
Microwave Ablation of Liver, Kidney and Lung Lesions: One-Month Response and Manufacturer’s Charts’ Reliability in Clinical Practice

 ,
, 
Abstract
:1. Introduction
2. Patients and Methods
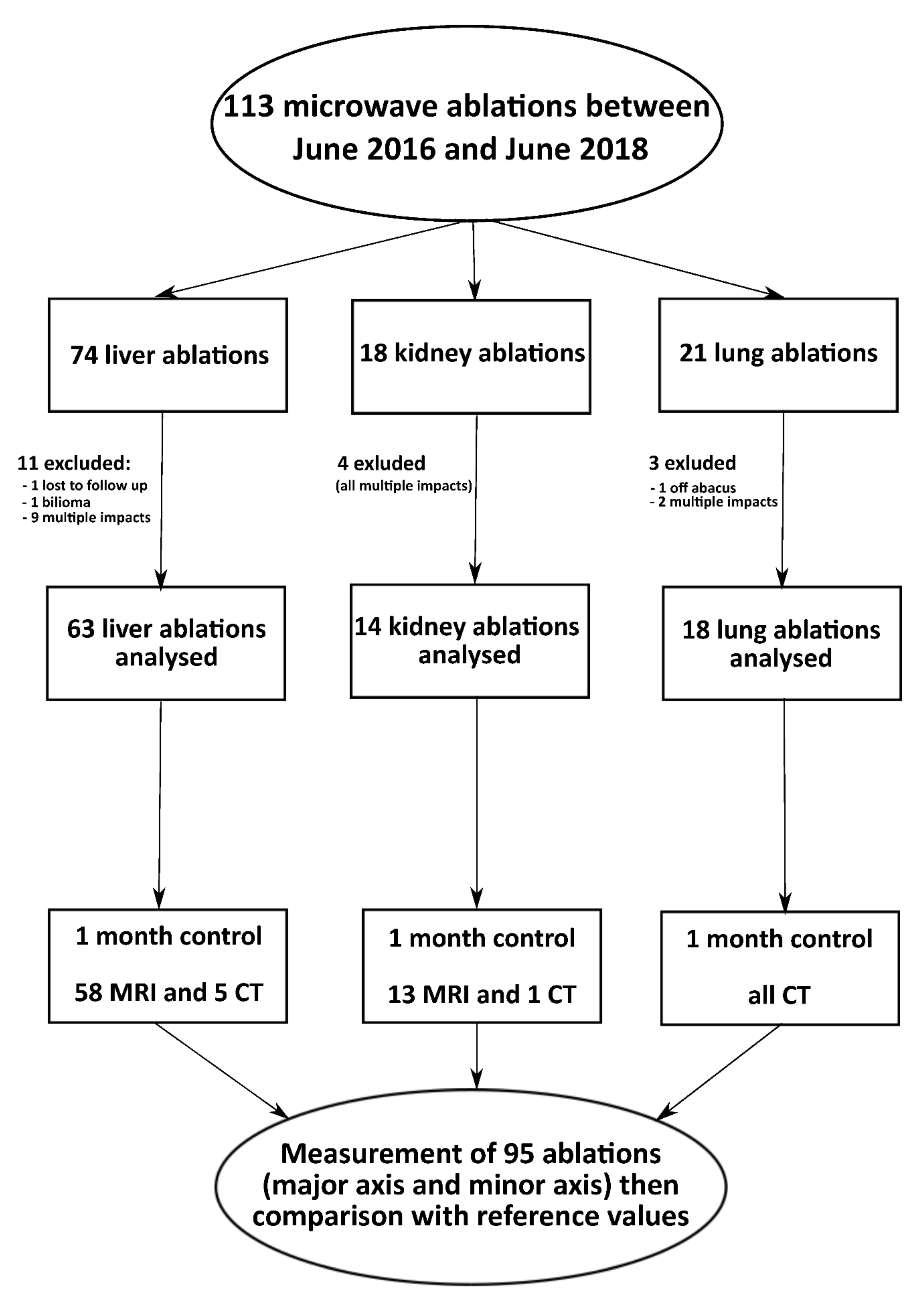
2.1. Patients
2.2. Ablation Procedure
2.3. Endpoints and Assessments
2.4. Statistical Analysis
3. Results
3.1. Patients and Lesions Characteristics
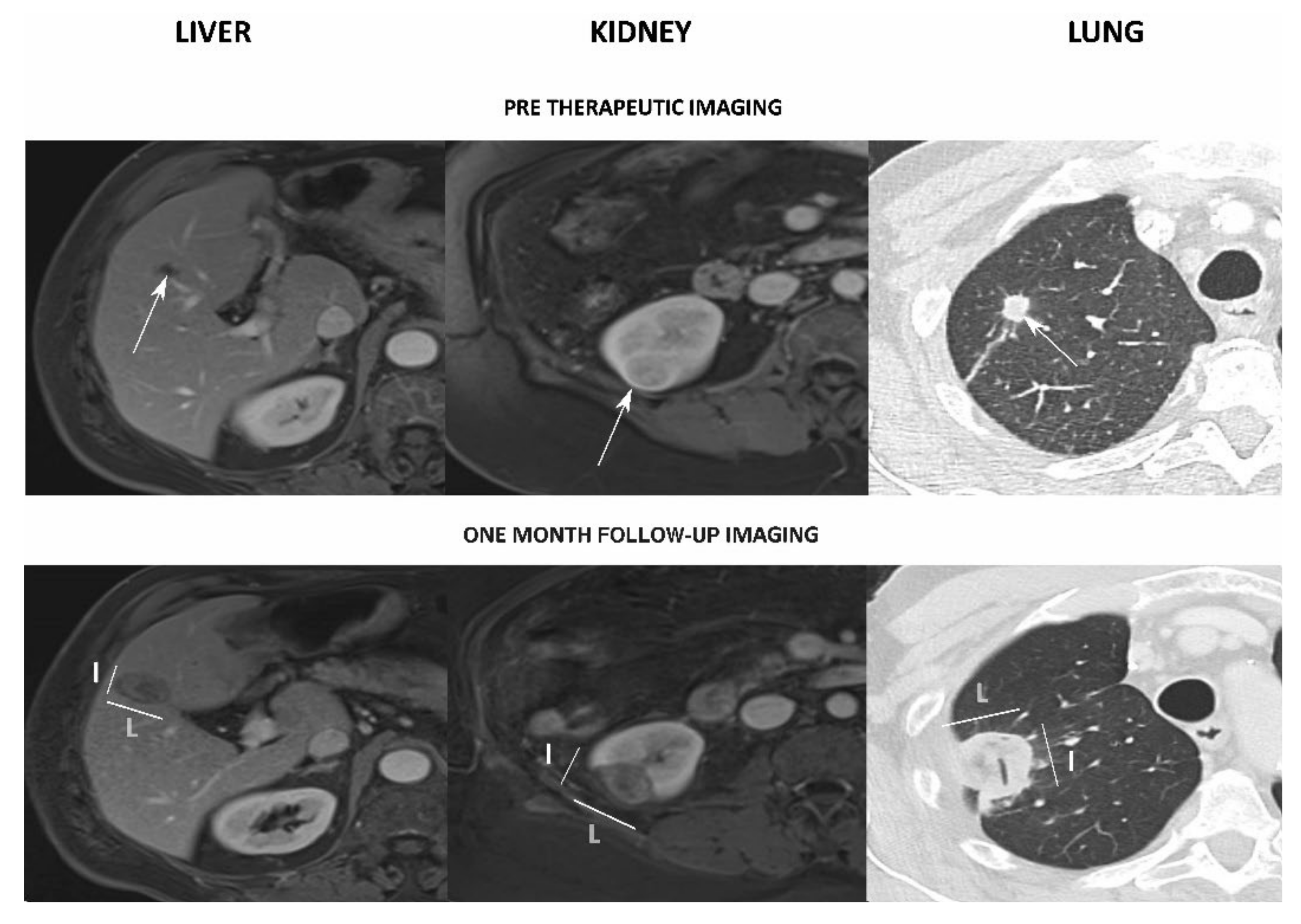
3.2. Early Local Response
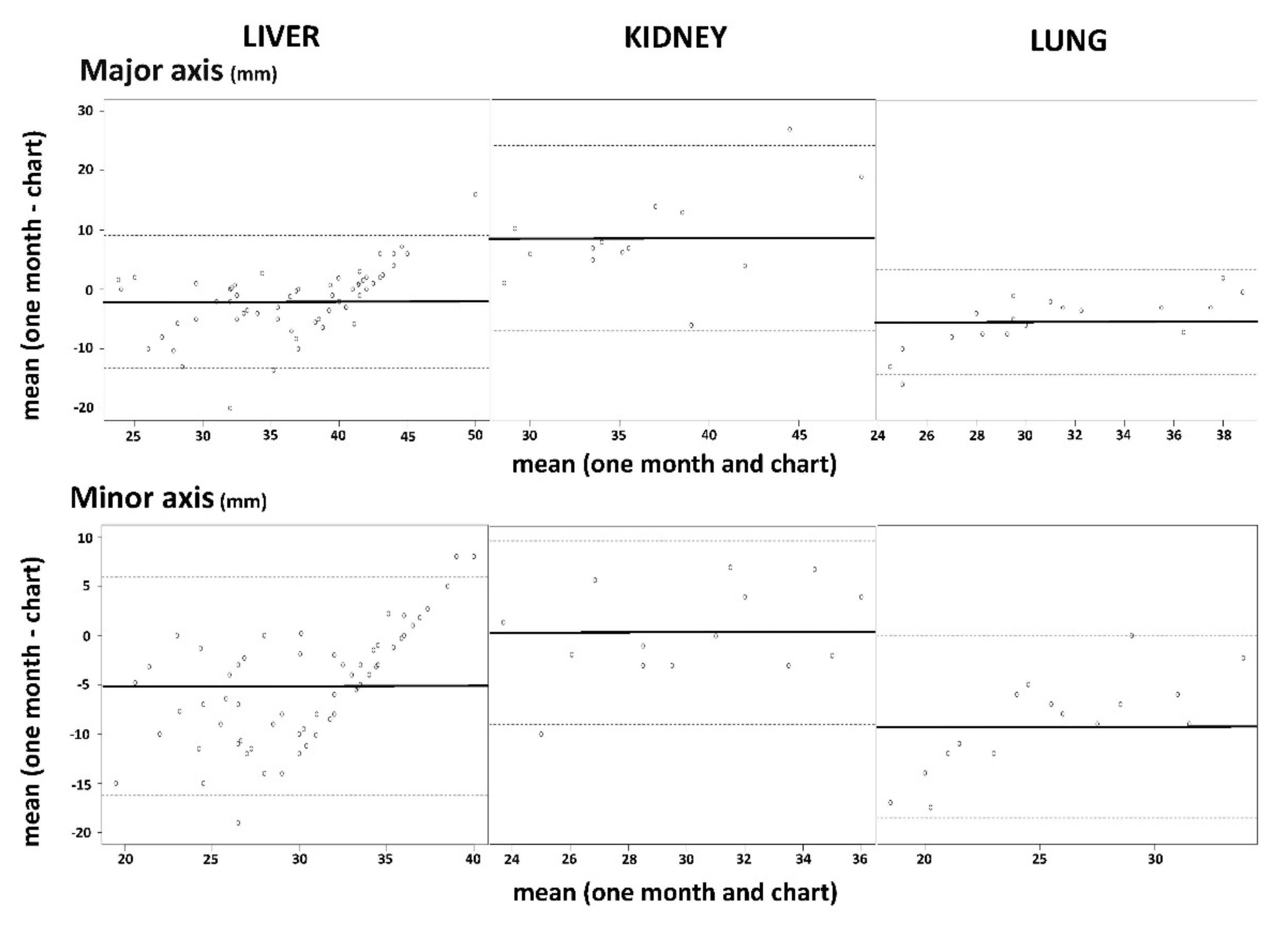
3.3. Microwave Ablations’ Reliability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eisele, R.M. Advances in local ablation of malignant liver lesions. World J. Gastroenterol. 2016, 22, 3885–3891. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liu, B.; Cao, P.; Wang, W.; Wang, W.; Chang, H.; Li, D.; Li, X.; Zhao, X.; Li, Y. Comparison between computed tomography-guided percutaneous microwave ablation and thoracoscopic lobectomy for stage I non-small cell lung cancer. Thorac. Cancer 2018, 9, 1376–1382. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.; Uzzo, R.G.; Allaf, M.E.; Bass, E.B.; Cadeddu, J.A.; Chang, A.; Clark, P.E.; Davis, B.J.; Derweesh, I.H.; Giambarresi, L. Renal Mass and Localized Renal Cancer: AUA Guideline. J. Urol. 2017, 198, 520–529. [Google Scholar] [CrossRef] [Green Version]
- Wright, A.S.; Sampson, L.A.; Warner, T.F.; Mahvi, D.M.; Lee, F.T. Radiofrequency versus microwave ablation in a hepatic porcine model. Radiology 2005, 236, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Schramm, W.; Yang, D.; Haemmerich, D. Contribution of direct heating, thermal conduction and perfusion during radiofrequency and microwave ablation. In Proceedings of the International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 5013–5016. [Google Scholar] [CrossRef]
- Yu, N.C.; Raman, S.S.; Kim, Y.J.; Lassman, C.; Chang, X.; Lu, D.S.K. Microwave liver ablation: Influence of hepatic vein size on heat-sink effect in a porcine model. J. Vasc. Interv. Radiol. 2008, 19, 1087–1092. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, R.; Rempp, H.; Erhard, L.; Blumenstock, G.; Pereira, P.L.; Claussen, C.D.; Clasen, S. Comparison of four microwave ablation devices: An experimental study in ex vivo bovine liver. Radiology 2013, 268, 89–97. [Google Scholar] [CrossRef]
- Winokur, R.S.; Du, J.Y.; Pua, B.B.; Talenfeld, A.D.; Sista, A.K.; Schiffman, M.A.; Trost, D.W.; Madoff, D.C. Characterization of in vivo ablation zones following percutaneous microwave ablation of the liver with two commercially available devices: Are manufacturer published reference values useful? J. Vasc. Interv. Radiol. 2014, 25, 1939–1946. [Google Scholar] [CrossRef]
- Alonzo, M.; Bos, A.; Bennett, S.; Ferral, H. The EmprintTM Ablation System with ThermosphereTM Technology: One of the Newer Next-Generation Microwave Ablation Technologies. Semin. Interv. Radiol. 2015, 32, 335–338. [Google Scholar] [CrossRef] [Green Version]
- De Cobelli, F.; Marra, P.; Ratti, F.; Ambrosi, A.; Colombo, M.; Damascelli, A.; Sallemi, C.; Gusmini, S.; Salvioni, M.; Diana, P.; et al. Microwave ablation of liver malignancies: Comparison of effects and early outcomes of percutaneous and intraoperative approaches with different liver conditions: New advances in interventional oncology: State of the art. Med. Oncol. 2017, 34, 49. [Google Scholar] [CrossRef]
- Zaidi, N.; Okoh, A.; Yigitbas, H.; Yazici, P.; Ali, N.; Berber, E. Laparoscopic microwave thermosphere ablation of malignant liver tumors: An analysis of 53 cases. J. Surg. Oncol. 2016, 113, 130–134. [Google Scholar] [CrossRef]
- Ierardi, A.M.; Mangano, A.; Floridi, C.; Dionigi, G.; Biondi, A.; Duka, E.; Lucchina, N.; Lianos, G.D.; Carrafiello, G. A new system of microwave ablation at 2450 MHz: Preliminary experience. Updates Surg. 2015, 67, 39–45. [Google Scholar] [CrossRef]
- Bottiglieri, A.; Ruvio, G.; O’Halloran, M.; Farina, L. Exploiting Tissue Dielectric Properties to Shape Microwave Thermal Ablation Zones. Sensors 2020, 20, 3960. [Google Scholar] [CrossRef] [PubMed]
- Cavagnaro, M.; Amabile, C.; Cassarino, S.; Tosoratti, N.; Pinto, R.; Lopresto, V. Influence of the target tissue size on the shape of ex vivo microwave ablation zones. Int. J. Hyperthermia. 2015, 31, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Hines-Peralta, A.U.; Pirani, N.; Clegg, P.; Cronin, N.; Ryan, T.P.; Liu, Z.; Goldberg, S.N. Microwave ablation: Results with a 2.45-GHz applicator in ex vivo bovine and in vivo porcine liver. Radiology 2006, 239, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Kodama, H.; Ueshima, E.; Howk, K.; Lee, S.W.; Erinjeri, J.P.; Solomon, S.B.; Srimathveeravalli, G. Temporal evaluation of the microwave ablation zone and comparison of CT and gross sizes during the first month post-ablation in swine lung. Diagn. Interv. Imaging 2019, 100, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Brace, C.L.; Diaz, T.A.; Hinshaw, J.L.; Lee, F.T. Tissue contraction caused by radiofrequency and microwave ablation: A laboratory study in liver and lung. J. Vasc. Interv. Radiol. 2010, 21, 1280–1286. [Google Scholar] [CrossRef] [Green Version]
- Sommer, C.M.; Sommer, S.A.; Mokry, T.; Gockner, T.; Gnutzmann, D.; Bellemann, N.; Schmitz, A.; Radeleff, B.A.; Kauczor, H.U.; Stampfl, U.; et al. Quantification of tissue shrinkage and dehydration caused by microwave ablation: Experimental study in kidneys for the estimation of effective coagulation volume. J. Vasc. Interv. Radiol. 2013, 24, 1241–1248. [Google Scholar] [CrossRef]
- Lee, J.K.; Siripongsakun, S.; Bahrami, S.; Raman, S.S.; Sayre, J.; Lu, D.S. Microwave ablation of liver tumors: Degree of tissue contraction as compared to RF ablation. Abdom. Radiol. 2016, 41, 659–666. [Google Scholar] [CrossRef]
- Meloni, M.F.; Smolock, A.; Cantisani, V.; Bezzi, M.; D’Ambrosio, F.; Proiti, M.; Lee, F.; Aiani, L.; Calliada, F.; Ferraioli, G. Contrast enhanced ultrasound in the evaluation and percutaneous treatment of hepatic and renal tumors. Eur. J. Radiol. 2015, 84, 1666–1674. [Google Scholar] [CrossRef]
- Lv, Y.; Jin, Y.; Yan, Q.; Yuan, D.; Wang, Y.; Li, X.; Shen, Y. The value of 64-slice spiral CT perfusion imaging in the treatment of liver cancer with argon-helium cryoablation. Oncol. Lett. 2016, 12, 4584–4588. [Google Scholar] [CrossRef] [Green Version]
- Joo, I.; Morrow, K.W.; Raman, S.S.; McWilliams, J.P.; Sayre, J.W.; Lu, D.S. CT-monitored minimal ablative margin control in single-session microwave ablation of liver tumors: An effective strategy for local tumor control. Eur. Radiol. 2022, 1, 1–9. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Organ | Power (Watt)/Time (Min) (Number of Ablations) | Major Axis Expected (mm) | Minor Axis Expected (mm) |
|---|---|---|---|
| Liver * (n = 63) | 100 w/10 min (n = 23) | 41 | 36 |
| 100 w/7 min (n = 8) | 40 | 35 | |
| 100 w/5 min (n = 1) | 39 | 34 | |
| 100 w/4 min (n = 1) | 38 | 33 | |
| 75 w/10 min (n = 7) | 36 | 33 | |
| 75 w/7 min (n = 2) | 35 | 32 | |
| 75 w/5 min (n = 5) | 33 | 30 | |
| 75 w/4 min (n = 2) | 32 | 29 | |
| 75 w/2.30 min (n = 8) | 30 | 27 | |
| 45 w/5 min (n = 2) | 27 | 27 | |
| 45 w/4 min (n = 2) | 26 | 26 | |
| 45 w/2.30 min (n = 2) | 24 | 23 | |
| Kidney ** (n = 14) | 100 w/2.30 min (n = 2) | 29 | 26 |
| 75 w/7 min (n = 5) | 32 | 31 | |
| 75 w/5 min (n = 2) | 30 | 29 | |
| 75 w/4 min (n = 2) | 28 | 27 | |
| 75 w/2.30 min (n = 2) | 25 | 23 | |
| 45 w/5 min (n = 1) | 25 | 25 | |
| Lung * (n = 18) | 75 w/5 min (n = 1) | 38 | 34 |
| 75 w/4 min (n = 1) | 38 | 33 | |
| 75 w/2.30 min (n = 3) | 37 | 32 | |
| 45 w/10 min (n = 1) | 34 | 30 | |
| 45 w/5 min (n = 4) | 33 | 29 | |
| 45 w/2.30 min (n = 8) | 32 | 27 |
| Characteristics | Liver | Kidney | Lung |
|---|---|---|---|
| Patients, n (men/women) | 31 (22/9) | 13 (9/4) | 11 (6/5) |
| Lesions, n | 63 | 14 | 18 |
| Mean age, years (SD) | 68 (±10) | 71 (±13) | 65 (±9) |
| Tumour origin, n (%) | |||
| Primitive | 14/31 (45%) | 12/13 (92%) | 3/11 (27%) |
| Metastatic | 17/31 (55%) | 1/13 (8%) | 8/11 (63%) |
| Metastatic origin, n (%) | |||
| Colon | 16/17 (94%) | 1/1 (100%) | 7/8 (87%) |
| Others | 1/17 (6%) | 0/1 (0%) | 1/8 (23%) |
| Tumour size, mean (SD) [range], mm | |||
| Long axis | 19.5 (±7.6) [8;35] | 23.7 (±6.5) [13;37] | 9.9 (±5.5) [5;25] |
| Minor axis | 15.5 (±6.2) [6;29] | 19.4 (±6.6) [9;30] | 7.5 (±4.8) [2;19] |
| Needle guidance (per lesion), n (%) | |||
| CT | 19/63 (30%) | 12/14 (86%) | 12/18 (67%) |
| CBCT | 2/63 (3%) | 2/14 (4%) | 6/18 (33%) |
| US | 42/63 (67%) | 0/14 (0%) | 0/18 (0%) |
| Follow-up imaging (per patient), n (%) | |||
| MRI | 28/31 (90%) | 12/13 (92%) | 0/11 (0%) |
| CT | 3/31 (10%) | 1/13 (8%) | 11/11 (100%) |
| One-month response (per lesion), n (%) | |||
| Complete | 58/63 (92%) | 13/14 (93%) | 18/18 (100%) |
| Partial | 5/63 (8%) | 1/14 (7%) | 0/18 (0%) |
| Charts (mm) | One-Month Follow-Up (mm) | p-Values | |
|---|---|---|---|
| Liver | |||
| Major axis, mean (SD) [range] (mm) | 37.4 (±5.1) [24;44] | 35.3 (±7.9) [22–46] | 0.006 |
| Minor axis, mean (SD) [range] (mm) | 32.9 (±3.9) [23;36] | 27.7 (±7.0) [12–38] | <0.001 |
| Sphericity index, mean (SD) [range] | 0.78 (±0.06) [0.7;1] | 0.63 (±0.17) [0.32–0.9] | <0.001 |
| Kidney | |||
| Major axis, mean (SD) [range] (mm) | 32.0 (±5.1) [24;42] | 40.7 (±8.5) [29–58] | 0.003 |
| Minor axis, mean (SD) [range] (mm) | 29.9 (±3.7) [23;36] | 30.3 (±5.3) [20–38] | 0.67 |
| Sphericity index, mean (SD) [range] | 0.89 (±0.09) [0.7;1] | 0.60 (±0.23) [0.43–0.97] | 0.005 |
| Lung | |||
| Major axis, mean (SD) [range] (mm) | 33.7 (±3.3) [30;40] | 28.2 (±6.4) [17–39] | <0.001 |
| Minor axis, mean (SD) [range] (mm) | 29.5 (±3.0) [27;36] | 20.2 (±6.6) [10–33] | <0.001 |
| Sphericity index, mean (SD) [range] | 0.77 (±0.03) [0.71;0.81] | 0.52 (±0.2) [0.25–0.93] | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frandon, J.; Akessoul, P.; Kammoun, T.; Dabli, D.; de Forges, H.; Beregi, J.-P.; Greffier, J. Microwave Ablation of Liver, Kidney and Lung Lesions: One-Month Response and Manufacturer’s Charts’ Reliability in Clinical Practice. Sensors 2022, 22, 3973. https://0-doi-org.brum.beds.ac.uk/10.3390/s22113973
Frandon J, Akessoul P, Kammoun T, Dabli D, de Forges H, Beregi J-P, Greffier J. Microwave Ablation of Liver, Kidney and Lung Lesions: One-Month Response and Manufacturer’s Charts’ Reliability in Clinical Practice. Sensors. 2022; 22(11):3973. https://0-doi-org.brum.beds.ac.uk/10.3390/s22113973
Chicago/Turabian StyleFrandon, Julien, Philippe Akessoul, Tarek Kammoun, Djamel Dabli, Hélène de Forges, Jean-Paul Beregi, and Joël Greffier. 2022. "Microwave Ablation of Liver, Kidney and Lung Lesions: One-Month Response and Manufacturer’s Charts’ Reliability in Clinical Practice" Sensors 22, no. 11: 3973. https://0-doi-org.brum.beds.ac.uk/10.3390/s22113973