
Personalised Gait Recognition for People with Neurological Conditions

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
Pre-Processing
2.2. Deep Learning Models
2.2.1. Neural Network Based on Extracted Features
2.2.2. Convolutional Neural Network
2.3. Personalisation Method
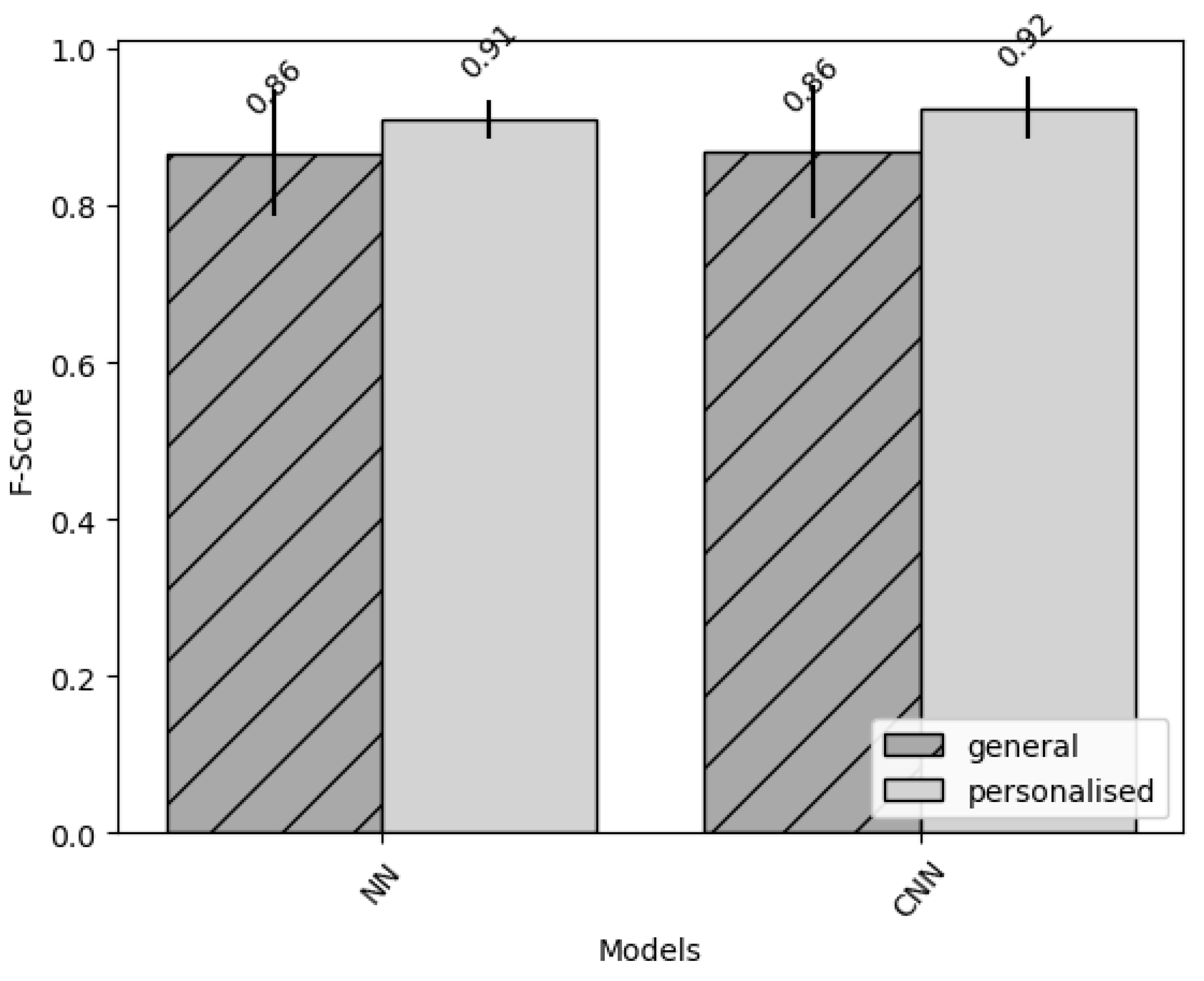
3. Results
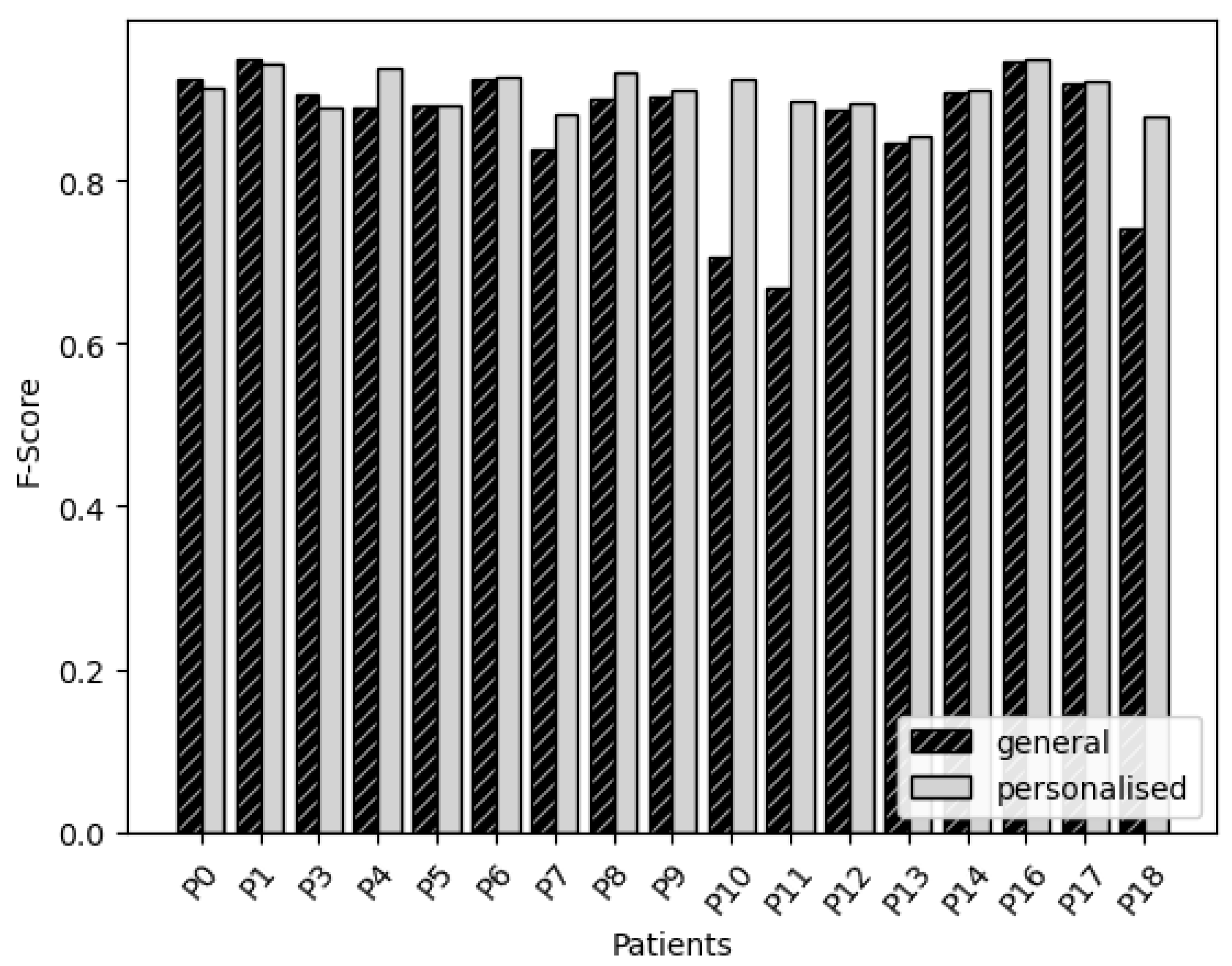
3.1. Neural Network Based on Features
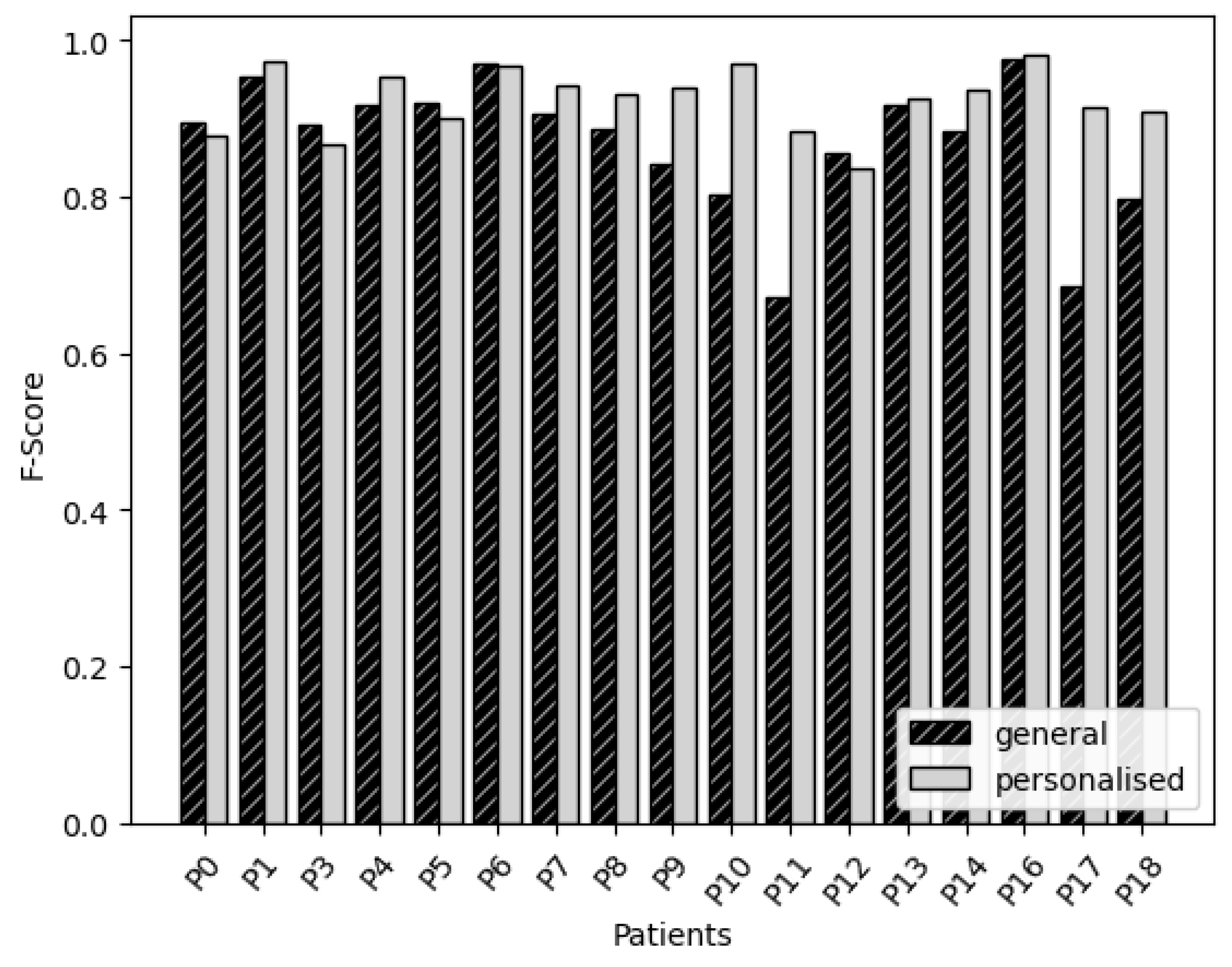
3.2. Convolutional Neural Network
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PNCs | People with Neurological Conditions |
| PD | Parkinson’s Disease |
| FOG | Freeze Of Gait |
| DL | Deep Learning |
| ML | Machine Learning |
| NN | Neural Network |
| CNN | Convolutional Neural Network |
| CNS | Campus Neurólogico Sénior |
| MDS-UPDRS | Movement Disorder Society’s Unified Parkinson’s Disease Rating Scale |
| H&Y | Hoehn and Yahr |
| S&E | Schwab and England |
| ADL | Activities of Daily Living |
| MiniBEST | Mini-Best Test |
| OM | Open Movement |
| Vector Magnitude |
References
- Tinazzi, M.; Geroin, C.; Erro, R.; Marcuzzo, E.; Cuoco, S.; Ceravolo, R.; Mazzucchi, S.; Pilotto, A.; Padovani, A.; Romito, L.M.; et al. Functional motor disorders associated with other neurological diseases: Beyond the boundaries of “organic” neurology. Eur. J. Neurol. 2021, 28, 1752–1758. [Google Scholar] [CrossRef] [PubMed]
- Moon, Y.; Sung, J.; An, R.; Hernandez, M.E.; Sosnoff, J.J. Gait variability in people with neurological disorders: A systematic review and meta-analysis. Hum. Mov. Sci. 2016, 47, 197–208. [Google Scholar] [CrossRef] [PubMed]
- Del Din, S.; Godfrey, A.; Mazzà, C.; Lord, S.; Rochester, L. Free-living monitoring of Parkinson’s disease: Lessons from the field. Mov. Disord. 2016, 31, 1293–1313. [Google Scholar] [CrossRef]
- Del Din, S.; Godfrey, A.; Galna, B.; Lord, S.; Rochester, L. Free-living gait characteristics in ageing and Parkinson’s disease: Impact of environment and ambulatory bout length. J. Neuroeng. Rehabil. 2016, 13, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouça-Machado, R.; Branco, D.; Fonseca, G.; Fernandes, R.; Abreu, D.; Guerreiro, T.; Ferreira, J.J.; Guerreiro, D.; Caniça, V.; Queimado, F.; et al. Kinematic and clinical outcomes to evaluate the efficacy of a multidisciplinary intervention on functional mobility in Parkinson’s disease. Front. Neurol. 2021, 12, 294. [Google Scholar] [CrossRef]
- Rehman, R.Z.U.; Guan, Y.; Shi, J.Q.; Alcock, L.; Yarnall, A.J.; Rochester, L.; Del Din, S. Investigating the Impact of Environment and Data Aggregation by Walking Bout Duration on Parkinson’s Disease Classification Using Machine Learning. Front. Aging Neurosci. 2022, 14, 808518. [Google Scholar] [CrossRef]
- Pham, M.H.; Elshehabi, M.; Haertner, L.; Del Din, S.; Srulijes, K.; Heger, T.; Synofzik, M.; Hobert, M.A.; Faber, G.S.; Hansen, C.; et al. Validation of a Step Detection Algorithm during Straight Walking and Turning in Patients with Parkinson’s Disease and Older Adults Using an Inertial Measurement Unit at the Lower Back. Front. Neurol. 2017, 8, 457. [Google Scholar] [CrossRef] [Green Version]
- Ji, N.; Zhou, H.; Guo, K.; Samuel, O.W.; Huang, Z.; Xu, L.; Li, G. Appropriate Mother Wavelets for Continuous Gait Event Detection Based on Time-Frequency Analysis for Hemiplegic and Healthy Individuals. Sensors 2019, 19, 3462. [Google Scholar] [CrossRef] [Green Version]
- Del Din, S.; Godfrey, A.; Rochester, L. Validation of an Accelerometer to Quantify a Comprehensive Battery of Gait Characteristics in Healthy Older Adults and Parkinson’s Disease: Toward Clinical and at Home Use. IEEE J. Biomed. Health Inform. 2016, 20, 838–847. [Google Scholar] [CrossRef]
- Rezvanian, S.; Lockhart, T.E. Towards Real-Time Detection of Freezing of Gait Using Wavelet Transform on Wireless Accelerometer Data. Sensors 2016, 16, 475. [Google Scholar] [CrossRef]
- Salarian, A.; Russmann, H.; Vingerhoets, F.; Dehollain, C.; Blanc, Y.; Burkhard, P.; Aminian, K. Gait Assessment in Parkinson’s Disease: Toward an Ambulatory System for Long-Term Monitoring. IEEE Trans. biomed. Eng. 2004, 51, 1434–1443. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.; Roth, N.; Haji Ghassemi, N.; Hannink, J.; Seel, T.; Klucken, J.; Gaßner, H.; Eskofier, B. Development and clinical validation of inertial sensor-based gait-clustering methods in Parkinson’s disease. J. NeuroEng. Rehabil. 2019, 16, 77. [Google Scholar] [CrossRef] [PubMed]
- Fu, Z.; He, X.; Wang, E.; Huo, J.; Huang, J.; Wu, D. Personalized Human Activity Recognition Based on Integrated Wearable Sensor and Transfer Learning. Sensors 2021, 21, 885. [Google Scholar] [CrossRef] [PubMed]
- Hammerla, N.; Halloran, S.; Ploetz, T. Deep, Convolutional, and Recurrent Models for Human Activity Recognition using Wearables. arXiv 2016, arXiv:1604.08880. [Google Scholar]
- Guan, Y.; Plötz, T. Ensembles of Deep LSTM Learners for Activity Recognition Using Wearables. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2017, 1, 1–28. [Google Scholar] [CrossRef] [Green Version]
- Gao, J.; Gu, P.; Ren, Q.; Zhang, J.; Song, X. Abnormal Gait Recognition Algorithm Based on LSTM-CNN Fusion Network. IEEE Access 2019, 7, 163180–163190. [Google Scholar] [CrossRef]
- Wang, J.; Chen, Y.; Hao, S.; Peng, X.; Hu, L. Deep learning for sensor-based activity recognition: A survey. Pattern Recognit. Lett. 2019, 119, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Khandelwal, S.; Wickström, N. Identification of gait events using expert knowledge and continuous wavelet transform analysis. In Proceedings of the 7th International Conference on Bio-inspired Systems and Signal Processing (BIOSIGNALS 2014), Angers, France, 3–6 March 2014; pp. 197–204. [Google Scholar]
- Ekinci, M. Human identification using gait. Turk. J. Electr. Eng. Comput. Sci. 2006, 14, 267–291. [Google Scholar]
- Boyd, J.E.; Little, J.J. Biometric Gait Recognition. In Advanced Studies in Biometrics, Proceedings of the Summer School on Biometrics, Alghero, Italy, 2–6 June 2003; Revised Selected Lectures and Papers; Springer: Berlin/Heidelberg, Germany, 2005; pp. 19–42. [Google Scholar] [CrossRef] [Green Version]
- Cola, G.; Avvenuti, M.; Musso, F.; Vecchio, A. Personalized gait detection using a wrist-worn accelerometer. In Proceedings of the 2017 IEEE 14th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Eindhoven, The Netherlands, 9–12 May 2017; pp. 173–177. [Google Scholar] [CrossRef]
- Rodríguez-Martín, D.; Samà, A.; Pérez-López, C.; Català, A.; Moreno Arostegui, J.M.; Cabestany, J.; Bayés, À.; Alcaine, S.; Mestre, B.; Prats, A.; et al. Home detection of freezing of gait using support vector machines through a single waist-worn triaxial accelerometer. PLoS ONE 2017, 12, e0171764. [Google Scholar] [CrossRef]
- Cook, D.; Feuz, K.D.; Krishnan, N.C. Transfer learning for activity recognition: A survey. Knowl. Inf. Syst. 2013, 36, 537–556. [Google Scholar] [CrossRef] [Green Version]
- Ding, R.; Li, X.; Nie, L.; Li, J.; Si, X.; Chu, D.; Liu, G.; Zhan, D. Empirical study and improvement on deep transfer learning for human activity recognition. Sensors 2018, 19, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- An, S.; Bhat, G.; Gumussoy, S.; Ogras, U. Transfer Learning for Human Activity Recognition using Representational Analysis of Neural Networks. arXiv 2020, arXiv:2012.04479. [Google Scholar]
- Sadeghzadehyazdi, N.; Batabyal, T.; Acton, S.T. Modeling spatiotemporal patterns of gait anomaly with a CNN-LSTM deep neural network. Expert Syst. Appl. 2021, 185, 115582. [Google Scholar] [CrossRef]
- Li, F.; Shirahama, K.; Nisar, M.A.; Huang, X.; Grzegorzek, M. Deep Transfer Learning for Time Series Data Based on Sensor Modality Classification. Sensors 2020, 20, 4271. [Google Scholar] [CrossRef] [PubMed]
- Bächlin, M.; Hausdorff, J.; Roggen, D.; Giladi, N.; Plotnik, M.; Tröster, G. Online Detection of Freezing of Gait in Parkinson’s Disease Patients: A Performance Characterization. In Proceedings of the BODYNETS 2009—4th International ICST Conference on Body Area Networks, Los Angeles, CA, USA, 1–3 April 2009; p. 11. [Google Scholar] [CrossRef] [Green Version]
- Ladha, C.; Ladha, K.; Jackson, D.; Olivier, P. Shaker table validation of OpenMovement AX3 accelerometer. In Proceedings of the ICAMPAM 2013 AMHERST: 3rd International Conference on Ambulatory Monitoring of Physical Activity and Movement, Amherst, MA, USA, 17–19 June 2013; pp. 69–70. [Google Scholar]
- Siderowf, A. Schwab and England activities of daily living scale. In Encyclopedia of Movement Disorders; Academic Press: New York, NY, USA, 2010. [Google Scholar] [CrossRef]
- Schwab, R.S. Projection technique for evaluating surgery in Parkinson’s disease. In Proceedings of the Third Symposium on Parkinson’s Disease, Edinburgh, UK, 1 January 1969; E&S Livingstone: Edinburgh, UK, 1969; pp. 152–157. [Google Scholar]
- Franchignoni, F.; Horak, F.; Godi, M.; Nardone, A.; Giordano, A. Using psychometric techniques to improve the Balance Evaluation Systems Test: The mini-BESTest. J. Rehabil. Med. 2010, 42, 323–331. [Google Scholar] [CrossRef] [Green Version]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov. Disord. Off. J. Mov. Disord. Soc. 2008, 23, 2129–2170. [Google Scholar] [CrossRef]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression, and mortality. Neurology 1998, 50, 318. [Google Scholar] [CrossRef]
- Tsang, C.S.; Liao, L.R.; Chung, R.C.; Pang, M.Y. Psychometric properties of the Mini-Balance Evaluation Systems Test (Mini-BESTest) in community-dwelling individuals with chronic stroke. Phys. Ther. 2013, 93, 1102–1115. [Google Scholar] [CrossRef] [Green Version]
- Leddy, A.L.; Crowner, B.E.; Earhart, G.M. Utility of the Mini-BESTest, BESTest, and BESTest sections for balance assessments in individuals with Parkinson disease. J. Neurol. Phys. Ther. JNPT 2011, 35, 90. [Google Scholar] [CrossRef] [Green Version]
- Jackson, D. Open Movement. 2021. Available online: https://github.com/digitalinteraction/omconvert (accessed on 12 May 2022).
- Van Hees, V.T.; Fang, Z.; Langford, J.; Assah, F.; Mohammad, A.; Da Silva, I.C.; Trenell, M.I.; White, T.; Wareham, N.J.; Brage, S. Autocalibration of accelerometer data for free-living physical activity assessment using local gravity and temperature: An evaluation on four continents. J. Appl. Physiol. 2014, 117, 738–744. [Google Scholar] [CrossRef] [Green Version]
- Bulling, A.; Blanke, U.; Schiele, B. A Tutorial on Human Activity Recognition Using Body-Worn Inertial Sensors. ACM Comput. Surv. 2013, 46, 1–33. [Google Scholar] [CrossRef]
- Chong, J.; Tjurin, P.; Niemelä, M.; Jämsä, T.; Farrahi, V. Machine-learning models for activity class prediction: A comparative study of feature selection and classification algorithms. Gait Posture 2021, 89, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.M.; Lee, Y.K.; Lee, S.Y.; Kim, T.S. A triaxial accelerometer-based physical-activity recognition via augmented-signal features and a hierarchical recognizer. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 1166–1172. [Google Scholar] [CrossRef] [PubMed]
- Wallace, B.C.; Dahabreh, I.J. Class Probability Estimates are Unreliable for Imbalanced Data (and How to Fix Them). In Proceedings of the 2012 IEEE 12th International Conference on Data Mining, Brussels, Belgium, 10–13 December 2012; pp. 695–704. [Google Scholar] [CrossRef]
- Zebin, T.; Scully, P.J.; Ozanyan, K.B. Human activity recognition with inertial sensors using a deep learning approach. In Proceedings of the 2016 IEEE Sensors, Orlando, FL, USA, 30 October–3 November 2016; pp. 1–3. [Google Scholar]
- Gjoreski, H.; Bizjak, J.; Gjoreski, M.; Gams, M. Comparing deep and classical machine learning methods for human activity recognition using wrist accelerometer. In Proceedings of the IJCAI 2016 Workshop on Deep Learning for Artificial Intelligence, New York, NY, USA, 9–15 July 2016; Volume 10, p. 970. [Google Scholar]
- Yang, Q.; Zhang, Y.; Dai, W.; Pan, S.J. Transfer Learning; Cambridge University Press: Cambridge, UK, 2020. [Google Scholar] [CrossRef]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA; London, UK, 2016. [Google Scholar]
- Latah, M. Human action recognition using support vector machines and 3D convolutional neural networks. Int. J. Adv. Intell. Inform. 2017, 3, 47. [Google Scholar] [CrossRef]
- Jahn, K.; Zwergal, A.; Schniepp, R. Gait disturbances in old age: Classification, diagnosis, and treatment from a neurological perspective. Dtsch. Ärzteblatt Int. 2010, 107, 306. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Type of Parameter | Measurement Tool |
|---|---|
| Demographic and clinical data | Clinical interview |
| Disease-specific symptoms | PD patients—MDS-UPDRS and Hoehn and Yard scale |
| Stroke patients—STREAM and PASS | |
| Disease severity | Patient global impression (PGI) |
| Clinical global impression (CGI) | |
| Gait | 10 m walk test |
| Postural instability | Mini-Best Test |
| Functional mobility | The Timed Up and Go (TUG) test with and without a cognitive and manual dual-task |
| Physical capacity | 2 min step test |
| Five times sit to stand | |
| Functionality in daily living | Schwab and England Activities of Daily Living scale |
| Kinematic gait analysis | Axivity sensors during the 10 m walk test (S&E) |
| Assessment | Evaluates | Pathology | Scoring |
|---|---|---|---|
| S&E [30,31] | Independence in ADL | Any | 0–100: Higher S&E corresponds to a higher independence for ADL |
| MiniBEST [32] | Balance | Any | 0–32: Higher rating in MiniBEST corresponds to a better balance |
| MDS-UPDRS [33] | PD disease severity | PD | 0–200: Higher rating corresponds to higher disease severity |
| H&Y [34] | PD disease severity | PD | 1–5: Higher rating corresponds to higher disease severity |
| P | Pathology | YD | S&E | MiniBEST | MDS-UPDRS | H&Y | Age | G |
|---|---|---|---|---|---|---|---|---|
| P0 | PD | 2007 | 80 | 29 | 39 | 2 | 56 | M |
| P1 | PD | 2006 | 60 | 14 | 79 | 4 | 86 | M |
| P2 | Epilepsy | 1954 | Accelerometer problems | 84 | F | |||
| P3 | PD | NA | 80 | 29 | 49 | 2 | 79 | M |
| P4 | PD | NA | 100 | 29 | 56 | 1 | 68 | F |
| P5 | PD | 2004 | 70 | 24 | 93 | 2 | 75 | M |
| P6 | PD | 2014 | 50 | 11 | 115 | 4 | 78 | M |
| P7 | Stroke | 2019 | 70 | 30 | - | - | 65 | M |
| P8 | Polyneuropathy | 2019 | 70 | 10 | - | - | 80 | M |
| P9 | Lewy body dementia | 2011 | 40 | 14 | - | - | 79 | M |
| P10 | Alzheimer | 2016 | 20 | Aborted | - | - | 81 | F |
| P11 | PD | 2017 | 20 | 0 | 128 | 5 | 87 | F |
| P12 | Stroke | 2018 | 80 | 25 | - | - | 78 | F |
| P13 | Dementia | 2017 | 20 | 6 | - | - | 90 | F |
| P14 | Mild cognitive impairment | 2019 | 40 | 20 | - | - | 89 | M |
| P15 | PD | 2013 | Accelerometer problems | 70 | M | |||
| P16 | PD | 2001 | 90 | 31 | 43 | 2 | 57 | M |
| P17 | PD | 2008 | 60 | 24 | 90 | 4 | 67 | M |
| P18 | PD | NA | 40 | 17 | 107 | 2 | 77 | F |
| P19 | PD | 2009 | Accelerometer problems | 66 | M | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ingelse, L.; Branco, D.; Gjoreski, H.; Guerreiro, T.; Bouça-Machado, R.; Ferreira, J.J.; The CNS Physiotherapy Study Group. Personalised Gait Recognition for People with Neurological Conditions. Sensors 2022, 22, 3980. https://0-doi-org.brum.beds.ac.uk/10.3390/s22113980
Ingelse L, Branco D, Gjoreski H, Guerreiro T, Bouça-Machado R, Ferreira JJ, The CNS Physiotherapy Study Group. Personalised Gait Recognition for People with Neurological Conditions. Sensors. 2022; 22(11):3980. https://0-doi-org.brum.beds.ac.uk/10.3390/s22113980
Chicago/Turabian StyleIngelse, Leon, Diogo Branco, Hristijan Gjoreski, Tiago Guerreiro, Raquel Bouça-Machado, Joaquim J. Ferreira, and The CNS Physiotherapy Study Group. 2022. "Personalised Gait Recognition for People with Neurological Conditions" Sensors 22, no. 11: 3980. https://0-doi-org.brum.beds.ac.uk/10.3390/s22113980