Implementation and Operational Analysis of an Interactive Intensive Care Unit within a Smart Health Context

 ,
,  ,
,  ,
,  ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Scenario under Test: Intensive Care Units (ICU)
2.1.1. Brief Overview of ICUs
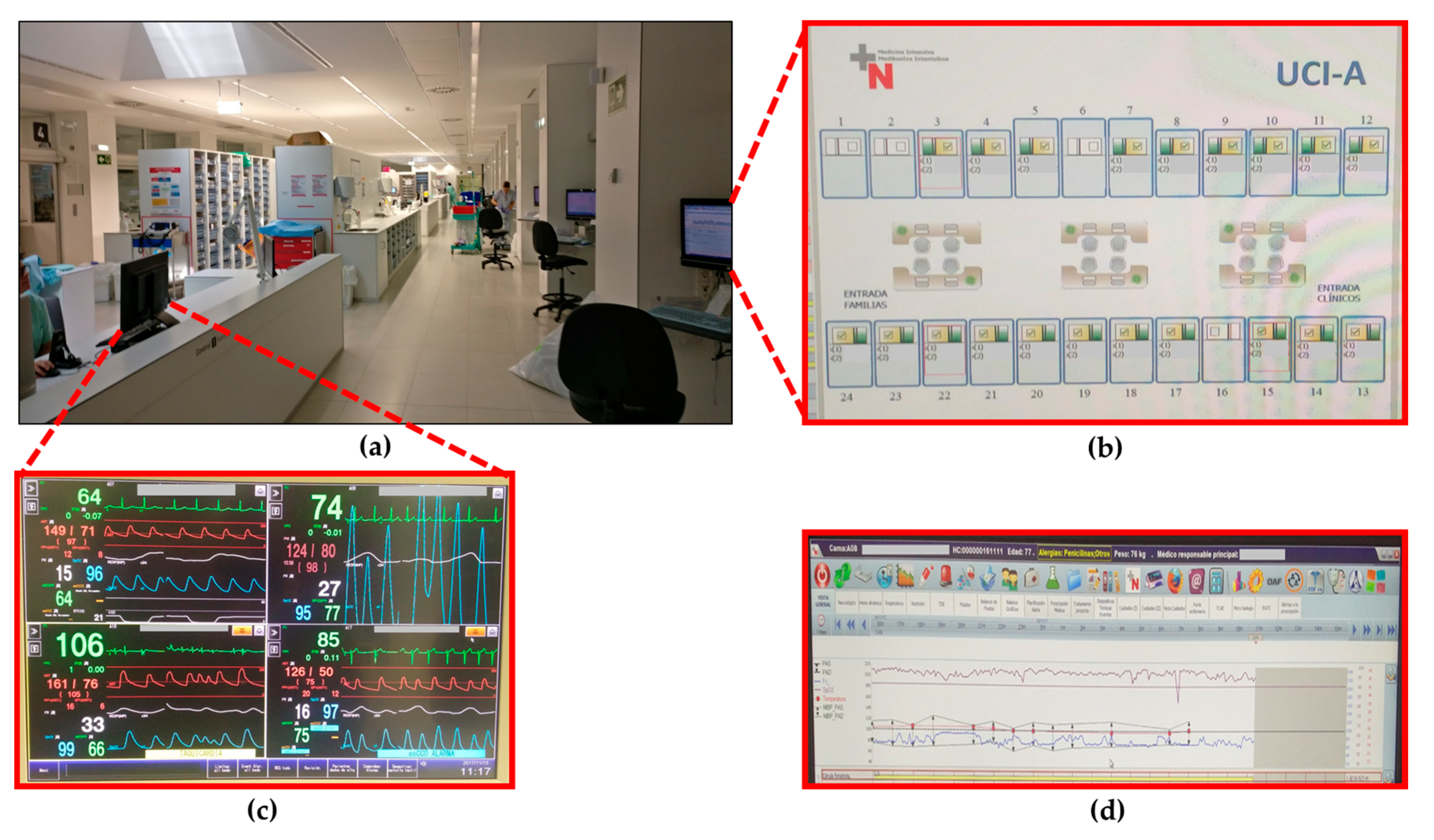
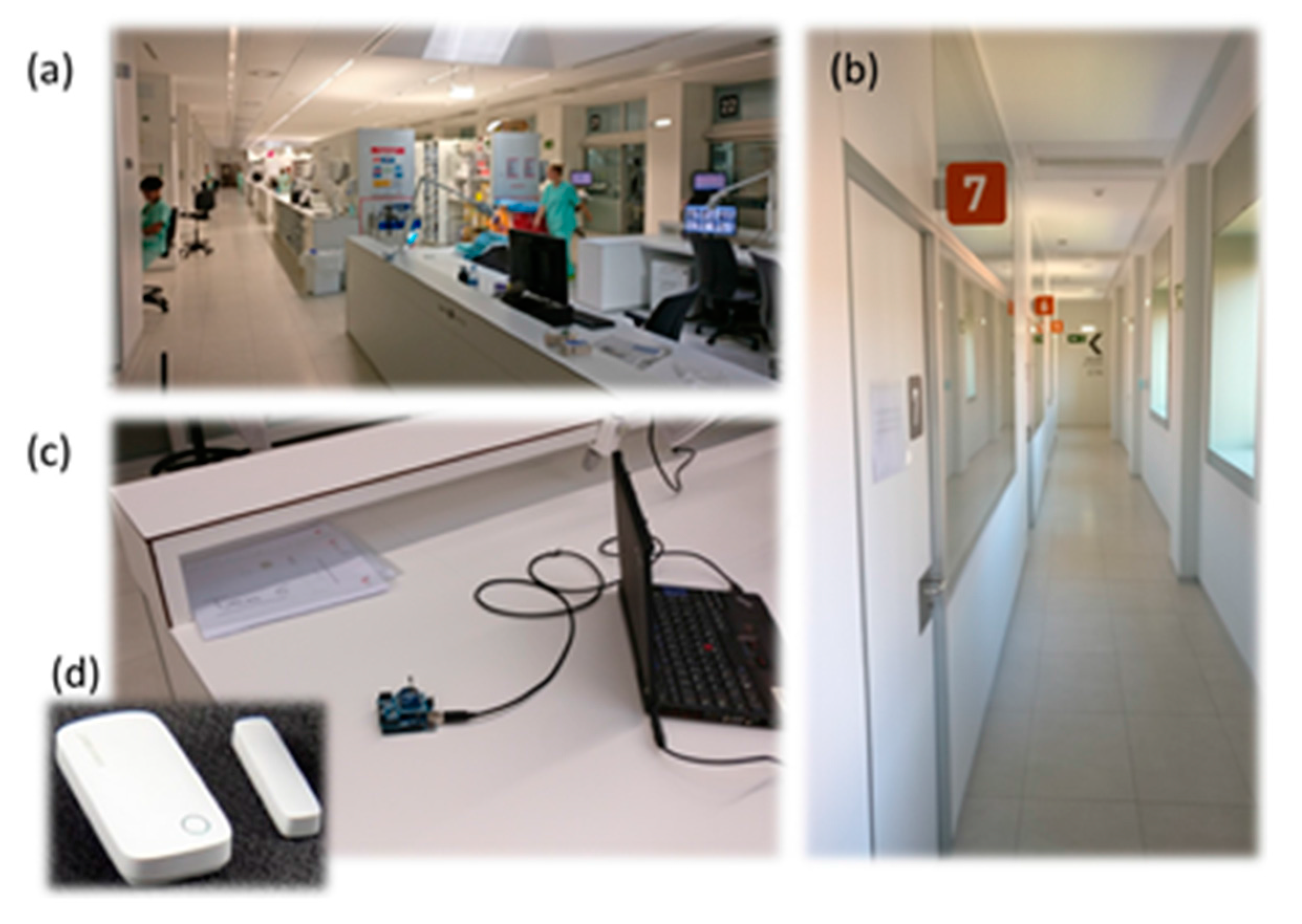
2.1.2. ICU of the “Hospital Complex of Navarra” (HCN)
2.2. Ray Launching Simulation Technique
2.2.1. Background
2.2.2. The Ray Launching Technique
3. Results
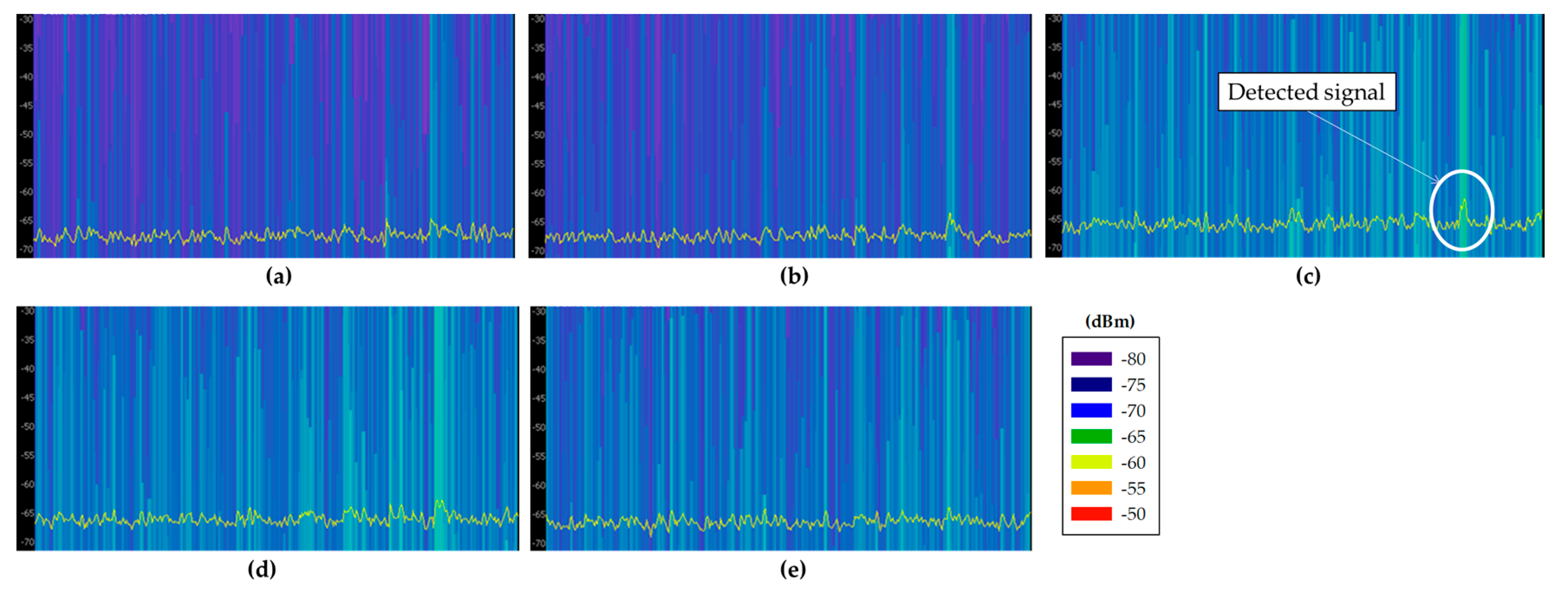
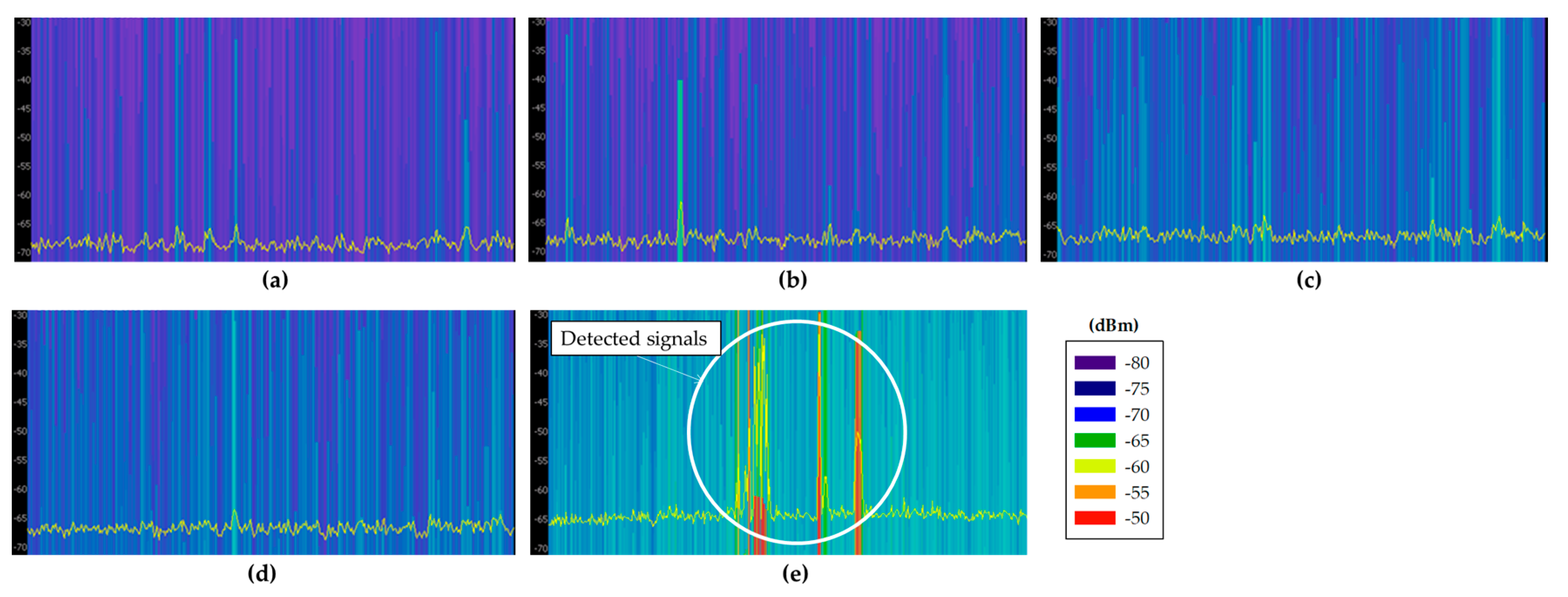
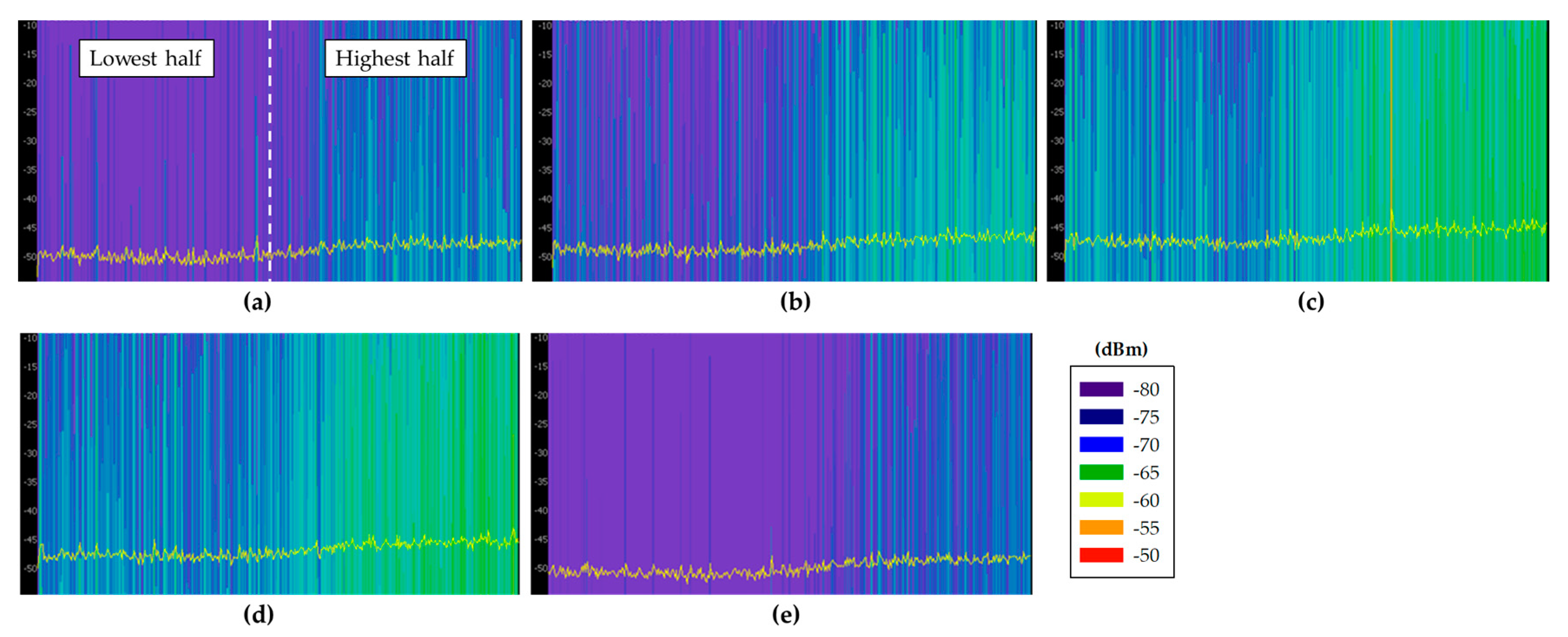
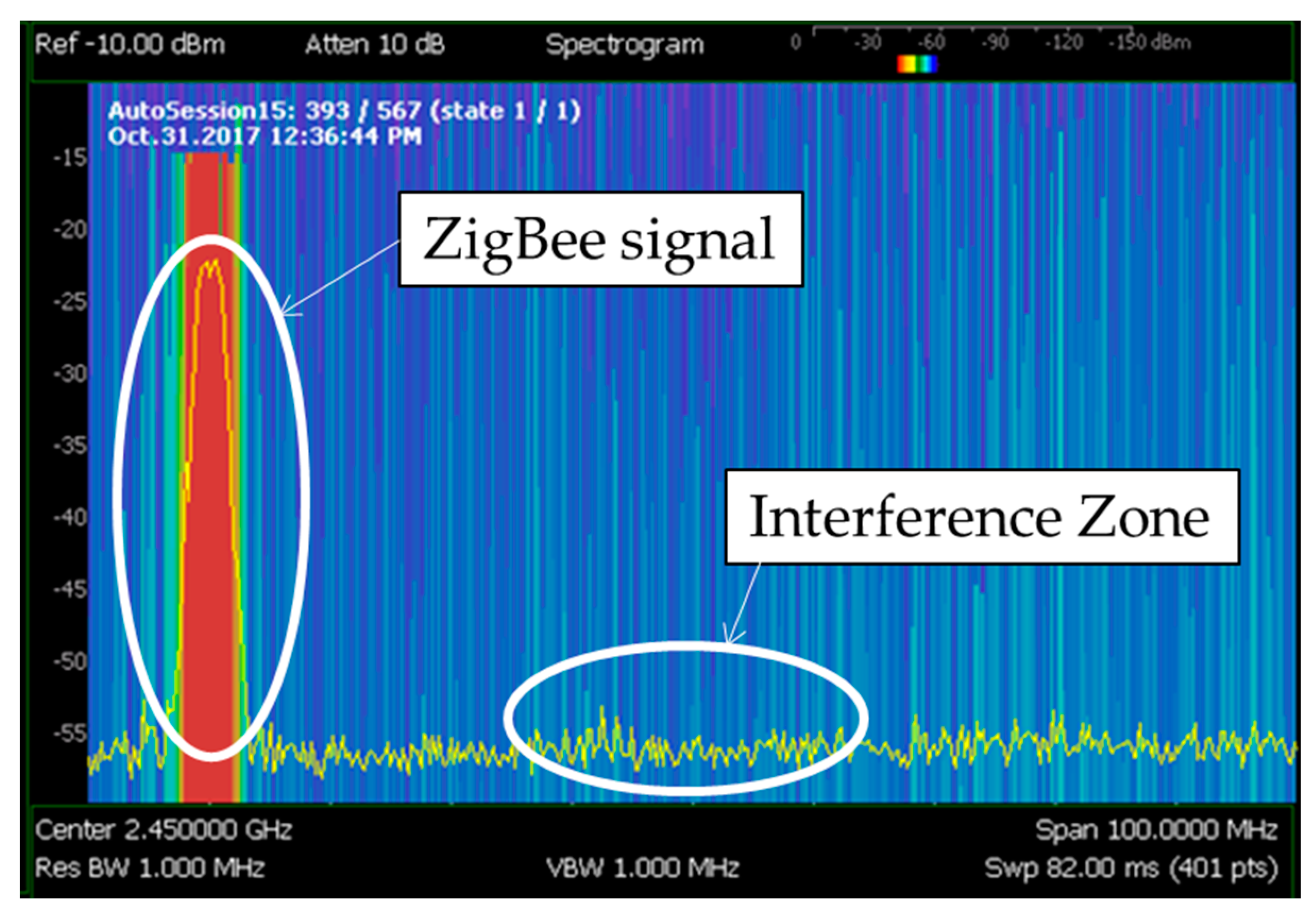
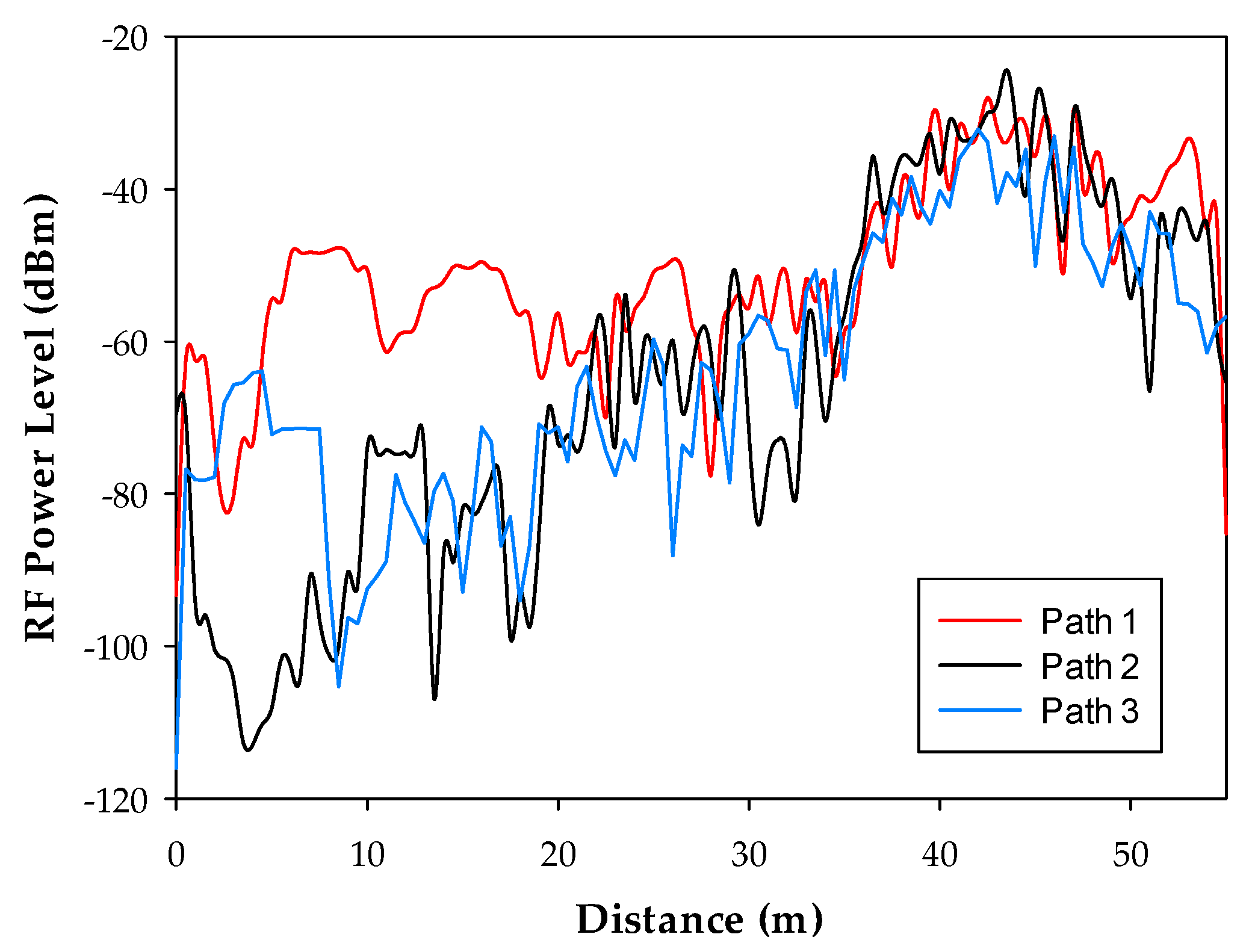
3.1. RF Assessment of the Environment
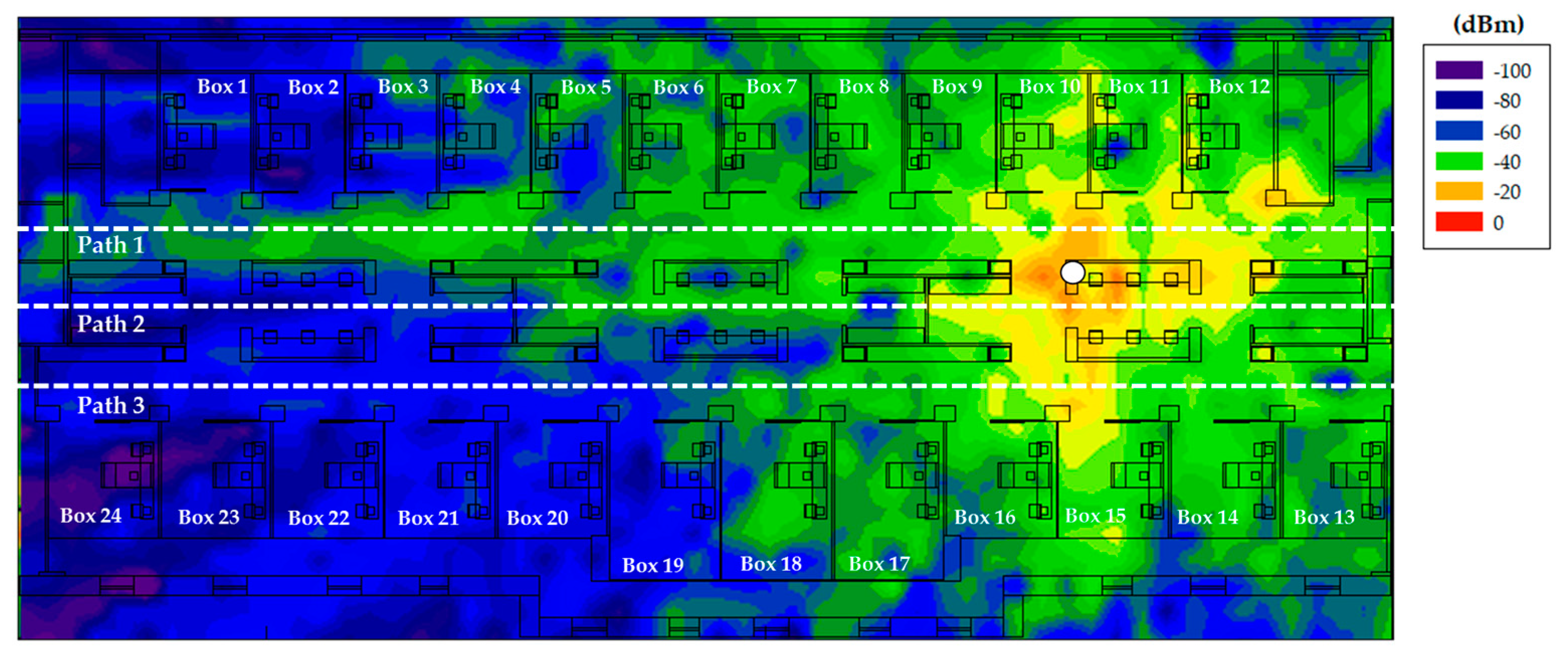
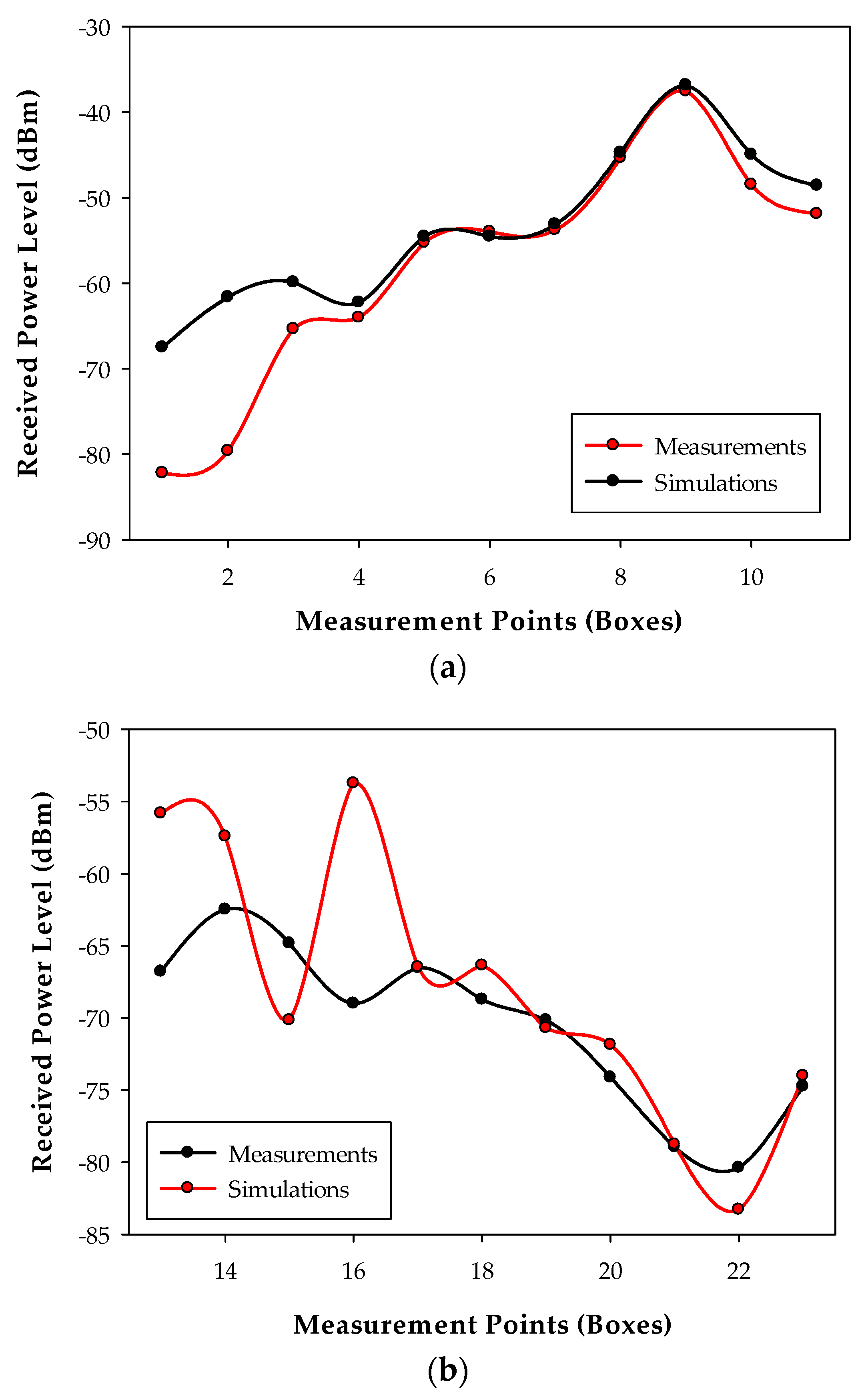
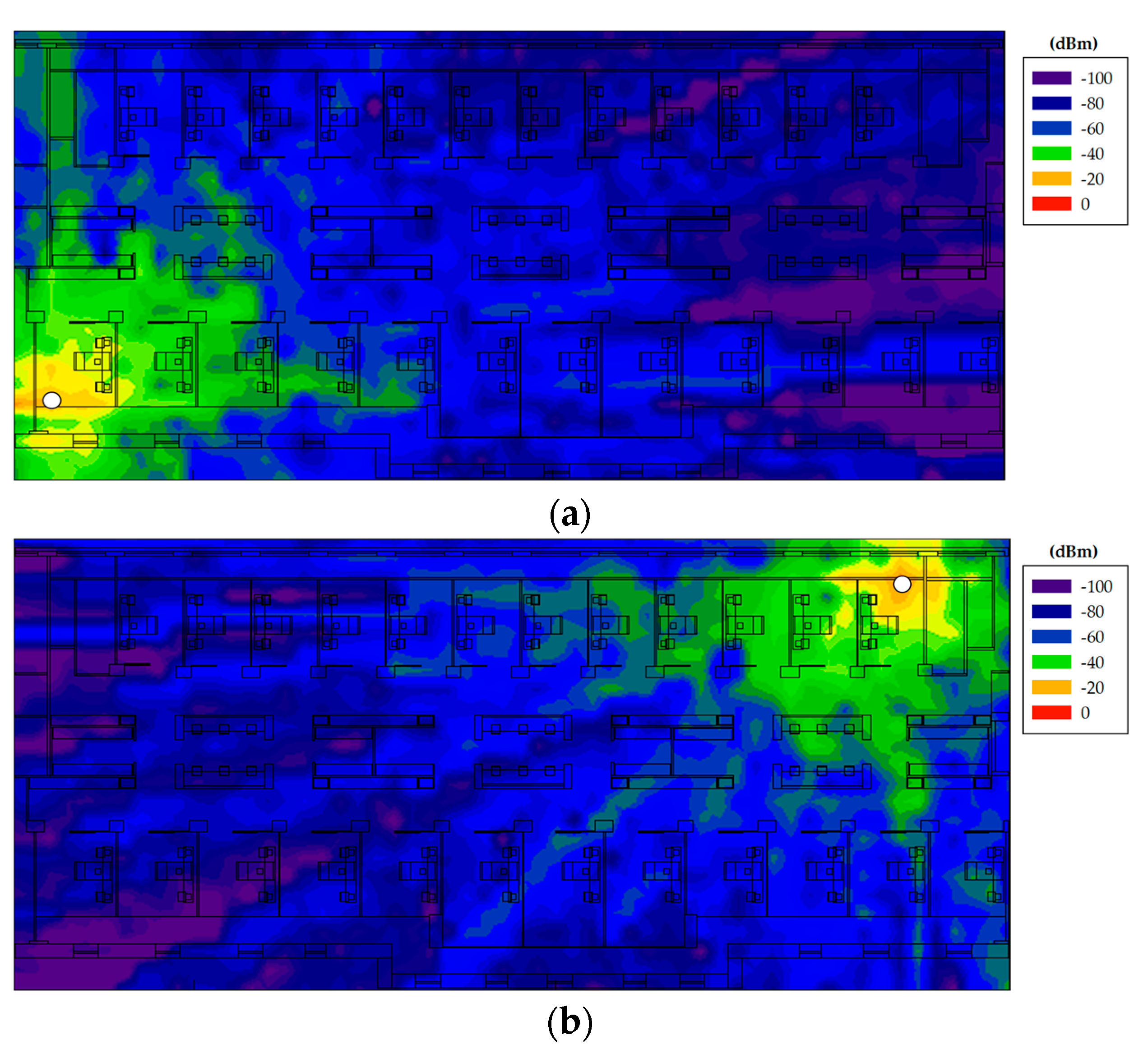
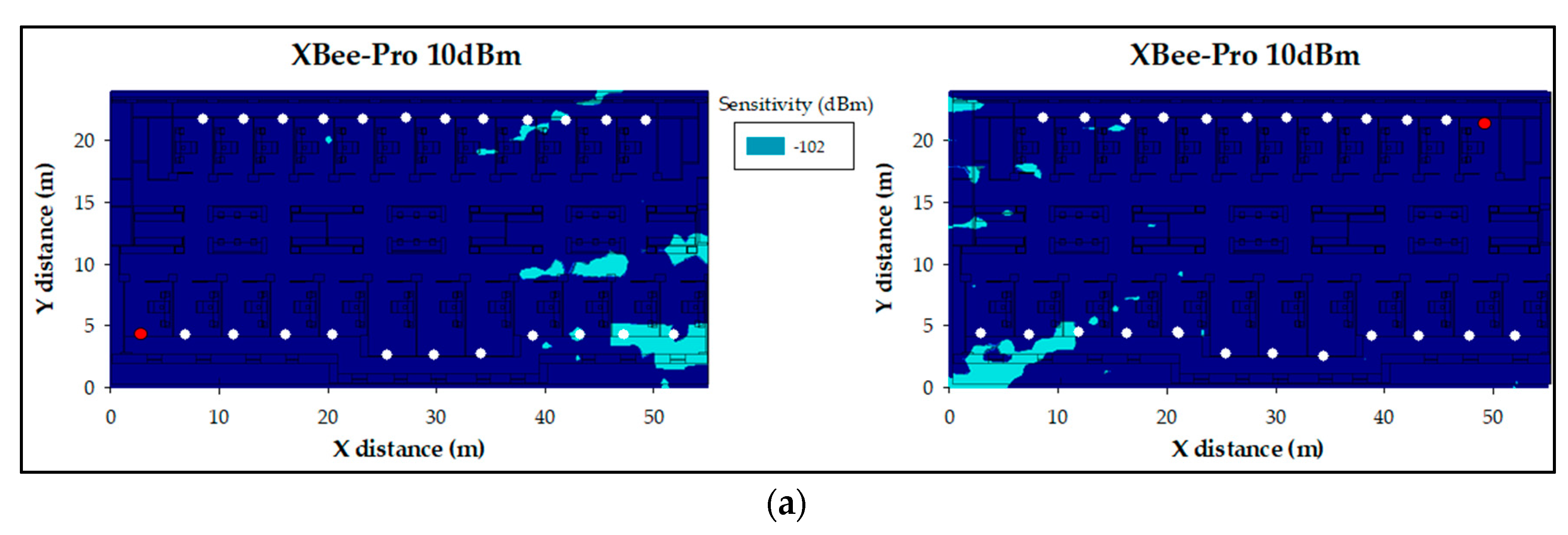
3.2. Ray Launching Simulation Results
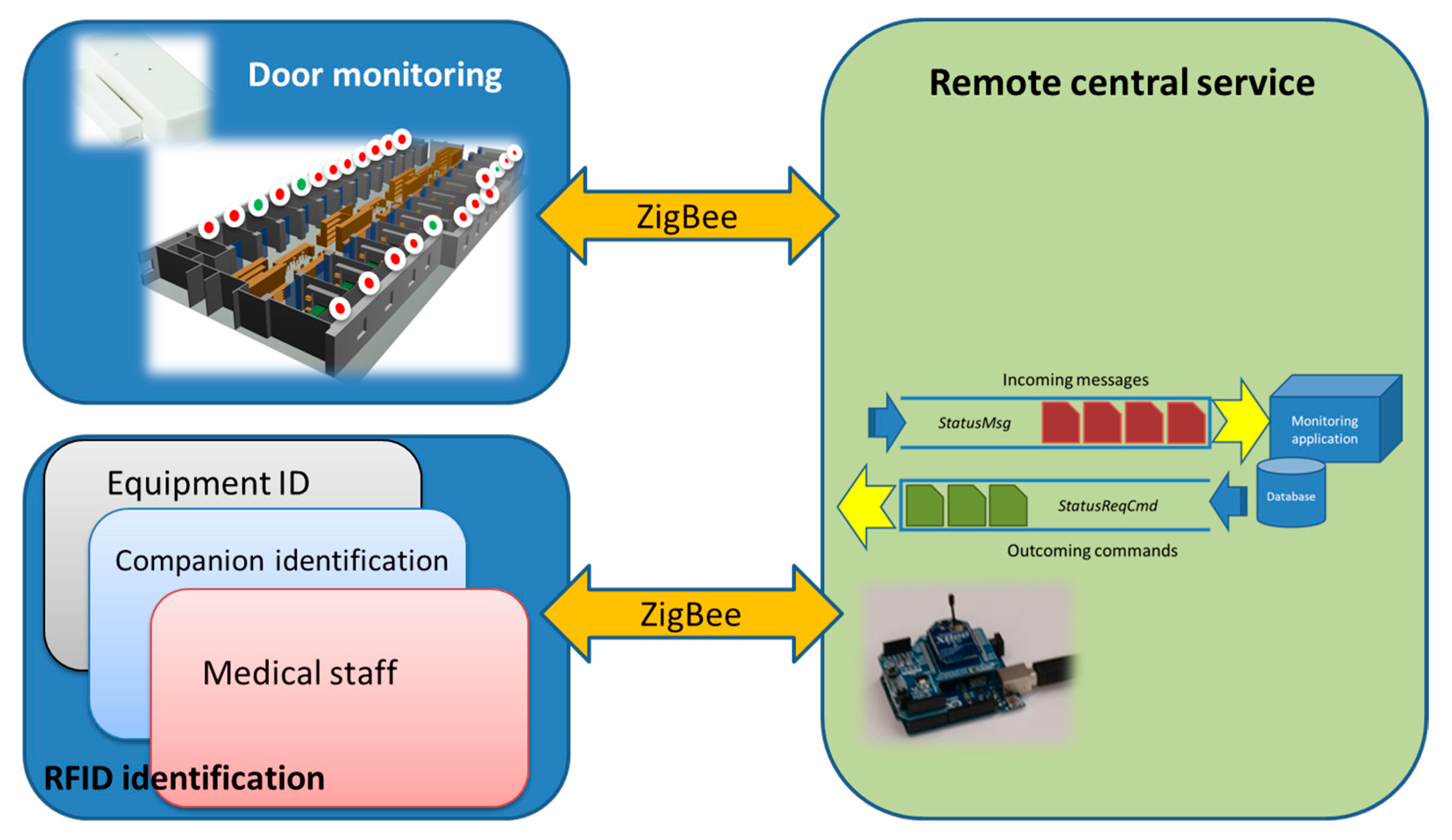
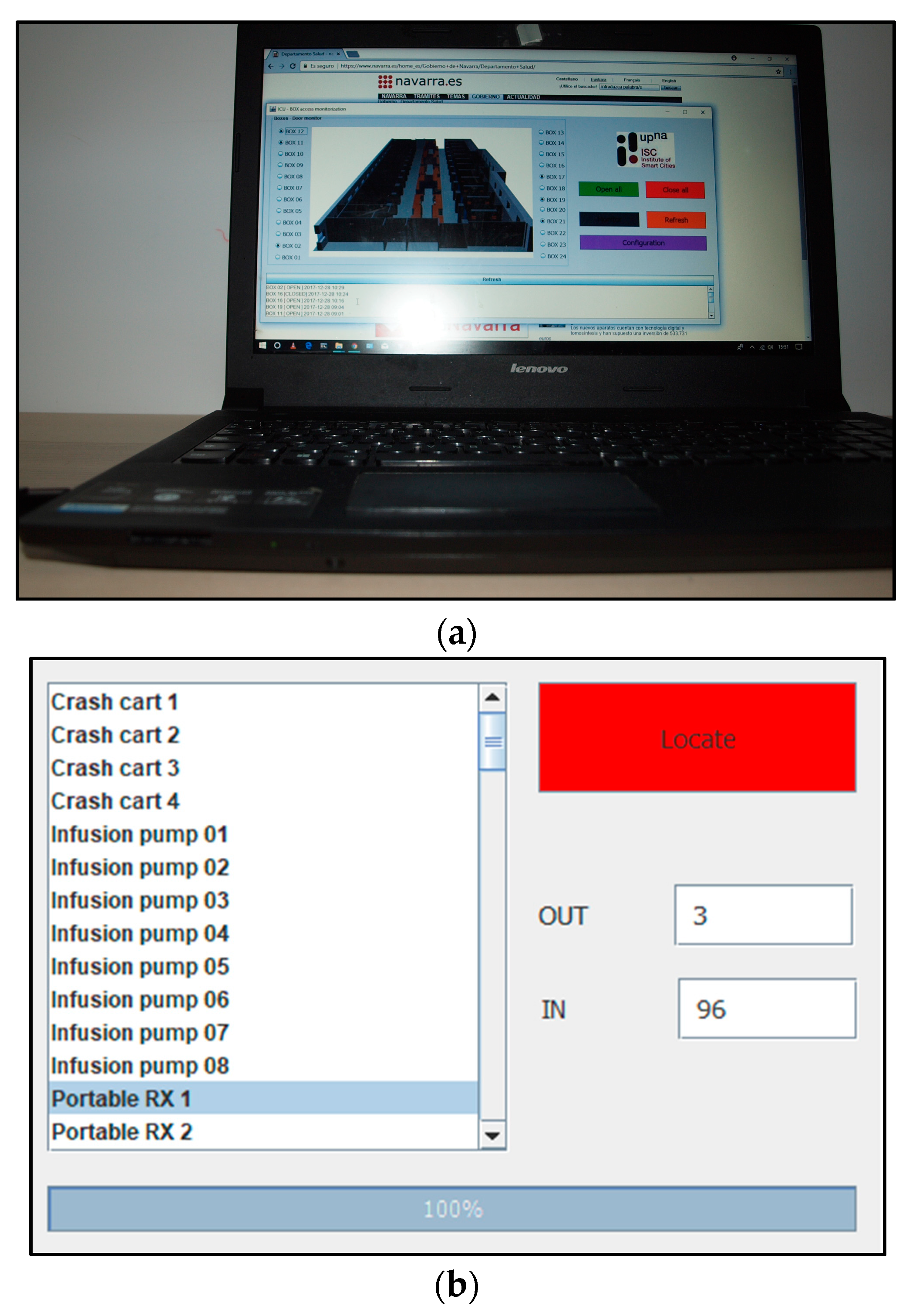
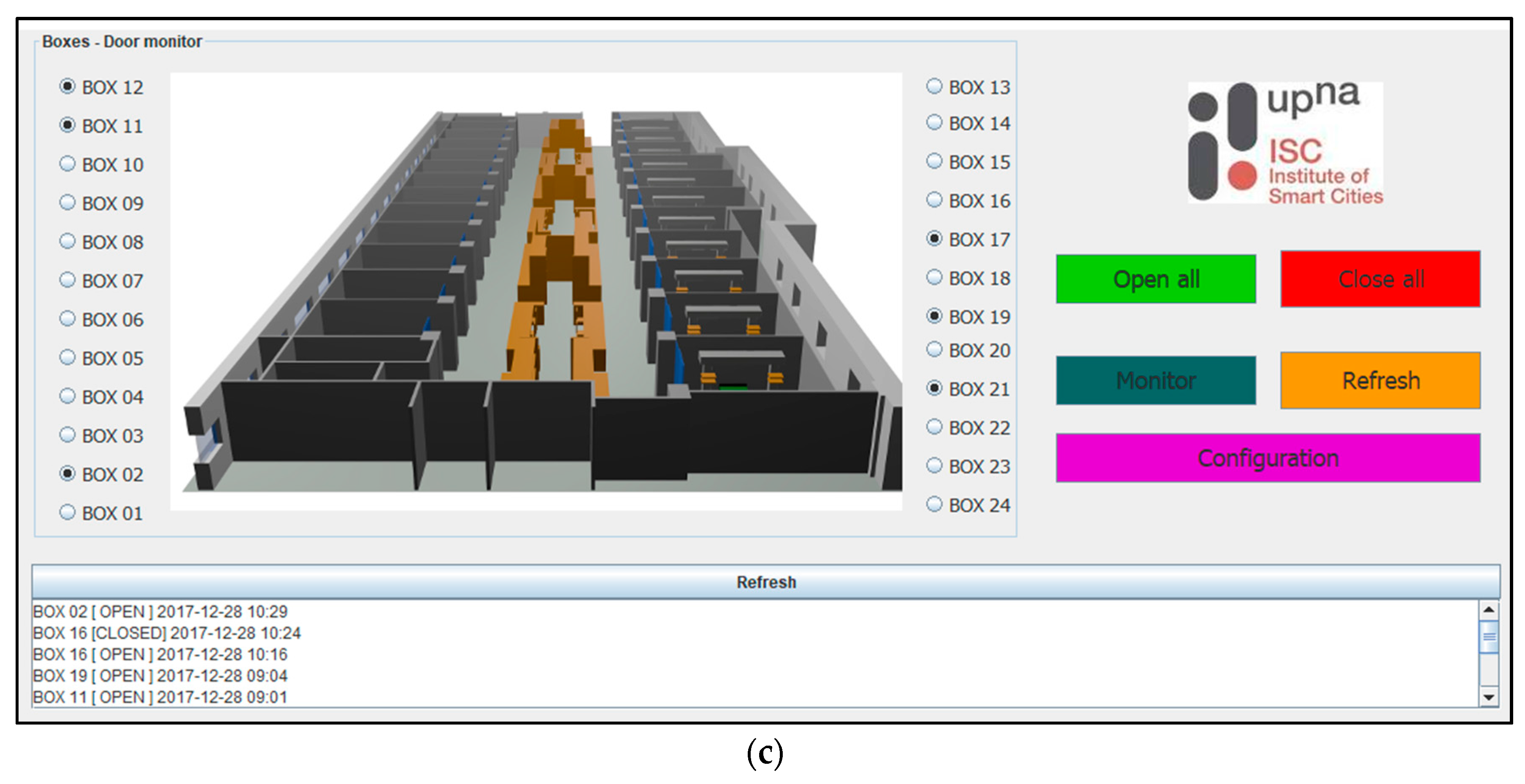
4. Visitor Access Control Application
5. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Aguirre, E.; Led, S.; Lopez-Iturri, P.; Azpilicueta, L.; Serrano, L.; Falcone, F. Implementation of Context Aware e-Health Environments Based on Social Sensor Networks. Sensors 2016, 16, 310. [Google Scholar] [CrossRef] [PubMed]
- Solanas, A.; Patsakis, C.; Conti, M.; Vlachos, I.S.; Ramos, V.; Falcone, F.; Postolache, O.; Perez-Martınez, P.A.; Di Pietro, R.; Perrea, D.N.; et al. Smart Health: A Context-Aware Health Paradigm within Smart Cities. IEEE Commun. Mag. 2014, 52, 74–81. [Google Scholar] [CrossRef]
- Shieh, J.; Fu, M.; Huang, S.; Kao, M. Comparison of the Applicability of Rule-Based and Self-Organizing Fuzzy Logic Controllers for Sedation Control of Intracranial Pressure Pattern in a Neurosurgical Intensive Care Unit. IEEE Trans. Biomed. Eng. 2006, 53, 1700–1705. [Google Scholar] [CrossRef] [PubMed]
- Gholami, B.; Bailey, J.M.; Haddad, W.M.; Tannenbaum, A.R. Clinical Decision Support and Closed-Loop Control for Cardiopulmonary Management and Intensive Care Unit Sedation Using Expert Systems. IEEE Trans. Control Syst. Technol. 2012, 20, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Clifford, G.; Silva, I.; Moody, B.; Li, Q.; Kella, D.; Chahin, A.; Kooistra, T.; Perry, D.; Mark, R. False alarm reduction in critical care. Physiol. Meas. 2016, 37, 5–23. [Google Scholar] [CrossRef] [PubMed]
- Behar, J.; Oster, J.; Li, Q.; Clifford, G.D. ECG Signal Quality during Arrhythmia and Its Application to False Alarm Reduction. IEEE Trans. Biomed. Eng. 2013, 60, 1660–1666. [Google Scholar] [CrossRef] [PubMed]
- Krasteva, V.; Jekova, I.; Leber, R.; Schmid, R.; Abächerli, R. Real-time arrhythmia detection with supplementary ECG quality and pulse wave monitoring for the reduction of false alarms in ICUs. Physiol. Meas. 2015, 37, 1273–1297. [Google Scholar] [CrossRef] [PubMed]
- Lameski, P.; Zdravevski, E.; Koceski, S.; Kulakov, A.; Trajkovik, V. Suppression of Intensive Care Unit False Alarms Based on the Arterial Blood Pressure Signal. IEEE Access 2017, 5, 5829–5836. [Google Scholar] [CrossRef]
- Villarroel, M.; Guazzi, A.; Jorge, J.; Davis, S.; Watkinson, P.; Green, G.; Shenvi, A.; McCormick, K.; Tarassenko, L. Continuous non-contact vital sign monitoring in neonatal intensive care unit. Healthc. Technol. Lett. 2014, 1, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Raboshchuk, G.; Nadeu, C.; Jancovic, P.; Peiro Lilja, A.; Kokuer, M.; Muñoz Mahamud, B.; de Veciana, A.R. A Knowledge-Based Approach to Automatic Detection of Equipment Alarm Sounds in a Neonatal Intensive Care Unit Environment. J. Transl. Eng. Health Med. 2017. [Google Scholar] [CrossRef]
- Silva, R.; Silva, J.; Silva, A.; Pinto, F.; Simek, M.; Boavida, F. Wireless Sensor Networks in Intensive Care Units. In Proceedings of the IEEE International Conference on Communications Workshops, Dresden, Germany, 14–18 June 2009; pp. 1–5. [Google Scholar]
- Smith, G.; Nielsen, M. Criteria for admission. BMJ 1999, 318, 1544–1547. [Google Scholar] [CrossRef] [PubMed]
- Palanca, I.; Sánchez, A.; Elola, J. Unidad de Cuidados Intensivos: Estándares y Recomendaciones; Ministerio de Sanidad y Política Social: Madrid, Spain, 2010. [Google Scholar]
- Haslam, J.; Ball, J.; Rhodes, A.; MacNaughton, P. Monitoring. In ABC of Intensive Care; Nimmo, G.R., Singer, M., Eds.; Wiley-Blackwell: Hoboken, NJ, USA, 2011; ISBN 978-1-4051-7803-7. [Google Scholar]
- Batchelor, A.; Nightingale, N. General principles of intensive management. In ABC of Intensive Care; Nimmo, G.R., Singer, M., Eds.; Wiley-Blackwell: Hoboken, NJ, USA, 2011; ISBN 978-1-4051-7803-7. [Google Scholar]
- Bennett, D.; Bion, J. Organisation of intensive care. BMJ 1999, 318, 1468–1470. [Google Scholar] [CrossRef] [PubMed]
- Giannini, A.; Garrouste-Orgeas, M.; Latour, J.M. What’s new in ICU visiting policies: Can we continue to keep the doors closed? Intensiv. Care Med. 2014, 40, 730–733. [Google Scholar] [CrossRef] [PubMed]
- McAdam, J.L.; Puntillo, K.A. Open visitation policies and practices in US ICUs: Can we ever get there? Crit. Care 2013, 17, 171. [Google Scholar] [CrossRef] [PubMed]
- Kyrö, M.; Haneda, K.; Simola, J.; Takizawa, K.; Hagiwara, H.; Vainikainen, P. Statistical Channel Models for 60 GHz Radio Propagation in Hospital Environments. IEEE Trans. Antennas Propag. 2012, 60, 1569–1577. [Google Scholar] [CrossRef]
- Cui, P.-F.; Yu, Y.; Lu, W.-J.; Liu, Y.; Zhu, H.-B. Measurement and Modeling of Wireless Off-Body Propagation Characteristics under Hospital Environment at 6–8.5 GHz. IEEE Access 2017, 5, 10915–10923. [Google Scholar] [CrossRef]
- Iskander, M.F.; Yun, Z. Propagation prediction models for wireless communication systems. IEEE Trans. Microw. Theory Tech. 2002, 50, 662–673. [Google Scholar] [CrossRef]
- Islam, M.J.; Reza, A.W.; Kausar, A.S.M.Z.; Ramiah, H. New Ray Tracing Method to Investigate the Various Effects on Wave Propagation in Medical Scenario: An Application of Wireless Body Area Network. Sci. World J. 2014, 2014, 306270. [Google Scholar] [CrossRef] [PubMed]
- Järveläinen, J.; Haneda, K.; Kyro, M.; Kolmonen, V.-M.; Takada, J.; Hagiwara, H. 60 GHz Radio Wave Propagation Prediction in a Hospital Environment Using an Accurate Room Structural Model. In Proceedings of the Lourghborough Antennas & Propagation Conference, Loughborough, UK, 12–13 November 2012. [Google Scholar]
- Schäfer, T.M.; Wiesbeck, W. Simulation of Radiowave Propagation in Hospitals Based on FDTD and Ray-Optical Methods. IEEE Trans. Antennas Propag. 2005, 53, 2181–2388. [Google Scholar] [CrossRef]
- Granda, F.; Azpilicueta, L.; Vargas-Rosales, C.; Lopez-Iturri, P.; Aguirre, E.; Astrain, J.J.; Villadangos, J.; Falcone, F. Spatial Characterization of Radio Propagation Channel in Urban Vehicle-to-Infrastructure Environments to Support WSNs Deployment. Sensors 2017, 17, 1313. [Google Scholar] [CrossRef] [PubMed]
- Azpilicueta, L.; López-Iturri, P.; Aguirre, E.; Martínez, C.; Astráin, J.J.; Villadangos, J.; Falcone, F. Evaluation of Deployment Challenges of Wireless Sensor Networks at Signalized Intersections. Sensors 2016, 16, 1140. [Google Scholar] [CrossRef] [PubMed]
- Azpilicueta, L.; Astrain, J.J.; Lopez-Iturri, P.; Granda, F.; Vargas-Rosales, C.; Villadangos, J.; Perallos, A.; Bahillo, A.; Falcone, F. Optimization and Design of Wireless Systems for the Implementation of Context Aware Scenarios in Railway Passenger Vehicles. IEEE Trans. Intell. Transp. Syst. 2017, 18, 2838–2850. [Google Scholar] [CrossRef]
- Aguirre, A.; López-Iturri, P.; Azpilicueta, L.; Rivares, C.; Astráin, J.J.; Villadangos, J.; Falcone, F. Design and Performance Analysis of Wireless Body Area Networks in Complex Indoor e-Health Hospital Environments for Patient Remote Monitoring. Int. J. Distrib. Sens. Netw. 2016, 12. [Google Scholar] [CrossRef]
- Azpilicueta, L.; Rawat, M.; Rawat, K.; Ghannouchi, F.; Falcone, F. A Ray Launching-Neural Network Approach for Radio Wave Propagation Analysis in Complex Indoor Environments. IEEE Trans. Antennas Propag. 2014, 62, 2777–2786. [Google Scholar] [CrossRef]
- Azpilicueta, L.; Falcone, F.; Janaswamy, R. A Hybrid Ray Launching-Diffusion Equation Approach for Propagation Prediction in Complex Indoor Environments. IEEE Antennas Wirel. Propag. Lett. 2017, 16, 214–217. [Google Scholar] [CrossRef]
- Casino, F.; Azpilicueta, L.; López-Iturri, P.; Aguirre, E.; Falcone, F.; Solanas, A. Optimised Wireless Channel Characterisation in Large Complex Environments by Hybrid Ray Launching-Collaborative Filtering Approach. IEEE Antennas Wirel. Propag. Lett. 2017, 16, 780–783. [Google Scholar] [CrossRef]
- Kim, S.; Brendle, C.; Lee, H.-Y.; Walter, M.; Gloeggler, S.; Krueger, S.; Leonhardt, S. Evaluation of a 433 MHz Band Body Sensor Network for Biomedical Applications. Sensors 2013, 13, 898–917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conway, G.A.; Scanlon, W.G. Wearable Antennas for Medical Monitoring Systems. In Proceedings of the International Workshop on Antenna Technology (iWAT), Seoul, Korea, 4–6 March 2015. [Google Scholar]
- Hemapriya, D.; Viswanath, P.; Mithra, V.M.; Nagalakshmi, S.; Umarani, G. Wearable Medical Devices—Design Challenges and Issues. In Proceedings of the IEEE International Conference on Innovations in Green Energy and Healthcare Technologies (ICIGEHT’17), Coimbatore, India, 16–18 March 2017. [Google Scholar]
- Balid, W.; Al Kalaa, M.O.; Rajab, S.; Tafish, H.; Refai, H.H. Development of Measurement Techniques and Tools for Coexistence Testing of Wireless Medical Devices. In Proceedings of the IEEE Wireless Communications and Networking Conference Workshops (WCNCW), Doha, Qatar, 3–6 April 2016. [Google Scholar]
- Staniec, K. IEEE 802.15.4 (ZigBee) immunity to in-band interference and multipath propagation. In Proceedings of the Radio and Antenna Days of the Indian Ocean (RADIO), Belle Mare, Mauritius, 21–24 September 2015. [Google Scholar]
- Lopez-Iturri, P.; Aguirre, E.; Azpilicueta, L.; Astrain, J.J.; Villadangos, J.; Falcone, F. Implementation and Analysis of ISM 2.4 GHz Wireless Sensor Network Systems in Judo Training Venues. Sensors 2016, 16, 1247. [Google Scholar] [CrossRef] [PubMed]























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Equipment | Parameters/Techniques |
|---|---|
| Multi parameter monitor | Electrocardiogram |
| Capnography | |
| Arterial pressure | |
| Pulse oximetry | |
| Cardiac output | |
| Electroencephalogram (EEG) | |
| Bispectral Index (derived from EEG) | |
| Renal monitor | Slow continuous ultrafiltration |
| Continuous venovenous hemodiafiltration | |
| Continuous venovenous hemofiltration | |
| Molecular Adsorbent Recirculating System (MARS) | |
| Plasmapheresis | |
| Extracorporeal membrane oxygenation (ECMO) machine | Venovenous ECMO |
| Venoarterial ECMO | |
| Mechanical ventilator | Up to 60 different modes |
| High-flow oxygen therapy system | - |
| Hypothermia monitor | - |
| Antenna | Central Frequency | Bandwidth | Maximum Gain (dB) |
|---|---|---|---|
| FLEXI-SMA90-433 | 433 MHz | 20 MHz | Unknown |
| ANT-868-CW-HWR | 868 MHz | 30 MHz | 2 |
| ACA-4HSRPP-2458 | 2.45 GHz | 100 MHz | 1 |
| ACA-4HSRPP-2458 | 5.5 GHz | 600 MHz | 1 |
| Parameter | Value |
|---|---|
| Operation Frequency | 2.41 GHz |
| Data rate | 250 kbps |
| Transmitted power level | 18 dBm |
| Antenna type | Monopole |
| Antenna gain (Transmitter) | 1.2 dB |
| Antenna gain (Receiver) | 1 dB |
| Permitted reflections | 6 |
| Launched rays angular resolution | 1° |
| Cuboids size | 0.5 m × 0.5 m × 0.5 m |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopez-Iturri, P.; Aguirre, E.; Trigo, J.D.; Astrain, J.J.; Azpilicueta, L.; Serrano, L.; Villadangos, J.; Falcone, F. Implementation and Operational Analysis of an Interactive Intensive Care Unit within a Smart Health Context. Sensors 2018, 18, 389. https://0-doi-org.brum.beds.ac.uk/10.3390/s18020389
Lopez-Iturri P, Aguirre E, Trigo JD, Astrain JJ, Azpilicueta L, Serrano L, Villadangos J, Falcone F. Implementation and Operational Analysis of an Interactive Intensive Care Unit within a Smart Health Context. Sensors. 2018; 18(2):389. https://0-doi-org.brum.beds.ac.uk/10.3390/s18020389
Chicago/Turabian StyleLopez-Iturri, Peio, Erik Aguirre, Jesús Daniel Trigo, José Javier Astrain, Leyre Azpilicueta, Luis Serrano, Jesús Villadangos, and Francisco Falcone. 2018. "Implementation and Operational Analysis of an Interactive Intensive Care Unit within a Smart Health Context" Sensors 18, no. 2: 389. https://0-doi-org.brum.beds.ac.uk/10.3390/s18020389