
The Pharmacology of Xenobiotics after Intracerebro Spinal Fluid Administration: Implications for the Treatment of Brain Tumors


Abstract
:1. Introduction
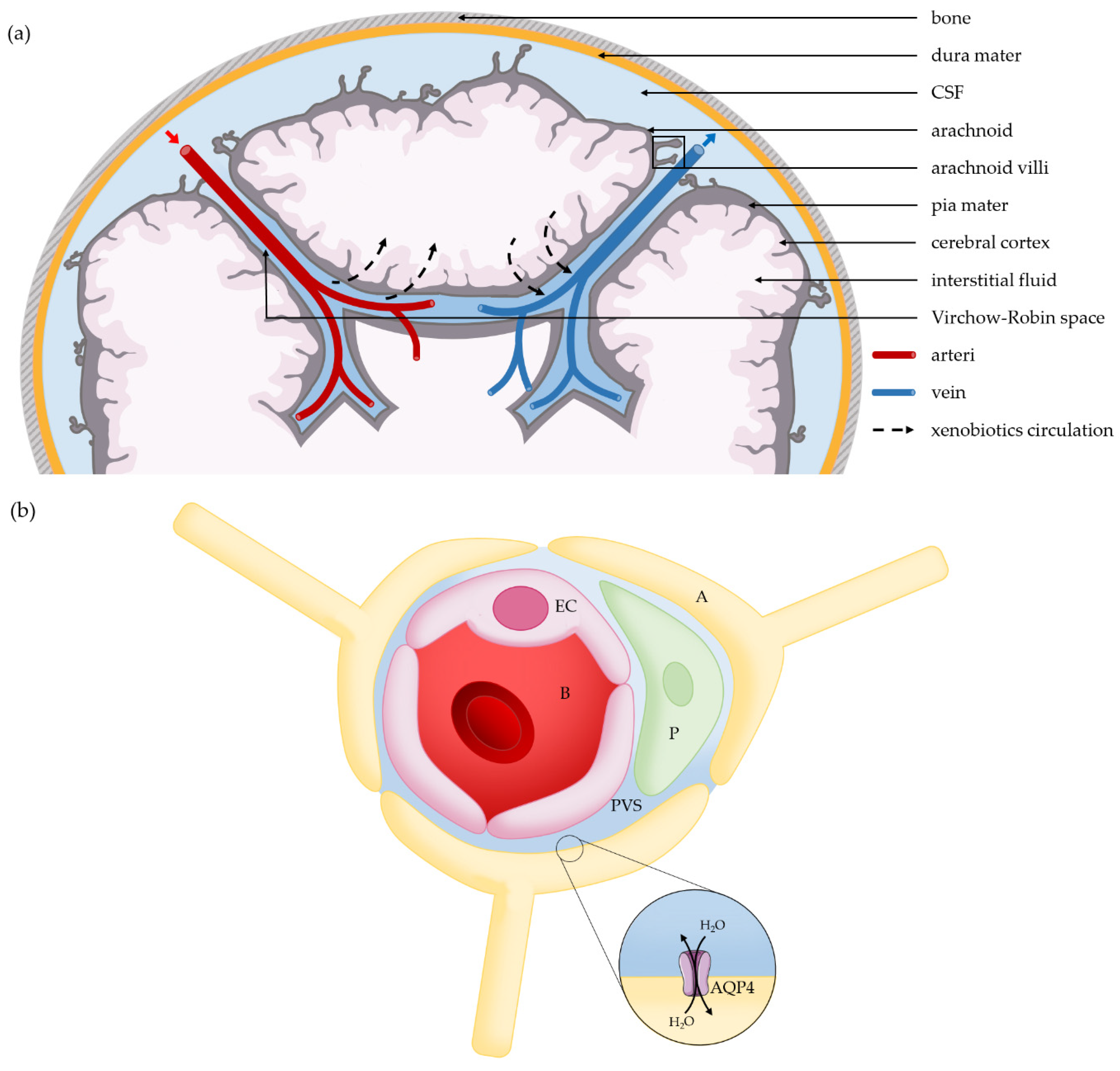
2. Turnover in the Glymphatic System
2.1. Transport through the Glymphatic System, Astrocyte Regulation Function
2.2. Drug Diffusion in the Extracellular Space of Brain
2.3. Clearance of the Cerebral Interstitial Fluid
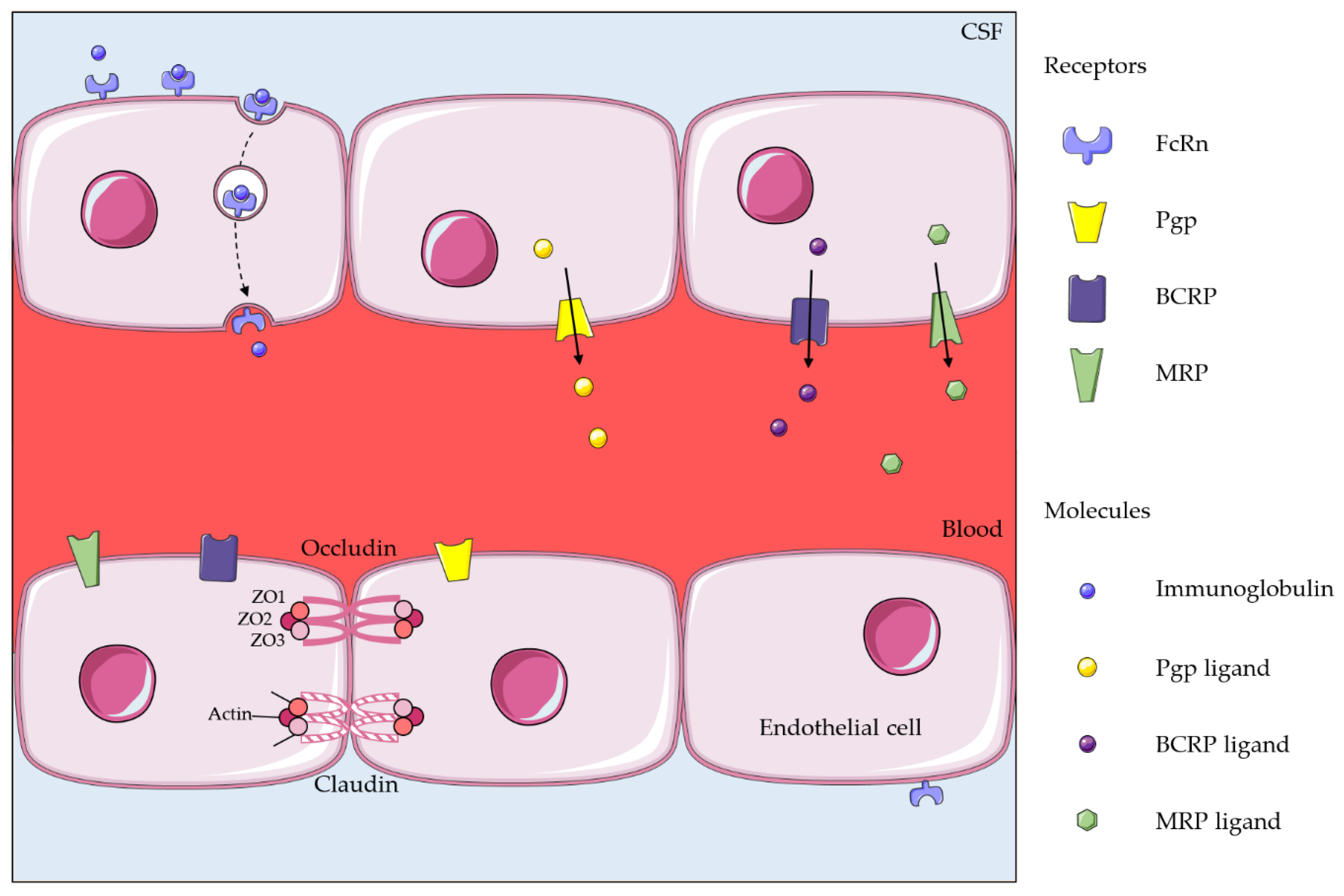
3. Efflux Systems and Drug Clearance
3.1. ABC Transporters
3.2. FcRn
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
Abbreviations
| ABC | ATP-Binding Cassette |
| BBB | Blood–Brain Barrier |
| BCRP | Breast Cancer Resistance Protein |
| CSF | Cerebrospinal Fluid |
| FcRn | Neonatal Fc Receptor |
| MRD | Multidrug Resistance Protein |
| Pgp | P-Glycoprotein |
References
- Pardridge, W.M. CNS drug design based on principles of blood-brain barrier transport. J. Neurochem. 1998, 70, 1781–1792. [Google Scholar] [CrossRef]
- Angeli, E.; Nguyen, T.T.; Janin, A.; Bousquet, G. How to Make Anticancer Drugs Cross the Blood-Brain Barrier to Treat Brain Metastases. Int. J. Mol. Sci. 2019, 21, 22. [Google Scholar] [CrossRef] [Green Version]
- Nayak, L.; Lee, E.Q.; Wen, P.Y. Epidemiology of brain metastases. Curr. Oncol. Rep. 2012, 14, 48–54. [Google Scholar] [CrossRef]
- Suh, J.H.; Kotecha, R.; Chao, S.T.; Ahluwalia, M.S.; Sahgal, A.; Chang, E.L. Current approaches to the management of brain metastases. Nat. Rev. Clin. Oncol. 2020, 17, 279–299. [Google Scholar] [CrossRef]
- Scoccianti, S.; Ricardi, U. Treatment of brain metastases: Review of phase III randomized controlled trials. Radiother. Oncol. 2012, 102, 168–179. [Google Scholar] [CrossRef] [Green Version]
- Tsukada, Y.; Fouad, A.; Pickren, J.W.; Lane, W.W. Central nervous system metastasis from breast carcinoma. Autopsy study. Cancer 1983, 52, 2349–2354. [Google Scholar] [CrossRef]
- Sampson, J.H.; Carter, J.H., Jr.; Friedman, A.H.; Seigler, H.F. Demographics, prognosis, and therapy in 702 patients with brain metastases from malignant melanoma. J. Neurosurg. 1998, 88, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Lowery, F.J.; Yu, D. Brain metastasis: Unique challenges and open opportunities. Biochim. Biophys. Acta Rev. Cancer 2017, 1867, 49–57. [Google Scholar] [CrossRef] [Green Version]
- Caroli, M.; Di Cristofori, A.; Lucarella, F.; Raneri, F.A.; Portaluri, F.; Gaini, S.M. Surgical brain metastases: Management and outcome related to prognostic indexes: A critical review of a ten-year series. ISRN Surg. 2011, 2011, 207103. [Google Scholar] [CrossRef]
- Ramakrishna, N.; Temin, S.; Chandarlapaty, S.; Crews, J.R.; Davidson, N.E.; Esteva, F.J.; Giordano, S.H.; Gonzalez-Angulo, A.M.; Kirshner, J.J.; Krop, I.; et al. Recommendations on disease management for patients with advanced human epidermal growth factor receptor 2-positive breast cancer and brain metastases: American Society of Clinical Oncology clinical practice guideline. J. Clin. Oncol. 2014, 32, 2100–2108. [Google Scholar] [CrossRef]
- Bonneau, C.; Paintaud, G.; Tredan, O.; Dubot, C.; Desvignes, C.; Dieras, V.; Taillibert, S.; Tresca, P.; Turbiez, I.; Li, J.; et al. Phase I feasibility study for intrathecal administration of trastuzumab in patients with HER2 positive breast carcinomatous meningitis. Eur. J. Cancer 2018, 95, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Stemmler, H.J.; Schmitt, M.; Harbeck, N.; Willems, A.; Bernhard, H.; Lassig, D.; Schoenberg, S.; Heinemann, V. Application of intrathecal trastuzumab (Herceptintrade mark) for treatment of meningeal carcinomatosis in HER2-overexpressing metastatic breast cancer. Oncol. Rep. 2006, 15, 1373–1377. [Google Scholar] [PubMed] [Green Version]
- Wolak, D.J.; Thorne, R.G. Diffusion of macromolecules in the brain: Implications for drug delivery. Mol. Pharm. 2013, 10, 1492–1504. [Google Scholar] [CrossRef] [PubMed]
- Jessen, N.A.; Munk, A.S.; Lundgaard, I.; Nedergaard, M. The Glymphatic System: A Beginner’s Guide. Neurochem. Res. 2015, 40, 2583–2599. [Google Scholar] [CrossRef] [Green Version]
- Cserr, H.F.; Ostrach, L.H. Bulk flow of interstitial fluid after intracranial injection of blue dextran 2000. Exp. Neurol. 1974, 45, 50–60. [Google Scholar] [CrossRef]
- Neuroscience Nedergaard, M. Garbage truck of the brain. Science 2013, 340, 1529–1530. [Google Scholar] [CrossRef] [Green Version]
- Iliff, J.J.; Wang, M.; Liao, Y.; Plogg, B.A.; Peng, W.; Gundersen, G.A.; Benveniste, H.; Vates, G.E.; Deane, R.; Goldman, S.A.; et al. A paravascular pathway facilitates CSF flow through the brain parenchyma and the clearance of interstitial solutes, including amyloid beta. Sci. Transl. Med. 2012, 4, 147ra111. [Google Scholar] [CrossRef] [Green Version]
- Mathiisen, T.M.; Lehre, K.P.; Danbolt, N.C.; Ottersen, O.P. The perivascular astroglial sheath provides a complete covering of the brain microvessels: An electron microscopic 3D reconstruction. Glia 2010, 58, 1094–1103. [Google Scholar] [CrossRef]
- Zhou, J.; Kong, H.; Hua, X.; Xiao, M.; Ding, J.; Hu, G. Altered blood-brain barrier integrity in adult aquaporin-4 knockout mice. Neuroreport 2008, 19, 1–5. [Google Scholar] [CrossRef]
- Kress, B.T.; Iliff, J.J.; Xia, M.; Wang, M.; Wei, H.S.; Zeppenfeld, D.; Xie, L.; Kang, H.; Xu, Q.; Liew, J.A.; et al. Impairment of paravascular clearance pathways in the aging brain. Ann. Neurol. 2014, 76, 845–861. [Google Scholar] [CrossRef]
- Schroth, G.; Klose, U. Cerebrospinal fluid flow. I. Physiology of cardiac-related pulsation. Neuroradiology 1992, 35, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Zieman, S.J.; Melenovsky, V.; Kass, D.A. Mechanisms, pathophysiology, and therapy of arterial stiffness. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 932–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, R.L.; Kassem, N.A.; Redzic, Z.B.; Chen, C.P.; Segal, M.B.; Preston, J.E. Age-related changes in choroid plexus and blood-cerebrospinal fluid barrier function in the sheep. Exp. Gerontol. 2009, 44, 289–296. [Google Scholar] [CrossRef] [Green Version]
- Fleischman, D.; Berdahl, J.P.; Zaydlarova, J.; Stinnett, S.; Fautsch, M.P.; Allingham, R.R. Cerebrospinal fluid pressure decreases with older age. PLoS ONE 2012, 7, e52664. [Google Scholar] [CrossRef]
- Xie, L.; Kang, H.; Xu, Q.; Chen, M.J.; Liao, Y.; Thiyagarajan, M.; O’Donnell, J.; Christensen, D.J.; Nicholson, C.; Iliff, J.J.; et al. Sleep drives metabolite clearance from the adult brain. Science 2013, 342, 373–377. [Google Scholar] [CrossRef] [Green Version]
- Szentistvanyi, I.; Patlak, C.S.; Ellis, R.A.; Cserr, H.F. Drainage of interstitial fluid from different regions of rat brain. Am. J. Physiol. 1984, 246, F835–F844. [Google Scholar] [CrossRef]
- Cserr, H.F.; Cooper, D.N.; Milhorat, T.H. Flow of cerebral interstitial fluid as indicated by the removal of extracellular markers from rat caudate nucleus. Exp. Eye Res. 1977, 25, 461–473. [Google Scholar] [CrossRef]
- Bradbury, M.W.; Cserr, H.F.; Westrop, R.J. Drainage of cerebral interstitial fluid into deep cervical lymph of the rabbit. Am. J. Physiol. 1981, 240, F329–F336. [Google Scholar] [CrossRef]
- Cserr, H.F.; Cooper, D.N.; Suri, P.K.; Patlak, C.S. Efflux of radiolabeled polyethylene glycols and albumin from rat brain. Am. J. Physiol. 1981, 240, F319–F328. [Google Scholar] [CrossRef]
- Zagouri, F.; Sergentanis, T.N.; Bartsch, R.; Berghoff, A.S.; Chrysikos, D.; de Azambuja, E.; Dimopoulos, M.A.; Preusser, M. Intrathecal administration of trastuzumab for the treatment of meningeal carcinomatosis in HER2-positive metastatic breast cancer: A systematic review and pooled analysis. Breast Cancer Res. Treat. 2013, 139, 13–22. [Google Scholar] [CrossRef]
- Hopkins, K.; Kemshead, J.T. Progress review: Intrathecal and intratumoral injection of radiolabelled monoclonal antibodies (MoAbs) for the treatment of central nervous system (CNS) malignancies. J. Drug. Target. 1993, 1, 175–183. [Google Scholar] [CrossRef]
- Schinkel, A.H.; Wagenaar, E.; Mol, C.A.; van Deemter, L. P-glycoprotein in the blood-brain barrier of mice influences the brain penetration and pharmacological activity of many drugs. J. Clin. Investig. 1996, 97, 2517–2524. [Google Scholar] [CrossRef]
- Zhang, Y.; Pardridge, W.M. Mediated efflux of IgG molecules from brain to blood across the blood-brain barrier. J. Neuroimmunol. 2001, 114, 168–172. [Google Scholar] [CrossRef]
- Abbott, N.J. Blood-brain barrier structure and function and the challenges for CNS drug delivery. J. Inherit. Metab. Dis. 2013, 36, 437–449. [Google Scholar] [CrossRef]
- Loscher, W.; Potschka, H. Drug resistance in brain diseases and the role of drug efflux transporters. Nat. Rev. Neurosci. 2005, 6, 591–602. [Google Scholar] [CrossRef]
- Robey, R.W.; Pluchino, K.M.; Hall, M.D.; Fojo, A.T.; Bates, S.E.; Gottesman, M.M. Revisiting the role of ABC transporters in multidrug-resistant cancer. Nat. Rev. Cancer 2018, 18, 452–464. [Google Scholar] [CrossRef]
- Loscher, W.; Potschka, H.; Sisodiya, S.M.; Vezzani, A. Drug Resistance in Epilepsy: Clinical Impact, Potential Mechanisms, and New Innovative Treatment Options. Pharmacol. Rev. 2020, 72, 606–638. [Google Scholar] [CrossRef]
- Dean, M.; Rzhetsky, A.; Allikmets, R. The human ATP-binding cassette (ABC) transporter superfamily. Genome Res. 2001, 11, 1156–1166. [Google Scholar] [CrossRef]
- Chen, Z.; Shi, T.; Zhang, L.; Zhu, P.; Deng, M.; Huang, C.; Hu, T.; Jiang, L.; Li, J. Mammalian drug efflux transporters of the ATP binding cassette (ABC) family in multidrug resistance: A review of the past decade. Cancer Lett. 2016, 370, 153–164. [Google Scholar] [CrossRef]
- Ng, W.F.; Sarangi, F.; Zastawny, R.L.; Veinot-Drebot, L.; Ling, V. Identification of members of the P-glycoprotein multigene family. Mol. Cell. Biol. 1989, 9, 1224–1232. [Google Scholar] [CrossRef] [Green Version]
- Ueda, K.; Cardarelli, C.; Gottesman, M.M.; Pastan, I. Expression of a full-length cDNA for the human “MDR1” gene confers resistance to colchicine, doxorubicin, and vinblastine. Proc. Natl. Acad. Sci. USA 1987, 84, 3004–3008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang-Wai, D.F.; Kajiji, S.; DiCapua, F.; de Graaf, D.; Roninson, I.B.; Gros, P. Human (MDR1) and mouse (mdr1, mdr3) P-glycoproteins can be distinguished by their respective drug resistance profiles and sensitivity to modulators. Biochemistry 1995, 34, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Schinkel, A.H.; Roelofs, E.M.; Borst, P. Characterization of the human MDR3 P-glycoprotein and its recognition by P-glycoprotein-specific monoclonal antibodies. Cancer Res. 1991, 51, 2628–2635. [Google Scholar]
- Devault, A.; Gros, P. Two members of the mouse mdr gene family confer multidrug resistance with overlapping but distinct drug specificities. Mol. Cell. Biol. 1990, 10, 1652–1663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juliano, R.L.; Ling, V. A surface glycoprotein modulating drug permeability in Chinese hamster ovary cell mutants. Biochim. Biophys. Acta 1976, 455, 152–162. [Google Scholar] [CrossRef]
- Fojo, A.T.; Ueda, K.; Slamon, D.J.; Poplack, D.G.; Gottesman, M.M.; Pastan, I. Expression of a multidrug-resistance gene in human tumors and tissues. Proc. Natl. Acad. Sci. USA 1987, 84, 265–269. [Google Scholar] [CrossRef] [Green Version]
- Thiebaut, F.; Tsuruo, T.; Hamada, H.; Gottesman, M.M.; Pastan, I.; Willingham, M.C. Cellular localization of the multidrug-resistance gene product P-glycoprotein in normal human tissues. Proc. Natl. Acad. Sci. USA 1987, 84, 7735–7738. [Google Scholar] [CrossRef] [Green Version]
- Bello-Reuss, E.; Ernest, S. Expression and function of P-glycoprotein in human mesangial cells. Am. J. Physiol. 1994, 267, C1351–C1358. [Google Scholar] [CrossRef]
- Cordon-Cardo, C.; O’Brien, J.P.; Casals, D.; Rittman-Grauer, L.; Biedler, J.L.; Melamed, M.R.; Bertino, J.R. Multidrug-resistance gene (P-glycoprotein) is expressed by endothelial cells at blood-brain barrier sites. Proc. Natl. Acad. Sci. USA 1989, 86, 695–698. [Google Scholar] [CrossRef] [Green Version]
- Stewart, P.A.; Beliveau, R.; Rogers, K.A. Cellular localization of P-glycoprotein in brain versus gonadal capillaries. J. Histochem. Cytochem. 1996, 44, 679–685. [Google Scholar] [CrossRef] [Green Version]
- Thiebaut, F.; Tsuruo, T.; Hamada, H.; Gottesman, M.M.; Pastan, I.; Willingham, M.C. Immunohistochemical localization in normal tissues of different epitopes in the multidrug transport protein P170: Evidence for localization in brain capillaries and crossreactivity of one antibody with a muscle protein. J. Histochem. Cytochem. 1989, 37, 159–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pardridge, W.M.; Golden, P.L.; Kang, Y.S.; Bickel, U. Brain microvascular and astrocyte localization of P-glycoprotein. J. Neurochem. 1997, 68, 1278–1285. [Google Scholar] [CrossRef] [PubMed]
- Jette, L.; Tetu, B.; Beliveau, R. High levels of P-glycoprotein detected in isolated brain capillaries. Biochim. Biophys. Acta 1993, 1150, 147–154. [Google Scholar] [CrossRef]
- Schinkel, A.H.; Smit, J.J.; van Tellingen, O.; Beijnen, J.H.; Wagenaar, E.; van Deemter, L.; Mol, C.A.; van der Valk, M.A.; Robanus-Maandag, E.C.; te Riele, H.P.; et al. Disruption of the mouse mdr1a P-glycoprotein gene leads to a deficiency in the blood-brain barrier and to increased sensitivity to drugs. Cell 1994, 77, 491–502. [Google Scholar] [CrossRef]
- Riordan, J.R.; Deuchars, K.; Kartner, N.; Alon, N.; Trent, J.; Ling, V. Amplification of P-glycoprotein genes in multidrug-resistant mammalian cell lines. Nature 1985, 316, 817–819. [Google Scholar] [CrossRef]
- Xu, D.; Knaust, E.; Pisa, P.; Palucka, K.; Lundeberg, J.; Arestrom, I.; Peterson, C.; Gruber, A. Levels of mdr1 and mrp mRNA in leukaemic cell populations from patients with acute myelocytic leukaemia are heterogenous and inversely correlated to cellular daunorubicin accumulation. Br. J. Haematol. 1996, 92, 847–854. [Google Scholar] [CrossRef]
- Chan, G.N.; Patel, R.; Cummins, C.L.; Bendayan, R. Induction of P-glycoprotein by antiretroviral drugs in human brain microvessel endothelial cells. Antimicrob. Agents Chemother. 2013, 57, 4481–4488. [Google Scholar] [CrossRef] [Green Version]
- Chan, G.N.; Saldivia, V.; Yang, Y.; Pang, H.; de Lannoy, I.; Bendayan, R. In vivo induction of P-glycoprotein expression at the mouse blood-brain barrier: An intracerebral microdialysis study. J. Neurochem. 2013, 127, 342–352. [Google Scholar] [CrossRef]
- Fallacara, A.L.; Zamperini, C.; Podolski-Renic, A.; Dinic, J.; Stankovic, T.; Stepanovic, M.; Mancini, A.; Rango, E.; Iovenitti, G.; Molinari, A.; et al. A New Strategy for Glioblastoma Treatment: In Vitro and In Vivo Preclinical Characterization of Si306, a Pyrazolo[3,4-d]Pyrimidine Dual Src/P-Glycoprotein Inhibitor. Cancers 2019, 11, 848. [Google Scholar] [CrossRef] [Green Version]
- Elkhayat, H.A.; Aly, R.H.; Elagouza, I.A.; El-Kabarity, R.H.; Galal, Y.I. Role of P-glycoprotein inhibitors in children with drug-resistant epilepsy. Acta Neurol. Scand. 2017, 136, 639–644. [Google Scholar] [CrossRef]
- Choo, E.F.; Kurnik, D.; Muszkat, M.; Ohkubo, T.; Shay, S.D.; Higginbotham, J.N.; Glaeser, H.; Kim, R.B.; Wood, A.J.; Wilkinson, G.R. Differential in vivo sensitivity to inhibition of P-glycoprotein located in lymphocytes, testes, and the blood-brain barrier. J. Pharmacol. Exp. Ther. 2006, 317, 1012–1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, C.C.; Bauer, M.; Karch, R.; Feurstein, T.; Kopp, S.; Chiba, P.; Kletter, K.; Loscher, W.; Muller, M.; Zeitlinger, M.; et al. A pilot study to assess the efficacy of tariquidar to inhibit P-glycoprotein at the human blood-brain barrier with (R)-11C-verapamil and PET. J. Nucl. Med. 2009, 50, 1954–1961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martins, E.; Silva, V.; Lemos, A.; Palmeira, A.; Puthongking, P.; Sousa, E.; Rocha-Pereira, C.; Ghanem, C.I.; Carmo, H.; Remiao, F.; et al. Newly Synthesized Oxygenated Xanthones as Potential P-Glycoprotein Activators: In Vitro, Ex Vivo, and In Silico Studies. Molecules 2019, 24, 707. [Google Scholar] [CrossRef] [Green Version]
- Sterz, K.; Mollmann, L.; Jacobs, A.; Baumert, D.; Wiese, M. Activators of P-glycoprotein: Structure-activity relationships and investigation of their mode of action. ChemMedChem 2009, 4, 1897–1911. [Google Scholar] [CrossRef]
- Cooray, H.C.; Blackmore, C.G.; Maskell, L.; Barrand, M.A. Localisation of breast cancer resistance protein in microvessel endothelium of human brain. Neuroreport 2002, 13, 2059–2063. [Google Scholar] [CrossRef] [PubMed]
- Eisenblatter, T.; Huwel, S.; Galla, H.J. Characterisation of the brain multidrug resistance protein (BMDP/ABCG2/BCRP) expressed at the blood-brain barrier. Brain Res. 2003, 971, 221–231. [Google Scholar] [CrossRef]
- Litman, T.; Brangi, M.; Hudson, E.; Fetsch, P.; Abati, A.; Ross, D.D.; Miyake, K.; Resau, J.H.; Bates, S.E. The multidrug-resistant phenotype associated with overexpression of the new ABC half-transporter, MXR (ABCG2). J. Cell Sci. 2000, 113 Pt 11, 2011–2021. [Google Scholar]
- Burger, H.; van Tol, H.; Boersma, A.W.; Brok, M.; Wiemer, E.A.; Stoter, G.; Nooter, K. Imatinib mesylate (STI571) is a substrate for the breast cancer resistance protein (BCRP)/ABCG2 drug pump. Blood 2004, 104, 2940–2942. [Google Scholar] [CrossRef]
- Yanase, K.; Tsukahara, S.; Asada, S.; Ishikawa, E.; Imai, Y.; Sugimoto, Y. Gefitinib reverses breast cancer resistance protein-mediated drug resistance. Mol. Cancer Ther. 2004, 3, 1119–1125. [Google Scholar]
- Agarwal, S.; Sane, R.; Ohlfest, J.R.; Elmquist, W.F. The role of the breast cancer resistance protein (ABCG2) in the distribution of sorafenib to the brain. J. Pharmacol. Exp. Ther. 2011, 336, 223–233. [Google Scholar] [CrossRef] [Green Version]
- Cisternino, S.; Mercier, C.; Bourasset, F.; Roux, F.; Scherrmann, J.M. Expression, up-regulation, and transport activity of the multidrug-resistance protein Abcg2 at the mouse blood-brain barrier. Cancer Res. 2004, 64, 3296–3301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durmus, S.; Xu, N.; Sparidans, R.W.; Wagenaar, E.; Beijnen, J.H.; Schinkel, A.H. P-glycoprotein (MDR1/ABCB1) and breast cancer resistance protein (BCRP/ABCG2) restrict brain accumulation of the JAK1/2 inhibitor, CYT387. Pharmacol. Res. 2013, 76, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Agarwal, S.; Elmquist, W.F. Brain efflux index to investigate the influence of active efflux on brain distribution of pemetrexed and methotrexate. Drug. Metab. Dispos. 2013, 41, 659–667. [Google Scholar] [CrossRef] [Green Version]
- Sane, R.; Agarwal, S.; Mittapalli, R.K.; Elmquist, W.F. Saturable active efflux by p-glycoprotein and breast cancer resistance protein at the blood-brain barrier leads to nonlinear distribution of elacridar to the central nervous system. J. Pharmacol. Exp. Ther. 2013, 345, 111–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kodaira, H.; Kusuhara, H.; Ushiki, J.; Fuse, E.; Sugiyama, Y. Kinetic analysis of the cooperation of P-glycoprotein (P-gp/Abcb1) and breast cancer resistance protein (Bcrp/Abcg2) in limiting the brain and testis penetration of erlotinib, flavopiridol, and mitoxantrone. J. Pharmacol. Exp. Ther. 2010, 333, 788–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poller, B.; Wagenaar, E.; Tang, S.C.; Schinkel, A.H. Double-transduced MDCKII cells to study human P-glycoprotein (ABCB1) and breast cancer resistance protein (ABCG2) interplay in drug transport across the blood-brain barrier. Mol. Pharm. 2011, 8, 571–582. [Google Scholar] [CrossRef] [PubMed]
- Nies, A.T.; Jedlitschky, G.; Konig, J.; Herold-Mende, C.; Steiner, H.H.; Schmitt, H.P.; Keppler, D. Expression and immunolocalization of the multidrug resistance proteins, MRP1-MRP6 (ABCC1-ABCC6), in human brain. Neuroscience 2004, 129, 349–360. [Google Scholar] [CrossRef]
- Soontornmalai, A.; Vlaming, M.L.; Fritschy, J.M. Differential, strain-specific cellular and subcellular distribution of multidrug transporters in murine choroid plexus and blood-brain barrier. Neuroscience 2006, 138, 159–169. [Google Scholar] [CrossRef]
- Zhang, Y.; Han, H.; Elmquist, W.F.; Miller, D.W. Expression of various multidrug resistance-associated protein (MRP) homologues in brain microvessel endothelial cells. Brain. Res. 2000, 876, 148–153. [Google Scholar] [CrossRef]
- Barrand, M.A.; Bagrij, T.; Neo, S.Y. Multidrug resistance-associated protein: A protein distinct from P-glycoprotein involved in cytotoxic drug expulsion. Gen. Pharmacol. 1997, 28, 639–645. [Google Scholar] [CrossRef]
- Seelig, A.; Blatter, X.L.; Wohnsland, F. Substrate recognition by P-glycoprotein and the multidrug resistance-associated protein MRP1: A comparison. Int. J. Clin. Pharmacol. Ther. 2000, 38, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Sparreboom, A.; van Asperen, J.; Mayer, U.; Schinkel, A.H.; Smit, J.W.; Meijer, D.K.; Borst, P.; Nooijen, W.J.; Beijnen, J.H.; van Tellingen, O. Limited oral bioavailability and active epithelial excretion of paclitaxel (Taxol) caused by P-glycoprotein in the intestine. Proc. Natl. Acad. Sci. USA 1997, 94, 2031–2035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, J.D.; Brinkhuis, R.F.; van Deemter, L.; Wijnholds, J.; Schinkel, A.H. Extensive contribution of the multidrug transporters P-glycoprotein and Mrp1 to basal drug resistance. Cancer Res. 2000, 60, 5761–5766. [Google Scholar] [PubMed]
- van Waterschoot, R.A.; Lagas, J.S.; Wagenaar, E.; Rosing, H.; Beijnen, J.H.; Schinkel, A.H. Individual and combined roles of CYP3A, P-glycoprotein (MDR1/ABCB1) and MRP2 (ABCC2) in the pharmacokinetics of docetaxel. Int. J. Cancer 2010, 127, 2959–2964. [Google Scholar] [CrossRef] [PubMed]
- Ballard, P.; Yates, J.W.; Yang, Z.; Kim, D.W.; Yang, J.C.; Cantarini, M.; Pickup, K.; Jordan, A.; Hickey, M.; Grist, M.; et al. Preclinical Comparison of Osimertinib with Other EGFR-TKIs in EGFR-Mutant NSCLC Brain Metastases Models, and Early Evidence of Clinical Brain Metastases Activity. Clin. Cancer Res. 2016, 22, 5130–5140. [Google Scholar] [CrossRef] [Green Version]
- Soria, J.C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Stephens, R.H.; O’Neill, C.A.; Warhurst, A.; Carlson, G.L.; Rowland, M.; Warhurst, G. Kinetic profiling of P-glycoprotein-mediated drug efflux in rat and human intestinal epithelia. J. Pharmacol. Exp. Ther. 2001, 296, 584–591. [Google Scholar]
- Richter, M.; Gyemant, N.; Molnar, J.; Hilgeroth, A. Comparative effects on intestinal absorption in situ by P-glycoprotein-modifying HIV protease inhibitors. Pharm. Res. 2004, 21, 1862–1866. [Google Scholar] [CrossRef]
- Hendrikse, N.H.; Franssen, E.J.; van der Graaf, W.T.; Vaalburg, W.; de Vries, E.G. Visualization of multidrug resistance in vivo. Eur. J. Nucl. Med. 1999, 26, 283–293. [Google Scholar] [CrossRef]
- Evers, R.; de Haas, M.; Sparidans, R.; Beijnen, J.; Wielinga, P.R.; Lankelma, J.; Borst, P. Vinblastine and sulfinpyrazone export by the multidrug resistance protein MRP2 is associated with glutathione export. Br. J. Cancer 2000, 83, 375–383. [Google Scholar] [CrossRef] [Green Version]
- Chu, X.Y.; Suzuki, H.; Ueda, K.; Kato, Y.; Akiyama, S.; Sugiyama, Y. Active efflux of CPT-11 and its metabolites in human KB-derived cell lines. J. Pharmacol. Exp. Ther. 1999, 288, 735–741. [Google Scholar] [PubMed]
- Hirohashi, T.; Suzuki, H.; Sugiyama, Y. Characterization of the transport properties of cloned rat multidrug resistance-associated protein 3 (MRP3). J. Biol. Chem. 1999, 274, 15181–15185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemper, E.M.; van Zandbergen, A.E.; Cleypool, C.; Mos, H.A.; Boogerd, W.; Beijnen, J.H.; van Tellingen, O. Increased penetration of paclitaxel into the brain by inhibition of P-Glycoprotein. Clin. Cancer Res. 2003, 9, 2849–2855. [Google Scholar] [PubMed]
- Kemper, E.M.; Verheij, M.; Boogerd, W.; Beijnen, J.H.; van Tellingen, O. Improved penetration of docetaxel into the brain by co-administration of inhibitors of P-glycoprotein. Eur. J. Cancer 2004, 40, 1269–1274. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, F.E.; O’Connor, R.M.; Clarke, G.; Dinan, T.G.; Griffin, B.T.; Cryan, J.F. P-glycoprotein inhibition increases the brain distribution and antidepressant-like activity of escitalopram in rodents. Neuropsychopharmacology 2013, 38, 2209–2219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ejsing, T.B.; Linnet, K. Influence of P-glycoprotein inhibition on the distribution of the tricyclic antidepressant nortriptyline over the blood-brain barrier. Hum. Psychopharmacol. 2005, 20, 149–153. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, F.E.; Clarke, G.; Fitzgerald, P.; Dinan, T.G.; Griffin, B.T.; Cryan, J.F. Inhibition of P-glycoprotein enhances transport of imipramine across the blood-brain barrier: Microdialysis studies in conscious freely moving rats. Br. J. Pharmacol. 2012, 166, 1333–1343. [Google Scholar] [CrossRef] [Green Version]
- Sadiq, M.W.; Uchida, Y.; Hoshi, Y.; Tachikawa, M.; Terasaki, T.; Hammarlund-Udenaes, M. Validation of a P-Glycoprotein (P-gp) Humanized Mouse Model by Integrating Selective Absolute Quantification of Human MDR1, Mouse Mdr1a and Mdr1b Protein Expressions with In Vivo Functional Analysis for Blood-Brain Barrier Transport. PLoS ONE 2015, 10, e0118638. [Google Scholar] [CrossRef] [Green Version]
- Kemper, E.M.; Cleypool, C.; Boogerd, W.; Beijnen, J.H.; van Tellingen, O. The influence of the P-glycoprotein inhibitor zosuquidar trihydrochloride (LY335979) on the brain penetration of paclitaxel in mice. Cancer Chemother. Pharmacol. 2004, 53, 173–178. [Google Scholar] [CrossRef]
- Dai, H.; Marbach, P.; Lemaire, M.; Hayes, M.; Elmquist, W.F. Distribution of STI-571 to the brain is limited by P-glycoprotein-mediated efflux. J. Pharmacol. Exp. Ther. 2003, 304, 1085–1092. [Google Scholar] [CrossRef] [Green Version]
- Tang, S.C.; Lagas, J.S.; Lankheet, N.A.; Poller, B.; Hillebrand, M.J.; Rosing, H.; Beijnen, J.H.; Schinkel, A.H. Brain accumulation of sunitinib is restricted by P-glycoprotein (ABCB1) and breast cancer resistance protein (ABCG2) and can be enhanced by oral elacridar and sunitinib coadministration. Int. J. Cancer 2012, 130, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.C.; Lankheet, N.A.; Poller, B.; Wagenaar, E.; Beijnen, J.H.; Schinkel, A.H. P-glycoprotein (ABCB1) and breast cancer resistance protein (ABCG2) restrict brain accumulation of the active sunitinib metabolite N-desethyl sunitinib. J. Pharmacol. Exp. Ther. 2012, 341, 164–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karbownik, A.; Sobanska, K.; Plotek, W.; Grabowski, T.; Klupczynska, A.; Plewa, S.; Grzeskowiak, E.; Szalek, E. The influence of the coadministration of the p-glycoprotein modulator elacridar on the pharmacokinetics of lapatinib and its distribution in the brain and cerebrospinal fluid. Investig. New Drugs 2020, 38, 574–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durmus, S.; Sparidans, R.W.; Wagenaar, E.; Beijnen, J.H.; Schinkel, A.H. Oral availability and brain penetration of the B-RAFV600E inhibitor vemurafenib can be enhanced by the P-GLYCOprotein (ABCB1) and breast cancer resistance protein (ABCG2) inhibitor elacridar. Mol. Pharm. 2012, 9, 3236–3245. [Google Scholar] [CrossRef]
- Tang, S.C.; Nguyen, L.N.; Sparidans, R.W.; Wagenaar, E.; Beijnen, J.H.; Schinkel, A.H. Increased oral availability and brain accumulation of the ALK inhibitor crizotinib by coadministration of the P-glycoprotein (ABCB1) and breast cancer resistance protein (ABCG2) inhibitor elacridar. Int. J. Cancer 2014, 134, 1484–1494. [Google Scholar] [CrossRef]
- Agarwal, S.; Sane, R.; Gallardo, J.L.; Ohlfest, J.R.; Elmquist, W.F. Distribution of gefitinib to the brain is limited by P-glycoprotein (ABCB1) and breast cancer resistance protein (ABCG2)-mediated active efflux. J. Pharmacol. Exp. Ther. 2010, 334, 147–155. [Google Scholar] [CrossRef] [Green Version]
- Drion, N.; Lemaire, M.; Lefauconnier, J.M.; Scherrmann, J.M. Role of P-glycoprotein in the blood-brain transport of colchicine and vinblastine. J. Neurochem. 1996, 67, 1688–1693. [Google Scholar] [CrossRef]
- Israel, E.J.; Taylor, S.; Wu, Z.; Mizoguchi, E.; Blumberg, R.S.; Bhan, A.; Simister, N.E. Expression of the neonatal Fc receptor, FcRn, on human intestinal epithelial cells. Immunology 1997, 92, 69–74. [Google Scholar] [CrossRef]
- Antohe, F.; Radulescu, L.; Gafencu, A.; Ghetie, V.; Simionescu, M. Expression of functionally active FcRn and the differentiated bidirectional transport of IgG in human placental endothelial cells. Hum. Immunol. 2001, 62, 93–105. [Google Scholar] [CrossRef]
- Leach, J.L.; Sedmak, D.D.; Osborne, J.M.; Rahill, B.; Lairmore, M.D.; Anderson, C.L. Isolation from human placenta of the IgG transporter, FcRn, and localization to the syncytiotrophoblast: Implications for maternal-fetal antibody transport. J. Immunol. 1996, 157, 3317–3322. [Google Scholar]
- Roopenian, D.C.; Akilesh, S. FcRn: The neonatal Fc receptor comes of age. Nat. Rev. Immunol. 2007, 7, 715–725. [Google Scholar] [CrossRef] [PubMed]
- Schlachetzki, F.; Zhu, C.; Pardridge, W.M. Expression of the neonatal Fc receptor (FcRn) at the blood-brain barrier. J. Neurochem. 2002, 81, 203–206. [Google Scholar] [CrossRef] [PubMed]
- Cooper, P.R.; Ciambrone, G.J.; Kliwinski, C.M.; Maze, E.; Johnson, L.; Li, Q.; Feng, Y.; Hornby, P.J. Efflux of monoclonal antibodies from rat brain by neonatal Fc receptor, FcRn. Brain Res. 2013, 1534, 13–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ober, R.J.; Martinez, C.; Vaccaro, C.; Zhou, J.; Ward, E.S. Visualizing the site and dynamics of IgG salvage by the MHC class I-related receptor, FcRn. J. Immunol. 2004, 172, 2021–2029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Liu, L. Modern methods for delivery of drugs across the blood-brain barrier. Adv. Drug. Deliv. Rev. 2012, 64, 640–665. [Google Scholar] [CrossRef]
- Rubenstein, J.L.; Fridlyand, J.; Abrey, L.; Shen, A.; Karch, J.; Wang, E.; Issa, S.; Damon, L.; Prados, M.; McDermott, M.; et al. Phase I study of intraventricular administration of rituximab in patients with recurrent CNS and intraocular lymphoma. J. Clin. Oncol. 2007, 25, 1350–1356. [Google Scholar] [CrossRef]
- Zylber-Katz, E.; Gomori, J.M.; Schwartz, A.; Lossos, A.; Bokstein, F.; Siegal, T. Pharmacokinetics of methotrexate in cerebrospinal fluid and serum after osmotic blood-brain barrier disruption in patients with brain lymphoma. Clin. Pharmacol. Ther. 2000, 67, 631–641. [Google Scholar] [CrossRef]
- Morikawa, N.; Mori, T.; Abe, T.; Kawashima, H.; Takeyama, M.; Hori, S. Pharmacokinetics of etoposide and carboplatin in cerebrospinal fluid and plasma during hyperosmotic disruption of the blood brain barrier and intraarterial combination chemotherapy. Biol. Pharm. Bull. 1999, 22, 428–431. [Google Scholar] [CrossRef] [Green Version]
- Brightman, M.W.; Hori, M.; Rapoport, S.I.; Reese, T.S.; Westergaard, E. Osmotic opening of tight junctions in cerebral endothelium. J. Comp. Neurol. 1973, 152, 317–325. [Google Scholar] [CrossRef]
- Knuutinen, O.; Kuitunen, H.; Alahuhta, S.; Isokangas, J.M.; Sonkajarvi, E.; Turpeenniemi-Hujanen, T.; Kuittinen, O. Case Report: Chemotherapy in Conjunction With Blood-Brain Barrier Disruption for a Patient With Germ Cell Tumor With Multiple Brain Metastases. Clin. Genitourin. Cancer 2018, 16, e993–e996. [Google Scholar] [CrossRef] [Green Version]
- Fortin, D.; Gendron, C.; Boudrias, M.; Garant, M.P. Enhanced chemotherapy delivery by intraarterial infusion and blood-brain barrier disruption in the treatment of cerebral metastasis. Cancer 2007, 109, 751–760. [Google Scholar] [CrossRef] [PubMed]
- Haluska, M.; Anthony, M.L. Osmotic blood-brain barrier modification for the treatment of malignant brain tumors. Clin. J. Oncol. Nurs. 2004, 8, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Toung, T.J.; Sapirstein, A.; Bhardwaj, A. Effect of duration of osmotherapy on blood-brain barrier disruption and regional cerebral edema after experimental stroke. J. Cereb. Blood Flow Metab. 2006, 26, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.D.; Liao, H.; Qin, T.; Zhang, L.; Wei, W.D.; Liang, J.Z.; Xu, F.; Dinglin, X.X.; Ma, S.X.; Chen, L.K. Blood-brain barrier permeability of gefitinib in patients with brain metastases from non-small-cell lung cancer before and during whole brain radiation therapy. Oncotarget 2015, 6, 8366–8376. [Google Scholar] [CrossRef]
- Pollack, I.F.; Stewart, C.F.; Kocak, M.; Poussaint, T.Y.; Broniscer, A.; Banerjee, A.; Douglas, J.G.; Kun, L.E.; Boyett, J.M.; Geyer, J.R. A phase II study of gefitinib and irradiation in children with newly diagnosed brainstem gliomas: A report from the Pediatric Brain Tumor Consortium. Neuro. Oncol. 2011, 13, 290–297. [Google Scholar] [CrossRef] [Green Version]
- Yang, F.Y.; Lin, G.L.; Horng, S.C.; Chang, T.K.; Wu, S.Y.; Wong, T.T.; Wang, H.E. Pulsed high-intensity focused ultrasound enhances the relative permeability of the blood-tumor barrier in a glioma-bearing rat model. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2011, 58, 964–970. [Google Scholar] [CrossRef]
- Liu, X.F.; Fawcett, J.R.; Thorne, R.G.; DeFor, T.A.; Frey, W.H. 2nd, Intranasal administration of insulin-like growth factor-I bypasses the blood-brain barrier and protects against focal cerebral ischemic damage. J. Neurol. Sci. 2001, 187, 91–97. [Google Scholar] [CrossRef]
- Nguyen, T.T.; Angeli, E.; Darrouzain, F.; Nguyen, Q.T.; Desvignes, C.; Rigal, M.; Nevine, O.; Nicolas, P.; Le, Q.V.; Winterman, S.; et al. A successful compartmental approach for the treatment of breast cancer brain metastases. Cancer Chemother. Pharmacol. 2019, 83, 573–580. [Google Scholar] [CrossRef]
- Bousquet, G.; Darrouzain, F.; de Bazelaire, C.; Ternant, D.; Barranger, E.; Winterman, S.; Madelaine-Chambin, I.; Thiebaut, J.B.; Polivka, M.; Paintaud, G.; et al. Intrathecal Trastuzumab Halts Progression of CNS Metastases in Breast Cancer. J. Clin. Oncol. 2016, 34, e151–e155. [Google Scholar] [CrossRef]
- Hosoda, T.; Katayama, M. Epidemiology and prognosis of ommaya reservoir-related bacterial meningitis in adult patients with leptomeningeal metastases from solid tumors: A 10-year retrospective single-center study in Japan. J. Infect. Chemother. 2020. [Google Scholar] [CrossRef]
- Bousquet, G.; Janin, A. Patient-Derived Xenograft: An Adjuvant Technology for the Treatment of Metastatic Disease. Pathobiology 2016, 83, 170–176. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| ABC Transporters (Corresponding Gene) | Substrates | Biological Effect | Reference |
|---|---|---|---|
| Pgp (ABCB1) | Anticancer drug | ||
| Paclitaxel | Microtubule polymer stabilizer | [82,83] | |
| Docetaxel | Microtubule-disruptive drug | [83,84] | |
| Vinblastine | Microtubule-disruptive drug | [83] | |
| Vincristine | Topoisomerase II inhibitor | [83] | |
| Mitoxantrone | Topoisomerase II inhibitor | [83] | |
| Etoposide (VP16) | Topoisomerase II inhibitor | [83] | |
| Doxorubicin | DNA intercalating agent | [83] | |
| Daunorubicin | DNA intercalating agent | [83] | |
| Afatinib | EGFR-TKI | [85] | |
| Erlotinib | EGFR-TKI | [85,86] | |
| Gefitinib | EGFR-TKI | [85,86] | |
| Osimertinib | EGFR-TKI | [85,86] | |
| Rociletinib | EGFR-TKI | [85] | |
| Anti-arrhythmic agent | |||
| Digoxin | Sodium pump inhibitor | [87] | |
| Anti-retroviral drug | |||
| Ritonavir | Protease inhibitor | [88] | |
| Saquinavir | Protease inhibitor | [88] | |
| Anti-inflammatory | |||
| Colchicine | Microtubule assembly inhibitor | [89] | |
| MRP (ABCC1) | Anticancer drug | ||
| Etoposide (VP16) | Topoisomerase II inhibitor | [83] | |
| Anti-inflammatory | |||
| Colchicine | Microtubule assembly inhibitor | [89] | |
| MRP (ABCC2) | Anticancer drug | ||
| Vinblastine | Microtubule-disruptive drug | [83,90] | |
| Uricosuric drug | |||
| Sulfinpyrazone | Degranulation of platelets inhibitor | [90] | |
| MRP (ABCC3) | Anticancer drug | ||
| Topotecan | Topoisomerase I inhibitor | [83] | |
| Camptotecin (CPT-11) | Topoisomerase I inhibitor | [91] | |
| Etoposide (VP16) | Topoisomerase II inhibitor | [83] | |
| Mitoxantrone | Topoisomerase II inhibitor | [83] | |
| Doxorubicin | DNA intercalating agent | [83] | |
| Daunorubicin | DNA intercalating agent | [83] | |
| Methotrexate | Dihydrofolate reductase inhibitor | [92] | |
| Pgp Inhibitor (Mechanism of Action) | Dose | Time Lapse before Drug Administration | Drug Tested | Dose | Time Lapse before Brain Analysis | Increased Brain Parenchyma Penetration | Species | Reference |
|---|---|---|---|---|---|---|---|---|
| Cyclosporin A (Calcineurin inhibitor) | Anticancer drug | |||||||
| 50 mg/kg p.o | 1 h | Paclitaxel | 10 mg/kg i.v | 24 h | 3 times | Mice | [93] | |
| 50 mg/kg p.o | 1 h | Docetaxel | 33 mg/kg i.v | 24 h | 2.3 times | Mice | [94] | |
| Antidepressant | ||||||||
| 20 mg/kg i.p | 1 h | Escitalopram | 0.1 mg/kg i.p | 30 min | >2 times | Mice | [95] | |
| 20 mg/kg i.p | 1 h | Escitalopram | 1 mg/kg i.p | 30 min | >1.75 times | Mice | [95] | |
| 200 mg/kg i.p | 1 h | Nortriptyline | 10 mg/kg i.p | 1 h | 1.5 times | Rats | [96] | |
| 25 mg/kg i.v | 30 min | Imipramine | 5 mg/kg i.v | 4 h | 1.84 times | Rats | [97] | |
| Opioid | ||||||||
| 100 mg/kg i.p | 1 h | Oxycodone | 1 mg/kg s.c | 2 h | 1.4 times | Mice | [98] | |
| Zosuquidar (MDR1 inhibitor) | Anticancer drug | |||||||
| 25–80 mg/kg p.o | 1 h | Paclitaxel | 10 mg/kg i.v | 24 h | 2.1–5.6 times | Mice | [99] | |
| 25 mg/kg i.p | 30 min | Imatinib | 25 mg/kg p.o | 1 h | 2–3 times | Mice | [100] | |
| Elacridar (MDR1 and BRCP inhibitor) | Anticancer drug | |||||||
| 25 mg/kg p.o | 2 h | Paclitaxel | 10 mg/kg i.v | 24 h | 5 times | Mice | [94] | |
| 25 mg/kg p.o | 2 h | Docetaxel | 33 mg/kg i.v | 24 h | 3.6 times | Mice | [93] | |
| 100 mg/kg p.o | 2 h | Sunitinib | 10 mg/kg p.o | 1 h | 12 times | Mice | [101] | |
| 100 mg/kg p.o | 15 min | N-desethyl sunitinib | 5 mg/kg i.v | 1 h | 3.3 times | Mice | [102] | |
| 5 mg/kg i.p | 30 min | Lapatinib | 100 mg/kg p.o | 24 h | 1.5 times | Rats | [103] | |
| 100 mg/kg p.o | 2 h 30 min | Vemurafenib | 5 mg/kg p.o | 4 h | 3–5 times | Mice | [104] | |
| 100 mg/kg p.o | 2 h | Crizotinib | 5 mg/kg p.o | 4 h | 2.2 times | Mice | [105] | |
| 10 mg/kg i.v | 30 min | Gefitinib | 25 mg/kg p.o | 2 h | 4 times | Mice | [106] | |
| Valspodar (MDR1 inhibitor) | Anticancer drug | |||||||
| 25 mg/kg p.o | 1 h | Paclitaxel | 10 mg/kg i.v | 24 h | 6.5 times | Mice | [93] | |
| 25 mg/kg p.o | 1 h | Docetaxel | 33 mg/kg i.v | 24 h | 3.5 times | Mice | [94] | |
| 10 mg/kg i.v | 5 min | Vinblastine | brain perfusion | 20 s | 9.1 times | Rats | [107] | |
| Anti-inflammatory | ||||||||
| 10 mg/kg i.v | 5 min | Colchicine | brain perfusion | 20 s | 8.4 times | Rats | [107] | |
| Verapamil (Calcium channel inhibitor) | Anticancer drug | |||||||
| 1 mg/kg i.v | 5 min | Vinblastine | brain perfusion | 20 s | 3.7 times | Rats | [107] | |
| Anti-inflammatory | ||||||||
| 1 mg/kg i.v | 5 min | Colchicine | brain perfusion | 20 s | 3.7 times | Rats | [107] | |
| Antidepressant | ||||||||
| 20 mg/kg i.p | 1 h 30 min | Imipramine | 5 mg/kg i.v | 4 h | 1.44 times | Rats | [97] | |
| Opioid | ||||||||
| 3 mg/kg i.p | 1 h | Oxycodone | 1 mg/kg s.c | 2 h | 1.3 times | Mice | [98] | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paris, J.; Angeli, E.; Bousquet, G. The Pharmacology of Xenobiotics after Intracerebro Spinal Fluid Administration: Implications for the Treatment of Brain Tumors. Int. J. Mol. Sci. 2021, 22, 1281. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22031281
Paris J, Angeli E, Bousquet G. The Pharmacology of Xenobiotics after Intracerebro Spinal Fluid Administration: Implications for the Treatment of Brain Tumors. International Journal of Molecular Sciences. 2021; 22(3):1281. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22031281
Chicago/Turabian StyleParis, Justine, Eurydice Angeli, and Guilhem Bousquet. 2021. "The Pharmacology of Xenobiotics after Intracerebro Spinal Fluid Administration: Implications for the Treatment of Brain Tumors" International Journal of Molecular Sciences 22, no. 3: 1281. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22031281