
Feasibility of Overground Gait Training Using a Joint-Torque-Assisting Wearable Exoskeletal Robot in Children with Static Brain Injury

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
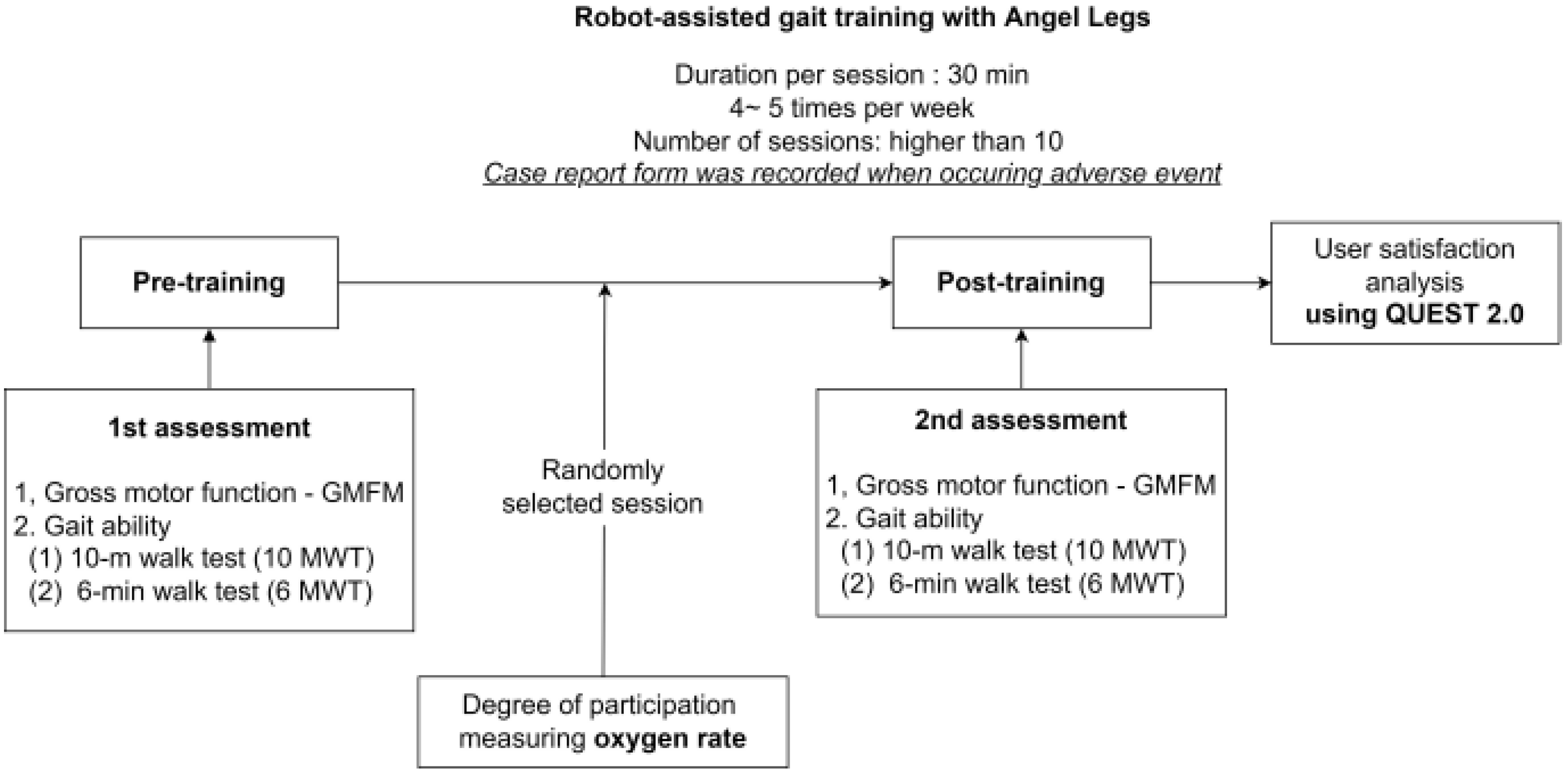
2.1. Design
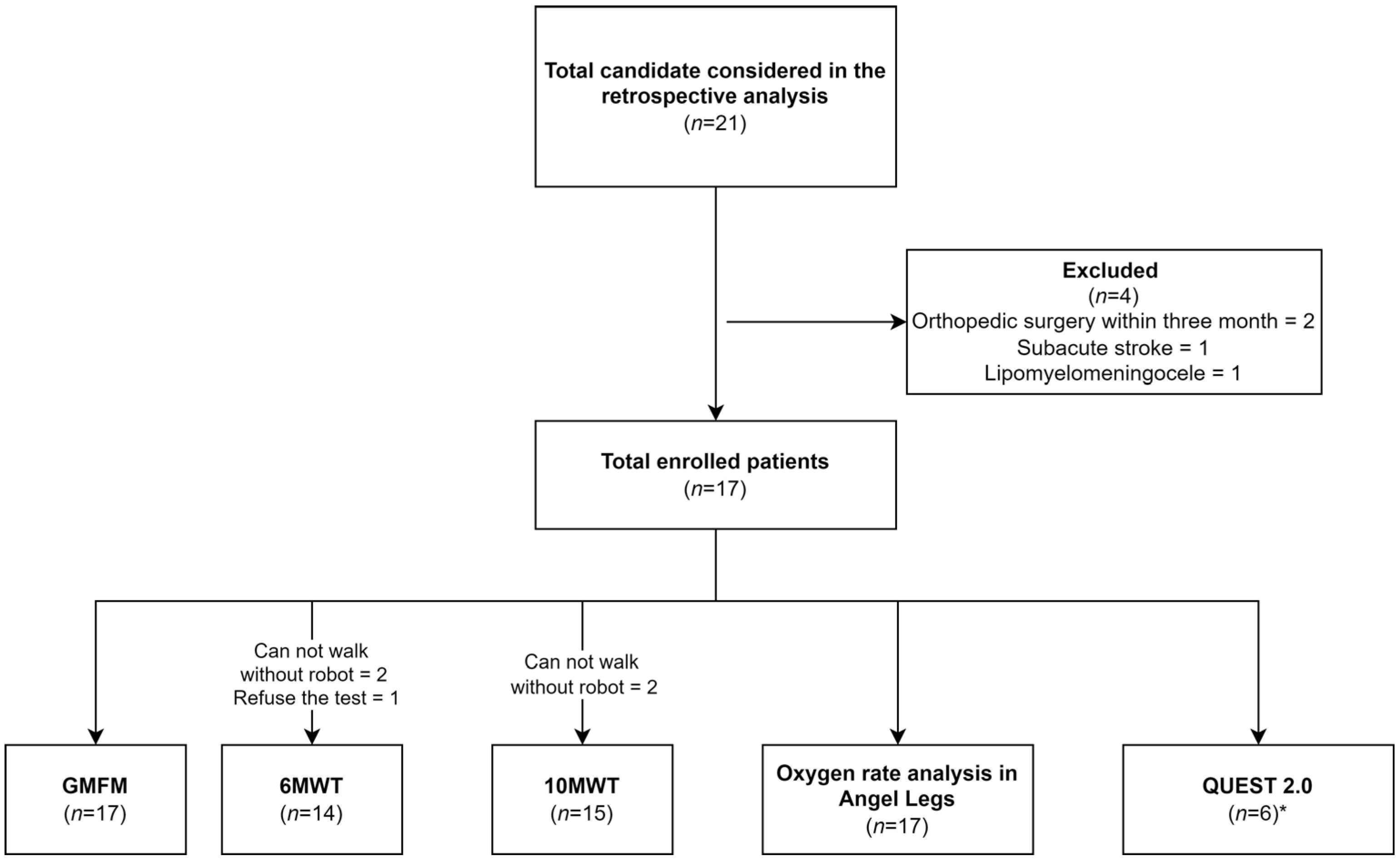
2.2. Participants
2.3. Wearable Joint-Torque-Assisting Exoskeletal Robot
2.4. Robot-Assisted Gait Training Protocol for Pediatric Patients
2.5. Clinical Evaluation
2.6. Gross Motor Function Measure
2.7. Six-Minute Walk Test
2.8. Ten-Meter Walk Test
2.9. Oxygen Consumption
2.10. QUEST 2.0-Korean Version
2.11. Statistics
3. Results
3.1. Patient Characteristics
3.2. Changes between Pre- and Post-Training
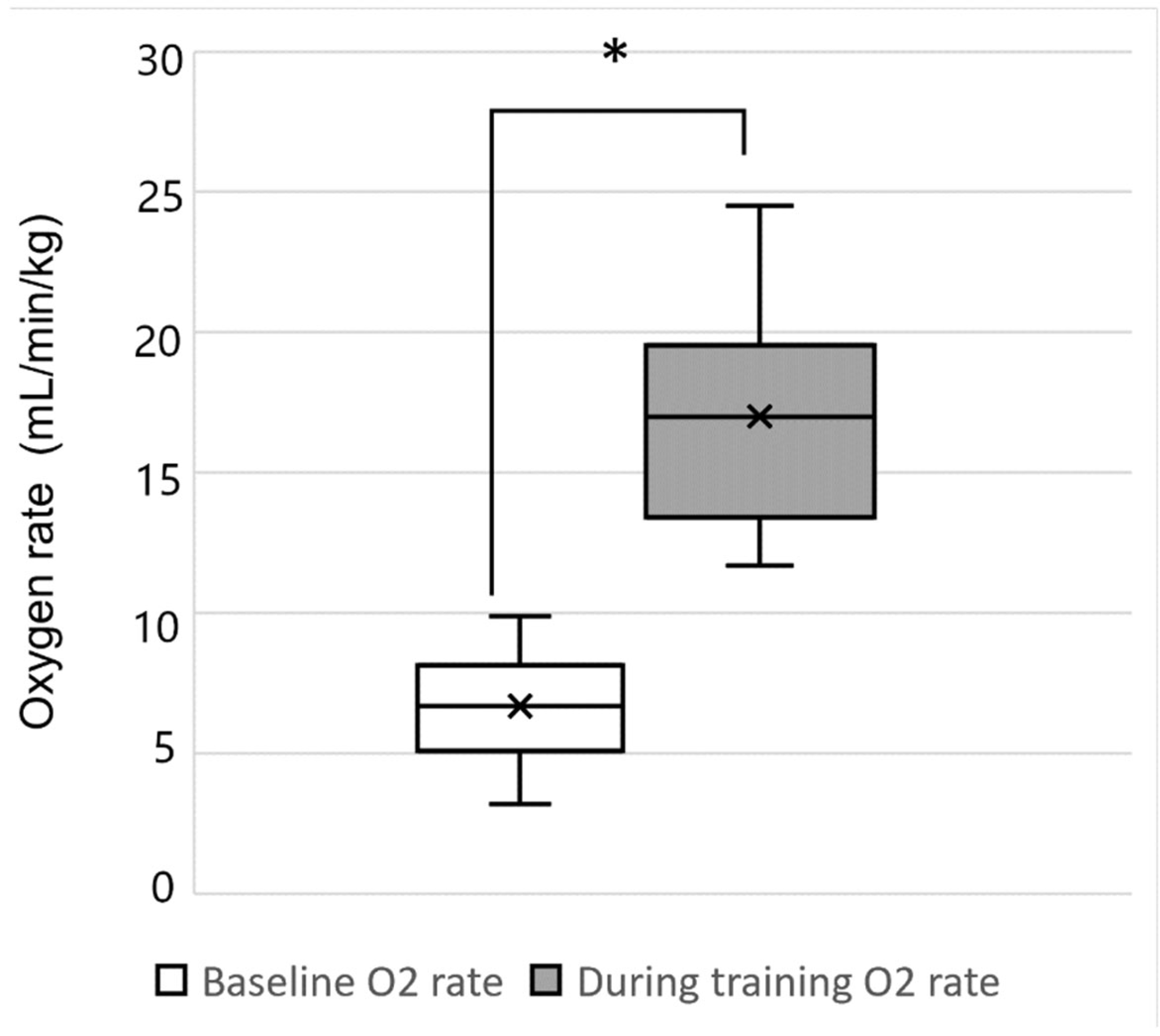
3.3. Changes in Physiologic Burden between Resting and Training States
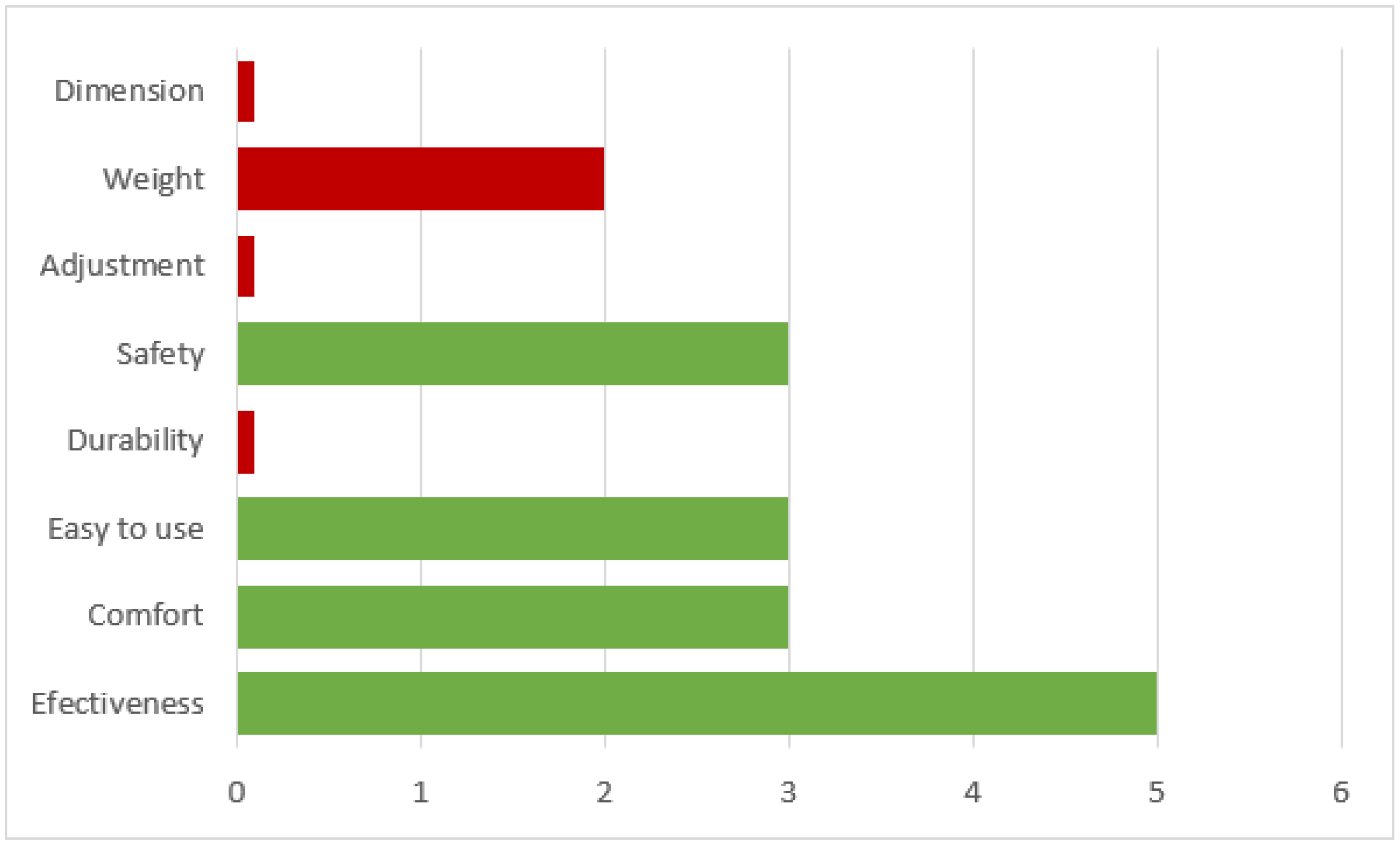
3.4. Satisfaction Questionnaire
3.5. Adverse Events
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stolze, H.; Klebe, S.; Baecker, C.; Zechlin, C.; Friege, L.; Pohle, S.; Deuschl, G. Prevalence of gait disorders in hospitalized neurological patients. Mov. Disord. 2005, 20, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Giladi, N.; Horak, F.B.; Hausdorff, J.M. Classification of gait disturbances: Distinguishing between continuous and episodic changes. Mov. Disord. 2013, 28, 1469–1473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baronchelli, F.; Zucchella, C.; Serrao, M.; Intiso, D.; Bartolo, M. The Effect of Robotic Assisted Gait Training with Lokomat® on Balance Control After Stroke: Systematic Review and Meta-Analysis. Front. Neurol. 2021, 12, 1073. [Google Scholar] [CrossRef] [PubMed]
- Tedla, J.S.; Dixit, S.; Gular, K.; Abohashrh, M. Robotic-Assisted Gait Training Effect on Function and Gait Speed in Subacute and Chronic Stroke Population: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Eur. Neurol. 2019, 81, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Beretta, E.; Storm, F.A.; Strazzer, S.; Frascarelli, F.; Petrarca, M.; Colazza, A.; Cordone, G.; Biffi, E.; Morganti, R.; Maghini, C.; et al. Effect of Robot-Assisted Gait Training in a Large Population of Children with Motor Impairment Due to Cerebral Palsy or Acquired Brain Injury. Arch. Phys. Med. Rehabil. 2020, 101, 106–112. [Google Scholar] [CrossRef] [Green Version]
- Morone, G.; Paolucci, S.; Cherubini, A.; De Angelis, D.; Venturiero, V.; Coiro, P.; Iosa, M. Robot-assisted gait training for stroke patients: Current state of the art and perspectives of robotics. Neuropsychiatr. Dis. Treat. 2017, 13, 1303–1311. [Google Scholar] [CrossRef] [Green Version]
- Mehrholz, J.; Thomas, S.; Werner, C.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2017, 5, Cd006185. [Google Scholar] [CrossRef]
- Ammann-Reiffer, C.; Bastiaenen, C.H.G.; Meyer-Heim, A.D.; van Hedel, H.J.A. Effectiveness of robot-assisted gait training in children with cerebral palsy: A bicenter, pragmatic, randomized, cross-over trial (PeLoGAIT). BMC Pediatr. 2017, 17, 64. [Google Scholar] [CrossRef] [Green Version]
- Aurich-Schuler, T.; Grob, F.; van Hedel, H.J.A.; Labruyère, R. Can Lokomat therapy with children and adolescents be improved? An adaptive clinical pilot trial comparing Guidance force, Path control, and FreeD. J. NeuroEng. Rehabil. 2017, 14, 76. [Google Scholar] [CrossRef] [Green Version]
- Emara, H.A.; El-Gohary, T.M.; Al-Johany, A.A. Effect of body-weight suspension training versus treadmill training on gross motor abilities of children with spastic diplegic cerebral palsy. Eur. J. Phys. Rehabil. Med. 2016, 52, 356–363. [Google Scholar]
- Willoughby, K.L.; Dodd, K.J.; Shields, N.; Foley, S. Efficacy of partial body weight-supported treadmill training compared with overground walking practice for children with cerebral palsy: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2010, 91, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Mataki, Y.; Mutsuzaki, H.; Kamada, H.; Takeuchi, R.; Nakagawa, S.; Yoshikawa, K.; Takahashi, K.; Kuroda, M.; Iwasaki, N.; Yamazaki, M. Effect of the Hybrid Assistive Limb on the Gait Pattern for Cerebral Palsy. Medicina 2020, 56, 673. [Google Scholar] [CrossRef] [PubMed]
- Manikowska, F.; Brazevic, S.; Krzyżańska, A.; Jóźwiak, M. Effects of Robot-Assisted Therapy on Gait Parameters in Pediatric Patients with Spastic Cerebral Palsy. Front. Neurol. 2021, 12, 724009. [Google Scholar] [CrossRef] [PubMed]
- Choi, H. Assistance of a Person with Muscular Weakness Using a Joint-Torque-Assisting Exoskeletal Robot. Appl. Sci. 2021, 11, 3114. [Google Scholar] [CrossRef]
- Lee, S.H.; Junh, B.K.; Park, S.Y. Korean Translation and Psychometric Properties of Quebec User Evaluation of Satisfaction Assistive Technology 2.0. J. Korea Acad. Ind. Coop. Soc. 2013, 14, 3284–3292. [Google Scholar]
- Adair, B.; Said, C.M.; Rodda, J.; Morris, M.E. Psychometric properties of functional mobility tools in hereditary spastic paraplegia and other childhood neurological conditions. Dev. Med. Child Neurol. 2012, 54, 596–605. [Google Scholar] [CrossRef]
- Russell, D.J.; Rosenbaum, P.L.; Cadman, D.T.; Gowland, C.; Hardy, S.; Jarvis, S. The gross motor function measure: A means to evaluate the effects of physical therapy. Dev. Med. Child Neurol. 1989, 31, 341–352. [Google Scholar] [CrossRef]
- Geiger, R.; Strasak, A.; Treml, B.; Gasser, K.; Kleinsasser, A.; Fischer, V.; Geiger, H.; Loeckinger, A.; Stein, J.I. Six-minute walk test in children and adolescents. J. Pediatr. 2007, 150, 395–399. [Google Scholar] [CrossRef]
- Thompson, P.; Beath, T.; Bell, J.; Jacobson, G.; Phair, T.; Salbach, N.M.; Wright, F.V. Test-retest reliability of the 10-metre fast walk test and 6-minute walk test in ambulatory school-aged children with cerebral palsy. Dev. Med. Child Neurol. 2008, 50, 370–376. [Google Scholar] [CrossRef]
- Demers, L.; Monette, M.; Lapierre, Y.; Arnold, D.L.; Wolfson, C. Reliability, validity, and applicability of the Quebec User Evaluation of Satisfaction with assistive Technology (QUEST 2.0) for adults with multiple sclerosis. Disabil. Rehabil. 2002, 24, 21–30. [Google Scholar] [CrossRef]
- Chisholm, A.E.; Alamro, R.A.; Williams, A.M.M.; Lam, T. Overground vs. treadmill-based robotic gait training to improve seated balance in people with motor-complete spinal cord injury: A case report. J. NeuroEng. Rehabil. 2017, 14, 27. [Google Scholar] [CrossRef] [PubMed]
- Thompson, L.A.; Badache, M.; Brusamolin, J.A.R.; Savadkoohi, M.; Guise, J.; Paiva, G.V.d.; Suh, P.; Sanchez Guerrero, P.; Shetty, D. Multidirectional Overground Robotic Training Leads to Improvements in Balance in Older Adults. Robotics 2021, 10, 101. [Google Scholar] [CrossRef]
- Lee, K.B.; Lim, S.H.; Kim, Y.D.; Yang, B.I.; Kim, K.H.; Lee, K.S.; Kim, E.J.; Hwang, B.Y. The contributions of balance to gait capacity and motor function in chronic stroke. J. Phys. Ther. Sci. 2016, 28, 1686–1690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, S.; Kim, H.-R.; Han, Z.-A.; Lee, B.-S.; Kim, S.; Shin, H.; Moon, J.-G.; Yang, S.-P.; Lim, M.-H.; Cho, D.-Y.; et al. Improved Gait Speed after Robot-Assisted Gait Training in Patients with Motor Incomplete Spinal Cord Injury: A Preliminary Study. Ann. Rehabil. Med. 2017, 41, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Ko, M.-S.; Chung, J.-H.; Jeon, H.-S. Correlation between Pediatric Balance Scale (PBS) and Gross Motor Function Measurement (GMFM) Scores in Children with Cerebral Palsy. J. Korean Soc. Phys. Med. 2010, 5, 281–288. [Google Scholar]
- Britto, H.; Mendes, L.; Moreno, C.; Silva, E.; Lindquist, A. Correlation between balance, speed, and walking ability in individuals with chronic hemiparesis. Fisioter. Mov. 2016, 29, 87–94. [Google Scholar] [CrossRef] [Green Version]
- Tang, L.; Liu, G.; Yang, M.; Li, F.; Ye, F.; Li, C. Joint design and torque feedback experiment of rehabilitation robot. Adv. Mech. Eng. 2014, 12, 1687814020924498. [Google Scholar] [CrossRef]
- Zhang, L.; Guo, S.; Sun, Q. Development and Assist-As-Needed Control of an End-Effector Upper Limb Rehabilitation Robot. Appl. Sci. 2020, 10, 6684. [Google Scholar] [CrossRef]
- Holt, R.L.; Mikati, M.A. Care for child development: Basic science rationale and effects of interventions. Pediatr. Neurol. 2011, 44, 239–253. [Google Scholar] [CrossRef]
- Marsh, A.P.; Katula, J.A.; Pacchia, C.F.; Johnson, L.C.; Koury, K.L.; Rejeski, W.J. Effect of treadmill and overground walking on function and attitudes in older adults. Med. Sci. Sports Exerc. 2006, 38, 1157–1164. [Google Scholar] [CrossRef]
- Moore, J.L.; Bø, E.; Erichsen, A.; Rosseland, I.; Halvorsen, J.; Bratlie, H.; Hornby, T.G.; Nordvik, J.E. Development and Results of an Implementation Plan for High-Intensity Gait Training. J. Neurol. Phys. Ther. 2021, 45, 282. [Google Scholar] [CrossRef] [PubMed]
- Duschau-Wicke, A.; Caprez, A.; Riener, R. Patient-cooperative control increases active participation of individuals with SCI during robot-aided gait training. J. NeuroEng. Rehabil. 2010, 7, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waters, R.L.; Lunsford, B.R.; Perry, J.; Byrd, R. Energy-speed relationship of walking: Standard tables. J. Orthop. Res. 1988, 6, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Asselin, P.; Knezevic, S.; Kornfeld, S.; Cirnigliaro, C.; Agranova-Breyter, I.; Bauman, W.A.; Spungen, A.M. Heart rate and oxygen demand of powered exoskeleton-assisted walking in persons with paraplegia. J. Rehabil. Res. Dev. 2015, 52, 147–158. [Google Scholar] [CrossRef]
- Reinkensmeyer, D.J.; Akoner, O.M.; Ferris, D.P.; Gordon, K.E. Slacking by the human motor system: Computational models and implications for robotic orthoses. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 2129–2132. [Google Scholar]
- Babič, J.; Laffranchi, M.; Tessari, F.; Verstraten, T.; Novak, D.; Šarabon, N.; Ugurlu, B.; Peternel, L.; Torricelli, D.; Veneman, J.F. Challenges and solutions for application and wider adoption of wearable robots. Wearable Technol. 2021, 2, e14. [Google Scholar] [CrossRef]
- Shingarey, D.; Kaul, L.; Asfour, T. Torque-Based Velocity Control for Safe Human-Humanoid Interaction. In Advances in Service and Industrial Robotics; Springer: Cham, Switzerland, 2020; pp. 61–68. [Google Scholar]
- Murchland, S.; Kernot, J.; Parkyn, H. Children’s Satisfaction with Assistive Technology Solutions for Schoolwork Using the QUEST 2.1: Children’s Version. Assist. Technol. 2011, 23, 162–176. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Value | |
|---|---|
| Total patients | 17 |
| Age, years | 9.40 (8, 17) |
| Sex, M:F | 9:8 |
| Height, cm | 136.00 (116.6, 172.0) |
| Weight, kg | 36.00 (22.7, 59.0) |
| Training session | 20.0 (10, 23) |
| Diagnosis | |
| Cerebral palsy, spastic type | 12 |
| Ataxic quadriparesis | 4 |
| Traumatic brain injury | 1 |
| Pre-Training | Post-Training | |
|---|---|---|
| Lying and rolling | 100.0 (100.0, 100.0) | 100.0 (100.0, 100.0) |
| Sitting | 100.0 (65.0, 100.0) | 100.0 (70.0, 100.0) * |
| Crawling and kneeling | 86.9 (9.5, 100.0) | 94.1 (11.9, 100.0) * |
| Standing | 57.7 (2.6, 94.9) | 69.2 (12.8, 94.9) * |
| Walking, running, and jumping | 49.3 (0.0, 97.2) | 50.0 (6.9, 97.2) * |
| Total GMFM | 78.86 (35.41, 98.41) | 82.38 (49.26, 98.41) * |
| Distance at Time | Pre-Training | Post-Training |
|---|---|---|
| 1 min | 35.45 (1.58, 63.52) | 43.21 (7.50, 120.30) * |
| 2 min | 77.28 (3.16, 121.10) | 95.54 (13.50, 186.90) * |
| 3 min | 117.58 (4.72, 193.80) | 145.09 (17.20, 278.30) * |
| 4 min | 155.15 (6.40, 257.92) | 190.87 (21.00, 341.34) * |
| 5 min | 188.22 (7.82, 337.14) | 239.43 (26.40, 425.82) * |
| 6 min | 223.10 (9.48, 415.50) | 284.28 (30.80, 500.12) * |
| Pre-Training | Post-Training | |
|---|---|---|
| 10 MWT (comfortable speed, m/s) | 0.49 (0.03, 1.03) | 0.69 (0.13, 2.40) * |
| 10 MWT (maximal speed, m/s) | 0.68 (0.03, 1.51) | 0.91 (0.14, 2.55 ) * |
| Median (Minimum, Maximum) | |
|---|---|
| Dimensions | 4.0 (4.0, 5.0) |
| Weight | 3.0 (2.0, 4.0) |
| Adjustment | 3.0 (3.0, 5.0) |
| Safety | 4.5 (3.0, 5.0) |
| Durability | 4.5 (4.0, 5.0) |
| Ease of use | 4.0 (3.0, 5.0) |
| Comfort | 4.0 (2.0, 5.0) |
| Effectiveness | 5.0 (3.0, 5.0) |
| Total | 34.0 (25.0, 37.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, J.; Lee, J.; Choi, T.; Choi, W.; Kim, T.; Kwak, K.; Kim, S.; Kim, K.; Kim, D. Feasibility of Overground Gait Training Using a Joint-Torque-Assisting Wearable Exoskeletal Robot in Children with Static Brain Injury. Sensors 2022, 22, 3870. https://0-doi-org.brum.beds.ac.uk/10.3390/s22103870
Hong J, Lee J, Choi T, Choi W, Kim T, Kwak K, Kim S, Kim K, Kim D. Feasibility of Overground Gait Training Using a Joint-Torque-Assisting Wearable Exoskeletal Robot in Children with Static Brain Injury. Sensors. 2022; 22(10):3870. https://0-doi-org.brum.beds.ac.uk/10.3390/s22103870
Chicago/Turabian StyleHong, Juntaek, Jongweon Lee, Taeyoung Choi, Wooin Choi, Taeyong Kim, Kyuwan Kwak, Seongjun Kim, Kyeongyeol Kim, and Daehyun Kim. 2022. "Feasibility of Overground Gait Training Using a Joint-Torque-Assisting Wearable Exoskeletal Robot in Children with Static Brain Injury" Sensors 22, no. 10: 3870. https://0-doi-org.brum.beds.ac.uk/10.3390/s22103870