
Intraoperative Optical Monitoring of Spinal Cord Hemodynamics Using Multiwavelength Imaging System

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
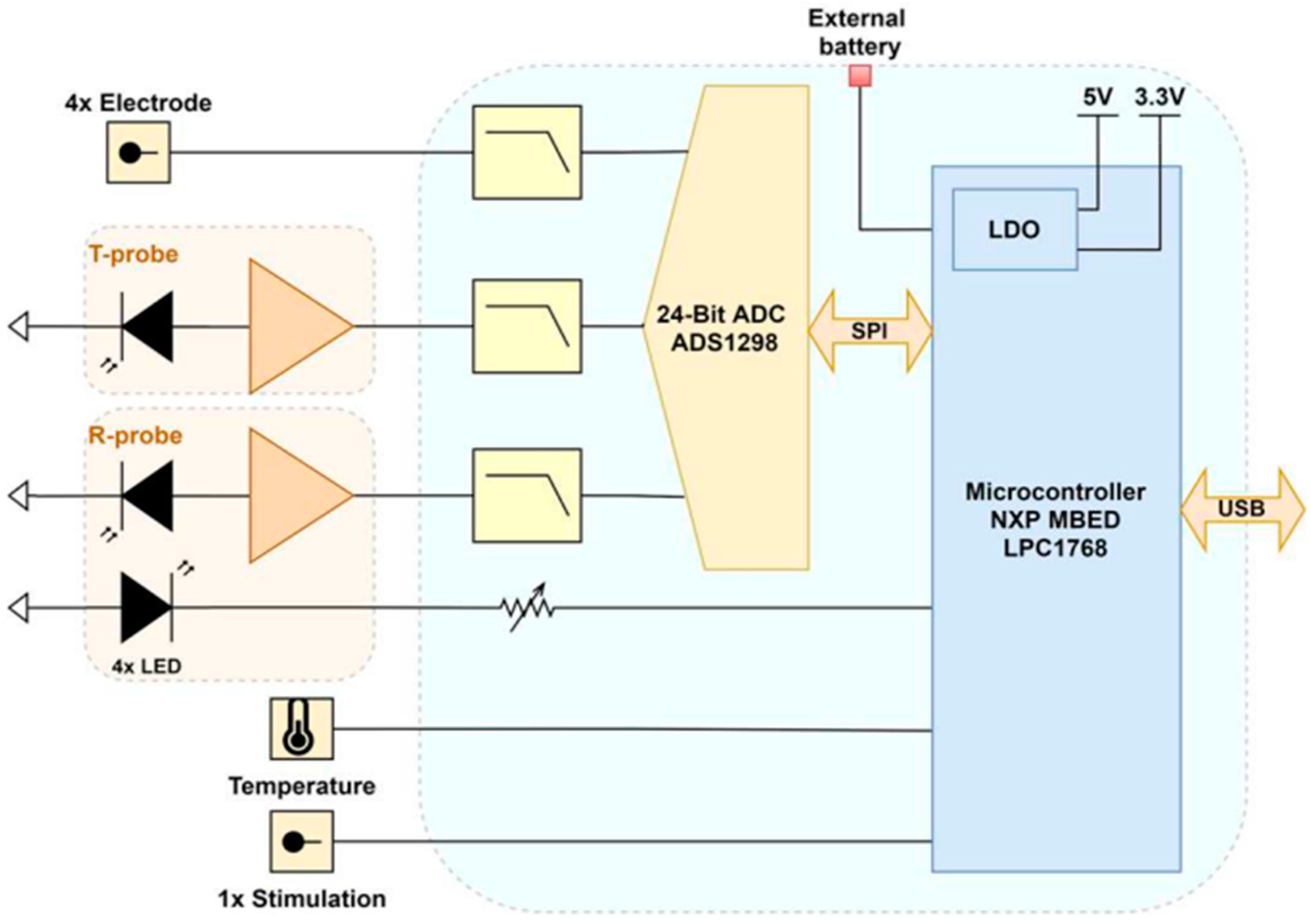
2.1. Acquisition Platform Design Overview
2.1.1. Acquisition Board
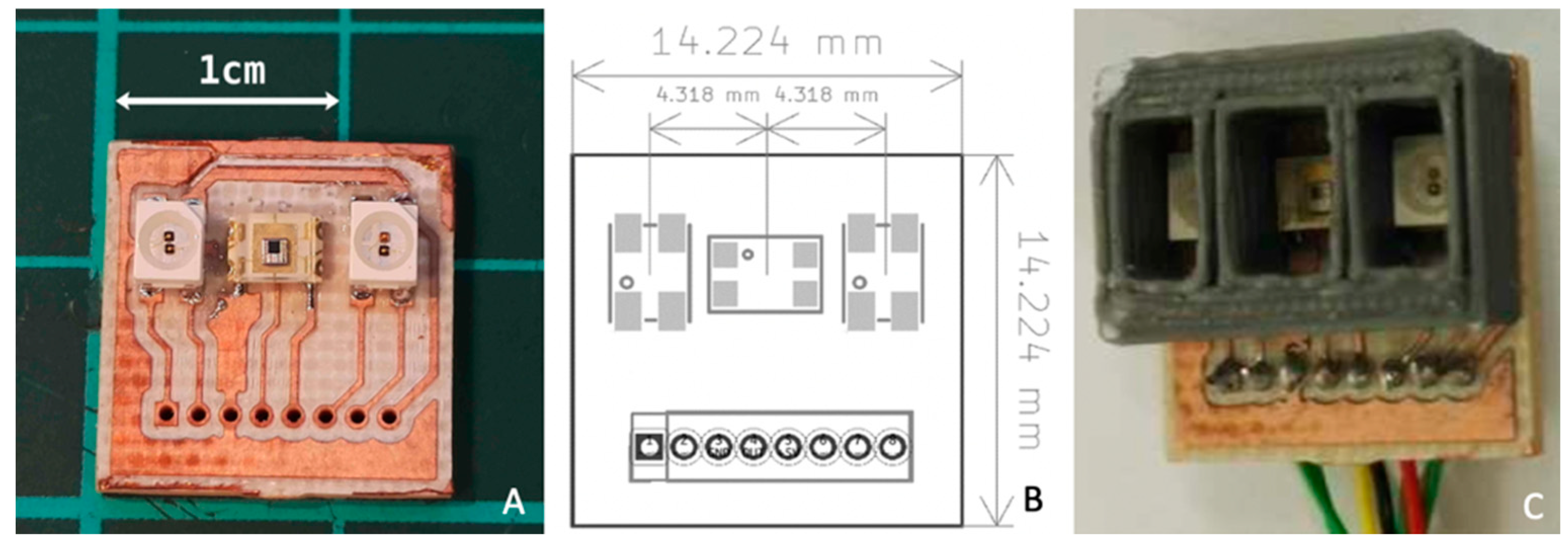
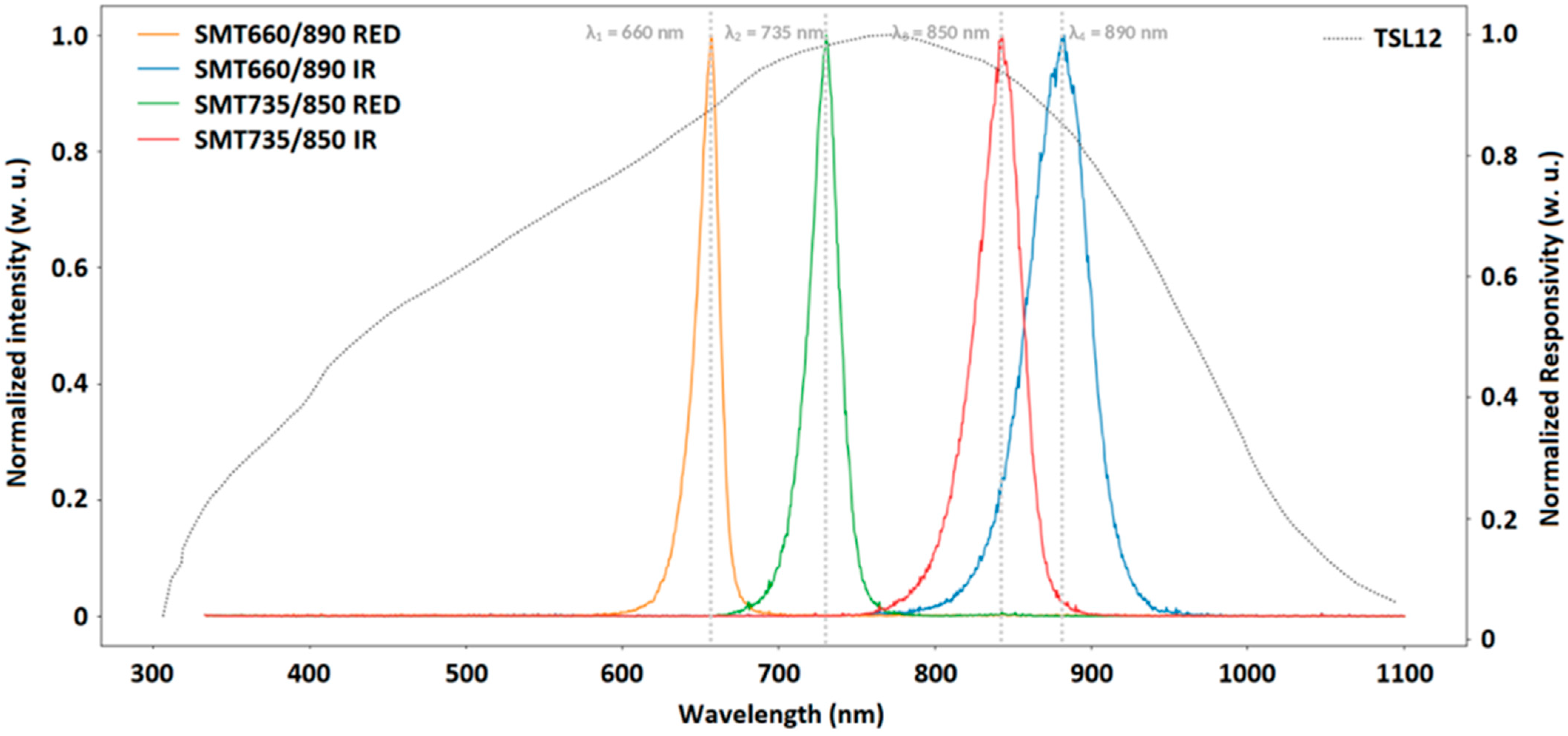
2.1.2. Trans-Reflectance Optodes
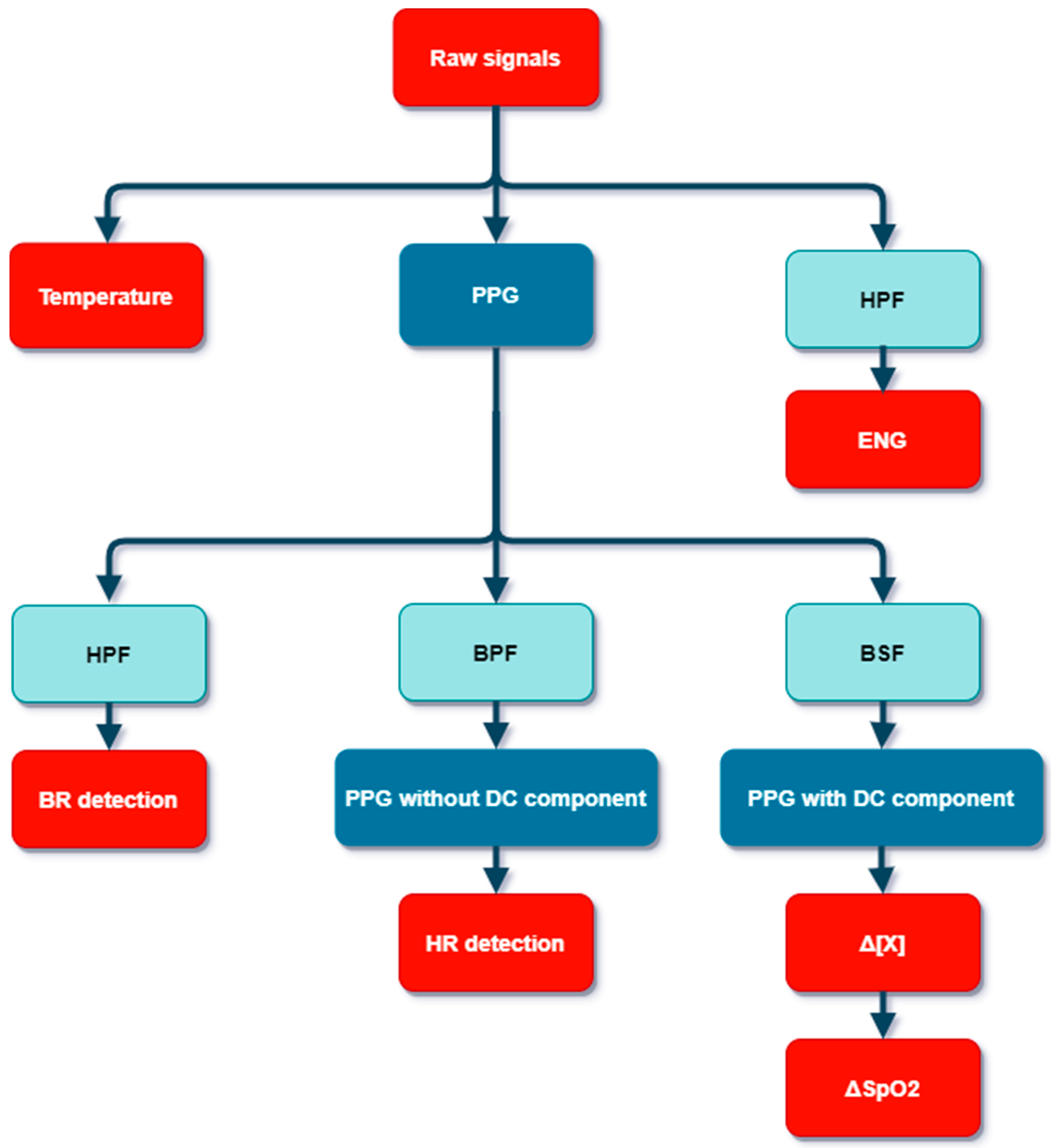
2.1.3. Signal Acquisition and Pre-Processing
2.2. Physiological Estimations Parameters
3. Results
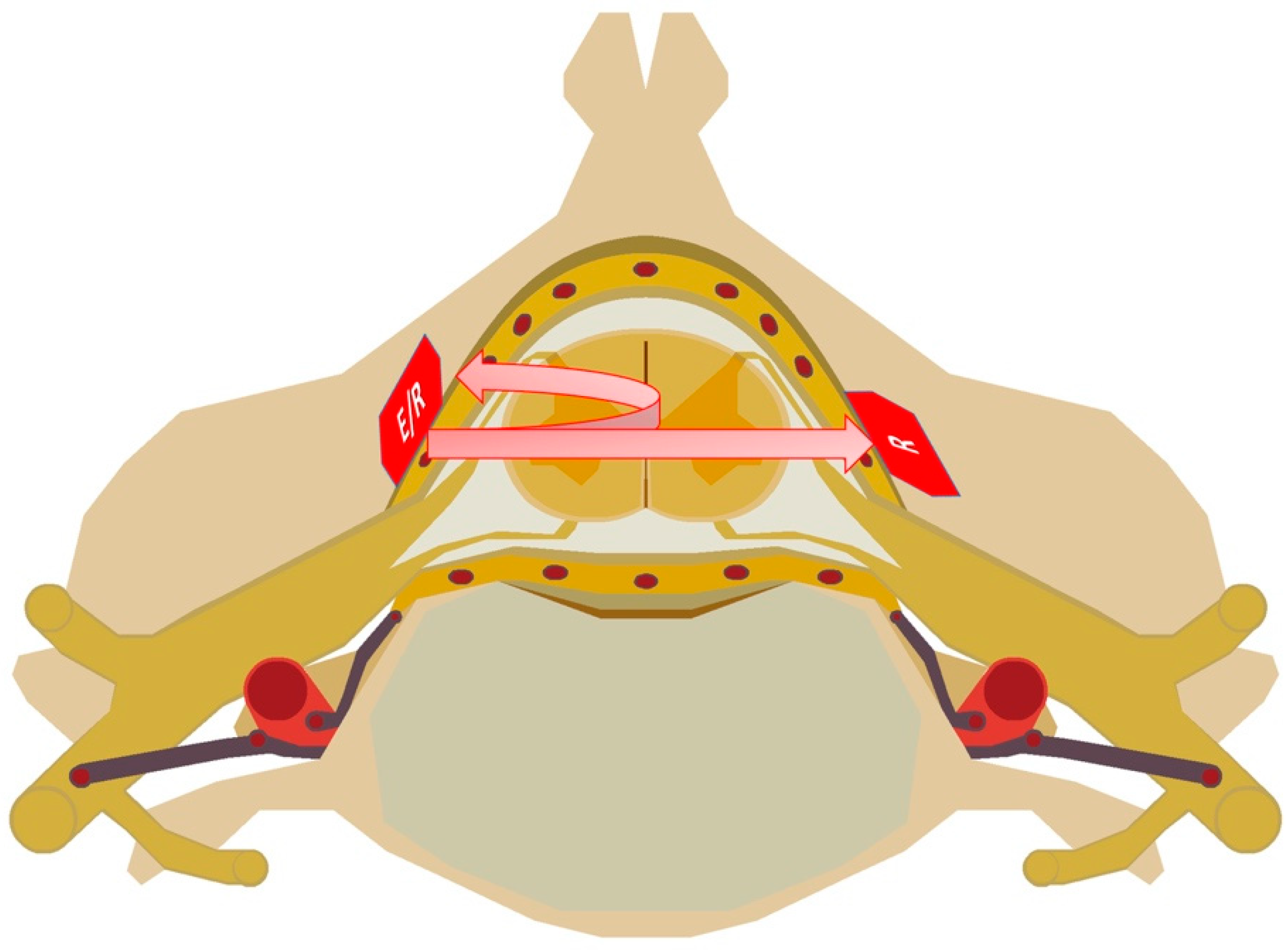
3.1. Pig Experimentation
3.2. Raw Signals
3.3. Reflection Mode Versus Transmission Mode
3.4. Extracted Physiological Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bican, O.; Minagar, A.; Pruitt, A.A. The Spinal Cord: A Review of Functional Neuroanatomy. Neurol. Clin. 2013, 31, 1–18. [Google Scholar] [CrossRef] [PubMed]
- McDonald, J.W.; Sadowsky, C. Spinal-Cord Injury. Lancet 2002, 359, 417–425. [Google Scholar] [CrossRef]
- Coe, J.D.; Arlet, V.; Donaldson, W.; Berven, S.; Hanson, D.S.; Mudiyam, R.; Perra, J.H.; Shaffrey, C.I. Complications in spinal fusion for adolescent idiopathic scoliosis in the new millennium. A report of the Scoliosis Research Society Morbidity and Mortality Committee. Spine 2006, 31, 345–349. [Google Scholar] [CrossRef] [Green Version]
- Diab, M.; Smith, A.R.; Kuklo, T.R.; Spinal Deformity Study Group. Neural Complications in the Surgical Treatment of Adolescent Idiopathic Scoliosis. Spine 2007, 32, 2759–2763. [Google Scholar] [CrossRef]
- Kewin, M.; Rajaram, A.; Milej, D.; Abdalmalak, A.; Morrison, L.; Diop, M.; Lawrence, K. Evaluation of Hyperspectral NIRS for Quantitative Measurements of Tissue Oxygen Saturation by Comparison to Time-Resolved NIRS. Biomed. Opt. Express 2019, 10, 4789–4802. [Google Scholar] [CrossRef]
- Iacobelli, L.; Lucchini, A.; Asnaghi, E.; Nesci, M. Oxygen Saturation Monitoring. Minerva Anestesiol. 2002, 68, 488–491. [Google Scholar] [PubMed]
- Rashnavadi, T.; Macnab, A.; Cheung, A.; Shadgan, A.; Kwon, B.K.; Shadgan, B. Monitoring Spinal Cord Hemodynamics and Tissue Oxygenation: A Review of the Literature with Special Focus on the near-Infrared Spectroscopy Technique. Spinal Cord 2019, 57, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Zhong, W.; Ji, Z.; Sun, C. A Review of Monitoring Methods for Cerebral Blood Oxygen Saturation. Healthcare 2021, 9, 1104. [Google Scholar] [CrossRef]
- Chance, B. Optical Method. Annu. Rev. Biophys. Biophys. Chem. 1991, 20, 1–30. [Google Scholar] [CrossRef]
- Jöbsis, F.F. Noninvasive, Infrared Monitoring of Cerebral and Myocardial Oxygen Sufficiency and Circulatory Parameters. Science 1977, 198, 1264–1267. [Google Scholar] [CrossRef]
- Murkin, J.M.; Arango, M. Near-Infrared Spectroscopy as an Index of Brain and Tissue Oxygenation. Br. J. Anaesth. 2009, 103, i3–i13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boezeman, R.P.E.; Moll, F.L.; Ünlü, Ç.; de Vries, J.-P.P.M. Systematic Review of Clinical Applications of Monitoring Muscle Tissue Oxygenation with Near-Infrared Spectroscopy in Vascular Disease. Microvasc. Res. 2016, 104, 11–22. [Google Scholar] [CrossRef]
- Near Infrared Reflectance Spectroscopy (NIRS): Analysis of Forage Quality; U.S. Department of Agriculture, Agricultural Research Service: Beltsville, MD, USA, 1985.
- Obrig, H. NIRS in Clinical Neurology—A ‘Promising’ Tool? NeuroImage 2014, 85, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Chance, B.; Cooper, C.E.; Delpy, D.T.; Reynolds, E.O.R.; Delpy, D.T.; Cope, M. Quantification in Tissue near–Infrared Spectroscopy. Philos. Trans. R. Soc. London. Ser. B Biol. Sci. 1997, 352, 649–659. [Google Scholar] [CrossRef] [Green Version]
- Tsiakaka, O.; Feruglio, S. Toward the Monitoring of the Spinal Cord: A Feasibility Study. Microelectron. J. 2019, 88, 145–153. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Yan, B.P.-Y.; Dai, W.-X.; Ding, X.-R.; Zhang, Y.-T.; Zhao, N. Multi-Wavelength Photoplethysmography Method for Skin Arterial Pulse Extraction. Biomed. Opt. Express 2016, 7, 4313–4326. [Google Scholar] [CrossRef] [Green Version]
- Wyser, D.; Lambercy, O.; Scholkmann, F.; Wolf, M.; Gassert, R. Wearable and Modular Functional Near-Infrared Spectroscopy Instrument with Multidistance Measurements at Four Wavelengths. Neurophotonics 2017, 4, 041413. [Google Scholar] [CrossRef]
- Tsiakaka, O.; Gosselin, B.; Feruglio, S. Source-Detector Spectral Pairing-Related Inaccuracies in Pulse Oximetry: Evaluation of the Wavelength Shift. Sensors 2020, 20, 3302. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Elgendi, M.; Chen, Z.; Ward, R. An Optimal Filter for Short Photoplethysmogram Signals. Sci. Data 2018, 5, 180076. [Google Scholar] [CrossRef] [PubMed]
- Kolyva, C.; Tachtsidis, I.; Ghosh, A.; Moroz, T.; Cooper, C.E.; Smith, M.; Elwell, C.E. Systematic investigation of changes in oxidized cerebral cytochrome c oxidase concentration during frontal lobe activation in healthy adults. Biomed. Opt. Express 2012, 3, 2550–2566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mousavi, S.S.; Firouzmand, M.; Charmi, M.; Hemmati, M.; Moghadam, M.; Ghorbani, Y. Blood Pressure Estimation from Appropriate and Inappropriate PPG Signals Using A Whole-Based Method. Biomed. Signal Process. Control 2019, 47, 196–206. [Google Scholar] [CrossRef]
- Oshina, I.; Spigulis, J. Beer-Lambert Law for Optical Tissue Diagnostics: Current State of the Art and the Main Limitations. J. Biomed. Opt. 2021, 26, 100901. [Google Scholar] [CrossRef] [PubMed]
- Matcher, S.J.; Elwell, C.E.; Cooper, C.E.; Cope, M.; Delpy, D.T. Performance Comparison of Several Published Tissue Near-Infrared Spectroscopy Algorithms. Anal. Biochem. 1995, 227, 54–68. [Google Scholar] [CrossRef] [PubMed]
- Pavlin, M.; Jarm, T.; Miklavcic, D. Monte-Carlo Simulation of Light Transport for NIRS Measurements in Tumors of Elliptic Geometry. Adv. Exp. Med. Biol. 2003, 530, 41–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scholkmann, F.; Wolf, M. General Equation for the Differential Pathlength Factor of the Frontal Human Head Depending on Wavelength and Age. J. Biomed. Opt. 2013, 18, 105004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toossi, A.; Bergin, B.; Marefatallah, M.; Parhizi, B.; Tyreman, N.; Everaert, D.G.; Rezaei, S.; Seres, P.; Gatenby, J.C.; Perlmutter, S.I.; et al. Comparative Neuroanatomy of the Lumbosacral Spinal Cord of the Rat, Cat, Pig, Monkey, and Human. Sci. Rep. 2021, 11, 1955. [Google Scholar] [CrossRef]
- Strauch, J.T.; Lauten, A.; Zhang, N.; Wahlers, T.; Griepp, R.B. Anatomy of Spinal Cord Blood Supply in the Pig. Ann. Thorac. Surg. 2007, 83, 2130–2134. [Google Scholar] [CrossRef]
- Moerman, A.; Van Herzeele, I.; Vanpeteghem, C.; Vermassen, F.; François, K.; Wouters, P. Near-Infrared Spectroscopy for Monitoring Spinal Cord Ischemia during Hybrid Thoracoabdominal Aortic Aneurysm Repair. J. Endovasc. Ther. 2011, 18, 91–95. [Google Scholar] [CrossRef]
- Badner, N.H.; Nicolaou, G.; Clarke, C.F.M.; Forbes, T.L. Use of Spinal Near-Infrared Spectroscopy for Monitoring Spinal Cord Perfusion During Endovascular Thoracic Aortic Repairs. J. Cardiothorac. Vasc. Anesth. 2011, 25, 316–319. [Google Scholar] [CrossRef]
- Chay, W.; Kirshblum, S. Predicting Outcomes After Spinal Cord Injury. Phys. Med. Rehabil. Clin. N. Am. 2020, 31, 331–343. [Google Scholar] [CrossRef]
- Dolan, E.J.; Transfeldt, E.E.; Tator, C.H.; Simmons, E.H.; Hughes, K.F. The Effect of Spinal Distraction on Regional Spinal Cord Blood Flow in Cats. J. Neurosurg. 1980, 53, 756–764. [Google Scholar] [CrossRef]
- Wu, D.; Zheng, C.; Wu, J.; Xue, J.; Huang, R.; Wu, D.; Song, Y. The Pathologic Mechanisms Underlying Lumbar Distraction Spinal Cord Injury in Rabbits. Spine J. 2017, 17, 1665–1673. [Google Scholar] [CrossRef] [PubMed]
- Seyal, M.; Mull, B. Mechanisms of Signal Change during Intraoperative Somatosensory Evoked Potential Monitoring of the Spinal Cord. J. Clin. Neurophysiol. 2002, 19, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Van Den Hauwe, L.; Sundgren, P.C.; Flanders, A.E. Spinal Trauma and Spinal Cord Injury (SCI). In Diseases of the Brain, Head and Neck, Spine 2020–2023: Diagnostic Imaging; Hodler, J., Kubik-Huch, R.A., von Schulthess, G.K., Eds.; IDKD Springer Series; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Freund, P.; Seif, M.; Weiskopf, N.; Friston, K.; Fehlings, M.G.; Thompson, A.J.; Curt, A. MRI in Traumatic Spinal Cord Injury: From Clinical Assessment to Neuroimaging Biomarkers. Lancet Neurol. 2019, 18, 1123–1135. [Google Scholar] [CrossRef]
- Eli, I.; Lerner, D.P.; Ghogawala, Z. Acute Traumatic Spinal Cord Injury. Neurol Clin. 2021, 39, 471–488. [Google Scholar] [CrossRef] [PubMed]
- Phang, I.; Zoumprouli, A.; Saadoun, S.; Papadopoulos, M.C. Safety Profile and Probe Placement Accuracy of Intraspinal Pressure Monitoring for Traumatic Spinal Cord Injury: Injured Spinal Cord Pressure Evaluation Study. J. Neurosurg. Spine 2016, 25, 398–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Werndle, M.C.; Saadoun, S.; Phang, I.; Czosnyka, M.; Varsos, G.V.; Czosnyka, Z.H.; Smielewski, P.; Jamous, A.; Bell, B.A.; Zoumprouli, A.; et al. Monitoring of Spinal Cord Perfusion Pressure in Acute Spinal Cord Injury: Initial Findings of the Injured Spinal Cord Pressure Evaluation Study. Crit. Care Med. 2014, 42, 646–655. [Google Scholar] [CrossRef]
- Thirumala, P.D.; Huang, J.; Thiagarajan, K.; Cheng, H.; Balzer, J.; Crammond, D.J. Diagnostic Accuracy of Combined Multimodality Somatosensory Evoked Potential and Transcranial Motor Evoked Potential Intraoperative Monitoring in Patients with Idiopathic Scoliosis. Spine 2016, 41, E1177–E1184. [Google Scholar] [CrossRef]
- Thirumala, P.D.; Cheng, H.L.; Loke, Y.K.; Kojo Hamilton, D.; Balzer, J.; Crammond, D.J. Diagnostic Accuracy of Somatosensory Evoked Potential Monitoring during Scoliosis Fusion. J. Clin. Neurosci. 2016, 30, 8–14. [Google Scholar] [CrossRef] [Green Version]
- Zuccaro, M.; Zuccaro, J.; Samdani, A.F.; Pahys, J.M.; Hwang, S.W. Intraoperative Neuromonitoring Alerts in a Pediatric Deformity Center. Neurosurg. Focus 2017, 43, E8. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, D.M.; Auerbach, J.D.; Dormans, J.P.; Flynn, J.; Drummond, D.S.; Bowe, J.A.; Laufer, S.; Shah, S.A.; Bowen, J.R.; Pizzutillo, P.D.; et al. Neurophysiological Detection of Impending Spinal Cord Injury during Scoliosis Surgery. J. Bone Jt. Surg. Am. 2007, 89, 2440–2449. [Google Scholar] [CrossRef]
- Han, S.; Roh, D.; Park, J.; Shin, H. Design of Multi-Wavelength Optical Sensor Module for Depth-Dependent Photoplethysmography. Sensors 2019, 19, 5441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.; Kim, M.; Park, H.-K.; Kim, I.Y. Motion Artifact Reduction in Wearable Photoplethysmography Based on Multi-Channel Sensors with Multiple Wavelengths. Sensors 2020, 20, 1493. [Google Scholar] [CrossRef] [Green Version]
- Alharbi, S.; Hu, S.; Mulvaney, D.; Barrett, L.; Yan, L.; Blanos, P.; Elsahar, Y.; Adema, S. Oxygen Saturation Measurements from Green and Orange Illuminations of Multi-Wavelength Optoelectronic Patch Sensors. Sensors 2018, 19, 118. [Google Scholar] [CrossRef] [Green Version]
- Roldán, M.; Kyriacou, P.A. Near-Infrared Spectroscopy (NIRS) in Traumatic Brain Injury (TBI). Sensors 2021, 21, 1586. [Google Scholar] [CrossRef] [PubMed]
- Cheng, O.S.K.; Prowse, S.; Strong, A.J. Oscillations in the Near-Infrared Signal in Patients with Severe Head Injury. Acta Neurochir. Suppl. 2002, 81, 135–137. [Google Scholar] [CrossRef]
- Tachtsidis, I.; Tisdall, M.M.; Pritchard, C.; Leung, T.S.; Ghosh, A.; Elwell, C.E.; Smith, M. Analysis of the Changes in the Oxidation of Brain Tissue Cytochrome-c-Oxidase in Traumatic Brain Injury Patients during Hypercapnoea: A Broadband NIRS Study. Adv. Exp. Med. Biol. 2011, 701, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, A.; Tachtsidis, I.; Kolyva, C.; Highton, D.; Elwell, C.; Smith, M. Normobaric Hyperoxia Does Not Change Optical Scattering or Pathlength but Does Increase Oxidised Cytochrome C Oxidase Concentration in Patients with Brain Injury. Adv. Exp. Med. Biol. 2013, 765, 67–72. [Google Scholar] [CrossRef] [Green Version]
- Kampfl, A.; Pfausler, B.; Denchev, D.; Jaring, H.P.; Schmutzhard, E. Near Infrared Spectroscopy (NIRS) in Patients with Severe Brain Injury and Elevated Intracranial Pressure. A Pilot Study. Acta Neurochir. Suppl. 1997, 70, 112–114. [Google Scholar] [CrossRef]
- Vilkė, A.; Bilskienė, D.; Šaferis, V.; Gedminas, M.; Bieliauskaitė, D.; Tamašauskas, A.; Macas, A. Predictive Value of Early Near-Infrared Spectroscopy Monitoring of Patients with Traumatic Brain Injury. Medicina 2014, 50, 263–268. [Google Scholar] [CrossRef]
- Kim, M.N.; Edlow, B.L.; Durduran, T.; Frangos, S.; Mesquita, R.C.; Levine, J.M.; Greenberg, J.H.; Yodh, A.G.; Detre, J.A. Continuous Optical Monitoring of Cerebral Hemodynamics during Head-of-Bed Manipulation in Brain-Injured Adults. Neurocrit. Care 2014, 20, 443–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macnab, A.J.; Gagnon, R.E.; Gagnon, F.A. Near Infrared Spectroscopy for Intraoperative Monitoring of the Spinal Cord. Spine 2002, 27, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Kunihara, T.; Shiiya, N.; Matsuzaki, K.; Sata, F.; Matsui, Y. Near-Infrared Spectrophotometry Is Useful to Detect the Beneficial Pharmacological Effects of Alprostadil on Spinal Cord Deoxygenation. Ann. Thorac. Cardiovasc. Surg. 2008, 14, 376–381. [Google Scholar] [PubMed]
- Busch, D.R.; Davis, J.; Kogler, A.; Galler, R.M.; Parthasarathy, A.B.; Yodh, A.G.; Floyd, T.F. Laser Safety in Fiber-Optic Monitoring of Spinal Cord Hemodynamics: A Preclinical Evaluation. J. Biomed. Opt. 2018, 23, 065003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kogler, A.S.; Bilfinger, T.V.; Galler, R.M.; Mesquita, R.C.; Cutrone, M.; Schenkel, S.S.; Yodh, A.G.; Floyd, T.F. Fiber-Optic Monitoring of Spinal Cord Hemodynamics in Experimental Aortic Occlusion. Anesthesiology 2015, 123, 1362–1373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busch, D.R.; Lin, W.; Cai, C.; Cutrone, A.; Tatka, J.; Kovarovic, B.J.; Yodh, A.G.; Floyd, T.F.; Barsi, J. Multi-Site Optical Monitoring of Spinal Cord Ischemia during Spine Distraction. J. Neurotrauma 2020, 37, 2014–2022. [Google Scholar] [CrossRef]
- Shadgan, B.; Manouchehri, N.; So, K.; Shortt, K.; Fong, A.; Streijger, F.; Macnab, A.; Kwon, B.K. Optical Monitoring of Spinal Cord Subcellular Damage after Acute Spinal Cord Injury. In Optical Diagnostics and Sensing XVIII: Toward Point-of-Care Diagnostics; SPIE: Bellingham, WA, USA, 2018; Volume 10501, pp. 107–113. [Google Scholar] [CrossRef]
- Shadgan, B.; Macnab, A.; Fong, A.; Manouchehri, N.; So, K.; Shortt, K.; Streijger, F.; Cripton, P.A.; Sayre, E.C.; Dumont, G.A.; et al. Optical Assessment of Spinal Cord Tissue Oxygenation Using a Miniaturized Near Infrared Spectroscopy Sensor. J. Neurotrauma 2019, 36, 3034–3043. [Google Scholar] [CrossRef]
- Cheung, A.; Tu, L.; Manouchehri, N.; Kim, K.-T.; So, K.; Webster, M.; Fisk, S.; Tigchelaar, S.; Dalkilic, S.S.; Sayre, E.C.; et al. Continuous Optical Monitoring of Spinal Cord Oxygenation and Hemodynamics during the First Seven Days Post-Injury in a Porcine Model of Acute Spinal Cord Injury. J. Neurotrauma 2020, 37, 2292–2301. [Google Scholar] [CrossRef]
- Tsiakaka, O.; Terosiet, M.; Romain, O.; Histace, A.; Benali, H.; Pradat, P.-F.; Vallette, F.; Feher, M.; Feruglio, S. In Vivo NIRS Monitoring in Pig Spinal Cord Tissues. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 4262–4265. [Google Scholar] [CrossRef]
- Shadgan, B.; Kwon, B.K.; Streijger, F.; Manouchehri, N.; So, K.; Shortt, K.; Cripton, P.A.; Macnab, A. Optical Monitoring of Spinal Cord Hemodynamics, a Feasibility Study. In Optical Diagnostics and Sensing XVII: Toward Point-of-Care Diagnostics; SPIE: Bellingham, WA, USA, 2017; Volume 10072, pp. 135–143. [Google Scholar] [CrossRef]
- Berens, R.J.; Stuth, E.A.; Robertson, F.A.; Jaquiss, R.D.; Hoffman, G.M.; Troshynski, T.J.; Staudt, S.R.; Cava, J.R.; Tweddell, J.S.; Bert Litwin, S. Near Infrared Spectroscopy Monitoring during Pediatric Aortic Coarctation Repair. Pediatr. Anesth. 2006, 16, 777–781. [Google Scholar] [CrossRef]
- Etz, C.D.; Von Aspern, K.; Gudehus, S.; Luehr, M.; Girrbach, F.F.; Ender, J.; Borger, M.; Mohr, F.W. Near-Infrared Spectroscopy Monitoring of the Collateral Network Prior to, during, and after Thoracoabdominal Aortic Repair: A Pilot Study. Eur. J. Vasc. Endovasc. Surg. 2013, 46, 651–656. [Google Scholar] [CrossRef] [Green Version]
- Boezeman, R.P.E.; Van Dongen, E.P.; Morshuis, W.J.; Sonker, U.; Boezeman, E.H.J.F.; Waanders, F.G.J.; De Vries, J.-P.P.M. Spinal Near-Infrared Spectroscopy Measurements during and after Thoracoabdominal Aortic Aneurysm Repair: A Pilot Study. Ann. Thorac. Surg. 2015, 99, 1267–1274. [Google Scholar] [CrossRef] [PubMed]
- Griepp, R.B.; Griepp, E.B. Spinal Cord Perfusion and Protection During Descending Thoracic and Thoracoabdominal Aortic Surgery: The Collateral Network Concept. Ann. Thorac. Surg. 2007, 83, S865–S869. [Google Scholar] [CrossRef] [PubMed]
- Amiri, A.R.; Lee, C.H.; Leung, T.S.; Hetreed, M.; Craggs, M.D.; Casey, A.T.H. Intraoperative Assessment of Human Spinal Cord Perfusion Using near Infrared Spectroscopy with Indocyanine Green Tracer Technique. Spine J. 2013, 13, 1818–1825. [Google Scholar] [CrossRef] [PubMed]
- Sevick-Muraca, E.M.; Houston, J.P.; Gurfinkel, M. Fluorescence-Enhanced, near Infrared Diagnostic Imaging with Contrast Agents. Curr. Opin. Chem. Biol. 2002, 6, 642–650. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Wavelength | ||||
|---|---|---|---|---|
| λ1: 735 nm | 464.5 | 1295.6 | 168.8 | 1800.5 |
| λ2: 850 nm | 1159.3 | 785.9 | 530.9 | 2289.9 |
| λ3: 660 nm | 334.5 | 3439.9 | 609.4 | 4399.8 |
| λ4: 890 nm | 1313.4 | 866.8 | 890.9 | 1958.9 |
| Wavelength | Reflection | Transmission |
|---|---|---|
| λ1: 735 nm | 6.21 | 3.49 |
| λ2: 850 nm | 6.08 | 3.41 |
| λ3: 660 nm | 5.00 | 2.80 |
| λ4: 890 nm | 3.56 | 2.00 |
| Wavelength | Bravais–Pearson Coefficient (w. u.) | Angle (°) |
|---|---|---|
| λ1: 735 nm | −0.75 | 4.1 |
| λ2: 850 nm | −0.83 | 3.4 |
| λ3: 660 nm | −0.84 | 7.9 |
| λ4: 890 nm | −0.84 | 4.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mainard, N.; Tsiakaka, O.; Li, S.; Denoulet, J.; Messaoudene, K.; Vialle, R.; Feruglio, S. Intraoperative Optical Monitoring of Spinal Cord Hemodynamics Using Multiwavelength Imaging System. Sensors 2022, 22, 3840. https://0-doi-org.brum.beds.ac.uk/10.3390/s22103840
Mainard N, Tsiakaka O, Li S, Denoulet J, Messaoudene K, Vialle R, Feruglio S. Intraoperative Optical Monitoring of Spinal Cord Hemodynamics Using Multiwavelength Imaging System. Sensors. 2022; 22(10):3840. https://0-doi-org.brum.beds.ac.uk/10.3390/s22103840
Chicago/Turabian StyleMainard, Nicolas, Olivier Tsiakaka, Songlin Li, Julien Denoulet, Karim Messaoudene, Raphael Vialle, and Sylvain Feruglio. 2022. "Intraoperative Optical Monitoring of Spinal Cord Hemodynamics Using Multiwavelength Imaging System" Sensors 22, no. 10: 3840. https://0-doi-org.brum.beds.ac.uk/10.3390/s22103840