Verification of a Portable Motion Tracking System for Remote Management of Physical Rehabilitation of the Knee

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. IMU Motion Tracking Sensor Description and Calibration Procedure
2.2. Video-Based Motion Tracking System Description and Calibration Procedure
2.3. Measurement of Knee Joint Angles
2.4. interACTION Application
2.5. Data Collection
2.6. Data Analysis
2.6.1. Variability and Accuracy
2.6.2. Visual Feedback
2.6.3. Survey Data
3. Results
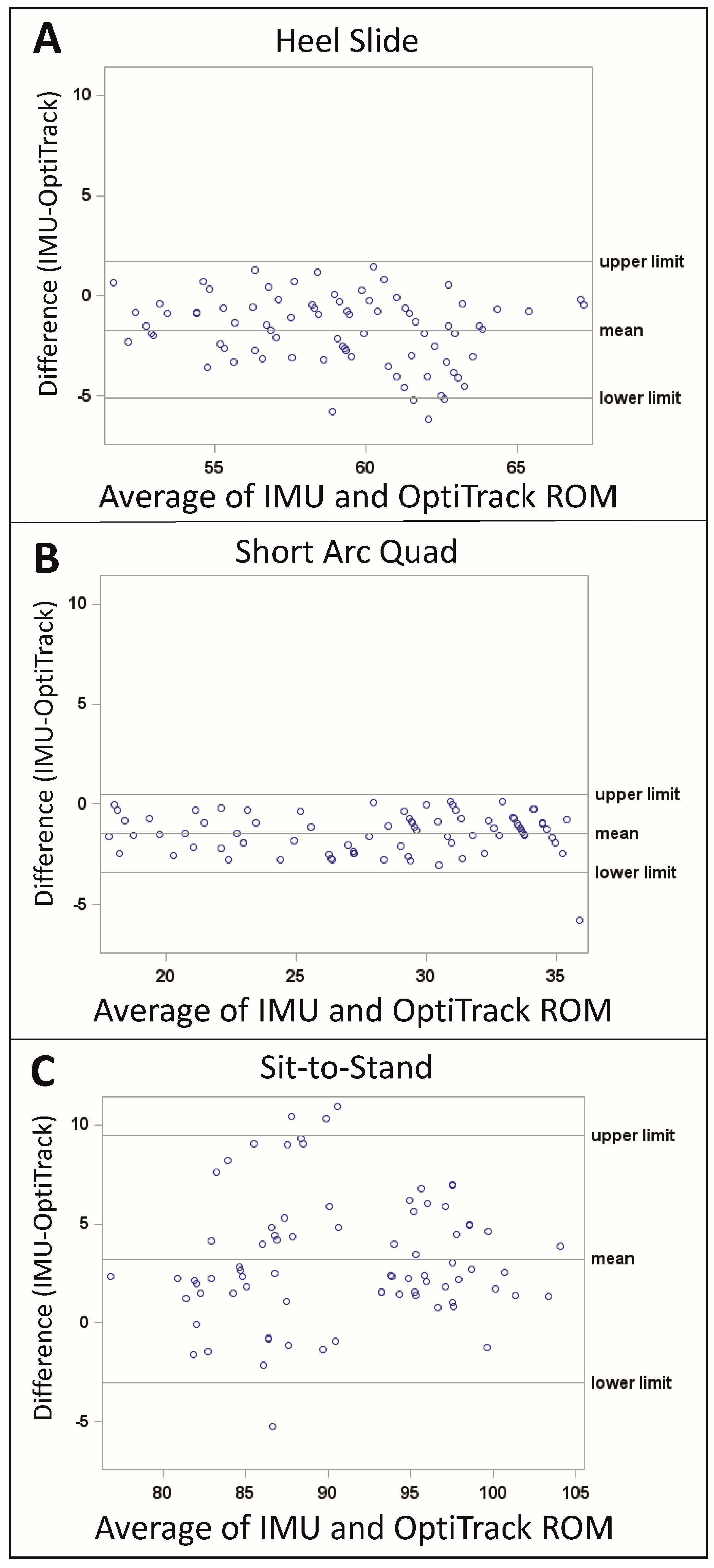
3.1. Variability and Accuracy
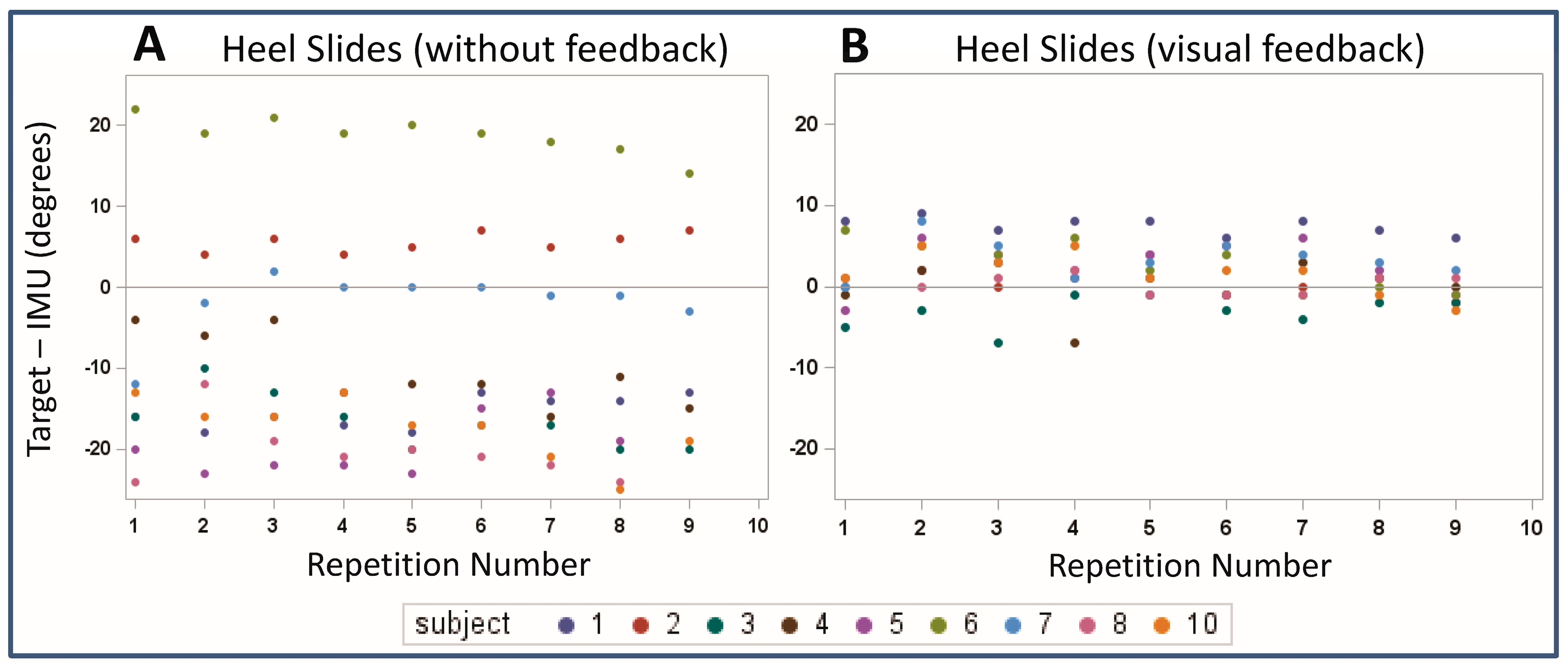
3.2. Visual Feedback
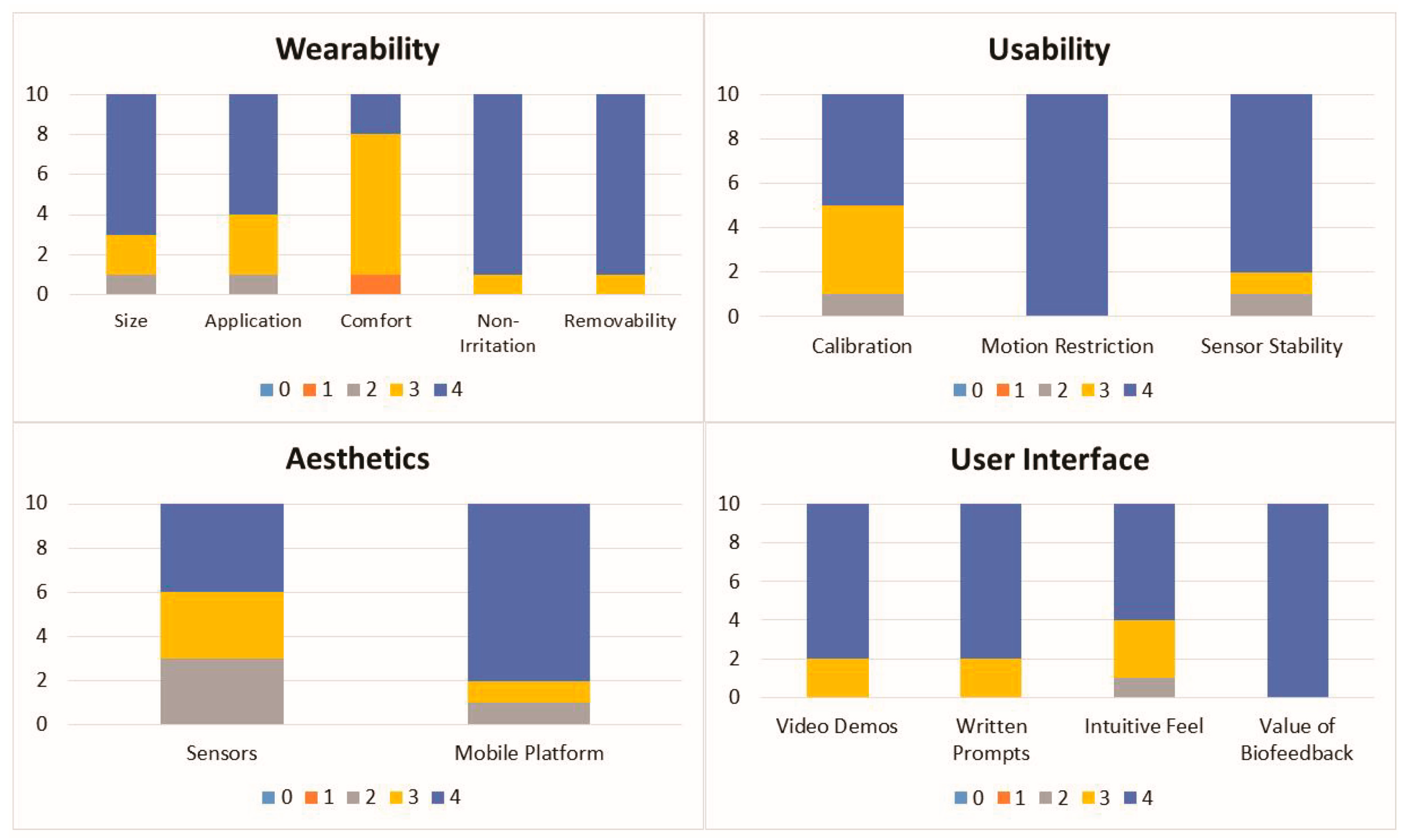
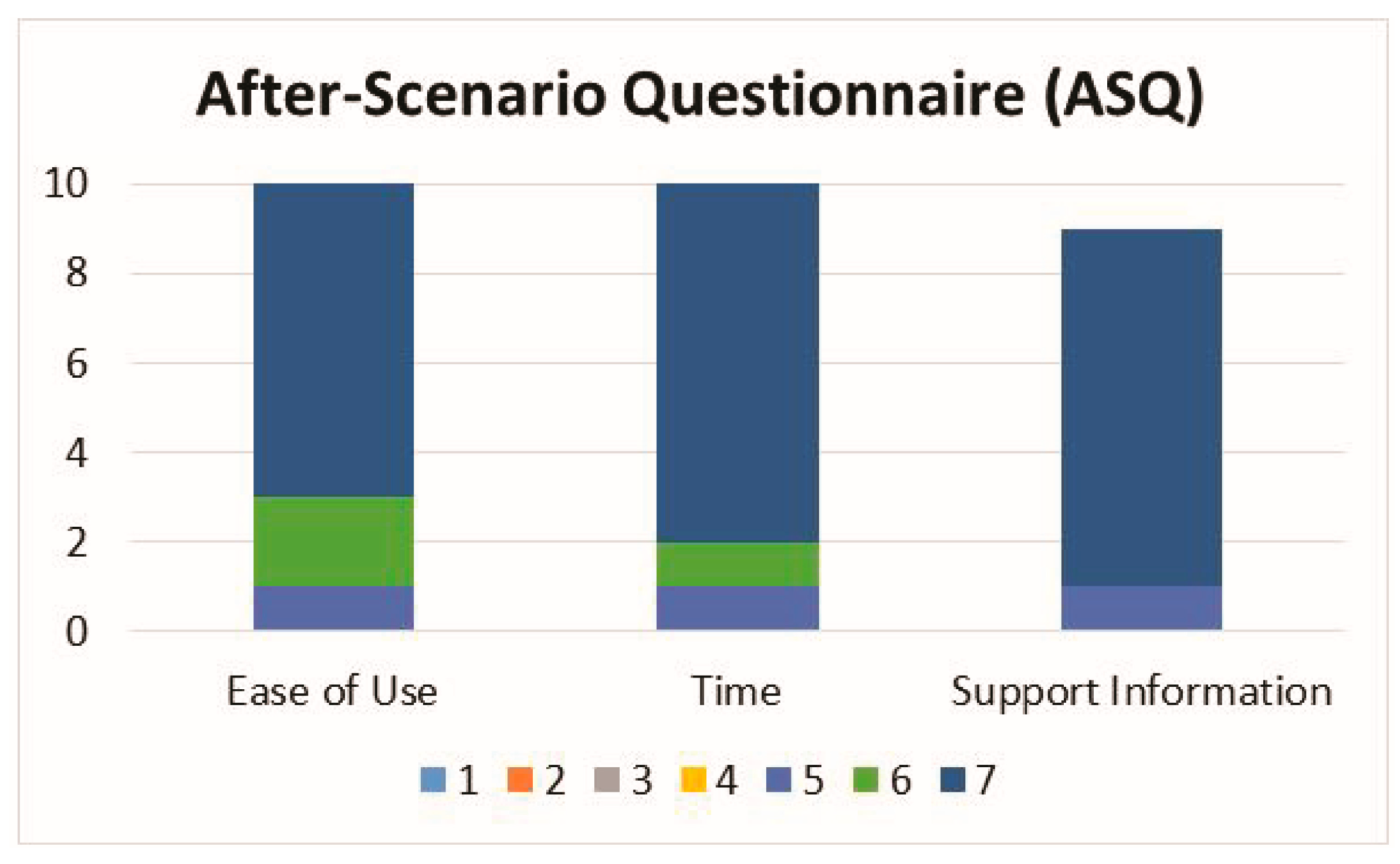
3.3. Survey Data
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Marks, R. Knee osteoarthritis and exercise adherence: A review. Curr. Aging Sci. 2012, 5, 72–83. [Google Scholar] [CrossRef] [PubMed]
- Ontario, H.Q. Physiotherapy rehabilitation after total knee or hip replacement: An evidence-based analysis. Ont. Health Technol. Assess. Ser. 2005, 5, 1–91. [Google Scholar]
- Sluijs, E.M.; Kok, G.J.; van der Zee, J. Correlates of exercise compliance in physical therapy. Phys. Ther. 1993, 73, 771–782. [Google Scholar] [CrossRef] [PubMed]
- Groen, J.W.; Stevens, M.; Kersten, R.F.; Reininga, I.H.; van den Akker-Scheek, I. After total knee arthroplasty, many people are not active enough to maintain their health and fitness: An observational study. J. Physiother. 2012, 58, 113–116. [Google Scholar] [CrossRef]
- Jack, K.; McLean, S.M.; Moffett, J.K.; Gardiner, E. Barriers to treatment adherence in physiotherapy outpatient clinics: A systematic review. Man. Ther. 2010, 15, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Issa, K.; Naziri, Q.; Johnson, A.J.; Memon, T.; Dattilo, J.; Harwin, S.F.; Mont, M.A. Evaluation of patient satisfaction with physical therapy following primary tha. Orthopedics 2013, 36, e538–e542. [Google Scholar] [CrossRef] [PubMed]
- Pivec, R.; Issa, K.; Given, K.; Harwin, S.F.; Greene, K.A.; Hitt, K.D.; Shi, S.; Mont, M.A. A prospective, longitudinal study of patient satisfaction following total knee arthroplasty using the short-form 36 (sf-36) survey stratified by various demographic and comorbid factors. J. Arthroplast. 2015, 30, 374–378. [Google Scholar] [CrossRef] [PubMed]
- Westby, M.D.; Backman, C.L. Patient and health professional views on rehabilitation practices and outcomes following total hip and knee arthroplasty for osteoarthritis:A focus group study. BMC Health Serv. Res. 2010, 10. [Google Scholar] [CrossRef] [PubMed]
- Noble, P.C.; Gordon, M.J.; Weiss, J.M.; Reddix, R.N.; Conditt, M.A.; Mathis, K.B. Does total knee replacement restore normal knee function? Clin.Orthop. Relat. Res. 2005, 431, 157–165. [Google Scholar] [CrossRef]
- Piva, S.R.; Moore, C.G.; Schneider, M.; Gil, A.B.; Almeida, G.J.; Irrgang, J.J. A randomized trial to compare exercise treatment methods for patients after total knee replacement: Protocol paper. BMC Musculoskelet. Disord. 2015, 16. [Google Scholar] [CrossRef] [PubMed]
- Hoaas, H.; Andreassen, H.K.; Lien, L.A.; Hjalmarsen, A.; Zanaboni, P. Adherence and factors affecting satisfaction in long-term telerehabilitation for patients with chronic obstructive pulmonary disease: A mixed methods study. BMC Med. Inform. Decis. Mak. 2016, 16. [Google Scholar] [CrossRef] [PubMed]
- Wood, C.L.; Clements, S.A.; McFann, K.; Slover, R.; Thomas, J.F.; Wadwa, R.P. Use of telemedicine to improve adherence to american diabetes association standards in pediatric type 1 diabetes. Diabetes Technol. Ther. 2016, 18, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Giggins, O.M.; Persson, U.M.; Caulfield, B. Biofeedback in rehabilitation. J. Neuroeng. Rehabil. 2013, 10. [Google Scholar] [CrossRef] [PubMed]
- Hussain, M.S.; Li, J.; Brindal, E.; van Kasteren, Y.; Varnfield, M.; Reeson, A.; Berkovsky, S.; Freyne, J. Supporting the delivery of total knee replacements care for both patients and their clinicians with a mobile app and web-based tool: Randomized controlled trial protocol. JMIR Res. Protoc. 2017, 6. [Google Scholar] [CrossRef] [PubMed]
- Fung, V.; Ho, A.; Shaffer, J.; Chung, E.; Gomez, M. Use of nintendo wii fit in the rehabilitation of outpatients following total knee replacement: A preliminary randomised controlled trial. Physiotherapy 2012, 98, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Ficklscherer, A.; Stapf, J.; Meissner, K.M.; Niethammer, T.; Lahner, M.; Wagenhauser, M.; Muller, P.E.; Pietschmann, M.F. Testing the feasibility and safety of the nintendo wii gaming console in orthopedic rehabilitation: A pilot randomized controlled study. Arch. Med. Sci. AMS 2016, 12, 1273–1278. [Google Scholar] [CrossRef] [PubMed]
- Baltaci, G.; Harput, G.; Haksever, B.; Ulusoy, B.; Ozer, H. Comparison between nintendo wii fit and conventional rehabilitation on functional performance outcomes after hamstring anterior cruciate ligament reconstruction: Prospective, randomized, controlled, double-blind clinical trial. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 880–887. [Google Scholar] [CrossRef] [PubMed]
- Piqueras, M.; Marco, E.; Coll, M.; Escalada, F.; Ballester, A.; Cinca, C.; Belmonte, R.; Muniesa, J.M. Effectiveness of an interactive virtual telerehabilitation system in patients after total knee arthoplasty: A randomized controlled trial. J. Rehabil. Med. 2013, 45, 392–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correia, F.D.; Nogueira, A.; Magalhaes, I.; Guimaraes, J.; Moreira, M.; Barradas, I.; Teixeira, L.; Tulha, J.; Seabra, R.; Lains, J.; et al. Home-based rehabilitation with a novel digital biofeedback system versus conventional in-person rehabilitation after total knee replacement: A feasibility study. Sci. Rep. 2018, 8, 11299. [Google Scholar] [CrossRef] [PubMed]
- Madgwick, S.O.; Harrison, A.J.; Vaidyanathan, A. Estimation of imu and marg orientation using a gradient descent algorithm. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011. [Google Scholar]
- Abhayasinghe, N.; Murray, I. The application of “off-the-shelf” components for buildings imus for navigation research. In Proceedings of the 2014 International Conference on Indoor Positioning and Indoor Navigation, Busan, Korea, 27–30 October 2014; pp. 116–121. [Google Scholar]
- Chandrasiri, R.; Abhayasinghe, N.; Murray, I. Bluetooth embedded inertial measurement unit for real-time data collection for gait analysis. In Proceedings of the 2013 International Conference on Indoor Positioning and Indoor Navigation, Montbeliard, France, 28–31 October 2013. [Google Scholar]
- Thewlis, D.; Bishop, C.; Daniell, N.; Paul, G. Next-generation low-cost motion capture systems can provide comparable spatial accuracy to high-end systems. J. Appl. Biomech. 2013, 29, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Carse, B.; Meadows, B.; Bowers, R.; Rowe, P. Affordable clinical gait analysis: An assessment of the marker tracking accuracy of a new low-cost optical 3d motion analysis system. Physiotherapy 2013, 99, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Picerno, P. 25 years of lower limb joint kinematics by using inertial and magnetic sensors: A review of methodological approaches. Gait Posture 2017, 51, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Favre, J.; Jolles, B.M.; Aissaoui, R.; Aminian, K. Ambulatory measurement of 3d knee joint angle. J. Biomech. 2008, 41, 1029–1035. [Google Scholar] [CrossRef] [PubMed]
- Picerno, P.; Cereatti, A.; Cappozzo, A. Joint kinematics estimate using wearable inertial and magnetic sensing modules. Gait Posture 2008, 28, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Bakhshi, S.M.; Mahoor, M.H.; Davidson, B.S. Development of a body joint angle measurement system using imu sensors. In Proceedings of the 33rd Annual International Conference of the IEEE EMBS, Boston, MA, USA, 30 August–3 September 2011; pp. 6923–6926. [Google Scholar]
- Lewis, J.R. Ibm computer usability satisfaction questionnaires: Psychometric evaluation and instructions for use. Int. J. Hum.-Comput. Interact. 1995, 7, 57–78. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Cooper, G.; Sheret, I.; McMillan, L.; Siliverdis, K.; Sha, N.; Hodgins, D.; Kenney, L.; Howard, D. Inertial sensor-based knee flexion/extension angle estimation. J. Biomech. 2009, 42, 2678–2685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Findlow, A.; Goulermas, J.Y.; Nester, C.; Howard, D.; Kenney, L.P. Predicting lower limb joint kinematics using wearable motion sensors. Gait Posture 2008, 28, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Leardini, A.; Lullini, G.; Giannini, S.; Berti, L.; Ortolani, M.; Caravaggi, P. Validation of the angular measurements of a new inertial-measurement-unit based rehabilitation system comparison with start-of-the-art gait analysis. J. Neuroeng. Rehabil. 2014, 11. [Google Scholar] [CrossRef] [PubMed]
- Papi, E.; Osei-Kuffour, D.; Chen, Y.M.; McGregor, A.H. Use of wearable technology for performance assessment: A validation study. Med. Eng. Phys. 2015, 37, 698–704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tulipani, L.; Boocock, M.G.; Lomond, K.V.; El-Gohary, M.; Reid, D.A.; Henry, S.M. Validation of an inertial sensor system for physical therapists to quantify movement coordination during functional tasks. J. Appl. Biomech. 2018, 34, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.Y.; Laprade, J.; Fung, E.H. A real-time gyroscopic system for three-dimensional measurement of lumbar spine motion. Med. Eng. Phys. 2003, 25, 817–824. [Google Scholar] [CrossRef]
- Saber-Sheikh, K.; Bryant, E.C.; Glazzard, C.; Hamel, A.; Lee, R.Y. Feasibility of using inertial sensors to assess human movement. Man. Ther. 2010, 15, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Tognetti, A.; Lorussi, F.; Carbonaro, N.; de Rossi, D. Wearable goniometer and accelerometer sensory fusion for knee joint angle measurement in daily life. Sensors 2015, 15, 28435–28455. [Google Scholar] [CrossRef] [PubMed]
- Al-Amri, M.; Nicholas, K.; Button, K.; Sparkes, V.; Sheeran, L.; Davies, J.L. Inertial measurement units for clinical movement analysis: Reliability and concurrent validity. Sensors 2018, 18, 719. [Google Scholar] [CrossRef] [PubMed]
- Jaysrichai, T.; Suputtitada, A.; Khovidhungij, W. Mobile sensor application for kinematic detection of the knees. Ann. Rehabil. Med. 2015, 39, 599–608. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.I.; Inoue, Y.; Shibata, K. Development of a wearable sensor system for quantitative gait analysis. Measurement 2009, 42, 978–988. [Google Scholar] [CrossRef]
- Bechly, K.E.; Carender, W.J.; Myles, J.D.; Sienko, K.H. Determining the preferred modality for real-time biofeedback during balance training. Gait Posture 2013, 37, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Franco, C.; Fleury, A.; Gumery, P.Y.; Diot, B.; Demongeot, J.; Vuillerme, N. Ibalance-abf: A smartphone-based audio-biofeedback balance system. IEEE Trans. Biomed. Eng. 2013, 60, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Ginis, P.; Nieuwboer, A.; Dorfman, M.; Ferrari, A.; Gazit, E.; Canning, C.G.; Rocchi, L.; Chiari, L.; Hausdorff, J.M.; Mirelman, A. Feasibility and effects of home-based smartphone-delivered automated feedback training for gait in people with parkinson’s disease: A pilot randomized controlled trial. Parkinsonism Relat. Disord. 2016, 22, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Halicka, Z.; Lobotkova, J.; Buckova, K.; Hlavacka, F. Effectiveness of different visual biofeedback signals for human balance improvement. Gait Posture 2014, 39, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.Z.; Wong, D.W.; Lam, W.K.; Wan, A.H.; Lee, W.C. Balance improvement effects of biofeedback systems with state-of-the-art wearable sensors: A systematic review. Sensors 2016, 16, 434. [Google Scholar] [CrossRef] [PubMed]
- Vadnerkar, A.; Figueiredo, S.; Mayo, N.E.; Kearney, R.E. Design and validation of a biofeedback device to improve heel-to-toe gait in seniors. IEEE J. Biomed. Health Inform. 2018, 22, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Bao, T.; Lee, U.H.; Kinnaird, C.; Carender, W.; Huang, Y.; Sienko, K.H.; Shull, P.B. Configurable, wearable sensing and vibrotactile feedback system for real-time postural balance and gait training: Proof-of-concept. J. Neuroeng. Rehabil. 2017, 14. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Heel Slides | Short Arc Quad | Sit-to-Stand | |
|---|---|---|---|
| RoM IMUs (Mean ± SD) | 58.2° ± 3.5° | 27.5° ± 5.3° | 92.5° ± 6.7° |
| RoM OptiTrack (Mean ± SD) | 59.9° ± 3.9° | 28.9° ± 5.3° | 89.3° ± 6.5° |
| Intra-Subject Variability IMUs | 2.4° | 2.0° | 2.5° |
| RMSE (IMUs vs. OptiTrack) | 2.4° | 2.0° | 2.9° |
| ICC (IMUs vs. OptiTrack) | 0.58 | 0.86 | 0.80 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bell, K.M.; Onyeukwu, C.; McClincy, M.P.; Allen, M.; Bechard, L.; Mukherjee, A.; Hartman, R.A.; Smith, C.; Lynch, A.D.; Irrgang, J.J. Verification of a Portable Motion Tracking System for Remote Management of Physical Rehabilitation of the Knee. Sensors 2019, 19, 1021. https://0-doi-org.brum.beds.ac.uk/10.3390/s19051021
Bell KM, Onyeukwu C, McClincy MP, Allen M, Bechard L, Mukherjee A, Hartman RA, Smith C, Lynch AD, Irrgang JJ. Verification of a Portable Motion Tracking System for Remote Management of Physical Rehabilitation of the Knee. Sensors. 2019; 19(5):1021. https://0-doi-org.brum.beds.ac.uk/10.3390/s19051021
Chicago/Turabian StyleBell, Kevin M., Chukwudi Onyeukwu, Michael P. McClincy, Marcus Allen, Laura Bechard, Abhigyan Mukherjee, Robert A. Hartman, Clair Smith, Andrew D. Lynch, and James J. Irrgang. 2019. "Verification of a Portable Motion Tracking System for Remote Management of Physical Rehabilitation of the Knee" Sensors 19, no. 5: 1021. https://0-doi-org.brum.beds.ac.uk/10.3390/s19051021