A Piezoresistive Sensor to Measure Muscle Contraction and Mechanomyography

 ,
,  ,
,  , , ,
, , , 
Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
- Strain gauges [19]: muscle contractions which cause direct stretching of the sensor;
- Change of electrical impedance of the muscles [20]: changes to global muscle resistivity when it goes from a resting state to an activity state, due to blood afflux in the muscles;
- A resonance-based active-muscle stiffness sensor [23]: where piezoelectric probes are used to measure stiffness changes in muscles;
- A small permanent magnet fixed on the skin, in conjunction with a Hall effect device, used to measure changes in muscle dimension [25];
- Pneumatic sensors [26]: muscular activity detected by measuring changes in air pressure in an air-bladder contacting the muscle;
- Change in optical properties [27]: LEDs and photodiodes can be combined to detect muscle contraction by measuring the backscattered light from the muscle tissue;
- Textile pressure sensors enclosed in garments [28].
2. Materials and Methods
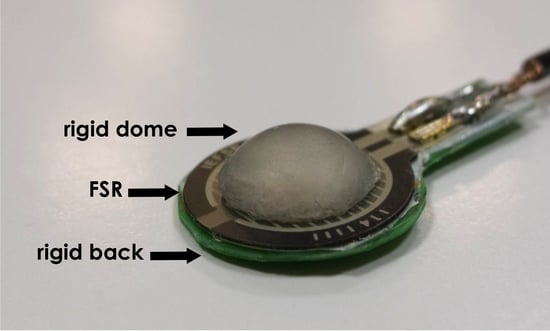
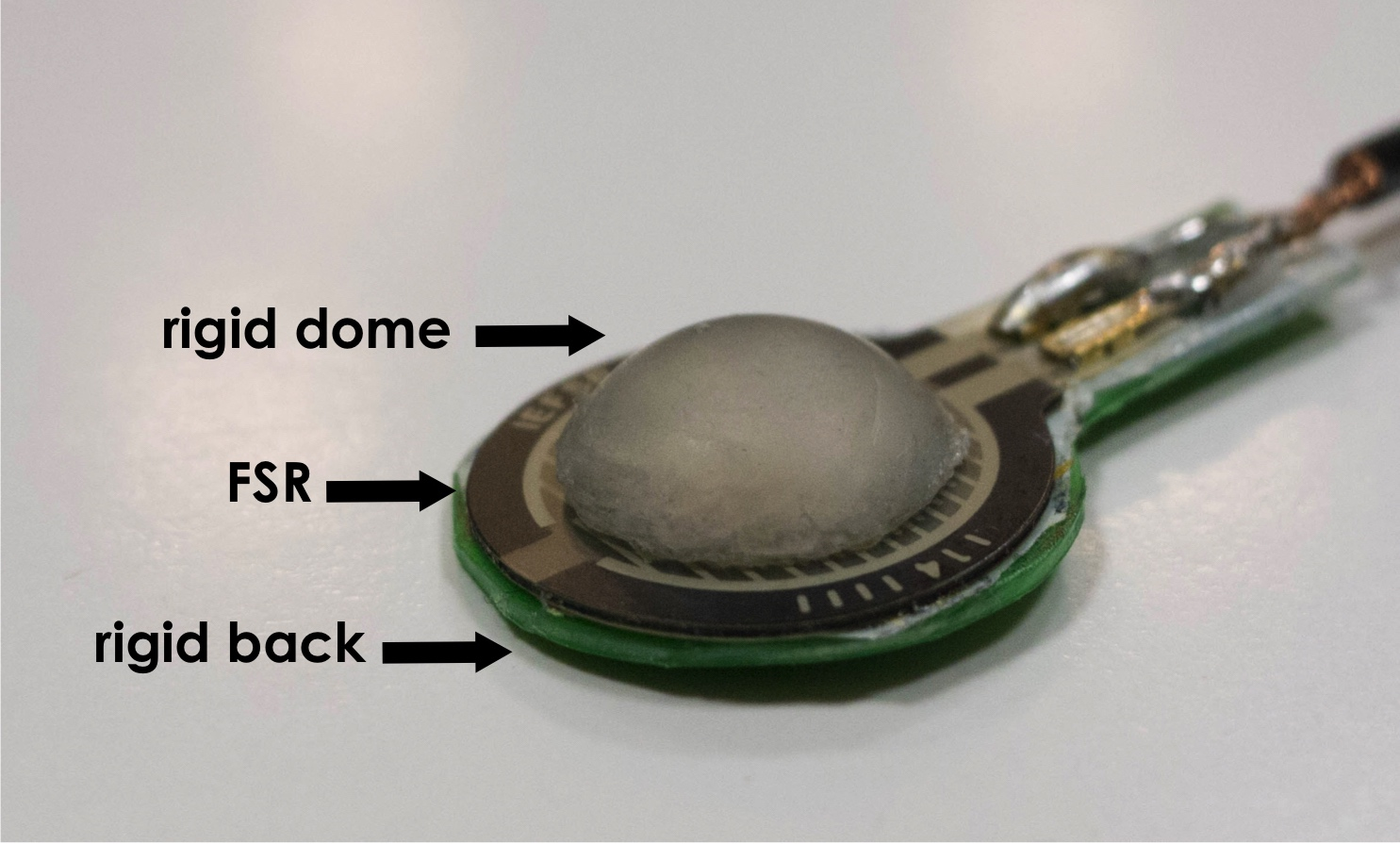
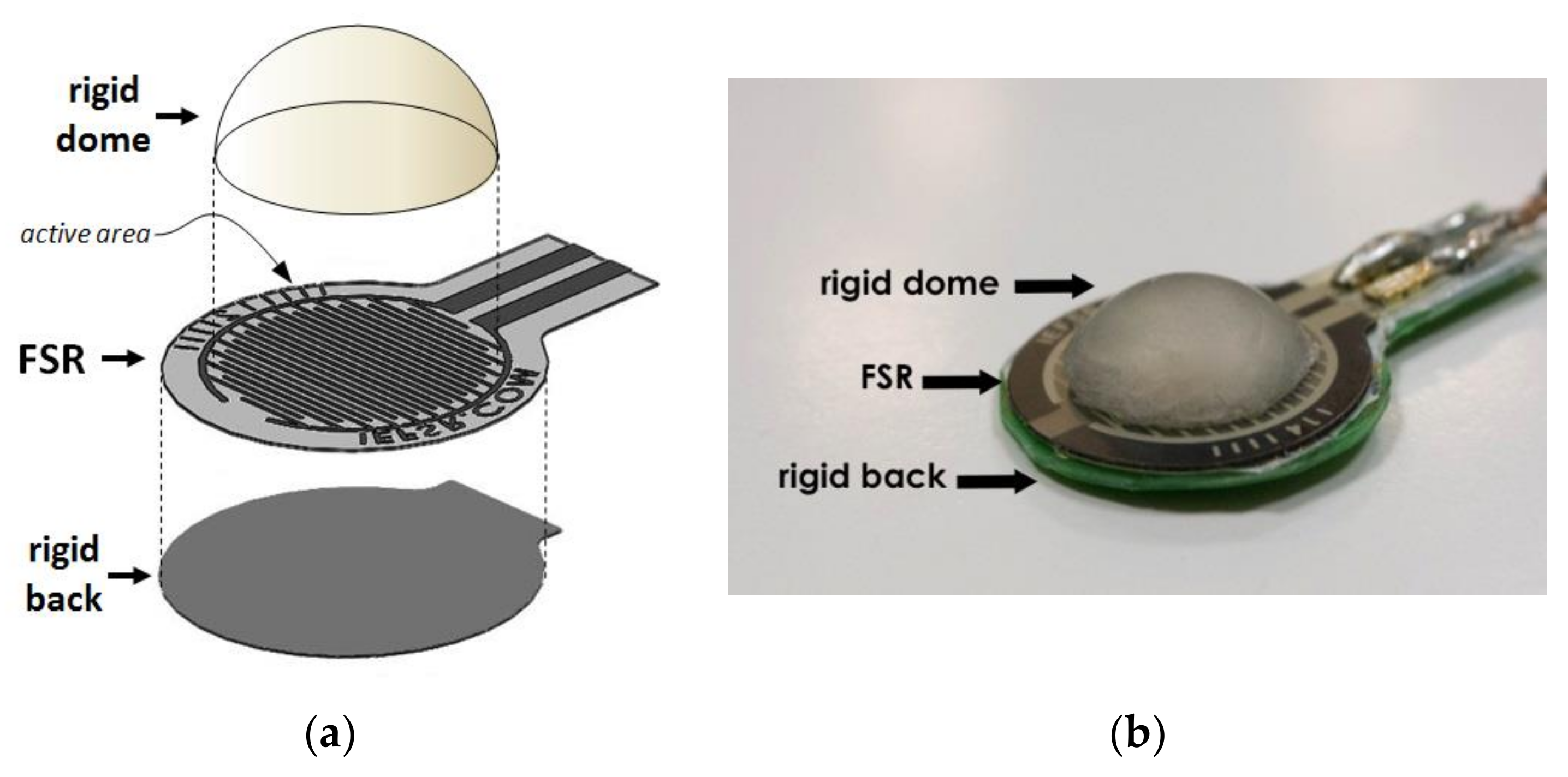
2.1. Sensor Design
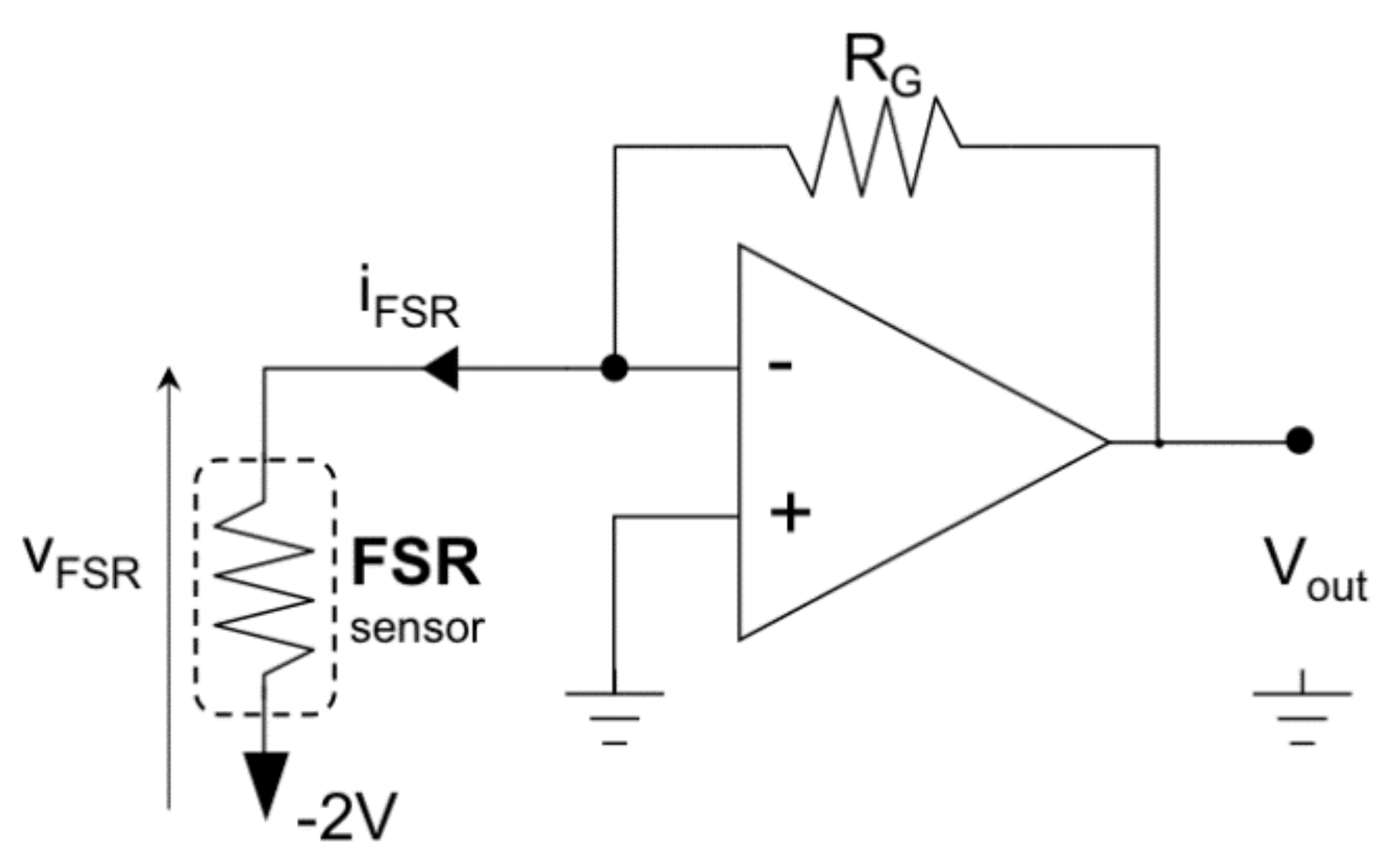
2.2. Sensor Conditioning
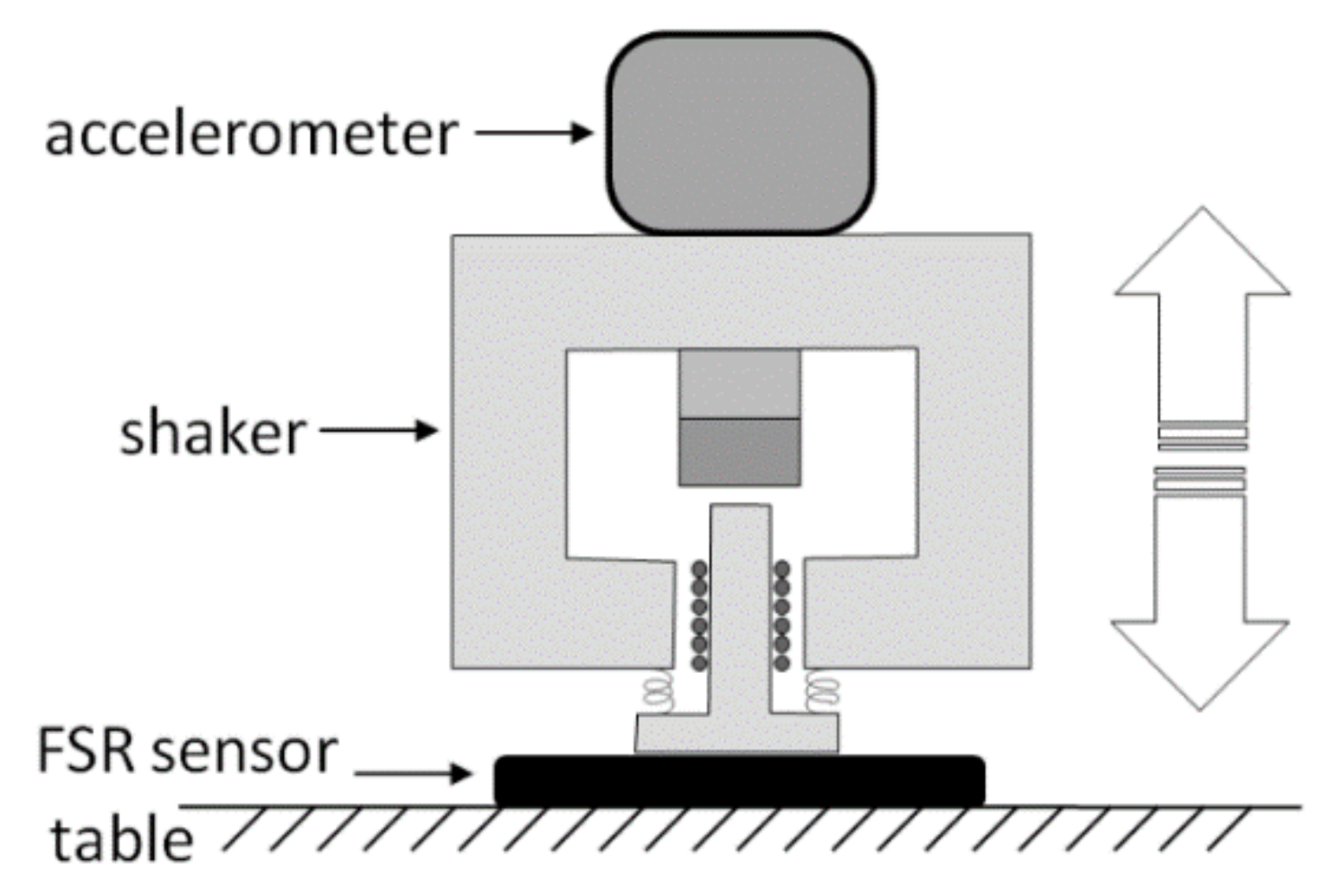
2.3. FSR Static and Dynamic Test
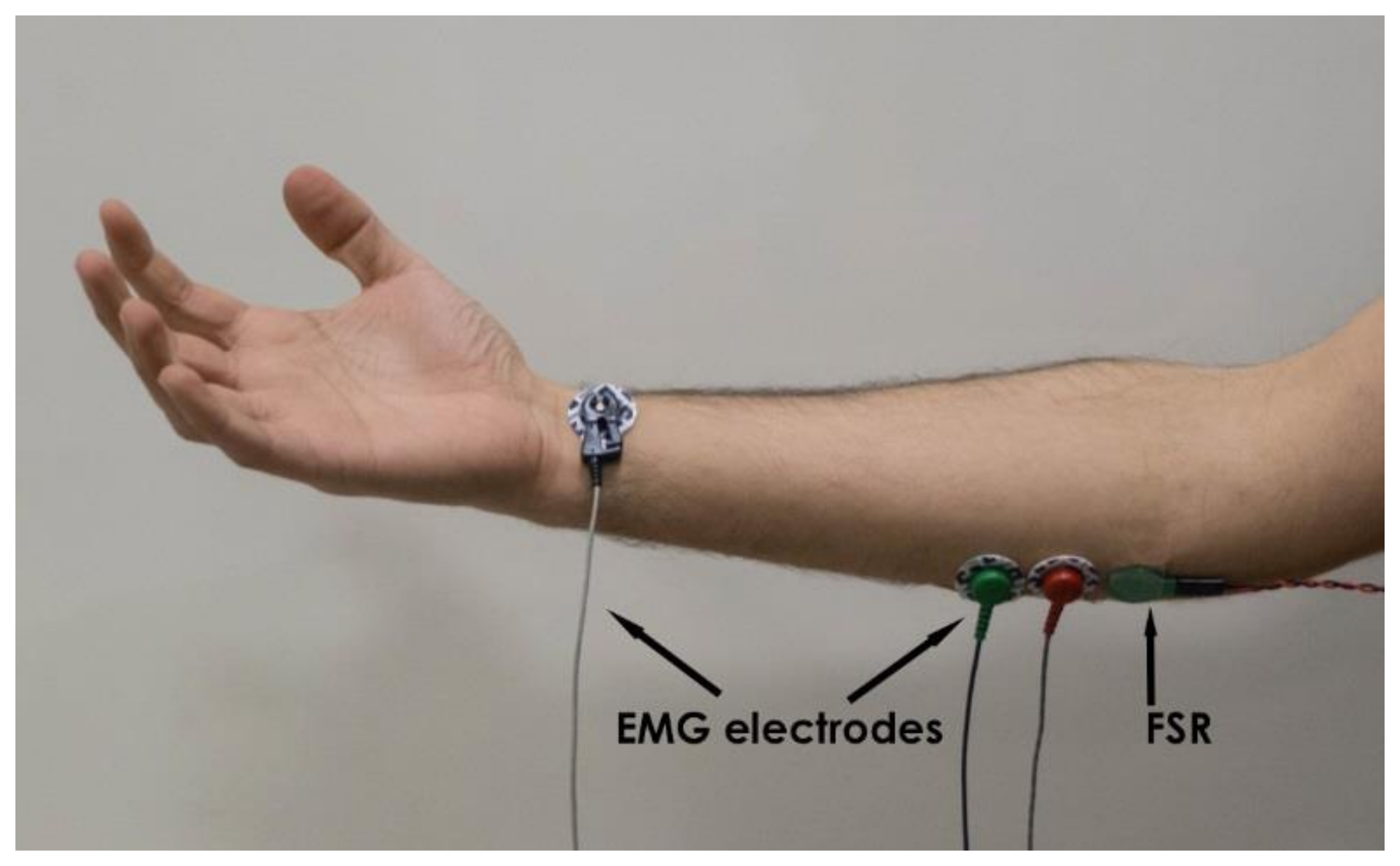
2.4. Comparison with the EMG Signal and Hand Prosthesis Control
3. Results
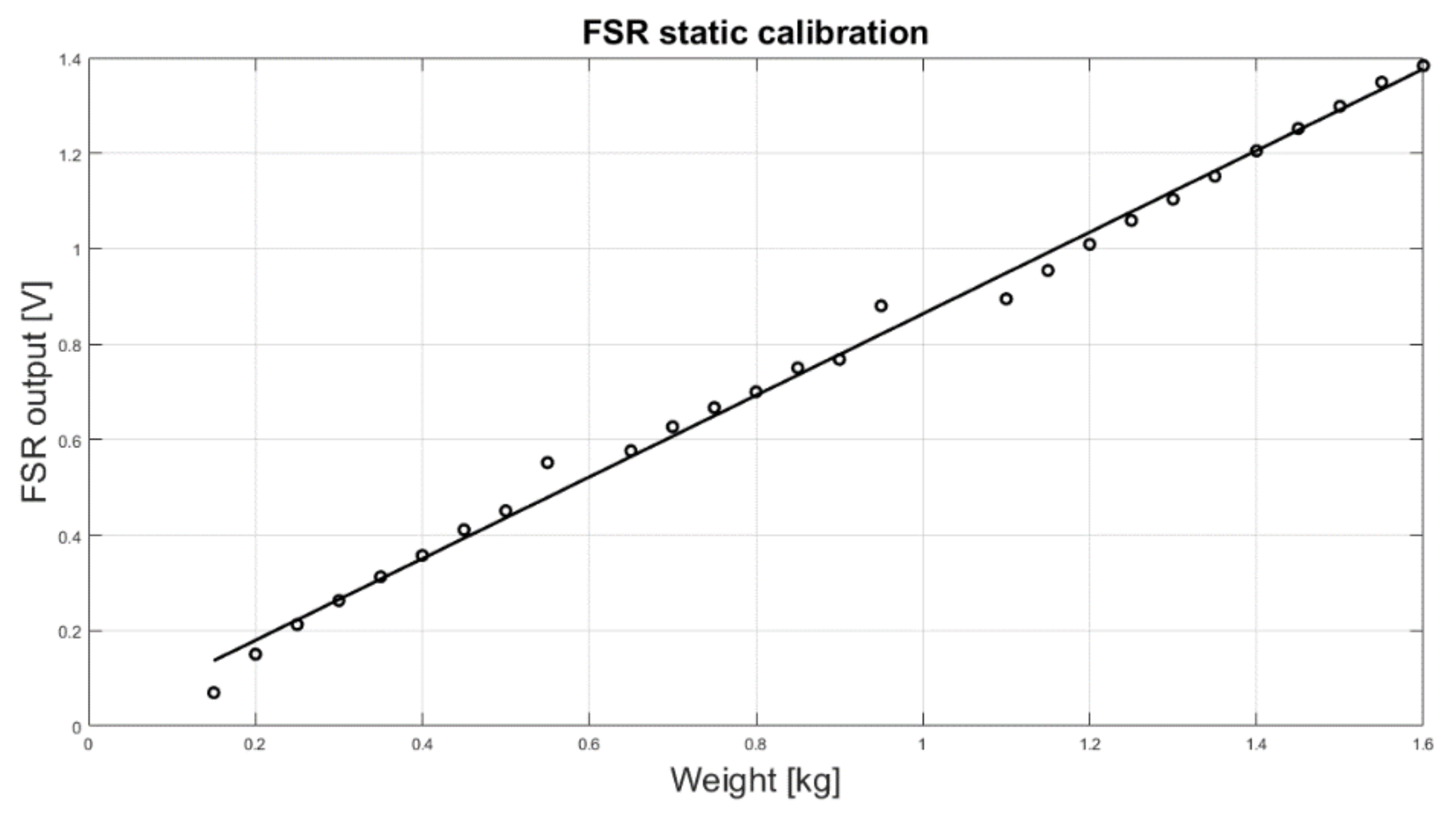
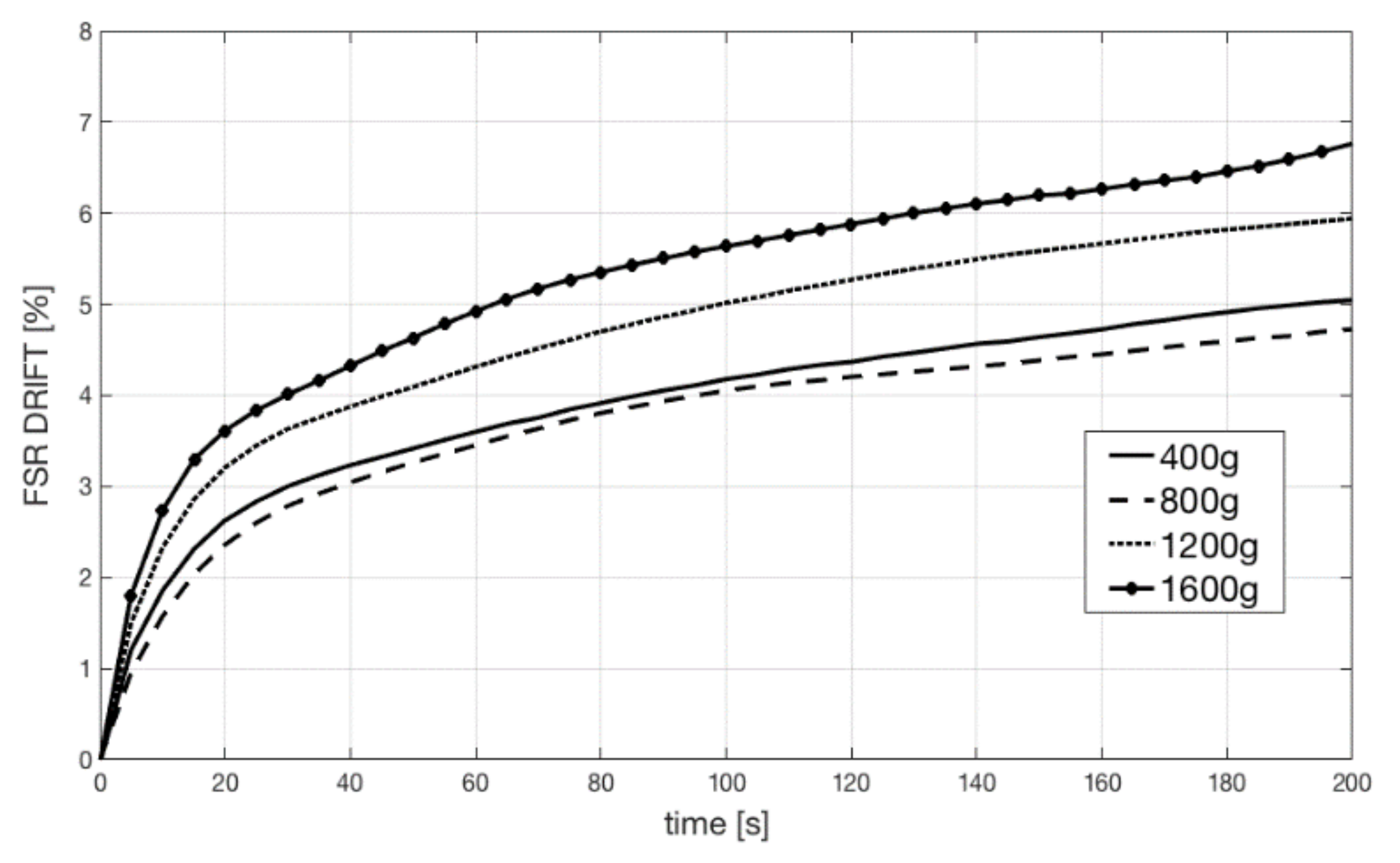
3.1. Static and Dynamic Test Results
3.2. EMG–FSR Comparison Results
4. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Statements
References
- Basmajian, J.V.; De Luca, C.J. Muscles Alive: Their Functions Revealed by Electromyography, 5th ed.; Williams & Wilkins: Baltimore, MD, USA, 1985; ISBN 068300414X. [Google Scholar]
- Spires, M.C.; Kelly, B.M.; Davis, A.J. Prosthetic Restoration and Rehabilitation of the Upper and Lower Extremity; Demos Medical Publishing: New York, NY, USA, 2013; ISBN 978-1-936287-66-6. [Google Scholar]
- Lobo-Prat, J.; Kooren, P.N.; Stienen, A.H.; Herder, J.L.; Koopman, B.F.; Veltink, P.H. Non-invasive control interfaces for intention detection in active movement-assistive devices. J. Neuroeng. Rehabil. 2014, 11, 168. [Google Scholar] [CrossRef] [PubMed]
- Gargiulo, G.D.; Bifulco, P.; Cesarelli, M.; Jin, C.; McEwan, A.; van Schaik, A. Wearable dry sensors with Bluetooth connection for use in remote patient monitoring systems. Stud. Health Technol. Inform. 2010, 161, 57–65. [Google Scholar] [PubMed]
- Amrutha, N.; Arul, V.H. A Review on Noises in EMG Signal and its Removal. Int. J. Sci. Res. Publ. 2017, 7, 23–27. [Google Scholar]
- Nazmi, N.; Abdul Rahman, M.A.; Yamamoto, S.; Ahmad, S.A.; Zamzuri, H.; Mazlan, S.A. A Review of Classification Techniques of EMG Signals during Isotonic and Isometric Contractions. Sensors 2016, 16, 1304. [Google Scholar] [CrossRef] [PubMed]
- Ibitoye, M.O.; Hamzaid, N.A.; Zuniga, J.M.; Abdul Wahab, A.K. Mechanomyography and muscle function assessment: A review of current state and prospects. Clin. Biomech. 2014, 29, 691–704. [Google Scholar] [CrossRef] [PubMed]
- Beck, T.W.; Housh, T.J.; Cramer, J.T.; Weir, J.P.; Johnson, G.O.; Coburn, J.W.; Malek, M.H.; Mielke, M. Mechanomyographic amplitude and frequency responses during dynamic muscle actions: A comprehensive review. Biomed. Eng. Online 2005, 4, 67. [Google Scholar] [CrossRef] [PubMed]
- Deffieux, T.; Gennisson, J.L.; Tanter, M.; Fink, M. Ultrafast imaging of in vivo muscle contraction using ultrasound. Appl. Phys. Lett. 2006, 89, 184107. [Google Scholar] [CrossRef]
- Barry, D.T.; Leonard, J.A.J.; Gitter, A.J.; Ball, R.D. Acoustic myography as a control signal for an externally powered prosthesis. Arch. Phys. Med. Rehabil. 1986, 67, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Posatskiy, A.O.; Chau, T. The effects of motion artifact on mechanomyography: A comparative study of microphones and accelerometers. J. Electromyogr. Kinesiol. 2012, 22, 320–324. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.; Heim, W.; Chau, T. A self-contained, mechanomyography-driven externally powered prosthesis. Arch. Phys. Med. Rehabil. 2005, 86, 2066–2070. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.; Chau, T. Coupled microphone-accelerometer sensor pair for dynamic noise reduction in MMG signal recording. Electron. Lett. 2003, 39, 1496–1498. [Google Scholar] [CrossRef]
- Antonelli, M.G.; Beomonte Zobel, P.; Giacomin, J. Use of MMG signals for the control of powered orthotic devices: Development of a rectus femoris measurement protocol. Assist. Technol. 2009, 21, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Plewa, K.; Samadani, A.; Chau, T. Comparing electro- and mechano-myographic muscle activation patterns in self-paced pediatric gait. J. Electromyogr. Kinesiol. 2017, 36, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Dahmane, R.; Valenčič, V.; Knez, N.; Eržen, I. Evaluation of the ability to make non-invasive estimation of muscle contractile properties on the basis of the muscle belly response. Med. Biol. Eng. Comput. 2001, 39, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Rusu, L.D.; Cosma, G.G.; Cernaianu, S.M.; Marin, M.N.; Rusu, P.F.; Ciocănescu, D.P.; Neferu, F.N. Tensiomyography method used for neuromuscular assessment of muscle training. J. Neuroeng. Rehabil. 2013, 10, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ditroilo, M.; Smith, I.J.; Fairweather, M.M.; Hunter, A.M. Long-term stability of tensiomyography measured under different muscle conditions. J. Electromyogr. Kinesiol. 2013, 23, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Đorđevicć, S.; Stančin, S.; Meglič, A.; Milutinović, V.; Tomažič, S. MC Sensor—A Novel Method for Measurement of Muscle Tension. Sensors 2011, 11, 9411–9425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, O.L.; Sousa, T.H.S.; Hoffman, I.O.; de Camargo, E.D.L.B.; de Moura, F.S.; Martins, A.R.C.; Biasi, C.; Fantoni, D.T.; Lima, R.G. A proposal to monitor muscle contraction through the change of electrical impedance inside a muscle. In Proceedings of the 5th IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (BioRob), São Paulo, Brazil, 12–15 August 2014. [Google Scholar]
- Bifulco, P.; Esposito, D.; Gargiulo, G.D.; Savino, S.; Niola, V.; Iuppariello, L.; Cesarelli, M. A stretchable, conductive rubber sensor to detect muscle contraction for prosthetic hand control. In Proceedings of the IEEE E-Health and Bioengineering Conference (EHB), Sinaia, Romania, 22–24 June 2017. [Google Scholar] [CrossRef]
- Kim, W.S.; Lee, H.D.; Lim, D.H.; Han, J.S.; Shin, K.S.; Han, C.S. Development of a muscle circumference sensor to estimate torque of the human elbow joint. Sens. Actuators A 2014, 208, 95–103. [Google Scholar] [CrossRef]
- Han, H.; Kim, J. Active muscle stiffness sensor based on piezoelectric resonance for muscle contraction estimation. Sens. Actuators A 2013, 194, 212–219. [Google Scholar] [CrossRef]
- Guo, J.Y.; Zheng, Y.P.; Xie, H.B.; Chen, X. Continuous monitoring of electromyography (EMG), mechanomyography (MMG), sonomyography (SMG) and torque output during ramp and step isometric contractions. Med. Eng. Phys. 2010, 32, 1032–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenney, L.P.; Lisitsa, I.; Bowker, P.; Heath, G.H.; Howard, D. Dimensional change in muscle as a control signal for powered upper limb prostheses: A pilot study. Med. Eng. Phys. 1999, 21, 589–597. [Google Scholar] [CrossRef]
- Jung, P.G.; Lim, G.; Kim, S.; Kong, K. A Wearable Gesture Recognition Device for Detecting Muscular Activities Based on Air-Pressure Sensors. IEEE Trans. Ind. Inform. 2015, 11, 485–494. [Google Scholar] [CrossRef]
- Bansal, A.K.; Hou, S.; Kulyk, O.; Bowman, E.M.; Samuel, I.D.W. Wearable Organic Optoelectronic Sensors for Medicine. Adv. Mater. 2015, 27, 1521–4095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, B.; Sundholm, M.; Cheng, J.; Cruz, H.; Lukowicz, P. Measuring muscle activities during gym exercises with textile pressure mapping sensors. Pervasive Mob. Comput. 2017, 38 Pt 2, 331–345. [Google Scholar] [CrossRef]
- Amft, O.; Junker, H.; Lukowicz, P.; Tröster, G.; Schuster, C. Sensing muscle activities with body-worn sensors. In Proceedings of the International Workshop on Wearable and Implantable Body Sensor Networks (BSN’06), Cambridge, MA, USA, 3–5 April 2006. [Google Scholar] [CrossRef]
- Lukowicz, P.; Hanser, F.; Szubski, C.; Schobersberger, W. Detecting and Interpreting Muscle Activity with Wearable Force Sensors. In Pervasive Computing, Proceedings of the International Conference on Pervasive Computing, Dublin, Ireland, 7–10 May 2006; Springer: Berlin/Heidelberg, Germany, 2006; Volume 3968, pp. 101–116. [Google Scholar] [CrossRef]
- Paredes-Madrid, L.; Matute, A.; Bareño, J.O.; Parra Vargas, C.A.; Gutierrez Velásquez, E.I. Underlying Physics of Conductive Polymer Composites and Force Sensing Resistors (FSRs). A Study on Creep Response and Dynamic Loading. Materials 2017, 10, 1334. [Google Scholar] [CrossRef] [PubMed]
- Cavanagh, P.R.; Komi, P.V. Electromechanical delay in human skeletal muscle under concentric and eccentric contractions. Eur. J. Appl. Physiol. Occup. Physiol. 1979, 42, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Viitasalo, J.T.; Komi, P.V. Interrelationships between electromyographic, mechanical, muscle structure and reflex time measurements in man. Acta Physiol. Scand. 1981, 111, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Ferris-Hood, K.; Threlkeld, A.J.; Horn, T.S.; Shapiro, R. Relaxation electromechanical delay of the quadriceps during selected movement velocities. Electromyogr. Clin. Neurophysiol. 1996, 36, 157–170. [Google Scholar] [PubMed]
- Esposito, F.; Limonta, E.; Cè, E. Passive stretching effects on electromechanical delay and time course of recovery in human skeletal muscle: New insights from an electromyographic and mechanomyographic combined approach. Eur. J. Appl. Physiol. 2011, 111, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, K.; Sasaki, T.; Ishii, N. Acceleration and force reveal different mechanisms of electromechanical delay. Med. Sci. Sports Exerc. 2011, 43, 1200–1206. [Google Scholar] [CrossRef] [PubMed]
- Esposito, F.; Cè, E.; Rampichini, S.; Limonta, E.; Venturelli, M.; Monti, E.; Bet, L.; Fossati, B.; Meola, G. Electromechanical delay components during skeletal muscle contraction and relaxation in patients with myotonic dystrophy type 1. Neuromuscul. Disord. 2016, 26, 60–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Interlink Electronics. FSR400 Series Datasheet. Available online: https://www.interlinkelectronics.com/request-data-sheets (accessed on 26 February 2018).
- Lebosse, C.; Renaud, P.; Bayle, B.; de Mathelin, M. Modeling and Evaluation of Low-Cost Force Sensors. IEEE Trans. Robot. 2011, 27, 815–822. [Google Scholar] [CrossRef]
- Tiwana, M.; Redmond, S.; Lovell, N. A review of tactile sensing technologies with applications in biomedical engineering. Sens. Actuators A Phys. 2012, 179, 17–31. [Google Scholar] [CrossRef]
- Paredes-Madrid, L.; Palacio, C.; Matute, A.; Parra Vargas, C. Underlying Physics of Conductive Polymer Composites and Force Sensing Resistors (FSRs) under Static Loading Conditions. Sensors 2017, 17, 2108. [Google Scholar] [CrossRef] [PubMed]
- Stassi, S.; Cauda, V.; Canavese, G.; Pirri, C. Flexible Tactile Sensing Based on Piezoresistive Composites: A Review. Sensors 2014, 14, 5296–5332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benatti, S.; Milosevic, B.; Farella, E.; Gruppioni, E.; Benini, L. A Prosthetic Hand Body Area Controller Based on Efficient Pattern Recognition Control Strategies. Sensors 2017, 17, 869. [Google Scholar] [CrossRef] [PubMed]
- Rossi, C.; Savino, S. An underactuated multi-finger grasping device. Int. J. Adv. Robot. Syst. 2014, 11, 20. [Google Scholar] [CrossRef]
- Savino, S. Underactuated Mechanical Hand Control by EMG Sensors. Int. J. Mech. Control 2016, 17, 67–75. [Google Scholar]
- Xie, H.B.; Zheng, Y.P.; Guo, J.Y. Classification of the mechanomyogram signal using a wavelet packet transform and singular value decomposition for multifunction prosthesis control. Physiol. Meas. 2009, 30, 441–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, T.W.; Housh, T.J.; Johnson, G.O.; Weir, J.P.; Cramer, J.T.; Coburn, J.W.; Malek, M.H. Mechanomyographic and electromyographic time and frequency domain responses during submaximal to maximal isokinetic muscle actions of the biceps brachii. Eur. J. Appl. Physiol. 2004, 92, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Gargiulo, G.D.; McEwan, A.L.; Bifulco, P.; Cesarelli, M.; Jin, C.; Tapson, J.; Thiagalingam, A.; van Schaik, A. Towards true unipolar bio-potential recording: A preliminary result for ECG. Physiol. Meas. 2013, 34. [Google Scholar] [CrossRef] [PubMed]
- Cesarelli, M.; Fratini, A.; Bifulco, P.; La Gatta, A.; Romano, M.; Pasquariello, G. Analysis and modelling of muscles motion during whole body vibration. EURASIP J. Adv. Signal Process. 2010, 30, S67–S68. [Google Scholar] [CrossRef]
- Cesarelli, M.; Bifulco, P.; Bracale, M. Quadriceps muscles activation in anterior knee pain during isokinetic exercise. Med. Eng. Phys. 1999, 21, 469–478. [Google Scholar] [CrossRef]








© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esposito, D.; Andreozzi, E.; Fratini, A.; Gargiulo, G.D.; Savino, S.; Niola, V.; Bifulco, P. A Piezoresistive Sensor to Measure Muscle Contraction and Mechanomyography. Sensors 2018, 18, 2553. https://0-doi-org.brum.beds.ac.uk/10.3390/s18082553
Esposito D, Andreozzi E, Fratini A, Gargiulo GD, Savino S, Niola V, Bifulco P. A Piezoresistive Sensor to Measure Muscle Contraction and Mechanomyography. Sensors. 2018; 18(8):2553. https://0-doi-org.brum.beds.ac.uk/10.3390/s18082553
Chicago/Turabian StyleEsposito, Daniele, Emilio Andreozzi, Antonio Fratini, Gaetano D Gargiulo, Sergio Savino, Vincenzo Niola, and Paolo Bifulco. 2018. "A Piezoresistive Sensor to Measure Muscle Contraction and Mechanomyography" Sensors 18, no. 8: 2553. https://0-doi-org.brum.beds.ac.uk/10.3390/s18082553