
An Adaptive Multi-Modal Control Strategy to Attenuate the Limb Position Effect in Myoelectric Pattern Recognition


Abstract
:1. Introduction
2. Materials and Methods
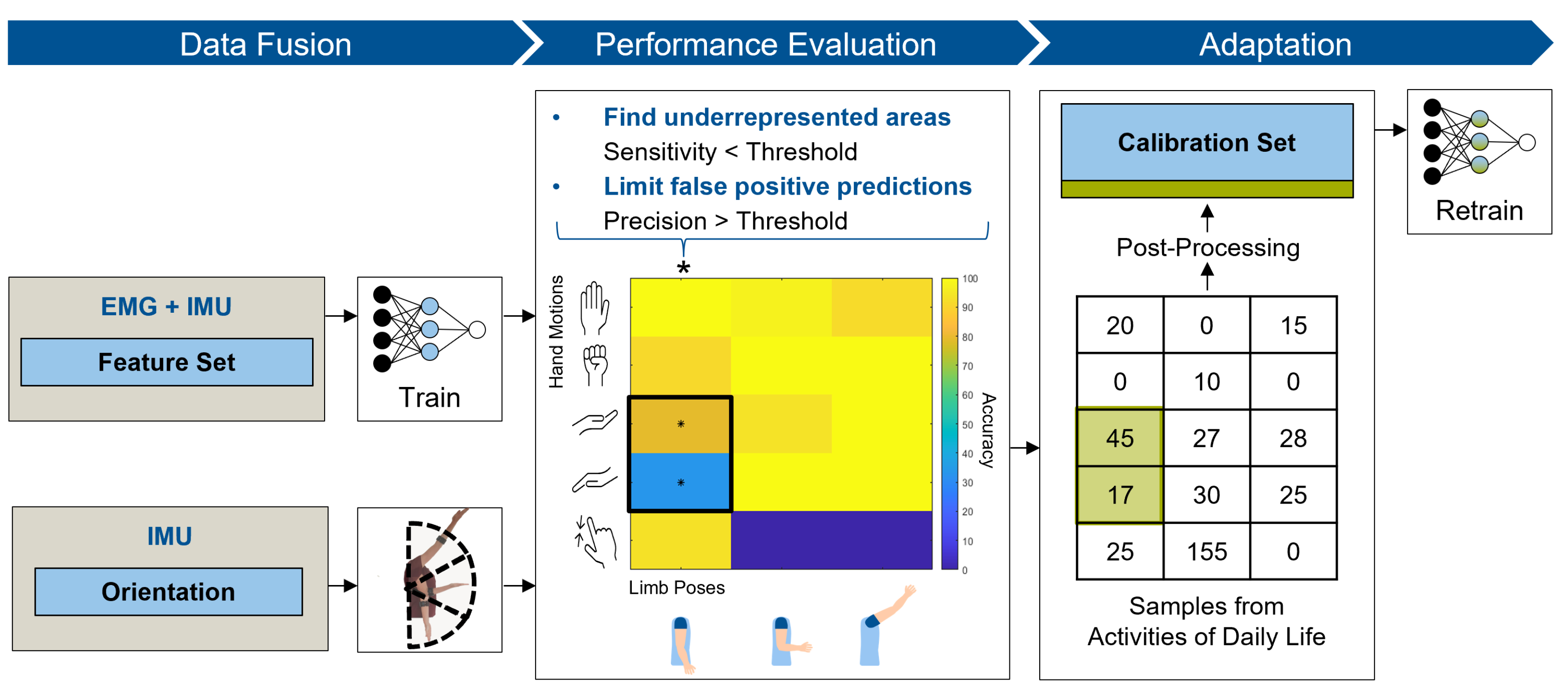
2.1. Multi-Modal Adaptive Algorithm
2.1.1. Data Fusion
- X rotation, as the orientation of the forearm;
- Y rotation, as flexion of the shoulder and/or the elbow and;
- Z rotation, as abduction of the shoulder and/or the elbow.
2.1.2. Performance Evaluation
2.1.3. Adaptation
2.2. Experimental Validation
2.2.1. Participants
2.2.2. Data Collection
- Completion rate, the relative amount of completed target motions;
- Completion time, the time required to reach the target position;
- Selection time, the time until the desired target hand motion is classified for the first time.
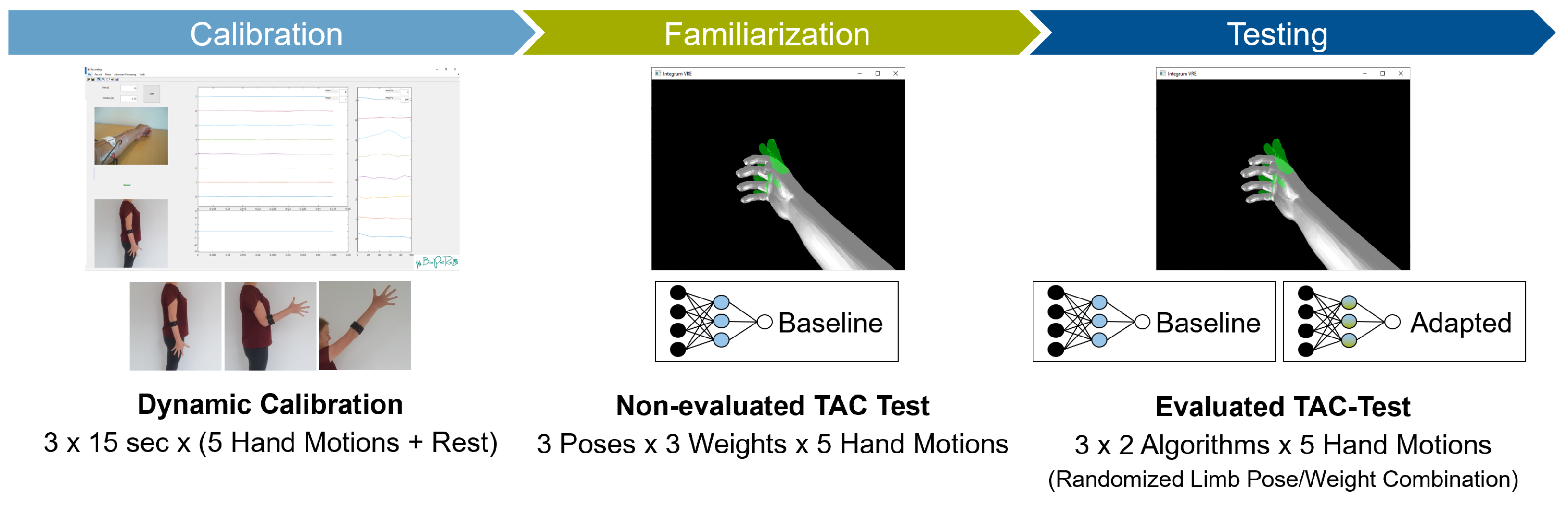
2.3. Experimental Protocol
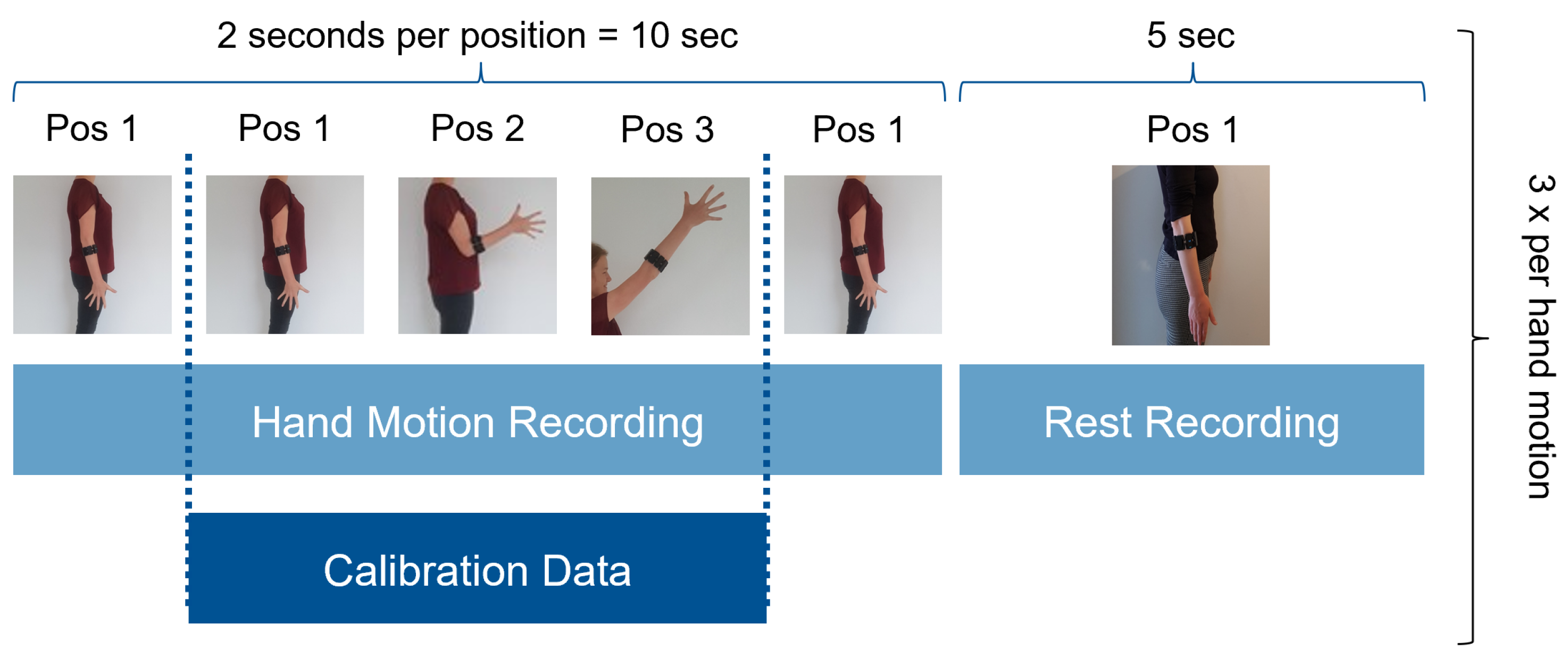
- Initial calibration, conducted dynamically. Figure 10 shows the order of instructed limb poses per hand motion. A video of the dynamic routine covering the identified limb poses guided the participants to reach and maintain a specific hand motion. Each hand motion was conducted continuously for 10 s, followed by a 5 s rest period. Within the hand motion recording, limb position instructions changed every 2 s. The aim was to record 2 s in each of the three predefined limb positions. To account for the subject’s reaction time, pose 1 was added in front and the end of the hand motion recording. Only the middle 6 s of the recording were stored as calibration dataset and labeled with the instructed hand motion. This procedure was repeated three times for all six hand motions, resulting in 18 s of labeled data per class. The recorded dataset was processed and used to train a baseline model.
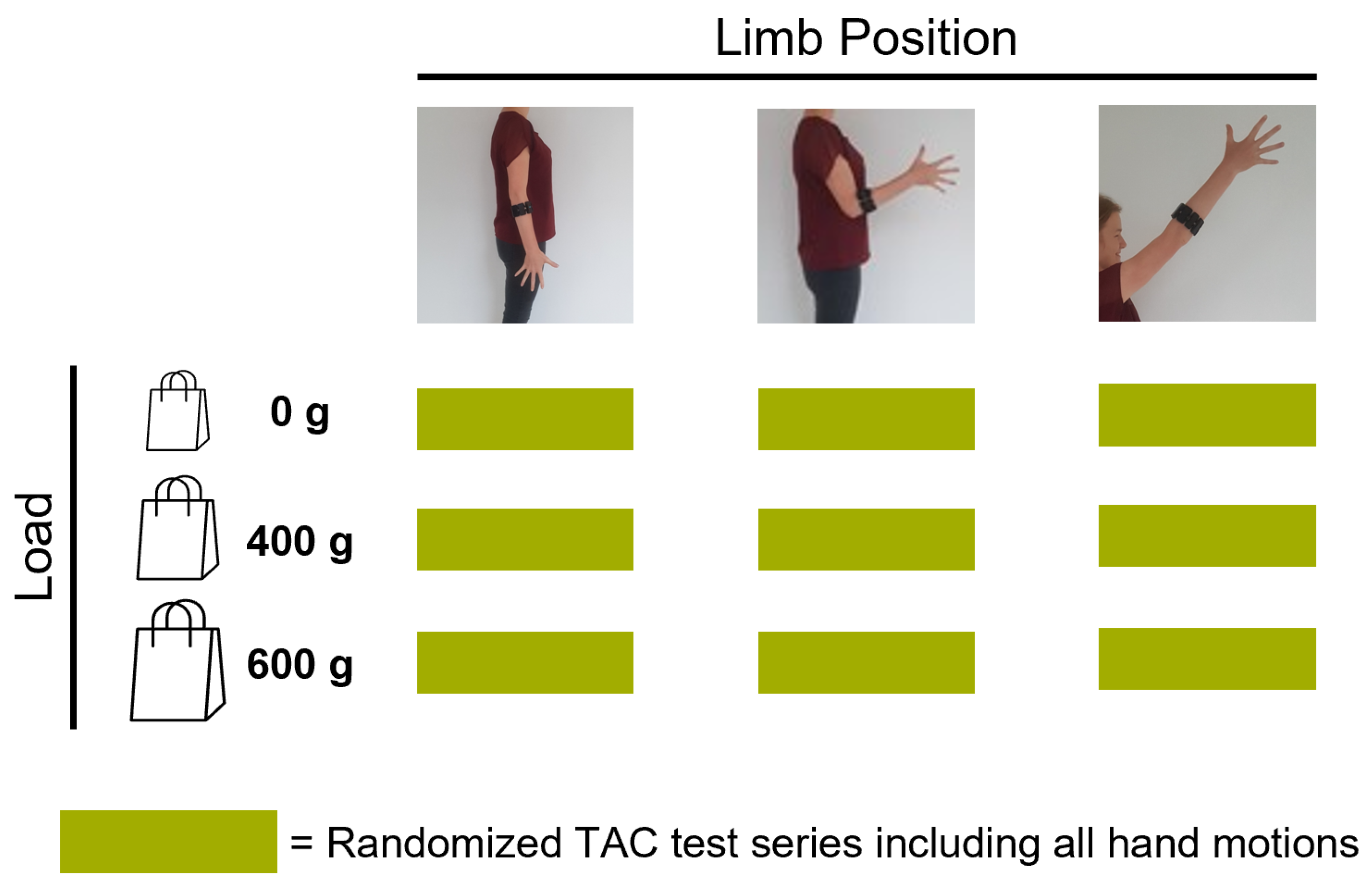
- Familiarization, where the subject was familiarized with the virtual environment by performing multiple series of TAC tests (one series is defined as five target displacements covering all predefined hand motions, excluding rest, in randomized order). Within the familiarization phase, external loads were added to simulate an unknown confounding factor during daily usage. EMG and IMU data were recorded and used to selectively adapt the calibration dataset (Section 2.1). Figure 11 shows the different variations of limb position and external loads applied. For each combination of limb position and external load, a series of TAC tests covering all hand motions was conducted. This resulted in nine repetitions of five targets with a maximum duration (timeout) of 15 s each, leading to a maximum total duration of 11 min and 15 s. At the end of the familiarization, a new classifier was trained based on the new calibration set. Before starting the testing phase, a five minute break was included to avoid fatigue.
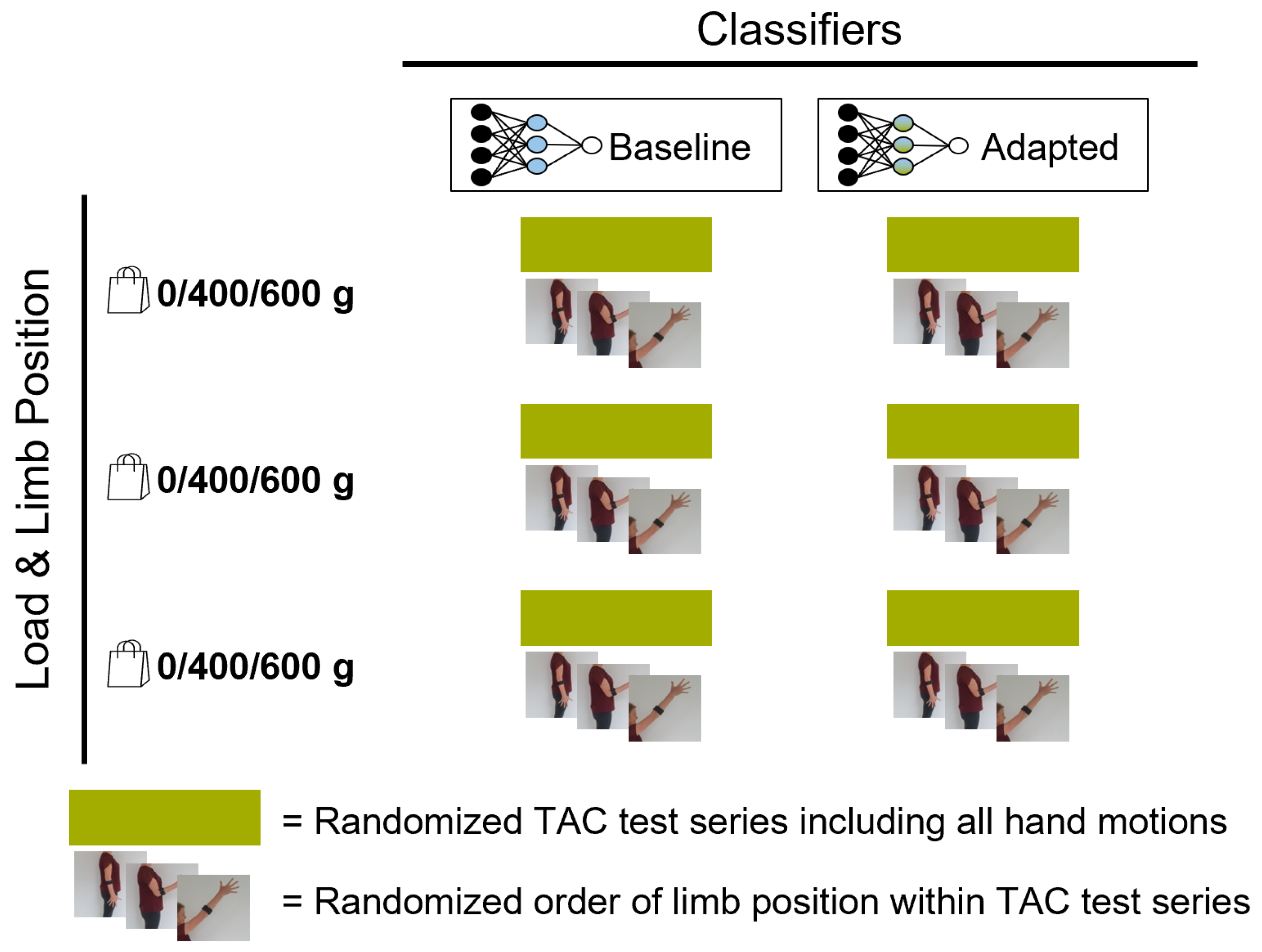
- Testing, where the baseline model and an adapted model were tested using the TAC test. Each hand motion was tested for both classifiers multiple times, and each variation in limb pose and external load was covered. Figure 12 presents the combination of TAC test series conducted during the testing phase. Each classifier was tested three times, in randomized alternating order. After completing a TAC series with both algorithms, the test recording was paused and a different variation of external load was applied. The order of weight variations, limb poses and hand motions was randomized for each pair of TAC series. The maximum total recording time for the testing phase was 7 min and 30 s (six tests with a maximum completion time of 75 s).
2.4. Data Processing
3. Results
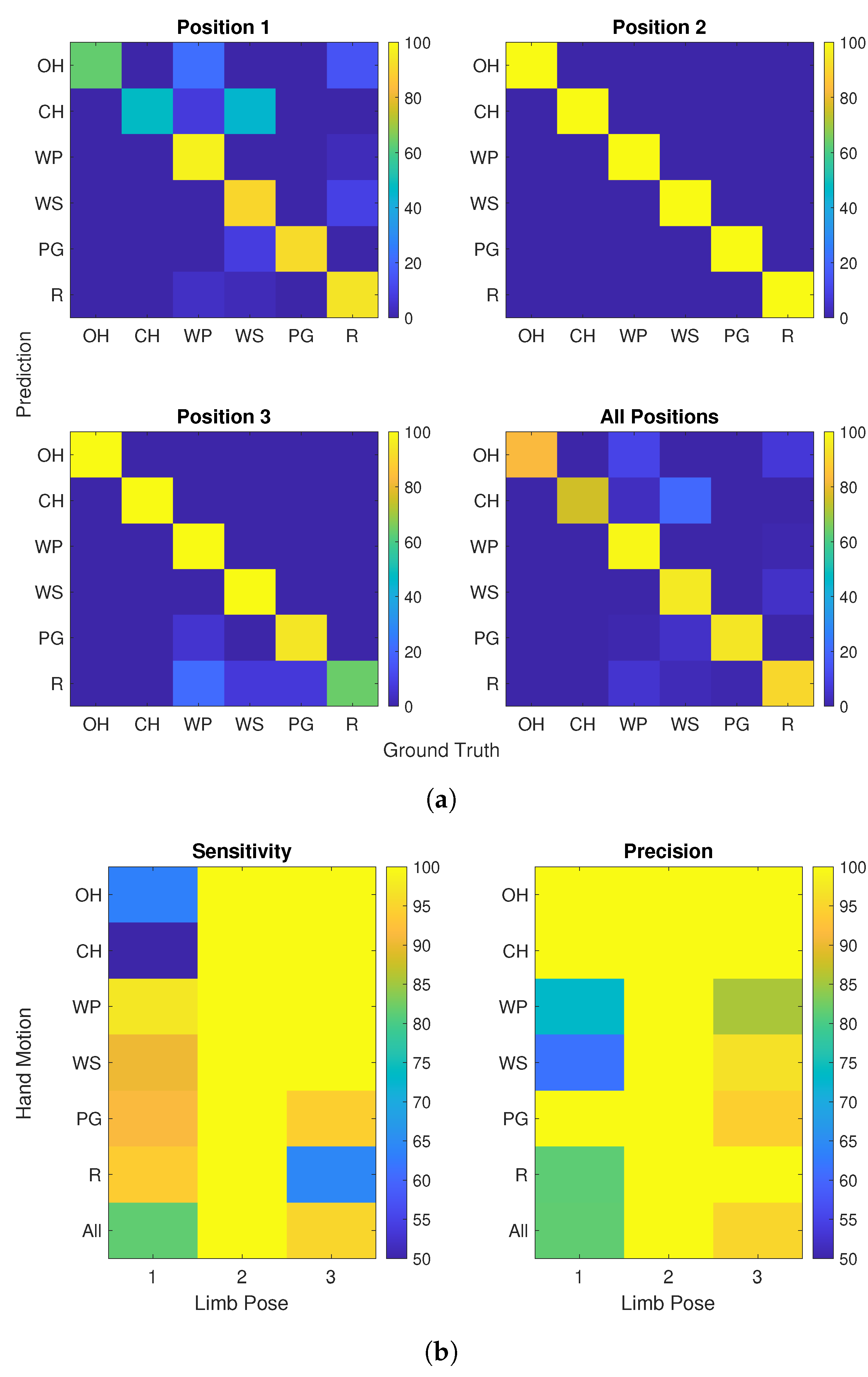
3.1. Limb Pose Estimation
3.2. Precision and Sensitivity
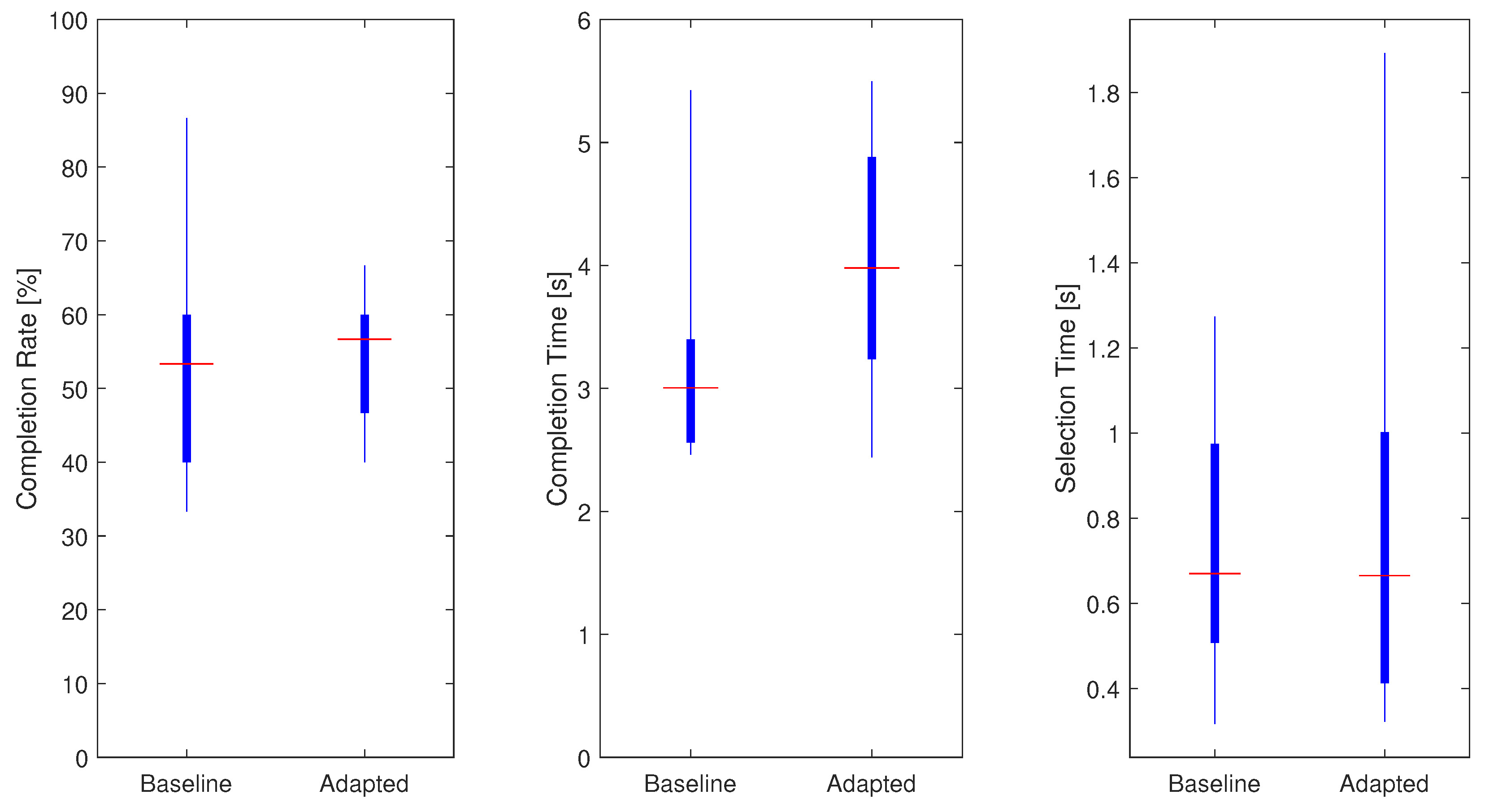
3.3. TAC Test Results—MAIN Evaluation Measures
3.4. TAC Test Results—Hand Motion Specific
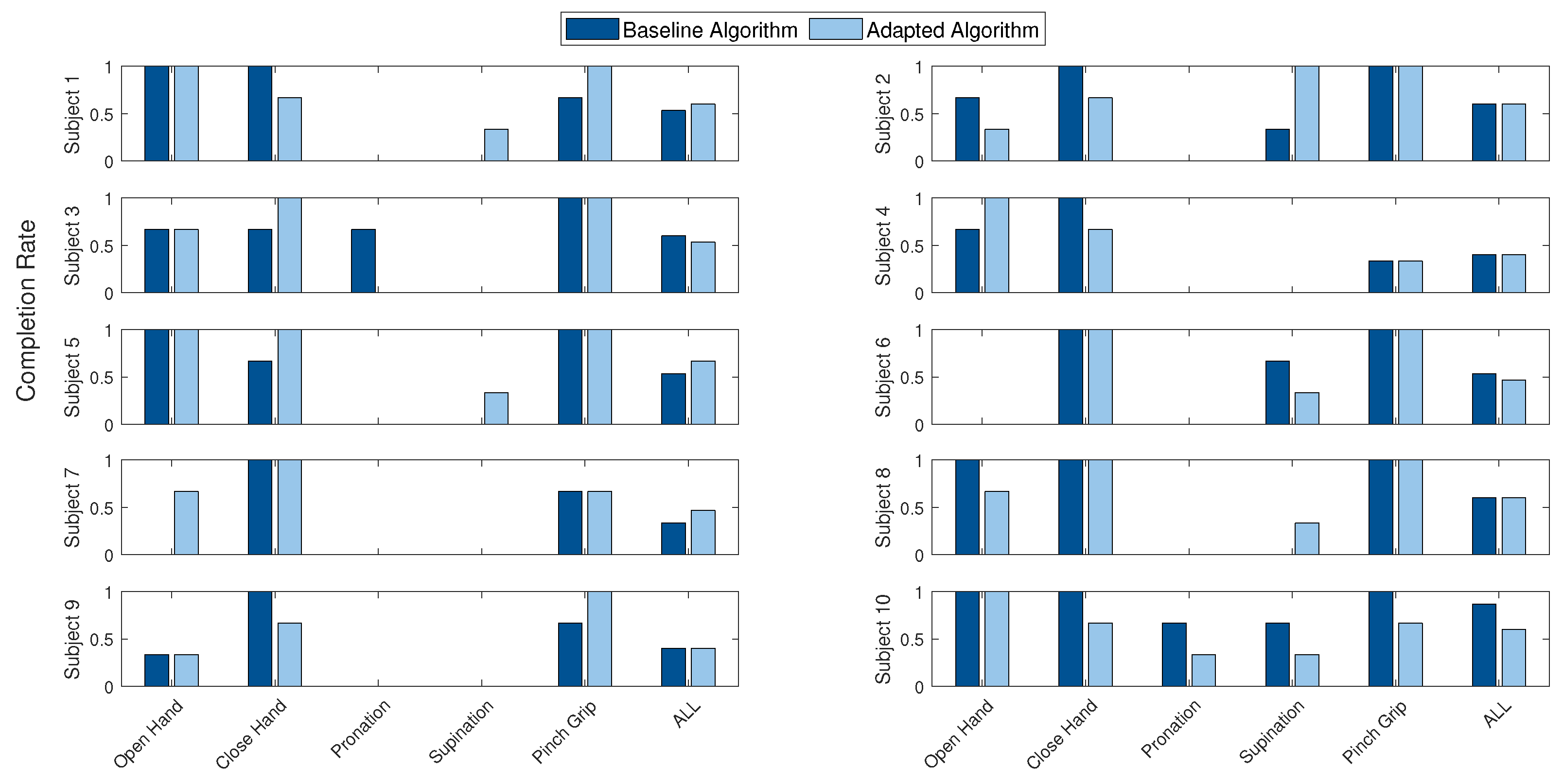
3.5. TAC Test Results—Subject Specific
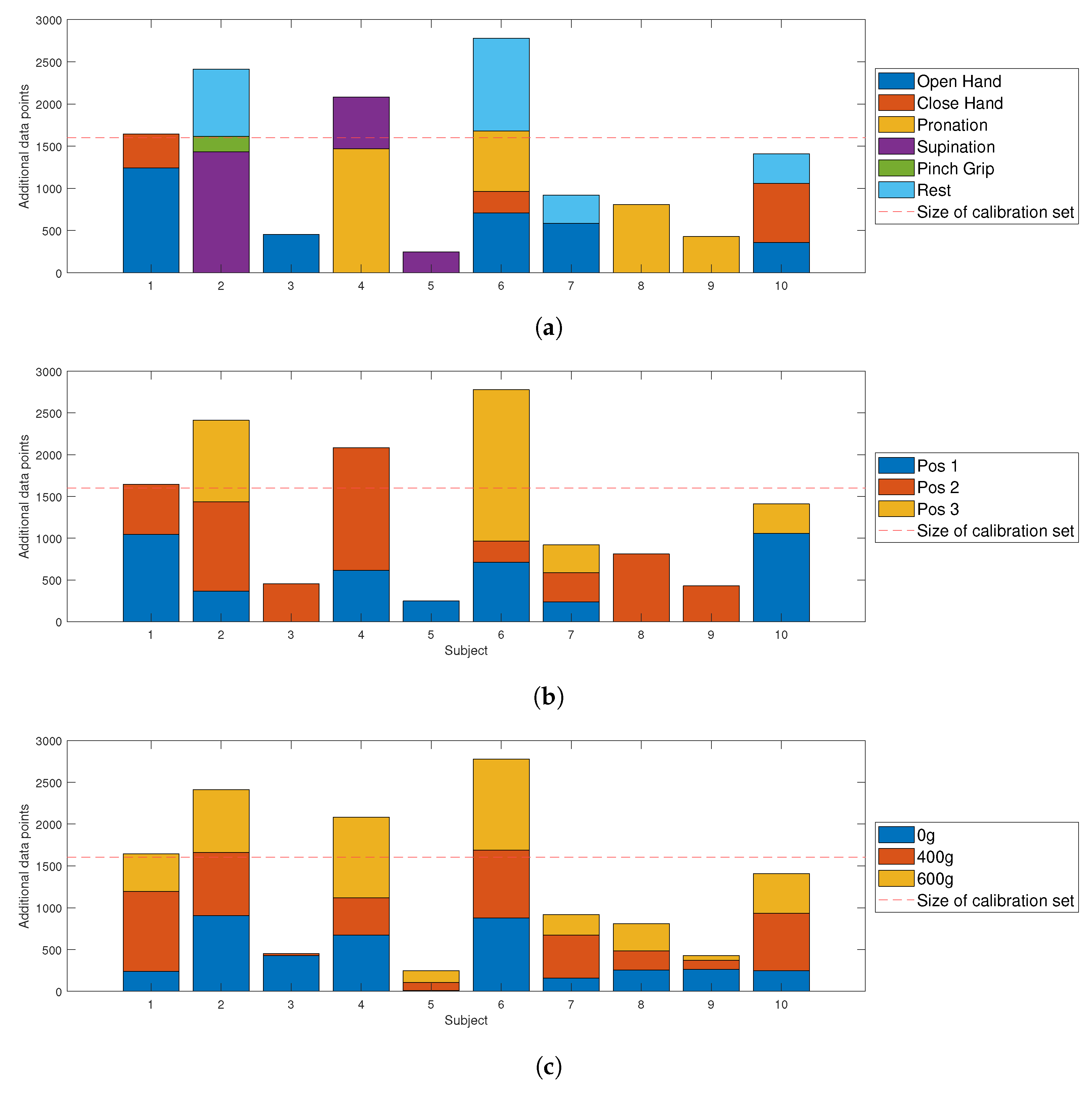
3.6. Adaptation—Overall
3.7. Adaptation—Subject Specific
4. Discussion and Conclusions
4.1. General Performance
4.2. Hand Motion Performance
4.3. The Influence of External Loads
4.4. Quality and Quantity of Adaptation Set
4.5. Evaluation Measures
4.6. Study Limitations and Future Work
- The amount of training data could influence the computation time of the algorithm. While the LDA itself is computationally efficient [72], a larger training dataset requires more time for the computation.
- Data included during the adaptation process may influence the class boundaries negatively. As mentioned in [35], an excessive amount of data is not necessarily beneficial because it may lead to over-fitting.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Farina, D.; Vujaklija, I.; Brånemark, R.; Bull, A.M.J.; Dietl, H.; Graimann, B.; Hargrove, L.J.; Hoffmann, K.-P.; Huang, H.H.; Ingvarsson, T.; et al. Toward higher-performance bionic limbs for wider clinical use. Nat. Biomed. Eng. 2021, 1–13. [Google Scholar] [CrossRef]
- Össur. iLimb Hand Prosthesis. Available online: https://www.ossur.com/ (accessed on 30 September 2021).
- Ottobock, Bebionic Hand Prosthesis. Available online: https://www.ottobockus.com/prosthetics/upper-limb-prosthetics/solution-overview/bebionic-hand/ (accessed on 30 September 2021).
- Taska, Taska Hand Prosthesis. Available online: https://www.taskaprosthetics.com/ (accessed on 30 September 2021).
- Mendez, V.; Iberite, F.; Shokur, S.; Micera, S. Current Solutions and Future Trends for Robotic Prosthetic Hands. Annu. Rev. Control Robot. Auton. Syst. 2021, 4, 595–627. [Google Scholar] [CrossRef]
- Cordella, F.; Ciancio, A.L.; Sacchetti, R.; Davalli, A.; Cutti, A.G.; Guglielmelli, E.; Zollo, L. Literature Review on Needs of Upper Limb Prosthesis Users. Front. Neurosci. 2016, 10, 209. [Google Scholar] [CrossRef]
- Smail, L.C.; Neal, C.; Wilkins, C.; Packham, T.L. Comfort and function remain key factors in upper limb prosthetic abandonment: Findings of a scoping review. Disabil. Rehabil. Assist. Technol. 2020, 16, 821–830. [Google Scholar] [CrossRef] [PubMed]
- Roche, A.D.; Rehbaum, H.; Farina, D.; Aszmann, O.C. Prosthetic Myoelectric Control Strategies: A Clinical Perspective. Curr. Surg. Rep. 2014, 2, 1–11. [Google Scholar] [CrossRef]
- Oskoei, M.A.; Hu, H. Myoelectric control systems—A survey. Biomed. Signal Process. Control 2007, 2, 275–294. [Google Scholar] [CrossRef]
- Hahne, J.M.; Biessmann, F.; Jiang, N.; Rehbaum, H.; Farina, D.; Meinecke, F.C.; Müller, K.-R.; Parra, L.C. Linear and nonlinear regression techniques for simultaneous and proportional myoelectric control. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.H.; Kuiken, T.A.; Hargrove, L.J. Evaluation of linear regression simultaneous myoelectric control using intramuscular EMG. IEEE Trans. Biomed. Eng. 2015, 63, 737–746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheme, E.; Englehart, K. Electromyogram pattern recognition for control of powered upper-limb prostheses: State of the art and challenges for clinical use. J. Rehabil. Res. Dev. 2011, 48, 643–659. [Google Scholar] [CrossRef] [PubMed]
- Naidu, D.; Chen, C.-H.; Perez, A.; Schoen, M.P. Control strategies for smart prosthetic hand technology: An overview. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; pp. 4314–4317. [Google Scholar]
- Huang, Y.; Englehart, K.B.; Hudgins, B.; Chan, A.D.C. A Gaussian mixture model based classification scheme for myoelectric control of powered upper limb prostheses. IEEE Trans. Biomed. Eng. 2005, 52, 1801–1811. [Google Scholar] [CrossRef] [PubMed]
- Hargrove, L.J.; Englehart, K.; Hudgins, B. A comparison of surface and intramuscular myoelectric signal classification. IEEE Trans. Biomed. Eng. 2007, 54, 847–853. [Google Scholar] [CrossRef]
- Atzori, M.; Gijsberts, A.; Castellini, C.; Caputo, B.; Hager, A.-G.M.; Elsig, S.; Giatsidis, G.; Bassetto, F.; Müller, H. Electromyography data for non-invasive naturally-controlled robotic hand prostheses. Sci. Data 2014, 1, 140053. [Google Scholar] [CrossRef] [Green Version]
- Ottobock, Myo Plus Pattern Recognition. Available online: https://www.ottobockus.com/prosthetics/upper-limb-prosthetics/solution-overview/myo-plus/myo-plus.html (accessed on 30 September 2021).
- CoApt LLC. Available online: https://www.coaptengineering.com/ (accessed on 30 September 2021).
- Li, G. Electromyography pattern-recognition-based control of powered multifunctional upper-limb prostheses. Adv. Appl Electromyogr. 2011, 6, 99–116. [Google Scholar]
- Batzianoulis, I.; Krausz, N.E.; Simon, A.M.; Hargrove, L.; Billard, A. Decoding the grasping intention from electromyography during reaching motions. J. Neuroeng. Rehabil. 2018, 15, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Resnik, L.; Huang, H.H.; Winslow, A.; Crouch, D.L.; Zhang, F.; Wolk, N. Evaluation of EMG pattern recognition for upper limb prosthesis control: A case study in comparison with direct myoelectric control. J. Neuroeng. Rehabil. 2018, 15, 23. [Google Scholar] [CrossRef] [PubMed]
- Englehart, K.; Hudgins, B. A robust, real-time control scheme for multifunction myoelectric control. IEEE Trans. Biomed. Eng. 2003, 50, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Al-Timemy, A.H.; Khushaba, R.N.; Bugmann, G.; Escudero, J. Improving the performance against force variation of EMG controlled multifunctional upper-limb prostheses for transradial amputees. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 24, 650–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, N.; Farina, D. Myoelectric Control of Upper Limb Prosthesis: Current Status, Challenges and Recent Advances. Presented at the MERIDIAN 30M Workshop, Brixen, Italy, 25 September 2014. [Google Scholar]
- Rodríguez-Tapia, B.; Soto, I.; Martínez, D.M.; Arballo, N.C. Myoelectric interfaces and related applications: Current state of EMG signal processing–A systematic review. IEEE Access 2020, 8, 7792–7805. [Google Scholar] [CrossRef]
- Chen, L.; Geng, Y.; Li, G. Effect of upper-limb positions on motion pattern recognition using electromyography. In Proceedings of the 2011 4th International Congress on Image and Signal Processing, Shanghai, China, 15–17 October 2011. [Google Scholar]
- Khushaba, R.N.; Al-Timemy, A.; Kodagoda, S.; Nazarpour, K. Combined influence of forearm orientation and muscular contraction on EMG pattern recognition. Expert Syst. Appl. 2016, 61, 154–161. [Google Scholar] [CrossRef] [Green Version]
- Castellini, C.; Fiorilla, A.E.; Sandini, G. Multi-subject/daily-life activity EMG-based control of mechanical hands. J. Neuroeng. Rehabil. 2009, 6, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teh, Y.; Hargrove, L.J. Understanding Limb Position and External Load Effects on Real-Time Pattern Recognition Control in Amputees. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 1605–1613. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Gu, Y.; Jiang, L.; Osborn, L.; Liu, H. Dynamic training protocol improves the robustness of PR-based myoelectric control. Biomed. Signal Process. Control 2017, 31, 249–256. [Google Scholar] [CrossRef]
- Fougner, A.; Scheme, E.; Chan, A.D.C.; Englehart, K.; Stavdahl, Ø. Resolving the limb position effect in myoelectric pattern recognition. IEEE Trans. Neural Syst. Rehabil. Eng. 2011, 19, 644–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boschmann, A.; Platzner, M. Towards robust HD EMG pattern recognition: Reducing electrode displacement effect using structural similarity. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014. [Google Scholar]
- Radmand, A.; Scheme, E.; Englehart, K. On the suitability of integrating accelerometry data with electromyography signals for resolving the effect of changes in limb position during dynamic limb movement. JPO J. Prosthetics Orthot. 2014, 26, 185–193. [Google Scholar] [CrossRef]
- Campbell, E.; Phinyomark, A.; Scheme, E. Current trends and confounding factors in myoelectric control: Limb position and contraction intensity. Sensors 2020, 20, 1613. [Google Scholar] [CrossRef] [Green Version]
- Sensinger, J.W.; Lock, B.A.; Kuiken, T.A. Adaptive pattern recognition of myoelectric signals: Exploration of conceptual framework and practical algorithms. IEEE Trans. Neural Syst. Rehabil. Eng. 2009, 17, 270–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franzke, A.W.; Kristoffersen, M.B.; Bongers, R.M.; Murgia, A.; Pobatschnig, B.; Unglaube, F.; van der Sluis, C.K. Users’ and therapists’ perceptions of myoelectric multi-function upper limb prostheses with conventional and pattern recognition control. PLoS ONE 2019, 14, e0220899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khushaba, R.N.; Takruri, M.; Miro, J.V.; Kodagoda, S. Towards limb position invariant myoelectric pattern recognition using time-dependent spectral features. Neural Netw. 2014, 55, 42–58. [Google Scholar] [CrossRef]
- Rajapriya, R.; Rajeswari, K.; Joshi, D.; Thiruvengadam, S.J. Forearm Orientation and Contraction Force Independent Method for EMG-Based Myoelectric Prosthetic Hand. IEEE Sens. J. 2021, 21, 6623–6633. [Google Scholar] [CrossRef]
- Scheme, E.; Fougner, A.; Stavdahl, Ø.; Chan, A.D.; Englehart, K. (Eds.) Examining the Adverse Effects of Limb Position on Pattern Recognition Based Myoelectric Control. In Proceedings of the 32th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Buenos Aires, Argentina, 31 August–4 September 2010. [Google Scholar]
- Geng, Y.; Zhou, P.; Li, G. Toward attenuating the impact of arm positions on electromyography pattern-recognition based motion classification in transradial amputees. J. Neuroeng. Rehabil. 2012, 9, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodward, R.B.; Hargrove, L.J. Adapting myoelectric control in real-time using a virtual environment. J. Neuroeng. Rehabil. 2019, 16, 11. [Google Scholar] [CrossRef]
- Jung, M.C.; Chai, R.; Zheng, J.; Nguyen, H. Enhanced myoelectric control against arm position change with weighted recursive Gaussian process. Neural Comput. Appl. 2021, 1–14. [Google Scholar] [CrossRef]
- Vidovic, M.M.-C.; Hwang, H.-J.; Amsuss, S.; Hahne, J.M.; Farina, D.; Muller, K.-R. Improving the Robustness of Myoelectric Pattern Recognition for Upper Limb Prostheses by Covariate Shift Adaptation. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 24, 961–970. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhang, D.; Zhu, X. Application of a self-enhancing classification method to electromyography pattern recognition for multifunctional prosthesis control. J. Neuroeng. Rehabil. 2013, 10, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, X.; Liu, J.; Zhang, D.; Sheng, X.; Jiang, N. Cascaded Adaptation Framework for Fast Calibration of Myoelectric Control. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Betthauser, J.L.; Hunt, C.L.; Osborn, L.E.; Masters, M.R.; Lévay, G.; Kaliki, R.R.; Thakor, N.V. Limb position tolerant pattern recognition for myoelectric prosthesis control with adaptive sparse representations from extreme learning. IEEE Trans. Biomed. Eng. 2017, 65, 770–778. [Google Scholar] [CrossRef]
- Simon, A.M.; Hargrove, L.J.; Lock, B.A.; Kuiken, T.A. The target achievement control test: Evaluating real-time myoelectric pattern recognition control of a multifunctional upper-limb prosthesis. J. Rehabil. Res. Dev. 2011, 48, 619. [Google Scholar] [CrossRef]
- Radmand, A.; Scheme, E.; Englehart, K. A characterization of the effect of limb position on EMG features to guide the development of effective prosthetic control schemes. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014. [Google Scholar]
- Parajuli, N.; Sreenivasan, N.; Bifulco, P.; Cesarelli, M.; Savino, S.; Niola, V.; Esposito, D.; Hamilton, T.J.; Naik, G.R.; Gunawardana, U. Real-time EMG based pattern recognition control for hand prostheses: A review on existing methods, challenges and future implementation. Sensors 2019, 19, 4596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rezazadeh, I.M.; Firoozabadi, M.; Hu, H.; Golpayegani, S.M.R.H. Co-adaptive and affective human–machine interface for improving training performances of virtual myoelectric forearm prosthesis. IEEE Trans. Affect. Comput. 2012, 3, 285–297. [Google Scholar] [CrossRef]
- Hassan, H.F.; Abou-Loukh, S.J.; Ibraheem, I.K. Teleoperated robotic arm movement using electromyography signal with wearable Myo armband. J. King Saud Univ.—Eng. Sci. 2020, 32, 378–387. [Google Scholar] [CrossRef]
- Pizzolato, S.; Tagliapietra, L.; Cognolato, M.; Reggiani, M.; Müller, H.; Atzori, M. Comparison of six electromyography acquisition setups on hand movement classification tasks. PLoS ONE 2017, 12, e0186132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortiz-Catalan, M.; Brånemark, R.; Håkansson, B. BioPatRec: A modular research platform for the control of artificial limbs based on pattern recognition algorithms. Source Code Biol. Med. 2013, 8, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gusman, J.; Mastinu, E.; Ortiz-Catalan, M. Evaluation of Computer-Based Target Achievement Tests for Myoelectric Control. IEEE J. Transl. Eng. Health Med. 2017, 5, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.; Huang, H. A robust model-based neural-machine interface across different loading weights applied at distal forearm. Biomed. Signal Process. Control 2021, 67, 102509. [Google Scholar] [CrossRef]
- Ameri, A.; Akhaee, M.A.; Scheme, E.; Englehart, K. Real-time, simultaneous myoelectric control using a convolutional neural network. PLoS ONE 2018, 13, e0203835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beaulieu, R.J.; Masters, M.R.; Betthauser, J.; Smith, R.J.; Kaliki, R.; Thakor, N.V.; Soares, A.B. Multi-position training improves robustness of pattern recognition and reduces limb-position effect in prosthetic control. J. Prosthetics Orthot. JPO 2017, 29, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khezri, M.; Jahed, M. Real-time intelligent pattern recognition algorithm for surface EMG signals. BioMed. Eng. Online 2007, 6, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samuel, O.W.; Li, X.; Fang, P.; Li, G. Examining the effect of subjects’ mobility on upper-limb motion identification based on EMG-pattern recognition. In Proceedings of the 2016 Asia-Pacific Conference on Intelligent Robot Systems (ACIRS 2016), Tokyo, Japan, 20–22 July 2016; pp. 137–141. [Google Scholar] [CrossRef]
- Hudgins, B.; Parker, P.; Scott, R.N. A new strategy for multifunction myoelectric control. IEEE Trans. Biomed. Eng. 1993, 40, 82–94. [Google Scholar] [CrossRef] [PubMed]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Fang, Y.; Hettiarachchi, N.; Zhou, D.; Liu, H. Multi-modal sensing techniques for interfacing hand prostheses: A review. IEEE Sens. J. 2015, 15, 6065–6076. [Google Scholar] [CrossRef] [Green Version]
- Gordon, K.D.; Pardo, R.D.; Johnson, J.A.; King, G.J.W.; Miller, T.A. Electromyographic activity and strength during maximum isometric pronation and supination efforts in healthy adults. J. Orthop. Res. 2004, 22, 208–213. [Google Scholar] [CrossRef]
- Coscia, M.; Cheung, V.C.K.; Tropea, P.; Koenig, A.; Monaco, V.; Bennis, C.; Micera, S.; Bonato, P. The effect of arm weight support on upper limb muscle synergies during reaching movements. J. Neuroeng. Rehabil. 2014, 11, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farina, D.; Jiang, N.; Rehbaum, H.; Holobar, A.; Graimann, B.; Dietl, H.; Aszmann, O.C. The extraction of neural information from the surface EMG for the control of upper-limb prostheses: Emerging avenues and challenges. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 797–809. [Google Scholar] [CrossRef] [PubMed]
- Atzori, M.; Gijsberts, A.; Kuzborskij, I.; Elsig, S.; Hager, A.-G.M.; Deriaz, O.; Castellini, C.; Muller, H.; Caputo, B. Characterization of a benchmark database for myoelectric movement classification. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 73–83. [Google Scholar] [CrossRef]
- He, J.; Zhang, D.; Jiang, N.; Sheng, X.; Farina, D.; Zhu, X. User adaptation in long-term, open-loop myoelectric training: Implications for EMG pattern recognition in prosthesis control. J. Neural Eng. 2015, 12, 46005. [Google Scholar] [CrossRef] [PubMed]
- Amsüss, S.; Paredes, L.P.; Rudigkeit, N.; Graimann, B.; Herrmann, M.J.; Farina, D. Long term stability of surface EMG pattern classification for prosthetic control. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 3622–4615. [Google Scholar]
- Amsüss, S.; Goebel, P.M.; Jiang, N.; Graimann, B.; Paredes, L.; Farina, D. Self-correcting pattern recognition system of surface EMG signals for upper limb prosthesis control. IEEE Trans. Biomed. Eng. 2013, 61, 1167–1176. [Google Scholar] [CrossRef]
- Ding, Q.; Zhao, X.; Han, J.; Bu, C.; Wu, C. Adaptive Hybrid Classifier for Myoelectric Pattern Recognition Against the Interferences of Outlier Motion, Muscle Fatigue, and Electrode Doffing. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 1071–1080. [Google Scholar] [CrossRef] [PubMed]
- Hargrove, L.; Losier, Y.; Lock, B.; Englehart, K.; Hudgins, B. A Real-Time Pattern Recognition Based Myoelectric Control Usability Study Implemented in a Virtual Environment. In Proceedings of the 2007 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007. [Google Scholar]
- Gu, Y.; Yang, D.; Huang, Q.; Yang, W.; Liu, H. Robust EMG pattern recognition in the presence of confounding factors: Features, classifiers and adaptive learning. Expert Syst. Appl. 2018, 96, 208–217. [Google Scholar] [CrossRef]
- Fukuda, O.; Tsuji, T.; Kaneko, M.; Otsuka, A. A human-assisting manipulator teleoperated by EMG signals and arm motions. IEEE Trans. Robot. Automat. 2003, 19, 210–222. [Google Scholar] [CrossRef] [Green Version]
- Liu, J. Adaptive myoelectric pattern recognition toward improved multifunctional prosthesis control. Med. Eng. Phys. 2015, 37, 424–430. [Google Scholar] [CrossRef]
- Hargrove, L.; Englehart, K.; Hudgins, B. The effect of electrode displacements on pattern recognition based myoelectric control. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 2203–3625. [Google Scholar] [CrossRef]




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Abbreviation | Value |
|---|---|---|
| Minimum sensitivity | 90% | |
| Minimum precision | 90% | |
| Majority voting segment length | 5 samples |
| Subject | Age | Gender | Forearm Length (in cm) | Absolute Myo Position (in cm) | Relative Myo Position | Tightness (No. of Clips) |
|---|---|---|---|---|---|---|
| 1 | 25 | m | 27 | 5.5 | 0.20 | 2 |
| 2 | 23 | w | 26 | 5 | 0.19 | 4 |
| 3 | 34 | m | 26 | 5.5 | 0.21 | 2 |
| 4 | 35 | m | 27 | 4 | 0.15 | 4 |
| 5 | 32 | m | 27 | 6.5 | 0.24 | 2 |
| 6 | 30 | w | 26 | 4.5 | 0.17 | 6 |
| 7 | 30 | w | 26.5 | 5 | 0.19 | 6 |
| 8 | 23 | w | 25 | 6 | 0.24 | 6 |
| 9 | 29 | m | 29 | 4 | 0.14 | 2 |
| 10 | 30 | m | 28 | 7 | 0.25 | 0 |
| Pos 1 | Pos 2 | Pos 3 | |
|---|---|---|---|
| Range |
| Limb Pose | 1 | 2 | 3 | Total |
|---|---|---|---|---|
| Absolute [samples] | 4278 | 5432 | 3476 | 13,186 |
| Relative | 0.32 | 0.41 | 0.26 | 1.0 |
| External Load | 0 g | 400 g | 600 g | Total |
|---|---|---|---|---|
| Absolute [samples] | 4064 | 4628 | 4494 | 13,186 |
| Relative | 0.31 | 0.35 | 0.34 | 1.0 |
| Hand Motion | r | Total | |||||
|---|---|---|---|---|---|---|---|
| Absolute [samples] | 3350 | 1355 | 3424 | 2297 | 182 | 2578 | 13,186 |
| Relative | 0.25 | 0.10 | 0.26 | 0.17 | 0.02 | 0.2 | 1.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spieker, V.; Ganguly, A.; Haddadin, S.; Piazza, C. An Adaptive Multi-Modal Control Strategy to Attenuate the Limb Position Effect in Myoelectric Pattern Recognition. Sensors 2021, 21, 7404. https://0-doi-org.brum.beds.ac.uk/10.3390/s21217404
Spieker V, Ganguly A, Haddadin S, Piazza C. An Adaptive Multi-Modal Control Strategy to Attenuate the Limb Position Effect in Myoelectric Pattern Recognition. Sensors. 2021; 21(21):7404. https://0-doi-org.brum.beds.ac.uk/10.3390/s21217404
Chicago/Turabian StyleSpieker, Veronika, Amartya Ganguly, Sami Haddadin, and Cristina Piazza. 2021. "An Adaptive Multi-Modal Control Strategy to Attenuate the Limb Position Effect in Myoelectric Pattern Recognition" Sensors 21, no. 21: 7404. https://0-doi-org.brum.beds.ac.uk/10.3390/s21217404