
Development of a Finger-Ring-Shaped Hybrid Smart Stethoscope for Automatic S1 and S2 Heart Sound Identification



Abstract
:1. Introduction
2. Methods
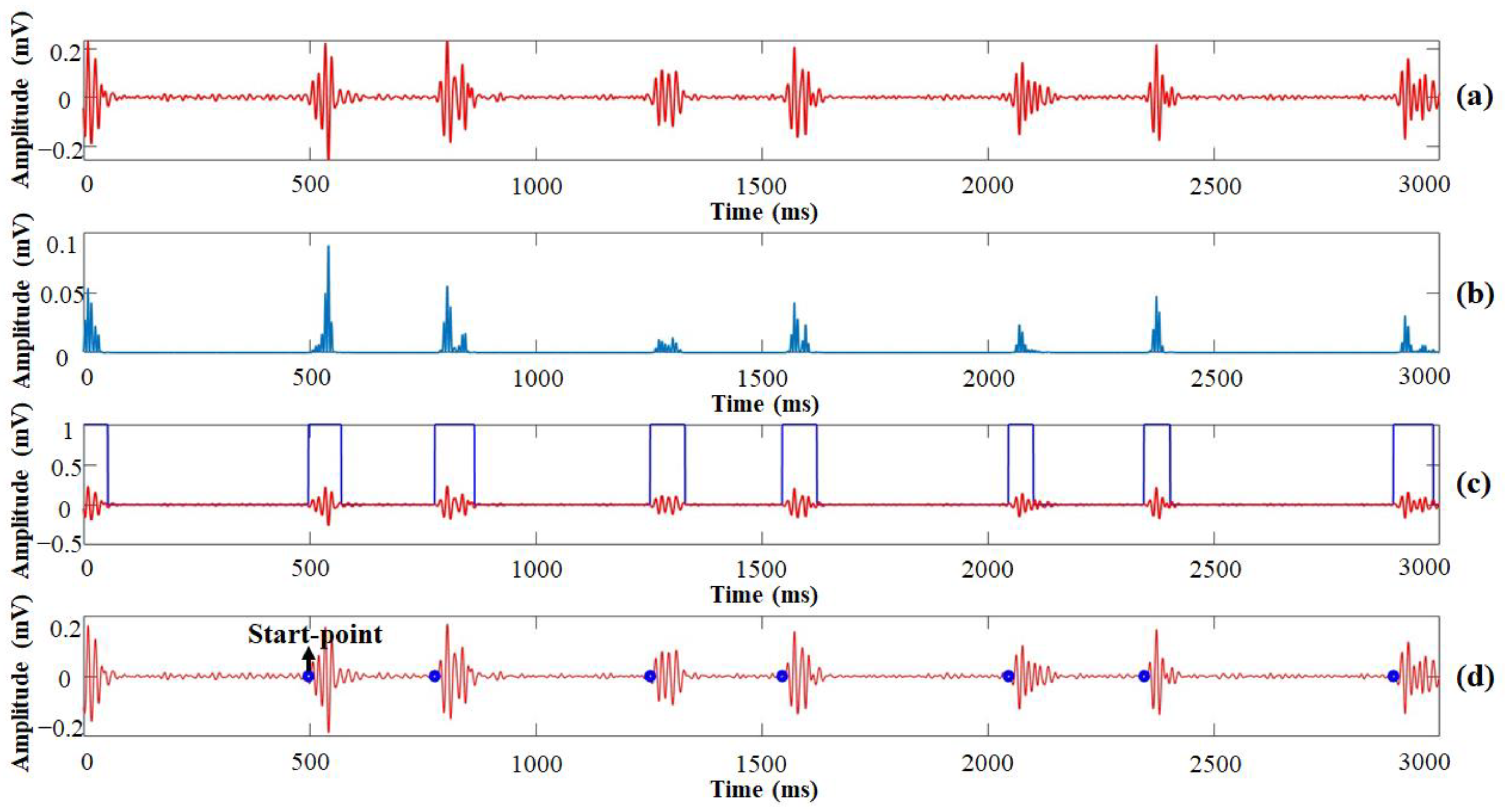
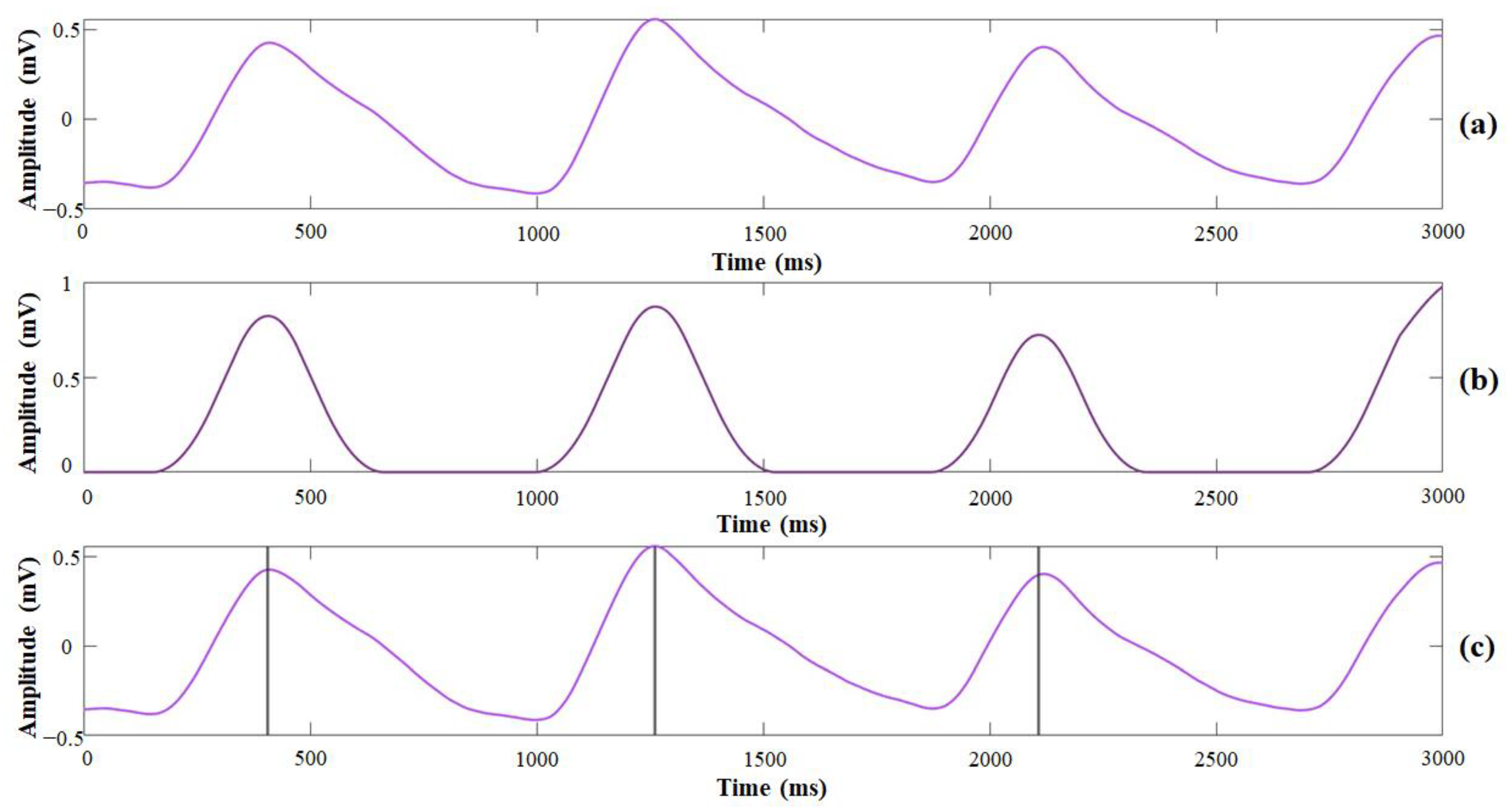
2.1. Development of the Automatic Heart-Sound-Analysis Algorithm
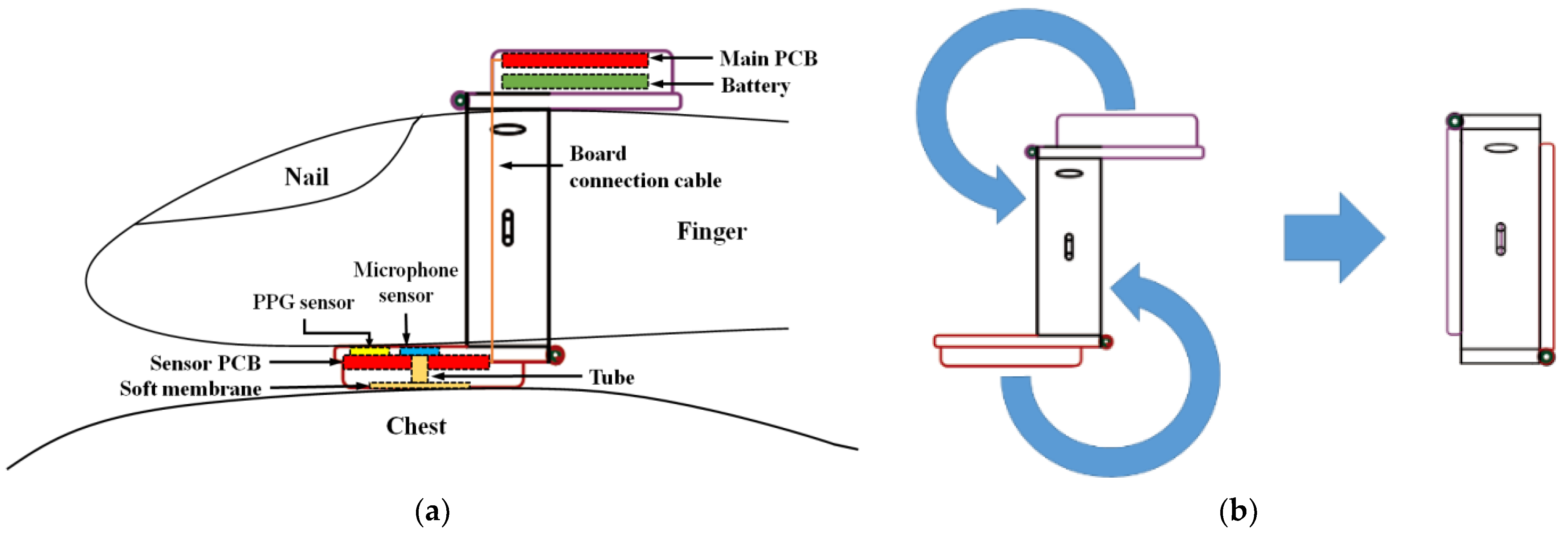
2.2. Embedded System Design of the Proposed Finger-Ring-Shaped Hybrid Smart Stethoscope
3. Materials and Experiment
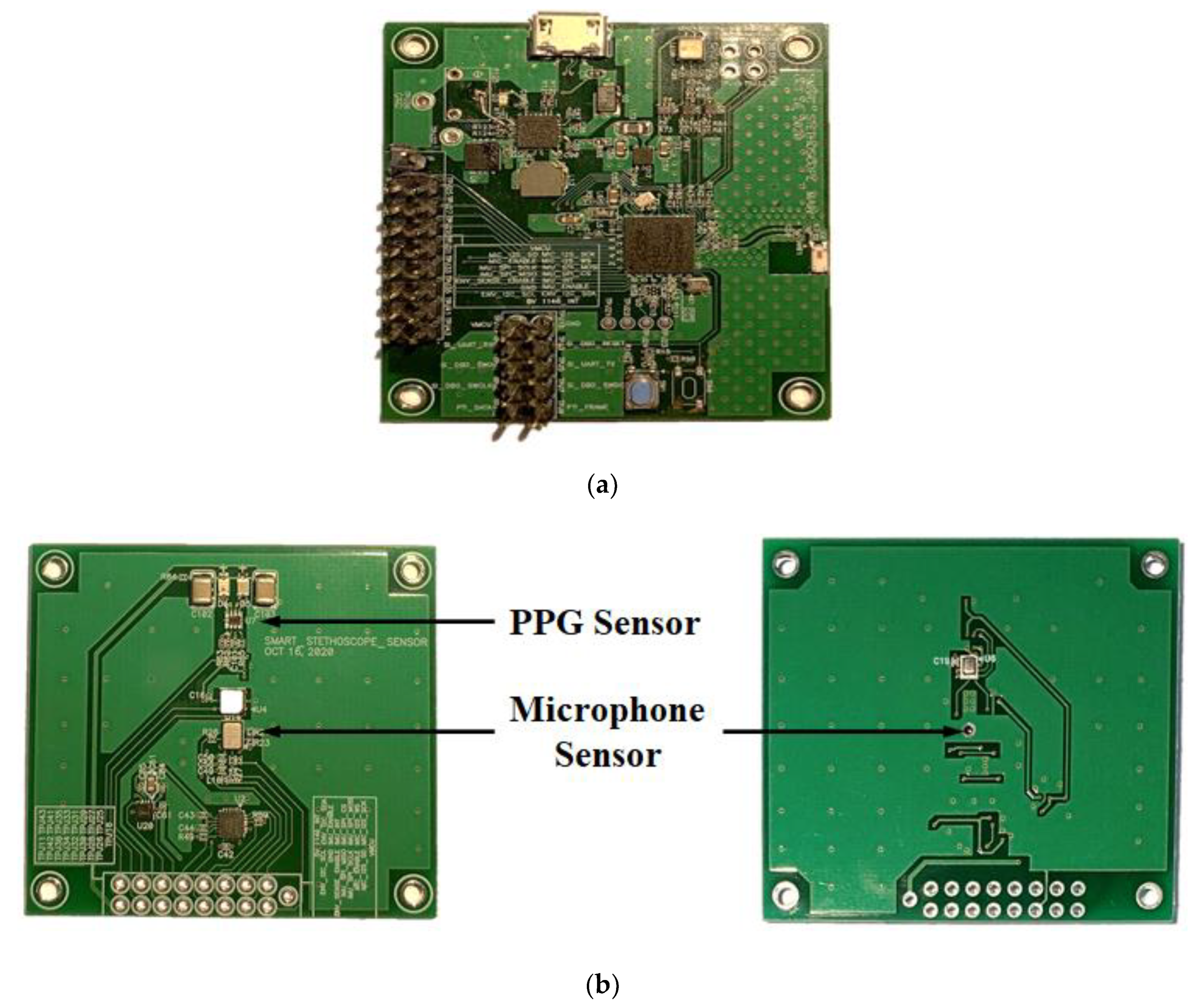
3.1. Design and PCG Manufacture
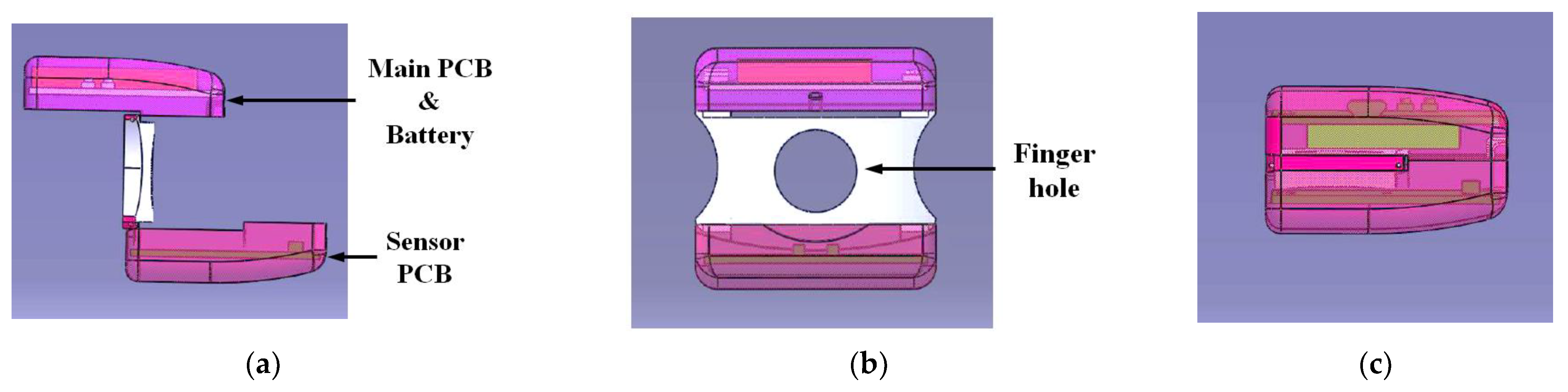
3.2. Case Design and Prototype Assembly
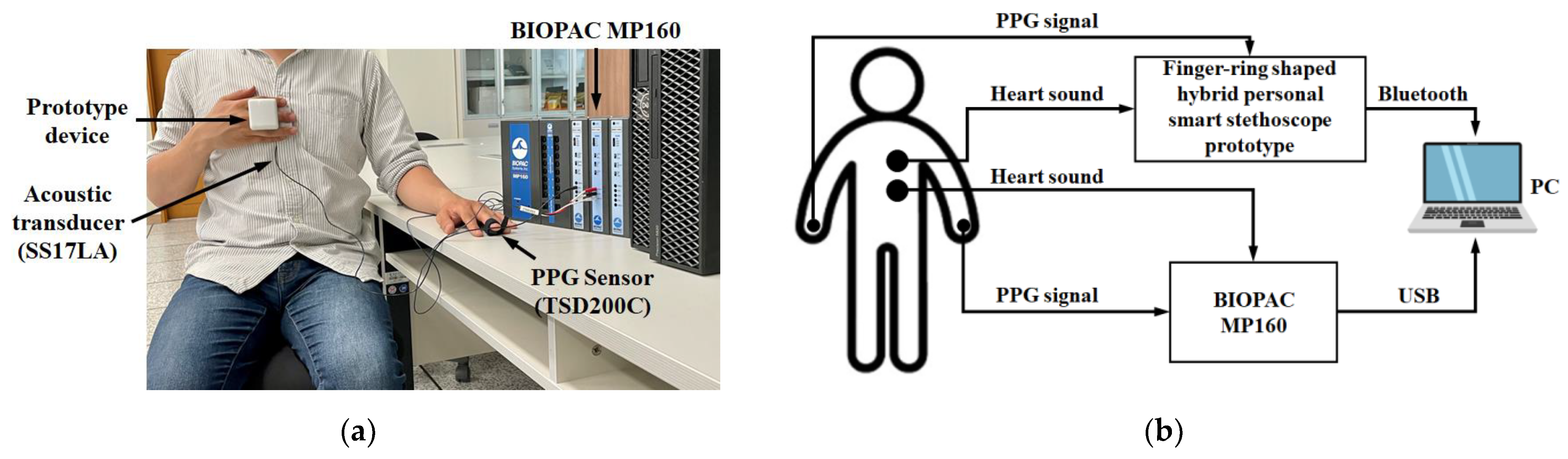
3.3. Experiment to Test the Performance of the Proposed Smart Stethoscope
4. Results and Discussion
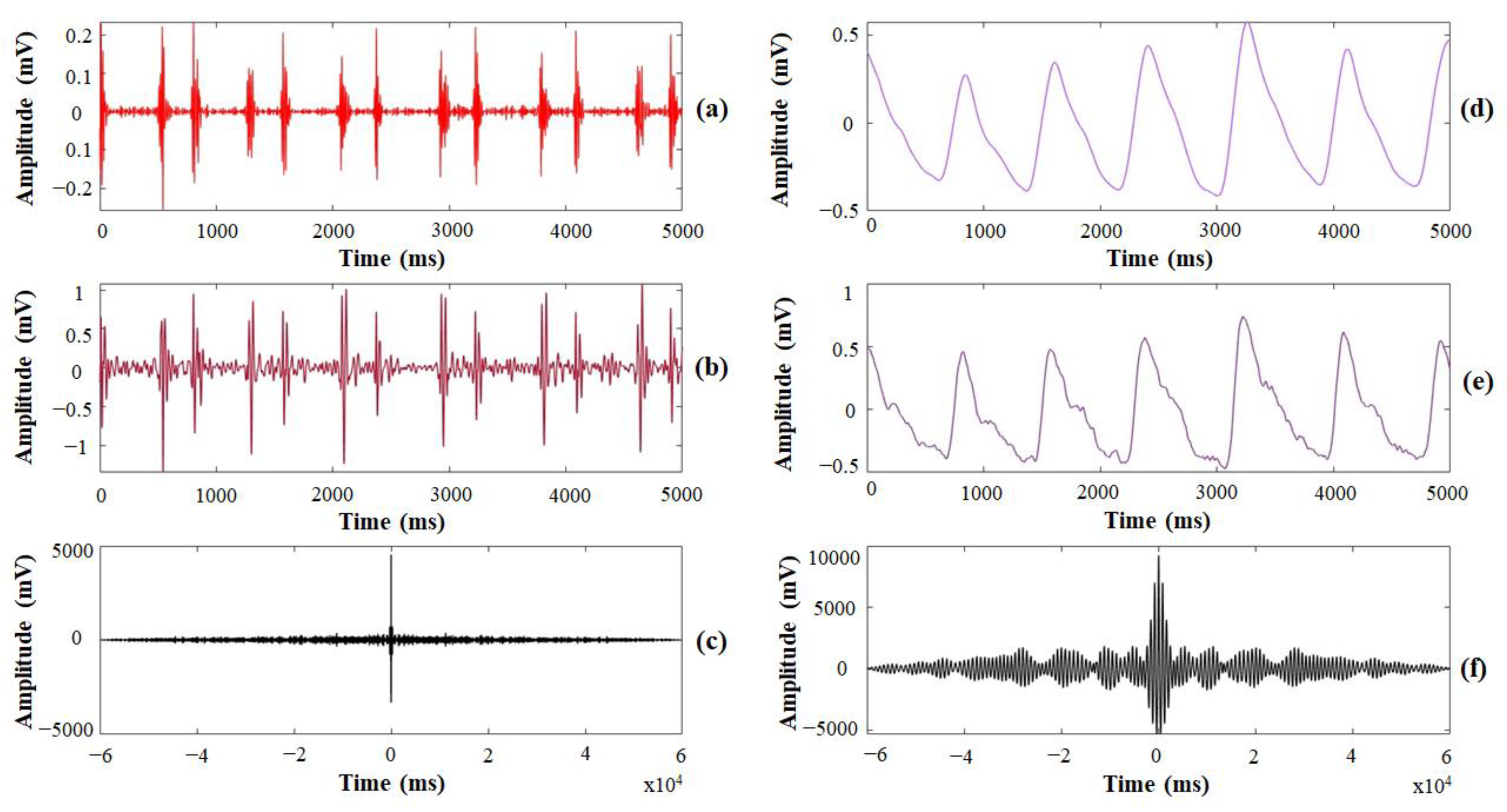
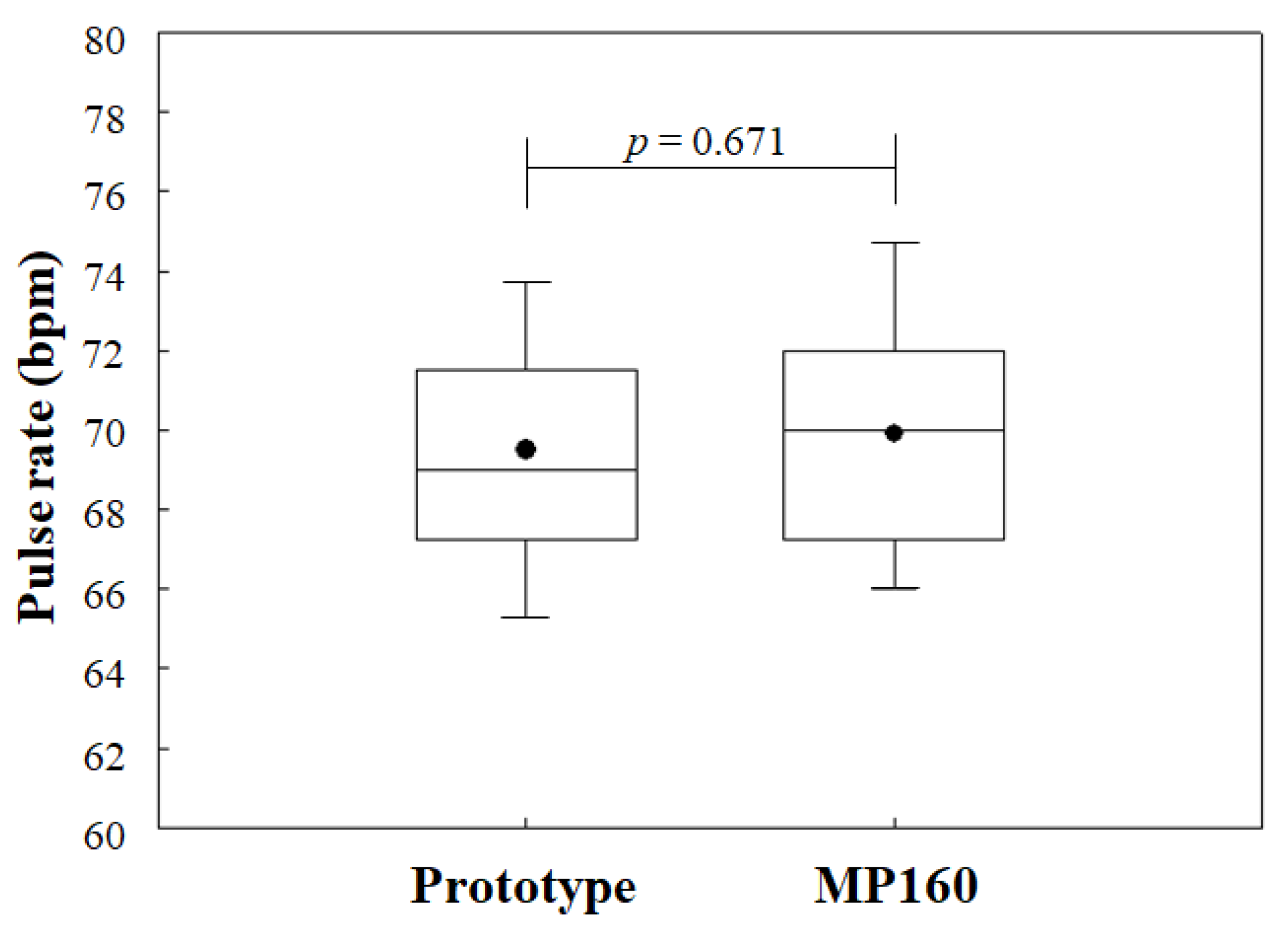
4.1. Results of PCG and PPG Detection
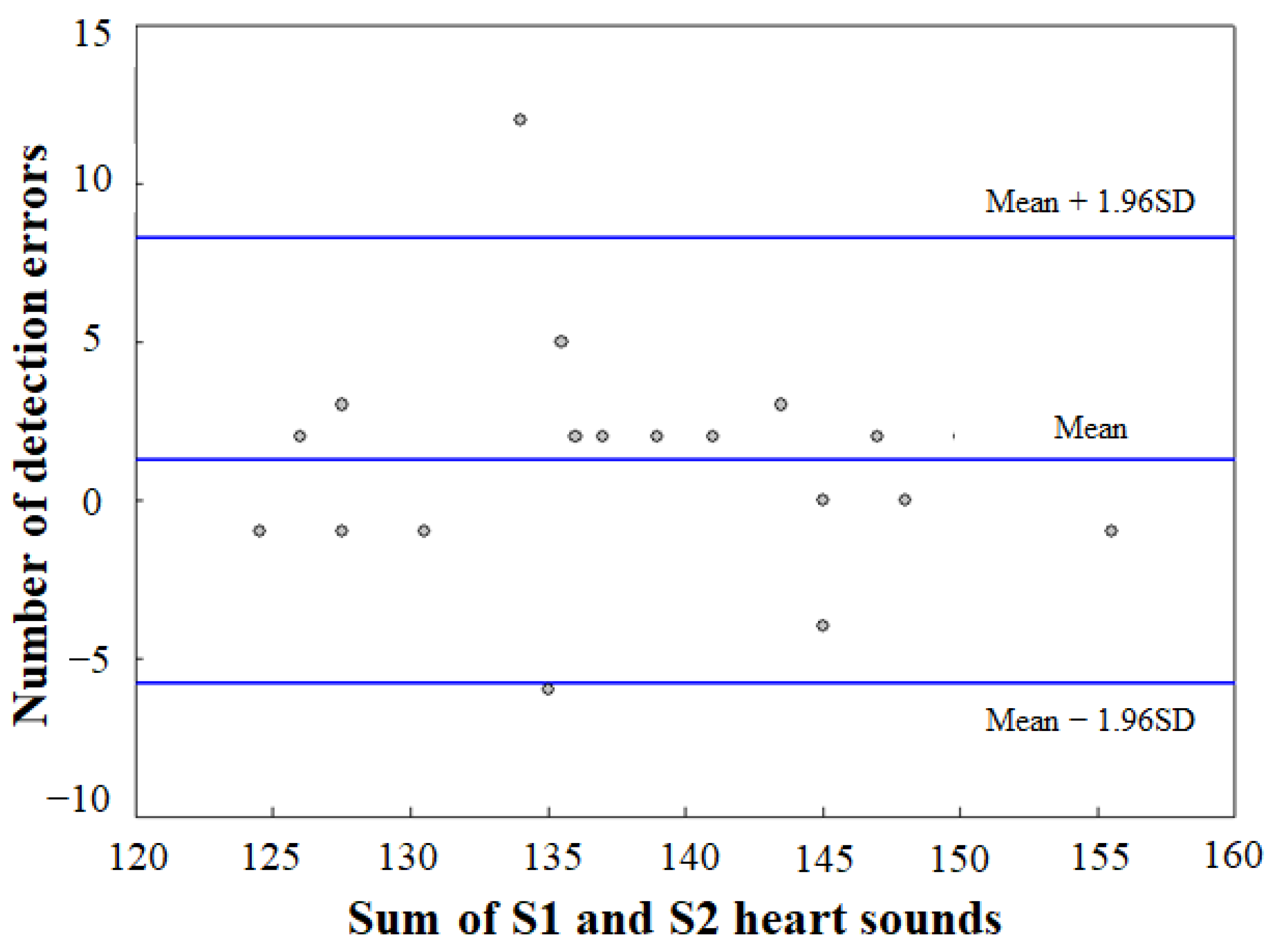
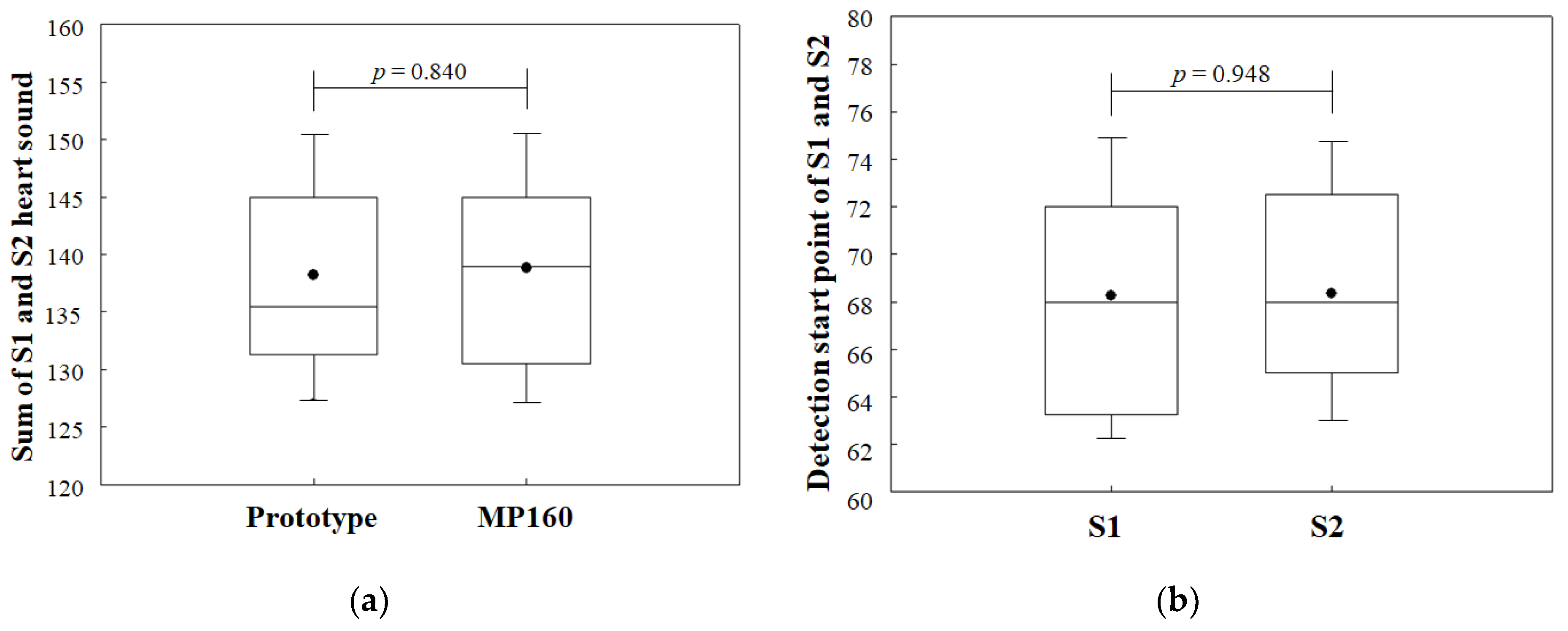
4.2. Automatic Identification of S1 and S2 Heart Sounds
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 9 December 2020).
- Wang, J.G.; Shi, X.B.; Wang, P.; He, W.; Dai, C.L. Remote heart sound monitoring system. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2006; pp. 2138–2140. [Google Scholar]
- Rubins, U.; Grabovskis, A.; Grube, J.; Kukulis, I. Photoplethysmography analysis of artery properties in patients with cardiovascular diseases. In Proceedings of the 14th Nordic-Baltic Conference on Biomedical Engineering and Medical Physics, Riga, Latvia, 16–20 June 2008; pp. 319–322. [Google Scholar]
- Denes, P.; Larson, J.C.; Lloyd-Jones, D.M.; Prineas, R.J.; Greenland, P. Major and minor ECG abnormalities in asymptomatic women and risk of cardiovascular events and mortality. JAMA 2007, 297, 978–985. [Google Scholar] [CrossRef]
- Appel, L.J.; Stason, W.B. Ambulatory blood pressure monitoring and blood pressure self-measurement in the diagnosis and management of hypertension. Ann. Intern. Med. 1993, 118, 867–882. [Google Scholar] [CrossRef]
- Healio Learn the Heart. Heart Sounds Topic Review. Available online: https://0-www-healio-com.brum.beds.ac.uk/cardiology/learn-the-heart/cardiology-review/topic-reviews/heart-sounds (accessed on 29 April 2015).
- Stein, P.D.; Sabbah, H.N.; Lakier, J.; Magilligan, D.J., Jr.; Gold-stein, D. Frequency of the first heart sound in the assessment of stiffening of mitral bioprosthetic valves. Circulation 1981, 63, 200–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Son, G.Y.; Kwon, S. Classification of heart sound signal using multiple features. Appl. Sci. 2018, 8, 2344. [Google Scholar]
- Mangione, S.; Nieman, L.Z. Cardiac auscultatory skills of internal medicine and family practice trainees: A comparison of diagnostic proficiency. JAMA 1997, 278, 717–722. [Google Scholar] [CrossRef] [PubMed]
- 3M™ Science Applied to Life, 3M™ Littmann® CORE Digital Stethoscope, 8480, Black Chestpiece, Tube, Stem and Headset, 27inch. Available online: https://www.3m.com/3M/en_US/p/d/v101191252/ (accessed on 4 April 2021).
- SMART SOUND, SKEEPER. Available online: http://www.ismartsound.com/skeeper-2/ (accessed on 20 January 2021).
- M3DICINE, Stethee Pro. Available online: https://www.m3dicine.com/ (accessed on 20 January 2021).
- Lehner, R.J.; Rangayyan, R.M. A three-channel microcomputer system for segmentation and characterization of the phonocardiogram. IEEE Trans. Biomed. Eng. 1987, 6, 485–489. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Zhao, H.; Ju, K.H.; Shin, K.S.; Lee, M.H.; Shelley, K.; Chon, K.H. Can photoplethysmography variability serve as an alternative approach to obtain heart rate variability information? J. Clin. Monit. Comput. 2008, 22, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Babu, K.A.; Ramkumar, B.; Manikandan, M.S. Real-time detection of S2 sound using simultaneous recording of PCG and PPG. In Proceedings of the TENCON 2017–2017 IEEE Region 10 Conference, Penang, Malaysia, 21 December 2017; pp. 1475–1480. [Google Scholar]
- Babu, K.A.; Ramkumar, B.; Manikandan, M.S. Automatic identification of S1 and S2 heart sounds using simultaneous PCG and PPG recordings. IEEE Sens. J. 2018, 18, 9430–9440. [Google Scholar] [CrossRef]
- Tom, E.M. A survey into paramedic accuracy in identifying the correct anatomic locations for cardiac auscultation. Br. Paramed. J. 2017, 2, 13–17. [Google Scholar]
- Dragomiretskiy, K.; Zosso, D. Variational mode decomposition. IEEE Trans. Signal Process. 2013, 62, 531–544. [Google Scholar] [CrossRef]
- Babu, K.A.; Ramkumar, B.; Manikandan, M.S. S1 and S2 heart sound segmentation using variational mode decomposition. In Proceedings of the TENCON 2017–2017 IEEE Region 10 Conference, Penang, Malaysia, 21 December 2017; pp. 1629–1634. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Target Heart Rate and Estimated Maximum Heart Rate. Available online: https://www.cdc.gov/physicalactivity/basics/measuring/heartrate.htm (accessed on 14 October 2020).
- Esmaili, A.; Kachuee, M.; Shabany, M. Nonlinear cuffless blood pressure estimation of healthy subjects using pulse transit time and arrival time. IEEE Trans. Instrum. Meas. 2017, 66, 3299–3308. [Google Scholar] [CrossRef] [Green Version]
- Tahar, O.; Nadia, O.; Redouane, B.; Nabil, D.; Fethi, B.R. New parameter available in phonocardiogram for blood pressure estimation. In Proceedings of the 6th International Work-Conference on Bioinformatics and Biomedical Engineering, Granada, Spain, 25–27 April 2018; pp. 301–310. [Google Scholar]
- Rajala, S.; Ahmaniemi, T.; Lindholm, H.; Taipalus, T. Pulse arrival time (PAT) measurement based on arm ECG and finger PPG signals-comparison of PPG feature detection methods for PAT calculation. In Proceedings of the 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Korea, 11–15 July 2017; pp. 250–253. [Google Scholar]
- Moraes, J.L.; Rocha, M.X.; Vasconcelos, G.G.; Vasconcelos Filho, J.E.; De Albuquerque, V.H.C.; Alexandria, A.R. Advances in photopletysmography signal analysis for biomedical applications. Sensors 2018, 18, 1894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsiao, C.C.; Horng, J.; Lee, R.G.; Lin, R. Design and implementation of auscultation blood pressure measurement using vascular transit time and physiological parameters. In Proceedings of the 2017 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Banff, AB, Canada, 5–8 October 2017; pp. 2996–3001. [Google Scholar]
- Shervegar, M.V.; Bhat, G.V. Automatic segmentation of phonocardiogram using the occurrence of the cardiac events. Inform. Med. Unlocked 2017, 9, 6–10. [Google Scholar] [CrossRef]
- Wang, X.; Li, Y.; Sun, C.; Liu, C. Detection of the first and second heart sound using heart sound energy. In Proceedings of the 2009 2nd International Conference on Biomedical Engineering and Informatics, Tianjin, China, 17–19 October 2009; pp. 1–4. [Google Scholar]
- Giordano, N.; Knaflitz, M. A novel method for measuring the timing of heart sound components through digital phonocardiography. Sensors 2019, 19, 1868. [Google Scholar] [CrossRef] [PubMed] [Green Version]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Signal Group | Heart Sounds | PPG Signals | ||
|---|---|---|---|---|
| Mean | Std. | Mean | Std. | |
| Original | 0.98 | 0.02 | 0.96 | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Wei, Q.; Park, H.; Na, Y.; Jeong, D.; Lim, H. Development of a Finger-Ring-Shaped Hybrid Smart Stethoscope for Automatic S1 and S2 Heart Sound Identification. Sensors 2021, 21, 6294. https://0-doi-org.brum.beds.ac.uk/10.3390/s21186294
Lee S, Wei Q, Park H, Na Y, Jeong D, Lim H. Development of a Finger-Ring-Shaped Hybrid Smart Stethoscope for Automatic S1 and S2 Heart Sound Identification. Sensors. 2021; 21(18):6294. https://0-doi-org.brum.beds.ac.uk/10.3390/s21186294
Chicago/Turabian StyleLee, Soomin, Qun Wei, Heejoon Park, Yuri Na, Donghwa Jeong, and Hongjoon Lim. 2021. "Development of a Finger-Ring-Shaped Hybrid Smart Stethoscope for Automatic S1 and S2 Heart Sound Identification" Sensors 21, no. 18: 6294. https://0-doi-org.brum.beds.ac.uk/10.3390/s21186294