
The Role of Sarcopenic Obesity in Cancer and Cardiovascular Disease: A Synthesis of the Evidence on Pathophysiological Aspects and Clinical Implications

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Definitions and Diagnostic Criteria for Sarcopenic Obesity
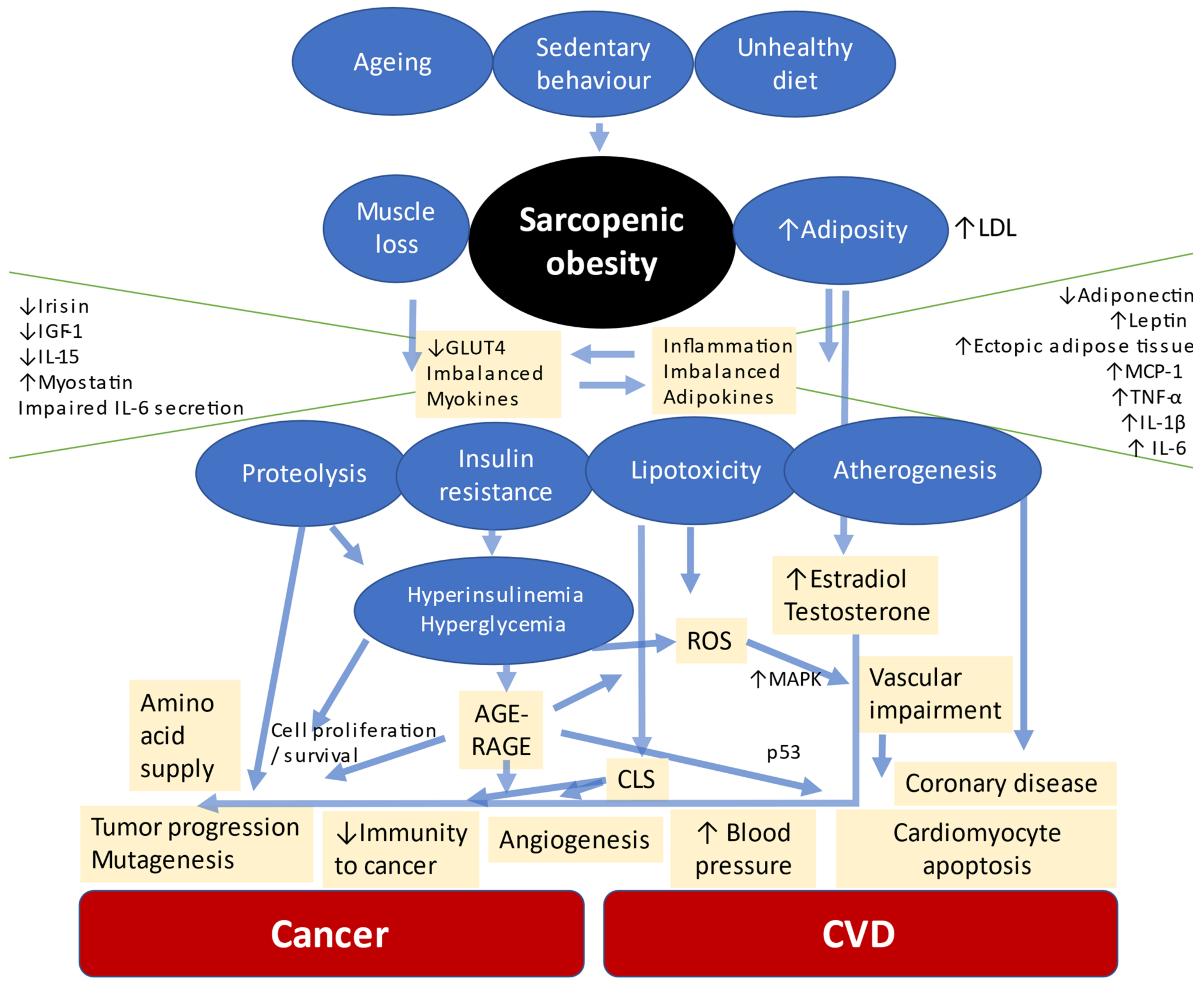
3. Pathophysiology of the Association of Sarcopenic Obesity, Cardiovascular Disease and Cancer
3.1. Cardiovascular Disease
3.2. Neoplasms
4. Epidemiological and Clinical Evidence of the Association between Sarcopenic Obesity and Cardiovascular Disease
5. Epidemiological and Clinical Evidence of the Association between Sarcopenic Obesity and Cancer
5.1. Occurrence and Association of Sarcopenic Obesity in the Occurrence of Cancer
5.2. Sarcopenic Obesity in the Complications of the Most Common Anticancer Treatments and Other Clinical Implications
5.3. Impact of Sarcopenic Obesity on Cancer Mortality
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Home Page. Available online: https://www.who.int/dietphysicalactivity/strategy/eb11344/strategy_english_web.pdf (accessed on 21 March 2021).
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K. Body Fatness and Cancer—ViewpoInt. of the IARC Working Group. N. Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef] [Green Version]
- Caleyachetty, R.; Thomas, G.N.; Toulis, K.A.; Mohammed, N.; Gokhale, K.M.; Balachandran, K.; Nirantkumar, K. Metabolically Healthy Obese and Incident Cardiovascular Disease Events Among 3.5 Million Men and Women. J. Am. Coll. Cardiol. 2017, 70, 1429–1437. [Google Scholar] [CrossRef]
- Silveira, E.A.; Kliemann, N.; Noll, M.; Sarrafzadegan, N.; Oliveira, C. Visceral Obesity and Incident Cancer and Cardiovascular Disease: An Integrative Review of the Epidemiological Evidence. Obes. Rev. 2021, 22, e13088. [Google Scholar] [CrossRef] [PubMed]
- Iwase, T.; Wang, X.; Shrimanker, T.V.; Kolonin, M.G.; Ueno, N.T. Body Composition and Breast Cancer Risk and Treatment: Mechanisms and Impact. Breast Cancer Res. Treat. 2021, 1–11. [Google Scholar] [CrossRef]
- Carneiro, I.P.; Mazurak, V.C.; Prado, C.M. Clinical Implications of Sarcopenic Obesity in Cancer. Curr. Oncol. Rep. 2016, 18, 62. [Google Scholar] [CrossRef] [PubMed]
- Baracos, V.E.; Arribas, L. Sarcopenic Obesity: Hidden Muscle Wasting and Its Impact for Survival and Complications of Cancer Therapy. Ann. Oncol. 2018, 29 (Suppl. 2), ii1–ii9. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, M.C.; Pastore, C.A.; Orlandi, S.P.; Heymsfield, S.B. Obesity Paradox in Cancer: New Insights Provided by Body Composition. Am. J. Clin. Nutr. 2014, 99, 999–1005. [Google Scholar] [CrossRef] [PubMed]
- Rier, H.N.; Jager, A.; Sleijfer, S.; van Rosmalen, J.; Kock, M.C.J.M.; Levin, M.D. Low Muscle Attenuation Is a Prognostic Factor for Survival in Metastatic Breast Cancer Patients Treated with First Line Palliative Chemotherapy. Breast 2017, 31, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Barazzoni, R.; Bischoff, S.C.; Boirie, Y.; Busetto, L.; Cederholm, T.; Dicker, D.; Toplak, H.; van Gossum, A.; Yumuk, V.; Vettor, R. Sarcopenic Obesity: Time to Meet the Challenge. Clin. Nutr. 2018, 37, 1787–1793. [Google Scholar] [CrossRef]
- Zhang, X.; Xie, X.; Dou, Q.; Liu, C.; Zhang, W.; Yang, Y.; Deng, R.; Cheng, A.S.K. Association of Sarcopenic Obesity with the Risk of All-Cause Mortality among Adults over a Broad Range of Different Settings: A Updated Meta-Analysis. BMC Geriatr. 2019, 19, 183. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European Consensus on Definition and Diagnosis. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirani, V.; Naganathan, V.; Blyth, F.; le Couteur, D.G.; Seibel, M.J.; Waite, L.M.; Handelsman, D.J.; Cumming, R.G. Longitudinal Associations between Body Composition, Sarcopenic Obesity and Outcomes of Frailty, Disability, Institutionalisation and Mortality in Community-Dwelling Older Men: The Concord Health and Ageing in Men Project. Age Ageing 2017, 46, 413–420. [Google Scholar] [CrossRef] [Green Version]
- Smeuninx, B.; McKendry, J.; Wilson, D.; Martin, U.; Breen, L. Age-Relatedanabolic Resistance of Myofibrillar Protein Synthesis Is Exacerbated in Obese Inactive Individuals. J. Clin. Endocrinol. Metab. 2017, 102, 3535–3545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, W.-Q.; Xiao, G.-L.; Fan, Y.-B.; He, M.; Lv, S.; Li, Y.-S. Sarcopenic Obesity: Research Advances in Pathogenesis and Diagnostic Criteria. Aging Clin. Exp. Res. 2021, 33, 247–252. [Google Scholar] [CrossRef]
- Hong, S.H.; Choi, K.M. Sarcopenic Obesity, Insulin Resistance, and Their Implications in Cardiovascular and Metabolic Consequences. Int. J. Mol. Sci. 2020, 21, 494. [Google Scholar] [CrossRef] [Green Version]
- Silveira, E.A.; Vaseghi, G.; de Santos, A.S.C.; Kliemann, N.; Masoudkabir, F.; Noll, M.; Mohammadifard, N.; Sarrafzadegan, N.; de Oliveira, C. Visceral Obesity and Its Shared Role in Cancer and Cardiovascular Disease: A Scoping Review of the Pathophysiology and Pharmacological Treatments. Int. J. Mol. Sci. 2020, 21, 9042. [Google Scholar] [CrossRef]
- Batsis, J.A.; Villareal, D.T. Sarcopenic Obesity in Older Adults: Aetiology, Epidemiology and Treatment Strategies. Nat. Rev. Endocrinol. 2018, 14, 513–537. [Google Scholar] [CrossRef]
- Silveira, E.A.; Pagotto, V.; Barbosa, L.S.; de Oliveira, C.; das Graças Pena, G.; Velasquez-Melendez, G. Accuracy of BMI and Waist Circumference Cut-off Points to Predict Obesity in Older Adults. Cienc. Saude Coletiva 2020, 25, 1073–1082. [Google Scholar] [CrossRef]
- Pagotto, V.; dos Santos, K.F.; Malaquias, S.G.; Bachion, M.M.; Silveira, E.A. Calf Circumference: Clinical Validation for Evaluation of Muscle Mass in the Elderly. Rev. Bras. Enferm. 2018, 71, 322–328. [Google Scholar] [CrossRef] [Green Version]
- Kara, M.; Kaymak, B.; Ata, A.M.; Özkal, Ö.; Kara, Ö.; Baki, A.; Ayçiçek, G.S.; Topuz, S.; Karahan, S.; Soylu, A.R.; et al. STAR—Sonographic Thigh Adjustment Ratio: A Golden Formula for the Diagnosis of Sarcopenia. Am. J. Phys. Med. Rehabil. 2020, 99, 902–908. [Google Scholar] [CrossRef]
- Hwang, A.C.; Liu, L.K.; Lee, W.J.; Peng, L.N.; Chen, L.K. Calf Circumference as a Screening Instrument for Appendicular Muscle Mass Measurement. J. Am. Med. Dir. Assoc. 2018, 19, 182–184. [Google Scholar] [CrossRef]
- Lodewick, T.M.; van Nijnatten, T.J.A.; van Dam, R.M.; van Mierlo, K.; Dello, S.A.W.G.; Neumann, U.P.; Damink, S.W.M.O.; Dejong, C.H.C. Are Sarcopenia, Obesity and Sarcopenic Obesity Predictive of Outcome in Patients with Colorectal Liver Metastases? HPB 2015, 17, 438–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montano-Loza, A.J.; Angulo, P.; Meza-Junco, J.; Prado, C.M.M.; Sawyer, M.B.; Beaumont, C.; Esfandiari, N.; Ma, M.; Baracos, V.E. Sarcopenic Obesity and Myosteatosis Are Associated with Higher Mortality in Patients with Cirrhosis. J. Cachexia Sarcopenia Muscle 2016, 7, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Hamer, M.; O’Donovan, G. Sarcopenic Obesity, Weight Loss, and Mortality: The English Longitudinal Study of Ageing. Am. J. Clin. Nutr. 2017, 106, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Fielding, R.A.; Vellas, B.; Evans, W.J.; Bhasin, S.; Morley, J.E.; Newman, A.B.; van Kan, G.A.; Andrieu, S.; Bauer, J.; Breuille, D.; et al. Sarcopenia: An Undiagnosed Condition in Older Adults. Current Consensus Definition: Prevalence, Etiology, and Consequences. International Working Group on Sarcopenia. J. Am. Med. Dir. Assoc. 2011, 12, 249–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batsis, J.A.; Mackenzie, T.A.; Barre, L.K.; Lopez-Jimenez, F.; Bartels, S.J. Sarcopenia, Sarcopenic Obesity and Mortality in Older Adults: Results from the National Health and Nutrition Examination Survey III. Eur. J. Clin. Nutr. 2014, 68, 1001–1007. [Google Scholar] [CrossRef] [Green Version]
- Stenholm, S.; Mehta, N.K.; Elo, I.T.; Heliövaara, M.; Koskinen, S.; Aromaa, A. Obesity and Muscle Strength as Long-Term Determinants of All-Cause Mortality—A 33-Year Follow-up of the Mini-Finland Health Examination Survey. Int. J. Obes. 2013, 38, 1126–1132. [Google Scholar] [CrossRef] [Green Version]
- Atkins, J.L.; Whincup, P.H.; Morris, R.W.; Lennon, L.T.; Papacosta, O.; Wannamethee, S.G. Sarcopenic Obesity and Risk of Cardiovascular Disease and Mortality: A Population-Based Cohort Study of Older Men. J. Am. Geriatr. Soc. 2014, 62, 253–260. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.K.; Chen, L.Y.; Yeh, K.P.; Lin, M.H.; Hwang, A.C.; Peng, L.N.; Chen, L.K. Sarcopenia, but Not Sarcopenic Obesity, Predicts Mortality for Older Old Men: A 3-Year Prospective Cohort Study. J. Clin. Gerontol. Geriatr. 2014, 5, 42–46. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.T.; Lin, J.; Chen, W.S.; Huang, Y.S.; Wu, R.S.; Chen, X.D.; Lou, N.; Chi, C.H.; Hu, C.Y.; Shen, X. Sarcopenic Obesity Is Associated with Severe Postoperative Complications in Gastric Cancer Patients Undergoing Gastrectomy: A Prospective Study. J. Gastrointest. Surg. 2018, 22, 1861–1869. [Google Scholar] [CrossRef]
- Hara, N.; Iwasa, M.; Sugimoto, R.; Mifuji-Moroka, R.; Yoshikawa, K.; Terasaka, E.; Hattori, A.; Ishidome, M.; Kobayashi, Y.; Hasegawa, H.; et al. Sarcopenia and Sarcopenic Obesity Are Prognostic Factors for Overall Survival in Patients with Cirrhosis. Intern. Med. 2016, 55, 863–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anker, S.D.; Morley, J.E.; von Haehling, S. Welcome to the ICD-10 Code for Sarcopenia. J. Cachexia Sarcopenia Muscle 2016, 7, 512–514. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Lu, C.W.; Yang, K.C.; Chang, H.H.; Lee, L.T.; Chen, C.Y.; Huang, K.C. Sarcopenic Obesity Is Closely Associated with Metabolic Syndrome. Obes. Res. Clin. Pract. 2013, 7, e301–e307. [Google Scholar] [CrossRef] [PubMed]
- Petermann-Rocha, F.; Yang, S.; Gray, S.R.; Pell, J.P.; Celis-Morales, C.; Ho, F.K. Sarcopenic Obesity and Its Association with Respiratory Disease Incidence and Mortality. Clin. Nutr. 2020, 39, 3461–3466. [Google Scholar] [CrossRef]
- Stoklossa, C.A.J.; Sharma, A.M.; Forhan, M.; Siervo, M.; Padwal, R.S.; Prado, C.M. Prevalence of Sarcopenic Obesity in Adults with Class II/III Obesity Using Different Diagnostic Criteria. J. Nutr. Metab. 2017, 2017. [Google Scholar] [CrossRef]
- Batsis, J.A.; Barre, L.K.; Mackenzie, T.A.; Pratt, S.I.; Lopez-Jimenez, F.; Bartels, S.J. Variation in the Prevalence of Sarcopenia and Sarcopenic Obesity in Older Adults Associated with Different Research Definitions: Dual-Energy X-Ray Absorptiometry Data from the National Health and Nutrition Examination Survey 1999–2004. J. Am. Geriatr. Soc. 2013, 61, 974–980. [Google Scholar] [CrossRef]
- Santos, C.M.; Dias, J.M.D.; Samora, G.A.R.; Perracini, M.R.; Guerra, R.O.; Dias, R.C. Prevalence of Obesity, Sarcopenic Obesity and Associated Factors: A FIBRA Network Study. Fisioter. Mov. 2017, 30 (Suppl. 1), 161–169. [Google Scholar] [CrossRef] [Green Version]
- Kalyani, R.R.; Corriere, M.; Ferrucci, L. Age-Related and Disease-Related Muscle Loss: The Effect of Diabetes, Obesity, and Other Diseases. Lancet Diabetes Endocrinol. 2014, 2, 819–829. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.C.; Yang, W.C.V. Hyperglycemia, Tumorigenesis, and Chronic Inflammation. Crit. Rev. Oncol. Hematol. 2016, 108, 146–153. [Google Scholar] [CrossRef]
- di Pino, A.; Defronzo, R.A. Insulin Resistance and Atherosclerosis: Implications for Insulin-Sensitizing Agents. Endocr. Rev. 2019, 40, 1447–1467. [Google Scholar] [CrossRef] [Green Version]
- Favre, G.A.; Esnault, V.L.M.; van Obberghen, E. Modulation of Glucose Metabolism by the Renin-Angiotensin-Aldosterone System. Am. J. Physiol. Endocrinol. Metab. 2015, 308, E435–E449. [Google Scholar] [CrossRef] [Green Version]
- Rhee, S.Y.; Kim, Y.S. The Role of Advanced Glycation End Products in Diabetic Vascular Complications. Diabetes Metab. J. 2018, 42, 188–195. [Google Scholar] [CrossRef]
- Rungratanawanich, W.; Qu, Y.; Wang, X.; Essa, M.M.; Song, B.-J. Advanced Glycation End Products (AGEs) and Other Adducts in Aging-Related Diseases and Alcohol-Mediated Tissue Injury. Exp. Mol. Med. 2021, 53, 168–188. [Google Scholar] [CrossRef]
- Kosmopoulos, M.; Drekolias, D.; Zavras, P.D.; Piperi, C.; Papavassiliou, A.G. Impact of Advanced Glycation End Products (AGEs) Signaling in Coronary Artery Disease. Biochim. Biophys. Acta Mol. Basis Dis. 2019, 1865, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Tsoporis, J.N.; Izhar, S.; Leong-Poi, H.; Desjardins, J.F.; Huttunen, H.J.; Parker, T.G. S100B Interaction with the Receptor for Advanced Glycation End Products (RAGE): A Novel Receptor-Mediated Mechanism for Myocyte Apoptosis Postinfarction. Circ. Res. 2010, 106, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Wei, S.G.; Zhang, Z.H.; Weiss, R.M.; Felder, R.B. ERK1/2 MAPK Signaling in Hypothalamic Paraventricular Nucleus Contributes to Sympathetic Excitation in Rats with Heart Failure after Myocardial Infarction. Am. J. Physiol. Heart Circ. Physiol. 2016, 310, H732–H739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brailoiu, E.; Deliu, E.; Sporici, R.A.; Brailoiu, G.C. Irisin Evokes Bradycardia by Activating Cardiac-Projecting Neurons of Nucleus Ambiguus. Physiol. Rep. 2015, 3, e12419. [Google Scholar] [CrossRef] [PubMed]
- de Freitas, V.P.; Passos, R.d.S.; Oliveira, A.A.; Ribeiro, Í.J.S.; Freire, I.V.; Schettino, L.; Teles, M.F.; Casotti, C.A.; Pereira, R. Sarcopenia Is Associated to an Impaired Autonomic Heart Rate Modulation in Community-Dwelling Old Adults. Arch. Gerontol. Geriatr. 2018, 76, 120–124. [Google Scholar] [CrossRef]
- Affourtit, C. Mitochondrial Involvement in Skeletal Muscle Insulin Resistance: A Case of Imbalanced Bioenergetics. Biochim Biophys. Acta Bioenergy 2016, 1857, 1678–1693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morley, J.E. Pharmacologic Options for the Treatment of Sarcopenia. Calcif. Tissue Int. 2016, 98, 319–333. [Google Scholar] [CrossRef]
- Zhu, S.; Tian, Z.; Torigoe, D.; Zhao, J.; Xie, P.; Sugizaki, T.; Sato, M.; Horiguchi, H.; Terada, K.; Kadomatsu, T.; et al. Aging- And Obesity-Related Peri-Muscular Adipose Tissue Accelerates Muscle Atrophy. PLoS ONE 2019, 14, e0221366. [Google Scholar] [CrossRef] [Green Version]
- Korytowski, W.; Wawak, K.; Pabisz, P.; Schmitt, J.C.; Chadwick, A.C.; Sahoo, D.; Girotti, A.W. Impairment of Macrophage Cholesterol Efflux by Cholesterol Hydroperoxide Trafficking Implications for Atherogenesis under Oxidative Stress. Arter. Thromb. Vasc. Biol. 2015, 35, 2104–2113. [Google Scholar] [CrossRef] [Green Version]
- Choi, K.M. Sarcopenia and Sarcopenic Obesity. Korean J. Intern. Med. 2016, 31, 1054–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohmann, A.E.; Goodwin, P.J.; Chlebowski, R.T.; Pan, K.; Stambolic, V.; Dowling, R.J.O. Association of Obesity-Related Metabolic Disruptions with Cancer Risk and Outcome. J. Clin. Oncol. 2016, 34, 4249–4255. [Google Scholar] [CrossRef] [PubMed]
- Mayers, J.R.; Torrence, M.E.; Danai, L.v.; Papagiannakopoulos, T.; Davidson, S.M.; Bauer, M.R.; Lau, A.N.; Ji, B.W.; Dixit, P.D.; Hosios, A.M.; et al. Tissue of Origin Dictates Branched-Chain Amino Acid Metabolism in Mutant Kras-Driven Cancers. Science 2016, 353, 1161–1165. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.M.; Kim, J.H.; Baik, S.J.; Chun, J.; Youn, Y.H.; Park, H. Sarcopenia and Sarcopenic Obesity as Novel Risk Factors for Gastric Carcinogenesis: A Health Checkup Cohort Study. Front. Oncol. 2019, 9, 1249. [Google Scholar] [CrossRef]
- Kang, R.; Loux, T.; Tang, D.; Schapiro, N.E.; Vernon, P.; Livesey, K.M.; Krasinskas, A.; Lotze, M.T.; Zeh, H.J. The Expression of the Receptor for Advanced Glycation Endproducts (RAGE) Is Permissive for Early Pancreatic Neoplasia. Proc. Natl. Acad. Sci. USA 2012, 109, 7031–7036. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Filipov, N.M.; Guo, T.L. Dietary Glycation Products Regulate Immune Homeostasis: Early Glycation Products Promote Prostate Cancer Cell Proliferation through Modulating Macrophages. Mol. Nutr. Food Res. 2018, 62, 1700641. [Google Scholar] [CrossRef]
- Kataoka, K.; Ono, T.; Murata, H.; Morishita, M.; Yamamoto, K.I.; Sakaguchi, M.; Huh, N.H. S100A7 Promotes the Migration and Invasion of Osteosarcoma Cells via the Receptor for Advanced Glycation End Products. Oncol. Lett. 2012, 3, 1149–1153. [Google Scholar] [CrossRef]
- Foster, D.; Spruill, L.; Walter, K.R.; Nogueira, L.M.; Fedarovich, H.; Turner, R.Y.; Ahmed, M.; Salley, J.D.; Ford, M.E.; Findlay, V.J.; et al. AGE Metabolites: A Biomarker Linked to Cancer Disparity? Cancer Epidemiol. Biomark. Prev. 2014, 23, 2186–2191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rojas, A.; Añazco, C.; González, I.; Araya, P. Extracellular Matrix Glycation and Receptor for Advanced Glycation End-Products Activation: A Missing Piece in the Puzzle of the Association between Diabetes and Cancer. Carcinogenesis 2018, 39, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Quail, D.F.; Dannenberg, A.J. The Obese Adipose Tissue Microenvironment in Cancer Development and Progression. Nat. Rev. Endocrinol. 2019, 15, 139–154. [Google Scholar] [CrossRef]
- Howe, L.R.; Subbaramaiah, K.; Hudis, C.A.; Dannenberg, A.J. Molecular Pathways: Adipose Inflammation as a Mediator of Obesity-Associated Cancer. Clin. Cancer Res. 2013, 19, 6074–6083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amano, S.U.; Cohen, J.L.; Vangala, P.; Tencerova, M.; Nicoloro, S.M.; Yawe, J.C.; Shen, Y.; Czech, M.P.; Aouadi, M. Local Proliferation of Macrophages Contributes to Obesity-Associated Adipose Tissue Inflammation. Cell Metab. 2014, 19, 162–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, B.W.; Wang, X.; Zecchin, A.; Thienpont, B.; Cornelissen, I.; Kalucka, J.; García-Caballero, M.; Missiaen, R.; Huang, H.; Brüning, U.; et al. The Role of Fatty Acid β-Oxidation in Lymphangiogenesis. Nature 2017, 542, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Baek, A.E.; Yu, Y.R.A.; He, S.; Wardell, S.E.; Chang, C.Y.; Kwon, S.; Pillai, R.v.; McDowell, H.B.; Thompson, J.W.; Dubois, L.G.; et al. The Cholesterol Metabolite 27 Hydroxycholesterol Facilitates Breast Cancer Metastasis through Its Actions on Immune Cells. Nat. Commun. 2017, 8, 1–11. [Google Scholar] [CrossRef]
- Voisin, M.; de Medina, P.; Mallinger, A.; Dalenc, F.; Huc-Claustre, E.; Leignadier, J.; Serhan, N.; Soules, R.; Ségala, G.; Mougel, A.; et al. Identification of a Tumor-Promoter Cholesterol Metabolite in Human Breast Cancers Acting through the Glucocorticoid Receptor. Proc. Natl. Acad. Sci. USA 2017, 114, E9346–E9355. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; di Martino, J.S.; Bowman, R.L.; Campbell, N.R.; Baksh, S.C.; Vermot, T.S.; Kim, I.S.; Haldeman, P.; Mondal, C.; Gonzales, V.Y.; et al. Adipocyte-Derived Lipids Mediate Melanoma Progression via FATP Proteins HHS Public Access. Cancer Discov. 2018, 8, 1006–1025. [Google Scholar] [CrossRef] [Green Version]
- Frasor, J.; Danes, J.M.; Komm, B.; Chang, K.C.N.; Lyttle, C.R.; Katzenellenbogen, B.S. Profiling of Estrogen Up- and down-Regulated Gene Expression in Human Breast Cancer Cells: Insights into Gene Networks and Pathways Underlying Estrogenic Control of Proliferation and Cell Phenotype. Endocrinology 2003, 144, 4562–4574. [Google Scholar] [CrossRef]
- Rothenberger, N.J.; Somasundaram, A.; Stabile, L.P. The Role of the Estrogen Pathway in the Tumor Microenvironment. Int. J. Mol. Sci. 2018, 19, 611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalamaga, M. Interplay of Adipokines and Myokines in Cancer Pathophysiology: Emerging Therapeutic Implications. World J. Exp. Med. 2013, 3, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Korta, P.; Pocheć, E.; Mazur-Biały, A. Irisin as a Multifunctional Protein: Implications for Health and Certain Diseases. Medicina 2019, 55, 485. [Google Scholar] [CrossRef] [Green Version]
- Marengo, A.; Rosso, C.; Bugianesi, E. Liver Cancer: Connections with Obesity, Fatty Liver, and Cirrhosis. Annu. Rev. Med. 2016, 67, 103–117. [Google Scholar] [CrossRef] [PubMed]
- Giudice, J.; Taylor, J.M. Muscle as a Paracrine and Endocrine Organ. Curr. Opin. Pharmacol. 2017, 34, 49–55. [Google Scholar] [CrossRef]
- Atkins, J.L.; Wannamathee, S.G. Sarcopenic Obesity in Ageing: Cardiovascular Outcomes and Mortality. Br. J. Nutr. 2020, 124, 1102–1113. [Google Scholar] [CrossRef]
- Lavie, C.J.; de Schutter, A.; Parto, P.; Jahangir, E.; Kokkinos, P.; Ortega, F.B.; Arena, R.; Milani, R.V. Obesity and Prevalence of Cardiovascular Diseases and Prognosis-The Obesity Paradox Updated. Prog. Cardiovasc. Dis. 2016, 58, 537–547. [Google Scholar] [CrossRef] [Green Version]
- Oreopoulos, A.; Padwal, R.; Kalantar-Zadeh, K.; Fonarow, G.C.; Norris, C.M.; McAlister, F.A. Body Mass Index and Mortality in Heart Failure: A Meta-Analysis. Am. Heart J. 2008, 156, 13–22. [Google Scholar] [CrossRef] [Green Version]
- Alalwan, T.A. Phenotypes of Sarcopenic Obesity: Exploring the Effects on Peri-Muscular Fat, the Obesity Paradox, Hormone-Related Responses and the Clinical Implications. Geriatrics 2020, 5, 8. [Google Scholar] [CrossRef] [Green Version]
- Carbone, S.; Canada, J.M.; Billingsley, H.E.; Siddiqui, M.S.; Elagizi, A.; Lavie, C.J. Obesity paradox in cardiovascular disease: Where do we stand? Vasc. Health Risk Manag. 2019, 15, 89–100. [Google Scholar] [CrossRef] [Green Version]
- Dominguez, L.J.; Barbagallo, M. The Cardiometabolic Syndrome and Sarcopenic Obesity in Older Persons. J. Cardiometab. Syndr. 2007, 2, 183–189. [Google Scholar] [CrossRef]
- Chung, J.Y.; Kang, H.T.; Lee, D.C.; Lee, H.R.; Lee, Y.J. Body Composition and Its Association with Cardiometabolic Risk Factors in the Elderly: A Focus on Sarcopenic Obesity. Arch. Gerontol. Geriatr. 2013, 56, 270–278. [Google Scholar] [CrossRef]
- Tabibi, H.; As’Habi, A.; Najafi, I.; Hedayati, M. Prevalence of Dynapenic Obesity and Sarcopenic Obesity and Their Associations with Cardiovascular Disease Risk Factors in Peritoneal Dialysis Patients. Kidney Res. Clin. Pract. 2018, 37, 404–413. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.N.; Choi, K.M. The Implications of Sarcopenia and Sarcopenic Obesity on Cardiometabolic Disease. J. Cell. Biochem. 2015, 116, 1171–1178. [Google Scholar] [CrossRef]
- Chuang, S.Y.; Hsu, Y.Y.; Chen, R.C.Y.; Liu, W.L.; Pan, W.H. Abdominal Obesity and Low Skeletal Muscle Mass Jointly Predict Total Mortality and Cardiovascular Mortality in an Elderly Asian Population. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 1049–1055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukuda, T.; Bouchi, R.; Takeuchi, T.; Tsujimoto, K.; Minami, I.; Yoshimoto, T.; Ogawa, Y. Sarcopenic Obesity Assessed Using Dual Energy X-Ray Absorptiometry (DXA) Can Predict Cardiovascular Disease in Patients with Type 2 Diabetes: A Retrospective Observational Study. Cardiovasc. Diabetol. 2018, 17, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, S.M.; Yoon, J.W.; Ahn, H.Y.; Kim, S.Y.; Lee, K.H.; Shin, H.; Choi, S.H.; Park, K.S.; Jang, H.C.; Lim, S. Android Fat Depot Is More Closely Associated with Metabolic Syndrome than Abdominal Visceral Fat in Elderly People. PLoS ONE 2011, 6, e27694. [Google Scholar] [CrossRef] [PubMed]
- Lee, K. Sarcopenic Obesity and 10-Year Cardiovascular Disease Risk Scores in Cancer Survivors and Non-Cancer Participants Using a Nationwide Survey. Eur. J. Cancer Care 2021, 30, e13365. [Google Scholar] [CrossRef] [PubMed]
- Farmer, R.E.; Mathur, R.; Schmidt, A.F.; Bhaskaran, K.; Fatemifar, G.; Eastwood, S.v.; Finan, C.; Denaxas, S.; Smeeth, L.; Chaturvedi, N. Associations between Measures of Sarcopenic Obesity and Risk of Cardiovascular Disease and Mortality: A Cohort Study and Mendelian Randomization Analysis Using the UK Biobank. J. Am. Heart Assoc. 2019, 8, e011638. [Google Scholar] [CrossRef]
- Cho, H.W.; Chung, W.; Moon, S.; Ryu, O.H.; Kim, M.K.; Kang, J.G. Effect of Sarcopenia and Body Shape on Cardiovascular Disease According to Obesity Phenotypes. Diabetes Metab. J. 2021, 45, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Santana, N.d.M.; Mendes, R.M.L.; da Silva, N.F.; Pinho, C.P.S. Sarcopenia and Sarcopenic Obesity as Prognostic Predictors in Hospitalized Elderly Patients with Acute Myocardial Infarction. Einstein 2019, 17, eAO4632. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, M.; Kamiya, K.; Matsunaga, A.; Kitamura, T.; Hamazaki, N.; Matsuzawa, R.; Nozaki, K.; Tanaka, S.; Nakamura, T.; Maekawa, E.; et al. Prognostic Value of Sarcopenic Obesity Estimated by Computed Tomography in Patients with Cardiovascular Disease and Undergoing Surgery. J. Cardiol. 2019, 74, 273–278. [Google Scholar] [CrossRef] [PubMed]
- del Fabbro, E.; Parsons, H.; Warneke, C.L.; Pulivarthi, K.; Litton, J.K.; Dev, R.; Palla, S.L.; Brewster, A.; Bruera, E. The Relationship between Body Composition and Response to Neoadjuvant Chemotherapy in Women with Operable Breast Cancer. Oncologist 2012, 17, 1240–1245. [Google Scholar] [CrossRef] [Green Version]
- Palmela, C.; Velho, S.; Agostinho, L.; Branco, F.; Santos, M.; Santos, M.P.C.; Oliveira, M.H.; Strecht, J.; Maio, R.; Cravo, M.; et al. Body Composition as a Prognostic Factor of Neoadjuvant Chemotherapy Toxicity and Outcome in Patients with Locally Advanced Gastric Cancer. J. Gastric Cancer 2017, 17, 74–87. [Google Scholar] [CrossRef] [Green Version]
- Gruber Id, E.S.; Id, G.J.; Tamandl, D.; Gnant, M.; Schindl, M.; Sahora, K. Sarcopenia and Sarcopenic Obesity Are Independent Adverse Prognostic Factors in Resectable Pancreatic Ductal Adenocarcinoma. PLoS ONE 2019, e0215915. [Google Scholar] [CrossRef]
- Rodrigues, V.; Landi, F.; Castro, S.; Mast, R.; Rodríguez, N.; Gantxegi, A.; Pradell, J.; López-Cano, M.; Armengol, M. Is Sarcopenic Obesity an Indicator of Poor Prognosis in Gastric Cancer Surgery? A Cohort Study in a Western Population. J. Gastrointest. Surg. 2020. [Google Scholar] [CrossRef]
- Flegal, K.M.; Graubard, B.I.; Williamson, D.F.; Gail, M.H. Cause-Specific Excess Deaths Associated with Underweight, Overweight, and Obesity. J. Am. Med. Assoc. 2007, 298, 2028–2037. [Google Scholar] [CrossRef] [Green Version]
- van Kruijsdijk, R.C.M.; van der Wall, E.; Visseren, F.L.J. Obesity and Cancer: The Role of Dysfunctional Adipose Tissue. Cancer Epidemiol. Biomark. Prev. 2009, 18, 2569–2578. [Google Scholar] [CrossRef] [Green Version]
- Clarke, M.A.; Fetterman, B.; Cheung, L.C.; Wentzensen, N.; Gage, J.C.; Katki, H.A.; Befano, B.; Demarco, M.; Schussler, J.; Kinney, W.K.; et al. Epidemiologic Evidence That Excess Body Weight Increases Risk of Cervical Cancer by Decreased Detection of Precancer. J. Clin. Oncol 2018, 36, 1184–1191. [Google Scholar] [CrossRef]
- American Institute for Cancer Research; World Cancer Research Fund. Available online: https://www.aicr.org/wp-content/uploads/2020/01/Body-fatness-and-weight-gain_0.pdf (accessed on 21 March 2021).
- Borges, T.C.; Gomes, T.L.N.; Pimentel, G.D. Corrigendum to “Sarcopenia as a Predictor of Nutritional Status and Comorbidities in Hospitalized Patients with Cancer: A Cross-Sectional Study” [Nutrition 2020;73:110703]. Nutrition 2021, 81, 110842. [Google Scholar] [CrossRef]
- Borges, T.C.; Gomes, T.L.; Pichard, C.; Laviano, A.; Pimentel, G.D. High Neutrophil to Lymphocytes Ratio Is Associated with Sarcopenia Risk in Hospitalized Cancer Patients. Clin. Nutr. 2021, 40, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Prado, C.M.; Lieffers, J.R.; McCargar, L.J.; Reiman, T.; Sawyer, M.B.; Martin, L.; Baracos, V.E. Prevalence and Clinical Implications of Sarcopenic Obesity in Patients with Solid Tumours of the Respiratory and Gastrointestinal Tracts: A Population-Based Study. Lancet Oncol. 2008, 9, 629–635. [Google Scholar] [CrossRef]
- Prado, C.M.M.; Lieffers, J.R.; Bowthorpe, L.; Baracos, V.E.; Mourtzakis, M.; McCargar, L.J. Sarcopenia and Physical Function in Overweight Patients with Advanced Cancer. Can. J. Diet. Pract. Res. 2013, 74, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Lodewick, T.M.; Roeth, A.A.J.; Damink, S.W.M.O.; Alizai, P.H.; van Dam, R.M.; Gassler, N.; Schneider, M.; Dello, S.A.W.G.; Schmeding, M.; Dejong, C.H.C.; et al. Sarcopenia, Obesity and Sarcopenic Obesity: Effects on Liver Function and Volume in Patients Scheduled for Major Liver Resection. J. Cachexia Sarcopenia Muscle 2015, 6, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.; Birdsell, L.; MacDonald, N.; Reiman, T.; Clandinin, M.T.; McCargar, L.J.; Murphy, R.; Ghosh, S.; Sawyer, M.B.; Baracos, V.E. Cancer Cachexia in the Age of Obesity: Skeletal Muscle Depletion Is a Powerful Prognostic Factor, Independent of Body Mass Index. J. Clin. Oncol. 2013, 31, 1539–1547. [Google Scholar] [CrossRef]
- Ligibel, J.A.; Schmitz, K.H.; Berger, N.A. Sarcopenia in Aging, Obesity, and Cancer. Transl. Cancer Res. 2020, 9, 5760–5771. [Google Scholar] [CrossRef]
- Peng, P.D.; van Vledder, M.G.; Tsai, S.; de Jong, M.C.; Makary, M.; Ng, J.; Edil, B.H.; Wolfgang, C.L.; Schulick, R.D.; Choti, M.A.; et al. Sarcopenia Negatively Impacts Short-Term Outcomes in Patients Undergoing Hepatic Resection for Colorectal Liver Metastasis. HPB 2011, 13, 439–446. [Google Scholar] [CrossRef] [Green Version]
- Reisinger, K.W.; Bosmans, J.W.A.M.; Uittenbogaart, M.; Alsoumali, A.; Poeze, M.; Sosef, M.N.; Derikx, J.P.M. Loss of skeletal muscle mass during neoadjuvant chemoradiotherapy predicts postoperative mortality in esophageal cancer surgery. Ann. Surg. Oncol. 2015, 22, 4445–4452. [Google Scholar] [CrossRef] [Green Version]
- Anandavadivelan, P.; Brismar, T.B.; Nilsson, M.; Johar, A.M.; Martin, L. Sarcopenic Obesity: A Probable Risk Factor for Dose Limiting Toxicity during Neo-Adjuvant Chemotherapy in Oesophageal Cancer Patients. Clin. Nutr. 2016, 35, 724–730. [Google Scholar] [CrossRef]
- Malietzis, G.; Currie, A.C.; Athanasiou, T.; Johns, N.; Anyamene, N.; Glynne-Jones, R.; Kennedy, R.H.; Fearon, K.C.H.; Jenkins, J.T. Influence of Body Composition Profile on Outcomes Following Colorectal Cancer Surgery. Br. J. Surg. 2016, 103, 572–580. [Google Scholar] [CrossRef]
- Han, J.S.; Ryu, H.; Park, I.J.; Kim, K.W.; Shin, Y.; Kim, S.O.; Lim, S.-B.; Kim, C.W.; Yoon, Y.S.; Lee, J.L.; et al. Association of body composition with long-term survival in non-metastatic rectal cancer patients. Cancer Res. Treat. 2020, 52, 563–572. [Google Scholar] [CrossRef] [Green Version]
- Tan, B.H.L.; Birdsell, L.A.; Martin, L.; Baracos, V.E.; Fearon, K.C.H. Sarcopenia in an Overweight or Obese Patient Is an Adverse Prognostic Factor in Pancreatic Cancer. Clin. Cancer Res. 2009, 15, 6973–6979. [Google Scholar] [CrossRef] [Green Version]
- Rollins, K.E.; Tewari, N.; Ackner, A.; Awwad, A.; Madhusudan, S.; Macdonald, I.A.; Fearon, K.C.H.; Lobo, D.N. The Impact of Sarcopenia and Myosteatosis on Outcomes of Unresectable Pancreatic Cancer or Distal Cholangiocarcinoma. Clin. Nutr. 2016, 35, 1103–1109. [Google Scholar] [CrossRef]
- Kobayashi, A.; Kaido, T.; Hamaguchi, Y.; Okumura, S.; Shirai, H.; Yao, S.; Kamo, N.; Yagi, S.; Taura, K.; Okajima, H.; et al. Impact of Sarcopenic Obesity on Outcomes in Patients Undergoing Hepatectomy for Hepatocellular Carcinoma. Ann. Surg. 2019, 269, 924–931. [Google Scholar] [CrossRef]
- Okumura, S.; Kaido, T.; Hamaguchi, Y.; Kobayashi, A.; Shirai, H.; Yao, S.; Yagi, S.; Kamo, N.; Hatano, E.; Okajima, H.; et al. Visceral Adiposity and Sarcopenic Visceral Obesity Are Associated with Poor Prognosis After Resection of Pancreatic Cancer. Ann. Surg. Oncol. 2017, 24, 3732–3740. [Google Scholar] [CrossRef] [PubMed]
- Cushen, S.J.; Power, D.G.; Murphy, K.P.; McDermott, R.; Griffin, B.T.; Lim, M.; Daly, L.; MacEneaney, P.; O’ Sullivan, K.; Prado, C.M.; et al. Impact of Body Composition Parameters on Clinical Outcomes in Patients with Metastatic Castrate-Resistant Prostate Cancer Treated with Docetaxel. Clin. Nutr. ESPEN 2016, 13, e39–e45. [Google Scholar] [CrossRef] [PubMed]
- Lou, N.; Chi, C.H.; Chen, X.D.; Zhou, C.J.; Wang, S.L.; Zhuang, C.L.; Shen, X. Sarcopenia in Overweight and Obese Patients Is a Predictive Factor for Postoperative Complication in Gastric Cancer: A Prospective Study. Eur. J. Surg. Oncol. 2017, 43, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Baracos, V.; Bertz, H.; Bozzetti, F.; Calder, P.C.; Deutz, N.E.P.; Erickson, N.; Laviano, A.; Lisanti, M.P.; Lobo, D.N.; et al. ESPEN expert group recommendations for action against cancer-related malnutrition. Clin. Nutr. 2017, 36, 1187–1196. [Google Scholar] [CrossRef] [Green Version]
- Batsis, J.A.; Mackenzie, T.A.; Emeny, R.T.; Lopez-Jimenez, F.; Bartels, S.J. Low Lean Mass with and Without Obesity, and Mortality: Results from the 1999–2004 National Health and Nutrition Examination Survey. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2017, 72, 1445–1451. [Google Scholar] [CrossRef] [Green Version]
- Dalal, S.; Hui, D.; Bidaut, L.; Lem, K.; del Fabbro, E.; Crane, C.; Reyes-Gibby, C.C.; Bedi, D.; Bruera, E. Relationships among Body Mass Index, Longitudinal Body Composition Alterations, and Survival in Patients with Locally Advanced Pancreatic Cancer Receiving Chemoradiation: A Pilot Study. J. Pain Symptom Manag. 2012, 44, 181–191. [Google Scholar] [CrossRef]
- Psutka, S.P.; Boorjian, S.A.; Moynagh, M.R.; Schmit, G.D.; Frank, I.; Carrasco, A.; Stewart, S.B.; Tarrell, R.; Thapa, P.; Tollefson, M.K. Mortality after Radical Cystectomy: Impact of Obesity versus Adiposity after Adjusting for Skeletal Muscle Wasting. J. Urol. 2015, 193, 1507–1513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pecorelli, N.; Carrara, G.; de Cobelli, F.; Cristel, G.; Damascelli, A.; Balzano, G.; Beretta, L.; Braga, M. Effect of Sarcopenia and Visceral Obesity on Mortality and Pancreatic Fistula Following Pancreatic Cancer Surgery. Br. J. Surg. 2016, 103, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Caan, B.J.; Feliciano, E.M.C.; Prado, C.M.; Alexeeff, S.; Kroenke, C.H.; Bradshaw, P.; Quesenberry, C.P.; Weltzien, E.K.; Castillo, A.L.; Olobatuyi, T.A.; et al. Association of Muscle and Adiposity Measured by Computed Tomography with Survival in Patients with Nonmetastatic Breast Cancer. JAMA Oncol. 2018, 4, 798–804. [Google Scholar] [CrossRef]
- Gallo, M.; Adinolfi, V.; Barucca, V.; Prinzi, N.; Renzelli, V.; Barrea, L.; di Giacinto, P.; Ruggeri, R.M.; Sesti, F.; Arvat, E.; et al. Expected and Paradoxical Effects of Obesity on Cancer Treatment Response. Rev. Endocr. Metab. Disord. 2020. [Google Scholar] [CrossRef]
- Amundson, D.E.; Djurkovic, S.; Matwiyoff, G.N. The Obesity Paradox. Crit. Care Clin. 2010, 26, 583–596. [Google Scholar] [CrossRef]
- Myers, J.; Lata, K.; Chowdhury, S.; McAuley, P.; Jain, N.; Froelicher, V. The Obesity Paradox and Weight Loss. Am. J. Med. 2011, 124, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Apollos, J.R.; Sami, S.; Prasanth, M.N.; Jeyakumar, J.; McFadyen, A.K. Pre-Diagnostic Delays Caused by Gastrointestinal Investigations Do Not Affect Outcomes in Pancreatic Cancer. Ann. Med. Surg. 2018, 34, 66–70. [Google Scholar] [CrossRef]
- American Cancer Society. Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/anual-cancer-facts-and-figures-2021.pdf (accessed on 21 March 2021).


{kind=link}
| Muscle or Lean Mass | Muscle Strength | Physical Performance | Obesity/Adiposity |
|---|---|---|---|
| CT [24,25] | Handgrip strength [26,27] | Gait speed [13,28] | BMI [25,26] |
| DXA [14,29] | 5 times stand test [13] | Timed up-and-go test [13] | % Body fat [14,29] |
| BIA [29,30] | Short physical performance battery [13] | Waist circumference [30,31] | |
| Ultrasonography [22] | 400-m walk test [13] | Visceral fat area [32,33] | |
| Anthropometry [21,30] | Fat mass index [8,30] |
| Author/Year | Setting/Population | Outcome(s) | Sarcopenic Obesity | Adjustment for | Association Sarcopenic Obesity and CVD | Summary |
|---|---|---|---|---|---|---|
| Cross-Sectional Studies | ||||||
| [84] | Korean National Health Examination and Nutrition Survey (KNHANES)/2943 subjects (1250 men and 1693 women) 60 years + older | Cardiometabolic risk factors, metabolic syndrome | Appendicular skeletal muscle mass (ASM) divided by weight BMI ≥ 25 kg/m2 | - | MetS prevalence Sarcopenic obese Men: 60.9% Women: 71.1% Non-sarcopenic, non-obese Men: 11.6 Women: 32.4 | Sarcopenic obesity was more closely associated with insulin resistance, metabolic syndrome, and cardiovascular disease (CVD) risk factors than any other group |
| [85] | 79 peritoneal dialysis patients | CVD risk factors | Low SMM plus low muscle function Percentage of total body fat | - | mean ± SD Hs-CRP Sarcopenic obese: 8.0 ± 0.3 non-sarcopenic obese: 6.8 ± 0.7 Triglyceride Sarcopenic obese: 234.0 ± 61.0 non-obese sarcopenic: 186.0 ± 28.0 non-sarcopenic obese: 185.0 ± 30.0 | Sarcopenic obese subjects had higher levels of hs-CRP and triglyceride compared with non-sarcopenic obese subjects No significant difference was found for total cholesterol, LDL, HDL, LPa, MDA, and sICAMI |
| [93] | 99 older adults patients with acute myocardial infarction | Cardiovascular risk and prognostic markers | Loss of muscle mass, loss of muscle strength and poor physical performance Abdominal obesity using sex-specific WC cutoff points | - | Median (IQR) Thrombolysis in myocardial infarction Sarcopenic obese: 4.0 (2.0–6.0) Creatine kinase MB isoenzyme Sarcopenic obese: 4.2 (1.4–17.4) Troponin Sarcopenic obese: 0.06 (0.02–0.86) | Sarcopenic obesity affected approximately one-third of patients and was not associated with any of the prognostic predictors |
| [92] | National Health and Nutrition Examination Survey 25,270 adults | CVD | Sarcopenia sex-specific ASMI cutoff points based on the revised European consensus BMI ≥ 25 kg/m2 | Age, sex, ethnicity, and smoking status | OR (95% CI): Sarcopenic obese, metabolically healthy: 8.59 (2.63, 28.04) Sarcopenic obese, metabolically unhealthy: 8.12 (4.04, 16.32) | Sarcopenic obesity was associated with increased risk of CVD |
| Cohort Studies | ||||||
| [30] | British Regional Heart Study/4252 men aged 60–79 years 11.3 years follow-up | CHD events CVD events | Low-fat free mass index (FFMI) High-percentile points of fat mass index (FMI) corresponding to the WC obesity | Age, smoking, alcohol, occupational social class, physical activity | HR (95% CI) CHD events 1.13 (0.82–1.56) CVD events 1.01 (0.79–1.29) | No significant association for any outcome |
| [88] | 716 Japanese diabetic patients (mean age 65 ± 13 years; 47.0% female) 2.6 years follow-up | CVD | The coexistence of low SMI and obesity determined by android to gynoid ratio | HDL cholesterol, HbA1c, eGFR, use ACEIs or ARBs, use DPP4 inhibitors, history of CVD | HR (95% CI) Sarcopenic obesity: 2.63 (1.10–6.28) | Sarcopenic obesity was a predictor of incident CVD |
| [91] | UK Biobank/452 931 men and women aged 40 and 69 years 5.1 y follow-up | CHD events and CVD events and | Handgrip strength Obesity = BMI > 0 Obesity = WHR ≥ 0.95 in men and ≥ 0.80 in women | Age, sex, ethnicity, smoking, alcohol consumption, diabetes, physical activity, deprivation | HR (95% CI) Sarcopenic obesity (BMI) CHD events NO history: 1.79 (1.54, 2.08) History: 1.52 (1.37, 1.70) CVD events NO history: 1.24 (1.11, 1.38) History: 1.10 (0.97, 1.24) Sarcopenic obesity (WHR) CVD events NO history: 1.30 (1.22, 1.39) History: 1.24 (1.15, 1.34) | Sarcopenic obese subjects greater risk of CHD events and mortality irrespective of their CVD history Regarding CVD events and mortality, there was a positive association only in those who did not have a history of CVD |
| [90] | Korea National Health and Nutrition Examination Survey/19,019 individuals 10 y follow-up | 10-year CVD risk scores based on Framingham risk model | handgrip strength, BMI | Sociodemographic dietary intake time cancer diagnosis current cancer therapy (in cancer survivors) | OR (95% CI) Cancer survivors 3.61 (1.60, 8.13) Noncancer participants 4.24 (3.44, 5.22) | Cancer survivors and noncancer with sarcopenic obesity had increased 10-year CVD risk scores |
| Mortality–Cohort Studies | ||||||
| [30] | British Regional Heart Study/4252 men aged 60–79 years 11.3 years follow-up | CVD mortality | Low-fat free mass index (FFMI) and high percentile point of fat mass index (FMI) corresponding to the WC obesity | Age, smoking, alcohol, occupational social class, physical activity | HR (95% CI) CVD mortality 1.11 (0.81–1.53) | No significant association |
| [87] | Elderly Nutrition and Health Survey/1485 elderly individuals aged over 65 years 9.2 years follow-up | Cardiovascular mortality | Low skeletal muscle mass index and abdominal obesity plus hypertriglyceridemia (>150 mg/dL) | Age, gender, BMI, high blood pressure, low HDLC, included hs-CRP, eGFR, comorbidities, smoking, drinking, physical activity | 11.3% (n = 168) CVD death recorded. HR (95% CI) 3.39 (1.57, 7.32) | Sarcopenic obese individuals had the highest risk of CVD mortality |
| [94] | A total of 664 consecutive cardiovascular surgery patients with a mean age of 65.8 ± 12.7 years | All-cause mortality as a prognosis | Psoas muscle attenuation (MA) and visceral adipose tissue (VAT) (abdominal obesity defined by WC) | EuroSCORE | HR (95% CI) 3.04 (1.25, 7.40) | Sarcopenic obesity was associated with all-cause mortality in patients undergoing cardiovascular surgery |
| [91] | UK Biobank/452 931 men and women aged 40 and 69 years 5.1 years follow-up | CHD events and CHD mortality, CVD events and CVD mortality | Handgrip strength Obesity = BMI >30 or waist to hip ratio ≥0.95 in men and ≥0.80 in women | Age, sex, ethnicity, smoking, alcohol consumption, diabetes, physical activity, deprivation | HR (95% CI) Sarcopenic obesity BMI CHD mortality NO history: 1.74 (1.26, 2.42) History: 1.53 (1.22, 1.93) CVD mortality NO history: 1.39 (1.07, 1.81) History: 1.14 (0.87, 1.48) Sarcopenic obesity WHR CVD mortality NO history of CVD: 2.04 (1.74, 2.38) History of CVD: 1.82 (1.55, 2.14) | Sarcopenic obese-associated CHD mortality irrespective of their CVD history CVD mortality associated only with those who did not have a history of CVD |
| Author, Year, Country | Study Design | Local and Stage of Tumor | Age (n;% Sex) | SO Definition | Prevalence |
|---|---|---|---|---|---|
| Digestive System | |||||
| [105] Canada | Retrospective cohort | Gastrointestinal tract or respiratory system/I, II, III e IV (mostly III and IV) | 35 to 88 years-old (n = 250; 54.4% male) | CT L3 SMI: ♀ ≤ 38.5 cm2/m2 and ♂ ≤ 52.4 cm2/m2; obesity: BMI ≥ 30 kg/m2 | 15% |
| [110] USA | Retrospective cohort | Colorectal/advanced | 58 ± 12 years-old (n = 259; 60.0% male) | Sarcopenia TPA: ≤ 500 mm2/m2; obesity: BMI ≥3 0 kg/m2 | 2% |
| [24] The Netherlands | Retrospective cohort | Colorectal/advanced | 24 to 86 years-old (n = 171; 60.8% male) | CT L3 SMI: ♀ < 41 cm2/m2 and ♂ < 43 cm2/m2 (BMI < 25 kg/m2) and < 53 cm2/m2 (BMI ≥ 25 kg/m2); obesity: % body fat > 44.4 ♀ and > 35.7 ♂ | 28.7% |
| [111] The Netherlands | Prospective cohort | Esophagus/I, II, III, and IV | 63 ± 10 years-old (n = 123; 82.1% male) | CT L3 SMI: ♀ ≤ 38.5 cm2/m2 and ♂ ≤ 52.4 cm2/m2; obesity: BMI > 30 kg/m2 or visceral adiposity (L3) | 2% (Sarcopenic obesity) 17% (Sarcopenic visceral obesity) |
| [107] Germany | Prospective cohort | Colorectal, cholangiocarcinoma, and liver/not specified | 28 to 82 years-old (n = 80; 63.75% male) | CT L3 SMI: ♀ < 41 cm2/m2 and ♂ < 43 cm2/m2 (BMI < 25 kg/m2) and < 53 cm2/m2 (BMI ≥ 25 kg/m2); obesity: % body fat > 44.4 for ♀ and > 35.7 for ♂ | 22% |
| [112] Sweden | Retrospective cohort | Esophagus/I, II, III, and IV (mostly advanced) | 47 to 83 years-old (n = 72; 85.0% male) | CT L3 SMI: ♀ ≤ 38.5 cm2/m2 and ♂ ≤ 52.4 cm2/m2; obesity: BMI ≥ 25 kg/m2 | 14% |
| [113] UK | Prospective database study | Colorectal/I, II, III, and IV | 61 to 77 years-old (n = 805; 58.6% male) | CT L3 SMI: ♀ ≤ 38.5 cm2/m2 and ♂ ≤ 52.4 cm2/m2; obesity: BMI ≥ 30 kg/m2 | 10% |
| [32] China | Prospective study | Stomach/I, II, III, and IV | 56 to 78 years-old (n = 636; 75.2% male) | Sarcopenia: L3 SMI ♂: ≤ 40.8 cm2/m2 and ♀: 34.9 cm2/m2; obesity: VFA ≥ 132.6 cm2 for ♂ and 91.5 cm2 for ♀ | 6.1% |
| [59] Korea | Cohort Study | Stomach (pre-cancerous and cancerous lesions) | 49.1 ± 11.6 years (n = 8356; 55.9% male) | SMI estimated by ASM/body weight× 100 (%): 29.3% in ♂ and 26.7% in ♀; obesity: BMI ≥ 25 kg/m2 | Pre-cancer: 14.6% Cancer 41.7% |
| [114] | Prospective study | nonmetastatic Rectal/I, II and III | 59.0 ± 10.9 years (n = 1384; 64.2% male) | CT L3 SMI: ♀ ≤ 38.5 cm2/m2 and ♂ ≤ 52.4 cm2/m2; obesity: BMI > 25 kg/m2 | 22.2% |
| [98] Spain | Cohort Study | Stomach/I, II, and III (>50% III) | 27 to 88 years-old (n = 198; 57.6% male) | CT L3 SMI: ♀ ≤ 38.5 cm2/m2 and ♂ ≤ 52.4 cm2/m2; obesity: VFA > 163.8 cm2 for ♂ and > 80.1 cm2 for ♀ | 28% |
| Endocrine System | |||||
| [115] Canada | Retrospective cohort | Pancreas/II to IV (mostly IV) | 64.4 ± 9.3 years-old (n = 111; 53.2% female) | CT L3 SMI: ♀ ≤ 38.5 cm2/m2 and ♂ ≤ 52.4 cm2/m2; obesity: BMI ≥ 25 kg/m2 | 16.2% |
| [116] UK | Retrospective cohort | Pancreas/advanced | Palliative chemo: n = 98; 56.1% male; 64.8 ± 8.7 years; No chemotherapy: n = 130; 53.1% male; 72.9 ± 11.1 | CT L3 SMI: ♀ < 41 cm2/m2 and ♂ < 43 cm2/m2 (BMI < 25 kg/m2) and < 53 cm2/m2 (BMI ≥ 25 kg/m2); obesity: BMI ≥ 30 kg/m2 | 25% |
| [117] Japan | Cross-sectional study | Liver/I, II, III, and IV | 73.6 ± 7.8 years-old among sarcopenic obese | SMI ♂: 40.31 cm2/m2 and ♀: 30.88 cm2/m2; obesity: VFA ≥ 100 cm2 | 7% |
| [118] Japan | Retrospective study | Pancreas/not reported | 68 years-old (n = 301; 55.8% male) | Sarcopenia: SMI ♂: 47.1 cm2/m2 and ♀: 36.6 cm2/m2; obesity: VFA ≥ 100 cm2 | 18.9% |
| [97] Austria | Retrospective analysis | Pancreas/III | 34 to 87 years-old (n = 133; 51.1% male) | CT L3 SMI: ♀ ≤ 38.5 cm2/m2 and ♂ ≤ 52.4 cm2/m2; obesity: BMI ≥ 25 kg/m2 | 25.6% |
| Genitourinary System | |||||
| [119] Republic of Ireland | Retrospective study | Prostate/not reported | 69 ± 8.3 years-old (n = 63; 100% male) | CT L3 SMI: ♀ < 41 cm2/m2 e ♂ < 43 cm2/m2 (BMI < 25 kg/m2) and < 53 cm2/m2 (BMI ≥ 25 kg/m2) | 12.6% |
| Integumentary System | |||||
| [95] USA | Retrospective Cohort | Breast/I, II, and III | Not reported (n = 67; 100% female) | CT L3 SMI: ♀ ≤ 38.5 cm2/m2 and ♂ ≤ 52.4 cm2/m2; obesity: BMI ≥ 30 kg/m2 | 2.3% |
| [9] The Netherlands | Retrospective study | Breast/not reported | 58.8 ± 11.3 years-old (n = 166; 100% female) | CT L3 SMI: ♀ < 41 cm2/m2 and ♂ < 43 cm2/m2 (BMI < 25 kg/m2) and < 53 cm2/m2 (BMI ≥ 25 kg/m2) | 7.2% |
| Author, Year | Study Design and Sample | Implications on Clinic Features and Survival |
|---|---|---|
| Functional Outcome | ||
| [105] | Retrospective cohort 35 to 88 y (n = 250; 54.4% male) | 47.0% of individuals with SO presented decreased functional status |
| [106] | Cross-sectional study 64.5 ± 9.5 y (n = 28; 68.0% male) | Decreased handgrip strength in men |
| Clinical and Surgical Outcome | ||
| [110] | Retrospective cohort 58 ± 12 y (n = 259; 60.0% male) | Prolonged hospitalization and higher postoperative complication rates, compared to non-sarcopenic |
| [95] | Retrospective cohort Age not reported (n = 67; 100% female) | Poorer prognostic compared to normal BMI. |
| [106] | Cross-sectional study 64.5 ± 9.5 y (n = 28; 68.0% male) | Men with SO showed more symptoms at Edmonton’s symptom assessment system (ESAS) compared to non-sarcopenic |
| [24] | Retrospective cohort 24 to 86 y (n = 171; 60.8% male) | Higher hospital readmission than non-SO |
| [112] | Retrospective cohort 47 to 83 y (n = 72; 85.0% male) | SO individuals showed higher toxicity risk during chemotherapy |
| [113] | Prospective database study 61 to 77 y (n = 805; 58.6% male) | SO increased postoperative complications compared to low muscle mass non-obesity along the same period |
| [120] | Prospective study (n = 206; 78.15% male) | Sarcopenia in overweight/obese individuals associated with a 6-fold increased postoperative risk of complications, higher hospital costs, and higher hospital readmission in 30 days after gastrectomy (compared to non-sarcopenic) |
| [96] | Retrospective analysis of a cohort 68 ± 10 y (n = 47; 68.1% male) | SO a risk factor for chemo-related toxicity in gastric cancer patients, leading to a premature stop |
| [97] | Retrospective analysis 34 to 87 y (n = 133; 51.1% male) | Higher complication rates |
| [32] | Prospective study 56 to 78 y (n = 636; 75.2% male) | Higher risk of postoperative complications |
| [119] | Retrospective study 69 ± 8.3 y (n = 63; 100% male) | SO not associated with chemo-related toxicity in castration-resistant metastatic prostate cancer |
| [59] | Cohort study 49.1 ± 11.6 y (n = 8.356; 55.9% men) | SO associated with gastric cancer diagnosis |
| [98] | Cohort study 27 to 88 y (n = 198; 57.6% male) | SO not associated with poorer postoperative recovery in gastric cancer patients |
| Mortality/Survival Outcome | ||
| [105] | Retrospective cohort 35 to 88 y (n = 250; 54.4% male) | Shorter survival compared to non-sarcopenic. |
| [115] | Retrospective cohort 64.4 ± 9.3 y (n = 111; 53.2% female) | Survival 2.7-fold smaller in SO |
| [123] | Prospective cohort 42 to 81 y (n = 41; 56.0% female) | SO associated with a 4-fold higher risk of mortality |
| [116] | Retrospective cohort Palliative-chemo group (n = 98; 56.1% male): 64.8 ± 8.7 y No-chemo group (n = 130; 53.1% male): 72.9 ± 11.1 | SO associated with smaller survival rates |
| [111] | Prospective cohort 63 ± 10 y (n = 123; 82.1% male) | SO not associated with postoperative mortality. Chemoradiotherapy-related muscle loss predicted postoperative mortality |
| [107] | Prospective cohort (n = 80; 63.75% male) | SO not associated with higher mortality |
| [124] | Retrospective cohort study 63 to 78 y (n = 262; 85.9% male) | SO not associated with mortality among bladder cancer patients |
| [96] | Retrospective cohort 68 ± 10 y (n = 47; 68.1% male) | SO associated with smaller survival rates among gastric cancer patients |
| [9] | Retrospective study 58.8 ± 11.3 y (n = 166; 100% female) | SO not associated with overall survival in women with metastatic breast cancer undergoing palliative care |
| [117] | Cross-sectional study 73.6 ± 7.8 y old among sarcopenic obese | Preoperative SO is an independent risk factor for death and recurrence of hepatocellular carcinoma in patients submitted to primary hepatectomy |
| [118] | Retrospective study 68 y (n = 301; 55.8% male) | SO associated with increased mortality |
| [97] | Retrospective analysis 34 to 87 y (n = 133; 51.1% male) | SO associated with shorter overall survival |
| [114] | Prospective study 59.0 ± 10.9 y (n = 1384; 64.2% male) | SO negatively associated with overall survival in nonmetastatic rectal cancer patients |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silveira, E.A.; da Silva Filho, R.R.; Spexoto, M.C.B.; Haghighatdoost, F.; Sarrafzadegan, N.; de Oliveira, C. The Role of Sarcopenic Obesity in Cancer and Cardiovascular Disease: A Synthesis of the Evidence on Pathophysiological Aspects and Clinical Implications. Int. J. Mol. Sci. 2021, 22, 4339. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22094339
Silveira EA, da Silva Filho RR, Spexoto MCB, Haghighatdoost F, Sarrafzadegan N, de Oliveira C. The Role of Sarcopenic Obesity in Cancer and Cardiovascular Disease: A Synthesis of the Evidence on Pathophysiological Aspects and Clinical Implications. International Journal of Molecular Sciences. 2021; 22(9):4339. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22094339
Chicago/Turabian StyleSilveira, Erika Aparecida, Rômulo Roosevelt da Silva Filho, Maria Claudia Bernardes Spexoto, Fahimeh Haghighatdoost, Nizal Sarrafzadegan, and Cesar de Oliveira. 2021. "The Role of Sarcopenic Obesity in Cancer and Cardiovascular Disease: A Synthesis of the Evidence on Pathophysiological Aspects and Clinical Implications" International Journal of Molecular Sciences 22, no. 9: 4339. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22094339