
Can Frailty Be a Predictor of ICD Shock after the Implantation of a Cardioverter Defibrillator in Elderly Patients?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.2. Study Participants and Selection
2.3. Ethical Considerations
2.4. Research Instruments
2.5. Statistical Analysis
3. Results
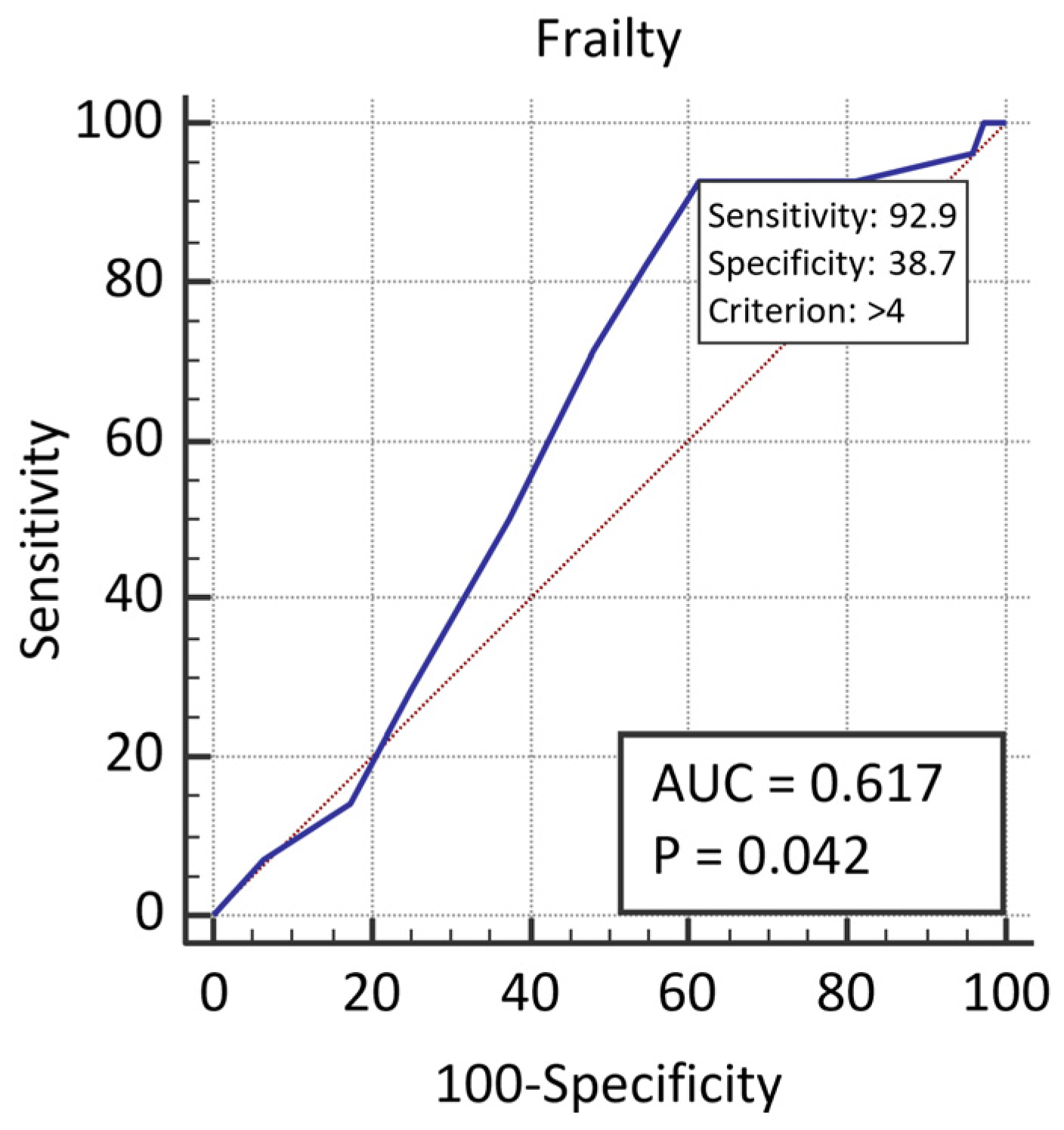
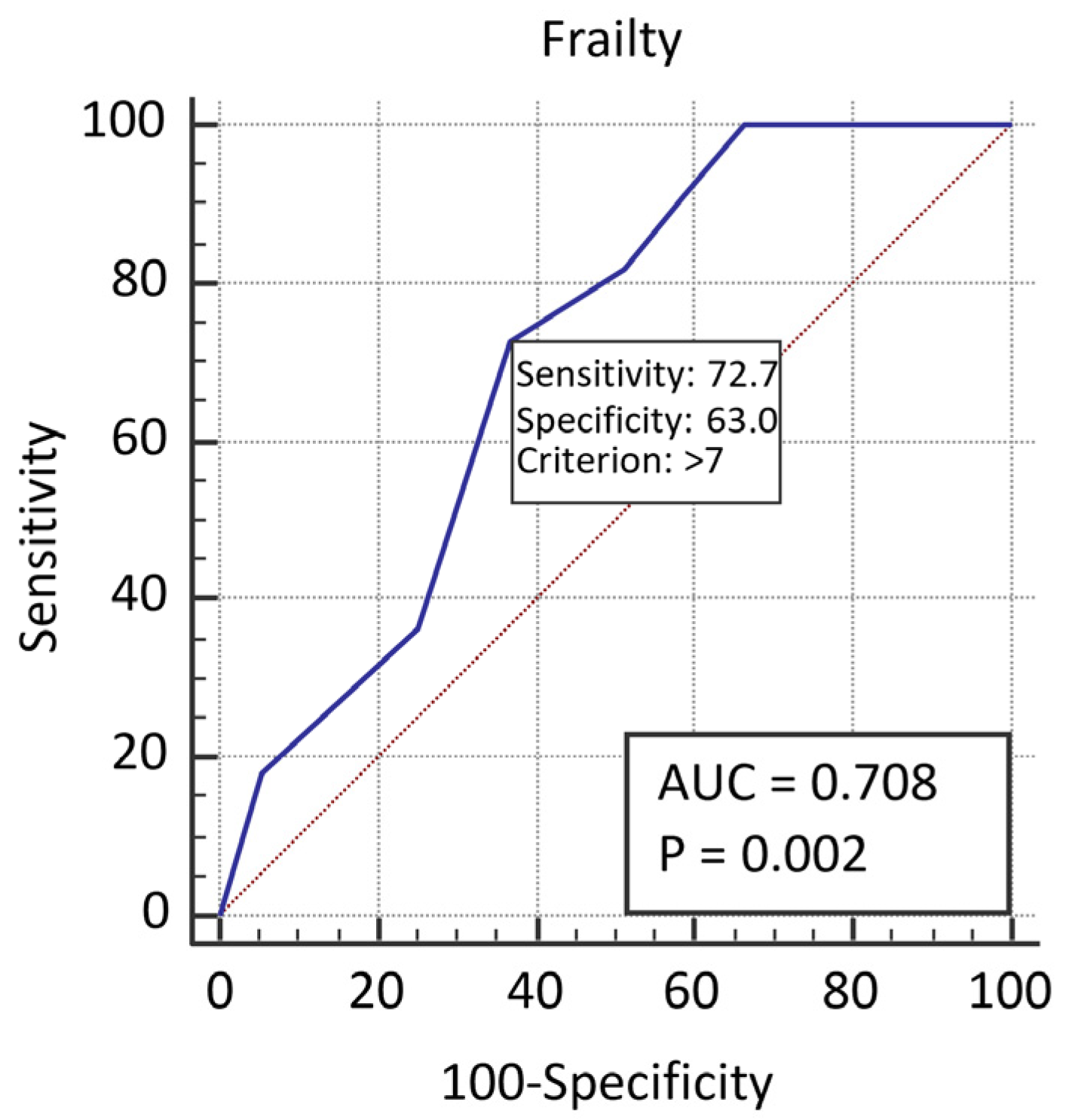
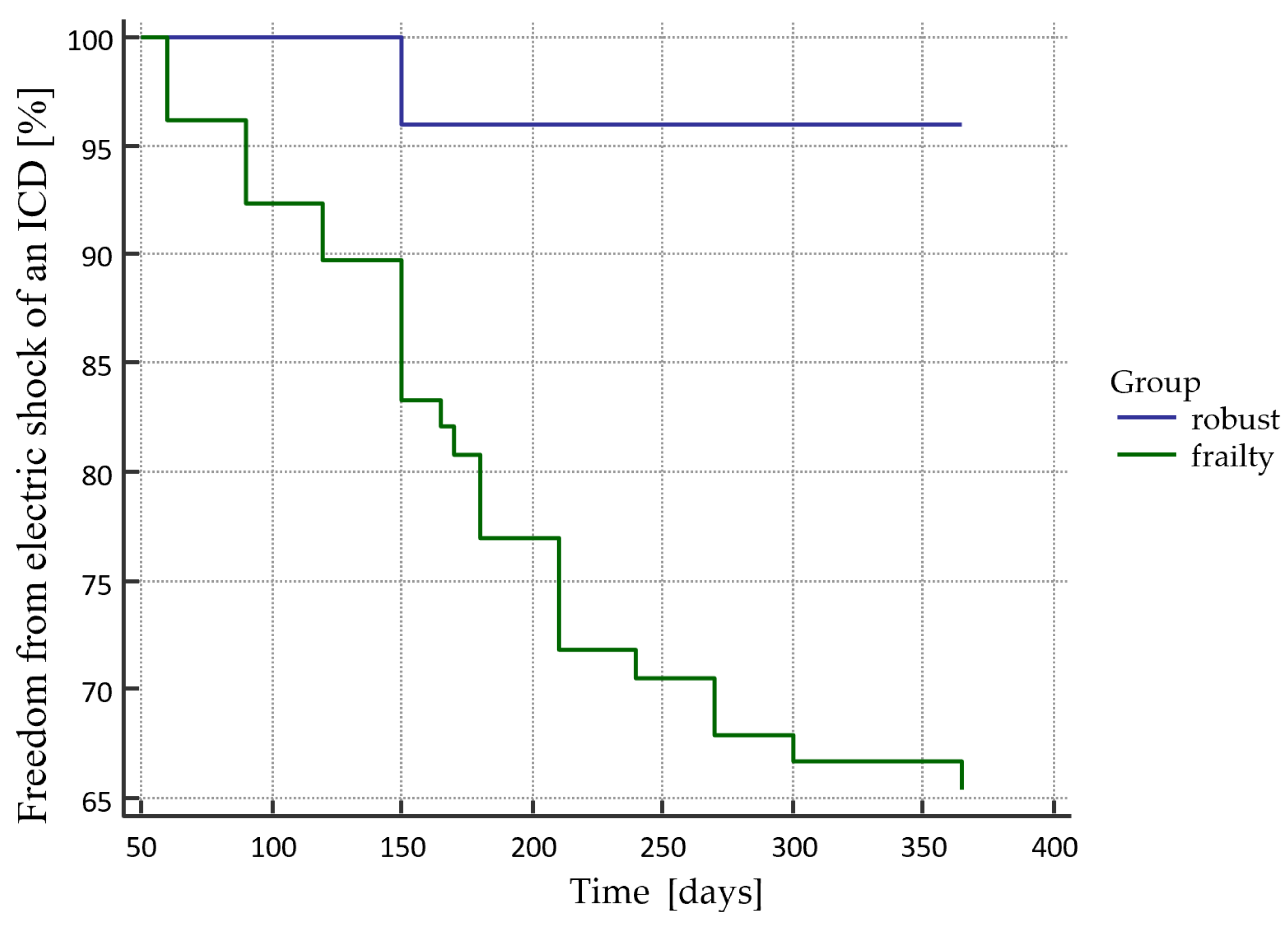
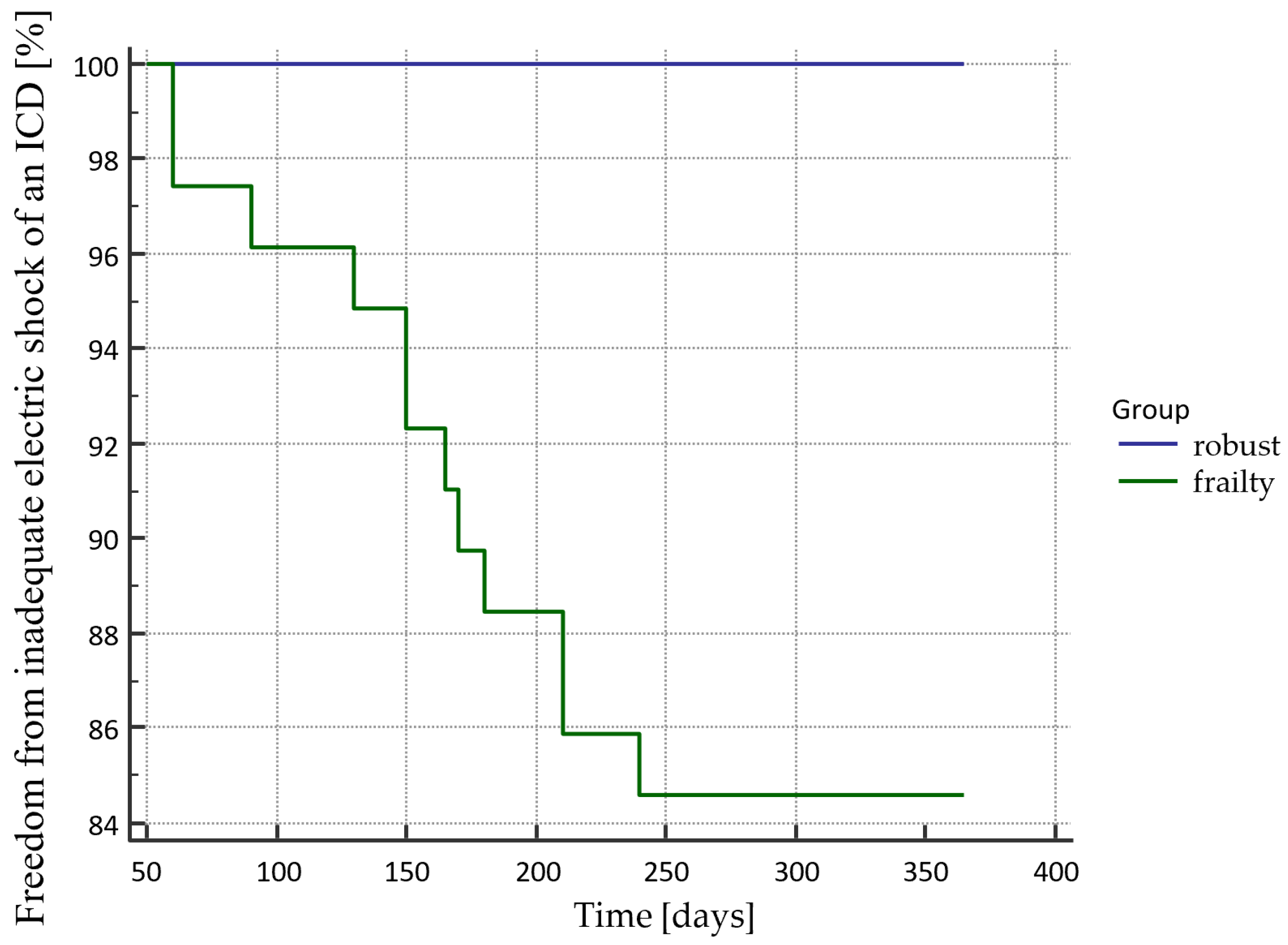
Endpoint Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goldstein, N.; Carlson, M.; Livote, E.; Kutner, J.S. Brief communication: Management of implantable cardioverter-defibrillators in hospice: A nationwide survey. Ann. Intern. Med. 2010, 152, 296–299. [Google Scholar] [CrossRef]
- Priori, S.G.; Blomström-Lundqvist, C.; Mazzanti, A.; Blom, N.; Borggrefe, M.; Camm, J.; Elliott, P.; Fitzsimons, D.; Hatala, R.; Hindricks, G.; et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Europace 2015, 17, 1601–1687. [Google Scholar] [CrossRef] [PubMed]
- Gradaus, R.; Block, M.; Brachmann, J.; Breithardt, G.; Huber, H.G.; Jung, W.; Kranig, W.; Mletzko, R.U.; Schoels, W.; Seidl, K.; et al. Mortality, Morbidity, and Complications in 3,344 Patients with Implantable Cardioverter Defibrillators: Esults From the German ICD Registry EURID. Pacing Clin. Electrophysiol. 2003, 26, 1511–1518. [Google Scholar] [CrossRef]
- Van der Velden, L.B.; Huybrechts, W.; Adriaensens, B.; Ector, J.; Ector, H.; Willems, R.; Heidbüchel, H. Appropriate and inappropriate implantable cardioverter defibrillator interventions during secondary prevention. Acta Cardiol. 2008, 63, 39–45. [Google Scholar] [CrossRef]
- Almendral, J.; Arribas, F.; Wolpert, C.; Ricci, R.; Adragao, P.; Cobo, E.; Navarro, X.; Quesada, A.; the DATAS Steering Committee and Writing Committee on behalf of the DATAS Investigators. Dual-chamber defibrillators reduce clinically significant adverse events compared with single-chamber devices: Results from the DATAS (Dual chamber and Atrial Tachyarrhythmias Adverse events Study) trial. Europace 2008, 10, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Berenbom, L.D.; Weiford, B.C.; Vacek, J.L.; Emert, M.P.; Hall, W.J.; Andrews, M.L.; McNitt, S.; Zareba, W.; Moss, A.J. Differences in outcomes between patients treated with single- versus dual-chamber implantable cardioverter defibrillators: A substudy of the Multicenter Automatic Defibrillator Implantation Trial II. Ann. Noninvasive Electrocardiol. 2005, 10, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Wathen, M.S.; Sweeney, M.O.; DeGroot, P.J.; Stark, A.J.; Koehler, J.L.; Chisner, M.B.; Machado, C.; Adkisson, W.O.; for the PainFREE Investigators. Shock Reduction Using Antitachycardia Pacing for Spontaneous Rapid Ventricular Tachycardia in Patients With Coronary Artery Disease. Circulation 2001, 104, 796–801. [Google Scholar] [CrossRef] [Green Version]
- Santos-Eggimann, B.; Cuenoud, P.; Spagnoli, J.; Junod, J. Prevalence of frailty in middle-aged and older community-dwelling Europeans living in 10 countries. J. Gerontol. 2009, 64, 675–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xue, Q.-L. The Frailty Syndrome: Definition and Natural History. Clin. Geriatr. Med. 2011, 27, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uchmanowicz, I.; Lisiak, M.; Wontor, R.; Łoboz-Rudnicka, M.; Jankowska-Polańska, B.; Łoboz-Grudzień, K.; Jaarsma, T. Frailty Syndrome in cardiovascular disease: Clinical significance and research tools. Eur. J. Cardiovasc. Nurs. 2015, 14, 303–309. [Google Scholar] [CrossRef] [Green Version]
- Newman, A.B.; Gottdiener, J.S.; McBurnie, M.A.; Hirsch, C.H.; Kop, W.J.; Tracy, R.; Walston, J.D.; Fried, L.P. Associations of Subclinical Cardiovascular Disease With Frailty. J. Gerontol. Ser. A: Boil. Sci. Med Sci. 2001, 56, M158–M166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cacciatore, F.; Abete, P.; Mazzella, F.; Viati, L.; DELLA Morte, D.; D’Ambrosio, D.; Gargiulo, G.; Testa, G.; De Santis, D.; Galizia, G.; et al. Frailty predicts long-term mortality in elderly subjects with chronic heart failure. Eur. J. Clin. Investig. 2005, 35, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Rowe, R.; Iqbal, J.; Murali-Krishnan, R.; Sultan, A.; Orme, R.; Briffa, N.; Denvir, M.; Gunn, J. Role of frailty assessment in patients undergoing cardiac interventions. Open Hear. 2014, 1, e000033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, M.M.; Ghali, W.A.; Faris, P.D.; Galbraith, P.D.; Norris, C.M.; Knudtson, M.L.; for the Alberta Provincial Project for Outcomes Assessment in Coronary Heart Disease (APPROACH) Investigators. Survival after coronary revascularization in the elderly. Circulation 2002, 105, 2378–2384. [Google Scholar] [CrossRef] [Green Version]
- Raatikainen, M.P.; Arnar, D.O.; Merkely, B.; Nielsen, J.C.; Hindricks, G.; Heidbuchel, H.; Camm, J. A Decade of Information on the Use of Cardiac Implantable Electronic Devices and Interventional Electrophysiological Procedures in the European Society of Cardiology Countries: 2017 Report from the European Heart Rhythm Association. Europace 2017, 19, ii1–ii90. [Google Scholar] [CrossRef]
- Gobbens, R.J.; van Assen, M.A.; Luijkx, K.G.; Wijnen-Sponselee, M.T.; Schols, J.M. The Tilburg Frailty Indicator: Psychometric Properties. J. Am. Med Dir. Assoc. 2010, 11, 344–355. [Google Scholar] [CrossRef]
- Uchmanowicz, I.; Jankowska-Polanska, B.; Loboz-Rudnicka, M.; Manulik, S.; Loboz-Grudzien, K.; Gobbens, R. Cross-cultural adaptation and reliability testing of the Tilburg Frailty Indicator for optimizing care of Polish patients with frailty syndrome. Clin. Interv. Aging 2014, 9, 997–1001. [Google Scholar] [CrossRef] [Green Version]
- Moss, A.J.; Zareba, W.; Hall, W.J.; Klein, H.; Wilber, D.J.; Cannom, D.S.; Daubert, J.P.; Higgins, S.L.; Brown, M.W.; Andrews, M.L. Prophylactic Implantation of a Defibrillator in Patients with Myocardial Infarction and Reduced Ejection Fraction. N. Engl. J. Med. 2002, 346, 877–883. [Google Scholar] [CrossRef] [Green Version]
- The Antiarrhythmics versus Implantable Defibrillators (AVID) Investigators. A comparison of antiarrhythmic-drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. N. Engl. J. Med. 1997, 337, 1576–1583. [Google Scholar] [CrossRef]
- Santangeli, P.; Biase, L.D.; Russo, A.D.; Casella, M.; Bartoletti, S.; Santarelli, P.; Pelagonio, G.; Natale, A. Meta-analysis: Age and effectiveness of prophylactic implantable cardioverter-defibrillators. Ann. Intern. Med. 2010, 153, 592–599. [Google Scholar] [CrossRef] [Green Version]
- Healey, J.S.; Hallstrom, A.P.; Kuck, K.-H.; Nair, G.; Schron, E.P.; Roberts, R.S.; Morillo, C.A.; Connolly, S.J. Role of the implantable defibrillator among elderly patients with a history of life-threatening ventricular arrhythmias. Eur. Hear. J. 2007, 28, 1746–1749. [Google Scholar] [CrossRef] [Green Version]
- Chan, P.S.; Nallamothu, B.K.; Spertus, J.A.; Masoudi, F.A.; Bartone, C.; Kereiakes, D.J.; Chow, T. Impact of age and medical comorbidity on the effectiveness of implantable cardioverter-defibrillators for primary prevention. Circ. Cardiovasc. Qual. Outcomes 2009, 2, 16–24. [Google Scholar] [CrossRef] [Green Version]
- Brullmann, S.; Dichtl, W.; Paoli, U.; Haegeli, L.; Schmied, C.; Steffel, J.; Brunckhorst, C.; Hintringer, F.; Seifert, B.; Duru, F.; et al. Comparison of benefit and mortality of implantable cardioverter-defibrillator therapy in patients aged ≥ 75 years versus those, 75 years. Am. J. Cardiol. 2012, 109, 712–717. [Google Scholar] [CrossRef]
- Green, A.; Leff, B.; Wang, Y.; Spatz, E.S.; Masoudi, F.A.; Peterson, P.N.; Daugherty, S.L.; Matlock, D.D. Geriatric conditions in patients undergoing defibrillator implantation for prevention of sudden cardiac death: Prevalence and impact on mortality. Cardiovasc. Qual. Outcomes 2016, 9, 23–30. [Google Scholar] [CrossRef] [Green Version]
- Mlynarska, A.; Mlynarski, R.; Golba, K. Frailty as a predictor of negative outcomes after cardiac resynchronization therapy. Pacing Clin. Electrophysiol. 2018, 41, 572–577. [Google Scholar] [CrossRef]
- Grimm, W.; Stula, A.; Sharkova, J.; Alter, P.; Maisch, B. Outcomes of Elderly Recipients of Implantable Cardioverter Defibrillators. Pacing Clin. Electrophysiol. 2007, 30, S134–S138. [Google Scholar] [CrossRef]
- Duray, G.; Richter, S.; Manegold, J.; Israel, C.; Gronefeld, G.; Hohnloser, S. Efficacy and safety of ICD therapy in a population of elderly patients treated with optimal back-ground medication. J. Interv. Card. Electrophysiol. 2005, 14, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Noseworthy, P.; Lashevsky, I.; Dorian, P.; Greene, M.; Cvitkovic, S.; Newman, D. Feasibility of implantable cardioverter defibrillator use in elderly patients: A case series of octogenarians. Pacing Clin. Electrophysiol. 2004, 27, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Kong, M.; Al-Khatib, S.; Sanders, G.; Hasselblad, V.; Peterson, E. Use of implantable cardioverter-defibrillators for primary prevention in older patients: A systematic literature review and meta-analysis. Cardiol. J. 2011, 18, 503–514. [Google Scholar] [CrossRef]
- Reynolds, M.R.; Cohen, D.J.; Kugelmass, A.D.; Brown, P.P.; Becker, E.R.; Culler, S.D.; Simon, A.W. The frequency and incremental cost of major complications among medic are beneficiaries receiving implantable cardioverter-defibrillators. J. Am. Coll. Cardiol. 2006, 47, 2493–2497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Khatib, S.M.; Greiner, M.A.; Peterson, E.D.; Hernandez, A.F.; Schulman, K.A.; Curtis, L.H. Patient and Implanting Physician Factors Associated With Mortality and Complications After Implantable Cardioverter-Defibrillator Implantation, 2002–2005. Circ. Arrhythmia Electrophysiol. 2008, 1, 240–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bardy, G.H.; Lee, K.L.; Mark, D.; Poole, J.E.; Packer, D.L.; Boineau, R.; Domanski, M.; Troutman, C.; Anderson, J.; Johnson, G.; et al. Amiodarone or an Implantable Cardioverter–Defibrillator for Congestive Heart Failure. N. Engl. J. Med. 2005, 352, 225–237. [Google Scholar] [CrossRef]
- Moss, A.J.; Schuger, C.; Beck, C.A.; Brown, M.W.; Cannom, D.S.; Daubert, J.P.; Estes, N.A.M., III; Greenberg, H.; Hall, W.J.; Huang, D.T.; et al. MADIT-RIT Trial Investigators. Reduction in inappropriate therapy and mortality through ICD programming. N. Engl. J. Med. 2012, 367, 2275–2283. [Google Scholar] [PubMed] [Green Version]
- Mlynarska, A.; Mlynarski, R.; Uchmanowicz, I.; Marcisz, C.; Golba, K. The Relationship between Frailty Syndrome and Concerns about an Implantable Cardioverter Defibrillator. Int. J. Environ. Res. Public Heal. 2020, 17, 1954. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall Population n=103 Median; [Q1;Q3] | With No Shock n=75 Median; [Q1;Q3] | Electric Shock n=28 Median; [Q1;Q3] | Inadequate Electric Shock n=11 Median; [Q1;Q3] | Electrical Storm n=3 Median; [Q1;Q3] | p | |
|---|---|---|---|---|---|---|
| Age [years] | 71; [64;78] | 71; [64;78] | 70.5; [65;79] | 67; [64;73] | 74; [63;85] | 0.8335 # |
| Gender woman | 17.47% | 21.33% | 7.14% | 18.18% | 66.67% | 0.0625 * |
| Weight [kg] | 79; [70;88] | 80.3; [67;91] | 77; [72;83] | 72.5; [71;75] | 69; [66;72] | 0.3260 # |
| BMI | 28.44; [25.28;31.63] | 28.51; [24.86;31.6] | 26.64; [24.96;30.76] | 26.16; [24.93;27.42] | 29.47; [28.19;30.76] | 0.5804 # |
| Place of residence - urban area - rural area | 81.55% 18.45% | 85.34% 14.66% | 67.86% 32.14% | 45.45% 54.55% | 33.33% 66.67% | 0.0043 * |
| Education - none or primary - secondary - vocational or higher | 37.87% 61.16% 0.97% | 36.00% 62.67% 1.33% | 42.85% 57.14% 0 | 36.37% 63.63% 0 | 66.67% 33.33% 0 | 0.6941* |
| Marital Status - married/living with a partner - unmarried - widow/widower | 90.29% 7.77% 1.94% | 93.33% 4.00% 2.66% | 85.71% 14.29% 0 | 100% 0 0 | 100% 0 0 | 0.2231 * |
| Professional status Working Retired Pensioner | 21.36% 71.84% 6.80% | 22.66% 72.00% 5.34% | 17.85% 75.00% 7.14% | 18.19% 9.09% 72.72% | 0 66.67% 33.33% | 0.8419 * |
| Smoking | 29.13% | 32.00% | 21.42% | 18.18% | 33.33% | 0.6252 * |
| Indication for implantation − primary | 49.51% | 53.33% | 39.28% | 27.27% | 33.33% | 0.2816 * |
| More than two diseases | 77.67% | 77.33% | 86.57% | 81.81% | 100% | 0.0001 * |
| TFI and Domain | Overall Population | With No Shock | Electric Shock | Inadequate Electric Shock | Electrical Storm | p |
|---|---|---|---|---|---|---|
| General (mean ± SD Median; [Q1;Q3]) | 6.66 ± 2.66 7; [4;9] | 6.27 ± 2.76 6; [4;8] | 7.38 ± 2.21 7.5; [6;9] | 8.56 ± 1.94 8; [5;11] | 8.00 ± 3.00 8; [5;11] | 0.0436 # |
| Physical (mean ± SD Median; [Q1;Q3]) | 4.58 ± 1.79 4; [3;6] | 3.83 ± 1.82 4; [2;5] | 4.73 ± 1.56 5; [4;6] | 5.22 ± 1.30 5; [3;6] | 4.67 ± 1.53 5; [3;6] | 0.0444 # |
| Psychological (mean ± SD Median; [Q1;Q3]) | 2.06 ± 1.11 2; [1;3] | 2.04 ± 1.14 2; [1;3] | 2.11 ± 0.99 2; [1;3] | 2.67 ± 0.87 3; [2;3] | 2.67 ± 0.58 3; [2;3] | 0.2856 # |
| Social (mean ± SD Median; [Q1;Q3]) | 0.44 ± 0.55 0; [0;1] | 0.40 ± 0.54 0; [0;1] | 0.54 ± 0.58 0.5; [0;1] | 0.67 ± 0.71 0; [0;2] | 0.67 ± 1.15 0; [0;2] | 0.6767 # |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mlynarska, A.; Mlynarski, R.; Uchmanowicz, B.; Mikuľáková, W. Can Frailty Be a Predictor of ICD Shock after the Implantation of a Cardioverter Defibrillator in Elderly Patients? Sensors 2021, 21, 6299. https://0-doi-org.brum.beds.ac.uk/10.3390/s21186299
Mlynarska A, Mlynarski R, Uchmanowicz B, Mikuľáková W. Can Frailty Be a Predictor of ICD Shock after the Implantation of a Cardioverter Defibrillator in Elderly Patients? Sensors. 2021; 21(18):6299. https://0-doi-org.brum.beds.ac.uk/10.3390/s21186299
Chicago/Turabian StyleMlynarska, Agnieszka, Rafal Mlynarski, Bartosz Uchmanowicz, and Wioletta Mikuľáková. 2021. "Can Frailty Be a Predictor of ICD Shock after the Implantation of a Cardioverter Defibrillator in Elderly Patients?" Sensors 21, no. 18: 6299. https://0-doi-org.brum.beds.ac.uk/10.3390/s21186299