Design and Validation of an FPGA-Based Configurable Transcranial Doppler Neurofeedback System for Chronic Pain Patients

 , ,
, ,  ,
,
Abstract
:1. Introduction
1.1. Related Work
1.2. Research Goals and Contributions
2. Materials and Methods
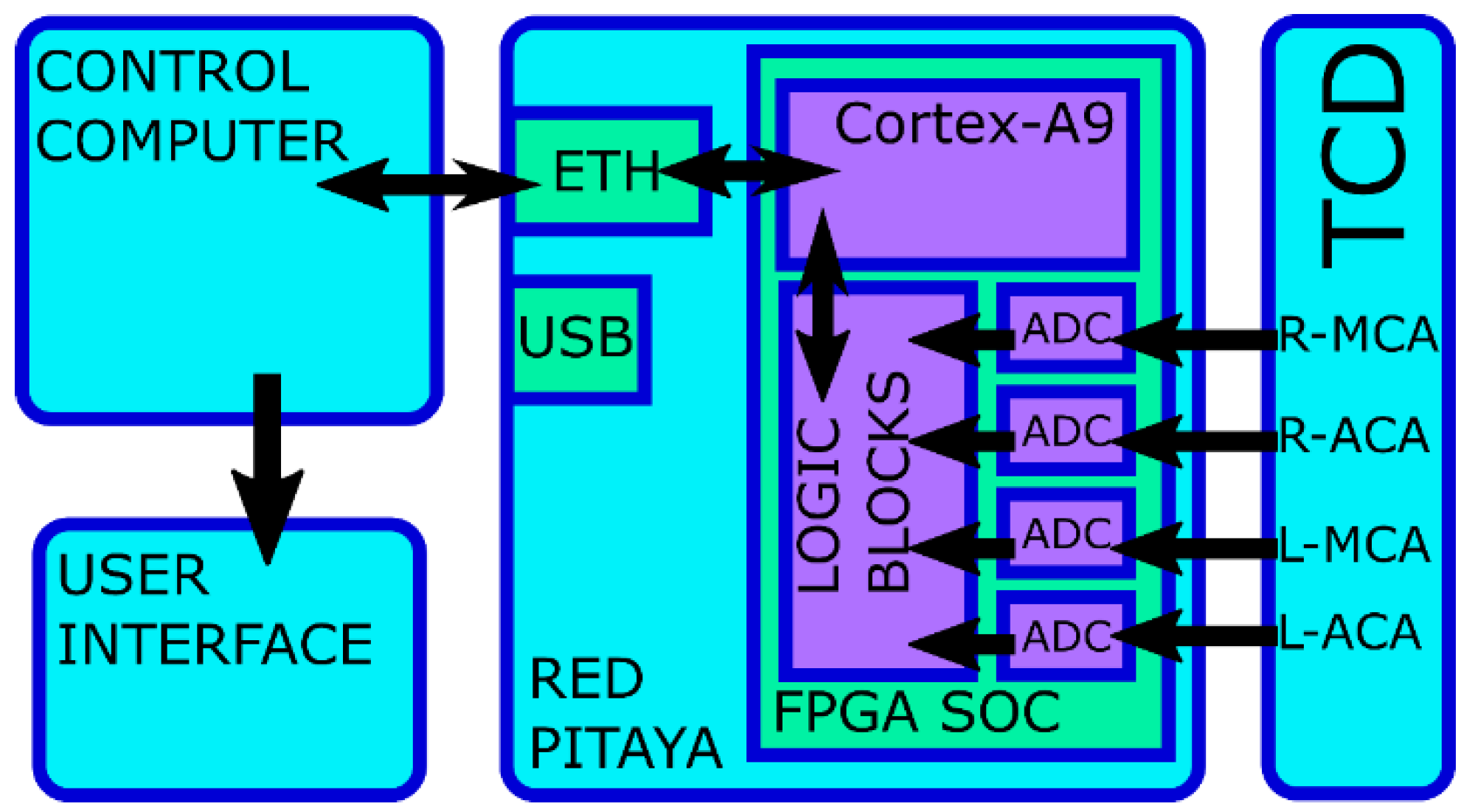
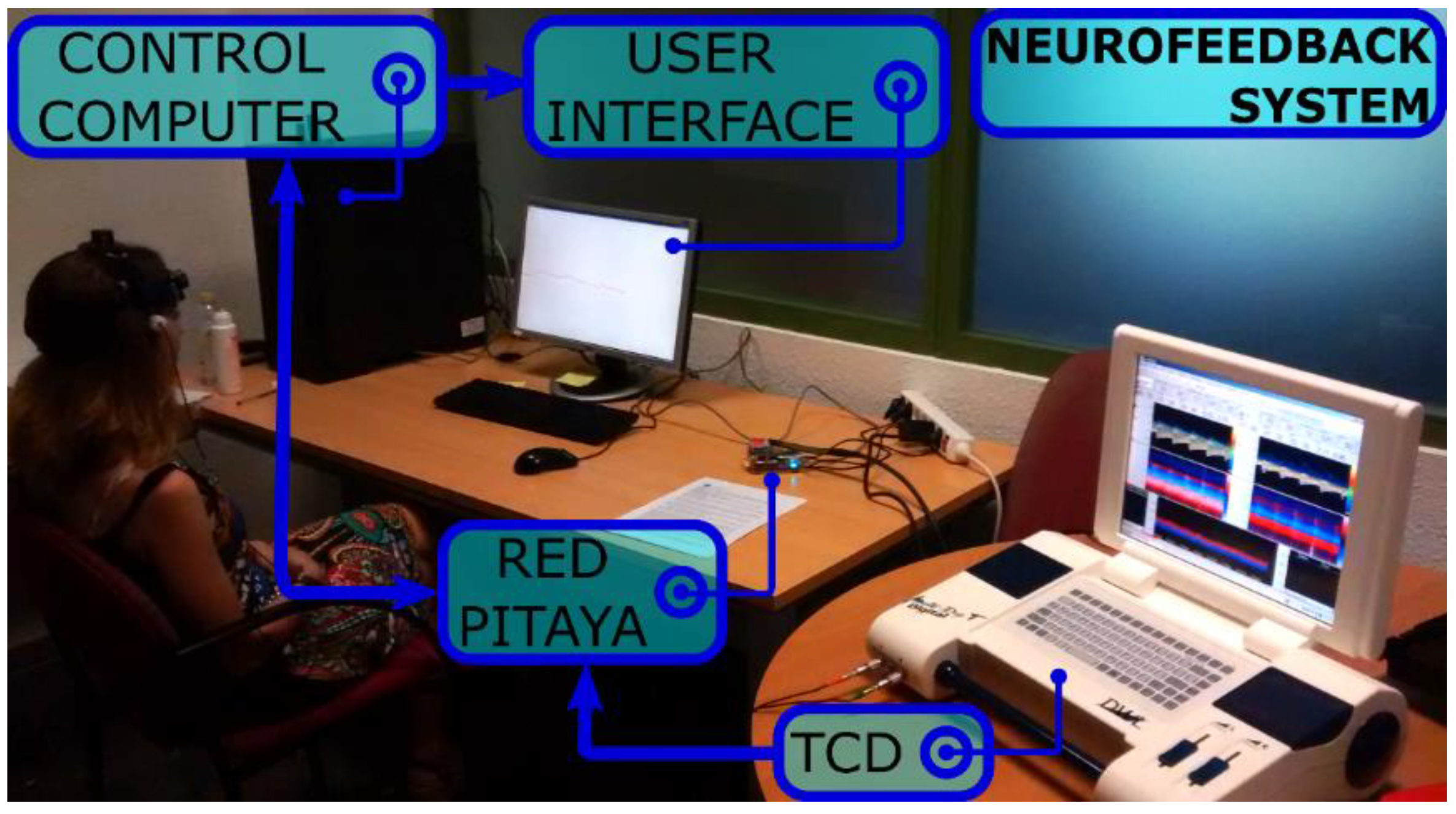
2.1. Technical Aspects of the System
2.1.1. Transcranial Doppler Monitoring
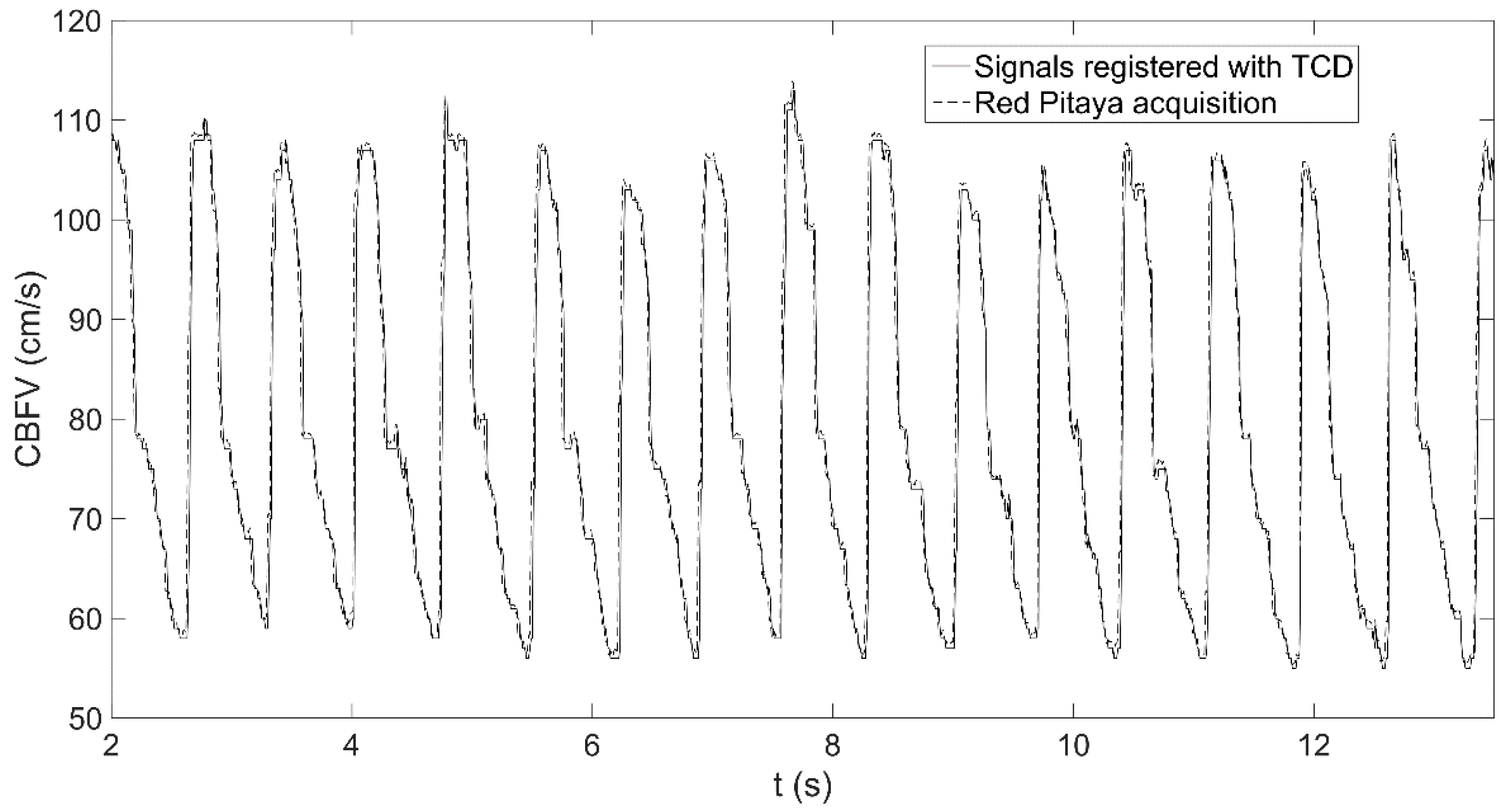
2.1.2. Digitalization
2.1.3. Data Processing
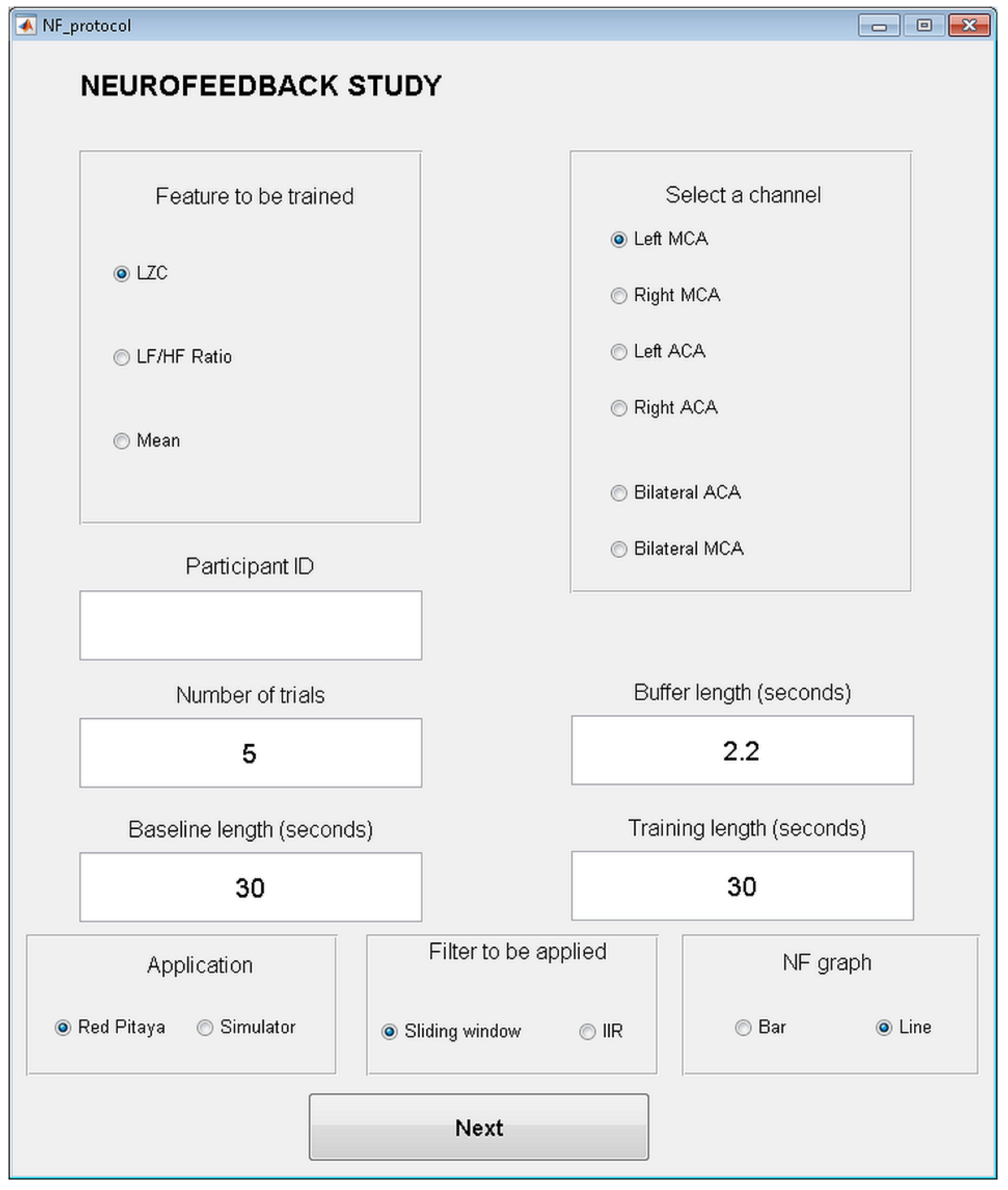
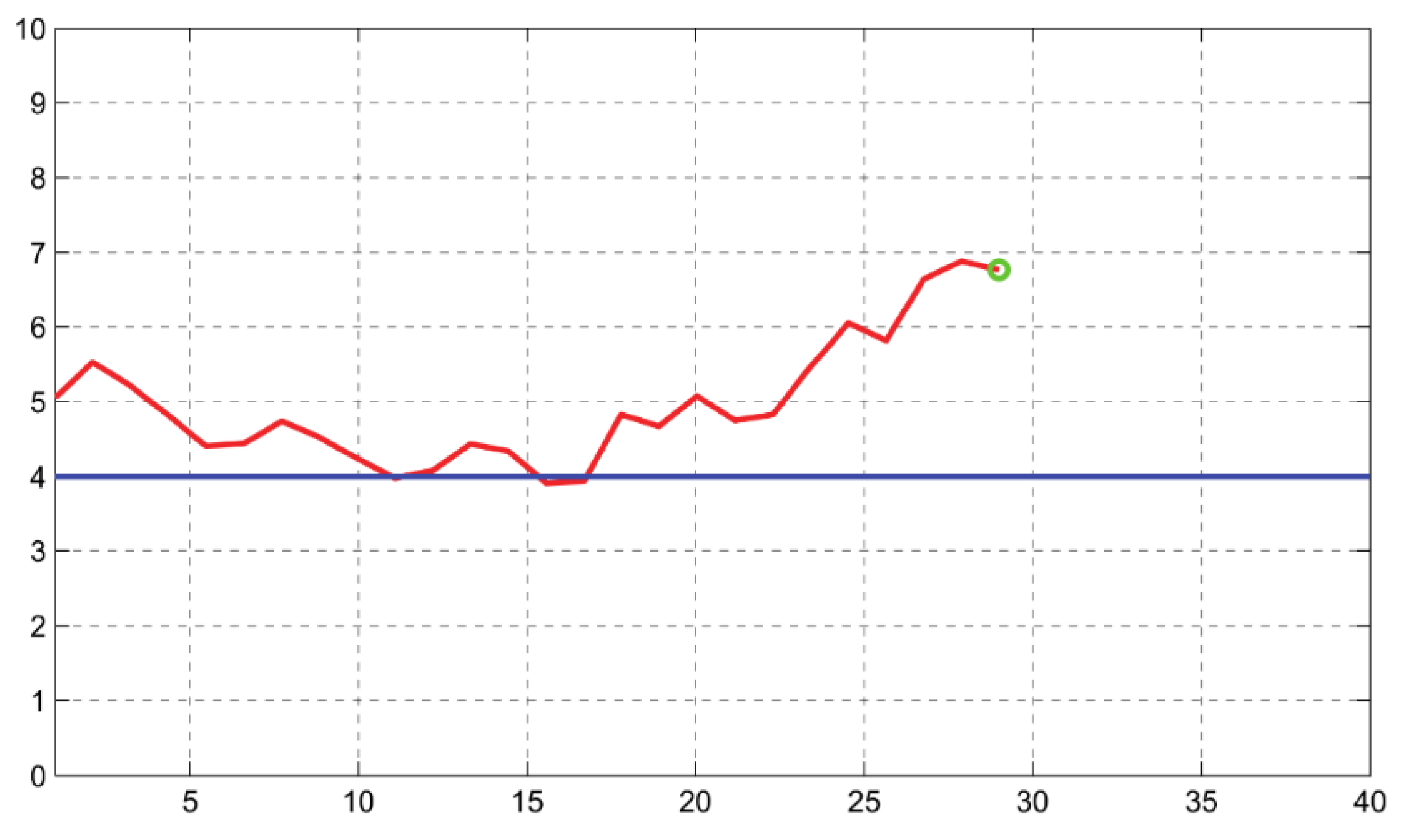
2.1.4. Neurofeedback Application
2.2. System Validation
2.2.1. Participants
2.2.2. Questionnaires
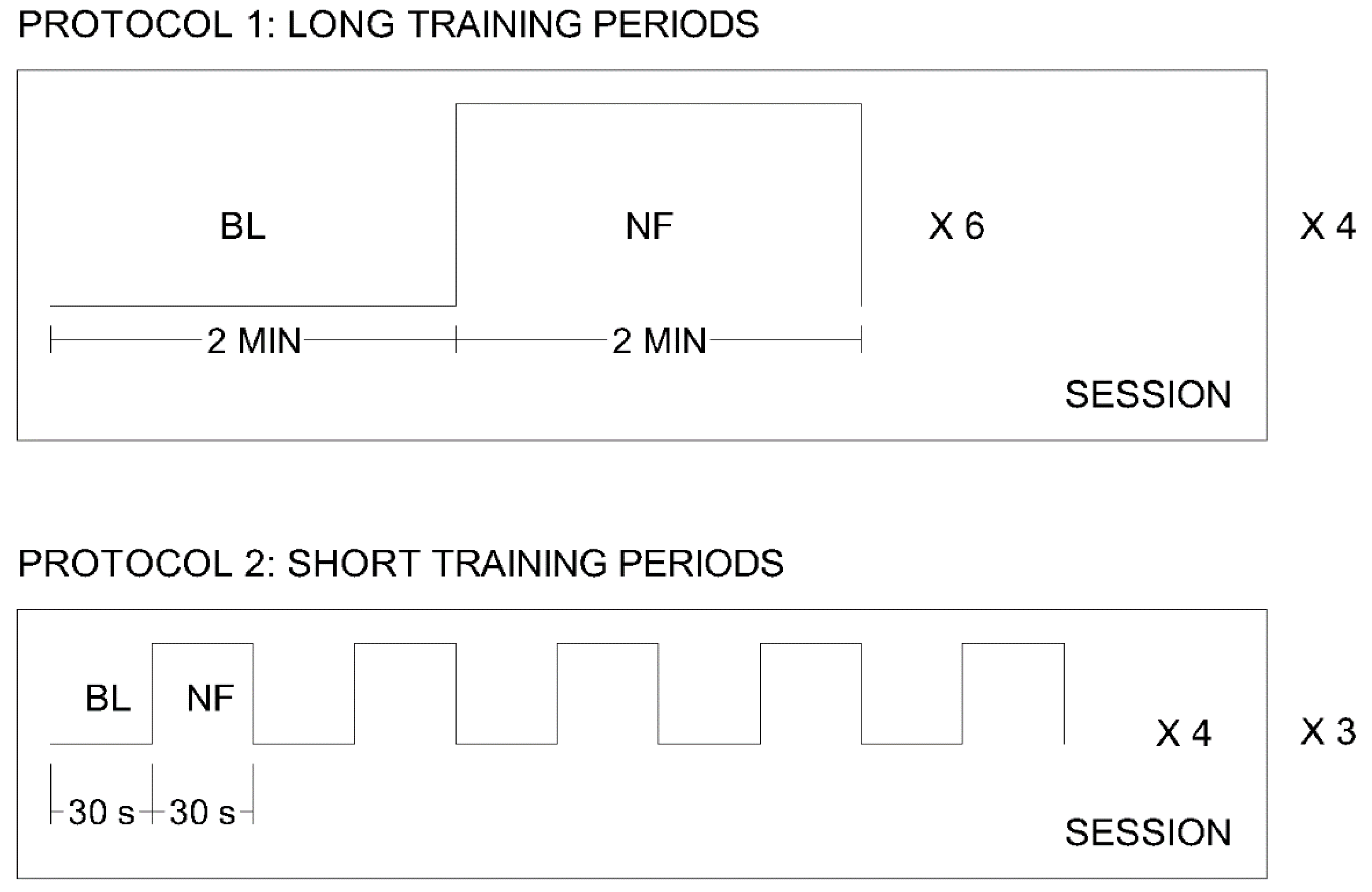
2.2.3. Experimental Design
2.2.4. Success Level
3. Results
3.1. Questionnaire Data
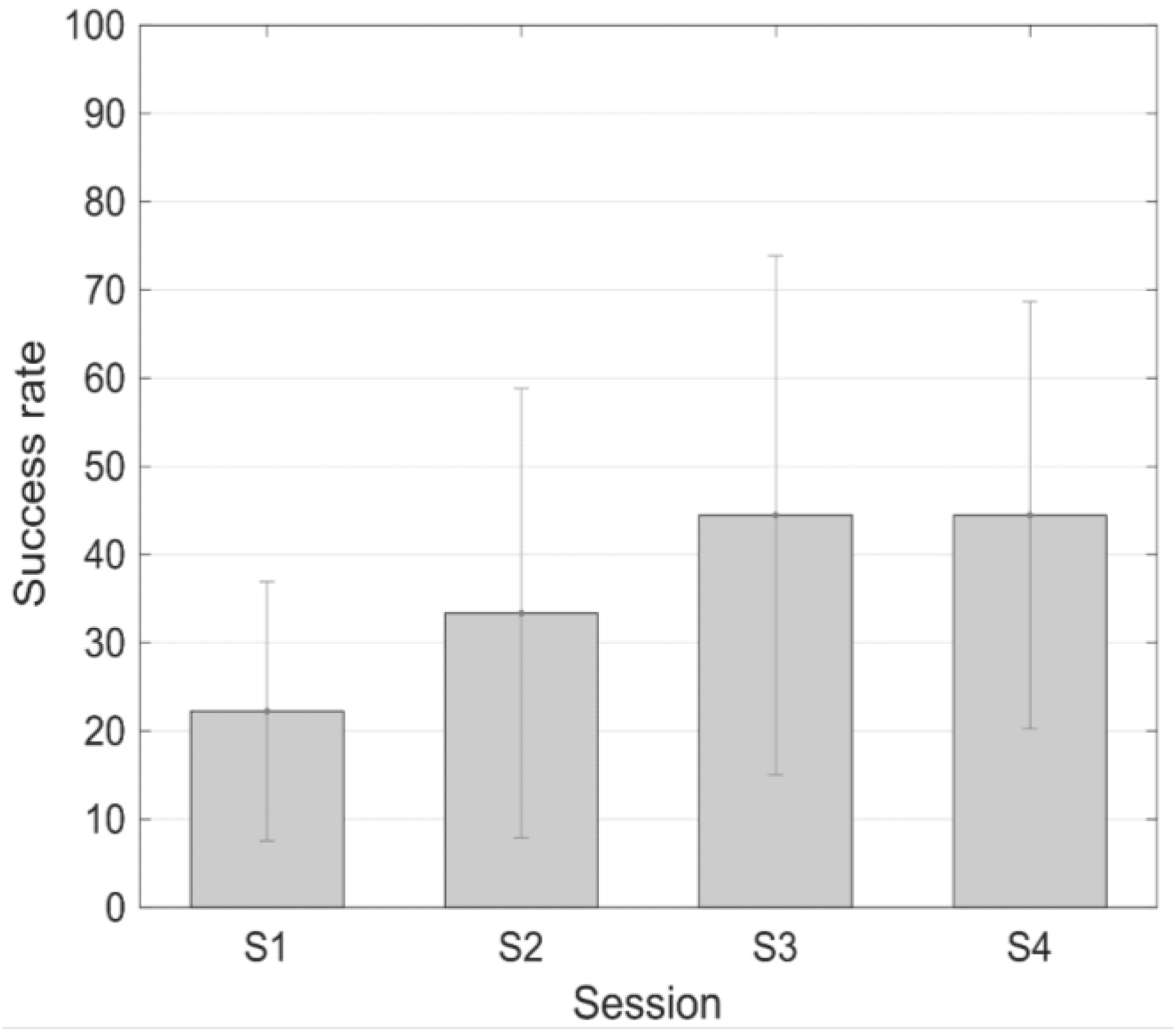
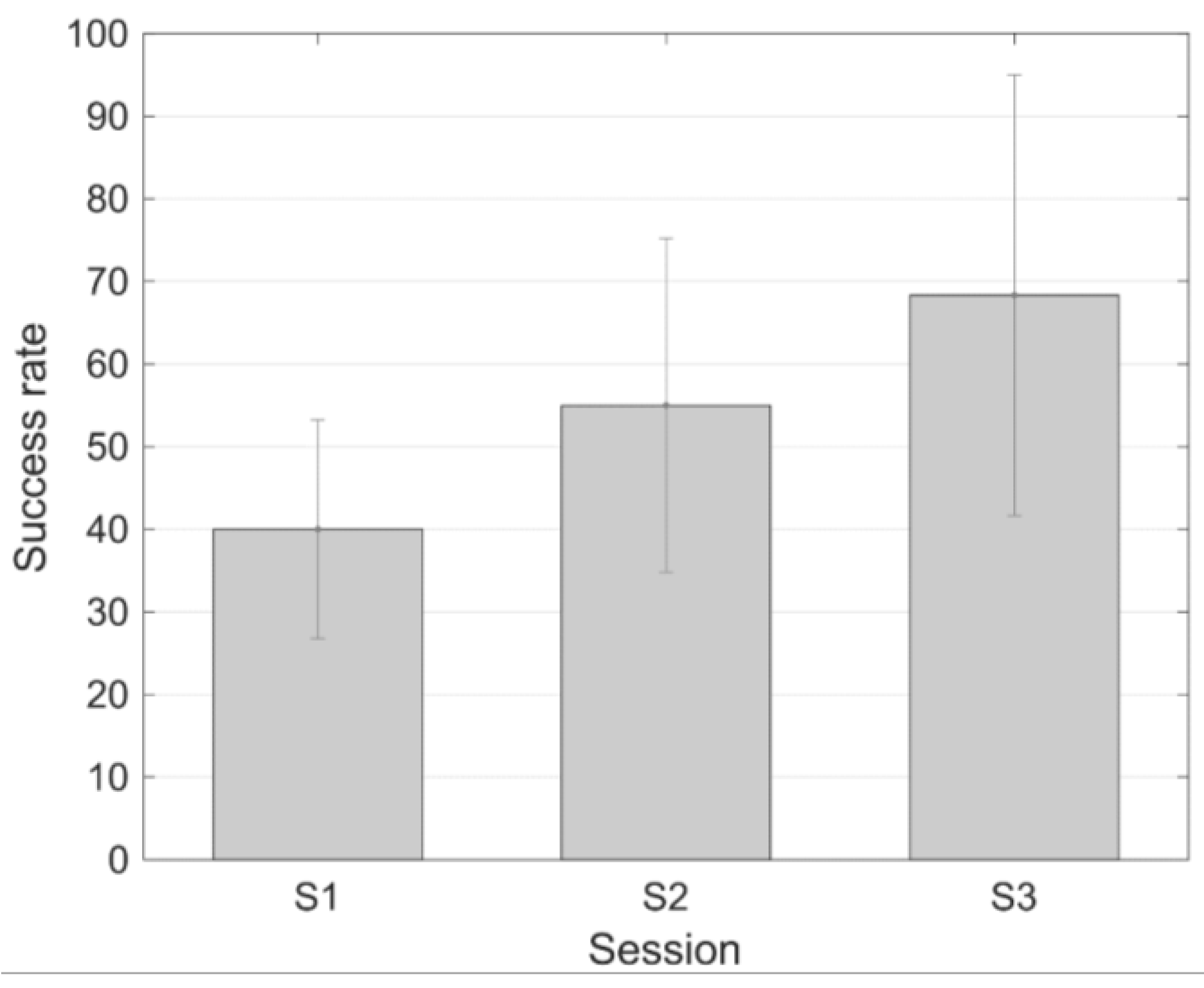
3.2. Success Level
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Birbaumer, N.; Ramos Murguialday, A.; Weber, C.; Montoya, P. Neurofeedback and brain-computer interface clinical applications. Int. Rev. Neurobiol. 2009, 86, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Thibault, R.T.; Lifshitz, M.; Raz, A. The self-regulating brain and neurofeedback: Experimental science and clinical promise. Cortex 2016, 74, 247–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apkarian, A.V.; Bushnell, M.C.; Treede, R.D.; Zubieta, J.K. Human brain mechanisms of pain perception and regulation in health and disease. Eur. J. Pain 2005, 9, 463–484. [Google Scholar] [CrossRef] [PubMed]
- Baliki, M.N.; Geha, P.Y.; Apkarian, A.V.; Chialvo, D.R. Beyond Feeling: Chronic Pain Hurts the Brain, Disrupting the Default-Mode Network Dynamics. J. Neurosci. 2008, 28, 1398–1403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, M.P.; Gertz, K.J.; Kupper, A.E.; Braden, A.L.; Howe, J.D.; Hakimian, S.; Sherlin, L.H. Steps toward developing an EEG biofeedback treatment for chronic pain. Appl. Psychophysiol. Biofeedback 2013, 38, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Emmert, K.; Breimhorst, M.; Bauermann, T.; Birklein, F.; Rebhorn, C.; Van De Ville, D.; Haller, S. Active pain coping is associated with the response in real-time fMRI neurofeedback during pain. Brain Imaging Behav. 2017, 11, 712–721. [Google Scholar] [CrossRef] [PubMed]
- De Charms, R.C.; Maeda, F.; Glover, G.H.; Ludlow, D.; Pauly, J.M.; Soneji, D.; Gabrieli, J.D.E.; Mackey, S.C. Control over brain activation and pain learned by using real-time functional MRI. Proc. Natl. Acad. Sci. USA 2005, 51, 18626–18631. [Google Scholar] [CrossRef] [PubMed]
- Aaslid, R.M.; Markwalder, T.-M.; Nornes, H. Noninvasive transcranial Doppler ultrasound recording of flow velocity in basal cerebral arteries. J. Neurosurg. 1982, 57, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Stroobant, N.; Vingerhoets, G. Transcranial Doppler Ultrasonography Monitoring of Cerebral Hemodynamics during Performance of Cognitive Tasks: A Review. Neuropsychol. Rev. 2000, 10, 213–231. [Google Scholar] [CrossRef] [PubMed]
- Duschek, S.; Schandry, R. Functional transcranial Doppler sonography as a tool in psychophysiological research. Psychophysiology 2003, 40, 436–454. [Google Scholar] [CrossRef] [PubMed]
- Kontos, H.A. Validity of cerebral arterial blood flow calculations from velocity measurements. Stroke 1989, 20, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Duschek, S.; Hellmann, N.; Merzoug, K.; Reyes del Paso, G.A.; Werner, N.S. Cerebral Blood Flow Dynamics during Pain Processing Investigated by Functional Transcranial Doppler Sonography. Pain Med. 2012, 13, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Duschek, S.; Mannhart, T.; Winkelmann, A.; Merzoug, K.; Werner, N.S.; Schuepbach, D.; Montoya, P. Cerebral blood flow dynamics during pain processing in patients with fibromyalgia syndrome. Psychosom. Med. 2012, 74, 802–809. [Google Scholar] [CrossRef] [PubMed]
- Montoro, C.I.; Duschek, S.; de Guevara, C.M.L.; Reyes del Paso, G.A. Patterns of Cerebral Blood Flow Modulation during Painful Stimulation in Fibromyalgia: A Transcranial Doppler Sonography Study. Pain Med. 2016, 17, 2256–2267. [Google Scholar] [CrossRef] [PubMed]
- Angevine, J.B.; Cotman, C.W. Principles of Neuroanatomy, 1st ed.; Oxford University Press: New York, NY, USA, 2008; ISBN 0-19-592885-6. [Google Scholar]
- Rodríguez, A.; Tembl, J.; Mesa-Gresa, P.; Muñoz, M.A.; Montoya, P.; Rey, B. Altered cerebral blood flow velocity features in fibromyalgia patients in resting-state conditions. PLoS ONE 2017, 12, e0180253. [Google Scholar] [CrossRef] [PubMed]
- Duschek, S.; Schuepbach, D.; Doll, A.; Werner, N.S.; Reyes del Paso, G.A.R. Self-regulation of cerebral blood flow by means of transcranial doppler sonography biofeedback. Ann. Behav. Med. 2011, 41, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Schalk, G.; McFarland, D.J.; Hinterberger, T.; Birbaumer, N.; Wolpaw, J.R. BCI2000: A General-Purpose Brain-Computer Interface (BCI) System. IEEE Trans. Biomed. Eng. 2004, 51, 1034–1043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, T.-Y.; Chang, D.-W.; Liu, Y.-D.; Liu, C.-W.; Young, C.-P.; Liang, S.-F.; Shaw, F.-Z. Portable Wireless Neurofeedback System of EEG Alpha Rhythm Enhances Memory. Biomed. Eng. Online 2017, 16, 128. [Google Scholar] [CrossRef] [PubMed]
- Birbaumer, N. Breaking the silence: brain-computer interfaces (BCI) for communication and motor control. Psychophysiology 2006, 43, 517–532. [Google Scholar] [CrossRef] [PubMed]
- Myrden, A.J.B.; Kushki, A.; Sejdic, E.; Guerguerian, A.-M.; Chau, T. A Brain-Computer Interface Based on Bilateral Transcranial Doppler Ultrasound. PLoS ONE 2011, 6, e24170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myrden, A.; Kushki, A.; Sejdic, E.; Chau, T. Towards Increased Data Transmission Rate for a Three-Class Metabolic Brain-Computer Interface based on Transcranial Doppler Ultrasound. Neurosci. Lett. 2012, 528, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Aleem, I.; Chau, T. Towards a Hemodynamic BCI using Transcranial Doppler without User-Specific Training Data. J. Neural Eng. 2013, 10, 016005. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Khondaker, A.M.; Chau, T. Pattern Classification to Optimize the Performance of Transcranial Doppler Ultrasonography-based Brain Machine Interfaces. Pattern Recognit. Lett. 2015, 66, 135–143. [Google Scholar] [CrossRef]
- Faress, A.; Chau, T. Towards a Multimodal Brain-Computer Interface: Combining fNIRS and fTCD Measurements to Enable Higher Classification Accuracy. Neuroimage 2013, 77, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Khalaf, A.; Sybeldon, M.; Sejdic, E.; Akcakaya, M. An EEG and fTCD Based BCI for Control. In Proceedings of the 50th Asilomar Conference on Signals, Systems and Computers, Pacific Grove, CA, USA, 6–9 November 2016; pp. 1285–1289. [Google Scholar] [CrossRef]
- Khalaf, A.; Sybeldon, M.; Sejdic, E.; Akcakaya, M. A Brain-Computer Interface Based on Functional Transcranial Doppler Ultrasound Using Wavelet Transform and Support Vector Machines. J. Neurosci. Methods 2018, 293, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Mamun, K.A.; Chau, T. Online Transcranial Doppler Ultrasonographic Control of an Onscreen Keyboard. Front. Hum. Neurosci. 2014, 8, 199. [Google Scholar] [CrossRef] [PubMed]
- Goyal, A.; Samadani, A.A.; Guerguerian, A.-M.; Chau, T. An Online Three-Class Transcranial Doppler Ultrasound Brain Computer Interface. Neurosci. Res. 2016, 107, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Sulzer, J.; Haller, S.; Scharnowski, F.; Weiskopf, N.; Birbaumer, N.; Blefari, M.L.; Bruehl, A.B.; Cohen, L.G.; deCharms, R.C.; Gassert, R.; et al. Real-time fMRI neurofeedback: Progress and challenges. NeuroImage 2013, 76, 386–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, S.; Shimojo, S.; O’Doherty, J.P. Direct instrumental conditioning of neural activity using functional magnetic resonance imaging-derived reward feedback. J. Neurosci. 2007, 27, 7498–7507. [Google Scholar] [CrossRef] [PubMed]
- Shibata, K.; Watanabe, T.; Sasaki, Y.; Kawato, M. Perceptual learning incepted by decoded fMRI neurofeedback without stimulus presentation. Science 2011, 334, 1413–1415. [Google Scholar] [CrossRef] [PubMed]
- Weiskopf, N.; Veit, R.; Erb, M.; Mathiak, K.; Grodd, W.; Goebel, R.; Birbaumer, N. Physiological self-regulation of regional brain activity using real-time functional magnetic resonance imaging (fMRI): methodology and exemplary data. NeuroImage 2003, 19, 577–586. [Google Scholar] [CrossRef]
- Aboy, M.; Hornero, R.; Abásolo, D.; Álvarez, D. Interpretation of the Lempel-Ziv complexity measure in the context of biomedical signal analysis. Title of the article. IEEE Trans. Biomed. 2006, 53, 2282–2288. [Google Scholar] [CrossRef] [PubMed]
- Abásolo, D.; Hornero, R.; Gómez, C.; García, M.; López, M. Analysis of EEG background activity in Alzheimer’s disease patients with Lempel–Ziv complexity and central tendency measure. Med. Eng. Phys. 2006, 28, 315–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, T.B.; Chern, C.M.; Sheng, W.Y.; Wong, W.J.; Hu, H.H. Frequency domain analysis of cerebral blood flow velocity and its correlation with arterial blood pressure. J. Cereb. Blood Flow Metab. 1998, 18, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Oldfield, R.C. The assessment and analysis of handedness: The Edinburgh inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef]
- Bryden, M.P. Measuring handedness with questionnaires. Neuropsychologia 1977, 15, 617–624. [Google Scholar] [CrossRef]
- Spielberger, R.E.; Gorsuch, C.D.; Lushene, R.L. Manual for the State-Trait Inventory, 1st ed.; Consulting Psychologists: Palo Alto, CA, USA, 1970. [Google Scholar]
- Caria, A.; Sitaram, R.; Veit, R.; Begliomini, C.; Birbaumer, N. Volitional control of anterior insula activity modulates the response to aversive stimuli. A real-time functional magnetic resonance imaging study. Biol. Psychiatry 2010, 68, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Koralek, A.C.; Jin, X.; Long, J.D.; Costa, R.M.; Carmena, J.M. Corticostriatal plasticity is necessary for learning intentional neuroprosthetic skills. Nature 2012, 483, 331–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston, S.J.; Boehm, S.G.; Healy, D.; Goebel, R.; Linden, D.E.J. Neurofeedback: A promising tool for the self-regulation of emotion networks. Neuroimage 2010, 49, 1066–1072. [Google Scholar] [CrossRef] [PubMed]
- Gruzelier, J.H. EEG-neurofeedback for optimizing performance. III: A review of methodological and theoretical considerations. Neurosci. Biobehav. Rev. 2014, 44, 159–182. [Google Scholar] [CrossRef] [PubMed]
- Huster, R.J.; Mokom, Z.N.; Enriquez-Geppert, S.; Herrmann, C.S. Brain-computer interfaces for EEG neurofeedback: Peculiarities and solutions. Int. J. Psychol. 2014, 91, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Allison, B.; Neuper, C. Could Anyone Use a BCI? In Brain Computer Interfaces, 1st ed.; Tan, D.S., Nijholt, A., Eds.; Springer: London, UK, 2010; pp. 34–54. ISBN 978-1-84996-271-1. [Google Scholar]
- Arns, M.; Heinrich, H.; Strehl, U. Evaluation of neurofeedback in ADHD: The long and winding road. Biol. Psychol. 2014, 95, 108–115. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Protocol | STAI-Trait | STAI-State PRE | STAI-State POST |
|---|---|---|---|
| Long training periods | 8.33 ± 14 | 13.67 ± 11.23 | 11 ± 2 |
| Short training periods | 14 ± 1.73 | 17.33 ± 8.14 | 17 ± 8.88 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rey, B.; Rodríguez, A.; Lloréns-Bufort, E.; Tembl, J.; Muñoz, M.Á.; Montoya, P.; Herrero-Bosch, V.; Monzo, J.M. Design and Validation of an FPGA-Based Configurable Transcranial Doppler Neurofeedback System for Chronic Pain Patients. Sensors 2018, 18, 2278. https://0-doi-org.brum.beds.ac.uk/10.3390/s18072278
Rey B, Rodríguez A, Lloréns-Bufort E, Tembl J, Muñoz MÁ, Montoya P, Herrero-Bosch V, Monzo JM. Design and Validation of an FPGA-Based Configurable Transcranial Doppler Neurofeedback System for Chronic Pain Patients. Sensors. 2018; 18(7):2278. https://0-doi-org.brum.beds.ac.uk/10.3390/s18072278
Chicago/Turabian StyleRey, Beatriz, Alejandro Rodríguez, Enrique Lloréns-Bufort, José Tembl, Miguel Ángel Muñoz, Pedro Montoya, Vicente Herrero-Bosch, and Jose M. Monzo. 2018. "Design and Validation of an FPGA-Based Configurable Transcranial Doppler Neurofeedback System for Chronic Pain Patients" Sensors 18, no. 7: 2278. https://0-doi-org.brum.beds.ac.uk/10.3390/s18072278