit. Rev. Toxicol. 2020, 50, 780–800. [Google Scholar] [CrossRef]
- Bubols, G.B.; da Rocha Vianna, D.; Medina-Remon, A.; von Poser, G.; Lamuela-Raventos, R.M.; Eifler-Lima, V.L.; Garcia, S.C. The Antioxidant Activity of Coumarins and Flavonoids. Mini Rev. Med. Chem. 2013, 13, 318–334. [Google Scholar] [CrossRef] [PubMed]
- Olas, B.; Bryś, M. Beer Components and Their Beneficial Effect on the Hemostasis and Cardiovascular Diseases—Truth or Falsehood. Food Chem. Toxicol. 2020, 146, 111782. [Google Scholar] [CrossRef] [PubMed]
- Almeida, A.F.; Borge, G.I.A.; Piskula, M.; Tudose, A.; Tudoreanu, L.; Valentová, K.; Williamson, G.; Santos, C.N. Bioavailability of Quercetin in Humans with a Focus on Interindividual Variation. Compr. Rev. Food Sci. Food Saf. 2018, 17, 714–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Gonzalez, P.D.; Lopez-Hernandez, F.J.; Perez-Barriocanal, F.; Morales, A.I.; Lopez-Novoa, J.M. Quercetin Reduces Cisplatin Nephrotoxicity in Rats without Compromising Its Anti-Tumour Activity. Nephrol. Dial. Transpl. 2011, 26, 3484–3495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-González, P.D.; López-Hernández, F.J.; Dueñas, M.; Prieto, M.; Sánchez-López, E.; Thomale, J.; Ruiz-Ortega, M.; López-Novoa, J.M.; Morales, A.I. Differential Effect of Quercetin on Cisplatin-Induced Toxicity in Kidney and Tumor Tissues. Food Chem. Toxicol. 2017, 107, 226–236. [Google Scholar] [CrossRef] [PubMed]
- Vicente-Vicente, L.; González-Calle, D.; Casanova, A.G.; Hernández-Sánchez, M.T.; Prieto, M.; Rama-Merchán, J.C.; Martín-Moreiras, J.; Martín-Herrero, F.; Sánchez, P.L.; López-Hernández, F.J.; et al. Quercetin, a Promising Clinical Candidate for The Prevention of Contrast-Induced Nephropathy. Int. J. Mol. Sci. 2019, 20, 4961. [Google Scholar] [CrossRef] [Green Version]
- Riva, A.; Ronchi, M.; Petrangolini, G.; Bosisio, S.; Allegrini, P. Improved Oral Absorption of Quercetin from Quercetin Phytosome®, a New Delivery System Based on Food Grade Lecithin. Eur. J. Drug Metab. Pharm. 2019, 44, 169–177. [Google Scholar] [CrossRef] [Green Version]
- Dabeek, W.M.; Marra, M.V. Dietary Quercetin and Kaempferol: Bioavailability and Potential Cardiovascular-Related Bioactivity in Humans. Nutrients 2019, 11, 2288. [Google Scholar] [CrossRef] [Green Version]
- Batrakova, E.V.; Kabanov, A.V. Pluronic Block Copolymers: Evolution of Drug Delivery Concept from Inert Nanocarriers to Biological Response Modifiers. J. Control. Release 2008, 130, 98–106. [Google Scholar] [CrossRef] [Green Version]
- Fraile, M.; Buratto, R.; Gómez, B.; Martín, Á.; Cocero, M.J. Enhanced Delivery of Quercetin by Encapsulation in Poloxamers by Supercritical Antisolvent Process. Ind. Eng. Chem. Res. 2014, 53, 4318–4327. [Google Scholar] [CrossRef]
- Nematbakhsh, M.; Ashrafi, F.; Nasri, H.; Talebi, A.; Pezeshki, Z.; Eshraghi, F.; Haghighi, M. A Model for Prediction of Cisplatin Induced Nephrotoxicity by Kidney Weight in Experimental Rats. J. Res. Med. Sci. 2013, 18, 370–373. [Google Scholar]
- Khwaja, A. KDIGO Clinical Practice Guidelines for Acute Kidney Injury. NEC 2012, 120, c179–c184. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A. Acute Kidney Injury Network: Report of an Initiative to Improve Outcomes in Acute Kidney Injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P. Acute Dialysis Quality Initiative workgroup Acute Renal Failure—Definition, Outcome Measures, Animal Models, Fluid Therapy and Information Technology Needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Corte, W.; Vanholder, R.; Dhondt, A.W.; De Waele, J.J.; Decruyenaere, J.; Danneels, C.; Claus, S.; Hoste, E.A.J. Serum Urea Concentration Is Probably Not Related to Outcome in ICU Patients with AKI and Renal Replacement Therapy. Nephrol. Dial. Transpl. 2011, 26, 3211–3218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casanova, A.; Vicente-Vicente, L.; Hernández-Sánchez, M.; Prieto, M.; Rihuete, M.; Ramis, L.; del Barco, E.; Cruz, J.; Ortiz, A.; Cruz-González, I.; et al. Urinary transferrin pre-emptively identifies the risk of renal damage posed by subclinical tubular alterations. Biomed. Pharmacother. 2019, 121, 109684. [Google Scholar] [CrossRef] [PubMed]
- Quiros, Y.; Ferreira, L.; Sancho-Martínez, S.M.; González-Buitrago, J.M.; López-Novoa, J.M.; López-Hernández, F.J. Sub-Nephrotoxic Doses of Gentamicin Predispose Animals to Developing Acute Kidney Injury and to Excrete Ganglioside M2 Activator Protein. Kidney Int. 2010, 78, 1006–1015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diskin, C.J. Creatinine and Glomerular Filtration Rate: Evolution of an Accommodation. Ann. Clin. Biochem. 2007, 44, 16–19. [Google Scholar] [CrossRef] [Green Version]
- Sancho-Martínez, S.M.; Blanco-Gozalo, V.; Quiros, Y.; Prieto-García, L.; Montero-Gómez, M.J.; Docherty, N.G.; Martínez-Salgado, C.; Morales, A.I.; López-Novoa, J.M.; López-Hernández, F.J. Impaired Tubular Reabsorption Is the Main Mechanism Explaining Increases in Urinary NGAL Excretion Following Acute Kidney Injury in Rats. Toxicol. Sci. 2020, 175, 75–86. [Google Scholar] [CrossRef]
- Bonventre, J.V. Kidney Injury Molecule-1 (KIM-1): A Urinary Biomarker and Much More. Nephrol. Dial. Transpl. 2009, 24, 3265–3268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinha, V.; Vence, L.M.; Salahudeen, A.K. Urinary Tubular Protein-Based Biomarkers in the Rodent Model of Cisplatin Nephrotoxicity: A Comparative Analysis of Serum Creatinine, Renal Histology, and Urinary KIM-1, NGAL, and NAG in the Initiation, Maintenance, and Recovery Phases of Acute Kidney Injury. J. Investig. Med. 2013, 61, 564–568. [Google Scholar] [CrossRef]
- Yuksel, Y.; Yuksel, R.; Yagmurca, M.; Haltas, H.; Erdamar, H.; Toktas, M.; Ozcan, O. Effects of Quercetin on Methotrexate-Induced Nephrotoxicity in Rats. Hum. Exp. Toxicol. 2017, 36, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Erboga, M.; Aktas, C.; Erboga, Z.F.; Donmez, Y.B.; Gurel, A. Quercetin Ameliorates Methotrexate-Induced Renal Damage, Apoptosis and Oxidative Stress in Rats. Ren. Fail. 2015, 37, 1492–1497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elbe, H.; Dogan, Z.; Taslidere, E.; Cetin, A.; Turkoz, Y. Beneficial Effects of Quercetin on Renal Injury and Oxidative Stress Caused by Ciprofloxacin in Rats: A Histological and Biochemical Study. Hum. Exp. Toxicol. 2016, 35, 276–281. [Google Scholar] [CrossRef]
- Nabavi, S.M.; Nabavi, S.F.; Habtemariam, S.; Moghaddam, A.H.; Latifi, A.M. Ameliorative Effects of Quercetin on Sodium Fluoride-Induced Oxidative Stress in Rat’s Kidney. Ren. Fail. 2012, 34, 901–906. [Google Scholar] [CrossRef] [Green Version]
- Shin, Y.J.; Kim, J.J.; Kim, Y.J.; Kim, W.H.; Park, E.Y.; Kim, I.Y.; Shin, H.-S.; Kim, K.S.; Lee, E.-K.; Chung, K.H.; et al. Protective Effects of Quercetin Against HgCl2-Induced Nephrotoxicity in Sprague-Dawley Rats. J. Med. Food 2015, 18, 524–534. [Google Scholar] [CrossRef]
- Morales, A.I.; Vicente-Sánchez, C.; Sandoval, J.M.S.; Egido, J.; Mayoral, P.; Arévalo, M.A.; Fernández-Tagarro, M.; López-Novoa, J.M.; Pérez-Barriocanal, F. Protective Effect of Quercetin on Experimental Chronic Cadmium Nephrotoxicity in Rats Is Based on Its Antioxidant Properties. Food Chem. Toxicol. 2006, 44, 2092–2100. [Google Scholar] [CrossRef]
- Gao, L.; Liu, G.; Wang, X.; Liu, F.; Xu, Y.; Ma, J. Preparation of a Chemically Stable Quercetin Formulation Using Nanosuspension Technology. Int. J. Pharm. 2011, 404, 231–237. [Google Scholar] [CrossRef]
- Lee, S.Y.; Lee, S.J.; Yim, D.G.; Hur, S.J. Changes in the Content and Bioavailability of Onion Quercetin and Grape Resveratrol During In Vitro Human Digestion. Foods 2020, 9, 694. [Google Scholar] [CrossRef]
- Ferry, D.R.; Smith, A.; Malkhandi, J.; Fyfe, D.W.; deTakats, P.G.; Anderson, D.; Baker, J.; Kerr, D.J. Phase I Clinical Trial of the Flavonoid Quercetin: Pharmacokinetics and Evidence for in Vivo Tyrosine Kinase Inhibition. Clin. Cancer Res. 1996, 2, 659–668. [Google Scholar] [PubMed]
- Wang, L.; Lin, S.Q.; He, Y.L.; Liu, G.; Wang, Z.Y. Protective Effects of Quercetin on Cadmium-Induced Cytotoxicity in Primary Cultures of Rat Proximal Tubular Cells. Biomed. Environ. Sci. 2013, 26, 258–267. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, M.R.; Nabavi, S.M.; Braidy, N.; Setzer, W.N.; Ahmed, T.; Nabavi, S.F. Quercetin and the Mitochondria: A Mechanistic View. Biotechnol. Adv. 2016, 34, 532–549. [Google Scholar] [CrossRef] [PubMed]
- Romero, J.C.; Lahera, V.; Salom, M.G.; Biondi, M.L. Role of the Endothelium-Dependent Relaxing Factor Nitric Oxide on Renal Function. J. Am. Soc. Nephrol. 1992, 2, 1371–1387. [Google Scholar]
- Kvam, F.I.; Ofstad, J.; Iversen, B.M. Role of Nitric Oxide in the Autoregulation of Renal Blood Flow and Glomerular Filtration Rate in Aging Spontaneously Hypertensive Rats. Kidney Blood Press. Res. 2000, 23, 376–384. [Google Scholar] [CrossRef]
- Galle, J.; Wanner, C. Impact of Nitric Oxide on Renal Hemodynamics and Glomerular Function: Modulation by Atherogenic Lipoproteins? Kidney Blood Press Res. 1996, 19, 2–15. [Google Scholar] [CrossRef]
- Ito, S.; Carretero, O.A.; Abe, K. Nitric Oxide in the Regulation of Renal Blood Flow. New Horiz. 1995, 3, 615–623. [Google Scholar]
- Lopez-Novoa, J.M.; Quiros, Y.; Vicente, L.; Morales, A.I.; Lopez-Hernandez, F.J. New Insights into the Mechanism of Aminoglycoside Nephrotoxicity: An Integrative Point of View. Kidney Int. 2011, 79, 33–45. [Google Scholar] [CrossRef] [Green Version]
- Suganya, N.; Dornadula, S.; Chatterjee, S.; Mohanram, R.K. Quercetin Improves Endothelial Function in Diabetic Rats through Inhibition of Endoplasmic Reticulum Stress-Mediated Oxidative Stress. Eur. J. Pharm. 2018, 819, 80–88. [Google Scholar] [CrossRef]
- Biegańska-Hensoldt, S.; Rosołowska-Huszcz, D. Polyphenols in Preventing Endothelial Dysfunction. Postepy Hig. Med. Dosw. 2017, 71, 227–235. [Google Scholar] [CrossRef]
- Choi, S.; Ryu, K.H.; Park, S.H.; Jun, J.Y.; Shin, B.C.; Chung, J.H.; Yeum, C.H. Direct Vascular Actions of Quercetin in Aorta from Renal Hypertensive Rats. Kidney Res. Clin. Pract. 2016, 35, 15–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eseberri, I.; Miranda, J.; Lasa, A.; Mosqueda-Solís, A.; González-Manzano, S.; Santos-Buelga, C.; Portillo, M.P. Effects of Quercetin Metabolites on Triglyceride Metabolism of 3T3-L1 Preadipocytes and Mature Adipocytes. Int. J. Mol. Sci. 2019, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Woude, H.; Boersma, M.G.; Vervoort, J.; Rietjens, I.M.C.M. Identification of 14 Quercetin Phase II Mono- and Mixed Conjugates and Their Formation by Rat and Human Phase II in Vitro Model Systems. Chem. Res. Toxicol. 2004, 17, 1520–1530. [Google Scholar] [CrossRef] [PubMed]
- Terao, J. Factors Modulating Bioavailability of Quercetin-Related Flavonoids and the Consequences of Their Vascular Function. Biochem. Pharmacol. 2017, 139, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, M. Ueber den Niederschlag welchen Pikrinsäure in normalen Harn erzeugt und über eine neue reaction des Kreatinins. Z. Physiol. Chem. 1886, 10, 391–400. [Google Scholar]
- Jung, D.; Biggs, H.; Erikson, J.; Ledyard, P.U. New Colorimetric reaction for end-point, continuous-flow, and kinetic measurement of urea. Clin. Chem. 1975, 8, 1136–1140. [Google Scholar] [CrossRef]
- Bradford, M.M. A Rapid and Sensitive Method for the Quantitation of Microgram Quantities of Protein Utilizing the Principle of Protein-Dye Binding. Anal. Biochem. 1976, 72, 248–254. [Google Scholar] [CrossRef]
- Sancho-Martínez, S.M.; Sánchez-Juanes, F.; Blanco-Gozalo, V.; Fontecha-Barriuso, M.; Prieto-García, L.; Fuentes-Calvo, I.; González-Buitrago, J.M.; Morales, A.I.; Martínez-Salgado, C.; Ramos-Barron, M.A.; et al. Urinary TCP1-Eta: A Cortical Damage Marker for the Pathophysiological Diagnosis and Prognosis of Acute Kidney Injury. Toxicol. Sci. 2020, 174, 3–15. [Google Scholar] [CrossRef]
- Miller, J. Using the Grubbs and Cochran Tests to Identify Outliers. Anal. Methods 2015, 7, 7948–7950. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formulation | AUC024 (µg·h/mL) | AUC0∞ (µg·h/mL) | MRT (h) | λ (h−1) | t1/2 (h) |
|---|---|---|---|---|---|
| Q | 13.43 | 44.20 | 73.81 | 1.3 × 10−2 | 55.31 |
| PQ | 57.70 | 133.70 | 45.82 | 2 × 10−2 | 34.66 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casanova, A.G.; Prieto, M.; Colino, C.I.; Gutiérrez-Millán, C.; Ruszkowska-Ciastek, B.; de Paz, E.; Martín, Á.; Morales, A.I.; López-Hernández, F.J. A Micellar Formulation of Quercetin Prevents Cisplatin Nephrotoxicity. Int. J. Mol. Sci. 2021, 22, 729. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22020729
Casanova AG, Prieto M, Colino CI, Gutiérrez-Millán C, Ruszkowska-Ciastek B, de Paz E, Martín Á, Morales AI, López-Hernández FJ. A Micellar Formulation of Quercetin Prevents Cisplatin Nephrotoxicity. International Journal of Molecular Sciences. 2021; 22(2):729. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22020729
Chicago/Turabian StyleCasanova, Alfredo G., Marta Prieto, Clara I. Colino, Carmen Gutiérrez-Millán, Barbara Ruszkowska-Ciastek, Esther de Paz, Ángel Martín, Ana I. Morales, and Francisco J. López-Hernández. 2021. "A Micellar Formulation of Quercetin Prevents Cisplatin Nephrotoxicity" International Journal of Molecular Sciences 22, no. 2: 729. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22020729