
Expression Pattern of iNOS, BCL-2 and MMP-9 in the Hip Synovium Tissue of Patients with Osteoarthritis

 , , and
, , and 
Abstract
:1. Introduction
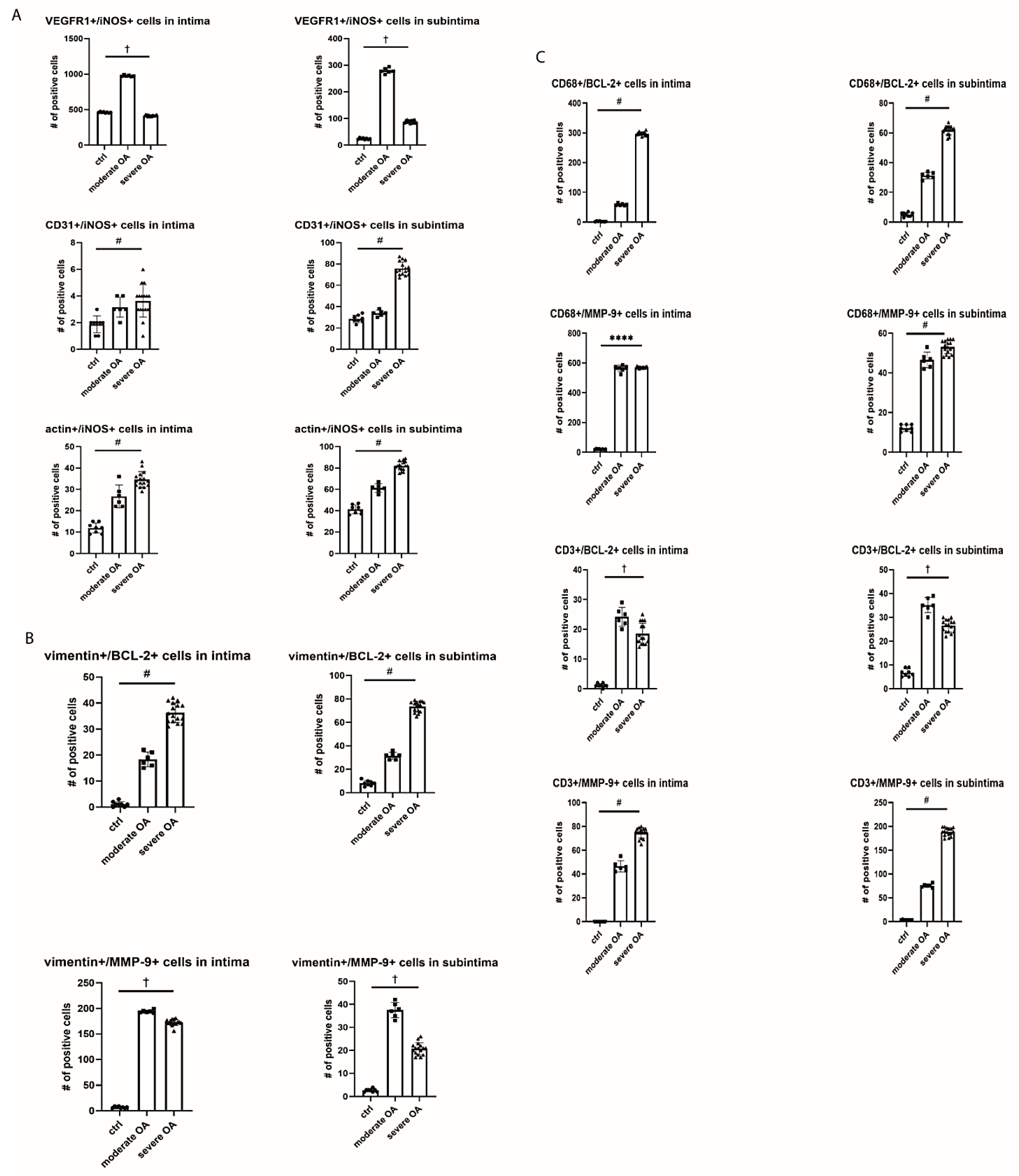
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Tissue Collection and Basic Staining Procedures
4.3. Double Immunofluorescence
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, D.; Shen, J.; Zhao, W.; Wang, T.; Han, L.; Hamilton, J.L.; Im, H.-J. Osteoarthritis: Toward a comprehensive understanding of pathological mechanism. Bone Res. 2017, 5, 16044. [Google Scholar] [CrossRef]
- Loeser, R.F.; Goldring, S.R.; Scanzello, C.R.; Goldring, M.B. Osteoarthritis: A disease of the joint as an organ. Arthritis Rheum. 2012, 64, 1697–1707. [Google Scholar] [CrossRef] [Green Version]
- Lawrence, R.C.; Felson, D.T.; Helmick, C.G.; Arnold, L.M.; Choi, H.; Deyo, R.A.; Gabriel, S.; Hirsch, R.; Hochberg, M.C.; Hunder, G.G.; et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part II. Arthritis Rheum. 2007, 58, 26–35. [Google Scholar] [CrossRef] [Green Version]
- Salmon, J.; Rat, A.-C.; Sellam, J.; Michel, M.; Eschard, J.; Guillemin, F.; Jolly, D.; Fautrel, B. Economic impact of lower-limb osteoarthritis worldwide: A systematic review of cost-of-illness studies. Osteoarthr. Cartil. 2016, 24, 1500–1508. [Google Scholar] [CrossRef] [Green Version]
- Solignac, M. COART France 2003 report on new socioeconomic data on osteoarthritis in France. Presse Médicale 2004, 33, 4–6. [Google Scholar]
- Jordan, J.M.; Helmick, C.G.; Renner, J.B.; Luta, G.; Dragomir, A.D.; Woodard, J.; Fang, F.; Schwartz, T.A.; Nelson, A.E.; Abbate, L.M.; et al. Prevalence of Hip Symptoms and Radiographic and Symptomatic Hip Osteoarthritis in African Americans and Caucasians: The Johnston County Osteoarthritis Project. J. Rheumatol. 2009, 36, 809–815. [Google Scholar] [CrossRef] [Green Version]
- Lahm, A.; Mrosek, E.; Spank, H.; Erggelet, C.; Kasch, R.; Esser, J.; Merk, H. Changes in content and synthesis of collagen types and proteoglycans in osteoarthritis of the knee joint and comparison of quantitative analysis with Photoshop-based image analysis. Arch. Orthop. Trauma Surg. 2009, 130, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Buckwalter, J.A.; Mankin, H.J.; Grodzinsky, A.J. Articular cartilage and osteoarthritis. Instr. Course Lect. 2005, 54, 465–480. [Google Scholar] [PubMed]
- Zhang, H.; Cai, D.; Bai, X.-C. Macrophages regulate the progression of osteoarthritis. Osteoarthr. Cartil. 2020, 28, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Man, G.S.; Mologhianu, G. Osteoarthritis pathogenesis—A complex process that involves the entire joint. J. Med. Life 2014, 7, 37–41. [Google Scholar] [PubMed]
- Goldring, M.B.; Otero, M.; Tsuchimochi, K.; Ijiri, K.; Li, Y. Defining the roles of inflammatory and anabolic cytokines in cartilage metabolism. Ann. Rheum. Dis. 2008, 67, iii75–iii82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Lange-Brokaar, B.; Ioan-Facsinay, A.; Van Osch, G.; Zuurmond, A.-M.; Schoones, J.; Toes, R.; Huizinga, T.W.J.; Kloppenburg, M. Synovial inflammation, immune cells and their cytokines in osteoarthritis: A review. Osteoarthr. Cartil. 2012, 20, 1484–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, M.D. The Normal Synovium. Open Rheumatol. J. 2011, 5, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Castrogiovanni, P.; Di Rosa, M.; Ravalli, S.; Castorina, A.; Guglielmino, C.; Imbesi, R.; Vecchio, M.; Drago, F.; Szychlinska, M.A.; Musumeci, G. Moderate Physical Activity as a Prevention Method for Knee Osteoarthritis and the Role of Synoviocytes as Biological Key. Int. J. Mol. Sci. 2019, 20, 511. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, K.; Tailor, P.; Leonard, C.; DiFrancesco, L.M.; Hart, D.A.; Matyas, J.; Frank, C.B.; Krawetz, R. Enumeration and Localization of Mesenchymal Progenitor Cells and Macrophages in Synovium from Normal Individuals and Patients with Pre-Osteoarthritis or Clinically Diagnosed Osteoarthritis. Int. J. Mol. Sci. 2017, 18, 774. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Lin, C.; Zeng, C.; Wang, Z.; Wang, H.; Lu, J.; Liu, X.; Shao, Y.; Zhao, C.; Pan, J.; et al. Synovial macrophage M1 polarisation exacerbates experimental osteoarthritis partially through R-spondin-2. Ann. Rheum. Dis. 2018, 77, 1524–1534. [Google Scholar] [CrossRef]
- Sellam, J.; Berenbaum, F. The role of synovitis in pathophysiology and clinical symptoms of osteoarthritis. Nat. Rev. Rheumatol. 2010, 6, 625–635. [Google Scholar] [CrossRef]
- Presle, N.; Pottie, P.; Dumond, H.; Guillaumé, C.; Lapicque, F.; Pallu, S.; Mainard, D.; Netter, P.; Terlain, B. Differential distribution of adipokines between serum and synovial fluid in patients with osteoarthritis. Contribution of joint tissues to their articular production. Osteoarthr. Cartil. 2006, 14, 690–695. [Google Scholar] [CrossRef] [Green Version]
- Abramson, S.B. Osteoarthritis and nitric oxide. Osteoarthr. Cartil. 2008, 16, S15–S20. [Google Scholar] [CrossRef] [Green Version]
- Loeuille, D.; Chary-Valckenaere, I.; Champigneulle, J.; Rat, A.-C.; Toussaint, F.; Pinzano-Watrin, A.; Goebel, J.C.; Mainard, D.; Blum, A.; Pourel, J.; et al. Macroscopic and microscopic features of synovial membrane inflammation in the osteoarthritic knee: Correlating magnetic resonance imaging findings with disease severity. Arthritis Rheum. 2005, 52, 3492–3501. [Google Scholar] [CrossRef] [Green Version]
- Berenbaum, F. Osteoarthritis as an inflammatory disease (osteoarthritis is not osteoarthrosis!). Osteoarthr. Cartil. 2013, 21, 16–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, D.; Fang, Y.; Tan, X.; Jiang, H.; Gong, X.; Wang, X.; Hong, W.; Tu, J.; Wei, W. The emerging role of fibroblast-like synoviocytes-mediated synovitis in osteoarthritis: An update. J. Cell. Mol. Med. 2020, 24, 9518–9532. [Google Scholar] [CrossRef]
- Pelletier, J.-P.; Martel-Pelletier, J.; Abramson, S.B. Osteoarthritis, an inflammatory disease: Potential implication for the selection of new therapeutic targets. Arthritis Rheum. 2001, 44, 1237–1247. [Google Scholar] [CrossRef]
- Ostojic, M.; Soljic, V.; Vukojević, K.; Dapic, T. Immunohistochemical characterization of early and advanced knee osteoarthritis by NF-κB and iNOS expression. J. Orthop. Res. 2017, 35, 1990–1997. [Google Scholar] [CrossRef] [Green Version]
- Rose, B.J.; Kooyman, D.L. A Tale of Two Joints: The Role of Matrix Metalloproteases in Cartilage Biology. Dis. Markers 2016, 2016, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maldonado, M.; Nam, J. The Role of Changes in Extracellular Matrix of Cartilage in the Presence of Inflammation on the Pathology of Osteoarthritis. BioMed Res. Int. 2013, 2013, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheleschi, S.; Gallo, I.; Barbarino, M.; Giannotti, S.; Mondanelli, N.; Giordano, A.; Tenti, S.; Fioravanti, A. MicroRNA Mediate Visfatin and Resistin Induction of Oxidative Stress in Human Osteoarthritic Synovial Fibroblasts Via NF-kappaB Pathway. Int. J. Mol. Sci. 2019, 20, 5200. [Google Scholar] [CrossRef] [Green Version]
- Hwang, H.S.; Kim, H.A. Chondrocyte Apoptosis in the Pathogenesis of Osteoarthritis. Int. J. Mol. Sci. 2015, 16, 26035–26054. [Google Scholar] [CrossRef]
- Ayral, X.; Pickering, E.; Woodworth, T.; MacKillop, N.; Dougados, M. Synovitis: A potential predictive factor of structural progression of medial tibiofemoral knee osteoarthritis—Results of a 1 year longitudinal arthroscopic study in 422 patients. Osteoarthr. Cartil. 2005, 13, 361–367. [Google Scholar] [CrossRef] [Green Version]
- Torres, L.; Dunlop, D.; Peterfy, C.; Guermazi, A.; Prasad, P.; Hayes, K.; Song, J.; Cahue, S.; Chang, A.; Marshall, M.; et al. The relationship between specific tissue lesions and pain severity in persons with knee osteoarthritis. Osteoarthr. Cartil. 2006, 14, 1033–1040. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, S.; Skwara, A.; Bloch, M.; Dankbar, B. Differential induction and regulation of matrix metalloproteinases in osteoarthritic tissue and fluid synovial fibroblasts. Osteoarthr. Cartil. 2004, 12, 409–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.-S.; Luo, W.; Zhu, S.-A.; Lei, G. T Cells in Osteoarthritis: Alterations and Beyond. Front. Immunol. 2017, 8, 356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Revell, P.A.; Mayston, V.; Lalor, P.; Mapp, P. The synovial membrane in osteoarthritis: A histological study including the characterisation of the cellular infiltrate present in inflammatory osteoarthritis using monoclonal antibodies. Ann. Rheum. Dis. 1988, 47, 300–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakkas, L.I.; Scanzello, C.; Johanson, N.; Burkholder, J.; Mitra, A.; Salgame, P.; Katsetos, C.D.; Platsoucas, C.D. T Cells and T-Cell Cytokine Transcripts in the Synovial Membrane in Patients with Osteoarthritis. Clin. Diagn. Lab. Immunol. 1998, 5, 430–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Favero, M.; El-Hadi, H.; Belluzzi, E.; Granzotto, M.; Porzionato, A.; Sarasin, G.; Rambaldo, A.; Iacobellis, C.; Cigolotti, A.; Fontanella, C.G.; et al. Infrapatellar fat pad features in osteoarthritis: A histopathological and molecular study. Rheumatology 2017, 56, 1784–1793. [Google Scholar] [CrossRef] [Green Version]
- Haynes, M.K.; Hume, E.L.; Smith, J.B. Phenotypic Characterization of Inflammatory Cells from Osteoarthritic Synovium and Synovial Fluids. Clin. Immunol. 2002, 105, 315–325. [Google Scholar] [CrossRef]
- Pessler, F.; Chen, L.X.; Dai, L.; Gomez-Vaquero, C.; Diaz-Torné, C.; Paessler, M.E.; Scanzello, C.; Cakir, N.; Einhorn, E.; Schumacher, H.R. A histomorphometric analysis of synovial biopsies from individuals with Gulf War Veterans’ Illness and joint pain compared to normal and osteoarthritis synovium. Clin. Rheumatol. 2008, 27, 1127–1134. [Google Scholar] [CrossRef]
- Mapp, P.I.; Walsh, D.A. Mechanisms and targets of angiogenesis and nerve growth in osteoarthritis. Nat. Rev. Rheumatol. 2012, 8, 390–398. [Google Scholar] [CrossRef]
- Krenn, V.; Morawietz, L.; Häupl, T.; Neidel, J.; Petersen, I.; König, A. Grading of Chronic Synovitis—A Histopathological Grading System for Molecular and Diagnostic Pathology. Pathol.-Res. Pr. 2002, 198, 317–325. [Google Scholar] [CrossRef]
- Haywood, L.; McWilliams, D.F.; Pearson, C.I.; Gill, S.E.; Ganesan, A.; Wilson, D.; Walsh, D.A. Inflammation and angiogenesis in osteoarthritis. Arthritis Rheum. 2003, 48, 2173–2177. [Google Scholar] [CrossRef]
- Sakkas, L.I.; Platsoucas, C.D. The role of T cells in the pathogenesis of osteoarthritis. Arthritis Rheum. 2007, 56, 409–424. [Google Scholar] [CrossRef] [PubMed]
- Perlman, H.; Georganas, C.; Pagliari, L.J.; Koch, A.E.; Haines, K.; Pope, R.M. Bcl-2 expression in synovial fibroblasts is essential for maintaining mitochondrial homeostasis and cell viability. J. Immunol. 2000, 164, 5227–5235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altman, R.; Alarcón, G.; Appelrouth, D.; Bloch, D.; Borenstein, D.; Brandt, K.; Brown, C.; Cooke, T.D.; Daniel, W.; Feldman, D.; et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hip. Arthritis Rheum. 1991, 34, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Vukojevic, K.; Skobic, H.; Saraga-Babic, M. Proliferation and differentiation of glial and neuronal progenitors in the development of human spinal ganglia. Differentiation 2009, 78, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Jurić, M.; Zeitler, J.; Vukojević, K.; Bočina, I.; Grobe, M.; Kretzschmar, G.; Saraga-Babić, M.; Filipović, N. Expression of Connexins 37, 43 and 45 in Developing Human Spinal Cord and Ganglia. Int. J. Mol. Sci. 2020, 21, 9356. [Google Scholar] [CrossRef]
- Kosovic, I.; Filipović, N.; Benzon, B.; Bočina, I.; Durdov, M.G.; Vukojević, K.; Saraga, M.; Saraga-Babić, M. Connexin Signaling in the Juxtaglomerular Apparatus (JGA) of Developing, Postnatal Healthy and Nephrotic Human Kidneys. Int. J. Mol. Sci. 2020, 21, 8349. [Google Scholar] [CrossRef]
- Urlić, M.; Urlić, I.; Urlić, H.; Mašek, T.; Benzon, B.; Vitlov Uljević, M.; Vukojevic, K.; Filipovic, N. Effects of Different n6/n3 PUFAs Dietary Ratio on Cardiac Diabetic Neuropathy. Nutrients 2020, 12, 2761. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Controls | Moderate OA | Severe OA | * p Value | |
|---|---|---|---|---|
| Age (median ± IQR, years) | 73 (72.25–76.75) | 72 (63.5–75.5) | 72 (67–77) | 0.884 |
| BMI (median ± IQR, kg/m2) | 25.67 (23.83–26.8) | 24.9 (23.28–25.88) | 26.9 (25.4–29.53) | 0.055 |
| K-L grade (median ± IQR) | 0.5 (0–1) | 2 (2–2) | 4 (3–4) | ˂0.0001 |
| Krenn score (median ± IQR) | 0 (0–0) | 6.5 (5.7–9) | 9 (7–9) | ˂0.0001 |
| OARSI (median ± IQR) | 1 (0.25–1) | 3 (1.5–4.5) | 2.5 (2–4.7) | 0.0005 |
| HHS (median ± IQR) | – | 48.9 (43.8–56.9) | 41 (33.18–49.7) | 0.271 |
| VAS (median ± IQR) | – | 6 (4.5–6.7) | 6 (5–7) | 0.781 |
| Total WOMAC (median ± IQR) | – | 46.1 (40–57.4) | 47.3 (36.1–55.3) | 0.917 |
| Disease Severity | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Control | Moderate OA | Severe OA | |||||||
| α | β | R2 | α | β | R2 | α | β | R2 | |
| Age (years) | |||||||||
| iNOS intima | 0 | 727.3 (692.9–761.6) | 0 | 556.6 (446.2–667) | 3003 (2212–3793) | 98% * | 372.7 (319.3–426.1) | 670.2 (220–1120) | 94% * |
| iNOS subintima | 0 | 59 (49.3–68.7) | 0 | supplementary Figure S1 | 7464 (7023–7904) | 99% * | 67.45 (53.85–81.04) | –154.9 (–269.5–0) | 89% * |
| BCL-2 intima | 0 | 3110 (2769–3451) | 0 | 0 | 3504 (3108–3900) | 0 | 177.2 (56.26–298.1) | 2022 (1003–3041) | 41% * |
| BCL-2 subintima | 0 | 4134 (3845–4423) | 0 | 0 | 4460 (4230–4689) | 0 | 0 | 7194 (6762–7626) | 0 |
| MMP-9 intima | 0 | 261 (234–288) | 0 | 0 | 7223 (7043–7404) | 0 | 0 | 7465 (7292–7638) | 0 |
| MMP-9 subintima | 0 | 33.88 (23.42–44.33) | 0 | 0 | 3252 (2652–3852) | 0 | 0 | 2184 (1304–3065) | 0 |
| Antibodies | Diagnosis | ||
|---|---|---|---|
| Moderate OA | Severe OA | Control | |
| iNOS | +++ | ++ | + |
| BCL-2 | ++ | +++ | ++ |
| MMP-9 | +++ | +++ | + |
| Antibodies | Host | Dilution | Structures Identified by Antibodies | Source |
|---|---|---|---|---|
| ab59348 (polyclonal antibody) | Rabbit | 1:500 | BCL-2 | Abcam (UK) |
| sc-651 (monoclonal antibody) | Rabbit | 1:200 | iNOS | Santacruz Biotechnology (Santa Cruz, CA, USA) |
| A0150 (polyclonal antibody) | Rabbit | 1:100 | MMP-9 | DAKO (Gloustrup, Denmark) |
| M0823 (monoclonal antibody) | Mouse | 1:20 | CD31 (endothelial cells of blood vessels) | DAKO (Gloustrup, Denmark) |
| M0851 (monoclonal antibody) | Mouse | 1:40 | Actin (smooth muscle cells of blood vessels) | DAKO (Gloustrup, Denmark) |
| ab212369 (monoclonal antibody) | Mouse | VEGFR1 | Abcam (UK) | |
| M0725 (monoclonal antibody) | Mouse | 1:50 | Vimentin (fibroblasts) | DAKO (Gloustrup, Denmark) |
| M0876 (monoclonal antibody) | Mouse | 1:75 | CD68 (macrophages) | DAKO (Gloustrup, Denmark) |
| M7254 (monoclonal antibody) | Mouse | 1:50 | CD3 (lymphocytes) | DAKO (Gloustrup, Denmark) |
| Rhodamine Goat AP124R | Mouse | 1:100 | Secondary antibody | MerckMillipore (Billerica, MA, USA) |
| Fluorescein Goat AP132F | Rabbit | 1:100 | Secondary antibody | MerckMillipore (Billerica, MA, USA) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caric, D.; Zekic Tomas, S.; Filipovic, N.; Soljic, V.; Benzon, B.; Glumac, S.; Rakovac, I.; Vukojevic, K. Expression Pattern of iNOS, BCL-2 and MMP-9 in the Hip Synovium Tissue of Patients with Osteoarthritis. Int. J. Mol. Sci. 2021, 22, 1489. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22031489
Caric D, Zekic Tomas S, Filipovic N, Soljic V, Benzon B, Glumac S, Rakovac I, Vukojevic K. Expression Pattern of iNOS, BCL-2 and MMP-9 in the Hip Synovium Tissue of Patients with Osteoarthritis. International Journal of Molecular Sciences. 2021; 22(3):1489. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22031489
Chicago/Turabian StyleCaric, Davor, Sandra Zekic Tomas, Natalija Filipovic, Violeta Soljic, Benjamin Benzon, Sandro Glumac, Ivan Rakovac, and Katarina Vukojevic. 2021. "Expression Pattern of iNOS, BCL-2 and MMP-9 in the Hip Synovium Tissue of Patients with Osteoarthritis" International Journal of Molecular Sciences 22, no. 3: 1489. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22031489