1. Introduction
Fracture healing is a complex and dynamic process, which involves both biological and mechanical aspects. About six million fractures occur annually in the United States, and 5 to 10% of these fractures proceed to a delayed union or a non-union [
1]. Generally, a non-union fracture occurs if the reparative processes end before the bone union takes place. The biological risk of non-union depends on the fracture severity and location, i.e., highest non-union rates are associated with scaphoid (15.5%), followed by tibia and fibula (14%), and femur (13.9%) [
2].
External fixators are widely used for the stabilization of long bone fractures [
3] with precise indications. Usually, pins are placed on both sides of the fracture and bars are attached to the pins by using clamps. The intramedullary nail is associated with fewer complications [
4], but also has many contraindications [
5], and therefore the external treatment is often preferred. Indeed, the positioning of an external fixator is faster and simpler [
6] and, furthermore, it also allows the dynamic adjustment of the degree of mechanical rigidity of the implant during the healing process. Moreover, external fixators have the advantage of being outside the body, allowing an objective evaluation without further surgical procedures. Successful treatment with an external fixator is strongly dependent on the identification of the correct timing for its removal. Premature removal of the fixator can lead to bone refracture, resulting in additional surgical procedures and an extended period of hospitalisation. On the other hand, delayed removal of the implant leads to an unnecessarily prolonged treatment time [
7]. Hence, prevention and an adequate healing assessment are essential factors for both the patient’s well-being and to reduce the costs associated with surgical re-interventions and follow-ups.
Currently, radiographic and clinical examination are the most common tools used to monitor bone healing; however, these are subjective, operator-dependent, and non-quantitative methods. Hence, there is a need for a reliable and objective method able to quantitatively establish the state of bone health, measuring: (a) the degree of mechanical stabilization of the bone implant, and (b) an objective endpoint of healing. The monitoring of the implant’s stability may avoid further surgical interventions related to refracture and/or non-union problems. On the other hand, a precise knowledge of the stages and endpoint of healing may allow the formulation of patient-specific rehabilitation protocols.
1.1. State-of-the-Art of Measurement Technologies
Many researchers proposed alternative methods for monitoring the bone fracture healing, as reviewed in [
1,
8,
9,
10]. In particular, mechanical assessment tools are based on the concept that bone callus stiffness increases from the early phases of callus formation to complete union, representing a useful index of healing. Vibrational testing has been proposed to evaluate the mechanical properties of the bone–external fixator system, evaluating its resonant response to an excitation input signal [
7,
11,
12]. However, this kind of approach suffers from metallic implant interference, and skin and soft tissue interference on the mechanical wave propagation; moreover, different studies are in disagreement on the definition of the healed fracture as its vibrational response [
8]. On the other hand, direct and/or indirect biomechanical tests have been performed in research to evaluate the mechanical behaviour of the system along the healing process. As direct methods (i.e., the assessment of the fracture stiffness by measuring the deflection at the fracture site [
9]) have the major disadvantage of removing the external fixator for each measurement, the indirect approach (i.e., the measurement of the strain through an external fixation [
1]) has been investigated more extensively. In indirect measurement approaches, the strain of the implant is evaluated against the healing time. Since the deformation of the frame is inversely proportional to the callus stiffness, information on the state of the bone can be obtained by monitoring the level of deformation on the external fixator [
13]. Only a few studies in the past have evaluated the displacement of the external fixator components as a mean for monitoring fracture healing. However, most of these studies focused only on the evaluation of the mechanical performance of the implant depending on the different frame configurations that were used [
14,
15,
16,
17], without considering the development of bone callus. Seide et al. [
18] used a hexapod external fixator embedded with force sensors to measure 3D external loads. This measurement device gave results in good agreement with the healing time, even if the system appeared cumbersome and lacked portability. Grasa et al. [
19] also sensorized an external fixator using a set of strain gauges to detect the bending loads on two different planes. The system was validated on animal models by recording the load transmission through the fixator during the gait cycle and over the healing time. However, as assessed by the authors, the results should be evaluated with caution, considering the high variability among the animals. Burny et al. [
13] highlighted the importance of considering the presence of bone callus as it can cause variations in load transmission. Authors covered the rods of a Hoffmann
® external fixator (Striker Corp., Kalamazoo, MI, USA) with strain gauges in order to monitor changes in the torque applied to the rods and the moments at the articulations. The analysis was made for different configuration of the external fixator, using springs of different stiffness to simulate bone callus healing. In 1983, Beaupre et al. [
20] analysed the change in pins displacements, also taking into account different degrees of bone callus stiffness using a dial gauge integrated with an external fixator. Recently, Di Puccio et al. [
21] measured the load transfer process between the external fixator and the fractured bone by means of strain gauges; this study allowed us to identify the optimum position of the strain gauges on the fixator to measure the load distribution during healing.
1.2. Beyond the State-of-the-Art and Organization of the Paper
To summarise, all the previous studies employed, primarily, strain gauges or dial gauges in order to measure the implant deformation over the healing time. However, strain gauges can only provide a measurement on a single axis and, therefore, several sensors have to be used in order to detect the translation on each axis; this consistently increases complexity and costs of the measurement system. On the other hand, dial gauges have the advantage of being cheaper, although they can only provide linear measurements.
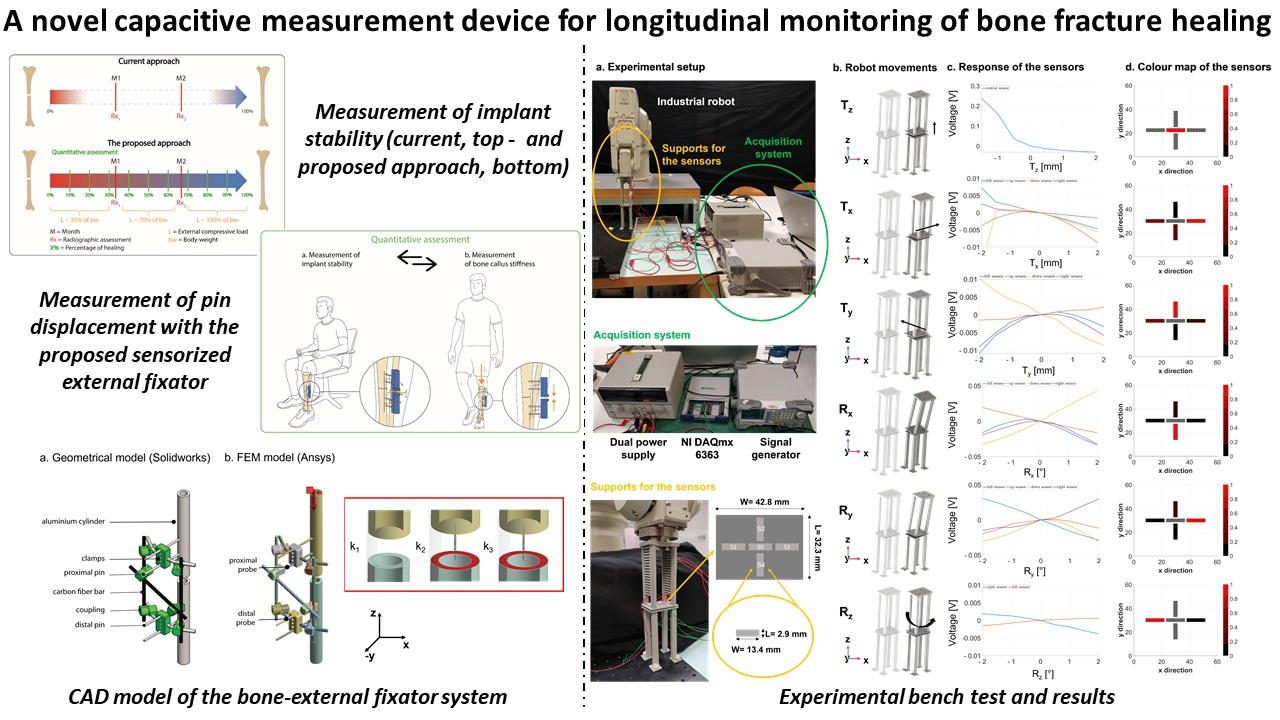
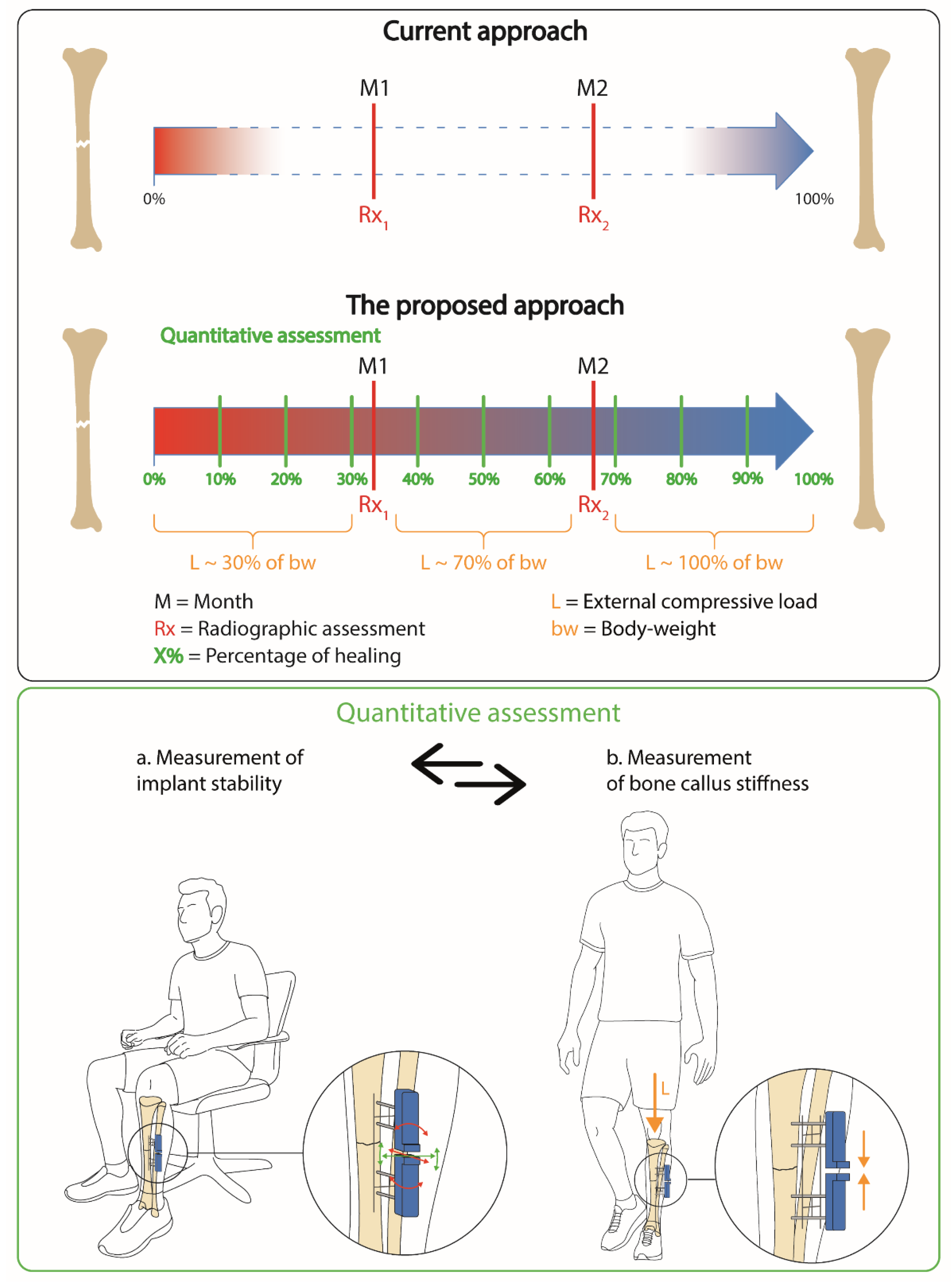
In this study, we propose a low-cost and customised solution composed of a 2D matrix of capacitive sensors that are able to detect both the relative translation and the rotations of the external fixator pins, as an index for determining the bone’s healing status. Indeed, capacitive sensors are cheap and easily scalable/adaptable to any non-regular surface. In particular, we decided to record the displacements of the pins, as they present the advantage of being in direct contact with the bone fragments: hence, if some movements occur at the bone level, they are directly transferred outside through the pins. The external fixator deforms when the bone is subjected to an external load (as during the weight bearing), and such deformation decreases when the bone callus stiffness increases. Usually, patients are encouraged to bear weight on the injured limb, as much as the pain allows it, from day one, in order to stimulate bone regeneration, while leading to a deformation of the external frame. Indeed, it has been shown that interfragmentary movements can significantly enhance callus formation [
22]. On the other hand, if the callus is not stiff enough, an excessive external load can lead to plastic deformation of the fixator, with the consequent need of surgical re-intervention [
9,
14]. Hence, after each weight bearing exercise, a measurement of the degree of deformation on the external frame is always needed to assess the stability of the external implant.
The authors decided to focus such study on tibia fractures since, as mentioned above, they are associated with the highest non-union rates. Moreover, a fracture which involves the lower limbs forces the patient not to move for a long period of time, causing discomfort that lasts for a long period of time in the case of non-union.
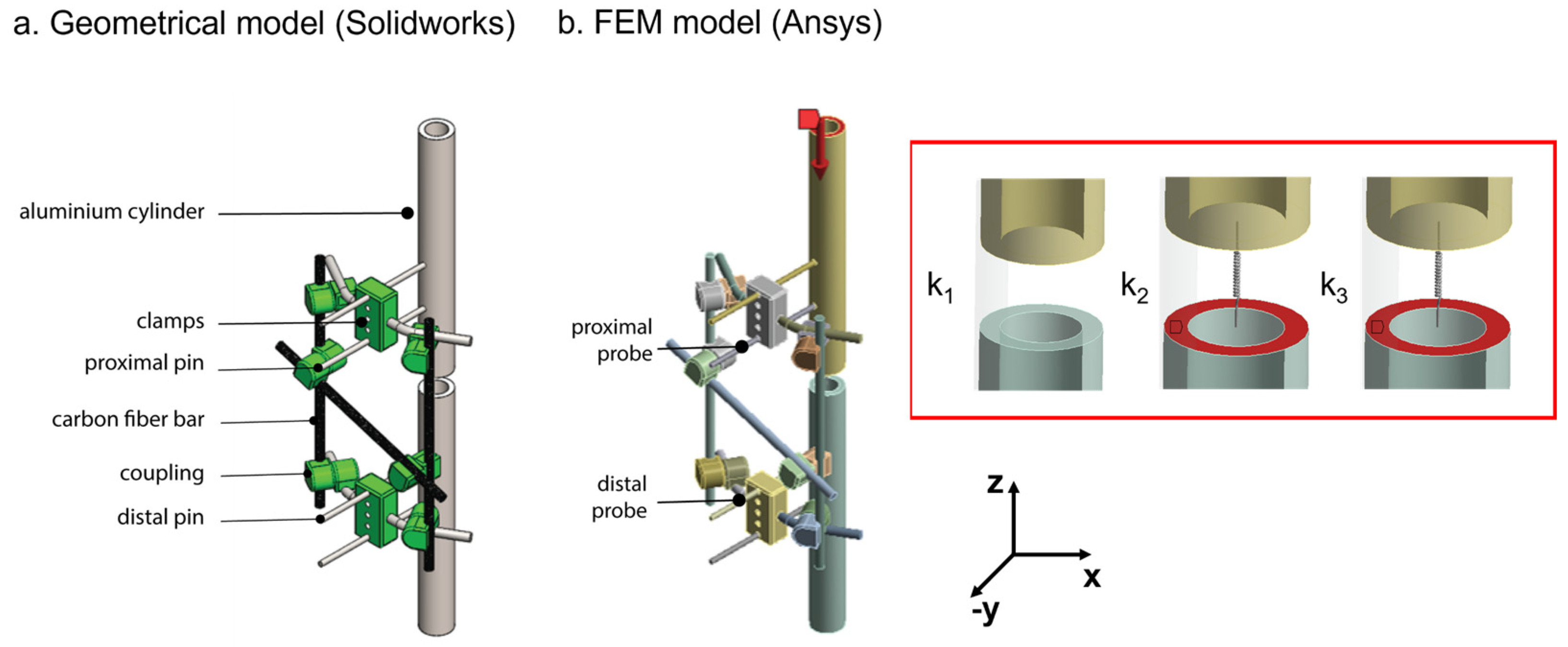
In this article, we first implemented and tested a finite element model (FEM) of a bone fracture model, stabilised with a Hoffman II
® external fixator (Striker Corp., Kalamazoo, MI, USA) in the standard configuration used for tibia fractures (see
Section 2.1). In
Section 2.2, this model was used to systematically analyse the pins displacements due to external loads for each condition of callus stiffness. Finally, in
Section 2.3, a novel capacitive technology was developed and integrated, as part of a novel measurement device, to discriminate the expected displacements of the external fixator pins during the healing time (
Section 2.3.1 and
Section 2.3.2). The results support the use of such capacitive sensor technology for quantitative and even remote assessment of external fixator stability and bone fracture healing. This study represents a first preliminary step toward a future in-vivo application of such a sensorized device.
4. Discussion
In this study, we developed and tested a novel low-cost and effective sensing methodology for monitoring the healing process in cases of long bone fractures treated with an external fixator. Different stabilization methods (i.e., intramedullary nailing, screwed plates, and external fixation) can be indicated for bone reduction, according to skin status, fracture type, location, and bone quality. External fixators are widely used, since they have the advantage of being flexible and have an adjustable mechanical rigidity in accordance with the natural bone growth [
36]. However, external fixators have to be removed, and the identification of correct indications for their removal is fundamental. In fact, to date, there are no standard methods to objectively recognize the stages and the endpoint of healing for removing the bone implant correctly. Moreover, a precise knowledge of the endpoint of healing could enable the definition of patient-specific rehabilitation protocols.
Since the deformation of the external fixator has been demonstrated to be in inverse proportion with the bone callus stiffness [
8], our scientific hypothesis seeks to obtain information on the state of the bone growth by measuring the displacement of the external frame over the healing time. The pins of the external fixator are self-drilled in the bone and are mostly external to the body, proving to be the ideal candidates for the sensorization. As the performance of the external fixation is strictly related to the arrangement and material properties of the main components, we systematically analysed, referencing the clinical standard but with a versatile approach, the mechanical behaviour of a Hoffman
® II external frame in the standard configuration used for tibia fractures. Indeed, our approach may also be translated to other types of external fixators, which allows access to external pins, such as uniplanar external fixators [
37]. We developed and tested in Ansys
® a FEM model of the bone–external fixator system to investigate the relative pins displacements due to the applied compressive loads. In
Figure 7, the percentage errors between the simulation values and the real values are calculated for three stiffness conditions: k
1 = 0 N/mm, k
2 = 0.153 N/mm and k
3 = 0.460 N/mm and for increasing compressive loads (from 0 to 300 N with steps of 50 N). The model was verified with a percentage error lower than 20% in most of the cases, and an overall error of 8%. The error bars rose with the increasing callus stiffness, reaching a percentage error greater than 20% for the lowest loads (i.e., 50 N) at the higher stiffness condition (i.e., k
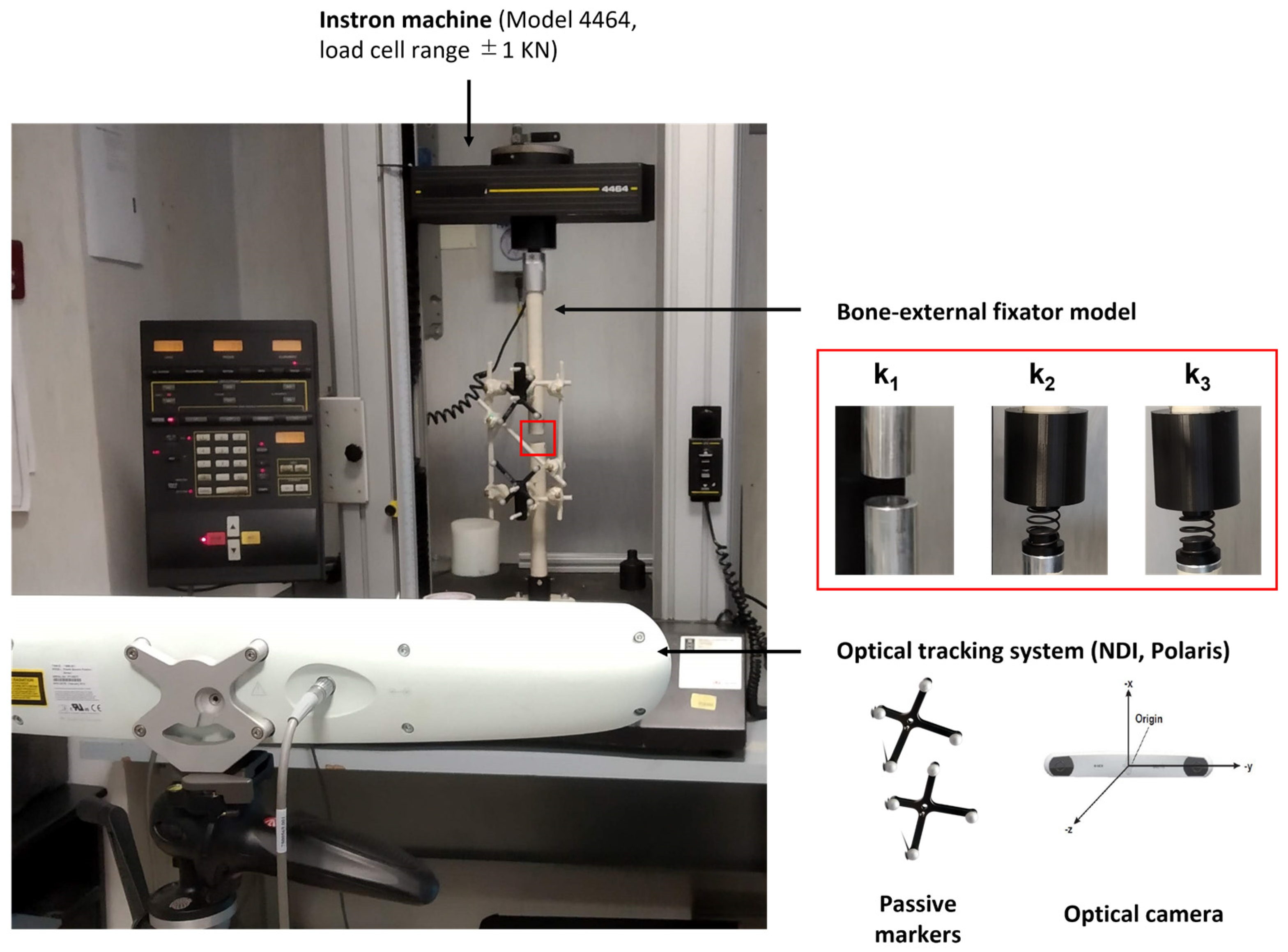
3 = 0.460 N/mm). Indeed, as stiffness increases, the recorded pins displacements reduced, and in particular, they were under the accuracy of the optical tracking system used (i.e., <0.25 mm [
26]). After the validation step, the FEM model was used to simulate the relative pins displacements for different spring stiffnesses, thus covering all the phases of healing, as shown in
Figure 8. Unfortunately, a standard rehabilitation protocol is not available so far for bone fracture treatment: in most cases, the patients are encouraged to bear as much weight on the leg as pain allows. For this reason, clinical indications were provided by expert orthopaedic surgeons in the field, co-authors of this study, and an indication of the maximum supported load for each healing phase was given as a percentage of the body weight of the patient, as usually performed in orthopaedic procedures. As expected, the simulated results (
Figure 8) indicate an increase in the pins displacements with an increasing external load and a decrease in the pins movements with increasing bone callus stiffness. A similar approach may have great potential in clinical practice: indeed, a FEM model may be built specifically for each patient and an estimation of the expected pins movements for each healing phase and for each external load can be obtained from such a model. If the pins displacements recorded by the sensorized external fixator are very different from those estimated by the model, it means that something wrong happened in the healing process, and thus the intervention of the physician is needed. Behind the cited advantages, it is worth mentioning that we have to consider the simulated results. They are strictly dependent on the position of the reading probe on the single pins: indeed, the movements were amplified as we moved the probe away from the fixator body. In our case, to bring the simulated results in line with our application with the embedded sensors, we placed the reading probes on the pins at the same coordinates at which the supports for the sensors were positioned in the experimental tests (see
Figure 6).
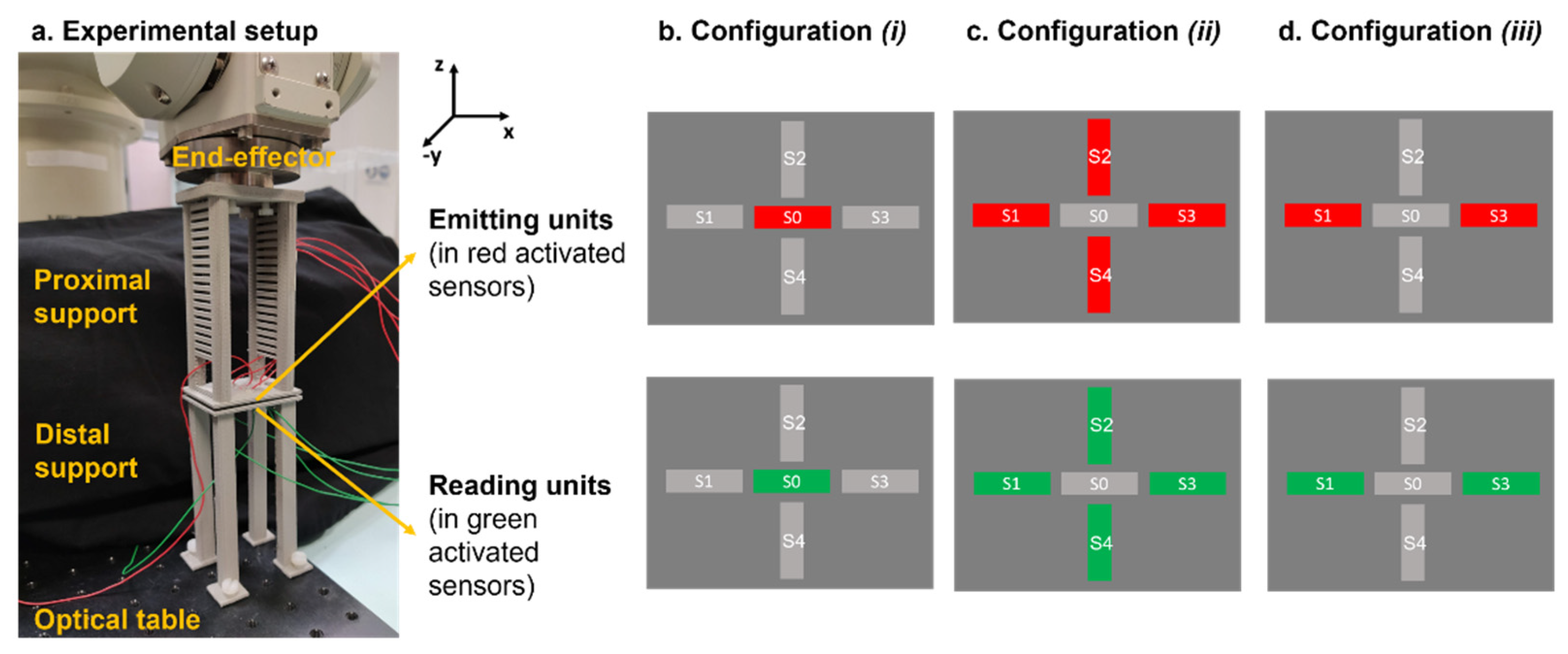
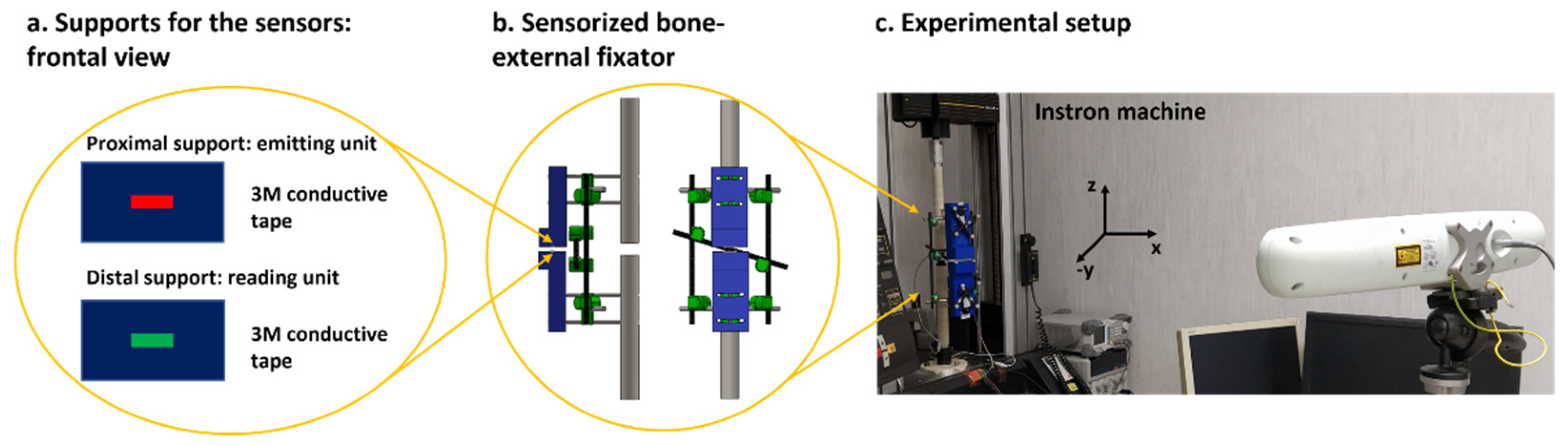
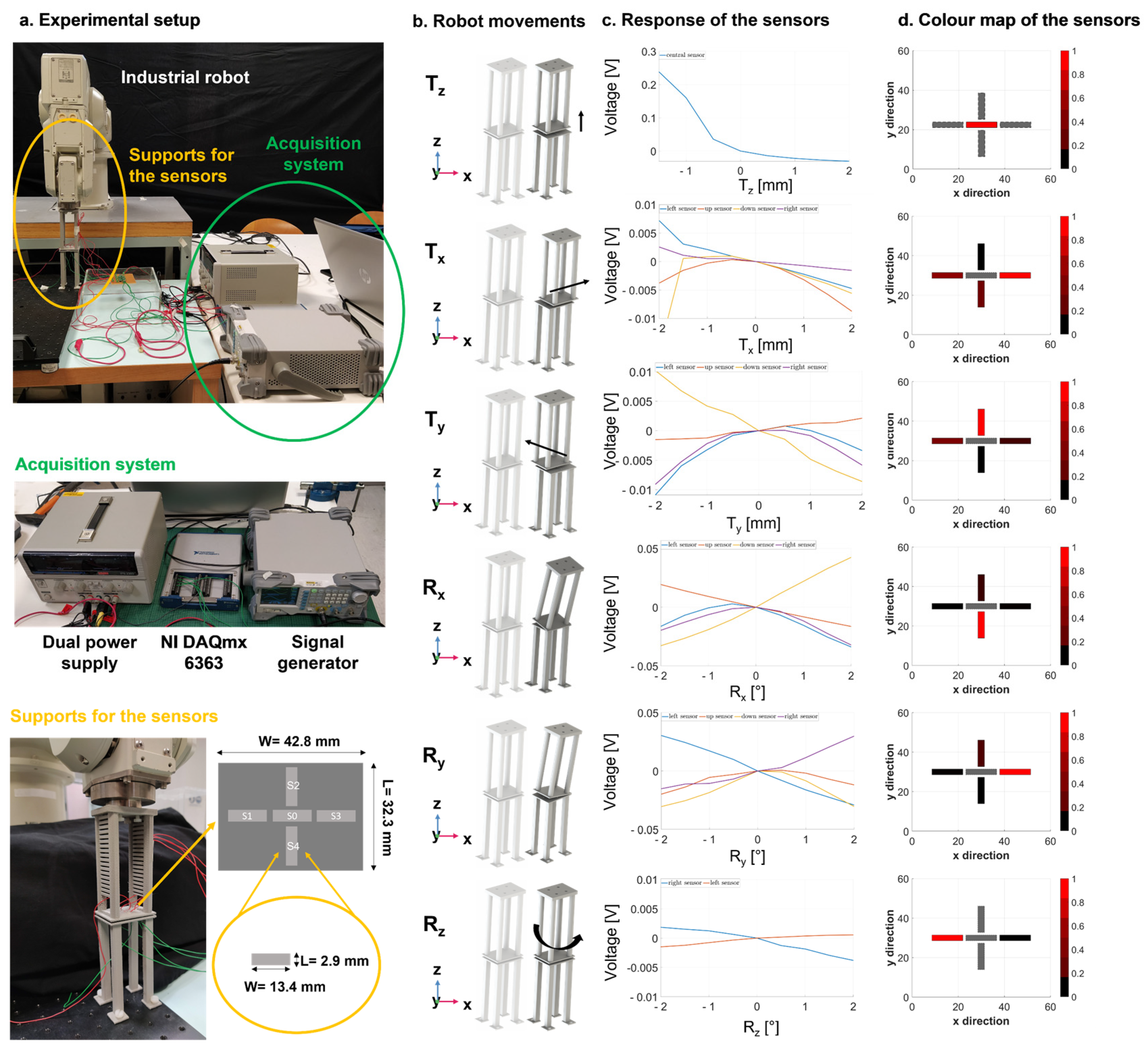
Considering the described results and requirements of the study, we developed a novel sensing measurement device based on a capacitive technology which is able to provide potentially longitudinal and non-invasive/portable monitoring. The proposed sensor technology has to satisfy a double objective: (a) the monitoring of implant stability by detecting unwanted movement of the pins in the 3D space, and (b) the measurement of bone callus stiffness, which depends on the relative pins displacements under external compressive loads. The primary aim of the sensorized device is to guarantee a longitudinal and objective monitoring during the healing time. In particular, we are not interested in calculating an absolute measure of healing (i.e., the callus stiffness); instead, we want to determine a patient-specific percentage of healing over time. For this reason, the pins displacements measurement made on each patient must be related to those of the previous days, ensuring that the bone–external fixator system has not undergone any displacements not related to the healing process. Since sensors are rigidly attached to the pins, any movement of the pins can be directly transferred to the sensor supports. We found that one single capacitive module was not enough to monitor the position of the external pins in the 3D space (see
Figure S2 of the Supplementary Materials). In this regard, a smart configuration of five sensors was implemented and integrated in the system, obtaining a total surface of 32.3 mm × 42.8 mm. Instead of activating all five electrodes at the same time, we found it more convenient to test three different configurations of activation, which are able to detect up to six degrees of freedom. When only the central module (S0) was activated, the displacement
Tz was accurately determined, with a resolution of 0.5 mm, as described in
Figure 9 (first row). Similarly, the four sensors (S1, S2, S3, and S4) worked simultaneously to detect the movements
Tx, Ty, Rx and
Ry successfully (see
Figure 9, second row–fifth row). Finally, the combination of the two lateral sensors (S1 and S3) proved to be the most suitable units to identify the rotations around the longitudinal axis (
Rz), as reported in
Figure 9 (last row). Usually, movements of the pins not related to the healing process are in the range ±1 mm and ±1°. The proposed technology was able to discriminate movements with a resolution of 0.5 mm and 0.5°, satisfying the clinical requirements.
As the deformation of the whole frame under compressive loads was demonstrated to be axial with good approximation (see
Figure S1 of the Supplementary Materials), a single sensing module centred on the sensor support proved to be enough to monitor the relative pins displacements. Experimental tests were performed to evaluate the pins displacements of the sensorized external fixator with a callus stiffness equal to k
1 = 0 N/mm under increasing compressive loads (from 0 to 500 N) with intervals of 50 N.
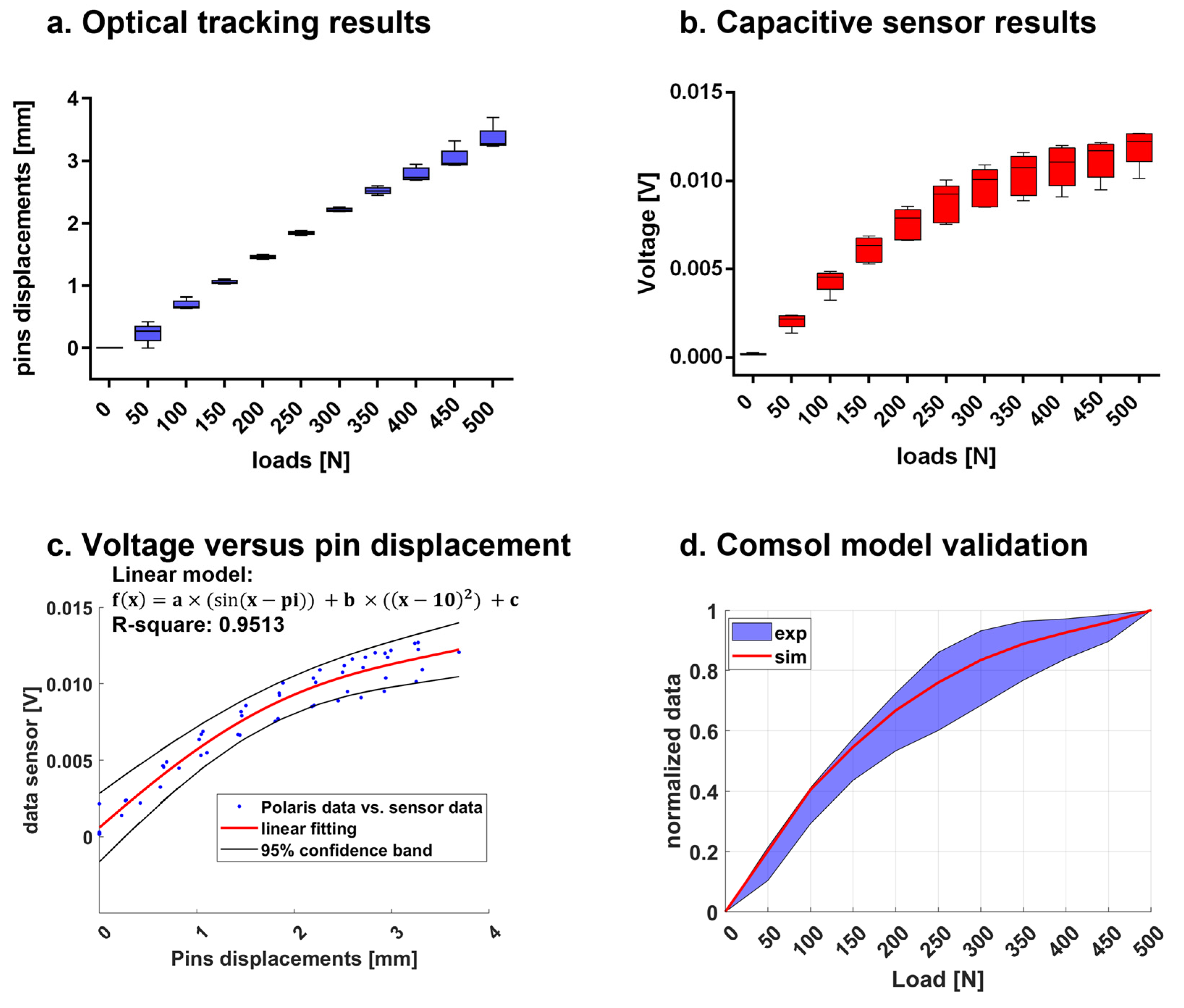
Figure 10b presents the sensor responses in terms of voltage at each loading step, showing an exponential trend. Such behaviour, consistent with the scientific literature of parallel plate capacitive sensors [
33], can be considered advantageous, since pins displacements due to very close loads (step of 50 N) can be easily detected and discriminated. A linear regression, validated with R2 statistic equal to 0.9513, was found when we correlated the voltage and pins displacements recorded by the optical tracking system, as described in
Figure 10c. Indeed, a reliable model correlating voltage and pins displacements allows us to determine the movements of the pins by reading the voltage response. All the considerations on the geometry, dimensions and positions of the sensor module were made by computing an optimization model implemented in Comsol Multiphysics
®. In our experiments, we recreated the same conditions of the simulation, and we compared the normalized results obtained with the Comsol Multiphysics
® model with respect to the normalized results from the experiments, achieving a good matching (as depicted in
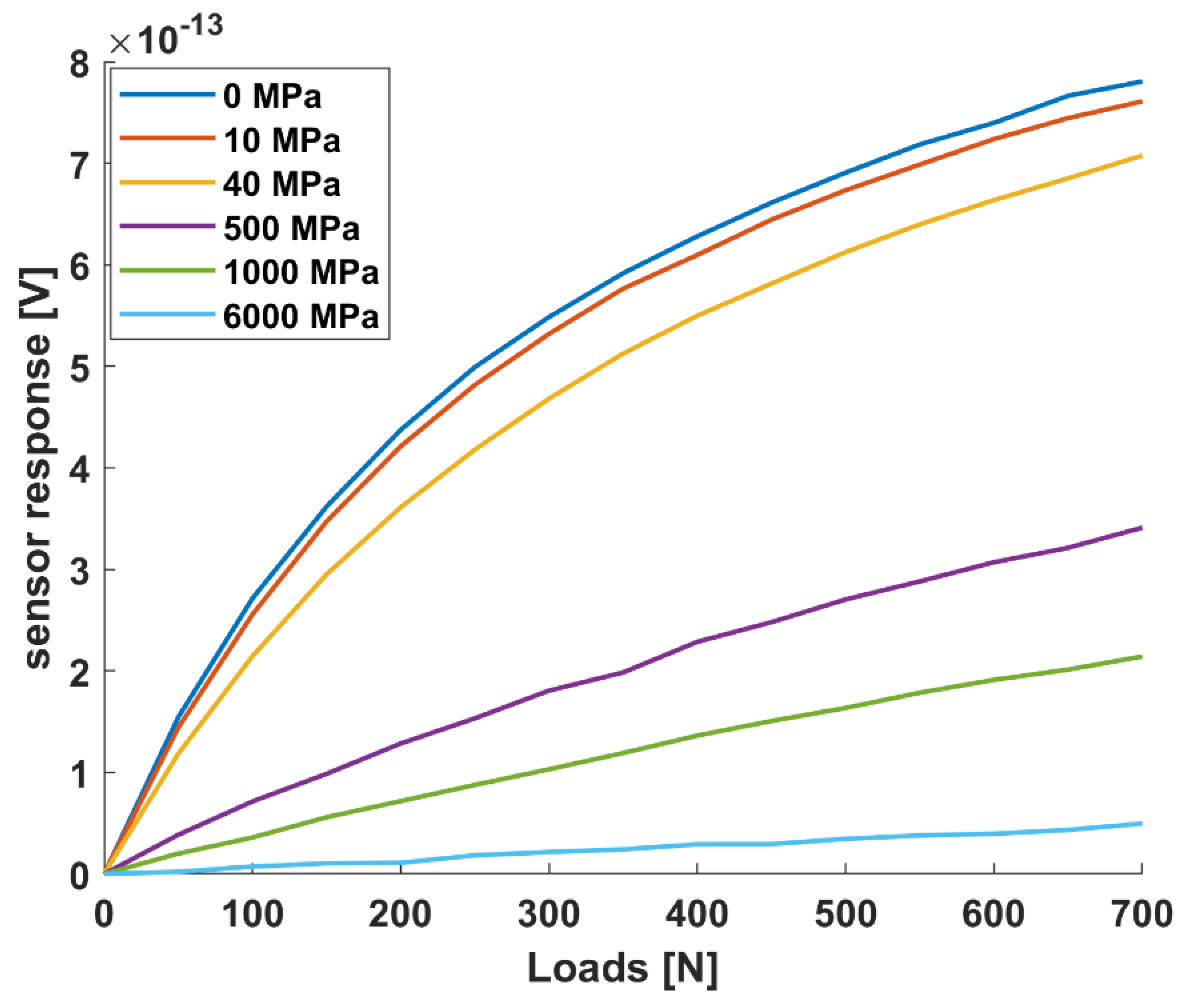
Figure 10d). The maximum percentage error between the real and the simulated sensor curve of response was 27% (at 50 N), proving the goodness of the implemented model, which was thus used as a predictive model for simulating other conditions (i.e., different stiffness). In this regard,
Figure 11 reports the simulated sensor response for six representative stiffness values (i.e., 0, 10, 40, 500, 1000 and 6000 MPa). The bone callus stiffness values of 0, 10 and 1000 MPa correspond to the beginning of the three main phases of healing, as indicated in
Table 1. These results suggest that our capacitive sensor technology can detect pins displacements due to external load associated with different healing phases with a resolution comparable to that of the optical tracking system (0.25 mm). Moreover, the capacitive sensing module can be easily integrated with an external fixator, being, in the future, portable for longitudinal monitoring, thanks to the small dimensions of the single unit (L = 2.9 mm and W = 13.4 mm) and its signal conditioning electronics.
Comparison with other works can only be relevant if the frames are constructed with identical geometry and identical material properties of the components. Indeed, different researchers used different loading conditions, experimental setup and measurement targets. Although Burny et al. [
13] declared the importance of considering the bone callus, since it can cause important variations in the load transmission, most of the previous studies did not consider the development of the bone callus in their analyses of the mechanical behaviour of the external frame [
13]. In previous studies, the authors developed sensorized external fixators aiming to detect the deflection or the bending of the fixator body [
8]. Moreover, these studies were mainly interested in evaluating the mechanical properties of different configurations of commercial external fixators, by using load cells [
15,
16], dial gauges [
14,
17] or strain gauges [
13,
38], rather than establishing a measurement of bone callus stiffness. Very few researchers worked on the sensorization of an external fixator to detect its displacement in relation to the healing time, such as Seide et al. [
18] and Grasa et al. [
19]; however, no advancements or applications of such technology were found in the recent literature. In conclusion, to the best of our knowledge, recent research in the context of bone fractures is still limited, and all of the previous works in this field employed measuring technologies, such as load cells, dial gauges and strain gauges. These measuring technologies present some disadvantage in view of future in-vivo applications: strain gauges are expensive, and more than one sensor is necessary to detect movements on different axes; load cells are cumbersome and not easily adaptable to any surface; dial gauges are also poor with regard to flexibility, and they can only provide linear measurements (not angular displacements). Below, a comparison between the current state-of-the-art technologies and the developed one is reported in
Table 2.
Table 2 evaluates different KPIs, such as sensitivity, resolution, accuracy, time of response and costs. Sensor performances were tested in a non-structured environment without showing any significant drift. Parsing the achieved performances reported in
Table 2, we can assert that the main advantages of the developed technology are its ability to be customizable according to the surface to be sensorized and to the demanded sensitivity range and resolution. Moreover, even if not strictly demanded by the application, the time of response of the capacitive sensor is below 10 ms, which allows researchers to use this technology for real-time applications. In summary, although the achieved accuracy is not comparable with that obtained with dials/strain gauges, the proposed capacitive-based measurement technology is suitable for our application at a reduced cost and with a higher flexibility and modularity with respect to the state-of-the-art.
We chose to implement capacitive technology, as it can overcome many of the mentioned issues, i.e., (1) it is cheap, (2) easily implemented, (3) adaptable to any non-regular surface, and furthermore (4) it has been proven to provide both proximity and pre-contact information [
33]. Since we were able to work at pre-contact distances (i.e., 2 mm) in our measurement device, we exploited the exponential curve of response of the capacitive sensors to increase the resolution and the accuracy of the sensing technology. Moreover, the performance of a capacitive technology in detecting deformations and loads was already proved [
43], paving the way for future orthopaedic applications.
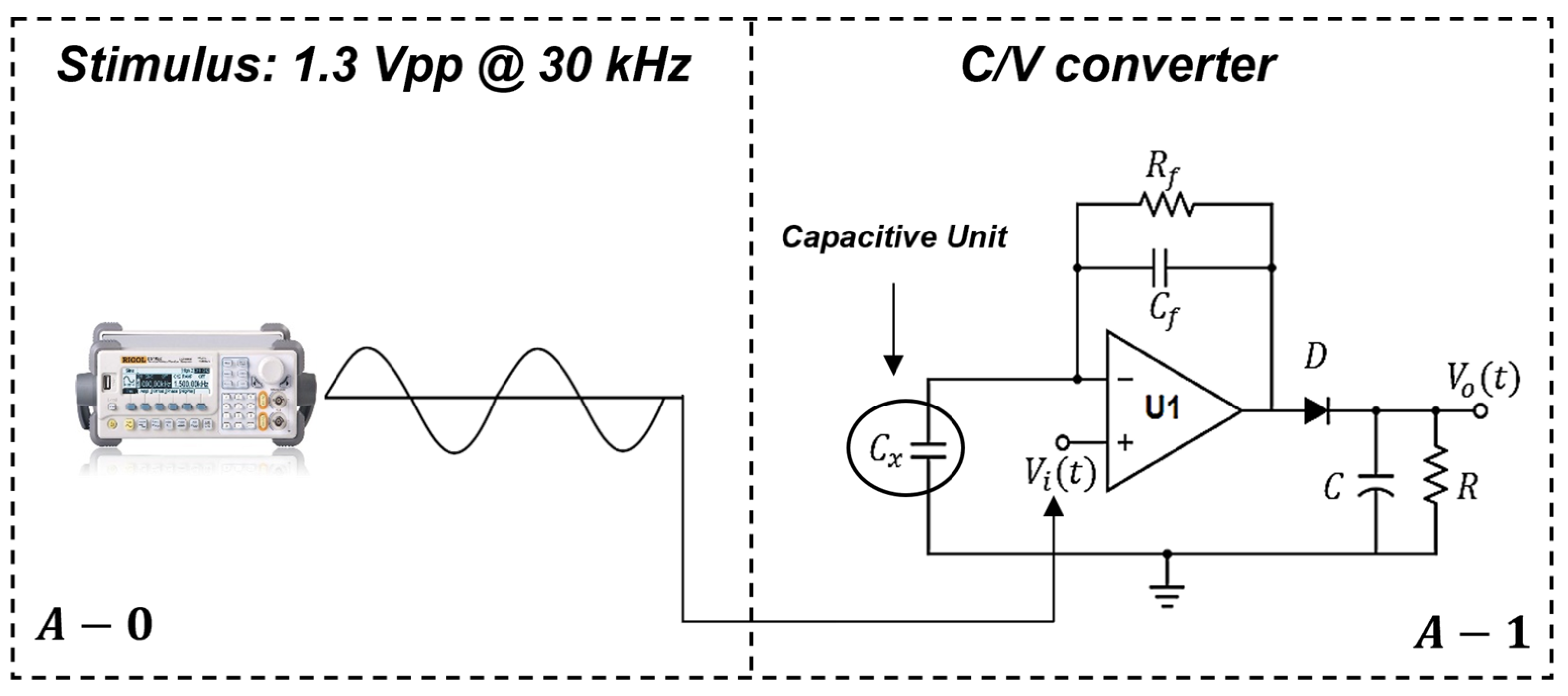
Further developments of the measurement device will be focused on the electronic circuit used for the system characterization to make it compatible, in the future, with portable configurations. In the current version, the stimulus generated by the external signal generator has a frequency of 30 kHz, with an amplitude of 1.3 Vpp and it can be easily substituted by a passive oscillator, which will generate a sinusoidal signal starting from a digital voltage generated by a commercial coin battery (3 V). Moreover, the power supply for the C/V converter (ADA4610-1, Analog Devices Inc., Norwood, MA, USA) will be generated by a dual boost DC-DC, which will act as a step-up voltage starting from the 3 V generated by the coin battery. Finally, a compact microcontroller embedding ADC channels and a Bluetooth module will be embedded into the measurement device with the purpose of converting and collecting the raw data coming from the sensors. All these electronic modifications will lead to the portable configuration of our measurement device.
It is worth mentioning that the in-vitro models are intrinsically limited, due to their inability to reproduce the natural complex environment. In this study, we considered a standard tibia fracture with a well-defined gap of 20 mm, but many other challenges can occur in the real setting, such as a complex facture site, the presence of soft tissue, blood vessels and swelling (especially in the first phase of healing). Such elements are strictly dependent on the patient, the type and the site of the fracture, playing an additional and unknown role in the load distribution. So, authors are aware that the in-vivo translation of such a technology implies some complications that have to be faced in future in-vivo pilot experiments to assess the suitability of the proposed approach in the clinical scenario; however, the study represents a fundamental and propaedeutic technological step forward for the development of future smart medical measurement devices in the orthopaedic field. The measured parameters could be interpreted as an objective percentage of healing with respect to the specific patient and implant. Such an objective metric may support both surgeons and physiotherapists to assess the endpoint of healing and to set patient-specific rehabilitation protocols. The proposed methodology may overlap with the current approach and may support the diagnosis with a longitudinal, low-cost, non-invasive, and potentially even remote measurement of bone healing, allowing both a reduction in X-ray exposition and the integration of the current qualitative information.


 ,
, 














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}