
Optimization of X-ray Investigations in Dentistry Using Optical Coherence Tomography


 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
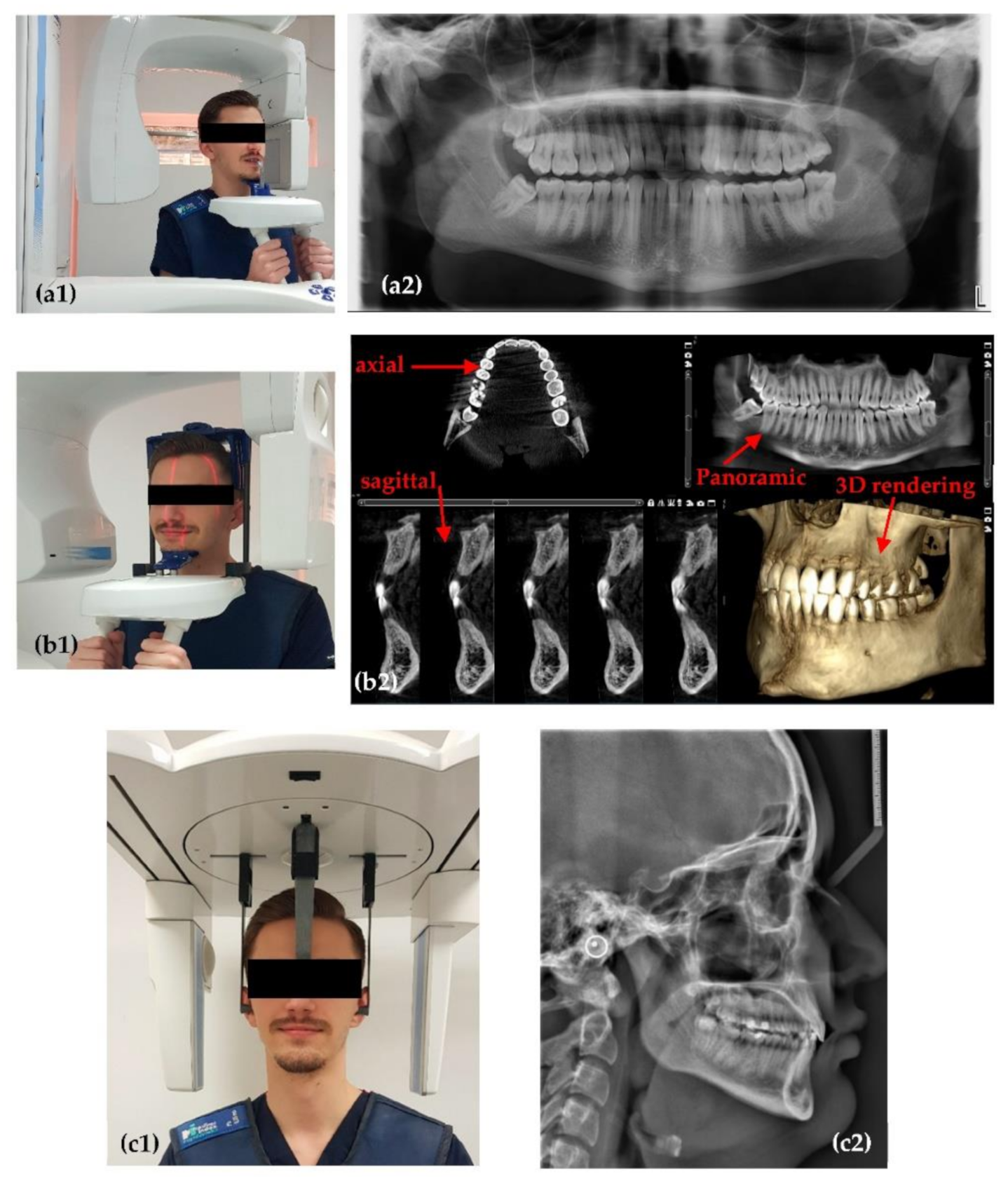
2.1. Planmeca ProMax 3D
2.2. Soredex Cranex 3D
2.3. OCT System
2.4. The Concept of X-ray Imaging Optimization Using OCT
- (1)
- An adjustment of X-ray tube and unit parameters cannot be done on patients (i.e., experimenting on them); it has to be carried out in vitro. Optimal settings thus determined could be then applied on patients. This logical sequence is used in the protocol to be developed in this work.
- (2)
- An essential question is: what method to employ for an X-ray system calibration? It must provide better and, ideally, higher-order (from a metrological point of view) resolution images than radiography but related to the same targets/samples. Then, the X-ray tube settings could be adjusted to match the radiographic results with those of the “calibration” method, following an appropriate metrological approach.
- (3)
- Finally, what type of higher-resolution system would be able to serve for such a calibration process? It has to be an imaging system, as devices used clinically for visual observation cannot allow for this planned calibration. Regarding imaging systems, all types of Computed Tomography (CT), including micro-CT are expensive and therefore out of reach of common dental practices, even of dental clinics, that would not invest in such equipment. The same cost limitation refers to high-resolution systems such as Scanning Electron Microscopy (SEM). On the other hand, dedicated devices for the oral cavity, such as the Diagnocam (KaVo Kerr, Brea, CA, USA) or the VistaCam (Dürr Dental SE, Bietigheim-Bissingen, Germany) may provide resolutions similar to those of radiographs (but only for certain areas that they are capable to investigate), therefore they are not a higher-order resolution method (on the metrological chain).
2.5. OCT versus Radiography
3. Results and Discussion
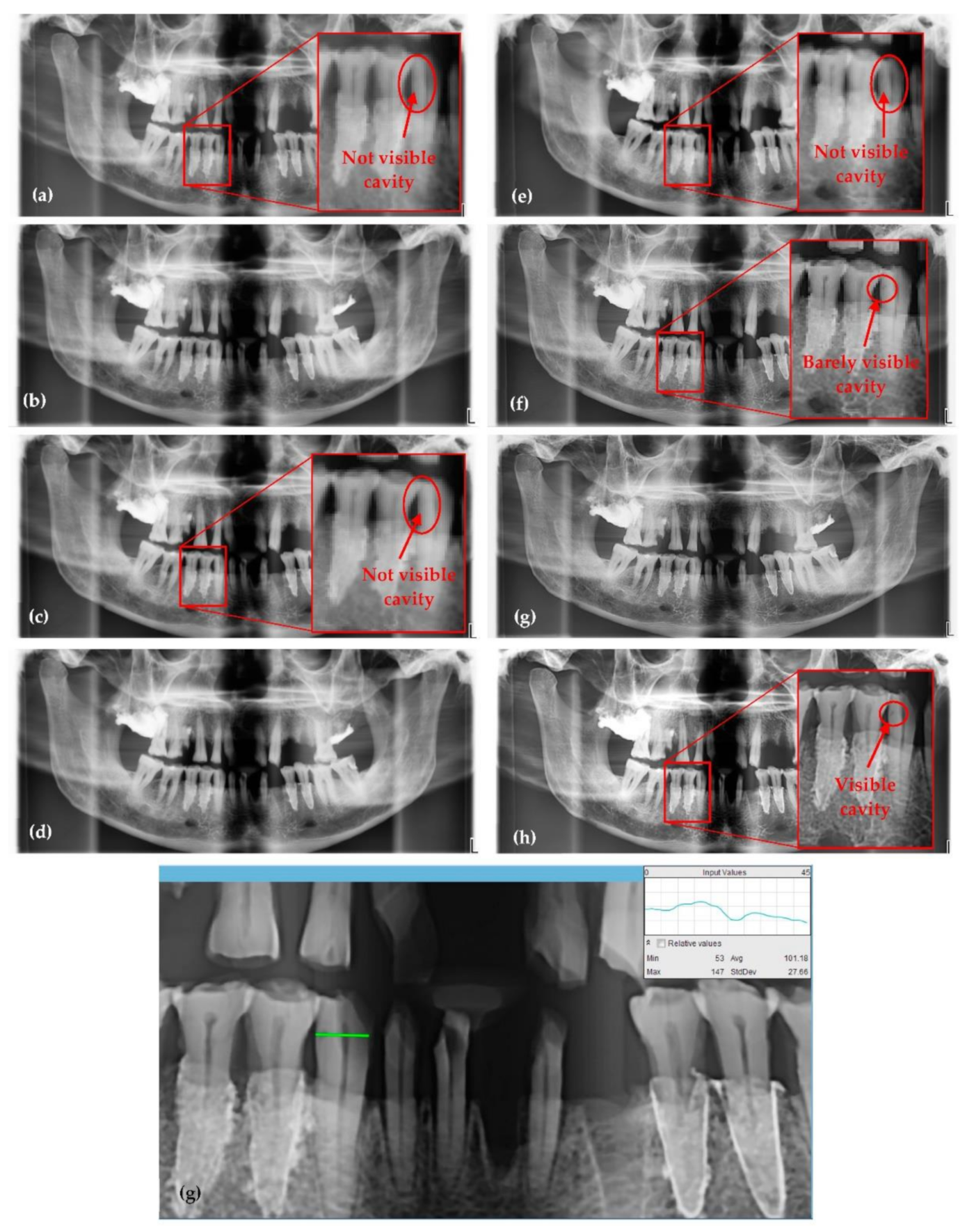
3.1. Optimized Protocol with OCT for X-ray Imaging Calibration. Panoramic Radiography
- (1)
- A higher value of anode voltage means higher energy of the X-ray beam, hence X-ray photons of shorter wavelengths. Therefore, the higher the voltage, the larger the differences in absorption of the radiation that passes through tissue (according to Lambert-Beer’s law), therefore more shades of gray appear in the images. At first sight this may seem a drawback but the increase in the number of shades of gray with sharp edges means more details on the image, which is advantageous for medical imaging. However, this voltage increase is limited, as explained, to keep the radiation dose at safe levels for the patient.
- (2)
- The number of X-ray photons emitted in time depends on the current intensity that is heating the filament of the X-ray tube. This quantity is also known as the intensity of the X-ray beam or radiation exposure.
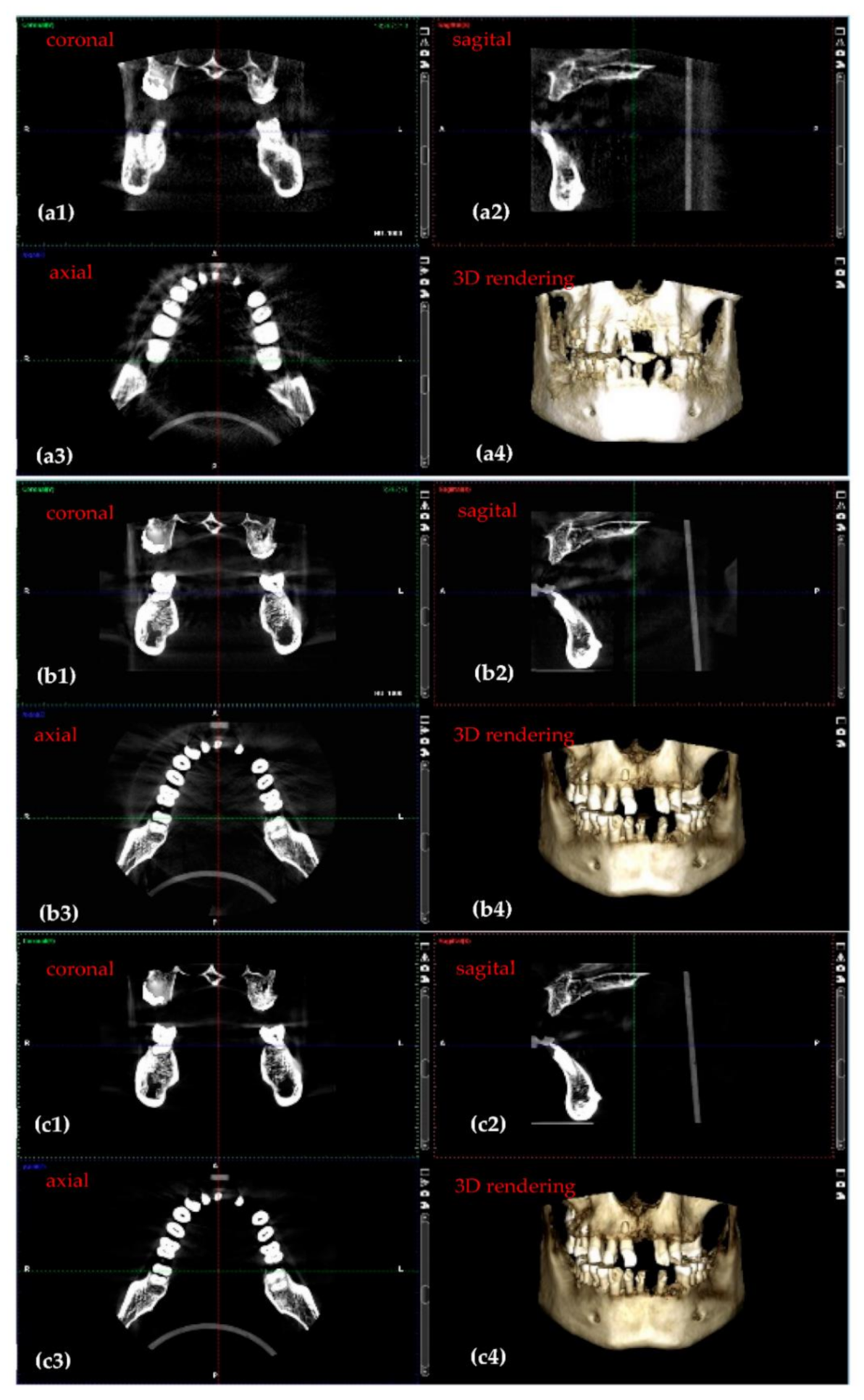
3.2. Optimized Protocol with OCT. 3D CBCT Calibration
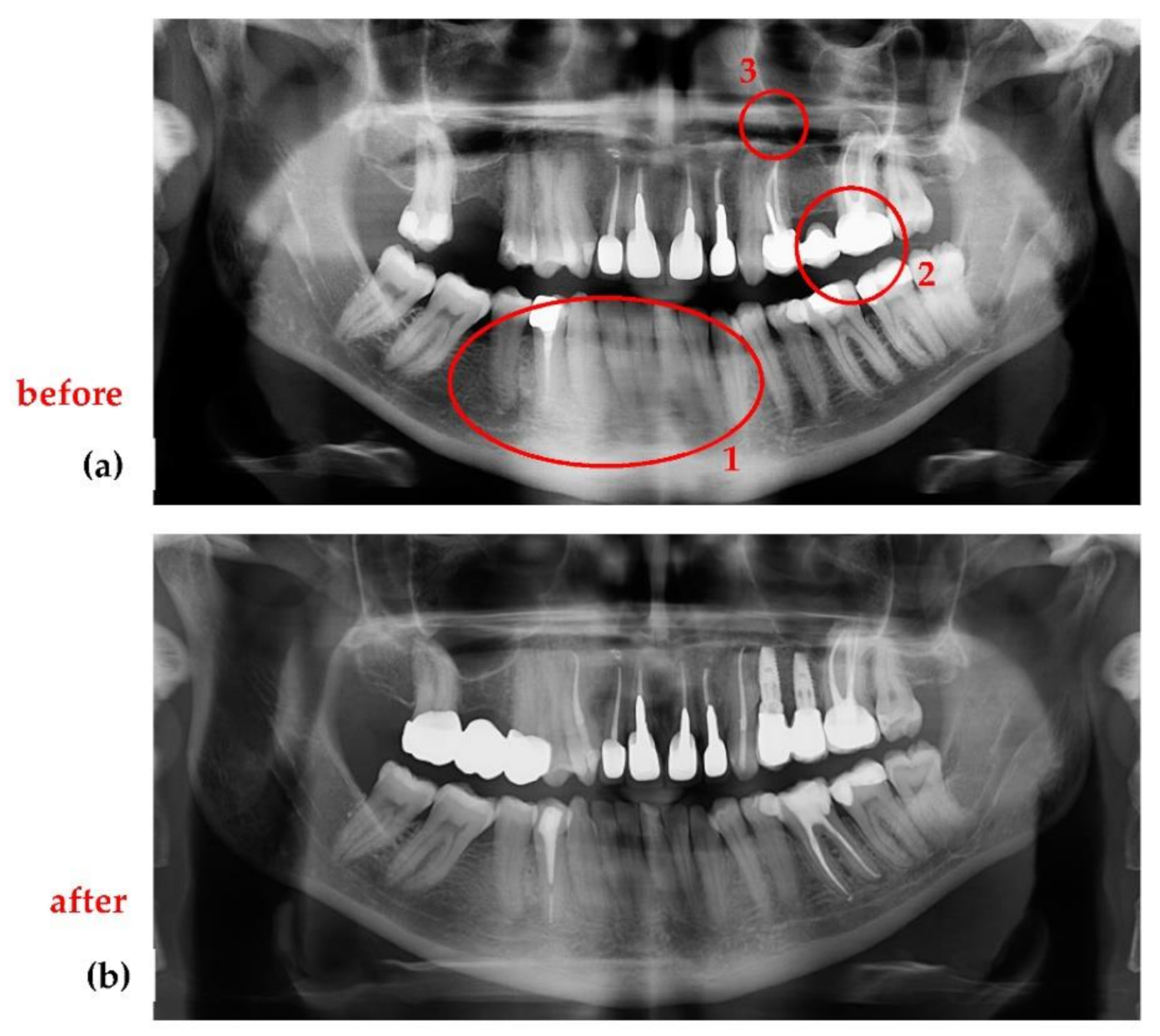
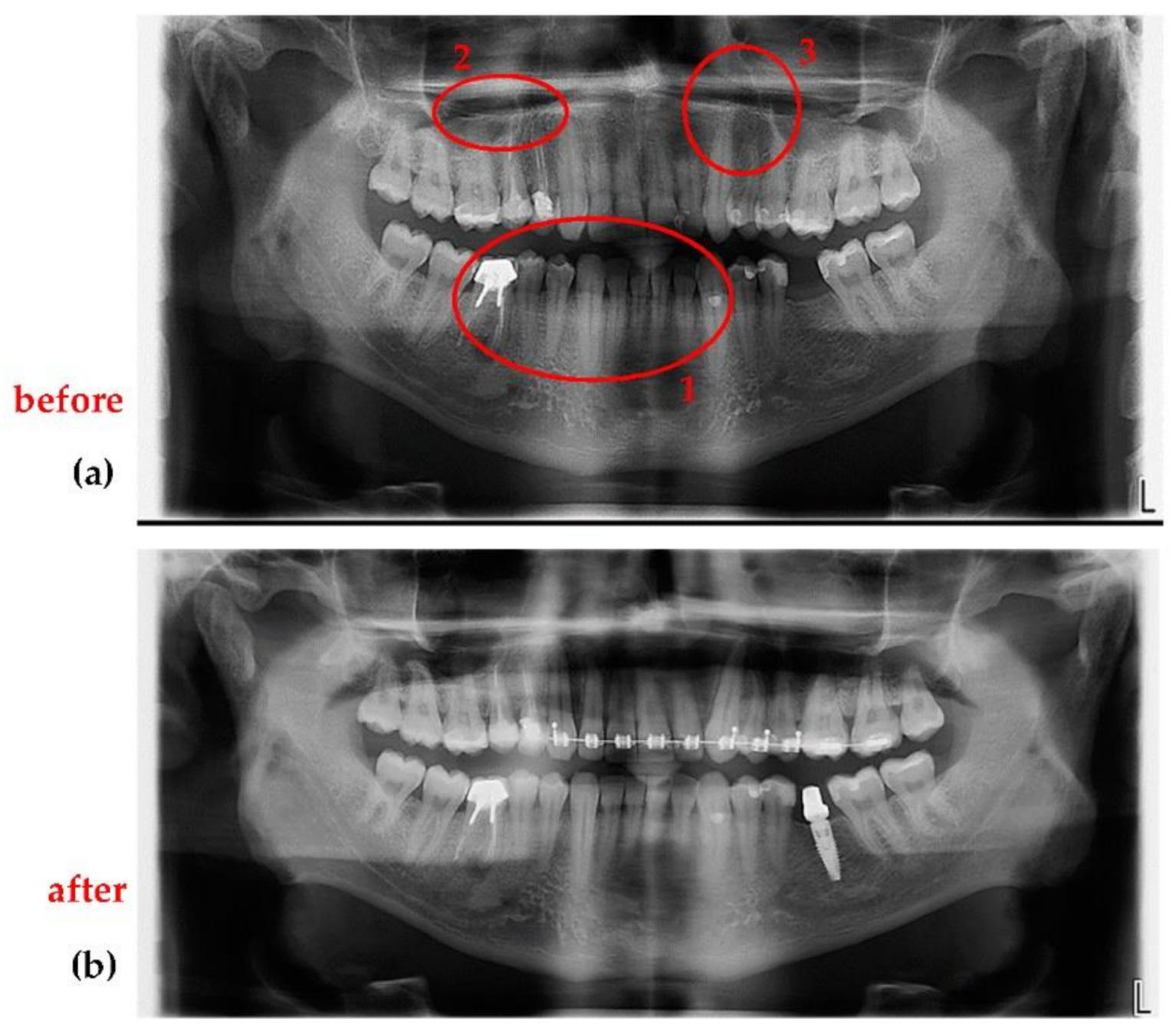
3.3. Application of the Optimization Protocol on Patients (In Vivo)
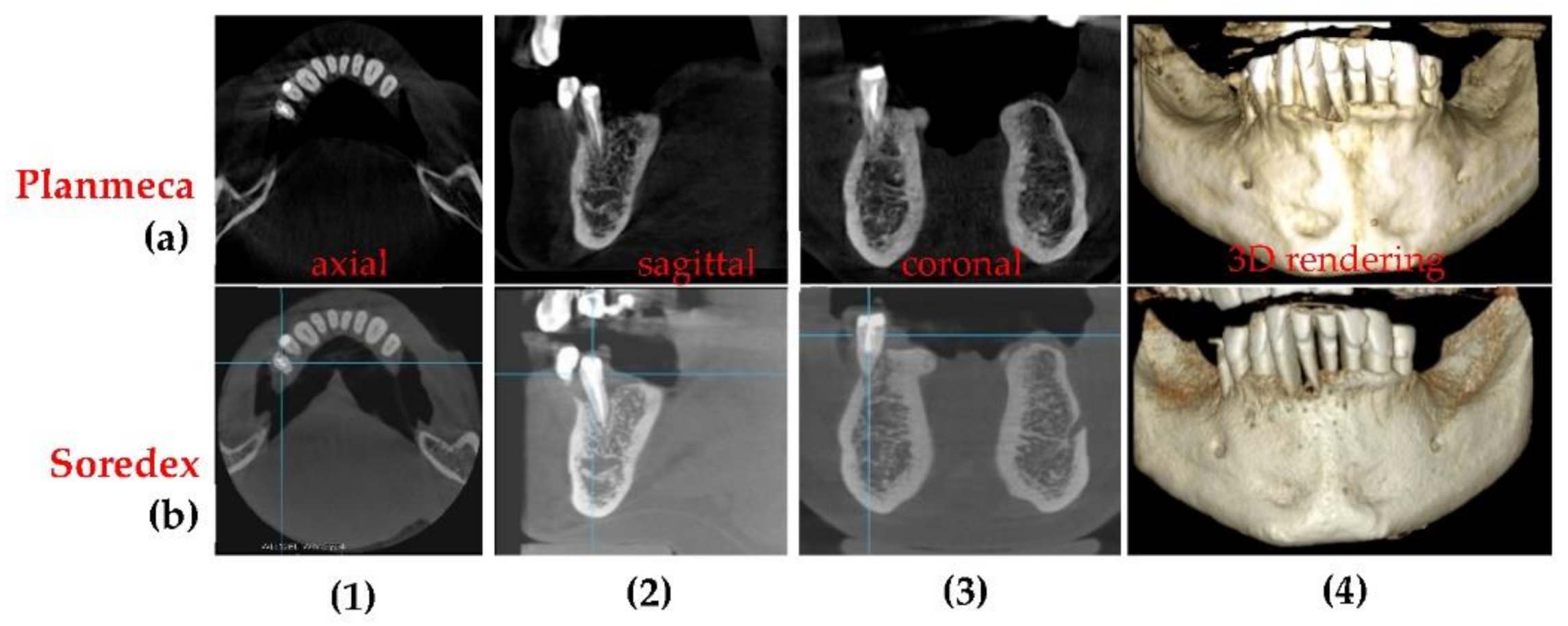
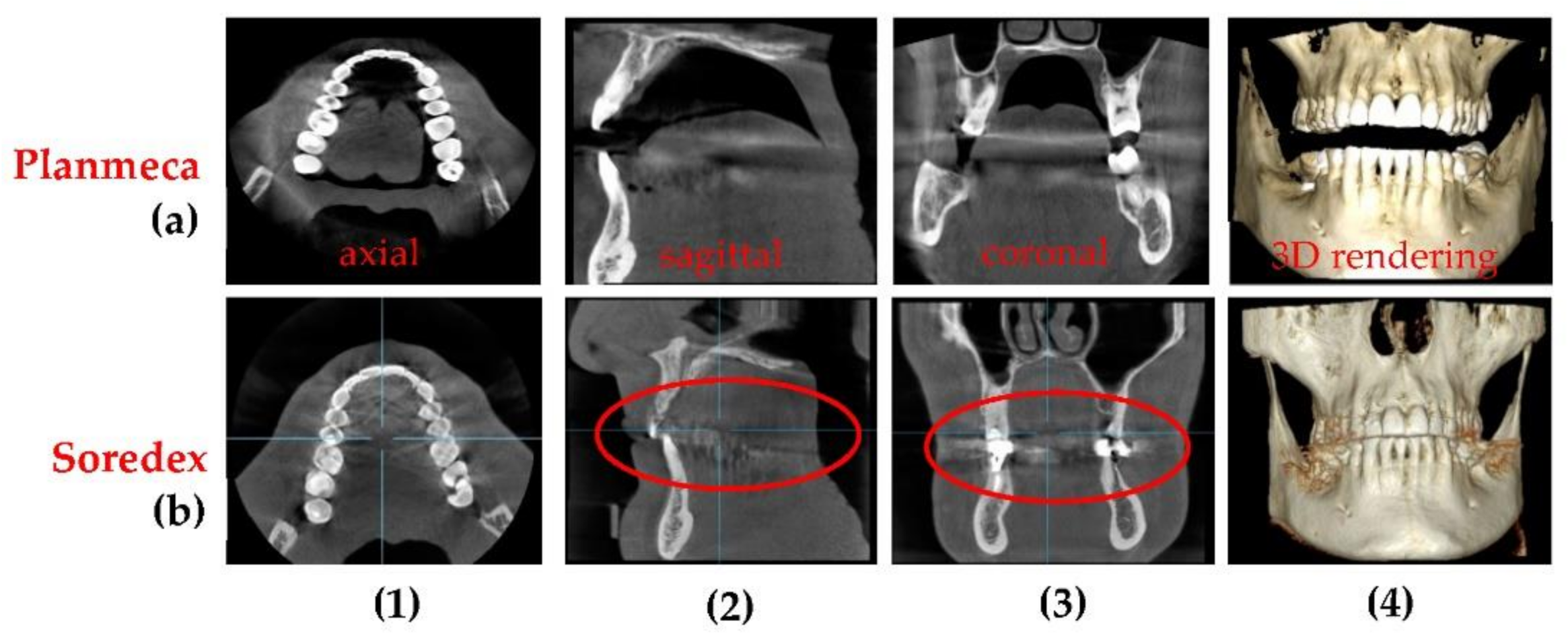
3.4. Differences Between the Planmeca and the Soredex System
3.5. Remarks
- (1)
- Different X-ray settings are needed for children, male or female patients (a different radiation dose is recommended to each of these three categories). Therefore, when the sample is changed, to achieve the optimum in X-ray imaging one must employ OCT again. However, a library of parameters can be obtained for different types of patients and for a specific machine.
- (2)
- Following on from the previous point, human anatomical characteristics that can influence the radiography must be considered. For example, an overweight patient with a larger amount of fat tissue on mandible and maxillary must be exposed to a higher X-ray dose than a patient with normal weight.
- (3)
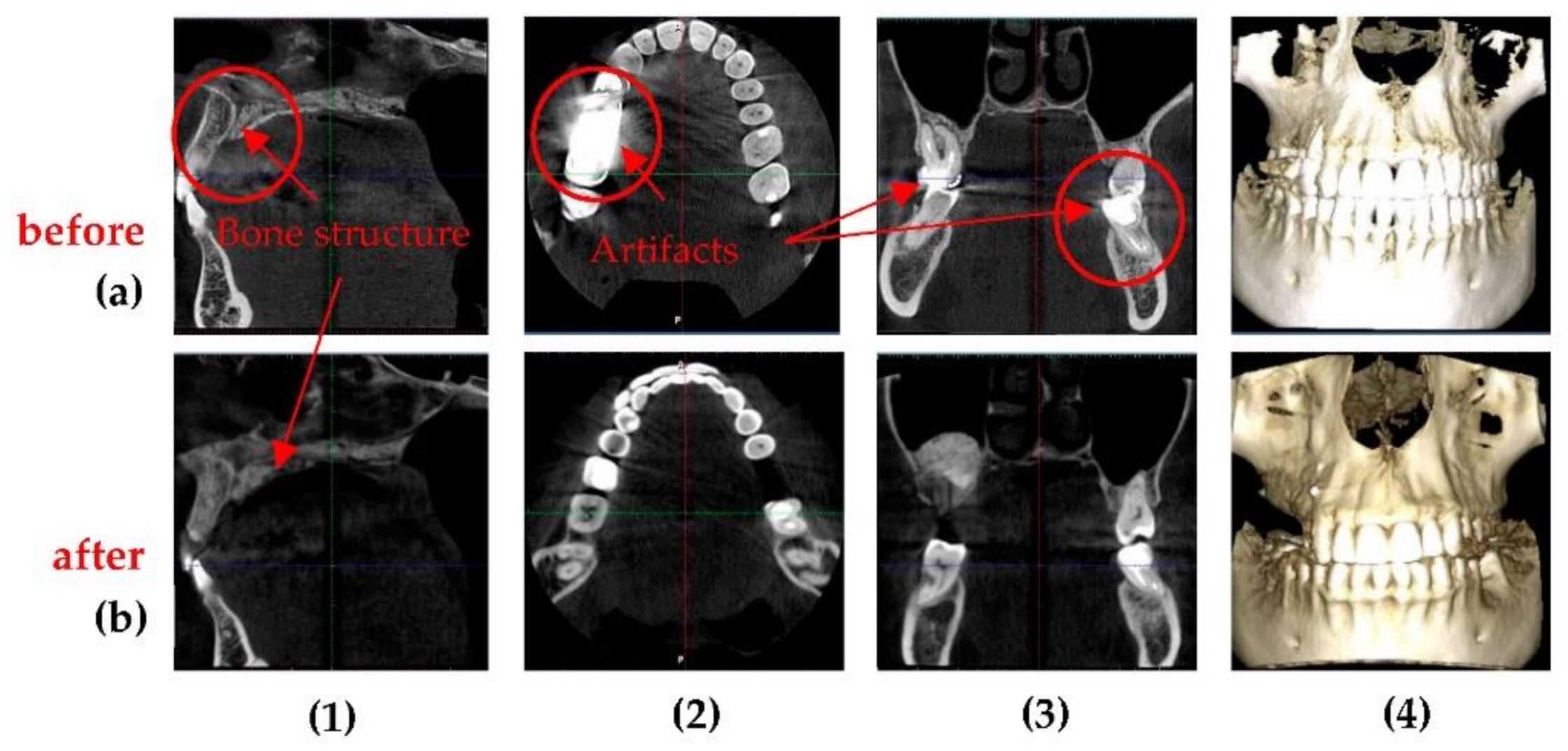
- Radio opacity of dental materials used in previous treatments influence the quality of the radiographs. A patient with numerous metal crowns, for example, must be exposed to a lower radiation dose because otherwise artifacts may appear due to the high quantity of X-ray radiation absorbed by metals. This means that the values determined in this study might be different for other X-ray units, although the principle of the procedure remains the same. Thus, to achieve the best possible image, every X-ray unit should be calibrated and the best settings for anode voltage, current intensity, and exposure time should be obtained.
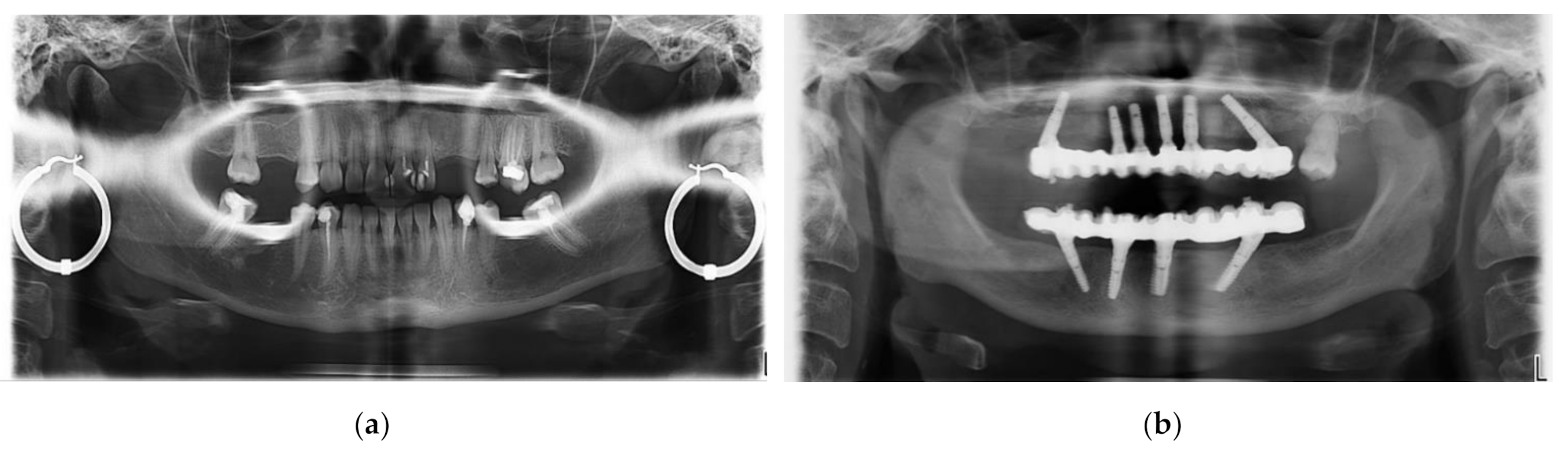
- (4)
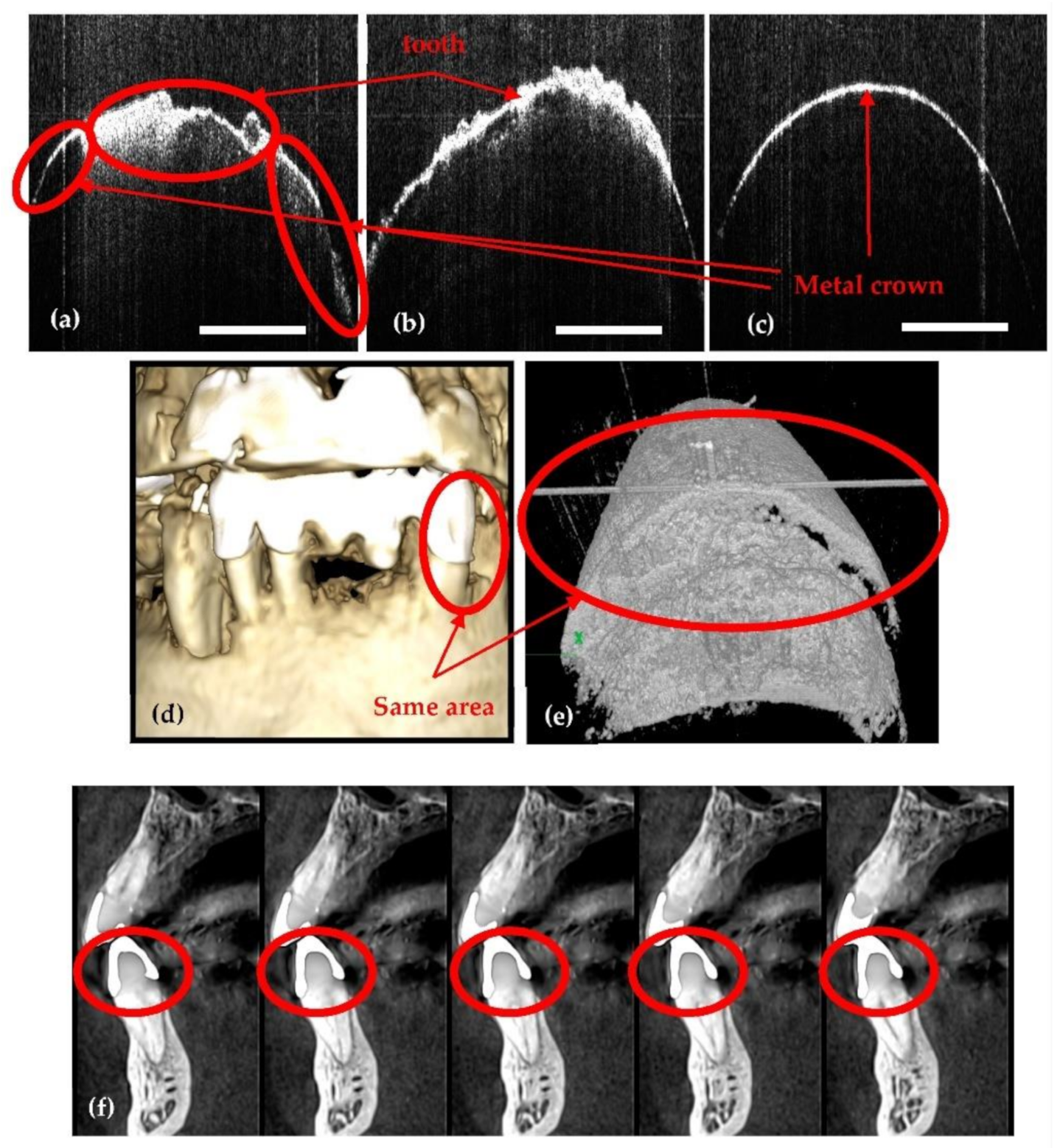
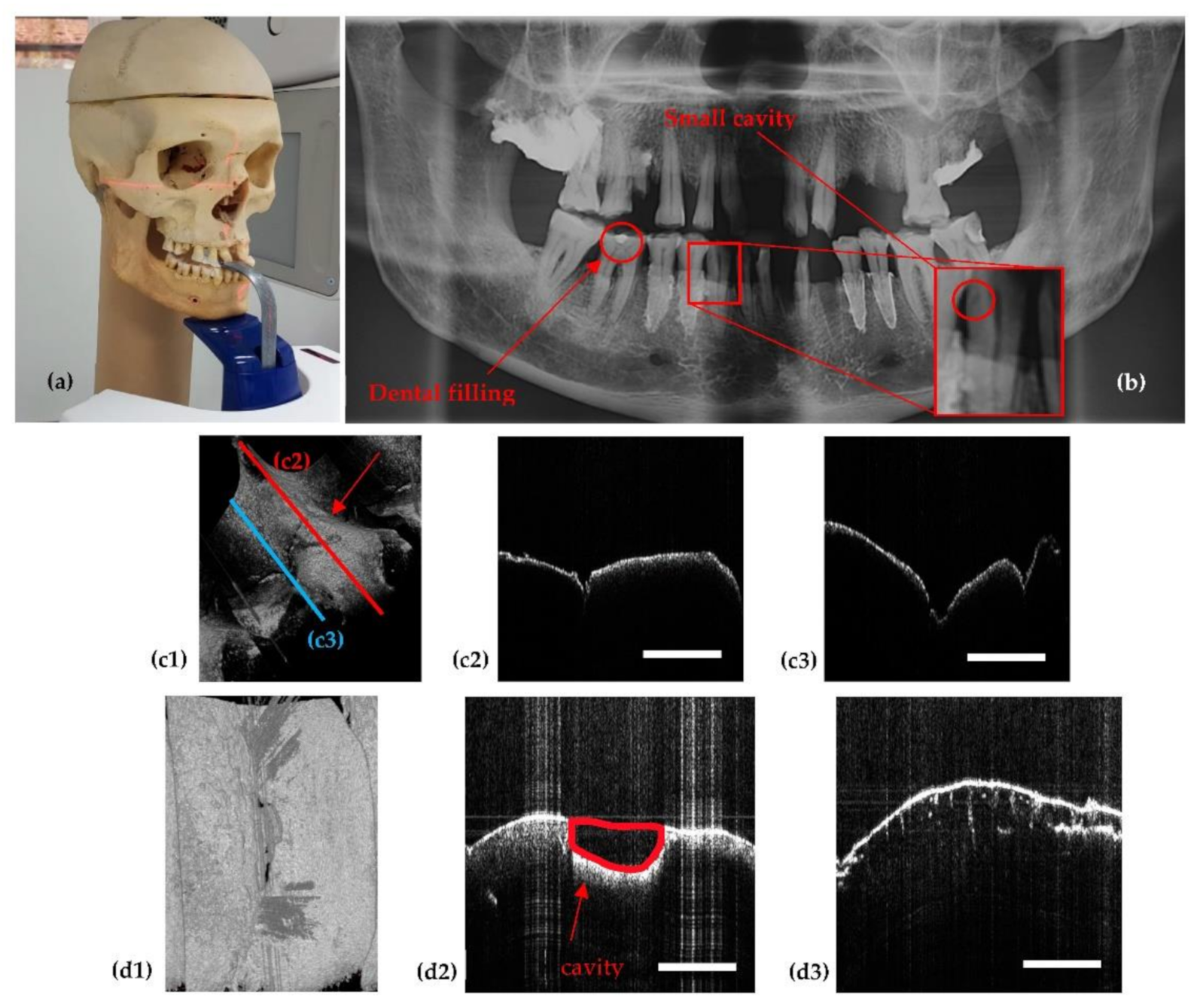
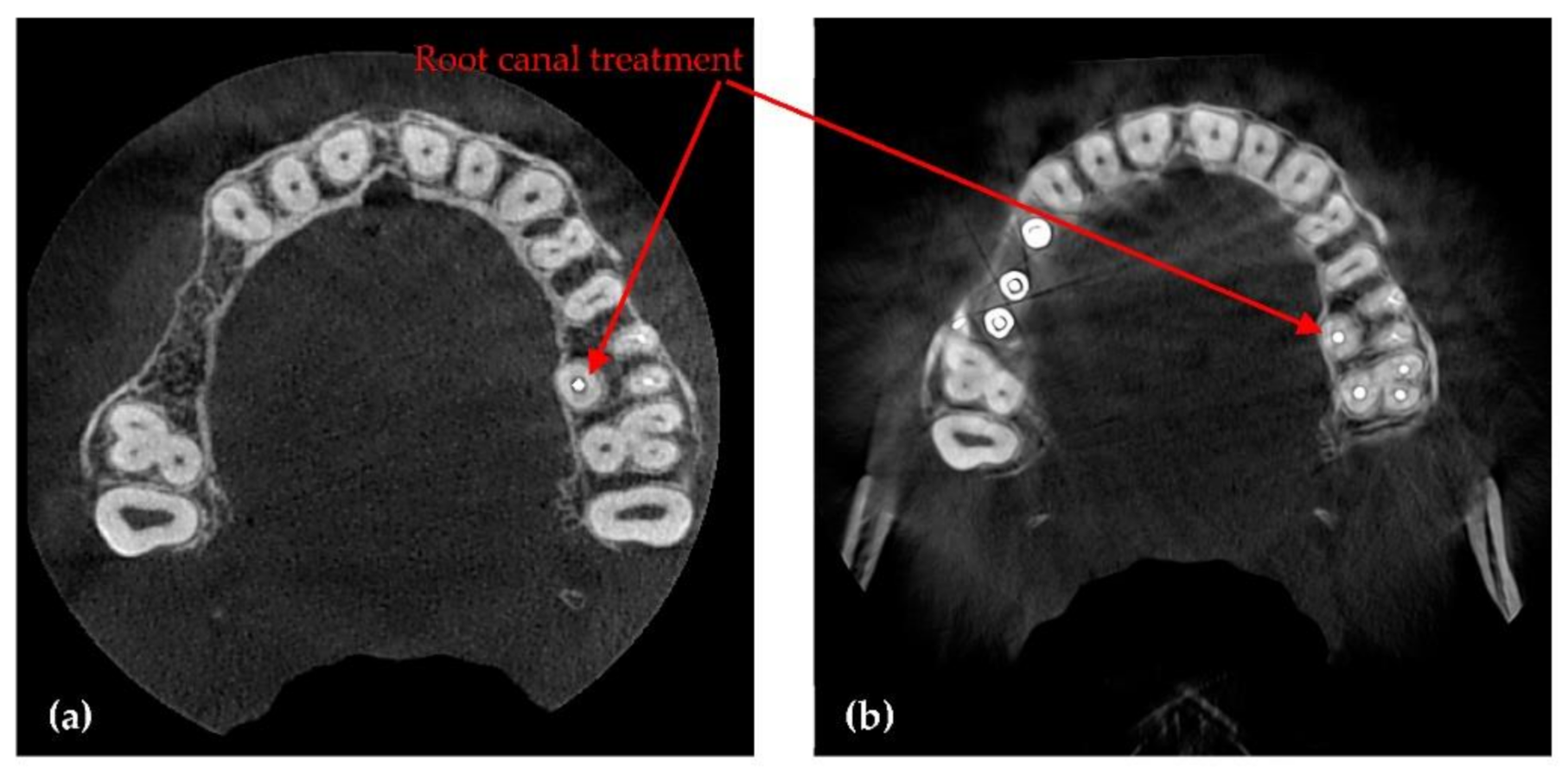
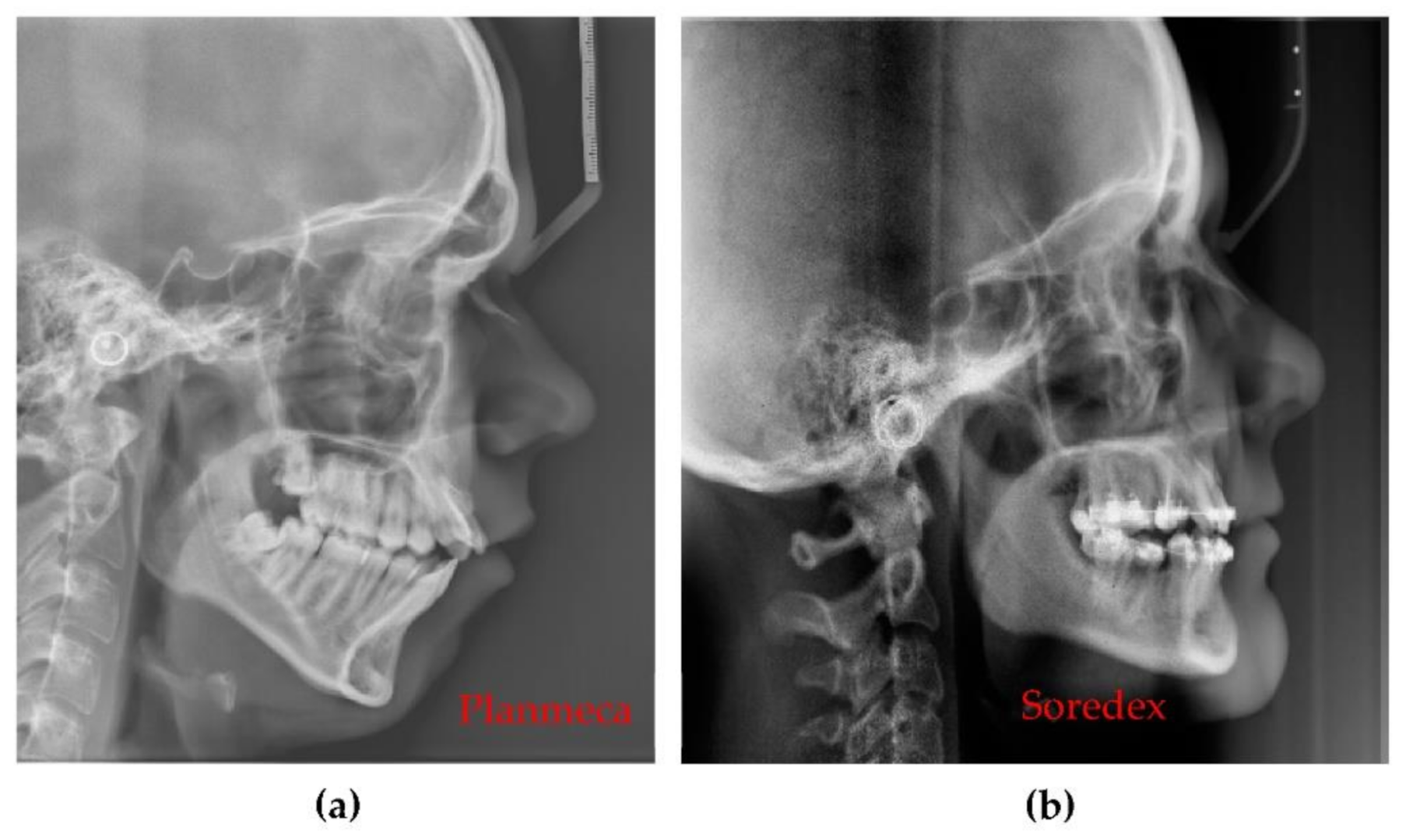
- Jewelry or any metal around the head or neck must be taken off, otherwise artifacts may appear on radiographs (Figure 17a). This is a general requirement, irrespective of the calibration procedure using OCT. On the other hand, implants and some materials used for dental crowns or dental fillings do not produce artifacts or sparkles around them on radiographs, as shown in the example in Figure 17b. This latter aspect must be considered during calibrations.
- (5)
- The performances of X-ray units evolve continuously, including improvement in their radiation dose, to better comply with the ALARA protocol. Thus, radiation doses for 3D CBCT images made with Planmeca and Soredex units considered in this study are smaller than radiation doses found in studies carried out two decades ago, for example. Thus, in a study published in 2002 [44], the effective dose for a multi-slice CT was 740 µSv, the effective dose for Planmeca’s 3D CBCT was 86.4 µSv and for Soredex, 93.7 µSv. In another study, published in 2003 [45], the radiation doses were even higher: for a total 3D CBCT the effective dose was 2100 µSv, for maxilary 1400 µSv, for mandible 1320 µSv, for panoramic 10 µSv, and for intraoral radiographs 5 µSv. This remark is essential, as it points out that in the future, as the level of radiation doses may decrease, higher increases in other parameters, such as current intensity and voltage can be made. Therefore, such an OCT-based optimization protocol of X-ray imaging may become even more practical.
- (6)
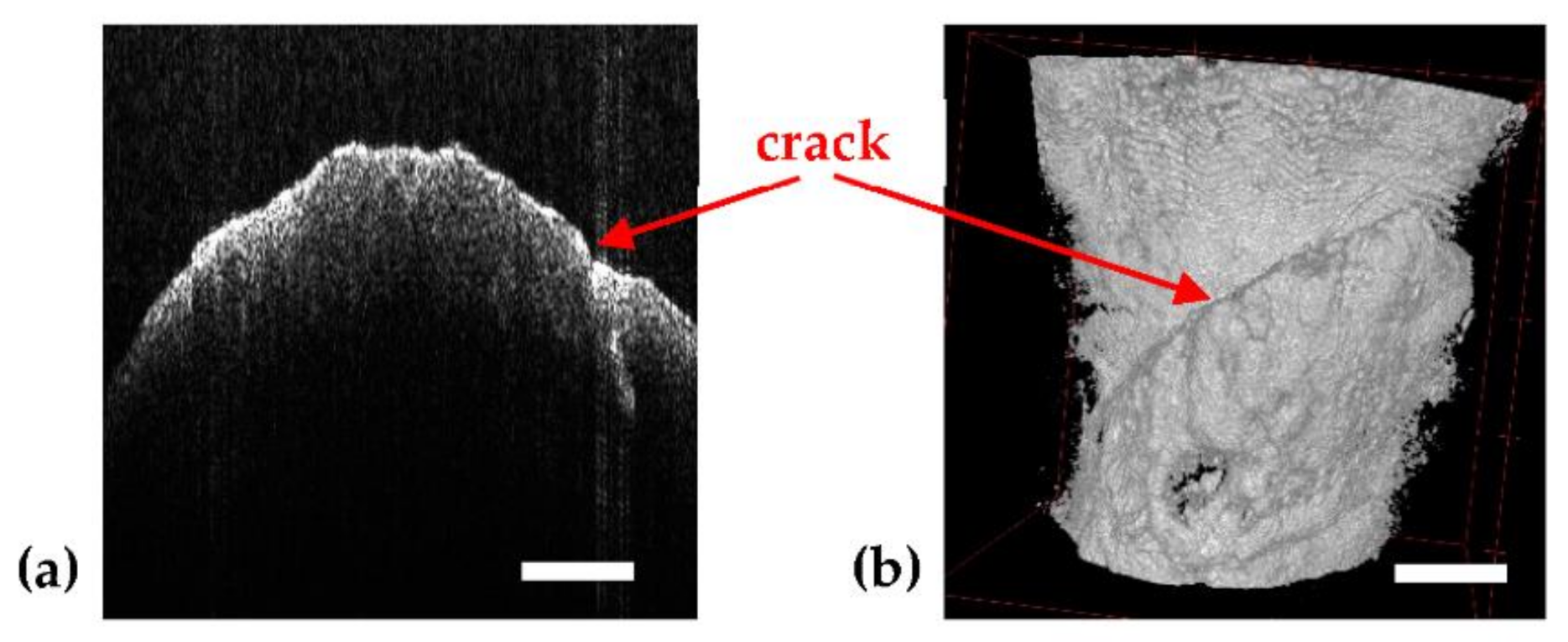
- Because it is using IR laser radiation, OCT does not penetrate metals, although studies of their roughness can be made [46] and, as shown in Figure 4, OCT can provide images near dental crowns, while 3D CBCT for example cannot achieve such images. Also, we have demonstrated that OCT can replace the gold standard of SEM in the study of metallic fractures [47,48]. Therefore, a subject of future work in our groups refers to OCT studies of metallic parts included in the oral cavity, for example dental implants.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pauwels, R. History of dental radiography: Evolution of 2D and 3D imaging modalities. Med. Phys. Int. J. 2020, 3, 235–277. [Google Scholar]
- Ruprecht, A. Oral and maxillofacial radiology. Then and now. JADA 2008, 139, 139. [Google Scholar] [CrossRef]
- Couceiro, C.P.; Vilella, O.V. 2D/3D Cone-Beam CT images or conventional radiography: Which is more reliable? Dent. Press J. Orthod. 2010, 15, 40–41. [Google Scholar] [CrossRef]
- Barone, S.; Paoli, A.; Razionale, A.V. Creation of 3D Multi-Body Orthodontic Models by Using Independent Imaging Sensors. Sensors 2013, 13, 2033–2050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalessandri, D.; Tonni, I.; Laffranchi, L.; Migliorati, M.; Isola, G.; Visconti, L.; Bonetti, S.; Paganelli, C. 2D vs. 3D Radiological Methods for Dental Age Determination around 18 Years: A Systematic Review. Appl. Sci. 2020, 10, 3094. [Google Scholar] [CrossRef]
- Weiss, R., II; Read-Fuller, A. Cone Beam Computed Tomography in Oral and Maxillofacial Surgery: An Evidence-Based Review. Dent. J. 2019, 7, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franchina, A.; Stefanelli, L.V.; Maltese, F.; Mandelaris, G.A.; Vantaggiato, A.; Pagliarulo, M.; Pranno, N.; Brauner, E.; Angelis, F.D.; Carlo, S.D. Validation of an Intra-Oral Scan Method Versus Cone Beam Computed Tomography Superimposition to Assess the Accuracy between Planned and Achieved Dental Implants: A Randomized In Vitro Study. Int. J. Environ. Res. Public Health 2020, 17, 9358. [Google Scholar] [CrossRef] [PubMed]
- Muruganandhan, J.; Sujatha, G.; Poorni, S.; Srinivasan, M.R.; Boreak, N.; Al-Kahtani, A.; Mashyakhy, M.; Chohan, H.; Bhandi, S.; Raj, A.T.; et al. Comparison of Four Dental Pulp-Capping Agents by Cone-Beam Computed Tomography and Histological Techniques—A Split-Mouth Design Ex Vivo Study. Appl. Sci. 2021, 11, 3045. [Google Scholar] [CrossRef]
- Mikla, V.I.; Rusin, V.I.; Boldizhar, P.A. Advances in imaging from the first X ray images. J. Optoelectron. Adv. Mater. 2012, 14, 559–570. [Google Scholar]
- Fernandez, J.E. Chapter II. Interaction of X-rays with matter. In Microscopical X-ray Fluorescence Analysis; Janssens, K., Adams, F., Rindby, A., Eds.; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 2000; pp. 17–62. [Google Scholar]
- Poppe, B.; Looe, H.K.; Pfaffenberger, A.; Chofor, N.; Eenboom, F.; Sering, M.; Rühmann, A.; Poplawski, A.; Willborn, K. Dose-area product measurements in panoramic dental radiology. Radiat. Prot. Dosim. 2007, 123, 131–134. [Google Scholar] [CrossRef] [Green Version]
- Erdelyi, R.A.; Duma, V.-F. Optimization of radiation doses and patients’ risk in dental radiography. AIP Conf. Proc. 2019, 2071, 1–6. [Google Scholar]
- Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotte, T.; Gregory, K.; Puliafito, C.A.; et al. Optical coherence tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choma, M.A.; Sarunic, M.V.; Yang, C.; Izatt, J.A. Sensitivity advantage of swept-source and Fourier-domain optical coherence tomography. Opt. Express 2003, 11, 2183–2189. [Google Scholar] [CrossRef] [Green Version]
- Drexler, W.; Liu, M.; Kumar, A.; Kamali, T.; Unterhuber, A.; Leitgeb, R.A. Optical coherence tomography today: Speed, contrast, and multimodality. J. Biomed. Opt. 2014, 19, 071412. [Google Scholar] [CrossRef]
- Lu, C.D.; Kraus, M.F.; Potsaid, B.; Liu, J.J.; Choi, W.; Jayaraman, V.; Cable, A.E.; Hornegger, J.; Duke, J.S.; Fujimoto, J.G. Handheld ultrahigh speed swept source optical coherence tomography instrument using a MEMS scanning mirror. Biomed. Opt. Express 2014, 5, 293–311. [Google Scholar] [CrossRef] [Green Version]
- Cogliati, A.; Canavesi, C.; Hayes, A.; Tankam, P.; Duma, V.-F.; Santhanam, A.; Thompson, K.P.; Rolland, J.P. MEMS-based handheld scanning probe for distortion-free images in Gabor-Domain Optical Coherence Microscopy. Opt. Express 2016, 24, 13365–13374. [Google Scholar] [CrossRef]
- Monroy, G.L.; Won, J.; Spillman, D.R.; Dsouza, R.; Boppart, S.A. Clinical translation of handheld optical coherence tomography: Practical considerations and recent advancements. J. Biomed. Opt. 2017, 22, 121715. [Google Scholar] [CrossRef] [Green Version]
- Demian, D.; Duma, V.-F.; Sinescu, C.; Negrutiu, M.L.; Cernat, R.; Topala, F.I.; Hutiu, G.; Bradu, A.; Podoleanu, A.G. Design and testing of prototype handheld scanning probes for optical coherence tomography. J. Eng. Med. 2014, 228, 743–753. [Google Scholar] [CrossRef] [Green Version]
- Duma, V.-F.; Dobre, G.; Demian, D.; Cernat, R.; Sinescu, C.; Topala, F.I.; Negrutiu, M.L.; Hutiu, G.; Bradu, A.; Podoleanu, A.G. Handheld scanning probes for optical coherence tomography. Rom. Rep. Phys. 2015, 67, 1346–1358. [Google Scholar]
- Schneider, H.; Ahrens, M.; Strumpski, M.; Rüger, C.; Häfer, M.; Hüttmann, G.; Theisen-Kunde, D.; Schulz-Hildebrandt, H.; Haak, R. An Intraoral OCT Probe to Enhanced Detection of Approximal Carious Lesions and Assessment of Restorations. J. Clin. Med. 2020, 9, 3257. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.S.; Staninec, M.; Fried, D. Imaging artificial caries under composite sealants and restorations. J. Biomed. Opt. 2004, 9, 1297–1304. [Google Scholar] [CrossRef] [PubMed]
- Turki, A.; Bakhsha, B.; Sadrb, A.; Shimadaa, Y.; Junji Tagamia, B.; Yasunori, S. Non-invasive quantification of resin–dentin interfacial gaps using optical coherence tomography: Validation against confocal microscopy. Dent. Mat. 2011, 27, 915–925. [Google Scholar]
- Monteiro, G.; de Melo, Q.; Montesa, M.A.J.R.; Gomes, A.S.L.; Motac, C.B.O.; Sérgio, L.; Freitas, A.Z. Marginal analysis of resin composite restorative systems using optical coherence tomography. Dent. Mat. 2011, 27, 213–223. [Google Scholar] [CrossRef] [PubMed]
- Isfeld, D.M.; Aparicio, C.; Jones, R.S. Assessing near infrared optical properties of ceramic orthodontic brackets using cross-polarization optical coherence tomography. J. Biomed. Mater. Res. B Appl. Biomater. 2014, 102, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Sinescu, C.; Bradu, A.; Duma, V.-F.; Topala, F.; Negrutiu, M.L.; Podoleanu, A. Effects of the temperature variations in the technology of metal ceramic dental prostheses: Non-destructive detection using optical coherence tomography. Appl. Sci. 2017, 7, 552. [Google Scholar] [CrossRef] [Green Version]
- Duma, V.-F.; Sinescu, C.; Bradu, A.; Podoleanu, A. Optical Coherence Tomography Investigations and Modeling of the Sintering of Ceramic Crowns. Materials 2019, 12, 947. [Google Scholar] [CrossRef] [Green Version]
- Erdelyi, R.-A.; Duma, V.-F.; Sinescu, C.; Dobre, G.M.; Bradu, A.; Podoleanu, A. Dental Diagnosis and Treatment Assessments: Between X-rays Radiography and Optical Coherence Tomography. Materials 2020, 13, 4825. [Google Scholar] [CrossRef]
- Hsieh, Y.-S.; Ho, Y.-C.; Lee, S.-Y.; Chuang, C.-C.; Tsai, J.-C.; Lin, K.-F.; Sun, C.-W. Dental Optical Coherence Tomography. Sensors 2013, 13, 8928–8949. [Google Scholar] [CrossRef] [Green Version]
- Lai, Y.-C.; Lin, J.-Y.; Yao, C.-Y.; Lyu, D.-Y.; Lee, S.-Y.; Chen, K.-W.; Chen, I.-Y. Interactive OCT-Based Tooth Scan and Reconstruction. Sensors 2019, 19, 4234. [Google Scholar] [CrossRef] [Green Version]
- Luong, M.N.; Shimada, Y.; Araki, K.; Yoshiyama, M.; Tagami, J.; Sadr, A. Diagnosis of Occlusal Caries with Dynamic Slicing of 3D Optical Coherence Tomography Images. Sensors 2020, 20, 1659. [Google Scholar] [CrossRef] [Green Version]
- Schneider, H.; Park, K.-J.; Häfer, M.; Rüger, C.; Schmalz, G.; Krause, F.; Schmidt, J.; Ziebolz, D.; Haak, R. Dental Applications of Optical Coherence Tomography (OCT) in Cariology. Appl. Sci. 2017, 7, 472. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, L.; Roriz, P.; Simões, J.; Frazão, O. New Trends in Dental Biomechanics with Photonics Technologies. Appl. Sci. 2015, 5, 1350–1378. [Google Scholar] [CrossRef] [Green Version]
- Mehreen, A.; Duker, J.S. Optical coherence tomography–current and future applications. Curr. Opin. Ophthalmol. 2013, 24, 213–221. [Google Scholar]
- Gambichler, T.; Jaedicke, V.; Terras, S. Optical coherence tomography in dermatology: Technical and clinical aspects. Arch. Derm. Res. 2011, 303, 457–473. [Google Scholar] [CrossRef] [PubMed]
- Kirtane, T.S.; Wagh, M.S. Endoscopic Opicat Coherence Tomography (OCT): Advances in Gastrointestinal Imaging. Gastroenterol. Res. Pract. 2014, 2014, 376367. [Google Scholar] [CrossRef] [PubMed]
- Podoleanu, A.; Bradu, A. Master–slave interferometry for parallel spectral domain interferometry sensing and versatile 3D optical coherence tomography. Opt. Express 2013, 21, 19324–19338. [Google Scholar] [CrossRef]
- Duma, V.-F.; Tankam, P.; Huang, J.; Won, J.J.; Rolland, J.P. Optimization of galvanometer scanning for Optical Coherence Tomography. Appl. Opt. 2015, 54, 5495–5507. [Google Scholar] [CrossRef] [PubMed]
- Duma, V.-F. Laser scanners with oscillatory elements: Design and optimization of 1D and 2D scanning functions. Appl. Math. Model. 2019, 67, 456–476. [Google Scholar] [CrossRef]
- Oancea, R.; Bradu, A.; Sinescu, C.; Negru, R.M.; Negrutiu, M.L.; Antoniac, I.; Duma, V.-F.; Podoleanu, A. Assessment of the sealant/tooth interface using optical coherence tomography. J. Adhes. Sci. Technol. 2015, 29, 49–58. [Google Scholar] [CrossRef]
- Shin, H.S.; Nam, K.C.; Park, H.; Choi, H.U.; Kim, H.Y.; Park, C.S. Effective doses from panoramic radiography and CBCT (cone beam CT) using dose area product (DAP) in dentistry. Dento Maxillo Facial Radiol. 2014, 43, 20130439. [Google Scholar] [CrossRef] [Green Version]
- Ludlow, J.B.; Timothy, R.; Walker, C.; Hunter, R.; Benavides, E.; Samuelson, D.B.; Scheske, M.J. Effective dose of dental CBCT-a meta analysis of published data and additional data for nine CBCT units. Dento Maxillo Facial Radiol. 2015, 44, 20140197. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.-S.; Kim, Y.-H.; Yoon, S.-J.; Kang, B.-C. Reference dose levels for dental panoramic radiography in Gwangju, Korea. Radiat. Prot. Dosim. 2010, 142, 184–190. [Google Scholar] [CrossRef]
- Cohnen, M.; Kemper, J.; Möbes, O.; Pawelzik, J.; Mödder, U. Radiation dose in dental radiology. Eur. Radiol. 2002, 12, 634–637. [Google Scholar] [CrossRef]
- Ngan, D.C.; Kharbanda, O.P.; Geenty, J.P.; Darendeliler, M. Comparison of radiation levels from computed tomography and conventional dental radiographs. Aust. Orthod. J. 2003, 19, 67–75. [Google Scholar] [PubMed]
- Feidenhans, N.A.; Hansen, P.E.; Pilný, L.; Madsen, M.H.; Bissacco, J.; Petersen, C.; Taboryski, R. Comparison of optical methods for surface roughness characterization. Meas. Sci. Technol. 2015, 26, 085208. [Google Scholar] [CrossRef] [Green Version]
- Hutiu, G.; Duma, V.-F.; Demian, D.; Bradu, A.; Podoleanu, A.G. Surface imaging of metallic material fractures using optical coherence tomography. Appl. Opt. 2014, 53, 5912–5916. [Google Scholar] [CrossRef]
- Hutiu, G.; Duma, V.-F.; Demian, D.; Bradu, A.; Podoleanu, A.G. Assessment of Ductile, Brittle, and Fatigue Fractures of Metals Using Optical Coherence Tomography. Metals 2018, 8, 117. [Google Scholar] [CrossRef] [Green Version]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Panoramic Radiographs (Figure 8) | Anode Voltage (kV) | Current Intensity (mA) | Exposure Time (s) | Radiation Dose (µSv) | ||
|---|---|---|---|---|---|---|
| a | 60 | 1 | 13.7 | 0.65 | 0.2 | 4.15 |
| b | 61 | 2 | 15 | 1.74 | 0.34 | 4.1 |
| c | 62 | 3.2 | 15 | 2.89 | 0.3 | 4 |
| d | 64 | 4 | 15 | 3.88 | 0.19 | 3.92 |
| e | 66 | 6.3 | 15 | 6.54 | 0.43 | 3.67 |
| f | 68 | 8 | 15 | 8.84 | 0.36 | 3.57 |
| g | 70 | 10 | 15 | 11.68 | 0.46 | 3.45 |
| h | 72 | 11 | 15 | 13.72 | 0.58 | 3.35 |
|
Panoramic Radiographs (Figure 8) | ||||||
|---|---|---|---|---|---|---|
| a | 3 | 3479 | 2104.47 | 1122.57 | 0.998 | 3.096 |
| b | 17 | 3377 | 2031.94 | 1094.54 | 0.989 | 3.069 |
| c | 20 | 3485 | 2012.62 | 1102.82 | 0.988 | 3.141 |
| d | 32 | 3317 | 1975.26 | 1060.52 | 0.980 | 3.097 |
| e | 31 | 3489 | 2106.08 | 1078.73 | 0.982 | 3.205 |
| f | 22 | 3456 | 2081.59 | 1056.53 | 0.987 | 3.250 |
| g | 70 | 3576 | 2172.58 | 1083.91 | 0.961 | 3.234 |
| h | 18 | 3593 | 2117.34 | 1095.44 | 0.990 | 3.263 |
| 3D CBCT Radiographs (Figure 9) | Anode Voltage (kV) | Current Intensity (mA) | Exposure Time (s) | Radiation Dose (µSv) |
|---|---|---|---|---|
| a | 60 | 1 | 4.95 | 1.25 |
| b | 75 | 8 | 5.09 | 25.87 |
| c | 90 | 14 | 5.08 | 86.37 |
|
3D CBCT (Figure 9) | ||||
|---|---|---|---|---|
| a | 552 | 2808 | 1680 | 0.67 |
| b | 302 | 2802 | 1552 | 0.8 |
| c | 296 | 3032 | 1664 | 0.82 |
| Diameter of Image Base (mm) | Image Height (mm) | Voxel Side (µm) | Anode Voltage (kV) | Current Intensity (mA) | Exposure Time (s) | ||
|---|---|---|---|---|---|---|---|
| Before | 80 | 200 | 84 | 14 | 12.057 | 1170 | |
| After | 80 | 150 | 90 | 14 | 5.072 | 691 |
| Radiograph | Characteristics | Planmeca | Soredex | |
|---|---|---|---|---|
| Panoramic | Anode voltage (kV) | 68 to 73 | 70 to 75 | |
| Current intensity (mA) | 8 to 11 | 8 to 11 | ||
| Exposure time (s) | 14.990 | 16 | ||
| DAP (mGy×cm2) | 97 to 117 | 175 to 250 | ||
| Effective Dose (µSv) | 7.8 to 9.2 | 14 to 20 | ||
| Pixel side (µm) | 127 | 100 | ||
| Total 3D CBCT | Anode voltage (kV) | 90 | 85 to 90 | |
| Current intensity (mA) | 11 to 14 | 6 to 10 | ||
| Exposure time (s) | 5 | 6 to 9 | ||
| DAP (mGy×cm2) | 691* | 749.5 ** | ||
| Effective Dose (µSv) | 86.4* | 93.7 ** | ||
| Voxel side (µm) | 150 | 200 | ||
| Base diameter (mm) | of the investigated volume | 110 | 150 | |
| Height (mm) | 80 | 80 | ||
| Segmental 3D CBCT | Anode voltage (kV) | 90 | 85 to 90 | |
| Current intensity (mA) | 11 to 14 | 6 to 10 | ||
| Exposure time (s) | 5 | 6 to 9 | ||
| DAP (mGy×cm2) | 329 * | 140 to 300 ** | ||
| Effective Dose (µSv) | 32.9 to 49.35 | 20 to 30 ** | ||
| Voxel side (µm) | 150 | 200 | ||
| Base diameter (mm) | of the investigated volume | 50 | 50 | |
| Height (mm) | 50 | 50 | ||
| Maxillary/mandible 3D CBCT | Anode voltage (kV) | 90 | 85 to 90 | |
| Current intensity (mA) | 11 to 14 | 6 to 10 | ||
| Exposure time (s) | 5 | 6 to 9 | ||
| DAP (mGy×cm2) | 429 * | 400 ± 50 ** | ||
| Effective Dose (µSv) | 42.9 to 64.35 | 40 ± to 60 ± ** | ||
| Voxel side (µm) | 150 | 200 | ||
| Base diameter (mm) | of the investigated volume | 110 | 61 | |
| Height (mm) | 50 | 78 | ||
| Method | Equipment | Advantages and Disadvantages |
|---|---|---|
| Panoramic | Planmeca and Soredex | Radiation dose is almost 50% smaller for Planmeca. Resolution is lower (127 µm) for Planmeca than for Soredex (100 µm). Images produced by Soredex have a lower contrast and sharpness even if they have better resolutions. |
| 3D CBCT | Planmeca and Soredex | Smaller exposure time (5 versus 9 s), smaller radiation dose (with at least 10 µSv), and smaller voxel side (with 25%) for Planmeca, which means better resolution, contrast, and image quality. The covered volume is larger for Soredex. |
| OCT | SS-OCT | Better resolution, usually, around 10 µm axial (i.e., in depth), but it can be as low as 2 µm [17]. Lateral resolution (i.e., on the sample surface) is adjustable by galvanometer scanners programming; in this study it was set to 6 µm (corresponding to 500 B-scans for a scan length of 3 mm) or to 10 µm (for 500 B-scans per 5 mm). In contrast, the smallest achievable linear resolution (on each spatial direction) for 3D CBCT is 75 µm. Low penetration depth, but no ionizing radiation for OCT. The maximum volume scanned with OCT is 5 × 5 × 2 mm, while for radiography the volume corresponds at least to a cylinder with the base diameter of 50 mm and the height of 50 mm. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erdelyi, R.-A.; Duma, V.-F.; Sinescu, C.; Dobre, G.M.; Bradu, A.; Podoleanu, A. Optimization of X-ray Investigations in Dentistry Using Optical Coherence Tomography. Sensors 2021, 21, 4554. https://0-doi-org.brum.beds.ac.uk/10.3390/s21134554
Erdelyi R-A, Duma V-F, Sinescu C, Dobre GM, Bradu A, Podoleanu A. Optimization of X-ray Investigations in Dentistry Using Optical Coherence Tomography. Sensors. 2021; 21(13):4554. https://0-doi-org.brum.beds.ac.uk/10.3390/s21134554
Chicago/Turabian StyleErdelyi, Ralph-Alexandru, Virgil-Florin Duma, Cosmin Sinescu, George Mihai Dobre, Adrian Bradu, and Adrian Podoleanu. 2021. "Optimization of X-ray Investigations in Dentistry Using Optical Coherence Tomography" Sensors 21, no. 13: 4554. https://0-doi-org.brum.beds.ac.uk/10.3390/s21134554