
Effects of Central and Peripheral Fatigue on Impact Characteristics during Running

 ,
,  ,
,  and
and
Abstract
:
1. Introduction
- We compared the impact acceleration response to fatigue under two well-stabilized protocols to allow us to understand the response after the central and peripheral fatigue situations.
- We compared the two methods to analyze the impact acceleration, time, and frequency analysis, which showed that the frequency-domain was the best option to detect fatigue-related changes.
- We present here that central fatigue increases the severity of impact acceleration, and propose to include these kinds of protocols in future studies focus on the identification of factors related to running-related injuries (RRIs).
2. Materials and Methods
2.1. Participants
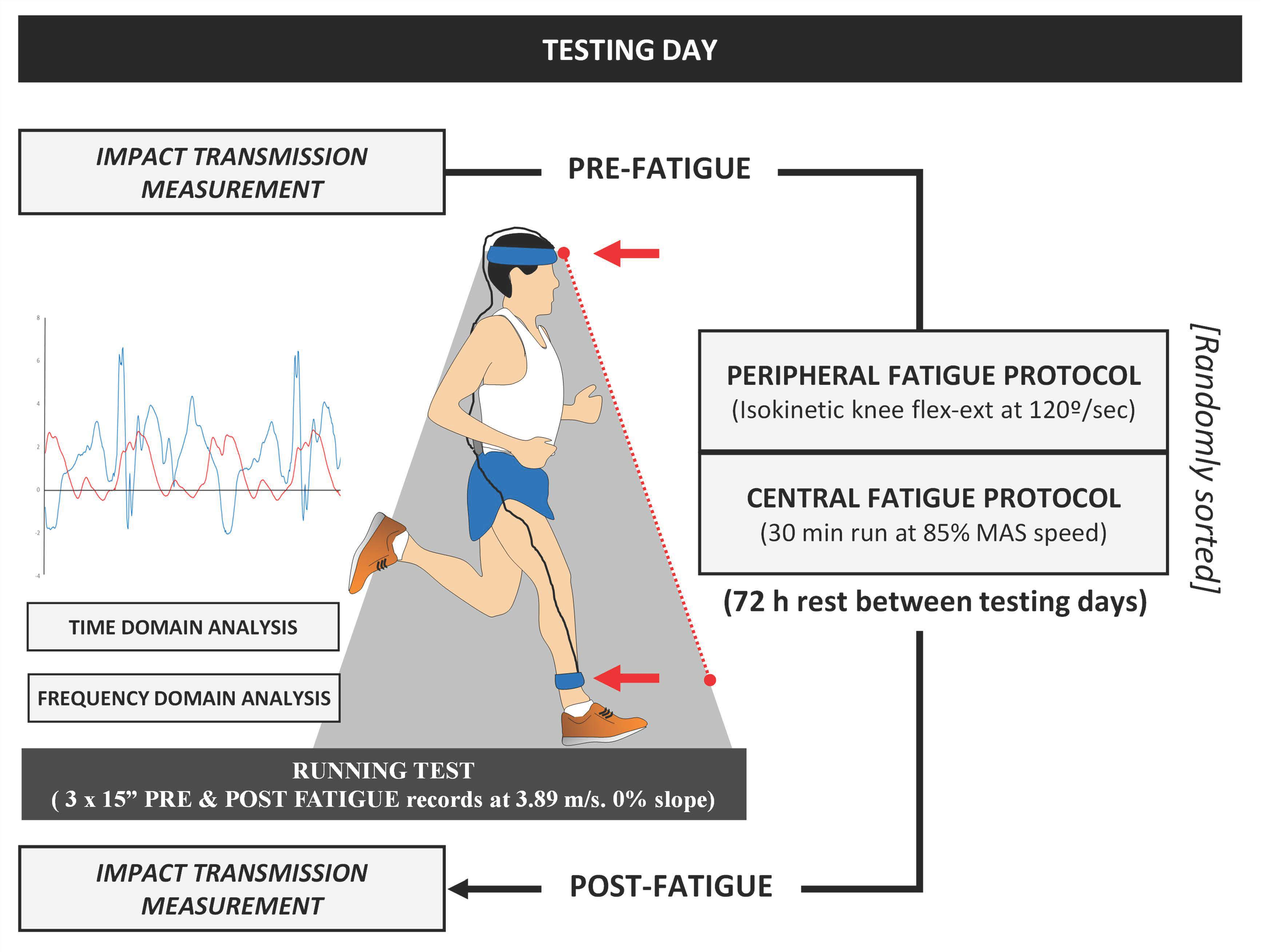
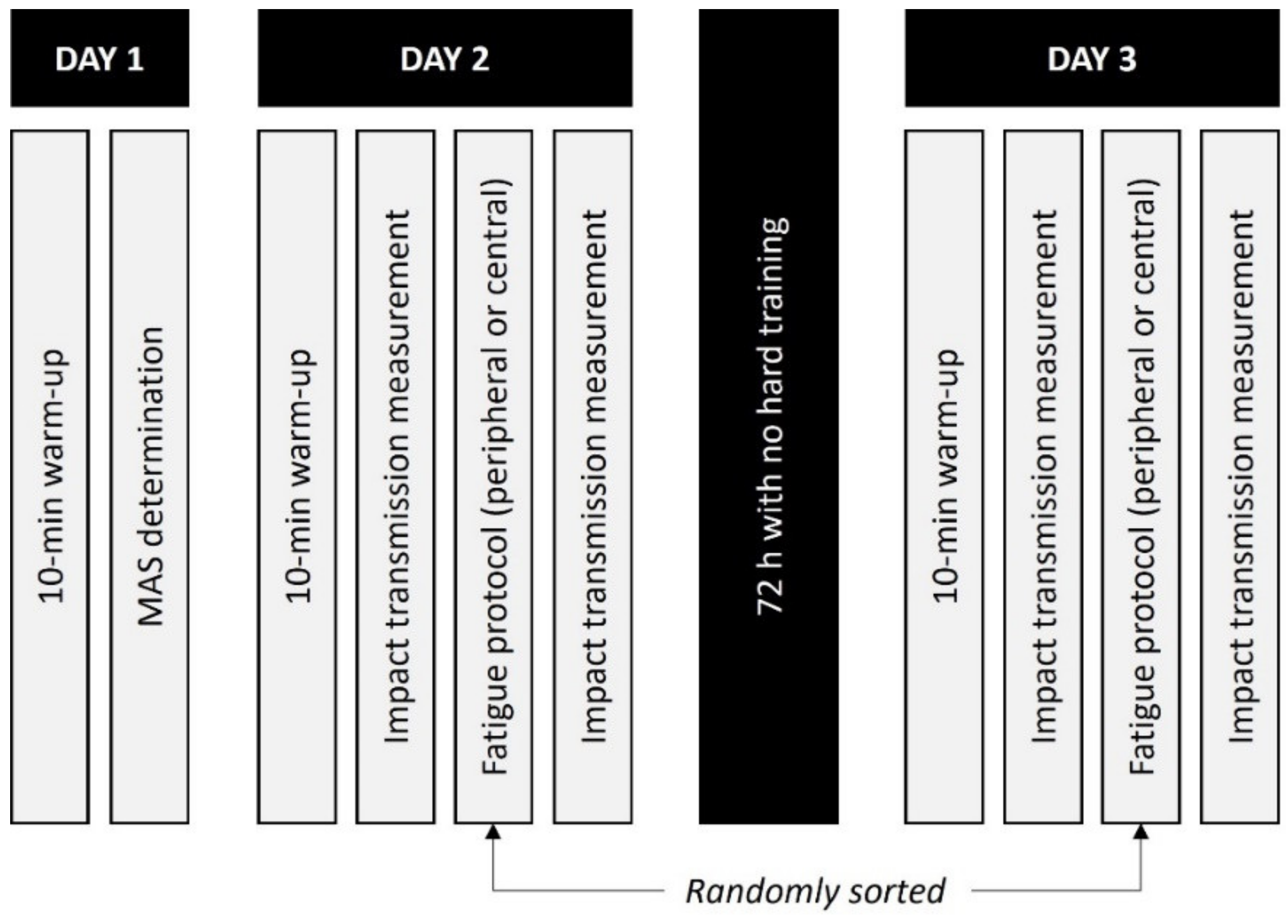
2.2. Experimental Protocol
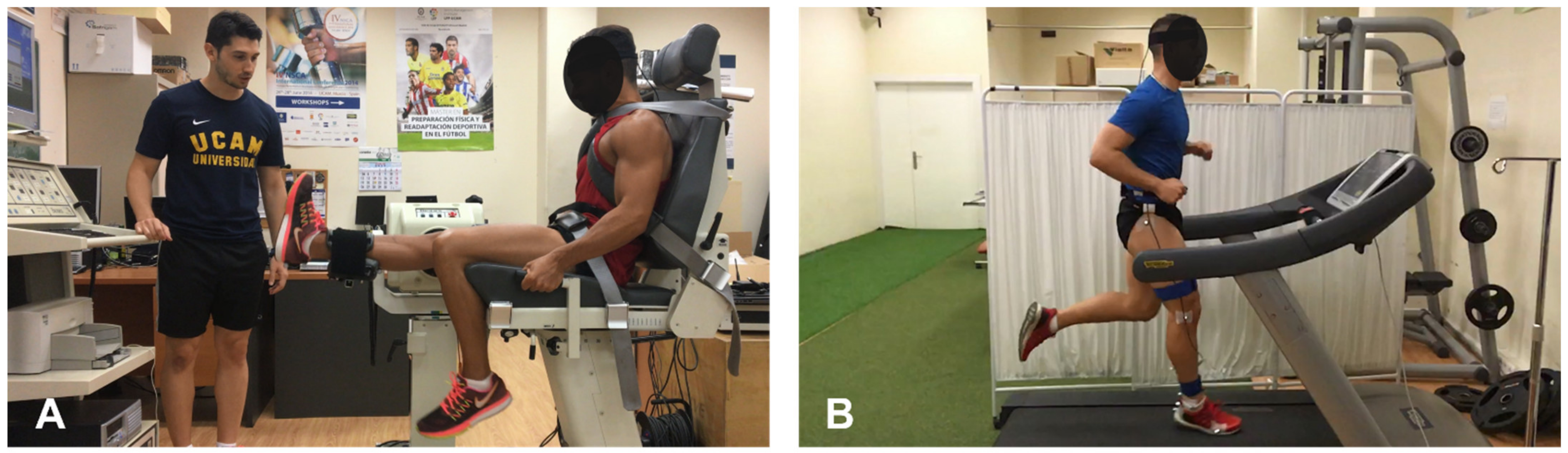
2.2.1. Central Fatigue Protocol
2.2.2. Peripheral Fatigue Protocol
2.3. Data Analysis
2.4. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fields, K.B.; Sykes, J.C.; Walker, K.M.; Jackson, J.C. Prevention of Running Injuries. Curr. Sports Med. Rep. 2010, 9, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Abt, J.P.; Sell, T.C.; Chu, Y.; Lovalekar, M.; Burdett, R.G.; Lephart, S.M. Running Kinematics and Shock Absorption Do Not Change after Brief Exhaustive Running. J. Strength Cond. Res. 2011, 25, 1479–1485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derrick, T.R.; Dereu, D.; Mclean, S.P. Impacts and Kinematic Adjustments during an Exhaustive Run. Med. Sci. Sports Exerc. 2002, 34, 998–1002. [Google Scholar] [CrossRef] [PubMed]
- Hamill, J.; Derrick, T.R.; Holt, K.G. Shock Attenuation and Stride Frequency during Running. Hum. Mov. Sci. 1995, 14, 45–60. [Google Scholar] [CrossRef]
- Encarnación-Martínez, A.; García-Gallart, A.; Gallardo, A.M.; Sánchez-Sáez, J.A.; Sánchez-Sánchez, J. Effects of Structural Components of Artificial Turf on the Transmission of Impacts in Football Players. Sports Biomech. 2018, 17, 251–260. [Google Scholar] [CrossRef]
- Gruber, A.H.; Boyer, K.A.; Derrick, T.R.; Hamill, J. Impact Shock Frequency Components and Attenuation in Rearfoot and Forefoot Running. J. Sport Health Sci. 2014, 3, 113–121. [Google Scholar] [CrossRef]
- Mercer, J.A.; Bates, B.T.; Dufek, J.S.; Hreljac, A. Characteristics of Shock Attenuation during Fatigued Running. J. Sports Sci. 2003, 21, 911–919. [Google Scholar] [CrossRef]
- Mizrahi, J.; Verbitsky, O.; Isakov, E. Shock Accelerations and Attenuation in Downhill and Level Running. Clin. Biomech. 2000, 15, 15–20. [Google Scholar] [CrossRef]
- Mizrahi, J.; Verbitsky, O.; Isakov, E.; Daily, D. Effect of Fatigue on Leg Kinematics and Impact Acceleration in Long Distance Running. Hum. Mov. Sci. 2000, 19, 139–151. [Google Scholar] [CrossRef]
- Verbitsky, O.; Mizrahi, J.; Voloshin, A.; Treiger, J.; Isakov, E. Shock Transmission and Fatigue in Human Running. J. Appl. Biomech. 1998, 14, 300–311. [Google Scholar] [CrossRef] [Green Version]
- Lucas-Cuevas, A.G.; Priego-Quesada, J.I.; Aparicio, I.; Giménez, J.V.; Llana-Belloch, S.; Pérez-Soriano, P. Effect of 3 Weeks Use of Compression Garments on Stride and Impact Shock during a Fatiguing Run. Int. J. Sports Med. 2015, 36, 826–831. [Google Scholar] [CrossRef] [PubMed]
- Millet, G.Y. Can Neuromuscular Fatigue Explain Running Strategies and Performance in Ultra-Marathons? The Flush Model. Sports Med. 2011, 41, 489–506. [Google Scholar] [CrossRef] [PubMed]
- García-Pérez, J.A.; Pérez-Soriano, P.; Llana Belloch, S.; Lucas-Cuevas, Á.G.; Sánchez-Zuriaga, D. Effects of Treadmill Running and Fatigue on Impact Acceleration in Distance Running. Sports Biomech. 2014, 13, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Voloshin, A.S.; Mizrahi, J.; Verbitsky, O.; Isakov, E. Dynamic Loading on the Human Musculoskeletal System–Effect of Fatigue. Clin. Biomech. 1998, 13, 515–520. [Google Scholar] [CrossRef]
- Mizrahi, J.; Verbitsky, O.; Isakov, E. Fatigue-Related Loading Imbalance on the Shank in Running: A Possible Factor in Stress Fractures. Ann. Biomed. Eng. 2000, 28, 463–469. [Google Scholar] [CrossRef]
- Christina, K.A.; White, S.C.; Gilchrist, L.A. Effect of Localized Muscle Fatigue on Vertical Ground Reaction Forces and Ankle Joint Motion during Running. Hum. Mov. Sci. 2001, 20, 257–276. [Google Scholar] [CrossRef]
- Marotta, L.; Scheltinga, B.L.; van Middelaar, R.; Bramer, W.M.; van Beijnum, B.-J.F.; Reenalda, J.; Buurke, J.H. Accelerometer-Based Identification of Fatigue in the Lower Limbs during Cyclical Physical Exercise: A Systematic Review. Sensors 2022, 22, 3008. [Google Scholar] [CrossRef]
- Shorten, M.R.; Winslow, D.S. Spectral Analysis of Impact Shock during Running. Int. J. Sport Biomech. 1992, 8, 288–304. [Google Scholar] [CrossRef]
- Berthon, P.; Fellmann, N.; Bedu, M.; Beaune, B.; Dabonneville, M.; Coudert, J.; Chamoux, A. A 5-Min Running Field Test as a Measurement of Maximal Aerobic Velocity. Eur. J. Appl. Physiol. Occup. Physiol. 1997, 75, 233–238. [Google Scholar] [CrossRef]
- Lussiana, T.; Gindre, C.; Mourot, L.; Hebert-Losier, K. Do Subjective Assessments of Running Patterns Reflect Objective Parameters? Eur. J. Sport Sci. 2017, 17, 847–857. [Google Scholar] [CrossRef]
- Lucas-Cuevas, A.G.; Pérez-Soriano, P.; Llana-Belloch, S.; Macián-Romero, C.; Sánchez-Zuriaga, D. Effect of Custom-Made and Prefabricated Insoles on Plantar Loading Parameters during Running with and without Fatigue. J. Sports Sci. 2014, 32, 1712–1721. [Google Scholar] [CrossRef]
- Ziegert, J.C.; Lewis, J.L. The Effect of Soft Tissue on Measurements of Vibrational Bone Motion by Skin-Mounted Accelerometers. J. Biomech. Eng. 1979, 101, 218–220. [Google Scholar] [CrossRef]
- Lucas-Cuevas, A.G.; Encarnación-Martínez, A.; Camacho-García, A.; Llana-Belloch, S.; Pérez-Soriano, P. The Location of the Tibial Accelerometer Does Influence Impact Acceleration Parameters during Running. J. Sports Sci. 2017, 35, 1734–1738. [Google Scholar] [CrossRef]
- Carroll, T.J.; Taylor, J.L.; Gandevia, S.C. Recovery of Central and Peripheral Neuromuscular Fatigue after Exercise. J. Appl. Physiol. 2017, 122, 1068–1076. [Google Scholar] [CrossRef] [Green Version]
- Hafer, J.F.; Brown, A.M.; Boyer, K.A. Exertion and Pain Do Not Alter Coordination Variability in Runners with Iliotibial Band Syndrome. Clin. Biomech. 2017, 47, 73–78. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical Bases of Perceived Exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Kellis, E.; Zafeiridis, A.; Amiridis, I.G. Muscle Coactivation before and after the Impact Phase of Running Following Isokinetic Fatigue. J. Athl. Train. 2011, 46, 11–19. [Google Scholar] [CrossRef] [Green Version]
- Soleimanifar, M.; Salavati, M.; Akhbari, B.; Moghadam, M. The Interaction between the Location of Lower Extremity Muscle Fatigue and Visual Condition on Unipedal Postural Stability. Eur. J. Appl. Physiol. 2012, 112, 3495–3502. [Google Scholar] [CrossRef]
- Mercer, J.A.; Vance, J.; Hreljac, A.; Hamill, J. Relationship between Shock Attenuation and Stride Length during Running at Different Velocities. Eur. J. Appl. Physiol. 2002, 87, 403–408. [Google Scholar] [CrossRef]
- Cohen, J. A Power Primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Hunter, J.E.; Schmidt, F.L. Methods of Meta-Analysis. Correcting Error and Bias in Research Findings; Sage: Thousand Oaks, CA, USA, 2004. [Google Scholar]
- Sawilowsky, S.S. New Effect Size Rules of Thumb. J. Mod. Appl. Stat. Methods 2009, 8, 597–599. [Google Scholar] [CrossRef]
- Derrick, T.R.; Hamill, J.; Caldwell, G.E. Energy Absorption of Impacts during Running at Various Stride Lengths. Med. Sci. Sports Exerc. 1998, 30, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Brüggemann, G.P.; Arndt, A.; Kersting, U.G.; Knicker, A.J. Influence of Fatigue on Impact Force and Rearfoot Motion during Running. In Proceedings of the XVth Congress of the International Society of Biomechanics, Jyväskylä, Finland, 2–6 July 1995; pp. 132–133. [Google Scholar]
- Gerritsen, K.G.; van den Bogert, A.J.; Nigg, B.M. Direct Dynamics Simulation of the Impact Phase in Heel-Toe Running. J. Biomech. 1995, 28, 661–668. [Google Scholar] [CrossRef]
- Nicol, C.; Komi, P.V.; Marconnet, P. Fatigue Effects of Marathon Running on Neuromuscular Performance: I. Changes in Muscle Force and Stiffness Characteristics. Scand. J. Med. Sci. Sports 1991, 1, 10–17. [Google Scholar] [CrossRef]
- Willson, J.D.; Kernozek, T.W. Plantar Loading and Cadence Alterations with Fatigue. Med. Sci. Sports Exerc. 1999, 31, 1828–1833. [Google Scholar] [CrossRef]
- Potthast, W.; Brüggemann, G.-P.; Lundberg, A.; Arndt, A. The Influences of Impact Interface, Muscle Activity, and Knee Angle on Impact Forces and Tibial and Femoral Accelerations Occurring after External Impacts. J. Appl. Biomech. 2010, 26, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Boccia, G.; Dardanello, D.; Tarperi, C.; Festa, L.; La Torre, A.; Pellegrini, B.; Schena, F.; Rainoldi, A. Women Show Similar Central and Peripheral Fatigue to Men after Half-Marathon. Eur. J. Sport Sci. 2018, 18, 695–704. [Google Scholar] [CrossRef]
- Martin, V.; Kerherve, H.; Messonnier, L.A.; Banfi, J.C.; Geyssant, A.; Bonnefoy, R.; Feasson, L.; Millet, G.Y. Central and Peripheral Contributions to Neuromuscular Fatigue Induced by a 24-h Treadmill Run. J. Appl. Physiol. 2010, 108, 1224–1233. [Google Scholar] [CrossRef]
- Thomas, K.; Goodall, S.; Stone, M.; Howatson, G.; St Clair Gibson, A.; Ansley, L. Central and Peripheral Fatigue in Male Cyclists after 4-, 20-, and 40-Km Time Trials. Med. Sci. Sports Exerc. 2015, 47, 537–546. [Google Scholar] [CrossRef]
- Cataneo, D.C.; Kobayasi, S.; De Carvalho, L.R.; Paccanaro, R.C.; Cataneo, A.J.M. Accuracy of Six Minute Walk Test, Stair Test and Spirometry Using Maximal Oxygen Uptake as Gold Standard. Acta Cirúrgica Bras. 2010, 25, 194–200. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Peripheral Fatigue | Central Fatigue | |||||
|---|---|---|---|---|---|---|
| Pre-Fatigue | Post-Fatigue | Δ | Pre-Fatigue | Post-Fatigue | Δ | |
| PAH (g) § | 1.44 (0.09) | 1.36 (0.08) | −0.085 (0.179) | 1.36 (0.07) | 1.27 (0.1) | −0.087 (0.168) |
| RAH (g) § | 1.86 (0.14) | 2.05 (0.11) | 0.167 (0.495) | 1.87 (0.11) | 1.85 (0.1) | −0.109 (0.454) |
| PAT (g) § | 5.71 (0.45) | 5.38 (0.37) | −0.321 (1.267) | 5.73 (0.59) | 5.91 (0.67) | 0.146 (1.256) |
| RAT (g) § | 7.24 (0.53) | 7.01 (0.45) | −0.237 (1.416) | 7.23 (0.62) | 7.37 (0.74) | 0.096 (1.296) |
| MIA (%) | 73.71 (1.53) | 73.77 (2.02) | −0.055 (5.900) | 73.89 (2.13) | 75.86 (2.35) | 1.972 (5.614) |
| Peripheral Fatigue | Central Fatigue | |||||
|---|---|---|---|---|---|---|
| Pre-Fatigue | Post-Fatigue | Δ | Pre-Fatigue | Post-Fatigue | Δ | |
| Stride Frequency (Hz) | 177.18 (2.48) | 176.65 (2.47) | −0.526 (0.959) | 176.39 (2.34) | 174.89 (2.14) | −1.503 (1.407) |
| Stride Length (m) | 2.63 (0.145) | 2.63 (0.145) | 0.006 (0.054) | 2.65 (0.143) | 2.68 (0.133) | −0.121 (0.603) |
| Peripheral Fatigue | Central Fatigue | |||||
|---|---|---|---|---|---|---|
| Pre-Fatigue | Post-Fatigue | Δ | Pre-Fatigue | Post-Fatigue | Δ | |
| MHSMlow (g2/Hz) | 0.19 (0.01) | 0.18 (0.01) | −0.006 (0.025) | 0.18 (0.01) | 0.17 (0.01) | −0.017 (0.040) |
| MTSMlow (g2/Hz) § | 0.14 (0.02) | 0.14 (0.01) | −0.008 (0.028) | 0.13 (0.01) | 0.13 (0.01) | 0.004 (0.019) |
| THSMlow (g2/Hz) | 1.76 (0.13) | 1.77 (0.14) | 0.018 (0.246) | 1.75 (0.13) | 1.63 (0.14) | −0.115 (0.362) |
| TTSMlow (g2/Hz) § | 4.33 (0.53) | 4.15 (0.41) | −0.166 (0.638) | 4.14 (0.45) | 4.20 (0.37) | 0.896 (0.474) |
| MHSMhigh (g2/Hz) § | 0.01 (0.00) | 0.01 (0.00) | 0.000 (0.003) | 0.01 (0.00) | 0.01 (0.00) | 0.000 (0.003) |
| MTSMhigh (g2/Hz) | 0.06 (0.01) | 0.06 (0.01) | 0.001 (0.013) | 0.06 (0.01) | 0.08 (0.01) †† | 0.017 (0.022) * |
| THSMhigh (g2/Hz) § | 0.44 (0.05) | 0.39 (0.04) | −0.063 (0.104) | 0.40 (0.04) | 0.41 (0.05) | 0.011 (0.192) |
| TTSMhigh (g2/Hz) § | 3.88 (0.48) | 3.80 (0.46) | −0.086 (0.899) | 3.56 (0.36) | 4.37 (0.47) †† | 0.811 (1.267) * |
| ATTlow (dB) § | −49.29 (17.61) | −50.75 (15.31) | −0.04 (6.66) | −54.73 (15.81) | −59.25 (16.12) †,‡‡ | 6.85 (12.37) ** |
| ATThigh (dB) | −116.44 (39.80) | −121.86 (34.80) | 7.58 (19.41) | −128.40 (14.95) | −147.41 (11.98) ††,‡‡ | 25.94 (8.90) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Encarnación-Martínez, A.; García-Gallart, A.; Sanchis-Sanchis, R.; Pérez-Soriano, P. Effects of Central and Peripheral Fatigue on Impact Characteristics during Running. Sensors 2022, 22, 3786. https://0-doi-org.brum.beds.ac.uk/10.3390/s22103786
Encarnación-Martínez A, García-Gallart A, Sanchis-Sanchis R, Pérez-Soriano P. Effects of Central and Peripheral Fatigue on Impact Characteristics during Running. Sensors. 2022; 22(10):3786. https://0-doi-org.brum.beds.ac.uk/10.3390/s22103786
Chicago/Turabian StyleEncarnación-Martínez, Alberto, Antonio García-Gallart, Roberto Sanchis-Sanchis, and Pedro Pérez-Soriano. 2022. "Effects of Central and Peripheral Fatigue on Impact Characteristics during Running" Sensors 22, no. 10: 3786. https://0-doi-org.brum.beds.ac.uk/10.3390/s22103786