
Diagnostic Accuracy of Cystic Lesions Using a Pre-Programmed Low-Dose and Standard-Dose Dental Cone-Beam Computed Tomography Protocol: An Ex Vivo Comparison Study



Abstract
:1. Introduction
2. Materials and Methods
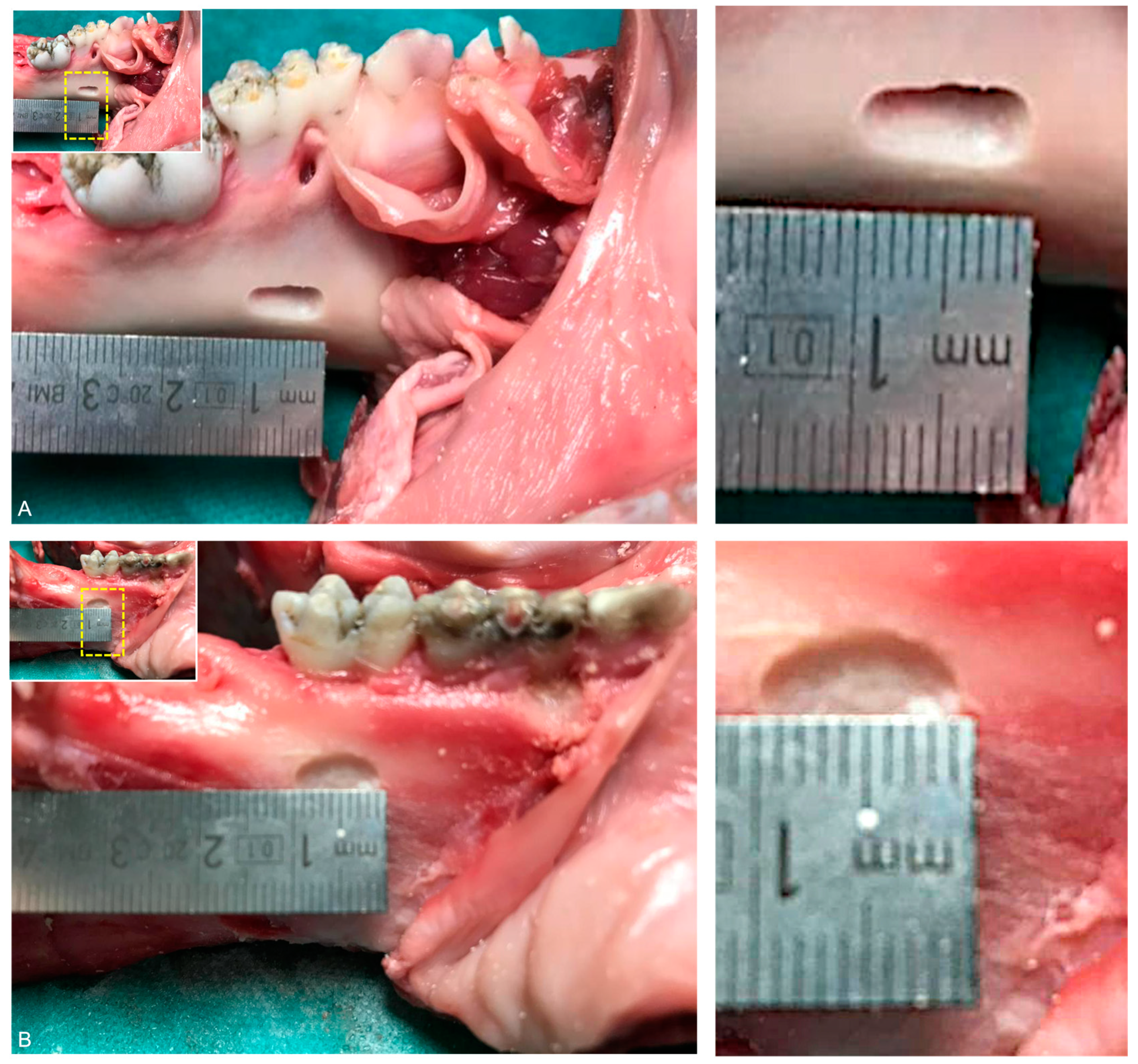
2.1. Preparation of Cystic Lesions
2.2. CBCT Data Acquisition
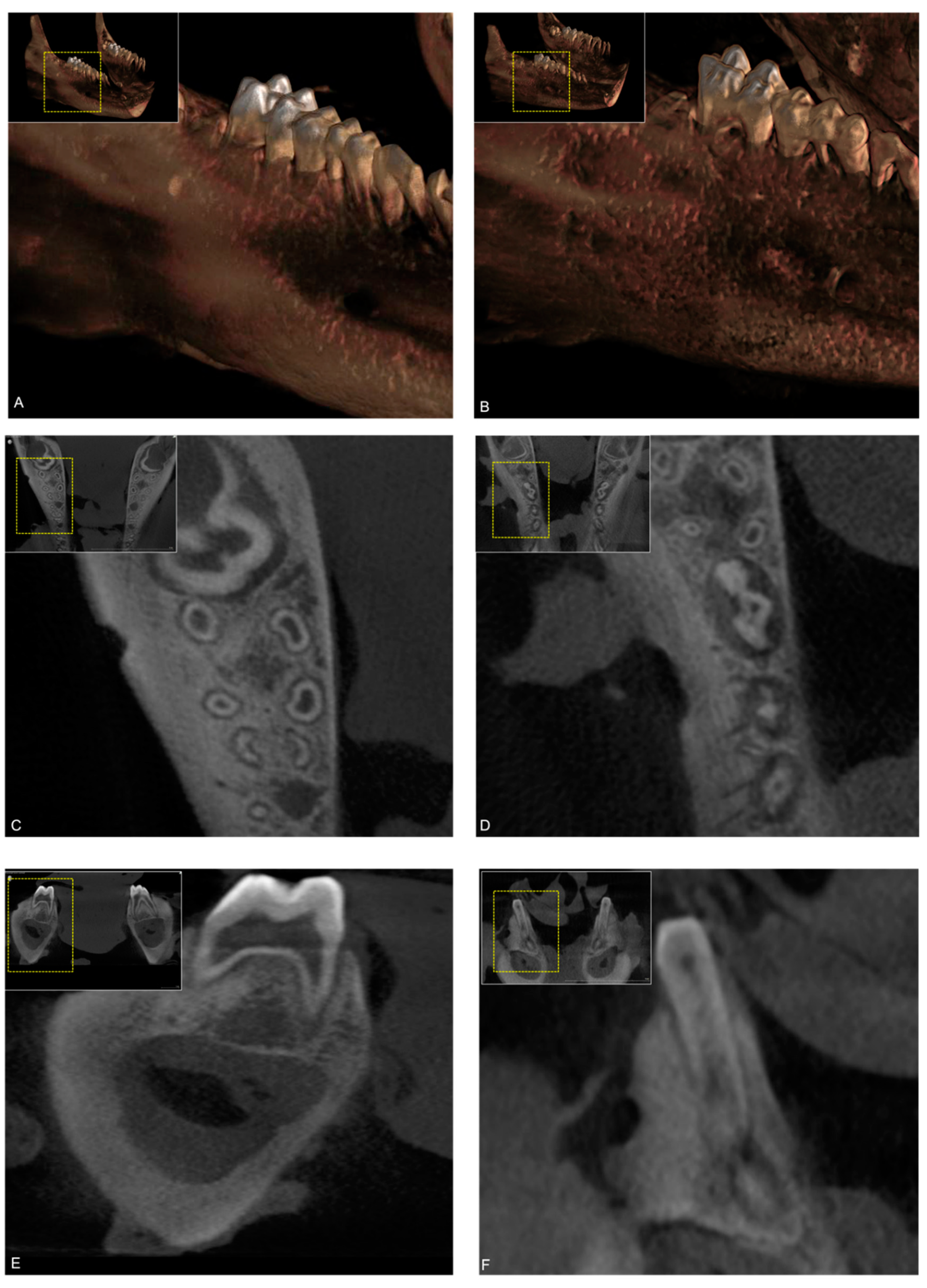
2.3. Image Evaluation
2.4. Statistical Analysis
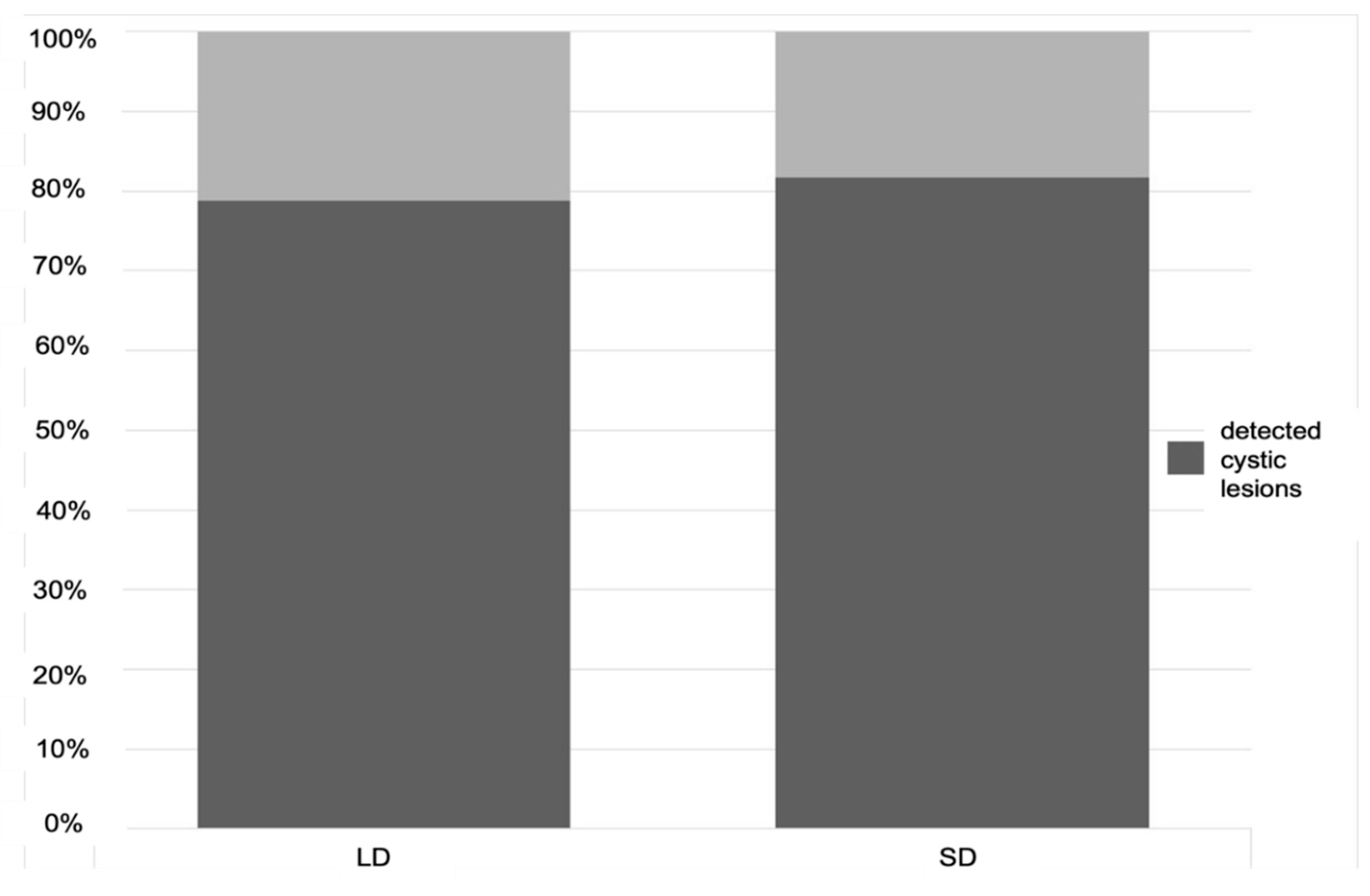
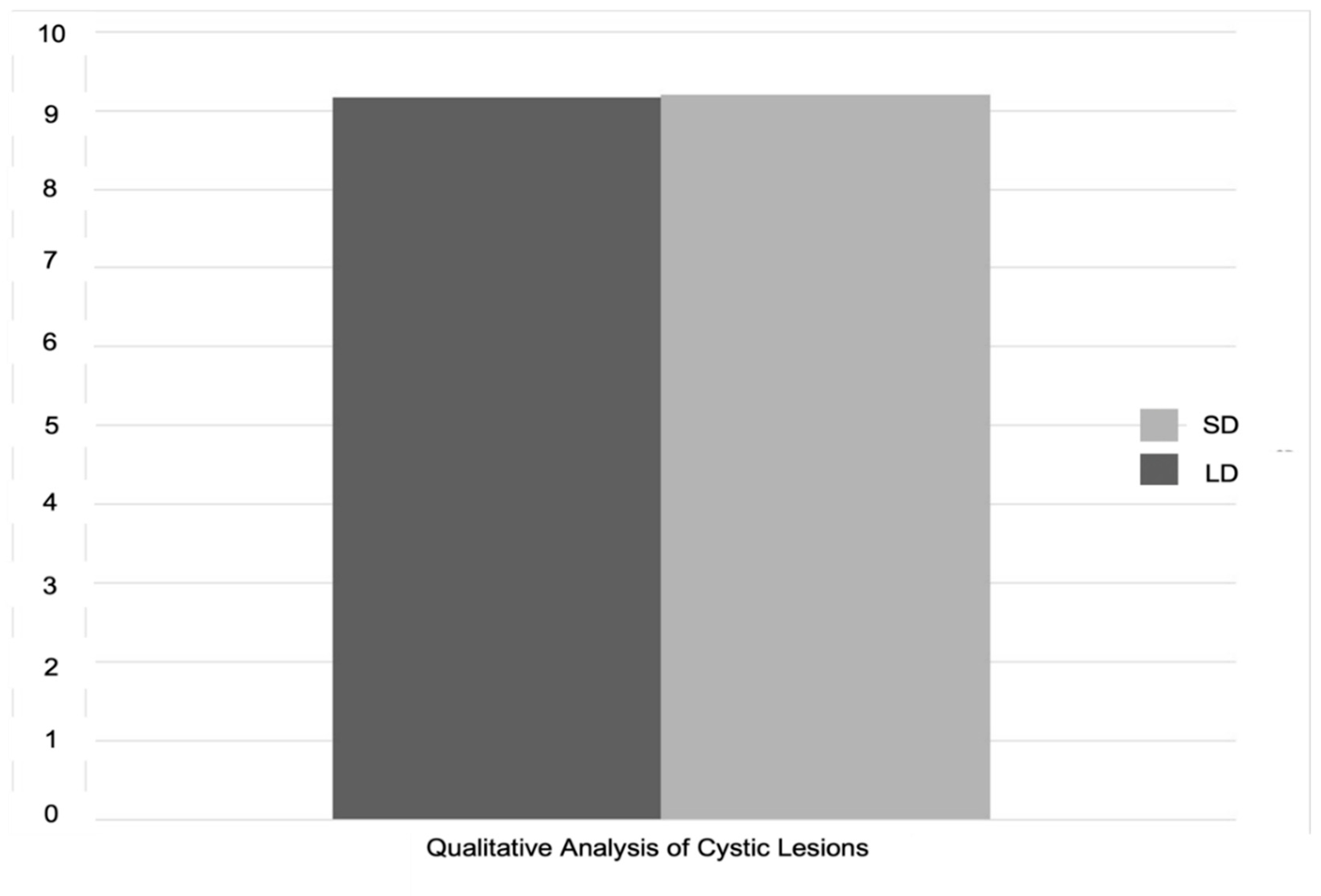
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Scholl, R.J.; Kellett, H.M.; Neumann, D.P.; Lurie, A.G. Cysts and cystic lesions of the mandible: Clinical and radiologic-histopathologic review. Radiographics 1999, 19, 1107–1124. [Google Scholar] [CrossRef] [Green Version]
- Robinson, R.A. Diagnosing the most common odontogenic cystic and osseous lesions of the jaws for the practicing pathologist. Mod. Pathol. 2017, 30, 96–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Consolo, U.; Bellini, P.; Melini, G.M.; Ferri, A.; Lizio, G. Analysis of Marsupialization of Mandibular Cysts in Improving the Healing of Related Bone Defects. J. Oral Maxillofac. Surg. 2020, 78, 1355.e1–1355.e11. [Google Scholar] [CrossRef] [PubMed]
- Lizio, G.; Sterrantino, A.F.; Ragazzini, S.; Marchetti, C. Volume reduction of cystic lesions after surgical decompression: A computerised three-dimensional computed tomographic evaluation. Clin. Oral Investig. 2012, 17, 1701–1708. [Google Scholar] [CrossRef] [PubMed]
- Valdec, S.; Schiefersteiner, M.; Rücker, M.; Stadlinger, B. Guided biopsy of osseous pathologies in the jaw bone using a 3D-printed, tooth-supported drilling template. Int. J. Oral Maxillofac. Surg. 2019, 48, 1028–1031. [Google Scholar] [CrossRef]
- Lotz, M.; Schumacher, C.; Stadlinger, B.; Ikenberg, K.; Rücker, M.; Valdec, S. Accuracy of guided biopsy of the jawbone in a clinical setting: A retrospective analysis. J. Craniomaxillofac. Surg. 2021, 49, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Jaju, P.P.; Jaju, S.P. Cone-beam computed tomography: Time to move from ALARA to ALADA. Imaging Sci. Dent. 2015, 45, 263–265. [Google Scholar] [CrossRef] [Green Version]
- Panmekiate, S.; Rungwittayathon, P.; Suptaweeponboon, W.; Tangtraitham, N.; Pauwels, R. Optimization of exposure parameters in dental cone beam computed tomography using a 3-step approach. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Feragalli, B.; Rampado, O.; Abate, C.; Macrì, M.; Festa, F.; Stromei, F.; Caputi, S.; Guglielmi, G. Cone beam computed tomography for dental and maxillofacial imaging: Technique improvement and low-dose protocols. Radiol. Med. 2017, 122, 581–588. [Google Scholar] [CrossRef]
- Al-Haj Husain, A.; Stadlinger, B.; Winklhofer, S.; Müller, M.; Piccirelli, M.; Valdec, S. Mandibular Third Molar Surgery: Intraosseous Localization of the Inferior Alveolar Nerve Using 3D Double-Echo Steady-State MRI (3D-DESS). Diagnostics 2021, 11, 1245. [Google Scholar] [CrossRef]
- Demirturk Kocasarac, H.; Geha, H.; Gaalaas, L.R.; Nixdorf, D.R. MRI for Dental Applications. Dent. Clin. N. Am. 2018, 62, 467–480. [Google Scholar] [CrossRef]
- Al-Haj Husain, A.; Solomons, M.; Stadlinger, B.; Pejicic, R.; Winklhofer, S.; Piccirelli, M.; Valdec, S. Visualization of the Inferior Alveolar Nerve and Lingual Nerve Using MRI in Oral and Maxillofacial Surgery: A Systematic Review. Diagnostics 2021, 11, 1657. [Google Scholar] [CrossRef]
- Di Nardo, D.; Gambarini, G.; Capuani, S.; Testarelli, L. Nuclear Magnetic Resonance Imaging in Endodontics: A Review. J. Endod. 2018, 44, 536–542. [Google Scholar] [CrossRef]
- Valdec, S.; Husain, A.A.-H.; Winklhofer, S.; Müller, M.; Piccirelli, M.; Stadlinger, B. Comparison of Preoperative Cone-Beam Computed Tomography and 3D-Double Echo Steady-State MRI in Third Molar Surgery. J. Clin. Med. 2021, 10, 4768. [Google Scholar] [CrossRef]
- Patil, S.; Alkahtani, A.; Bhandi, S.; Mashyakhy, M.; Alvarez, M.; Alroomy, R.; Hendi, A.; Varadarajan, S.; Reda, R.; Raj, A.; et al. Ultrasound Imaging versus Radiographs in Differentiating Periapical Lesions: A Systematic Review. Diagnostics 2021, 11, 1208. [Google Scholar] [CrossRef] [PubMed]
- Braun, X.; Ritter, L.; Jervøe-Storm, P.-M.; Frentzen, M. Diagnostic accuracy of CBCT for periodontal lesions. Clin. Oral Investig. 2013, 18, 1229–1236. [Google Scholar] [CrossRef] [PubMed]
- de Faria Vasconcelos, K.; Evangelista, K.M.; Rodrigues, C.D.; Estrela, C.; de Sousa, T.O.; Silva, M.A. Detection of periodontal bone loss using cone beam CT and intraoral radiography. Dentomaxillofac. Radiol. 2012, 41, 64–69. [Google Scholar] [CrossRef] [Green Version]
- Cassetta, M.; Stefanelli, L.V.; Di Carlo, S.; Pompa, G.; Barbato, E. The accuracy of CBCT in measuring jaws bone density. Eur. Rev. Med. Pharmacol. Sci. 2012, 16, 1425–1429. [Google Scholar]
- Kiljunen, T.; Kaasalainen, T.; Suomalainen, A.; Kortesniemi, M. Dental cone beam CT: A review. Phys. Medica 2015, 31, 844–860. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T. Dental MRI: A road beyond CBCT. Eur. Radiol. 2020, 30, 6389–6391. [Google Scholar] [CrossRef]
- Friedlander-Barenboim, S.; Hamed, W.; Zini, A.; Yarom, N.; Abramovitz, I.; Chweidan, H.; Finkelstein, T.; Almoznino, G. Patterns of Cone-Beam Computed Tomoography (CBCT) Utilization by Various Dental Specialties: A 4-Year Retrospective Analysis from a Dental and Maxillofacial Specialty Center. Healthcare 2021, 9, 1042. [Google Scholar] [CrossRef] [PubMed]
- Wolff, C.; Mücke, T.; Wagenpfeil, S.; Kanatas, A.; Bissinger, O.; Deppe, H. Do CBCT scans alter surgical treatment plans? Comparison of preoperative surgical diagnosis using panoramic versus cone-beam CT images. J. Craniomaxillofac. Surg. 2016, 44, 1700–1705. [Google Scholar] [CrossRef]
- Tsapaki, V. Radiation protection in dental radiology—Recent advances and future directions. Phys. Medica 2017, 44, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Stratis, A.; Zhang, G.; Jacobs, R.; Bogaerts, R.; Bosmans, H. The growing concern of radiation dose in paediatric dental and maxillofacial CBCT: An easy guide for daily practice. Eur. Radiol. 2019, 29, 7009–7018. [Google Scholar] [CrossRef] [PubMed]
- Sodickson, A.; Baeyens, P.F.; Andriole, K.P.; Prevedello, L.; Nawfel, R.D.; Hanson, R.; Khorasani, R. Recurrent CT, Cumulative Radiation Exposure, and Associated Radiation-induced Cancer Risks from CT of Adults. Radiology 2009, 251, 175–184. [Google Scholar] [CrossRef] [PubMed]
- McGuigan, M.B.; Duncan, H.F.; Horner, K. An analysis of effective dose optimization and its impact on image quality and diagnostic efficacy relating to dental cone beam computed tomography (CBCT). Swiss Dent. J. 2018, 128, 297–316. [Google Scholar] [PubMed]
- Yeung, A.W.K.; Jacobs, R.; Bornstein, M.M. Novel low-dose protocols using cone beam computed tomography in dental medicine: A review focusing on indications, limitations, and future possibilities. Clin. Oral Investig. 2019, 23, 2573–2581. [Google Scholar] [CrossRef] [PubMed]
- Almadi, D.M.; Al-Hadlaq, M.A.; Alotaibi, O.; Alshagroud, R.S.; Al-Ekrish, A.A. Accuracy of mean grey density values obtained with small field of view cone beam computed tomography in differentiation between periapical cystic and solid lesions. Int. Endod. J. 2020, 53. [Google Scholar] [CrossRef]
- Al-Okshi, A.; Theodorakou, C.; Lindh, C. Dose optimization for assessment of periodontal structures in cone beam CT examinations. Dentomaxillofac. Radiol. 2017, 46, 20160311. [Google Scholar] [CrossRef]
- Döbelin, Q.; Stadlinger, B.; Wiedemeier, D.B.; Bichsel, D.; Rücker, M.; Valdec, S. Detectability of Osseous Lesions with a Pre-Programmed Low-Dose Protocol for Cone-Beam Computed Tomography. Appl. Sci. 2020, 10, 4961. [Google Scholar] [CrossRef]
- Wang, S.; Liu, Y.; Fang, D.; Shi, S. The miniature pig: A useful large animal model for dental and orofacial research. Oral Dis. 2007, 13, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Dentsply Sirona. Orthophos SL: Instruction Manual; Dentsply Sirona: Bensheim, Germany, 2018. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing [Computer Program]; R Foundation for Statistical Computing: Vienna, Austria, 2015; Available online: https://www.R-project.org/ (accessed on 28 August 2021).
- Kuznetsova, A.; Brockhoff, P.B.; Christensen, R.H.B. lmerTest Package: Tests in Linear Mixed EffectsModels. J. Stat. Softw. 2017, 82, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Lenth, R. Emmeans: Estimated Marginal Means, Aka Least-Squares Means [Computer Program]. R Package Version 1.2.3. 2018. Available online: https://CRAN.R-project.org/package=emmeans (accessed on 28 August 2021).
- Hartig, F. DHARMa: Residual Diagnostics for Hierarchical (Multi-Level/Mixed) Regression Models [Computer Program]. R Package Version 0.2.4. 2019. Available online: https://CRAN.R-project.org/package=DHARMa (accessed on 28 August 2021).
- Hedesiu, M.; Baciut, M.; Baciut, G.; Nackaerts, O.; Jacobs, R. Comparison of cone beam CT device and field of view for the detection of simulated periapical bone lesions. Dentomaxillofac. Radiol. 2012, 41, 548–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mardas, N.; Dereka, X.; Donos, N.; Dard, M. Experimental model for bone regeneration in oral and cranio-maxillo-facial surgery. J. Investig. Surg. 2014, 27, 32–49. [Google Scholar] [CrossRef]
- Oenning, A.C.C.; Jacobs, R.; Pauwels, R.; Stratis, A.; Hedesiu, M.; Salmon, B. Cone-beam CT in paediatric dentistry: DIMITRA project position statement. Pediatr. Radiol. 2017, 48, 308–316. [Google Scholar] [CrossRef]
- White, S.C.; Scarfe, W.C.; Schulze, R.K.; Lurie, A.G.; Douglass, J.M.; Farman, A.G.; Law, C.S.; Levin, M.D.; Sauer, R.A.; Valachovic, R.W.; et al. The Image Gently in Dentistry campaign: Promotion of responsible use of maxillofacial radiology in dentistry for children. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, 257–261. [Google Scholar] [CrossRef] [Green Version]
- Stoetzer, M.; Nickel, F.; Rana, M.; Lemound, J.; Wenzel, D.; Von See, C.; Gellrich, N.-C. Advances in assessing the volume of odontogenic cysts and tumors in the mandible: A retrospective clinical trial. Head Face Med. 2013, 9, 14. [Google Scholar] [CrossRef] [Green Version]
- Sacher, C.; Holzinger, D.; Grogger, P.; Wagner, F.; Sperl, G.; Seemann, R. Calculation of postoperative bone healing of cystic lesions of the jaw-a retrospective study. Clin. Oral Investig. 2019, 23, 3951–3957. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Li, L.; Shi, J.; Tu, J.; Niu, L.; Hu, X. Positional Changes of Mandibular Canal Before and After Decompression of Cystic Lesions in the Mandible. J. Oral Maxillofac. Surg. 2021, 79, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Buchbender, M.; Neukam, F.W.; Lutz, R.; Schmitt, C.M. Treatment of enucleated odontogenic jaw cysts: A systematic review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Yüzügüllü, B.; Araz, K. Validity of conventional surgical treatment methods for mandibular dentigerous cysts. Two case reports. N. Y. State Dent. J. 2011, 77, 36–39. [Google Scholar]
- Prabhusankar, K.; Yuvaraj, A.; Prakash, C.A.; Parthiban, J.; Praveen, B. CBCT Cyst Leasions Diagnosis Imaging Mandible Maxilla. J. Clin. Diagn. Res. 2014, 8, ZD03-5. [Google Scholar] [CrossRef]
- Mozzo, P.; Procacci, C.; Tacconi, A.; Martini, P.T.; Andreis, I.A.B. A new volumetric CT machine for dental imaging based on the cone-beam technique: Preliminary results. Eur. Radiol. 1998, 8, 1558–1564. [Google Scholar] [CrossRef]
- Visser, H.; Hermann, K.P.; Bredemeier, S.; Köhler, B. Dose measurements comparing conventional and digital panoramic radiography. Mund Kiefer Gesichtschir. 2000, 4, 213–216. [Google Scholar] [CrossRef] [PubMed]
- Ghaeminia, H.; Meijer, G.; Soehardi, A.; Borstlap, W.; Mulder, J.; Bergé, S. Position of the impacted third molar in relation to the mandibular canal. Diagnostic accuracy of cone beam computed tomography compared with panoramic radiography. Int. J. Oral Maxillofac. Surg. 2009, 38, 964–971. [Google Scholar] [CrossRef] [PubMed]
- Harris, D.; Horner, K.; Gröndahl, K.; Jacobs, R.; Helmrot, E.; Benic, G.I.; Bornstein, M.M.; Dawood, A.; Quirynen, M.E.A.O. guidelines for the use of diagnostic imaging in implant dentistry 2011. A consensus workshop organized by the European Association for Osseointegration at the Medical University of Warsaw. Clin. Oral Implants Res. 2012, 23, 1243–1253. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, R.; Zhang, G.; Theodorakou, C.; Walker, A.; Bosmans, H.; Jacobs, R.; Bogaerts, R.; Horner, K.; The SEDENTEXCT Project Consortium. Effective radiation dose and eye lens dose in dental cone beam CT: Effect of field of view and angle of rotation. Br. J. Radiol. 2014, 87, 20130654. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mode | FOV (cm) | kV/mA | Radiation Time (s) | Voxel Size (µm) | Effective Dose (µSv) |
|---|---|---|---|---|---|
| LD | 11 × 10 | 85/13 | 2.2 | 160 | 20 |
| SD | 11 × 10 | 85/13 | 4.4 | 160 | 145 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Haj Husain, A.; Döbelin, Q.; Giacomelli-Hiestand, B.; Wiedemeier, D.B.; Stadlinger, B.; Valdec, S. Diagnostic Accuracy of Cystic Lesions Using a Pre-Programmed Low-Dose and Standard-Dose Dental Cone-Beam Computed Tomography Protocol: An Ex Vivo Comparison Study. Sensors 2021, 21, 7402. https://0-doi-org.brum.beds.ac.uk/10.3390/s21217402
Al-Haj Husain A, Döbelin Q, Giacomelli-Hiestand B, Wiedemeier DB, Stadlinger B, Valdec S. Diagnostic Accuracy of Cystic Lesions Using a Pre-Programmed Low-Dose and Standard-Dose Dental Cone-Beam Computed Tomography Protocol: An Ex Vivo Comparison Study. Sensors. 2021; 21(21):7402. https://0-doi-org.brum.beds.ac.uk/10.3390/s21217402
Chicago/Turabian StyleAl-Haj Husain, Adib, Quirin Döbelin, Barbara Giacomelli-Hiestand, Daniel B. Wiedemeier, Bernd Stadlinger, and Silvio Valdec. 2021. "Diagnostic Accuracy of Cystic Lesions Using a Pre-Programmed Low-Dose and Standard-Dose Dental Cone-Beam Computed Tomography Protocol: An Ex Vivo Comparison Study" Sensors 21, no. 21: 7402. https://0-doi-org.brum.beds.ac.uk/10.3390/s21217402