
Molecular Processes in Stress Urinary Incontinence: A Systematic Review of Human and Animal Studies

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
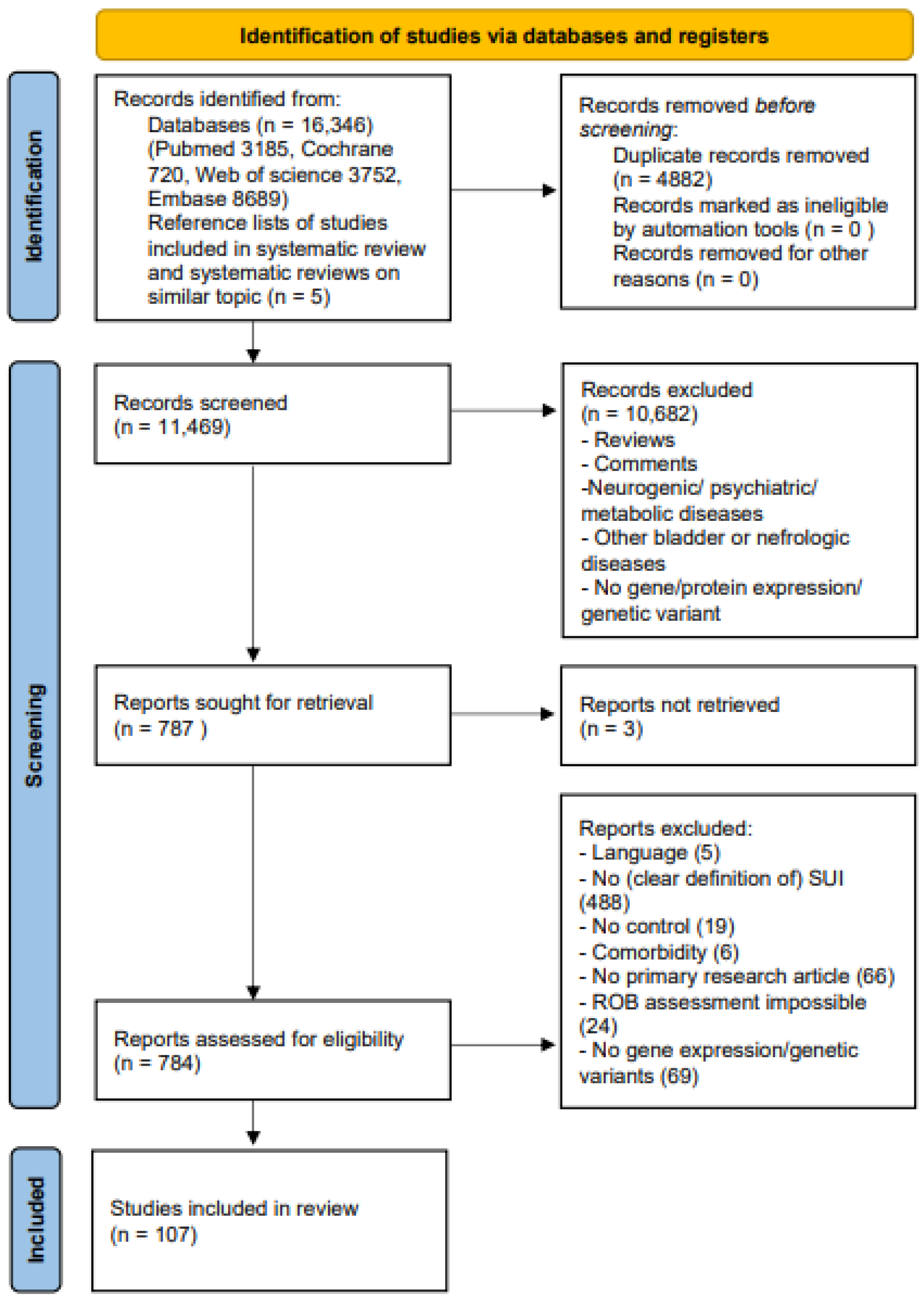
2.1. Study Selection
2.2. Study Characteristics
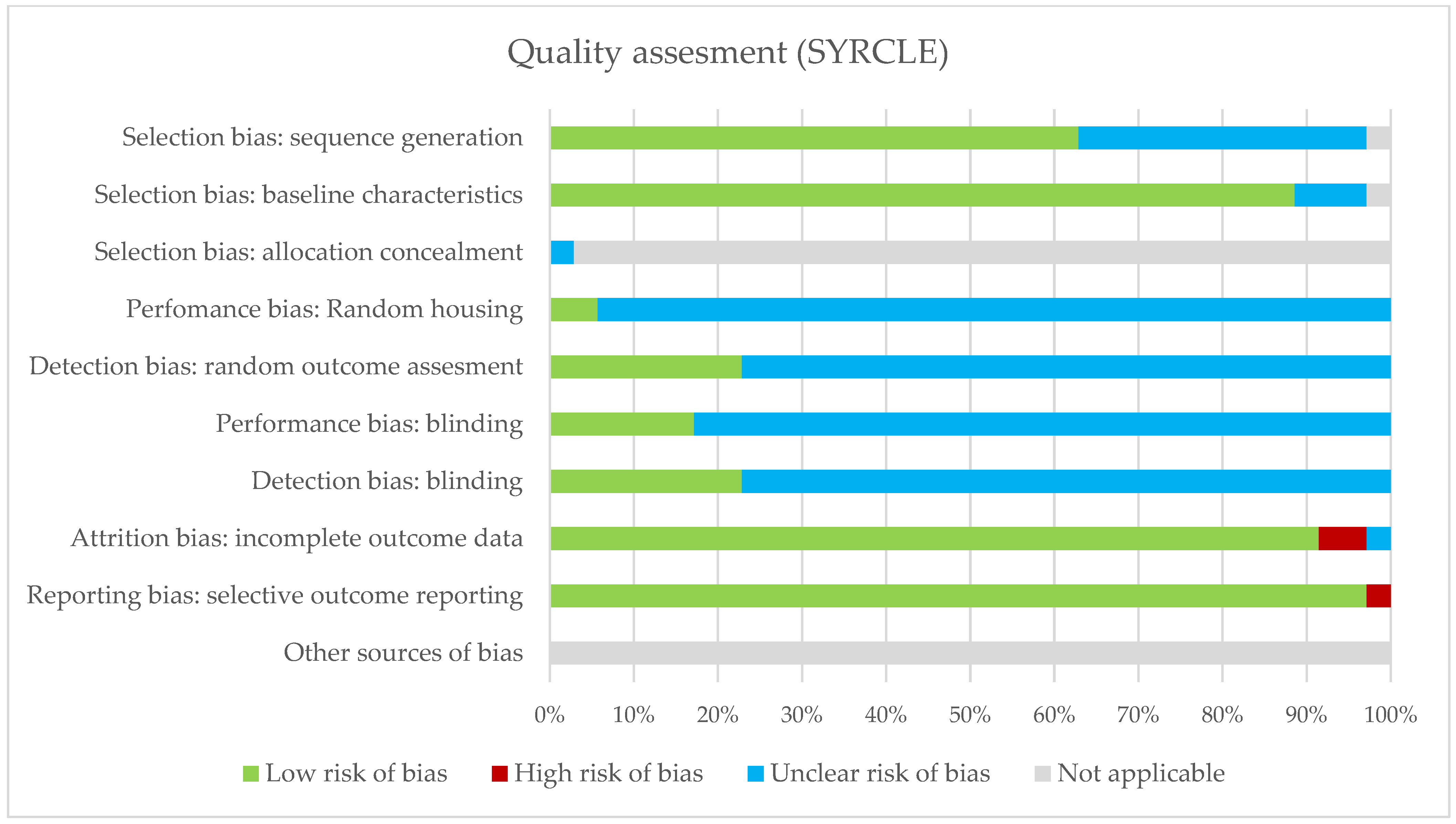
2.3. Risk of Bias of Included Studies
2.4. Synthesis of the Results
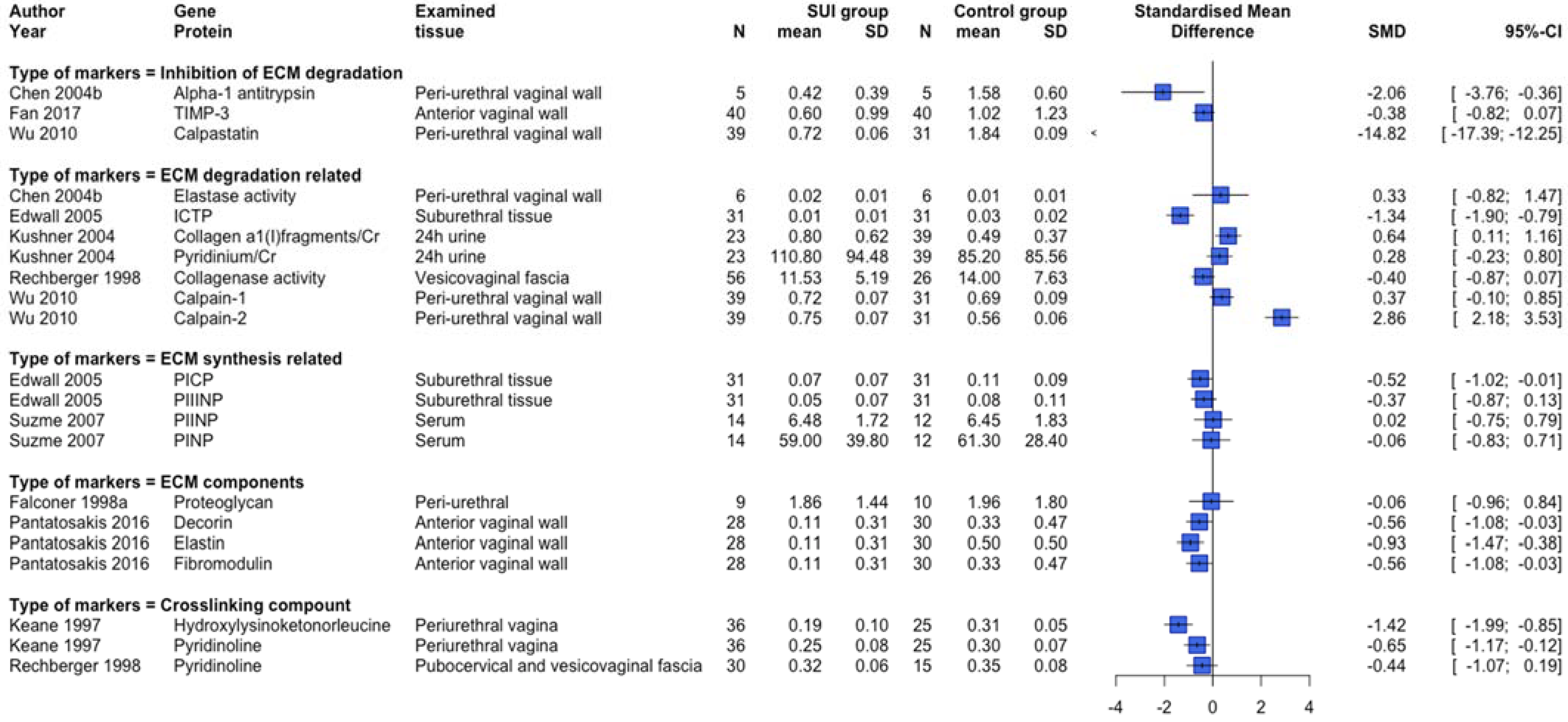
2.4.1. ECM Remodeling
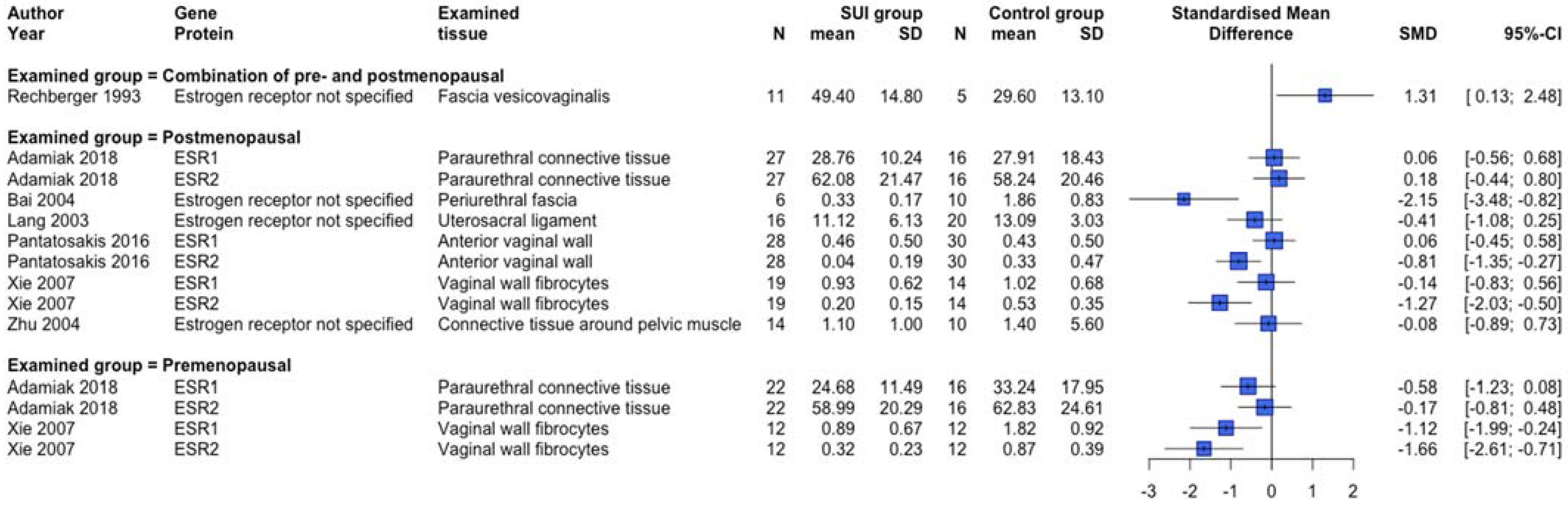
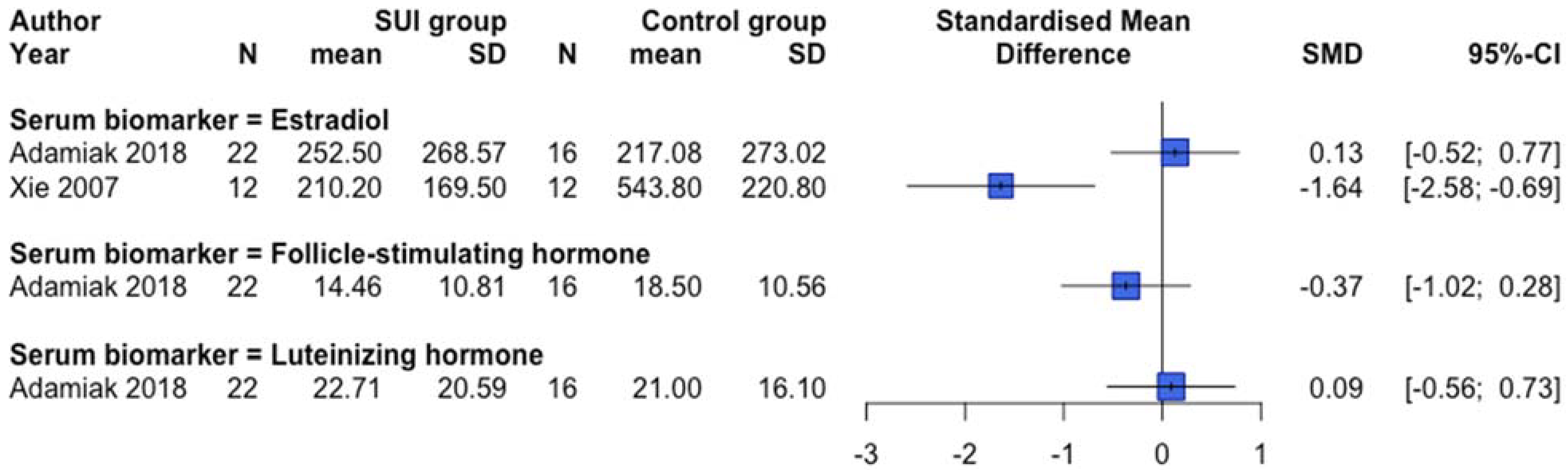
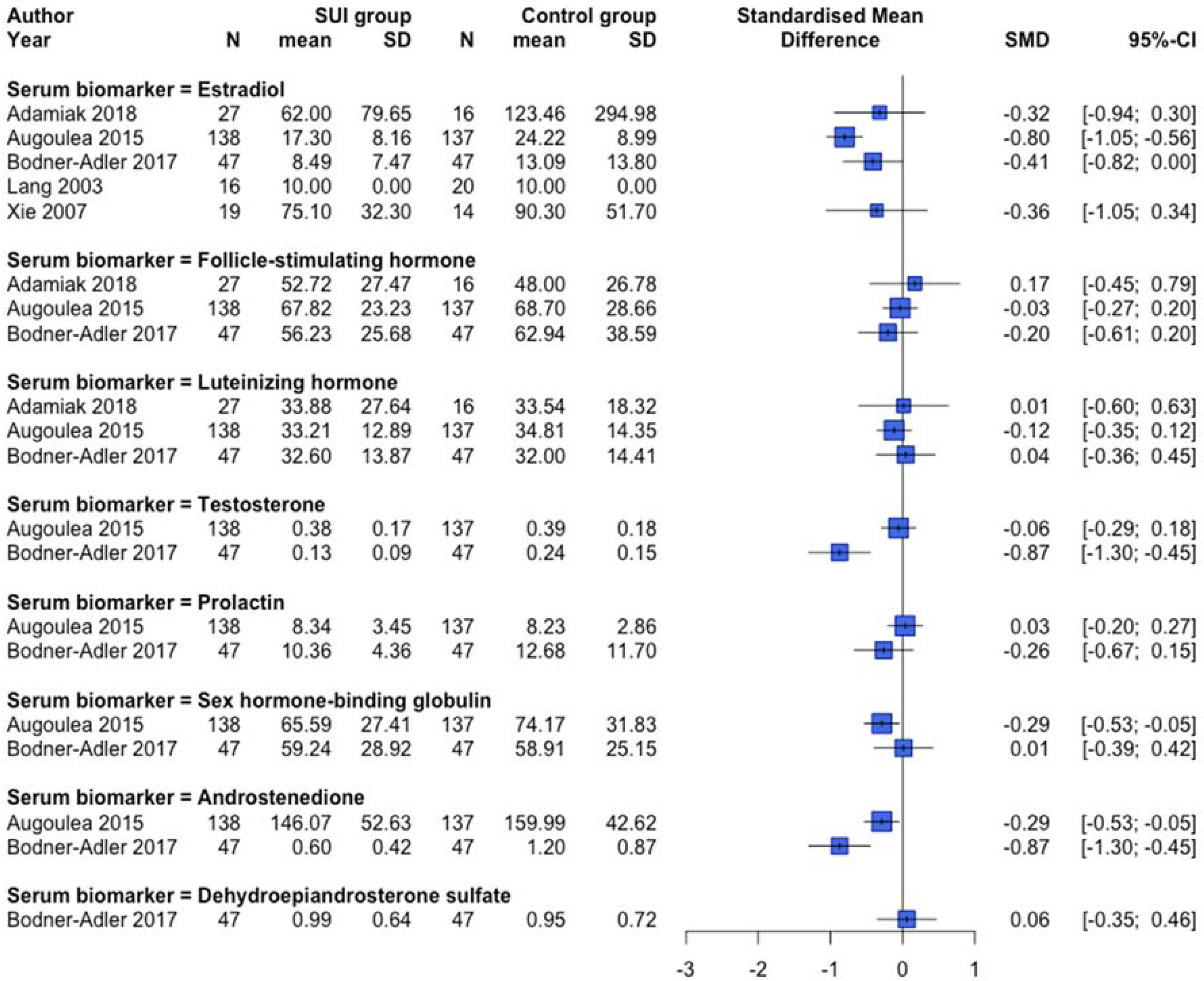
2.4.2. Reproduction-Related Endocrinology
2.4.3. Oxidative Stress and Apoptosis
2.4.4. Inflammation
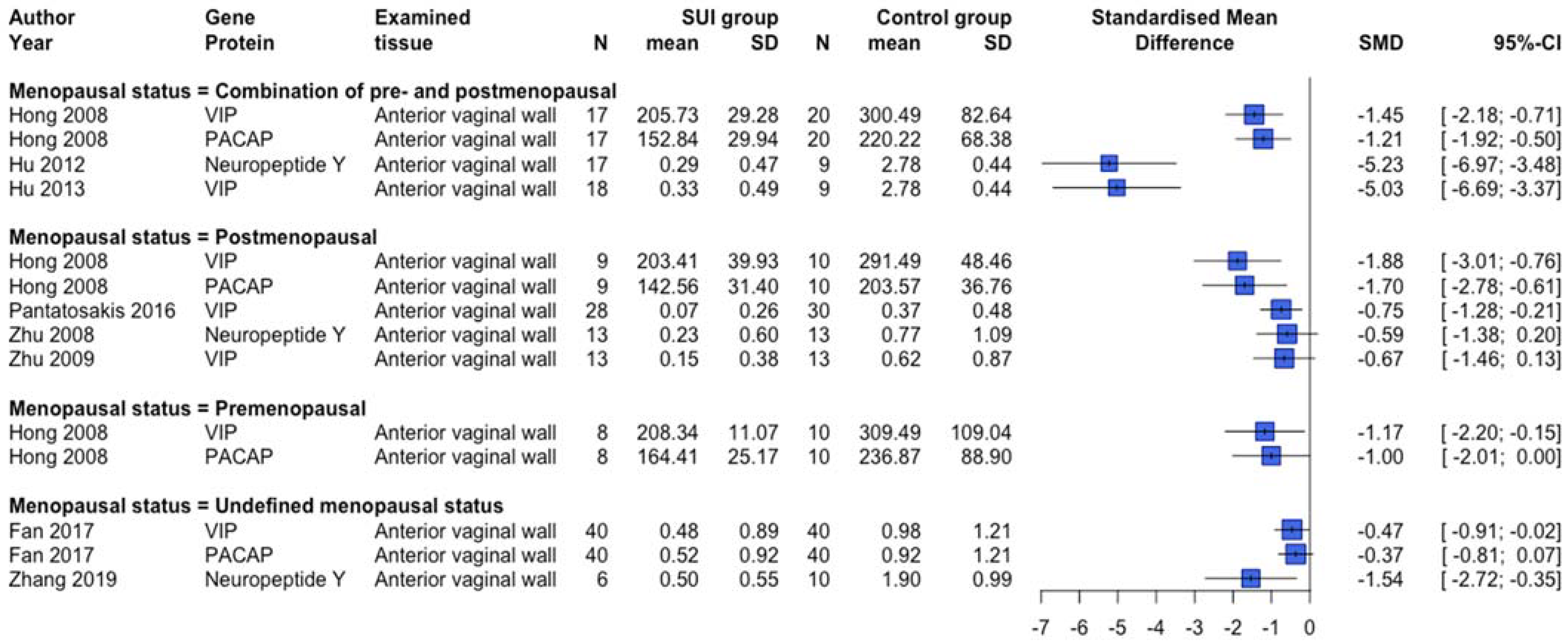
2.4.5. Cell-Specific Markers and Processes
2.4.6. Other
3. Discussion
3.1. Principal Findings
3.2. Comparison with Existing Literature
3.3. Strengths and Limitations
4. Materials and Methods
4.1. Eligibility Criteria
4.2. Information Sources and Search Strategy
4.3. Study Selection
4.4. Data Extraction
4.5. Assessment of Risk of Bias
4.6. Data Synthesis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Groutz, A.; Gordon, D.; Keidar, R.; Lessing, J.B.; Wolman, I.; David, M.P.; Chen, B. Stress urinary incontinence: Prevalence among nulliparous compared with primiparous and grand multiparous premenopausal women. Neurourol. Urodyn. 1999, 18, 419–425. [Google Scholar] [CrossRef]
- Haylen, B.T.; de Ridder, D.; Freeman, R.M.; Swift, S.E.; Berghmans, B.; Lee, J.; Monga, A.; Petri, E.; Rizk, D.E.; Sand, P.K.; et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol. Urodyn. 2010, 29, 4–20. [Google Scholar] [CrossRef] [PubMed]
- Irwin, D.E.; Milsom, I.; Hunskaar, S.; Reilly, K.; Kopp, Z.; Herschorn, S.; Coyne, K.; Kelleher, C.; Hampel, C.; Artibani, W.; et al. Population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: Results of the EPIC study. Eur. Urol. 2006, 50, 1306–1314, discussion 1314–1305. [Google Scholar] [CrossRef] [PubMed]
- Hunskaar, S.; Lose, G.; Sykes, D.; Voss, S. The prevalence of urinary incontinence in women in four European countries. BJU Int. 2004, 93, 324–330. [Google Scholar] [CrossRef]
- Ninomiya, S.; Naito, K.; Nakanishi, K.; Okayama, H. Prevalence and Risk Factors of Urinary Incontinence and Overactive Bladder in Japanese Women. Low Urin. Tract Symptoms 2018, 10, 308–314. [Google Scholar] [CrossRef]
- Chermansky, C.J.; Moalli, P.A. Role of pelvic floor in lower urinary tract function. Auton. Neurosci. 2016, 200, 43–48. [Google Scholar] [CrossRef]
- Thangarajah, F.; Hartmann-Wobbe, J.; Ratiu, D.; Pahmeyer, C.; Radosa, J.C.; Mallmann, P.; Ludwig, S. The Onset of Urinary Incontinence in Different Subgroups and its Relation to Menopausal Status: A Hospital-based Study. In Vivo 2020, 34, 923–928. [Google Scholar] [CrossRef] [Green Version]
- Mishra, G.D.; Cardozo, L.; Kuh, D. Menopausal transition and the risk of urinary incontinence: Results from a British prospective cohort. BJU Int. 2010, 106, 1170–1175. [Google Scholar] [CrossRef] [Green Version]
- Jueng-Anuwat, P.; Roongruangsilp, U.; Kochakarn, W.; Ratana-Olarn, K. Risk factors for stress urinary incontinence in middle aged and elderly Thai women. J. Med. Assoc. Thail. 2001, 84, 1121–1125. [Google Scholar]
- Singh, U.; Agarwal, P.; Verma, M.L.; Dalela, D.; Singh, N.; Shankhwar, P. Prevalence and risk factors of urinary incontinence in Indian women: A hospital-based survey. Indian J. Urol. 2013, 29, 31–36. [Google Scholar] [CrossRef]
- Jun, T.; Yoon, H.S.; Kim, H.S.; Lee, J.W.; Bae, J.; Lee, H.W. Recurrence rate of stress urinary incontinence in females with initial cure after transobturator tape procedure at 3-year follow-up. Investig Clin. Urol. 2017, 58, 54–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirchin, V.; Page, T.; Keegan, P.E.; Atiemo, K.O.; Cody, J.D.; McClinton, S.; Aluko, P. Urethral injection therapy for urinary incontinence in women. Cochrane Database Syst. Rev. 2017, 7, CD003881. [Google Scholar] [CrossRef]
- Falah-Hassani, K.; Reeves, J.; Shiri, R.; Hickling, D.; McLean, L. The pathophysiology of stress urinary incontinence: A systematic review and meta-analysis. Int. Urogynecol. J. 2021, 32, 501–552. [Google Scholar] [CrossRef] [PubMed]
- Aoki, Y.; Brown, H.W.; Brubaker, L.; Cornu, J.N.; Daly, J.O.; Cartwright, R. Urinary incontinence in women. Nat. Rev. Dis. Primers 2017, 3, 17042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khadzhieva, M.B.; Kolobkov, D.S.; Kamoeva, S.V.; Salnikova, L.E. Expression changes in pelvic organ prolapse: A systematic review and in silico study. Sci. Rep. 2017, 7, 7668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herschorn, S. Female pelvic floor anatomy: The pelvic floor, supporting structures, and pelvic organs. Rev. Urol. 2004, 6 (Suppl. 5), S2–S10. [Google Scholar] [PubMed]
- Isali, I.; Mahran, A.; Khalifa, A.O.; Sheyn, D.; Neudecker, M.; Qureshi, A.; Conroy, B.; Schumacher, F.R.; Hijaz, A.K.; El-Nashar, S.A. Gene expression in stress urinary incontinence: A systematic review. Int. Urogynecol. J. 2020, 31, 1–14. [Google Scholar] [CrossRef]
- Hannestad, Y.S.; Lie, R.T.; Rortveit, G.; Hunskaar, S. Familial risk of urinary incontinence in women: Population based cross sectional study. BMJ 2004, 329, 889–891. [Google Scholar] [CrossRef] [Green Version]
- Wennberg, A.L.; Altman, D.; Lundholm, C.; Klint, A.; Iliadou, A.; Peeker, R.; Fall, M.; Pedersen, N.L.; Milsom, I. Genetic influences are important for most but not all lower urinary tract symptoms: A population-based survey in a cohort of adult Swedish twins. Eur. Urol. 2011, 59, 1032–1038. [Google Scholar] [CrossRef] [Green Version]
- Altman, D.; Forsman, M.; Falconer, C.; Lichtenstein, P. Genetic influence on stress urinary incontinence and pelvic organ prolapse. Eur. Urol. 2008, 54, 918–922. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Ulmsten, U.; Ekman, G.; Giertz, G.; Malmstrom, A. Different biochemical composition of connective tissue in continent and stress incontinent women. Acta Obstet. Gynecol. Scand. 1987, 66, 455–457. [Google Scholar] [CrossRef] [PubMed]
- Falconer, C.; Ekman, G.; Malmstrom, A.; Ulmsten, U. Decreased collagen synthesis in stress-incontinent women. Obstet. Gynecol. 1994, 84, 583–586. [Google Scholar] [PubMed]
- Keane, D.P.; Sims, T.J.; Abrams, P.; Bailey, A.J. Analysis of collagen status in premenopausal nulliparous women with genuine stress incontinence. Br. J. Obstet. Gynaecol. 1997, 104, 994–998. [Google Scholar] [CrossRef] [PubMed]
- Falconer, C.; Blomgren, B.; Johansson, O.; Ulmsten, U.; Malmstrom, A.; Westergren-Thorsson, G.; Ekman-Ordeberg, G. Different organization of collagen fibrils in stress-incontinent women of fertile age. Acta Obstet. Gynecol. Scand. 1998, 77, 87–94. [Google Scholar] [CrossRef]
- Falconer, C.; Ekman-Ordeberg, G.; Blomgren, B.; Johansson, O.; Ulmsten, U.; Westergren-Thorsson, G.; Malmstrom, A. Paraurethral connective tissue in stress-incontinent women after menopause. Acta Obstet. Gynecol. Scand. 1998, 77, 95–100. [Google Scholar] [CrossRef]
- Rechberger, T.; Postawski, K.; Jakowicki, J.A.; Gunja-Smith, Z.; Woessner, J.F., Jr. Role of fascial collagen in stress urinary incontinence. Am. J. Obstet. Gynecol. 1998, 179, 1511–1514. [Google Scholar] [CrossRef]
- Chen, B.; Wen, Y.; Wang, H.; Polan, M.L. Differences in estrogen modulation of tissue inhibitor of matrix metalloproteinase-1 and matrix metalloproteinase-1 expression in cultured fibroblasts from continent and incontinent women. Am. J. Obstet. Gynecol. 2003, 189, 59–65. [Google Scholar] [CrossRef]
- Chen, B.; Wen, Y.; Zhang, Z.; Wang, H.; Warrington, J.A.; Polan, M.L. Menstrual phase-dependent gene expression differences in periurethral vaginal tissue from women with stress incontinence. Am. J. Obstet. Gynecol. 2003, 189, 89–97. [Google Scholar] [CrossRef]
- Cor, A.; Barbic, M.; Kralj, B. Differences in the quantity of elastic fibres and collagen type I and type III in endopelvic fascia between women with stress urinary incontinence and controls. Urol. Res. 2003, 31, 61–65. [Google Scholar] [CrossRef]
- Bai, S.W.; Jung, Y.W.; Kwon, H.S.; Yoon, J.M.; Shin, J.S.; Kim, S.K.; Park, K.H.; Park, J.H. The role of estrogen receptor, progesterone receptor and p53 in development of stress urinary incontinence. Yonsei Med. J. 2004, 45, 885–890. [Google Scholar] [CrossRef] [Green Version]
- Bakas, P.G.; Liapis, A.E.; Zervolea, I.; Voutsinas, G.; Kletsas, D.; Creatsas, G. mRNA assessment for procollagen production in women with genuine stress urinary incontinence. Int. Urogynecol. J. 2004, 15, 429–431; discussion 431. [Google Scholar] [CrossRef] [PubMed]
- Kushner, L.; Mathrubutham, M.; Burney, T.; Greenwald, R.; Badlani, G. Excretion of collagen derived peptides is increased in women with stress urinary incontinence. Neurourol. Urodyn. 2004, 23, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Edwall, L.; Carlstrom, K.; Jonasson, A.F. Markers of collagen synthesis and degradation in urogenital tissue from women with and without stress urinary incontinence. Neurourol. Urodyn. 2005, 24, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Radziszewski, P.; Borkowski, A.; Torz, C.; Bossowska, A.; Gonkowski, S.; Majewski, M. Distribution of collagen type VII in connective tissues of postmenopausal stress-incontinent women. Gynecol. Endocrinol. 2005, 20, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Wen, Y.; Zhang, Z.; Guo, Y.; Warrington, J.A.; Polan, M.L. Microarray analysis of differentially expressed genes in vaginal tissues from women with stress urinary incontinence compared with asymptomatic women. Hum. Reprod. 2006, 21, 22–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, Y.; Polan, M.L.; Chen, B. Do extracellular matrix protein expressions change with cyclic reproductive hormones in pelvic connective tissue from women with stress urinary incontinence? Hum. Reprod. 2006, 21, 1266–1273. [Google Scholar] [CrossRef] [Green Version]
- Chen, B.; Wen, Y.; Yu, X.; Polan, M.L. The role of neutrophil elastase in elastin metabolism of pelvic tissues from women with stress urinary incontinence. Neurourol. Urodyn. 2007, 26, 274–279. [Google Scholar] [CrossRef]
- Edwall, L.; Carlstrom, K.; Jonasson, A.F. Endocrine status and markers of collagen synthesis and degradation in serum and urogenital tissue from women with and without stress urinary incontinence. Neurourol. Urodyn. 2007, 26, 410–415. [Google Scholar] [CrossRef]
- Soderberg, M.W.; Johansson, B.; Masironi, B.; Bystrom, B.; Falconer, C.; Sahlin, L.; Ordeberg, G.E. Pelvic floor sex steroid hormone receptors, distribution and expression in pre- and postmenopausal stress urinary incontinent women. Acta Obstet. Gynecol. Scand. 2007, 86, 1377–1384. [Google Scholar] [CrossRef]
- Trabucco, E.; Soderberg, M.; Cobellis, L.; Torella, M.; Bystrom, B.; Ekman-Ordeberg, G.; Petraglia, F.; Colacurci, N. Role of proteoglycans in the organization of periurethral connective tissue in women with stress urinary incontinence. Maturitas 2007, 58, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Wen, Y.; Zhao, Y.Y.; Li, S.; Polan, M.L.; Chen, B.H. Differences in mRNA and protein expression of small proteoglycans in vaginal wall tissue from women with and without stress urinary incontinence. Hum. Reprod. 2007, 22, 1718–1724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, Z.W.; Shi, H.Y.; Zhou, C.Y.; Dong, M.Y.; Hong, L.H.; Jin, H.M. Alterations of estrogen receptor-α and -β in the anterior vaginal wall of women with urinary incontinence. Eur. J. Obstet. Gynecol. Reprod. Biol. 2007, 134, 254–258. [Google Scholar] [CrossRef]
- Wen, Y.; Man, W.C.; Sokol, E.R.; Polan, M.L.; Chen, B.H. Is α2-macroglobulin important in female stress urinary incontinence? Hum. Reprod. 2008, 23, 387–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soderberg, M.W.; Bystrom, B.; Hammarstrom, M.; Malmstrom, A.; Ekman-Ordeberg, G. Decreased gene expression of fibrillin-1 in stress urinary incontinence. Neurourol. Urodyn. 2010, 29, 476–481. [Google Scholar] [CrossRef]
- Tong, J.; Lang, J.; Zhu, L. Microarray analysis of differentially expressed genes in vaginal tissues in postmenopausal women. The role of stress urinary incontinence. Int. Urogynecol. J. 2010, 21, 1545–1551. [Google Scholar] [CrossRef]
- Wu, Y.; Zhang, L.; Jin, H.; Zhou, J.; Xie, Z. The role of calpain-calpastatin system in the development of stress urinary incontinence. Int. Urogynecol. J. 2010, 21, 63–68. [Google Scholar] [CrossRef]
- Cornu, J.N.; Merlet, B.; Cussenot, O.; Cancel-Tassin, G.; Ciofu, C.; Amarenco, G.; Haab, F. Genetic susceptibility to urinary incontinence: Implication of polymorphisms of androgen and oestrogen pathways. World J. Urol. 2011, 29, 239–242. [Google Scholar] [CrossRef]
- Sioutis, D.; Economou, E.; Lambrinoudaki, I.; Tsamadias, V.; Creatsa, M.; Liapis, A. Sp1 collagen I A1 polymorphism in women with stress urinary incontinence. Int. Urogynecol. J. 2011, 22, 835–839. [Google Scholar] [CrossRef]
- Wen, Y.; Whitin, J.; Yu, T.; Cohen, H.; Polan, M.L.; Chen, B. Identification of protein marker in vaginal wall tissues of women with stress urinary incontinence by protein chip array. J. Obstet. Gynaecol. Res. 2012, 38, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Huang, Q.; Jin, H.; Xie, Z.; Wang, M.; Chen, J.; Zhou, Y. The role of the ERK1/2 signalling pathway in the pathogenesis of female stress urinary incontinence. J. Int. Med. Res. 2013, 41, 1242–1251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozbek, E.; Polat, E.C.; Ozcan, L.; Otunctemur, A.; Emrence, Z.; Ustek, D. TT polymorphism in rs2165241 and rs1048661 region in lysyl oxidase like-1 gene may have a role in stress urinary incontinence physiopathology. J. Obstet. Gynaecol. Res. 2013, 39, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Lang, J.; Wu, S.; Cheng, L.; Wang, W.; Zhu, L. Differential expression of microRNAs in periurethral vaginal wall tissues of postmenopausal women with and without stress urinary incontinence. Menopause 2014, 21, 1122–1128. [Google Scholar] [CrossRef]
- Koch, M.; Mitulovic, G.; Hanzal, E.; Umek, W.; Seyfert, S.; Mohr, T.; Koelbl, H.; Laterza, R.M. Urinary proteomic pattern in female stress urinary incontinence: A pilot study. Int. Urogynecol. J. 2016, 27, 1729–1734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozbek, E.; Otunctemur, A.; Sahin, S.; Ozcan, L.; Dursun, M.; Polat, E.; Tulubas, F.; Cekmen, M. Low serum Insulin Like Growth Factor-1 in patients with Stress Urinary Incontinence. Int. Braz. J. Urol. 2016, 42, 787–792. [Google Scholar] [CrossRef]
- Pantatosakis, E.; Karandrea, D.; Liapis, E.; Kondi-Pafiti, A.; Liapis, A. Immunohistochemical expression of hormonal receptors, collagen, elastin, and proteoglycans in genuine urinary incontinence. Clin. Exp. Obstet. Gynecol. 2016, 43, 849–852. [Google Scholar] [CrossRef]
- Augoulea, A.; Sioutis, D.; Rizos, D.; Panoulis, C.; Triantafyllou, N.; Armeni, E.; Deligeoroglou, E.; Chrelias, C.; Creatsa, M.; Liapis, A.; et al. Stress urinary incontinence and endogenous sex steroids in postmenopausal women. Neurourol. Urodyn. 2017, 36, 121–125. [Google Scholar] [CrossRef]
- Bodner-Adler, B.; Bodner, K.; Kimberger, O.; Halpern, K.; Rieken, M.; Koelbl, H.; Umek, W. Role of serum steroid hormones in women with stress urinary incontinence: A case-control study. BJU Int. 2017, 120, 416–421. [Google Scholar] [CrossRef] [Green Version]
- Fan, B.; Jin, X.; Shi, Y.; Zhu, H.; Zhou, W.; Tu, W.; Ding, L. Expression and significance of TIMP-3, PACAP and VIP in vaginal wall tissues of patients with stress urinary incontinence. Exp. Ther. Med. 2017, 13, 624–628. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Xu, P.; Xie, Z.; Shen, F.; Chen, N.; Yu, L.; He, R. Downregulation of AQP2 in the anterior vaginal wall is associated with the pathogenesis of female stress urinary incontinence. Mol. Med. Rep. 2017, 16, 3503–3509. [Google Scholar] [CrossRef] [Green Version]
- Adamiak-Godlewska, A.; Tarkowski, R.; Winkler, I.; Romanek-Piva, K.; Skorupska, K.; Jakimiuk, A.J.; Rechberger, T. Stress urinary incontinent women, the influence of age and hormonal status on estrogen receptor alpha and beta gene expression and protein immunoexpression in paraurethral tissues. J. Physiol. Pharmacol. 2018, 69, 53–59. [Google Scholar] [CrossRef]
- Khadzhieva, M.B.; Kamoeva, S.V.; Ivanova, A.V.; Salnikova, L.E. Genetic Factors of Comorbidity of Pelvic Organ Prolapse, Stress Urinary Incontinence, and Chronic Venous Insufficiency of the Lower Limbs in Women. Russ. J. Genet. 2018, 54, 1479–1486. [Google Scholar] [CrossRef]
- Koch, M.; Umek, W.; Hanzal, E.; Mohr, T.; Seyfert, S.; Koelbl, H.; Mitulovic, G. Serum proteomic pattern in female stress urinary incontinence. Electrophoresis 2018, 39, 1071–1078. [Google Scholar] [CrossRef] [PubMed]
- Ozcan, L.; Polat, E.C.; Onen, E.; Otunctemur, A.; Ozbek, E.; Somay, A.; Ozbay, N. Neuronal Nitric Oxide Synthase Expression in the Anterior Vaginal Wall of Patients with Stress Urinary Incontinence. Urol. J. 2018, 15, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.H.; Wang, J.; Xu, J.; Bai, Y.; Guo, Z.J. MiR-93-mediated collagen expression in stress urinary incontinence via calpain-2. Mol. Med. Rep. 2018, 17, 624–629. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Liu, X.; Li, W.; Sun, X.; Xie, Z. Endoplasmic reticulum stress contributes to the pathogenesis of stress urinary incontinence in postmenopausal women. J. Int. Med. Res. 2018, 46, 5269–5277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Li, B.S.; Liu, C.; Hong, S.S.; Min, J.; Hu, M.; Tang, J.M.; Li, S.T.; Wang, T.T.; Zhou, H.X.; et al. Effect of integrin β1 in the treatment of stress urinary incontinence by electrical stimulation. Mol. Med. Rep. 2019, 19, 4727–4734. [Google Scholar] [CrossRef] [Green Version]
- Penney, K.L.; Townsend, M.K.; Turman, C.; Glass, K.; Staller, K.; Kraft, P.; Grodstein, F.; Minnassian, V.A. Genome-Wide Association Study for Urinary and Fecal Incontinence in Women. J. Urol. 2019, 203, 978–983. [Google Scholar] [CrossRef]
- Reischer, T.; Balendran-Braun, S.; Liebmann-Reindl, S.; Streubel, B.; Umek, W.; Koelbl, H.; Koch, M. Genetic association in female stress urinary incontinence based on proteomic findings: A case-control study. Int. Urogynecol. J. 2019, 31, 117–122. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Wang, C.; Huang, X.; Ye, G. The alteration of ERB5 and collagen metabolism is relevant to the development of stress urinary incontinence. Int. J. Clin. Exp. Med. 2019, 12, 5154–5161. [Google Scholar]
- Wei, A.; Wang, R.; Wei, K.; Dai, C.; Huang, Y.; Xu, P.; Xu, J.; Tang, H.; Zhang, Y.; Fan, Y. LncRNA and mRNA Expression Profiling in the Periurethral Vaginal Wall Tissues of Postmenopausal Women with Stress Urinary Incontinence. Reprod. Sci. 2020, 27, 1490–1501. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.M.; Luo, X. Clinical significance of neuropeptide Y expression in pelvic tissue in patients with pelvic floor dysfunction. Open Life Sci. 2019, 14, 126–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Y.; Hong, X.; Yu, Y.; Lin, Y. Changes of collagen type III and decorin in paraurethral connective tissue from women with stress urinary incontinence and prolapse. Int. Urogynecol. J. 2007, 18, 1459–1463. [Google Scholar] [CrossRef] [PubMed]
- Rechberger, T.; Donica, H.; Baranowski, W.; Jakowicki, J. Female urinary stress incontinence in terms of connective tissue biochemistry. Eur. J. Obstet. Gynecol. Reprod. Biol. 1993, 49, 187–191. [Google Scholar] [CrossRef]
- Bergman, A.; Elia, G.; Cheung, D.; Perelman, N.; Nimni, M.E. Biochemical composition of collagen in continent and stress urinary incontinent women. Gynecol. Obstet. Investig. 1994, 37, 48–51. [Google Scholar] [CrossRef]
- Liapis, A.; Bakas, P.; Pafiti, A.; Hassiakos, D.; Frangos-Plemenos, M.; Creatsas, G. Changes in the quantity of collagen type I in women with genuine stress incontinence. Urol. Res. 2000, 28, 323–326. [Google Scholar] [CrossRef]
- Liapis, A.; Bakas, P.; Pafiti, A.; Frangos-Plemenos, M.; Arnoyannaki, N.; Creatsas, G. Changes of collagen type III in female patients with genuine stress incontinence and pelvic floor prolapse. Eur. J. Obstet. Gynecol. Reprod. Biol. 2001, 97, 76–79. [Google Scholar] [CrossRef]
- Chen, B.H.; Wen, Y.; Li, H.; Polan, M.L. Collagen metabolism and turnover in women with stress urinary incontience and pelvic prolapse. Int. Urogynecol. J. 2002, 13, 80–87. [Google Scholar] [CrossRef]
- Lang, J.H.; Zhu, L.; Sun, Z.J.; Chen, J. Estrogen levels and estrogen receptors in patients with stress urinary incontinence and pelvic organ prolapse. Int. J. Gynecol. Obstet. 2003, 80, 35–39. [Google Scholar] [CrossRef]
- Busacchi, P.; Perri, T.; Paradisi, R.; Oliverio, C.; Santini, D.; Guerrini, S.; Barbara, G.; Stanghellini, V.; Corinaldesi, R.; De Giorgio, R. Abnormalities of somatic peptide-containing nerves supplying the pelvic floor of women with genitourinary prolapse and stress urinary incontinence. Urology 2004, 63, 591–595. [Google Scholar] [CrossRef]
- Chen, B.; Wen, Y.; Polan, M.L. Elastolytic activity in women with stress urinary incontinence and pelvic organ prolapse. Neurourol. Urodyn. 2004, 23, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; DeSautel, M.; Anderson, A.; Badlani, G.; Kushner, L. Collagen synthesis is not altered in women with stress urinary incontinence. Neurourol. Urodyn. 2004, 23, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Lang, J.; Feng, R.; Chen, J.; Wong, F. Estrogen receptor in pelvic floor tissues in patients with stress urinary incontinence. Int. Urogynecol. J. 2004, 15, 340–343. [Google Scholar] [CrossRef] [PubMed]
- Skorupski, P.; Krol, J.; Starega, J.; Adamiak, A.; Jankiewicz, K.; Rechberger, T. An α-1 chain of type I collagen Sp1-binding site polymorphism in women suffering from stress urinary incontinence. Am. J. Obstet. Gynecol. 2006, 194, 346–350. [Google Scholar] [CrossRef]
- Suzme, R.; Yalcin, O.; Gurdol, F.; Gungor, F.; Bilir, A. Connective tissue alterations in women with pelvic organ prolapse and urinary incontinence. Acta Obstet. Gynecol. Scand. 2007, 86, 882–888. [Google Scholar] [CrossRef] [PubMed]
- Hong, X.; Huang, L.; Song, Y. Role of vasoactive intestinal peptide and pituitary adenylate cyclase activating polypeptide in the vaginal wall of women with stress urinary incontinence and pelvic organ prolapse. Int. Urogynecol. J. 2008, 19, 1151–1157. [Google Scholar] [CrossRef]
- Zhu, L.; Lang, J.; Jiang, X.; Jiang, F.; Chen, J.; Wong, F. Neuropeptide Y expression in vaginal epithelium of women with pelvic organ prolapse and stress urinary incontinence. Int. J. Gynaecol. Obstet. 2008, 102, 65–68. [Google Scholar] [CrossRef]
- Zhu, L.; Lang, J.; Jiang, F.; Jiang, X.; Chen, J. Vasoactive intestinal peptide in vaginal epithelium of patients with pelvic organ prolapse and stress urinary incontinence. Int. J. Gynaecol. Obstet. 2009, 105, 223–225. [Google Scholar] [CrossRef]
- Athanasiou, S.; Lymberopoulos, E.; Kanellopoulou, S.; Rodolakis, A.; Vlachos, G.; Antsaklis, A. Proteomic analysis of pubocervical fascia in women with and without pelvic organ prolapse and urodynamic stress incontinence. Int. Urogynecol. J. 2010, 21, 1377–1384. [Google Scholar] [CrossRef]
- Skorupski, P.; Miotla, P.; Jankiewicz, K.; Rechberger, T. MMP-1 and MMP-3 gene encoding polymorphism and the risk of the development of pelvic organ prolapse and stress urinary incontinence. Ginekol. Pol. 2010, 81, 594–599. [Google Scholar]
- Hu, J.M.; Wang, L.; Cheng, X.; Zhou, L.H.; Li, Z.G. Neuropeptide Y innervation in the vaginal mucosa among patients with pelvic organ prolapse. Mol. Med. Rep. 2012, 5, 444–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, J.M.; Cheng, X.; Wang, L.; Zhu, J.N.; Zhou, L.H. Vasoactive intestinal peptide expression in the vaginal anterior wall of patients with pelvic organ prolapse. Taiwan. J. Obstet. Gynecol. 2013, 52, 233–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, L.; Wang, L.; Wang, Q.; Li, H.; Zang, H. Association between pelvic organ prolapse and stress urinary incontinence with collagen. Exp. Ther. Med. 2014, 7, 1337–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sievert, K.D.; Emre Bakircioglu, M.; Tsai, T.; Dahms, S.E.; Nunes, L.; Lue, T.F. The effect of simulated birth trauma and/or ovariectomy on rodent continence mechanism. Part I: Functional and structural change. J. Urol. 2001, 166, 311–317. [Google Scholar] [CrossRef]
- Resplande, J.; Gholami, S.S.; Graziottin, T.M.; Rogers, R.; Lin, C.S.; Leng, W.; Lue, T.F. Long-term effect of ovariectomy and simulated birth trauma on the lower urinary tract of female rats. J. Urol. 2002, 168, 323–330. [Google Scholar] [CrossRef]
- Lin, G.; Shindel, A.W.; Banie, L.; Deng, D.; Wang, G.; Hayashi, N.; Lin, C.S.; Lue, T.F. Molecular mechanisms related to parturition-induced stress urinary incontinence. Eur. Urol. 2009, 55, 1213–1222. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.Y.; Lin, Y.N.; Chen, Y.H.; Chen, W.C. Stress urinary incontinence following vaginal trauma involves remodeling of urethral connective tissue in female mice. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 163, 224–229. [Google Scholar] [CrossRef]
- Li, G.Y.; Cui, W.S.; Zhou, F.; Gao, Z.Z.; Xin, H.; Liu, T.; Li, W.R.; Gong, Y.Q.; Bai, G.Y.; Guo, Y.L.; et al. Pathology of urethral fibromuscular system related to parturition-induced stress urinary incontinence and TGF-β1/Smad pathway. Mol. Cell. Biochem. 2012, 364, 329–335. [Google Scholar] [CrossRef]
- Li, G.Y.; Zhou, F.; Gong, Y.Q.; Cui, W.S.; Yuan, Y.M.; Song, W.D.; Xin, H.; Liu, T.; Li, W.R.; Gao, Z.Z.; et al. Activation of VEGF and ERK1/2 and improvement of urethral function by adipose-derived stem cells in a rat stress urinary incontinence model. Urology 2012, 80, 953.E1–953.E8. [Google Scholar] [CrossRef]
- Chen, H.Y.; Chen, C.J.; Lin, Y.N.; Chen, Y.H.; Chen, W.C.; Chen, C.M. Proteomic analysis related to stress urinary incontinence following vaginal trauma in female mice. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 171, 171–179. [Google Scholar] [CrossRef]
- Hijaz, A.K.; Grimberg, K.O.; Tao, M.; Schmotzer, B.; Sadeghi, Z.; Lin, Y.H.; Kavran, M.; Ozer, A.; Xiao, N.; Daneshgari, F. Stem cell homing factor, CCL7, expression in mouse models of stress urinary incontinence. Female Pelvic Med. Reconstr. Surg. 2013, 19, 356–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, S.H.; Piao, S.; Kim, I.G.; Lee, J.Y.; Cho, H.J.; Kim, S.W.; Hwang, T.K.; Lee, J.Y. Comparison of three types of stress urinary incontinence rat models: Electrocauterization, pudendal denervation, and vaginal distension. Urology 2013, 81, 465.E1–465.E6. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Cheng, M.; Ding, Y.; Chen, L.; Hua, K. Modified vaginal dilation rat model for postpartum stress urinary incontinence. J. Obstet. Gynaecol. Res. 2013, 39, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Lenis, A.T.; Kuang, M.; Woo, L.L.; Hijaz, A.; Penn, M.S.; Butler, R.S.; Rackley, R.; Damaser, M.S.; Wood, H.M. Impact of parturition on chemokine homing factor expression in the vaginal distention model of stress urinary incontinence. J. Urol. 2013, 189, 1588–1594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.Y.; Chen, W.C.; Lin, Y.N.; Chen, Y.H. Synergistic effect of vaginal trauma and ovariectomy in a murine model of stress urinary incontinence: Upregulation of urethral nitric oxide synthases and estrogen receptors. Mediat. Inflamm. 2014, 2014, 314846. [Google Scholar] [CrossRef]
- Chen, Y.H.; Lin, Y.N.; Chen, W.C.; Hsieh, W.T.; Chen, H.Y. Treatment of stress urinary incontinence by ginsenoside Rh2. Am. J. Chin. Med. 2014, 42, 817–831. [Google Scholar] [CrossRef]
- Chen, Y.H.; Chen, C.J.; Lin, Y.N.; Wu, Y.C.; Hsieh, W.T.; Wu, B.T.; Ma, W.L.; Chen, W.C.; Tsai, K.S.; Wu, S.Y.; et al. Proteomic analysis of urethral protein expression in an estrogen receptor α-deficient murine model of stress urinary incontinence. World J. Urol. 2015, 33, 1635–1643. [Google Scholar] [CrossRef]
- Wang, H.; Liu, J.; Zeng, J.; Zeng, C.; Zhou, Y. Expression of TβR−2, Smad3 and Smad7 in the vaginal anterior wall of postpartum rats with stress urinary incontinence. Arch. Gynecol. Obstet. 2015, 291, 869–876. [Google Scholar] [CrossRef]
- Song, Q.X.; Balog, B.M.; Lin, D.L.; Jiang, H.H.; Gurel, V.; Spaulding, J.; Tobacyk, J.; McMichael, J.; Damaser, M.S. Combination histamine and serotonin treatment after simulated childbirth injury improves stress urinary incontinence. Neurourol. Urodyn. 2016, 35, 703–710. [Google Scholar] [CrossRef]
- Sumino, Y.; Yoshikawa, S.; Mori, K.I.; Mimata, H.; Yoshimura, N. IGF-1 as an Important Endogenous Growth Factor for Recovery from Impaired Urethral Continence Function in Rats with Simulated Childbirth Injury. J. Urol. 2016, 195, 1927–1935. [Google Scholar] [CrossRef]
- Min, J.; Li, B.; Liu, C.; Hong, S.; Tang, J.; Hu, M.; Liu, Y.; Li, S.; Hong, L. Therapeutic Effect and Mechanism of Electrical Stimulation in Female Stress Urinary Incontinence. Urology 2017, 104, 45–51. [Google Scholar] [CrossRef]
- Tang, J.; Li, B.; Liu, C.; Li, Y.; Li, Q.; Wang, L.; Min, J.; Hu, M.; Hong, S.; Hong, L. Mechanism of Mechanical Trauma-Induced Extracellular Matrix Remodeling of Fibroblasts in Association with Nrf2/ARE Signaling Suppression Mediating TGF-β1/Smad3 Signaling Inhibition. Oxid. Med. Cell. Longev. 2017, 2017, 8524353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, J.; Liu, C.; Min, J.; Hu, M.; Li, Y.; Hong, L. Potential therapeutic role of punicalagin against mechanical-trauma-induced stress urinary incontinence via upregulation of Nrf2 and TGF-β1 signaling: Effect of punicalagin on mechanical trauma induced SUI. Int. Urogynecol. J. 2017, 28, 947–955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, X.; Liu, C.; Chen, Y.B.; Gu, M.; Cai, Z.K.; Chen, Q.; Wang, Z. Sulforaphane Treatment of Stress Urinary Incontinence Via the Nrf2-ARE Pathway in a Rat Model. Cell. Physiol. Biochem. 2017, 44, 1912–1922. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, S.; Sumino, Y.; Kwon, J.; Suzuki, T.; Kitta, T.; Miyazato, M.; Yoshimura, N. Effects of multiple simulated birth traumas on urethral continence function in rats. Am. J. Physiol. 2017, 313, F1089–F1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilhar, A.P.M.; Bortolini, M.A.T.; Se, A.B.; Feitosa, S.M.; Salerno, G.R.F.; Zanoteli, E.; Simoes, M.J.; Castro, R.A. Molecular and immunohistochemical analysis of the urethra of female rats after induced trauma and intravenous therapy with muscle derived stem cells. Neurourol. Urodyn. 2018, 37, 2151–2159. [Google Scholar] [CrossRef]
- Iatsyna, O.; Vernygorodskyi, S.; Kostyev, F. Morphological assessment of NO-synthase distribution in overactive bladder and stress urine incontinence in animal models administered with experimental pharmacocorrection regimens. Georgian Med. News 2018, 279, 143–150. [Google Scholar]
- Jiang, H.H.; Song, Q.X.; Gill, B.C.; Balog, B.M.; Juarez, R.; Cruz, Y.; Damaser, M.S. Electrical stimulation of the pudendal nerve promotes neuroregeneration and functional recovery from stress urinary incontinence in a rat model. Am. J. Physiol. 2018, 315, F1555–F1564. [Google Scholar] [CrossRef]
- Li, Q.; Li, B.; Liu, C.; Wang, L.; Tang, J.; Hong, L. Protective role of Nrf2 against mechanical-stretch-induced apoptosis in mouse fibroblasts: A potential therapeutic target of mechanical-trauma-induced stress urinary incontinence. Int. Urogynecol. J. 2018, 29, 1469–1477. [Google Scholar] [CrossRef]
- Wu, A.K.; Zhang, X.; Wang, J.; Ning, H.; Zaid, U.; Villalta, J.D.; Wang, G.; Banie, L.; Lin, G.; Lue, T.F. Treatment of stress urinary incontinence with low-intensity extracorporeal shock wave therapy in a vaginal balloon dilation induced rat model. Transl. Androl. Urol. 2018, 7, S7–S16. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Liu, C.; Li, B.; Hong, S.; Min, J.; Hu, M.; Tang, J.; Wang, T.; Yang, L.; Hong, L. Electrical stimulation activates calpain 2 and subsequently upregulates collagens via the integrin β1/TGF-β1 signaling pathway. Cell. Signal. 2019, 59, 141–151. [Google Scholar] [CrossRef]
- Tang, J.; Liu, C.; Li, B.; Hong, S.; Li, Q.; Wang, L.; Min, J.; Hu, M.; Li, Y.; He, S.; et al. Protective Role of Nuclear Factor Erythroid-2-Related Factor 2 against Mechanical Trauma-Induced Apoptosis in a Vaginal Distension-Induced Stress Urinary Incontinence Mouse Model. Oxidative Med. Cell. Longev. 2019, 2019, 2039856. [Google Scholar] [CrossRef]
- Yang, B.; Li, M.; Lei, H.; Xu, Y.; Li, H.; Gao, Z.; Guan, R.; Xin, Z. Low Intensity Pulsed Ultrasound Influences the Myogenic Differentiation of Muscle Satellite Cells in a Stress Urinary Incontinence Rat Model. Urology 2019, 123, 297.e1–297.e8. [Google Scholar] [CrossRef]
- Zeng, J.; Liu, J.; Zeng, C.; Chen, D. Biological effects of electrical stimulation on pelvic floor muscle strength and neuropeptide y expression. Int. J. Clin. Exp. Med. 2019, 12, 2427–2434. [Google Scholar]
- Zordani, A.; Pisciotta, A.; Bertoni, L.; Bertani, G.; Vallarola, A.; Giuliani, D.; Puliatti, S.; Mecugni, D.; Bianchi, G.; de Pol, A.; et al. Regenerative potential of human dental pulp stem cells in the treatment of stress urinary incontinence: In vitro and in vivo study. Cell Prolif. 2019, 52, e12675. [Google Scholar] [CrossRef] [Green Version]
- Lo, T.S.; Lin, Y.H.; Uy-Patrimonio, M.C.; Chu, H.C.; Hsieh, W.C.; Chua, S. Dissecting of the paravesical space associated with lower urinary tract dysfunction—A rat model. Sci. Rep. 2020, 10, 1718. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.K.; Huang, J.Y.; Liu, J.Y.; Li, Y.H.; Gao, Y. BMMSC-sEV-derived miR-328a-3p promotes ECM remodeling of damaged urethral sphincters via the Sirt7/TGFβ signaling pathway. Stem Cell Res. Ther. 2020, 11, 286. [Google Scholar] [CrossRef]
- Zhang, X.; Ruan, Y.; Wu, A.K.; Zaid, U.; Villalta, J.D.; Wang, G.; Banie, L.; Reed-Maldonado, A.B.; Lin, G.; Lue, T.F. Delayed Treatment With Low-intensity Extracorporeal Shock Wave Therapy in an Irreversible Rat Model of Stress Urinary Incontinence. Urology 2020, 141, e181–e187. [Google Scholar] [CrossRef]
- Cartwright, R.; Kirby, A.C.; Tikkinen, K.A.; Mangera, A.; Thiagamoorthy, G.; Rajan, P.; Pesonen, J.; Ambrose, C.; Gonzalez-Maffe, J.; Bennett, P.; et al. Systematic review and metaanalysis of genetic association studies of urinary symptoms and prolapse in women. Am. J. Obstet. Gynecol. 2015, 212, 199.e1–199.e24. [Google Scholar] [CrossRef]
- Campeau, L.; Gorbachinsky, I.; Badlani, G.H.; Andersson, K.E. Pelvic floor disorders: Linking genetic risk factors to biochemical changes. BJU Int. 2011, 108, 1240–1247. [Google Scholar] [CrossRef]
- Chen, B.; Yeh, J. Alterations in connective tissue metabolism in stress incontinence and prolapse. J. Urol. 2011, 186, 1768–1772. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, P.; Rohozinski, J.; Badlani, G. Genetic influences on stress urinary incontinence. Curr. Opin. Urol. 2010, 20, 291–295. [Google Scholar] [CrossRef]
- Gregory, W.T.; Nygaard, I. Childbirth and pelvic floor disorders. Clin. Obstet. Gynecol. 2004, 47, 394–403. [Google Scholar] [CrossRef] [PubMed]
- Song, Q.X.; Balog, B.M.; Kerns, J.; Lin, D.L.; Sun, Y.; Damaser, M.S.; Jiang, H.H. Long-term effects of simulated childbirth injury on function and innervation of the urethra. Neurourol. Urodyn. 2015, 34, 381–386. [Google Scholar] [CrossRef] [Green Version]
- Post, W.M.; Ruiz-Zapata, A.M.; Grens, H.; de Vries, R.B.M.; Poelmans, G.; Coenen, M.J.H.; Janssen, D.A.W.; Heesakkers, J.; Oosterwijk, E.; Kluivers, K.B. Genetic variants and expression changes in urgency urinary incontinence: A systematic review. Neurourol. Urodyn. 2020, 39, 2089–2110. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernan, M.A.; Reeves, B.C.; Savovic, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Hooijmans, C.R.; Rovers, M.M.; de Vries, R.B.; Leenaars, M.; Ritskes-Hoitinga, M.; Langendam, M.W. SYRCLE’s risk of bias tool for animal studies. BMC Med. Res. Methodol. 2014, 14, 43. [Google Scholar] [CrossRef] [Green Version]
- National Toxicology Program. Monograph on Immunotoxicity Associated with Exposure to Perfluorooctanoic acid (PFOA) and perfluorooctane sulfonate (PFOS). Natl. Toxicol. Program 2016. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid.-Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, Version 6.2; (Updated February 2021). Cochrane 2021, Chapter 6, Section 6.5.2.10; Available online: www.training.cochrane.org/handbook (accessed on 17 November 2021).
- Schünemann, H.B.J.; Guyatt, G.; Oxman, A. (Eds.) GRADE Handbook for Grading Quality of Evidence and Strength of Recommendations. 2013. Updated October 2013. Available online: https://gdt.gradepro.org/app/handbook/handbook.html (accessed on 7 December 2021).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | SUI/SUI + POP | Genome/Transcriptome/Proteome | Assay Methods | No. of Patients | No. of Controls | Summary of Findings |
|---|---|---|---|---|---|---|
| Penney et al., 2019 | SUI | Genome | GWAS | 1809 | 4811 | No genome-wide significant SNPs, after adjusting for known risk factors, the top ranked SNP in the unadjusted SUI analysis became genome-wide significant (rs7607995, p = 4.5 × 10−8, chromosome 2p13.1, WDR54) |
| Chen et al., 2006 | SUI | Transcriptome | Microarray, RT-PCR, WB, QC-PCR, immunofluorescence | 17 | 19 | Differential expression of 79 genes. Up-regulated genes (involved in ECM metabolism): skin-derived protease inhibitor 3 (elafin); IL-1RA; keratin 6, 14 and 16; and psoriasin 1. Downregulated genes: α2 actin; actin depolymerizing factor; smooth muscle myosin; light polypeptide kinase; RAMP-1; tropomyosin 1; microfibril-associated glycoprotein-2; insulinlike growth factor binding protein 7; collagen type IV α chain, several large cDNA genes (named KIAA). |
| Tong et al., 2010 | SUI | Transcriptome | Microarray, RT-PCR, and IHC | 9 | 8 | Differential expression of 75 genes. The four most related pathways: solutable N-ethylmaleimidesensitive factor attachment protein receptor (SNARE) interactions in vesicular transport containing STX10, GOSR1 genes; neurodegenerative disorders containing GRB2, APOE genes; fructose and mannose metabolism containing TPl1, TSTA3 genes; and inositol metabolism containing GBA gene. |
| Liu et al., 2014 | SUI | Transcriptome | Microarray, RT-PCR, WB | 13 | 13 | Differential expression of 12 miRNAs, three miRNA-mRNA pairs. Target genes are associated with neurodegenerative conditions |
| Wei et al., 2020 | SUI | Transcriptome | Microarray, qRT-PCR | 11 | 11 | Differential expression of 8840 lncRNAs and 7102 mRNAs. Several lncRNAs are involved in the lysosome pathway associated with extracellular matrix (ECM) remodeling. Several mRNAs are involved in fibroblast pseudopodia formation, fibroblast growth, and the regulation of smooth muscle cell differentiation in the urinary tract. |
| Athanasiou et al., 2010 | SUI+POP | Proteome | 2-DE, MS and WB | 4 | 3 | Differential expression of seven proteins (more than two-fold): Overexpressed: Transgelin, Smooth muscle gamma-actin, myosin light polypeptide 6, precursor of alpha-1 antitrypsin, galectin-1. Underexpressed: two isoforms of transgelin. Only detected in patient group: type I keratin cytoskeletal 10 (CK10) and two isoforms of transgelin. These proteins are related to muscle contraction, cytoskeleton, cell maintenance, stability, and motility, smooth muscle differentiation, inhibition of extracellular matrix degradation, apoptosis. |
| Wen et al., 2012 | SUI | Proteome | SELDI-TOF MS, IHC, WB, RT-PCR | 10 | 10 | Differential expression of SM-22a. Associated with Fibroblast-to-myofibroblast differentiation, wound healing. |
| Koch et al., 2016 | SUI | Proteome | HPLCS and MS | 20 | 20 | 828 proteins identified six significant differences. Higher in SUI: plasma serine protease inhibitor (SERPINA5), leucine-rich alpha-2-glycoprotein (LRG1), lysosomal alpha-glucosidase (GAA), and peptidyl-prolyl cis- trans isomerase A (PPIA), associated with inflammation, degradation of glycogen to glucose. Lower in SUI: uromodulin and TALPID3, associated with prevention of urinary tract infection, water/electrolyte balance, and kidney innate immunity, and ciliogenesis and sonic hedgehog/SHH signaling |
| Koch et al., 2018 | SUI | Proteome | MS | 19 | 19 | 7012 proteins identified, 33 proteins were detected in SUI, not in controls, involved in inflammatory response, response to cellular stress, coagulation and cytoskeleton stability/motility. Five proteins were detected in controls, not in SUI, involved in immune/DNA damage response. |
| Author, Year | Type of Animal, Strain, etc. | Genome Transcriptome Proteome | Assay Method | No. of SUI Subjects | No. of Controls | Summary of Findings |
|---|---|---|---|---|---|---|
| Lin et al., 2009 | Sprague-Dawley rats, pregnant, primiparous | Transcriptome | Microarray | 10 | 14 | 23 genes overexpressed and 19 genes underexpressed associated with: apoptosis, neuron related, Rho A/Rho kinase pathway related, smooth muscle related, TGF signaling pathway related, wnt/Frizzled signaling pathway related, cellular adhesion, cellular metabolism, and transcriptional regulation. |
| Chen et al., 2013 | Virgin C57BL/6 strain mice, aged 6–8 weeks | Proteome | 2D DIGE and LC–MS/MS, WB, immunofluorescence staining, and IHC | 6 | 6 | 68 differentially expressed proteins, 19 proteins up-regulated and 49 were down-regulated. Involved in generation of precursor metabolites and energy, oxidation of reduction, regulation of apoptosis, and glycolysis. Myosin expression in the urethra was significantly decreased in the 8-mm VD group as compared with the non-instrumented control group |
| Chen et al., 2015 | ACTB-Cre/Esr1 knockout (Esr1−/−) mice and WT (Esr1 +/+) mice | Proteome | Genotyping via PCR, IHC and WB | 6x2 | 6 | 11 proteins differentially expressed in Esr1+/+ and Esr1−/− female mice. Five proteins were down-regulated (TPM3, DDAH2, DESM, TCTP, CAPR2) and six were up-regulated (MYL1, MLRS, MYL3, NDUS8, MYL1, UCHL1). Involved in muscle development, contraction, and regulation, as well as immune response (amphoterin signaling and phagocytosis), proteolysis, and cell adhesion (platelet aggregation and integrin-mediated cell–matrix adhesion). |
| Certainty Assessment | Certainty | ||||||
|---|---|---|---|---|---|---|---|
| Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | ||
| Extracellular matrix remodeling is associated with SUI | Observational studies | Serious 1 | Not serious | Not serious | Serious 4 | Not evaluated 5 | Moderate |
| Estrogen receptor expression is associated with SUI in premenopausal women | Observational studies | Serious 1 | Serious 2 | Serious 3 | Serious 4 | Not evaluated 5 | Low |
| Oxidative stress is associated with SUI | Observational studies | Serious 1 | Serious 2 | Serious 3 | Serious 4 | Not evaluated 5 | Low |
| Apoptosis is associated with SUI | Observational studies | Serious 1 | Serious 2 | Serious 3 | Serious 4 | Not evaluated 5 | Low |
| Inflammation is associated with SUI | Observational studies | Serious 1 | Serious 2 | Serious 3 | Serious 4 | Not evaluated 5 | Low |
| Neurodegenerative processes are associated with SUI | Observational studies | Serious 1 | Serious 2 | Serious 3 | Serious 4 | Not evaluated 5 | Low |
| Muscle cell differentiation is associated with SUI | Observational studies | Serious 1 | Serious 2 | Serious 3 | Serious 4 | Not evaluated 5 | Low |
| Muscle cell contractility is associated with SUI | Observational studies | Serious 1 | Serious 2 | Serious 3 | Serious 4 | Not evaluated 5 | Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Post, W.M.; Widomska, J.; Grens, H.; Coenen, M.J.H.; Martens, F.M.J.; Janssen, D.A.W.; IntHout, J.; Poelmans, G.; Oosterwijk, E.; Kluivers, K.B. Molecular Processes in Stress Urinary Incontinence: A Systematic Review of Human and Animal Studies. Int. J. Mol. Sci. 2022, 23, 3401. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23063401
Post WM, Widomska J, Grens H, Coenen MJH, Martens FMJ, Janssen DAW, IntHout J, Poelmans G, Oosterwijk E, Kluivers KB. Molecular Processes in Stress Urinary Incontinence: A Systematic Review of Human and Animal Studies. International Journal of Molecular Sciences. 2022; 23(6):3401. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23063401
Chicago/Turabian StylePost, Wilke M., Joanna Widomska, Hilde Grens, Marieke J. H. Coenen, Frank M. J. Martens, Dick A. W. Janssen, Joanna IntHout, Geert Poelmans, Egbert Oosterwijk, and Kirsten B. Kluivers. 2022. "Molecular Processes in Stress Urinary Incontinence: A Systematic Review of Human and Animal Studies" International Journal of Molecular Sciences 23, no. 6: 3401. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23063401