
The Effect of Far-Infrared Therapy on the Peritoneal Expression of Glucose Degradation Products in Diabetic Patients on Peritoneal Dialysis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
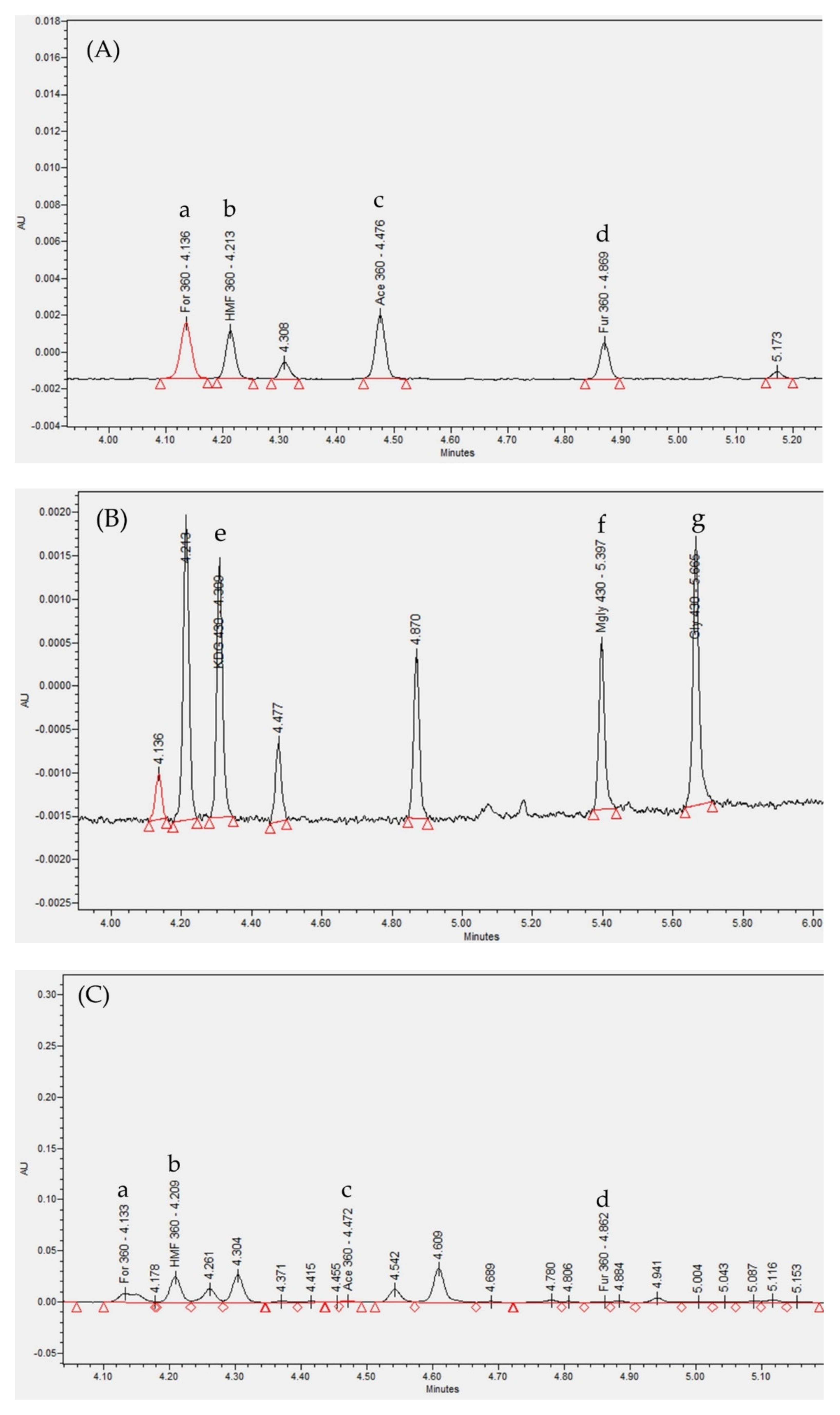
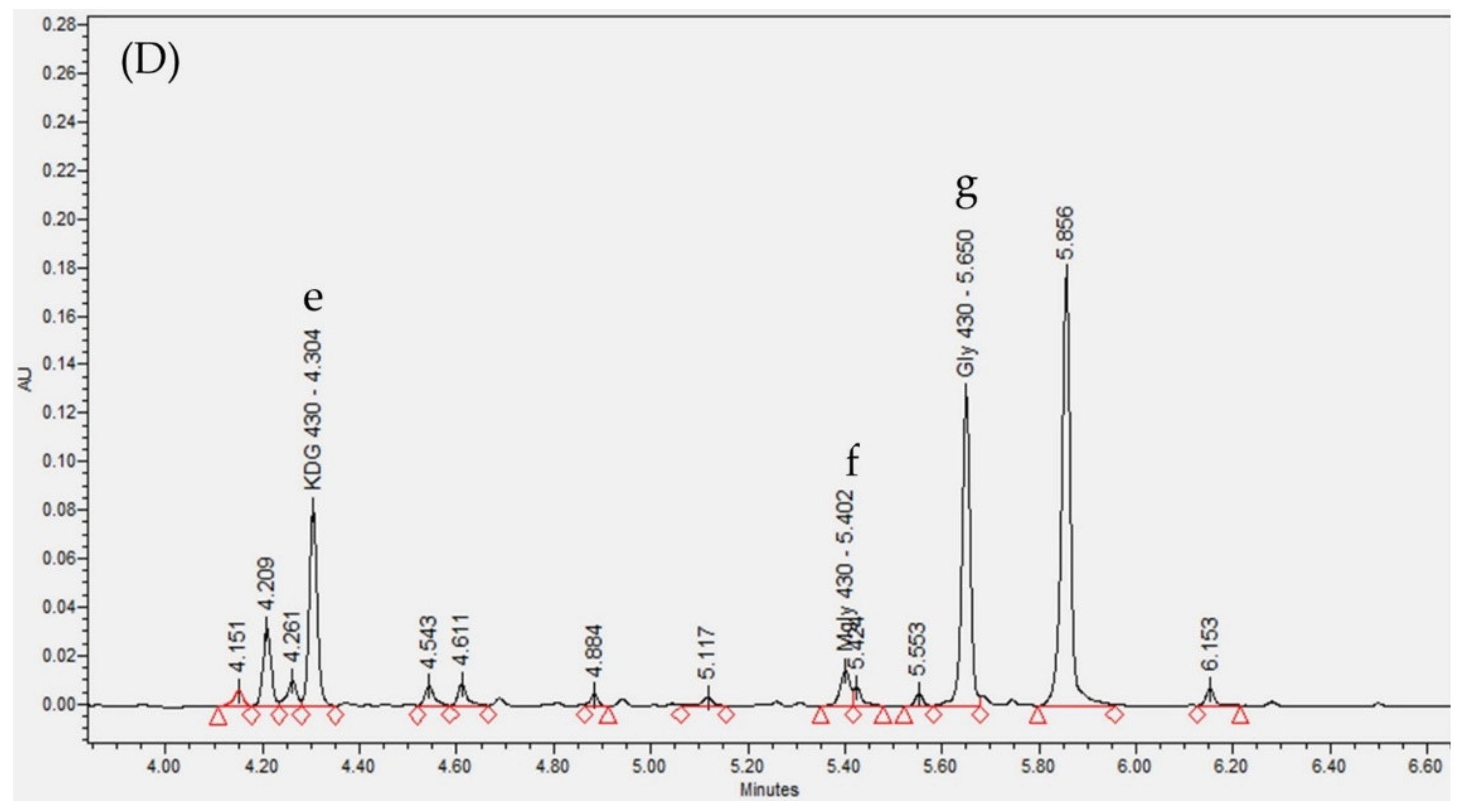
2.2. Determination of GDPs
2.3. Effect of FIR Therapy
2.3.1. Effect of FIR Therapy on Dialysate GDP Concentration, Peritoneal Function, and Serum Biochemical Parameters
2.3.2. Effect of FIR Therapy on Dialysate GDP Concentrations, Peritoneal Function, and Serum Biochemical Parameters in DM and non-DM Patients
3. Discussion
4. Materials and Methods
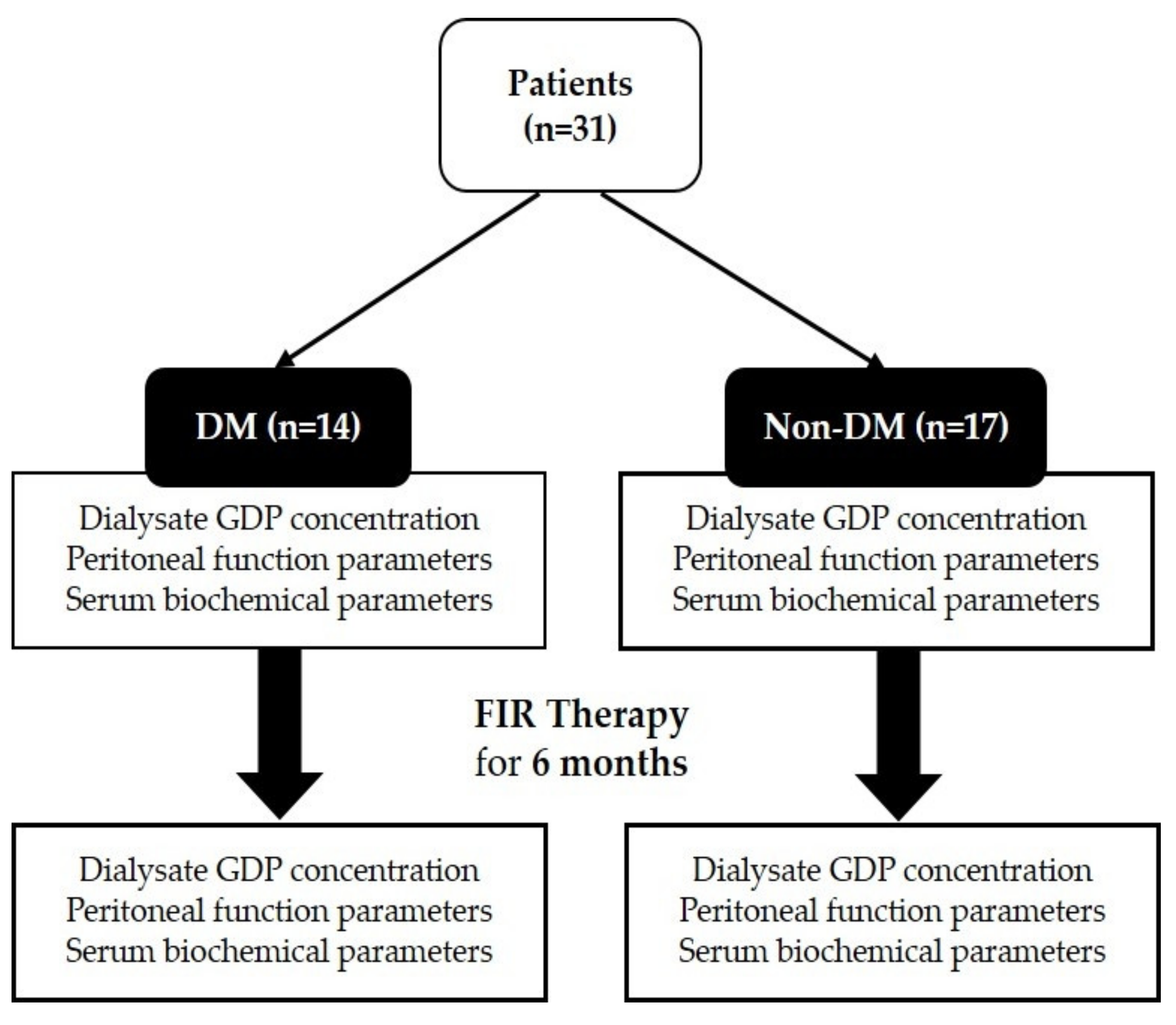
4.1. Study Design
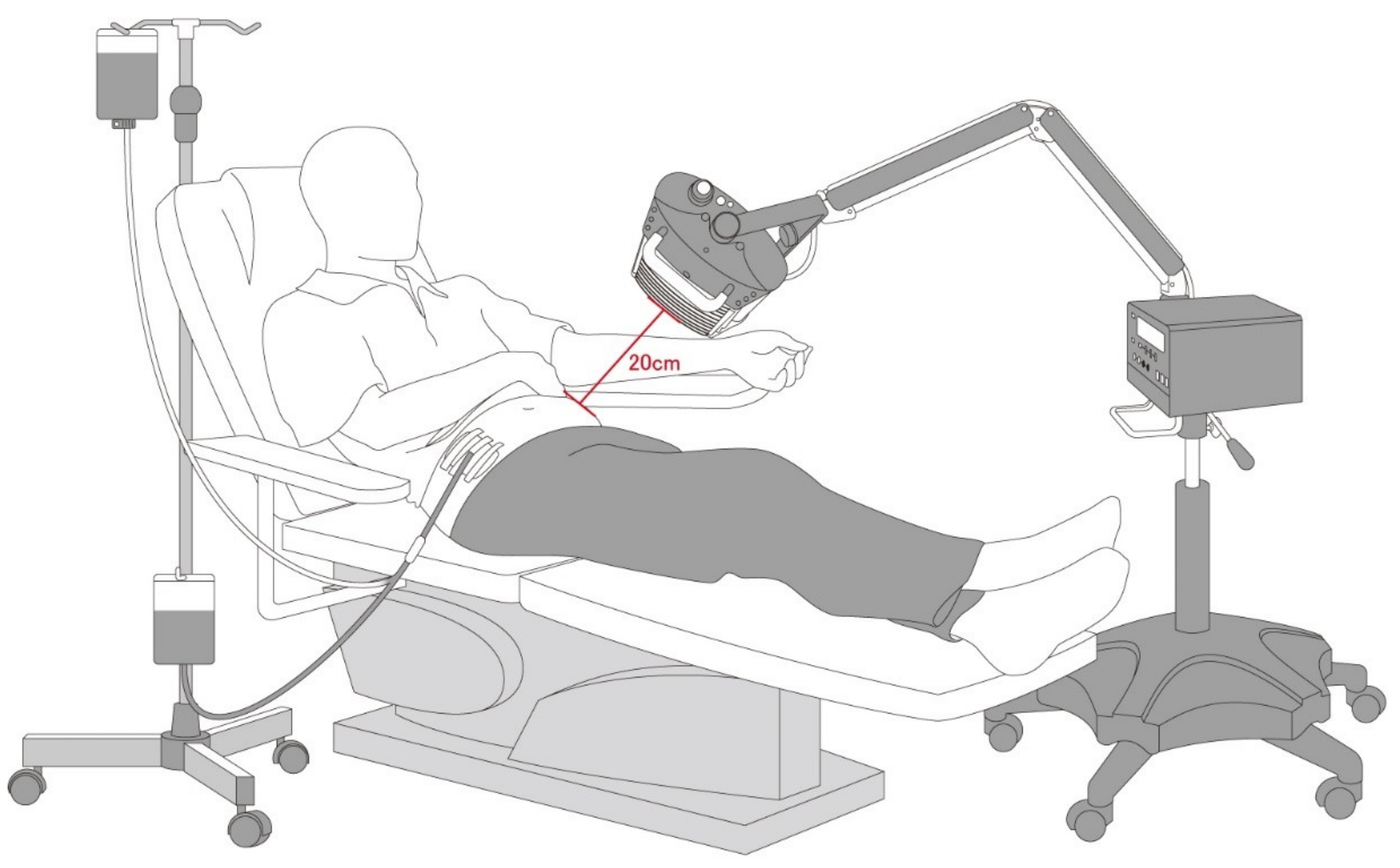
4.2. Far-Infrared Therapy
4.3. Determination of GDPs
4.3.1. Reagents and Chemicals
4.3.2. Derivatization Process of Standards
4.3.3. Instruments
4.3.4. Dialysate Sample Preparations
4.3.5. Quantification of GDPs
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sowinski, K.M.; Churchwell, M.D.; Decker, B.S. Hemodialysis and Peritoneal Dialysis. In Pharmacotherapy: A Pathophysiologic Approach, 11th ed.; DiPiro, J.T., Yee, G.C., Posey, L.M., Haines, S.T., Nolin, T.D., Ellingrod, V., Eds.; McGraw-Hill Education: New York, NY, USA, 2020. [Google Scholar]
- Mehrotra, R. Metabolic Effects of Peritoneal Dialysis. In Handbook of Dialysis Therapy, 5th ed.; Nissenson, A.R., Fine, R.N., Eds.; Elsevier: New York, NY, USA, 2017. [Google Scholar] [CrossRef]
- Haybrard, J.; Simon, N.; Danel, C.; Pinçon, C.; Barthélémy, C.; Tessier, F.J.; Décaudin, B.; Boulanger, E.; Odou, P. Factors Generating Glucose Degradation Products In Sterile Glucose Solutions For Infusion: Statistical Relevance Determination of Their Impacts. Sci. Rep. 2017, 7, 11932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodge, J.E. Dehydrated Foods, Chemistry of Browning Reactions in Model Systems. J. Agric. Food Chem. 1953, 1, 928–943. [Google Scholar] [CrossRef]
- Wieslander, A.P.; Nordin, M.K.; Kjellstrand, P.T.; Boberg, U.C. Toxicity of Peritoneal Dialysis Fluids on Cultured Fibroblasts, L-929. Kidney Int. 1991, 40, 77–79. [Google Scholar] [CrossRef] [Green Version]
- Wieslander, A.P.; Nordin, M.K.; Martinson, E.; Kjellstrand, P.T.; Boberg, U.C. Heat Sterilized PD-Fluids Impair Growth and Inflammatory Responses of Cultured Cell Lines and Human Leukocytes. Clin. Nephrol. 1993, 39, 343–348. [Google Scholar] [PubMed]
- Stinghen, A.E.; Massy, Z.A.; Vlassara, H.; Striker, G.E.; Boullier, A. Uremic Toxicity of Advanced Glycation End Products in CKD. J. Am. Soc. Nephrol. 2016, 27, 354–370. [Google Scholar] [CrossRef] [Green Version]
- Basta, G.; Schmidt, A.M.; De Caterina, R. Advanced Glycation End Products and Vascular Inflammation: Implications for Accelerated Atherosclerosis in Diabetes. Cardiovasc. Res. 2004, 63, 582–592. [Google Scholar] [CrossRef]
- Singh, R.; Barden, A.; Mori, T.; Beilin, L. Advanced Glycation End-Products: A Review. Diabetologia 2001, 44, 129–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldin, A.; Beckman, J.A.; Schmidt, A.M.; Creager, M.A. Advanced Glycation End Products: Sparking the Development of Diabetic Vascular Injury. Circulation 2006, 114, 597–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Liu, D.; Sun, L.; Lu, Y.; Zhang, Z. Advanced Glycation End Products and Neurodegenerative Diseases: Mechanisms and Perspective. J. Neurol. Sci. 2012, 317, 1–5. [Google Scholar] [CrossRef]
- Byun, K.; Yoo, Y.; Son, M.; Lee, J.; Jeong, G.B.; Park, Y.M.; Salekdeh, G.H.; Lee, B. Advanced Glycation End-Products Produced Systemically and by Macrophages: A Common Contributor to Inflammation and Degenerative Diseases. Pharmacol. Ther. 2017, 177, 44–55. [Google Scholar] [CrossRef]
- Mahiout, A.; Ehlerding, G.; Brunkhorst, R. Advanced Glycation End-Products in the Peritoneal Fluid and in the Peritoneal Membrane of Continuous Ambulant Peritoneal Dialysis Patients. Nephrol. Dial. Transplant. 1996, 11, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Honda, K.; Nitta, K.; Horita, S.; Yumura, W.; Nihei, H.; Nagai, R.; Ikeda, K.; Horiuchi, S. Accumulation of Advanced Glycation End Products in the Peritoneal Vasculature of Continuous Ambulatory Peritoneal Dialysis Patients with Low Ultrafiltration. Nephrol. Dial. Transplant. 1999, 14, 1541–1549. [Google Scholar] [CrossRef] [PubMed]
- Linden, T.; Forsbäck, G.; Deppisch, R.; Henle, T.; Wieslander, A. 3-Deoxyglucosone, a Promoter of Advanced Glycation end Products in Fluids for Peritoneal Dialysis. Perit. Dial. Int. 1998, 18, 290–293. [Google Scholar] [CrossRef] [PubMed]
- Nilsson-Thorell, C.B.; Muscalu, N.; Andrén, A.H.; Kjellstrand, P.T.; Wieslander, A.P. Heat Sterilization of Fluids for Peritoneal Dialysis Gives Rise to Aldehydes. Perit. Dial. Int. 1993, 13, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Mittelmaier, S.; Fünfrocken, M.; Fenn, D.; Fichert, T.; Pischetsrieder, M. Identification and Quantification of the Glucose Degradation Product Glucosone in Peritoneal Dialysis Fluids by HPLC/DAD/MSMS. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2010, 878, 877–882. [Google Scholar] [CrossRef]
- Basheer, C.; Pavagadhi, S.; Yu, H.; Balasubramanian, R.; Lee, H.K. Determination of Aldehydes in Rainwater Using Micro-Solid-Phase Extraction and High-Performance Liquid Chromatography. J. Chromatogr. A 2010, 1217, 6366–6372. [Google Scholar] [CrossRef]
- Fung, K.; Grosjean, D. Determination of Nanogram Amounts of Carbonyls as 2,4-Dinitrophenylhydrazones by High-Performance Liquid Chromatography. Anal. Chem. 1981, 53, 168–171. [Google Scholar] [CrossRef]
- Kuwata, K.; Uebori, M.; Yamasaki, H.; Kuge, Y.; Kiso, Y. Determination of Aliphatic Aldehydes in Air by Liquid Chromatography. Anal. Chem. 1983, 55, 2013–2016. [Google Scholar] [CrossRef]
- Steinberg, S.; Kaplan, I. The Determination of Low Molecular Weight Aldehydes in Rain, Fog and Mist by Reversed Phase Liquid Chromatography of the 2,4-Dinitrophenylhydrazone Derivatives. Int. J. Environ. Anal. Chem. 1984, 18, 253–266. [Google Scholar] [CrossRef]
- Adib, N.; Shekarchi, M.; Hajimehdipoor, H.; Shalviri, G.; Shekarchi, M.; Imaninejad, M. Cytotoxic Glucose Degradation Products in Fluids for Peritoneal Dialysis. Iran. J. Pharm. Res. 2011, 10, 113–117. [Google Scholar]
- Witowski, J.; Wisniewska, J.; Korybalska, K.; Bender, T.O.; Breborowicz, A.; Gahl, G.M.; Frei, U.; Passlick-Deetjen, J.; Jörres, A. Prolonged Exposure to Glucose Degradation Products Impairs Viability and Function of Human Peritoneal Mesothelial Cells. J. Am. Soc. Nephrol. 2001, 12, 2434–2441. [Google Scholar] [PubMed]
- Witowski, J.; Jörres, A.; Korybalska, K.; Ksiazek, K.; Wisniewska-Elnur, J.; Bender, T.O.; Passlick-Deetjen, J.; Breborowicz, A. Glucose Degradation Products in Peritoneal Dialysis Fluids: Do They Harm? Kidney Int. 2003, 63, S148–S151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witowski, J.; Bender, T.O.; Gahl, G.M.; Frei, U.; Jörres, A. Glucose Degradation Products and Peritoneal Membrane Function. Perit. Dial. Int. 2001, 21, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Vardhan, A.; Hutchison, A.J. Peritoneal Dialysis Solutions. In Handbook of Dialysis Therapy, 5th ed.; Nissenson, A.R., Fine, R.N., Eds.; Elsevier: New York, NY, USA, 2017. [Google Scholar] [CrossRef]
- Brown, E.A.; Bargman, J.; van Biesen, W.; Chang, M.-Y.; Finkelstein, F.O.; Hurst, H.; Johnson, D.W.; Kawanishi, H.; Lambie, M.; de Moraes, T.P.; et al. Length of Time on Peritoneal Dialysis and Encapsulating Peritoneal Sclerosis—Position Paper for ISPD: 2017 Update. Perit. Dial. Int. 2017, 37, 362–374. [Google Scholar] [CrossRef] [PubMed]
- Lambie, M.; Davies, S.J. Peritoneal Membrane Dysfunction: Inadequate Solute Removal, Ultrafiltration Failure, and Encapsulating Peritoneal Sclerosis. In Handbook of Dialysis Therapy, 5th ed.; Nissenson, A.R., Fine, R.N., Eds.; Elsevier: New York, NY, USA, 2017. [Google Scholar] [CrossRef]
- Ou, S.-M.; Hu, F.-H.; Yang, W.-C.; Lin, C.-C. Far-Infrared Therapy as a Novel Treatment for Encapsulating Peritoneal Sclerosis. Am. J. Gastroenterol. 2014, 109, 1957–1959. [Google Scholar] [CrossRef]
- Vatansever, F.; Hamblin, M.R. Far Infrared Radiation (FIR): Its Biological Effects and Medical Applications. Photonics Lasers Med. 2012, 4, 255–266. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.-C.; Liu, X.-M.; Peyton, K.; Wang, H.; Yang, W.-C.; Lin, S.-J.; Durante, W. Far Infrared Therapy Inhibits Vascular Endothelial Inflammation via the Induction of Heme Oxygenase-1. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 739–745. [Google Scholar] [CrossRef] [Green Version]
- Yu, S.-Y.; Chiu, J.-H.; Yang, S.D.; Hsu, Y.C.; Lui, W.Y.; Wu, C.W. Biological Effect of Far-Infrared Therapy on Increasing Skin Microcirculation in Rats. Photodermatol. Photoimmunol. Photomed. 2006, 22, 78–86. [Google Scholar] [CrossRef]
- Ikeda, Y.; Biro, S.; Kamogawa, Y.; Yoshifuku, S.; Eto, H.; Orihara, K.; Yu, B.; Kihara, T.; Miyata, M.; Hamasaki, S. Repeated Sauna Therapy Increases Arterial Endothelial Nitric Oxide Synthase Expression and Nitric Oxide Production in Cardiomyopathic Hamsters. Circ. J. 2005, 69, 722–729. [Google Scholar] [CrossRef] [Green Version]
- Akasaki, Y.; Miyata, M.; Eto, H.; Shirasawa, T.; Hamada, N.; Ikeda, Y.; Biro, S.; Otsuji, Y.; Tei, C. Repeated Thermal Therapy Up-Regulates Endothelial Nitric Oxide Synthase and Augments Angiogenesis in a Mouse Model of Hindlimb Ischemia. Circ. J. 2006, 70, 463–470. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y. The Effect of Far Infrared Radiation Therapy on Inflammation Regulation in Lipopolysaccharide-induced Peritonitis in Mice. SAGE Open Med. 2018, 6, 2050312118798941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, K.-H.; Li, W.-T. Clinical Effects of Far-Infrared Therapy in Patients with Allergic Rhinitis. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; pp. 1479–1482. [Google Scholar]
- Lin, C.-C.; Yang, W.-C.; Chen, M.-C.; Liu, W.-S.; Yang, C.-Y.; Lee, P.-C. Effect of Far Infrared Therapy on Arteriovenous Fistula Maturation: An Open-Label Randomized Controlled Trial. Am. J. Kidney Dis. 2013, 62, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-C.; Yang, W.-C.; Lin, S.-J.; Chen, T.-W.; Lee, W.-S.; Chang, C.-F.; Lee, P.-C.; Lee, S.-D.; Su, T.-S.; Fann, C.S.-J.; et al. Length Polymorphism in Heme Oxygenase-1 is Associated with Arteriovenous Fistula Patency in Hemodialysis Patients. Kidney Int. 2006, 69, 165–172. [Google Scholar] [CrossRef] [Green Version]
- Liau, B.-Y.; Leung, T.-K.; Ou, M.-C.; Ho, C.-K.; Yang, A.; Lin, Y.-S. Inhibitory Effects of Far-Infrared Ray-Emitting Belts on Primary Dysmenorrhea. Int. J. Photoenergy 2012, 2012, 238468. [Google Scholar] [CrossRef] [Green Version]
- European Commission. Analytical Quality Control and Method Validation Procedures For Pesticide Residues Analysis in Food and Feed; European Commission: Brussels, Belgium, 2020. [Google Scholar]
- Conaway, C.C.; Whysner, J.; Verna, L.K.; Williams, G.M. Formaldehyde Mechanistic Data and Risk Assessment: Endogenous Protection from DNA Adduct Formation. Pharmacol. Ther. 1996, 71, 29–55. [Google Scholar] [CrossRef]
- Witowski, J.; Korybalska, K.; Wisniewska, J.; Breborowicz, A.; Gahl, G.M.; Frei, U.; Passlick-Deetjen, J.; Jörres, A. Effect of Glucose Degradation Products on Human Peritoneal Mesothelial Cell Function. J. Am. Soc. Nephrol. 2000, 11, 729–739. [Google Scholar]
- Morgan, K.T. A Brief Review of Formaldehyde Carcinogenesis in Relation to Rat Nasal Pathology and Human Health Risk Assessment. Toxicol. Pathol. 1997, 25, 291–307. [Google Scholar] [CrossRef]
- Tuncer, M.; Sarıkaya, M.; Sezer, T.; Özcan, S.; Süleymanlar, G.; Yakupogˇlu, G.; Ersoy, F.F. Chemical Peritonitis Associated with High Dialysate Acetaldehyde Concentrations. Nephrol. Dial. Transplant. 2000, 15, 2037–2040. [Google Scholar] [CrossRef] [Green Version]
- Castellino, N.; Elmino, O.; Rozera, G. Experimental Research on Toxicity of Furfural. Arch. Environ. Health 1963, 7, 574–582. [Google Scholar] [CrossRef]
- Ulbricht, R.J.; Northup, S.J.; Thomas, J.A. A Review of 5-Hydroxymethylfurfural (HMF) in Parenteral Solutions. Fundam. Appl. Toxicol. 1984, 4, 843–853. [Google Scholar] [CrossRef]
- Uribarri, J.; Oh, M.S.; Carroll, H.J. Hyperkalemia in Diabetes Mellitus. J. Diabet. Complicat. 1990, 4, 3–7. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | DM (n = 14) | Non-DM (n = 17) | p |
|---|---|---|---|
| Age (years) | 59.5 ± 12.11 | 55.71 ± 14.29 | 0.48 |
| Gender | |||
| Male | 6 (42.9) | 6 (35.3) | 0.72 |
| Female | 8 (57.1) | 11 (64.7) | |
| Weight (kg) | 61.32 ± 7.21 | 57.89 ± 12.66 | 0.25 |
| BMI (kg/m2) | 24.16 ± 2.60 | 21.60 ± 3.75 | 0.03 * |
| PD duration (months) | 14.07 ± 16.91 | 25.65 ± 31.82 | 0.34 |
| Peritoneal fluid dextrose exposure (g/24 h) | 113.29 ± 35.55 | 116.10 ± 38.95 | 0.75 |
| Comorbidities | |||
| Hypertension | 14 (100) | 14 (82.4) | 0.23 |
| Hyperlipidemia | 4 (28.6) | 9 (52.9) | 0.28 |
| Congestive heart failure | 3 (21.4) | 3 (17.6) | 1.0 |
| Gout | 3 (21.4) | 8 (47.1) | 0.26 |
| Medications | |||
| Angiotensin receptor blockers | 8 (57.1) | 7 (41.2) | 0.48 |
| Beta blockers | 7 (50) | 9 (52.9) | 1.0 |
| HMG-CoA reductase inhibitors | 8 (57.1) | 12 (70.6) | 0.48 |
| Peritoneal function | |||
| D/D0 glucose | 0.38 ± 0.07 | 0.35 ± 0.08 | 0.23 |
| D/P creatinine | 0.67 ± 0.11 | 0.69 ± 0.10 | 0.34 |
| Peritoneal Kt/V | 1.78 ± 0.42 | 1.62 ± 0.33 | 0.31 |
| Peritoneal weekly CCr (L/week/1.73 m2) | 42.92 ± 7.97 | 39.56 ± 8.40 | 0.30 |
| Net ultrafiltration (mL) | 839.93 ± 564.45 | 1007 ± 517.64 | 0.51 |
| Urine output (mL) | 355 ± 298.19 | 523.82 ± 685.16 | 0.90 |
| nPCR (g/kg/day) | 1.02 ± 0.22 | 1.19 ± 0.21 | 0.06 |
| Serum biochemistry | |||
| Glucose (mg/dL) | 136 ± 60.52 | 102.53 ± 13.45 | 0.02 * |
| HbA1c (%) | 6.85 ± 1.21 | 5.57 ± 0.57 | 0.003 ** |
| Triglycerides (mg/dL) | 135.21 ± 79.25 | 124.47 ± 49.91 | 0.89 |
| BUN (mg/dL) | 74.29 ± 22.32 | 75.59 ± 14.08 | 0.50 |
| Creatinine (mg/dL) | 9.97 ± 2.78 | 11.88 ± 3.34 | 0.15 |
| Albumin (g/dL) | 3.25 ± 0.33 | 3.77 ± 0.43 | 0.001 ** |
| Potassium (mmol/L) | 4.24 ± 0.86 | 4.12 ± 0.47 | 0.84 |
| Calcium (mg/dL) | 9.72 ± 0.66 | 9.55 ± 0.52 | 0.39 |
| Phosphate (mg/dL) | 4.81 ± 1.27 | 5.32 ± 1.29 | 0.29 |
| Uric acid (mg/dL) | 5.16 ± 1.50 | 5.99 ± 1.36 | 0.09 |
| Hs-CRP (mg/dL) | 2.07 ± 5.22 | 0.36 ± 0.63 | 0.11 |
| GDP-DNPH Compounds | Linear Range | r2 |
|---|---|---|
| Formaldehyde-DNPH | 100 μg/L–5 mg/L | 0.997 |
| Acetaldehyde-DNPH | 25 μg/L–1 mg/L | 0.996 |
| Furfural-DNPH | 10 μg/L–500 μg/L | 0.998 |
| HMF-DNPH | 250 μg/L–10 mg/L | 0.998 |
| Glyoxal-bis-DNPH | 250 μg/L–10 mg/L | 0.998 |
| Methylglyoxal-bis-DNPH | 50 μg/L–2.5 mg/L | 0.997 |
| KDG-bis-DNPH | 250 μg/L–10 mg/L | 0.998 |
| Parameters | Pre-FIR | Post-FIR | p |
|---|---|---|---|
| GDPs (μg/L) | |||
| Formaldehyde | 4070.94 ± 1764.60 | 3362.85 ± 1233.10 | 0.06 |
| Acetaldehyde | 1811.45 ± 388.50 | 1909.26 ± 415.32 | 0.34 |
| Furfural | 1366.25 ± 726.71 | 876.11 ± 491.88 | 0.005 ** |
| HMF | 51,514.0266 ± 37,816.87 | 35,565.57 ± 25,674.87 | 0.03 * |
| Glyoxal | 7025.46 ± 3137.69 | 5713.31 ± 4798.52 | 0.20 |
| Methylglyoxal | 2260.49 ± 1497.04 | 1550.11 ± 1329.83 | 0.02 * |
| KDG | 33,879.82 ± 15,265.64 | 29,031.18 ± 16,173.89 | 0.18 |
| Peritoneal function | |||
| D/D0 glucose | 0.37 ± 0.08 | 0.39 ± 0.06 | 0.03 * |
| D/P creatinine | 0.68 ± 0.11 | 0.66 ± 0.08 | 0.15 |
| Peritoneal Kt/V | 1.69 ± 0.37 | 1.82 ± 0.39 | 0.09 |
| Peritoneal weekly CCr (L/week/1.73 m2) | 41.07 ± 8.25 | 41.69 ± 7.54 | 0.70 |
| nPCR (g/kg/d) | 1.11 ± 0.23 | 1.12 ± 0.30 | 0.89 |
| Serum biochemistry | |||
| Glucose (mg/dL) | 117.65 ± 44.39 | 132.19 ± 53.33 | 0.12 |
| HbA1c (%) | 6.14 ± 1.11 | 6.32 ± 1.21 | 0.25 |
| Triglycerides (mg/dL) | 127.5 ± 64.13 | 155.43 ± 111.97 | 0.12 |
| Albumin (g/dL) | 3.54 ± 0.46 | 3.49 ± 0.48 | 0.44 |
| Potassium (mmol/L) | 4.17 ± 0.67 | 3.81 ± 0.66 | 0.008 ** |
| Hs-CRP (mg/dL) | 1.13 ± 3.57 | 0.48 ± 0.82 | 0.23 |
| Δ GDPs (μg/L) | DM | p† | Non-DM | p† | p†† |
|---|---|---|---|---|---|
| Formaldehyde | −1082.07 −22.33) | 0.16 | −400.10 (−11.65) | 0.23 | 0.5 |
| Acetaldehyde | 5.98 (0.32) | 0.83 | 173.44 (9.93) | 0.25 | 0.34 |
| Furfural | −534.10 −36.40) | 0.08 | −453.94 (−35.38) | 0.11 | 0.81 |
| HMF | −13,822.86 (−24.54) | 0.16 | −17,698.96 (−37.22) | 0.16 | 1.0 |
| Glyoxal | −1909 (−27.14) | 0.16 | −820.62 (−11.69) | 0.59 | 0.43 |
| Methylglyoxal | −698.38 (−31.43) | 0.11 | −720.26 (−31.42) | 0.15 | 1.0 |
| KDG | −6543.83 (−17.01) | 0.51 | −3452.59 (−11.47) | 0.29 | 0.81 |
| Δ Clinical Parameters | DM | Non-DM | p |
|---|---|---|---|
| Peritoneal function | |||
| D/D0 glucose | 0.04 ± 0.09 | 0.02 ± 0.04 | 0.77 |
| D/P creatinine | −0.007 ± 0.10 | −0.03 ± 0.06 | 0.36 |
| Peritoneal Kt/V | −0.04 ± 0.24 | 0.27 ± 0.47 | 0.03 * |
| Peritoneal weekly CCr (L/week/1.73 m2) | −1.63 ± 8.14 | 2.46 ± 9.08 | 0.22 |
| nPCR (g/kg/d) | 0.003 ± 0.22 | 0.008 ± 0.22 | 0.85 |
| Serum biochemistry | |||
| Glucose (mg/dL) | 33.64 ± 70.05 | −1.18 ± 11.58 | 0.44 |
| HbA1c (%) | 0.24 ± 1.15 | 0.12 ± 0.46 | 0.74 |
| Albumin (g/dL) | −0.01 ± 0.38 | −0.08 ± 0.31 | 0.59 |
| Potassium (mmol/L) | −0.56 ± 0.61 | −0.20 ± 0.77 | 0.20 |
| Hs-CRP (mg/dL) | −1.32 ± 4.37 | −0.1 ± 0.65 | 0.61 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, C.-N.; Niu, C.-Y.; Tan, A.C.; Chan, C.-H.; Chen, C.-F.; Chen, T.-H.; Li, S.-Y.; Chen, Y.-T.; Chen, F.-Y.; Liu, W.-S.; et al. The Effect of Far-Infrared Therapy on the Peritoneal Expression of Glucose Degradation Products in Diabetic Patients on Peritoneal Dialysis. Int. J. Mol. Sci. 2021, 22, 3732. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22073732
Chang C-N, Niu C-Y, Tan AC, Chan C-H, Chen C-F, Chen T-H, Li S-Y, Chen Y-T, Chen F-Y, Liu W-S, et al. The Effect of Far-Infrared Therapy on the Peritoneal Expression of Glucose Degradation Products in Diabetic Patients on Peritoneal Dialysis. International Journal of Molecular Sciences. 2021; 22(7):3732. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22073732
Chicago/Turabian StyleChang, Chia-Ning, Chih-Yuan Niu, Ann Charis Tan, Chia-Hao Chan, Chun-Fan Chen, Tz-Heng Chen, Szu-Yuan Li, Yung-Tai Chen, Fan-Yu Chen, Wen-Sheng Liu, and et al. 2021. "The Effect of Far-Infrared Therapy on the Peritoneal Expression of Glucose Degradation Products in Diabetic Patients on Peritoneal Dialysis" International Journal of Molecular Sciences 22, no. 7: 3732. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22073732