
A Deep Learning Approach for Gait Event Detection from a Single Shank-Worn IMU: Validation in Healthy and Neurological Cohorts


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Data Pre-Processing
2.2.1. Marker Data
2.2.2. IMU Data
2.3. Model
2.3.1. Model Architecture
2.3.2. Hyperparameter Optimization
2.4. Analysis
2.4.1. Overall Detection Performance
2.4.2. Time Agreement
2.4.3. Stride-Specific Gait Parameters
3. Results
3.1. Overall Detection Performance
3.2. Time Agreement
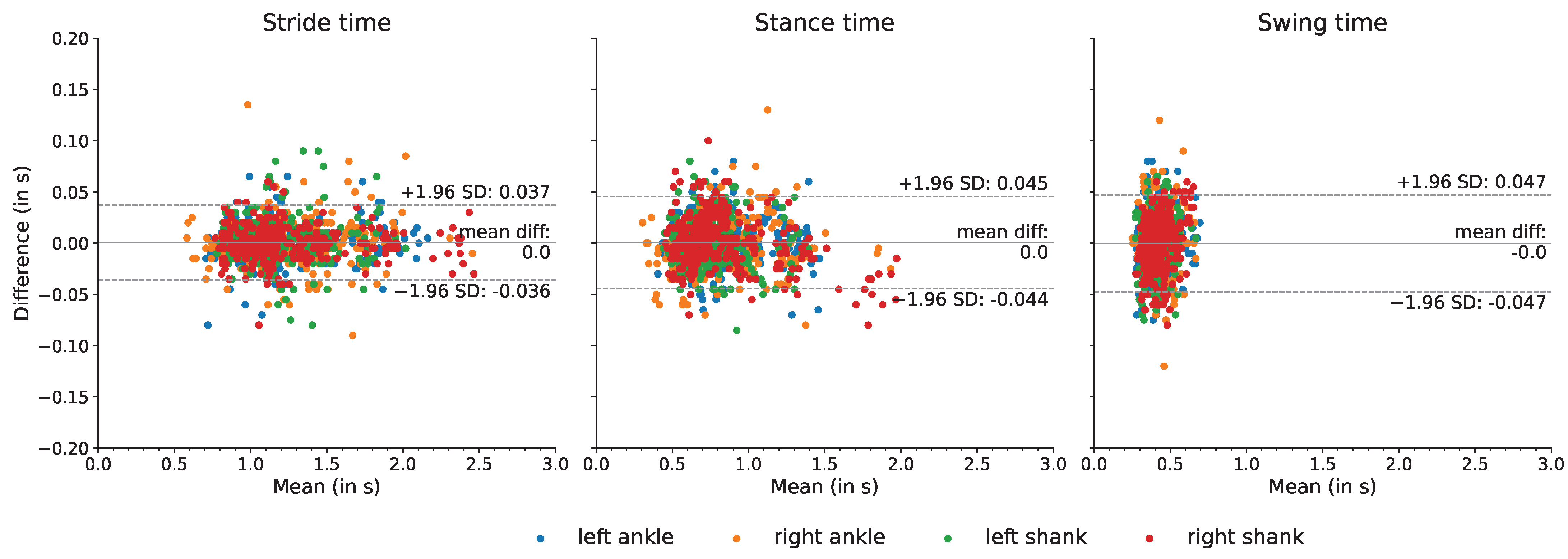
3.3. Stride-Specific Gait Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| cLBP | chronic low back pain |
| CNN | convolutional neural network |
| IMU | inertial measurement unit |
| MS | multiple sclerosis |
| No. | number |
| OA | older adults |
| PD | Parkinson’s disease |
| TCN | temporal convolutional network |
| YA | younger adults |
References
- Snijders, A.H.; van de Warrenburg, B.P.; Giladi, N.; Bloem, B.R. Neurological gait disorders in elderly people: Clinical approach and classification. Lancet Neurol. 2007, 6, 63–74. [Google Scholar] [CrossRef]
- Hodgins, D. The importance of measuring human gait. Med. Device Technol. 2008, 19, 44–47. [Google Scholar]
- Del Din, S.; Elshehabi, M.; Galna, B.; Hobert, M.A.; Warmerdam, E.; Suenkel, U.; Brockmann, K.; Metzger, F.; Hansen, C.; Berg, D.; et al. Gait analysis with wearables predicts conversion to Parkinson disease. Ann. Neurol. 2019, 86, 357–367. [Google Scholar] [CrossRef] [PubMed]
- König, A.; Klaming, L.; Pijl, M.; Demeurraux, A.; Davis, R.; Robert, P. Objective measurement of gait parameters in healthy and cognitively impaired elderly using the dual-task paradigm. Aging Clin. Exp. Res. 2017, 29, 1181–1189. [Google Scholar] [CrossRef]
- Bertoli, M.; Cereatti, A.; Trojaniello, D.; Avanzino, L.; Pelosin, E.; Del Din, S.; Rochester, L.; Ginis, P.; Bekkers, E.M.J.; Mirelman, A.; et al. Estimation of spatio-temporal parameters of gait from magneto-inertial measurement units: Multicenter validation among Parkinson, mildly cognitively impaired and healthy older adults. Biomed. Eng. Online 2018, 17, 58. [Google Scholar] [CrossRef] [Green Version]
- von Schroeder, H.P.; Coutts, R.D.; Lyden, P.D.; Billings, E., Jr.; Nickel, V.L. Gait parameters following stroke: A practical assessment. J. Rehabil. Res. Dev. 1995, 32, 25–31. [Google Scholar]
- Mohan, D.M.; Khandoker, A.H.; Wasti, S.A.; Ismail Ibrahim Ismail Alali, S.; Jelinek, H.F.; Khalaf, K. Assessment methods of post-stroke gait: A scoping review of technology-driven approaches to gait characterization and analysis. Front. Neurol. 2021, 12, 650024. [Google Scholar] [CrossRef]
- Griškevičius, J.; Apanskienė, V.; Žižienė, J.; Daunoravičienė, K.; Ovčinikova, A.; Kizlaitienė, R.; Sereikė, I.; Kaubrys, G.; Pauk, J.; Idźkowski, A. Estimation of temporal gait parameters of multiple sclerosis patients in clinical setting using inertial sensors. In Proceedings of the 11th International Conference BIOMDLORE 2016, Druskininkai, Lithuania, 20–22 October 2016; pp. 80–82. [Google Scholar]
- Flachenecker, F.; Gaßner, H.; Hannik, J.; Lee, D.H.; Flachenecker, P.; Winkler, J.; Eskofier, B.; Linker, R.A.; Klucken, J. Objective sensor-based gait measures reflect motor impairment in multiple sclerosis patients: Reliability and clinical validation of a wearable sensor device. Mult. Scler. Relat. Dis. 2019, 39, 101903. [Google Scholar] [CrossRef]
- Hannink, J.; Kautz, T.; Pasluosta, C.F.; Gaßmann, K.-G.; Klucken, J.; Eskofier, B.M. Sensor-Based Gait Parameter Extraction with Deep Convolutional Neural Networks. IEEE J. Biomed. Health 2017, 21, 85–93. [Google Scholar] [CrossRef] [Green Version]
- Perry, J.; Burnfield, J.M. Gait Analysis: Normal and Pathological Gait, 2nd ed.; SLACK Inc.: Thorofare, NJ, USA, 2010. [Google Scholar]
- Richards, J.; Levine, D.; Whittle, M. Whittle’s Gait Analysis, 5th ed.; Churchill Livingstone: London, UK, 2012. [Google Scholar]
- Rueterbories, J.; Spaich, E.G.; Larsen, B.; Andersen, O.K. Methods for gait event detection and analysis in ambulatory systems. Med. Eng. Phys. 2010, 32, 545–552. [Google Scholar] [CrossRef]
- Bruening, D.A.; Ridge, S.T. Automated event detection algorithms in pathological gait. Gait Posture 2014, 39, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Chiari, L.; Della Croce, U.; Leardini, A.; Cappozzo, A. Human movement analysis using stereophotogrammetry: Part 2: Instrumental errors. Gait Posture 2005, 21, 197–211. [Google Scholar] [CrossRef] [PubMed]
- Topley, M.; Richards, J.G. A comparison of currently available optoelectronic motion capture systems. J. Biomech. 2020, 106, 109820. [Google Scholar] [CrossRef] [PubMed]
- Iosa, M.; Picerno, P.; Paolucci, S.; Morone, G. Wearable inertial sensors for human movement analysis. Expert Rev. Med. Devices 2016, 13, 641–659. [Google Scholar] [CrossRef] [PubMed]
- Jarchi, D.; Pope, J.; Lee, T.K.M.; Tamjidi, L.; Mirzaei, A.; Sanei, S. A Review on Accelerometry-Based Gait Analysis and Emerging Clinical Applications. IEEE Rev. Biomed. Eng. 2018, 11, 177–194. [Google Scholar] [CrossRef]
- Hillel, I.; Gazit, E.; Nieuwboer, A.; Avanzino, L.; Rochester, L.; Cereatti, A.; Della Croce, U.; Rikkert, M.O.; Bloem, B.R.; Pelosin, E.; et al. Is every-day walking in older adults more analogous to dual-task walking or to usual walking? Elucidating the gaps between gait performance in the lab and during 24/7 monitoring. Eur. Rev. Aging Phys. A 2019, 16, 6. [Google Scholar]
- Warmerdam, E.; Hausdorff, J.M.; Atrsaei, A.; Zhou, Y.; Mirelman, A.; Aminian, K.; Espay, A.J.; Hansen, C.; Evers, L.J.W.; Keller, A.; et al. Long-term unsupervised mobility assessment in movement disorders. Lancet Neurol. 2020, 19, 462–470. [Google Scholar] [CrossRef]
- Atrsaei, A.; Corrá, M.F.; Dadashi, F.; Vila-Chã, N.; Maia, L.; Mariani, B.; Maetzler, W.; Aminian, K. Gait speed in clinical and daily living assessments in Parkinson’s disease patients: Performance versus capacity. Npj Parkinson’s Dis. 2021, 7, 24. [Google Scholar] [CrossRef]
- Del Din, S.; Godfrey, A.; Mazzà, C.; Lord, S.; Rochester, L. Free-living monitoring of Parkinson’s disease: Lessons from the field. Mov. Disord. 2016, 31, 1293–1313. [Google Scholar] [CrossRef]
- Shah, V.V.; McNames, J.; Mancini, M.; Carlson-Kuhta, P.; Nutt, J.G.; El-Gohary, M.; Lapidus, J.A.; Horak, F.B.; Curtze, C. Digital Biomarkers of Mobility in Parkinson’s Disease During Daily Living. J. Park. Dis. 2020, 10, 1099–1111. [Google Scholar] [CrossRef]
- Fasano, A.; Mancini, M. Wearable-based mobility monitoring: The long road ahead. Lancet Neurol. 2020, 19, 378–379. [Google Scholar] [CrossRef]
- Corrá, M.F.; Atrsaei, A.; Sardoreira, A.; Hansen, C.; Aminian, K.; Correia, M.; Vila-Chã, N.; Maetzler, W.; Maia, L. Comparison of Laboratory and Daily-Life Gait Speed Assessment during ON and OFF States in Parkinson’s Disease. Sensors 2021, 21, 3974. [Google Scholar] [CrossRef] [PubMed]
- Ben Mansour, K.; Rezzoug, N.; Gorce, P. Analysis of several methods and inertial sensors locations to assess gait parameters in able-bodied subjects. Gait Posture 2015, 42, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Storm, F.A.; Buckley, C.J.; Mazzà, C. Gait event detection in laboratory and real life settings: Accuracy of ankle and waist sensor based methods. Gait Posture 2016, 50, 42–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panebianco, G.P.; Bisi, M.C.; Stagni, R.; Fantozzi, S. Analysis of the performance of 17 algorithms from a systematic review: Influence of sensor position, analysed variable and computational approach in gait timing estimation from IMU measurements. Gait Posture 2018, 66, 76–82. [Google Scholar] [CrossRef]
- Niswander, W.; Kontson, K. Evaluating the Impact of IMU Sensor Location and Walking Task on Accuracy of Gait Event Detection Algorithms. Sensors 2021, 21, 3989. [Google Scholar] [CrossRef]
- Salarian, A.; Russmann, H.; Vingerhoets, F.J.; Dehollain, C.; Blanc, Y.; Burkhard, P.R.; Aminian, K. Gait assessment in Parkinson’s disease: Toward an ambulatory system for long-term monitoring. IEEE Trans. Biomed. Eng. 2004, 51, 1434–1443. [Google Scholar] [CrossRef]
- Catalfamo, P.; Ghoussayni, S.; Ewins, D. Gait Event Detection on Level Ground and Incline Walking Using a Rate Gyroscope. Sensors 2010, 10, 5683–5702. [Google Scholar] [CrossRef] [Green Version]
- Sabatini, A.; Martelloni, C.; Scapellato, S.; Cavallo, F. Assessment of Walking Features from Foot Inertial Sensing. IEEE Trans. Biomed. Eng. 2005, 52, 486–494. [Google Scholar] [CrossRef] [Green Version]
- Maqbool, H.F.; Husman, M.A.B.; Awad, M.; Abouhossein, A.; Mehryar, P.; Iqbal, N.; Dehghani-Sanij, A.A. Real-time gait event detection for lower limb amputees using a single wearable sensor. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; IEEE: Piscataway, NJ, USA, 2016. [Google Scholar]
- Romijnders, R.; Warmerdam, E.; Hansen, C.; Welzel, J.; Schmidt, G.; Maetzler, W. Validation of IMU-based gait event detection during curved walking and turning in older adults and Parkinson’s Disease patients. J. Neuroeng. Rehabil. 2021, 18, 28. [Google Scholar] [CrossRef]
- Jasiewicz, J.M.; Allum, J.H.; Middleton, J.W.; Barriskill, A.; Condie, P.; Purcell, B.; Li, R.C.T. Gait event detection using linear accelerometers or angular velocity transducers in able-bodied and spinal-cord injured individuals. Gait Posture 2006, 24, 502–509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trojaniello, D.; Cereatti, A.; Pelosin, E.; Avanzino, L.; Mirelman, A.; Hausdorff, J.M.; Della Croce, U. Estimation of step-by-step spatio-temporal parameters of normal and impaired gait using shank-mounted magneto-inertial sensors: Application to elderly, hemiparetic, parkinsonian and choreic gait. J. Neuroeng. Rehabil. 2014, 11, 152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferraris, F.; Grimaldi, U.; Parvis, M. Procedure for effortless in-field calibration of three-axis rate gyros and accelerometers. Sens. Mater. 1995, 7, 311–330. [Google Scholar]
- Greene, B.R.; McGrath, D.; O’Neill, R.; O’Donovan, K.J.; Burns, A.; Caulfield, B. An adaptive gyroscope-based algorithm for temporal gait analysis. Med. Biol. Eng. Comput. 2010, 48, 1251–1260. [Google Scholar] [CrossRef] [PubMed]
- Leineweber, M.J.; Gomez Orozco, M.D.; Andrysek, J. Evaluating the feasibility of two post-hoc correction techniques for mitigating posture-induced measurement errors associated with wearable motion capture. Med. Eng. Phys. 2019, 71, 38–44. [Google Scholar] [CrossRef]
- Pacher, L.; Chatellier, C.; Vauzelle, R.; Fradet, L. Sensor-to-Segment Calibration Methodologies for Lower-Body Kinematic Analysis with Inertial Sensors: A Systematic Review. Sensors 2020, 20, 3322. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Ter Haar Romeny, B.M. A Deeper Understanding of Deep Learning. In Artificial Intelligence in Medical Imaging: Opportunities, Applications and Risks; Ranschaert, E.R., Morozov, S., Algra, P.R., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 25–38. [Google Scholar]
- Iqbal, M.S.; Ahmad, I.; Bin, L.; Khan, S.; Rodrigues, J.J.P.C. Deep learning recognition of diseased and normal cell representation. Trans. Emerg. Tel. Tech. 2021, 32, e4017. [Google Scholar] [CrossRef]
- Eskofier, B.M.; Lee, S.I.; Daneault, J.-F.; Golabchi, F.N.; Ferreira-Carvalho, G.; Vergara-Diaz, G.; Sapienza, S.; Costante, G.; Klucken, J.; Kautz, T.; et al. Recent machine learning advancements in sensor-based mobility analysis: Deep learning for Parkinson’s disease assessment. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 655–658. [Google Scholar]
- Stober, S.; Sternin, A.; Owen, A.M.; Grahn, J.A. Deep Feature Learning for EEG Recordings. arXiv 2016, arXiv:1511.04306. [Google Scholar]
- Yao, Y.; Plested, J.; Gedeon, T. Deep Feature Learning and Visualization for EEG Recording Using Autoencoders. In Neural Information Processing; Springer International Publishing: Cham, Switzerland, 2018; pp. 554–566. [Google Scholar]
- Horst, F.; Lapuschkin, S.; Samek, W.; Müller, K.-R.; Schöllhorn, W.I. Explaining the unique nature of individual gait patterns with deep learning. Sci. Rep. 2019, 9, 2391. [Google Scholar] [CrossRef] [Green Version]
- Camps, J.; Samà, A.; Martín, M.; Rodríguez-Martín, D.; Pérez-López, C.; Moreno Arostegui, J.M.; Cabestany, J.; Català, A.; Alcaine, S.; Mestre, B.; et al. Deep learning for freezing of gait detection in Parkinson’s disease patients in their homes using a waist-worn inertial measurement unit. Knowl.-Based Syst. 2018, 139, 119–131. [Google Scholar] [CrossRef]
- Sharifi Renani, M.; Myers, C.A.; Zandie, R.; Mahoor, M.H.; Davidson, B.S.; Clary, C.W. Deep Learning in Gait Parameter Prediction for OA and TKA Patients Wearing IMU. Sensors 2020, 20, 5553. [Google Scholar] [CrossRef] [PubMed]
- Kidziński, Ł.; Delp, S.; Schwartz, M. Automatic real-time gait event detection in children using deep neural networks. PLoS ONE 2019, 14, e0211466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lempereur, M.; Rousseau, F.; Rémy-Néris, O.; Pons, C.; Houx, L.; Quellec, G.; Brochard, S. A new deep learning-based method for the detection of gait events in children with gait disorders: Proof-of-concept and concurrent validity. J. Biomech. 2020, 98, 109490. [Google Scholar] [CrossRef] [PubMed]
- Filtjens, B.; Nieuwboer, A.; D’cruz, N.; Spildooren, J.; Slaets, P.; Vanrumste, B. A data-driven approach for detecting gait events during turning in people with Parkinson’s disease and freezing of gait. Gait Posture 2020, 80, 130–136. [Google Scholar] [CrossRef]
- Gadaleta, M.; Cisotto, G.; Rossi, M.; Ur Rehman, R.Z.; Rochester, L.; Del Din, S. Deep Learning Techniques for Improving Digital Gait Segmentation. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; IEEE: Piscataway, NJ, USA, 2019. [Google Scholar]
- Warmerdam, E.; Romijnders, R.; Geritz, J.; Elshehabi, M.; Maetzler, C.; Otto, J.C.; Reimer, M.; Stuerner, K.; Baron, R.; Paschen, S.; et al. Proposed Mobility Assessments with Simultaneous Full-Body Inertial Measurement Units and Optical Motion Capture in Healthy Adults and Neurological Patients for Future Validation Studies: Study Protocol. Sensors 2021, 21, 5833. [Google Scholar] [CrossRef]
- Gibb, W.R.; Lees, A.J. The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 1988, 51, 745–752. [Google Scholar] [CrossRef] [Green Version]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Federolf, P.A. A Novel Approach to Solve the “Missing Marker Problem” in Marker-Based Motion Analysis That Exploits the Segment Coordination Patterns in Multi-Limb Motion Data. PLoS ONE 2013, 8, e78689. [Google Scholar] [CrossRef] [Green Version]
- Gløersen, Ø.; Federolf, P. Predicting Missing Marker Trajectories in Human Motion Data Using Marker Intercorrelations. PLoS ONE 2016, 11, e0152616. [Google Scholar]
- Rácz, K.; Rita, M.K. Marker displacement data filtering in gait analysis: A technical note. Biomed. Signal Proces. 2021, 70, 102974. [Google Scholar] [CrossRef]
- Kormylo, J.; Jain, V. Two-pass recursive digital filter with zero phase shift. IEEE Trans. Acoust. Speech 1974, 22, 384–387. [Google Scholar] [CrossRef]
- Pijnappels, M.; Bobbert, M.F.; Van Dieën, J.H. Changes in walking pattern caused by the possibility of a tripping reaction. Gait Posture 2001, 14, 11–18. [Google Scholar] [CrossRef]
- O’Connor, C.M.; Thorpe, S.K.; O’Malley, M.J.; Vaughan, C.L. Automatic detection of gait events using kinematic data. Gait Posture 2007, 25, 469–474. [Google Scholar] [CrossRef]
- Carcreff, L.; Gerber, C.; Paraschiv-Ionescu, A.; De Coulon, G.; Newman, C.; Armand, S.; Aminian, K. What is the best configuration of wearable sensors to measure spatiotemporal gait parameters in children with cerebral palsy? Sensors 2018, 18, 394. [Google Scholar] [CrossRef] [Green Version]
- Rémy, P. Temporal Convolutional Networks for Keras. GitHub Repos. 2020. Available online: https://github.com/philipperemy/keras-tcn (accessed on 17 March 2022).
- Bai, S.; Kolter, J.Z.; Koltun, V. An Empirical Evaluation of Generic Convolutional and Recurrent Networks for Sequence Modeling. arXiv 2018, arXiv:1803.01271. [Google Scholar]
- Yu, F.; Koltun, V. Multi-Scale Context Aggregation by Dilated Convolutions. In Proceedings of the 4th International Conference on Learning Representations (ICLR), San Juan, Puerto Rico, 2–4 May 2016. Conference Track Proceedings. [Google Scholar]
- Ioffe, S.; Szegedy, C. Batch Normalization: Accelerating Deep Network Training by Reducing Internal Covariate Shift. arXiv 2015, arXiv:1502.03167. [Google Scholar]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A simple way to prevent neural networks from overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar]
- van Rossum, G.; Drake, F.L. Python 3 Reference Manual; CreateSpace: Scotts Valley, CA, USA, 2009. [Google Scholar]
- Keras. 2015. Available online: https://keras.io (accessed on 16 December 2021).
- Lea, C.; Flynn, M.D.; Vidal, R.; Reiter, A.; Hager, G.D. Temporal convolutional networks for action segmentation and detection. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 22–25 July 2017; pp. 156–165. [Google Scholar]
- van den Oord, A.; Dieleman, S.; Zen, H.; Simonyan, K.; Vinyals, O.; Graves, A.; Kalchbrenner, N.; Senior, A.W.; Kavukcuoglu, K. WaveNet: A generative model for raw audio. arXiv 2016, arXiv:1609.03499. [Google Scholar]
- Kingma, D.P.; Ba, J. Adam: A Method for Stochastic Optimization. arXiv 2014, arXiv:1412.6980v9. [Google Scholar]
- Schmidt, R.M.; Schneider, F.; Henning, P. Descending through a crowded valley-benchmarking deep learning optimizers. In Proceedings of the 38th International Conference on Machine Learning (ICML), Online. 18–24 July 2021; pp. 9367–9376. [Google Scholar]
- KerasTuner. GitHub Repos. 2019. Available online: https://github.com/keras-team/keras-tuner (accessed on 19 March 2022).
- Bergstra, J.; Bengio, Y. Random Search for Hyper-Parameter Optimization. J. Mach. Learn. Res. 2012, 13, 281–305. [Google Scholar]
- Diez, D.; Çetinkaya-Rundel, M.; Barr, C.D. OpenIntro Statistics, 4th ed.; 2019; Available online: https://www.openintro.org/book/os/ (accessed on 1 April 2022).
- Ji, N.; Zhou, H.; Guo, K.; Samuel, O.W.; Huang, Z.; Xu, L.; Li, G. Appropriate Mother Wavelets for Continuous Gait Event Detection Based on Time-Frequency Analysis for Hemiplegic and Healthy Individuals. Sensors 2019, 19, 3462. [Google Scholar] [CrossRef] [Green Version]
- Aminian, K.; Najafi, B.; Büla, C.; Leyvraz, P.-F.; Robert, P. Spatio-temporal parameters of gait measured by an ambulatory system using miniature gyroscopes. J. Biomech. 2002, 35, 689–699. [Google Scholar] [CrossRef]
- van Uem, J.M.; Maier, K.S.; Hucker, S.; Scheck, O.; Hobert, M.A.; Santos, A.T.; Fagerbakke, Ø.; Larsen, F.; Ferreira, J.J.; Maetzler, W. Twelve-week sensor assessment in Parkinson’s disease: Impact on quality of life. Mov. Disord. 2016, 31, 1337–1338. [Google Scholar] [CrossRef]
- Fisher, J.M.; Hammerla, N.Y.; Rochester, L.; Andras, P.; Walker, R.W. Body-Worn Sensors in Parkinson’s Disease: Evaluating Their Acceptability to Patients. Telemed. E-Health 2016, 22, 63–69. [Google Scholar] [CrossRef] [Green Version]
- Adams, J.L.; Dinesh, K.; Xiong, M.; Tarolli, C.G.; Sharma, S.; Sheth, N.; Aranyosi, A.J.; Zhu, W.; Goldenthal, S.; Biglan, K.M.; et al. Multiple Wearable Sensors in Parkinson and Huntington Disease Individuals: A Pilot Study in Clinic and at Home. Digit. Biomark. 2017, 1, 52–63. [Google Scholar] [CrossRef] [Green Version]
- Godkin, F.E.; Turner, E.; Demnati, Y.; Vert, A.; Roberts, A.; Swartz, R.H.; McLaughlin, P.M.; Weber, K.S.; Thai, V.; Beyer, K.B.; et al. Feasibility of a continuous, multi-sensor remote health monitoring approach in persons living with neurodegenerative disease. J. Neurol. 2022, 269, 2673–2686. [Google Scholar] [CrossRef]
- Espay, A.J.; Hausdorff, J.M.; Sánchez-Ferro, Á.; Klucken, J.; Merola, A.; Bonato, P.; Paul, S.S.; Horak, F.B.; Vizcarra, J.A.; Mestre, T.A.; et al. A roadmap for implementation of patient-centered digital outcome measures in Parkinson’s disease obtained using mobile health technologies. Mov. Disord. 2019, 34, 657–663. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Gender | Number of Participants | Age years | Height cm | Weight kg |
|---|---|---|---|---|---|
| YA | F | 21 | 27 (7) | 173 (5) | 67 (9) |
| M | 21 | 29 (9) | 185 (8) | 80 (12) | |
| OA | F | 12 | 70 (6) | 167 (6) | 72 (17) |
| M | 10 | 73 (6) | 180 (6) | 83 (12) | |
| PD | F | 12 | 67 (6) | 168 (7) | 70 (15) |
| M | 19 | 61 (11) | 178 (7) | 86 (14) | |
| MS | F | 12 | 37 (10) | 174 (9) | 75 (9) |
| M | 9 | 42 (16) | 189 (9) | 96 (32) | |
| stroke | F | 4 | 66 (11) | 160 (7) | 65 (13) |
| M | 17 | 67 (18) | 178 (7) | 84 (15) | |
| cLBP | F | 3 | 64 (12) | 166 (6) | 65 (6) |
| M | 6 | 66 (17) | 177 (8) | 86 (14) | |
| other | F | 3 | 60 (16) | 166 (4) | 79 (19) |
| M | 8 | 68 (19) | 182 (7) | 85 (14) |
| Dataset | No. of Participants | No. of Trials | No. of Instances |
|---|---|---|---|
| Train | 61 | 749 | 3366 |
| Validation | 48 | 564 | 2570 |
| Test | 48 | 620 | 620 |
| Description | Possible Values |
|---|---|
| Number of filters | 8, 16, 32, 64, 128 |
| Kernel size | 3, 5, 7 |
| Dilations | [1, 2], [1, 2, 4], [1, 2, 4, 8] |
| Layer # | Layer Type | Hyperparameters | Output Shape |
|---|---|---|---|
| 0 | inputs | batch size × 400 × 6 | |
| 1a | conv | no. of filters: 16 | batch size × 400 × 16 |
| kernel size: 5 | |||
| stride: 1 | |||
| padding: same | |||
| dilation: 1 | |||
| 1b | conv | no. of filters: 16 | batch size × 400 × 16 |
| kernel size: 1 | |||
| stride: 1 | |||
| padding: same | |||
| dilation: 1 | |||
| 2 | conv | no. of filters: 16 | batch size × 400 × 16 |
| kernel size: 5 | |||
| stride: 1 | |||
| padding: same | |||
| dilation: 1 | |||
| 3 | conv | no. of filters: 16 | batch size × 400 × 16 |
| kernel size: 5 | |||
| stride: 1 | |||
| padding: same | |||
| dilation: 2 | |||
| 4 | conv | no. of filters: 16 | batch size × 400 × 16 |
| kernel size: 5 | |||
| stride: 1 | |||
| padding: same | |||
| dilation: 2 | |||
| 5 | conv | no. of filters: 16 | batch size × 400 × 16 |
| kernel size: 5 | |||
| stride: 1 | |||
| padding: same | |||
| dilation: 4 | |||
| 6 | conv | no. of filters: 16 | batch size × 400 × 16 |
| kernel size: 5 | |||
| stride: 1 | |||
| padding: same | |||
| dilation: 4 | |||
| 7a | dense | no. of units: 1 | batch size × 400 × 1 |
| 7b | dense | no. of units: 1 | batch size × 400 × 1 |
| Initial Contacts | Final Contacts | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tracked Point | TP | FN | FP | Recall | Precision | F1 | TP | FN | FP | Recall | Precision | F1 |
| Left ankle | 624 | 19 | 5 | 97% | 99% | 98% | 606 | 32 | 10 | 95% | 98% | 97% |
| Right ankle | 599 | 42 | 8 | 93% | 99% | 96% | 614 | 17 | 12 | 97% | 98% | 98% |
| Left shank | 605 | 38 | 15 | 94% | 98% | 96% | 585 | 53 | 18 | 92% | 97% | 94% |
| Right shank | 603 | 36 | 15 | 94% | 98% | 96% | 595 | 30 | 9 | 95% | 99% | 97% |
| Initial Contacts | Final Contacts | |||
|---|---|---|---|---|
| Tracked Point |
Median s |
IQR s |
Median s |
IQR s |
| Left ankle | 0.000 | 0.020 | 0.000 | 0.010 |
| Right ankle | 0.000 | 0.020 | −0.005 | 0.015 |
| Left shank | −0.005 | 0.020 | −0.005 | 0.020 |
| Right shank | −0.003 | 0.020 | −0.005 | 0.020 |
| Tracked Point | Parameters | Mean Difference s | Limits of Agreement (s, s) |
|---|---|---|---|
| Left ankle | stride time | 0.001 | (−0.035, 0.036) |
| stance time | 0.002 | (−0.039, 0.042) | |
| swing time | −0.001 | (−0.045, 0.043) | |
| Right ankle | stride time | 0.000 | (−0.039, 0.040) |
| stance time | −0.002 | (−0.048, 0.044) | |
| swing time | 0.003 | (−0.046, 0.051) | |
| Left shank | stride time | 0.001 | (−0.039, 0.041) |
| stance time | 0.002 | (−0.043, 0.046) | |
| swing time | −0.001 | (−0.049, 0.047) | |
| Right shank | stride time | −0.000 | (−0.031, 0.031) |
| stance time | 0.002 | (−0.046, 0.049) | |
| swing time | −0.002 | (−0.049, 0.046) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romijnders, R.; Warmerdam, E.; Hansen, C.; Schmidt, G.; Maetzler, W. A Deep Learning Approach for Gait Event Detection from a Single Shank-Worn IMU: Validation in Healthy and Neurological Cohorts. Sensors 2022, 22, 3859. https://0-doi-org.brum.beds.ac.uk/10.3390/s22103859
Romijnders R, Warmerdam E, Hansen C, Schmidt G, Maetzler W. A Deep Learning Approach for Gait Event Detection from a Single Shank-Worn IMU: Validation in Healthy and Neurological Cohorts. Sensors. 2022; 22(10):3859. https://0-doi-org.brum.beds.ac.uk/10.3390/s22103859
Chicago/Turabian StyleRomijnders, Robbin, Elke Warmerdam, Clint Hansen, Gerhard Schmidt, and Walter Maetzler. 2022. "A Deep Learning Approach for Gait Event Detection from a Single Shank-Worn IMU: Validation in Healthy and Neurological Cohorts" Sensors 22, no. 10: 3859. https://0-doi-org.brum.beds.ac.uk/10.3390/s22103859