Association between Polygenic Risk Score and One-Year Outcomes Following As-Needed Aflibercept Therapy for Exudative Age-Related Macular Degeneration

 ,
,
Abstract
:1. Introduction
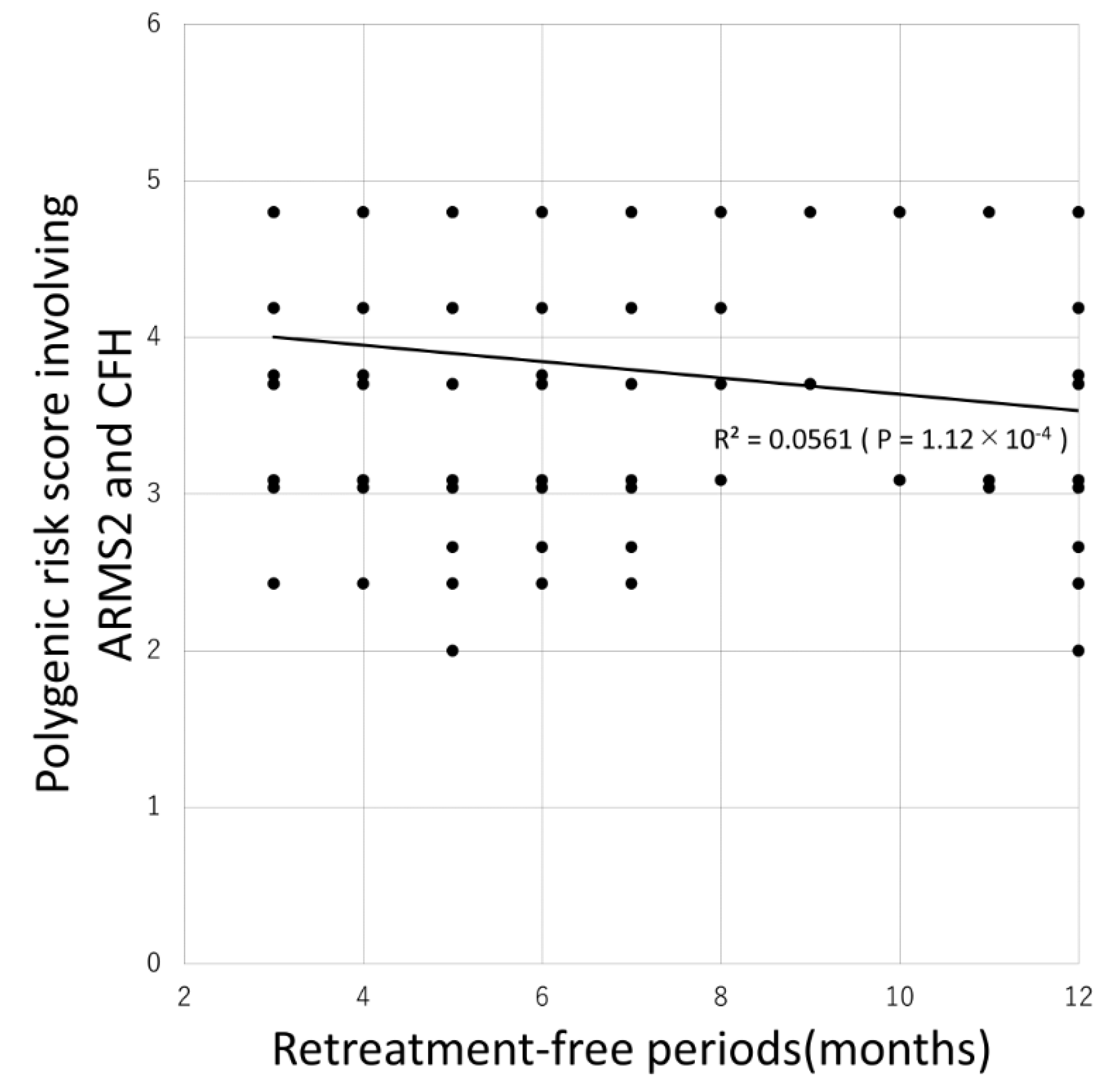
2. Results
3. Discussion
4. Materials and Methods
4.1. Subjects
4.2. Follow-Up
4.3. Genotyping and Calculation of PRSs
4.4. Statistical Analysis
Author Contributions
Funding
Conflicts of Interest
References
- Kawasaki, R.; Yasuda, M.; Song, S.J.; Chen, S.-J.; Jonas, J.B.; Wang, J.J.; Mitchell, P.; Wong, T.Y. The prevalence of age-related macular degeneration in Asians: A systematic review and meta-analysis. Ophthalmology 2010, 117, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Shijo, T.; Sakurada, Y.; Fukuda, Y.; Yoneyama, S.; Sugiyama, A.; Matsubara, M.; Kikushima, W.; Tanabe, N.; Parikh, R.; Kashiwagi, K. Association of CRP levels with ARMS2 and CFH variants in age-related macular degeneration. Int. Ophthalmol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.-Y.; Yamashiro, K.; Chen, L.J.; Ahn, J.; Huang, L.; Huang, L.; Cheung, C.M.G.; Miyake, M.; Cackett, P.D.; Yeo, I.Y.; et al. New loci and coding variants confer risk for age-related macular degeneration in East Asians. Nat. Commun. 2015, 6, 6063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holash, J.; Davis, S.; Papadopoulos, N.; Croll, S.D.; Ho, L.; Russell, M.; Boland, P.; Leidich, R.; Hylton, D.; Burova, E.; et al. VEGF-Trap: A VEGF blocker with potent antitumor effects. Proc. Natl. Acad. Sci. USA 2002, 99, 11393–11398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heier, J.S.; Brown, D.M.; Chong, V.; Korobelnik, J.-F.; Kaiser, P.K.; Nguyen, Q.D.; Kirchhof, B.; Ho, A.; Ogura, Y.; Yancopoulos, G.D.; et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology 2012, 119, 2537–2548. [Google Scholar] [CrossRef] [PubMed]
- Lalwani, G.A.; Rosenfeld, P.J.; Fung, A.E.; Dubovy, S.R.; Michels, S.; Feuer, W.; Davis, J.L.; Flynn, H.W., Jr.; Esquiabro, M. A variable-dosing regimen with intravitreal ranibizumab for neovascular age-related macular degeneration: Year 2 of the PrONTO Study. Am. J. Ophthalmol. 2009, 148, 43–58.e1. [Google Scholar] [CrossRef]
- Martin, D.F.; Maguire, M.G.; Ying, G.-S.; Grunwald, J.E.; Fine, S.L.; Jaffe, G.J.; CATT Research Group. Ranibizumab and bevacizumab for neovascular age-related macular degeneration. N. Engl. J. Med. 2011, 364, 1897–1908. [Google Scholar] [CrossRef] [Green Version]
- Chakravarthy, U.; Harding, S.P.; Rogers, C.A.; Downes, S.M.; Lotery, A.; Wordsworth, S.; Reeves, B.C. Ranibizumab versus bevacizumab to treat neovascular age-related macular degeneration: One-year findings from the IVAN randomized trial. Ophthalmology 2012, 119, 1399–1411. [Google Scholar] [CrossRef]
- Hatz, K.; Prunte, C. Treat and Extend versus Pro Re Nata regimens of ranibizumab in neovascular age-related macular degeneration: A comparative 12 Month study. Acta Ophthalmol. 2017, 95, e67–e72. [Google Scholar] [CrossRef]
- Augsburger, M.; Sarra, G.M.; Imesch, P. Treat and extend versus pro re nata regimens of ranibizumab and aflibercept in neovascular age-related macular degeneration: A comparative study. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 1889–1895. [Google Scholar] [CrossRef] [Green Version]
- Heesterbeek, T.J.; De Jong, E.K.; Acar, I.E.; Groenewoud, J.M.M.; Liefers, B.; Sánchez, C.I.; Peto, T.; Hoyng, C.B.; Pauleikhoff, D.; Hense, H.W.; et al. Genetic risk score has added value over initial clinical grading stage in predicting disease progression in age-related macular degeneration. Sci. Rep. 2019, 9, 6611. [Google Scholar] [CrossRef] [Green Version]
- Kang, H.M.; Kwon, H.J.; Yi, J.H.; Lee, C.S.; Lee, S.C. Subfoveal choroidal thickness as a potential predictor of visual outcome and treatment response after intravitreal ranibizumab injections for typical exudative age-related macular degeneration. Am. J. Ophthalmol. 2014, 157, 1013–1021. [Google Scholar] [CrossRef]
- Fukuda, Y.; Sakurada, Y.; Sugiyama, A.; Yoneyama, S.; Matsubara, M.; Kikushima, W.; Tanabe, N.; Parikh, R.; Kashiwagi, K. Pachydrusen in Fellow Eyes Predict Response to Aflibercept Monotherapy in Patients with Polypoidal Choroidal Vasculopathy. J. Clin. Med. 2020, 9, 2459. [Google Scholar] [CrossRef] [PubMed]
- Sakurada, Y.; Kikushima, W.; Sugiyama, A.; Yoneyama, S.; Tanabe, N.; Matsubara, M.; Iijima, H. AREDS simplified severity scale as a predictive factor for response to aflibercept therapy for typical neovascular age-related macular degeneration. Graefes Arch. Clin. Exp. Ophthalmol. 2018, 256, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Matsubara, M.; Sakurada, Y.; Sugiyama, A.; Fukuda, Y.; Parikh, R.; Kashiwagi, K. Response to photodynamic therapy combined with intravitreal aflibercept for polypoidal choroidal vasculopathy depending on fellow-eye condition:2-year results. PLoS ONE 2020, 15, e0237330. [Google Scholar] [CrossRef] [PubMed]
- Sakurada, Y.; Kubota, T.; Mabuchi, F.; Imasawa, M.; Tanabe, N.; Iijima, H. Association of LOC387715 A69S with vitreous hemorrhage in polypoidal choroidal vasculopathy. Am. J. Ophthalmol. 2008, 145, 1058–1062. [Google Scholar] [CrossRef]
- Sakurada, Y.; Kubota, T.; Imasawa, M.; Tsumura, T.; Mabuchi, F.; Tanabe, N.; Iijima, H. Angiographic lesion size associated with LOC387715 A69S genotype in subfoveal polypoidal choroidal vasculopathy. Retina 2009, 29, 1522–1526. [Google Scholar] [CrossRef]
- Sakurada, Y.; Kubota, T.; Imasawa, M.; Mabuchi, F.; Tateno, Y.; Tanabe, N.; Iijima, H. Role of complement factor H I62V and age-related maculopathy susceptibility 2 A69S variants in the clinical expression of polypoidal choroidal vasculopathy. Ophthalmology 2011, 118, 1402–1407. [Google Scholar] [CrossRef]
- Yoneyama, S.; Sakurada, Y.; Kikushima, W.; Sugiyama, A.; Tanabe, N.; Mabuchi, F.; Kubota, T.; Iijima, H. Genetic Factors Associated with Choroidal Vascular Hyperpermeability and Subfoveal Choroidal Thickness in Polypoidal Choroidal Vasculopathy. Retina 2016, 36, 1535–1541. [Google Scholar] [CrossRef]
- Fukuda, Y.; Sakurada, Y.; Yoneyama, S.; Kikushima, W.; Sugiyama, A.; Matsubara, M.; Tanabe, N.; Iijima, H. Clinical and genetic characteristics of pachydrusen in patients with exudative age-related macular degeneration. Sci. Rep. 2019, 9, 11906. [Google Scholar] [CrossRef] [Green Version]
- Kikushima, W.; Sakurada, Y.; Yoneyama, S.; Sugiyama, A.; Tanabe, N.; Kume, A.; Mabuchi, F.; Iijima, H. Incidence and risk factors of retreatment after three-monthly aflibercept therapy for exudative age-related macular degeneration. Sci. Rep. 2017, 7, 44020. [Google Scholar] [CrossRef] [PubMed]
- Valverde-Megias, A.; Veganzones-de-Castro, S.; Donate-Lopez, J.; Maestro-de-Las-Casas, M.L.; Megias-Fresno, A.; Garcia-Feijoo, J. ARMS2 A69S polymorphism is associated with the number of ranibizumab injections needed for exudative age-related macular degeneration in a pro re nata regimen during 4 years of follow-up. Graefes Arch. Clin. Exp. Ophthalmol. 2017, 255, 2091–2098. [Google Scholar] [CrossRef] [PubMed]
- Yamashiro, K.; Mori, K.; Honda, S.; Kano, M.; Yanagi, Y.; Obana, A.; Sakurada, Y.; Sato, T.; Nagai, Y.; Hikichi, T.; et al. A prospective multicenter study on genome wide associations to ranibizumab treatment outcome for age-related macular degeneration. Sci. Rep. 2017, 7, 9196. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, A.; Sakurada, Y.; Honda, S.; Miki, A.; Matsumiya, W.; Yoneyama, S.; Kikushima, W.; Iijima, H. Retreatment of Exudative Age-Related Macular Degeneration after Loading 3-Monthly Intravitreal Ranibizumab. Ophthalmologica 2018, 239, 52–59. [Google Scholar] [CrossRef]
- Yoneyama, S.; Sakurada, Y.; Kikushima, W.; Sugiyama, A.; Matsubara, M.; Fukuda, Y.; Tanabe, N.; Parikh, R.; Mabuchi, F.; Kashiwagi, K.; et al. Genetic factors associated with response to as-needed aflibercept therapy for typical neovascular age-related macular degeneration and polypoidal choroidal vasculopathy. Sci. Rep. 2020, 10, 7188. [Google Scholar] [CrossRef]
- Kuroda, Y.; Yamashiro, K.; Miyake, M.; Yoshikawa, M.; Nakanishi, H.; Oishi, A.; Tamura, H.; Ooto, S.; Tsujikawa, A.; Yoshimura, N. Factors Associated with Recurrence of Age-Related Macular Degeneration after Anti-Vascular Endothelial Growth Factor Treatment: A Retrospective Cohort Study. Ophthalmology 2015, 122, 2303–2310. [Google Scholar] [CrossRef]
- Mabuchi, F.; Mabuchi, N.; Sakurada, Y.; Yoneyama, S.; Kashiwagi, K.; Iijima, H.; Yamagata, Z.; Takamoto, M.; Aihara, M.; Iwata, T.; et al. Additive effects of genetic variants associated with intraocular pressure in primary open-angle glaucoma. PLoS ONE 2017, 12, e0183709. [Google Scholar] [CrossRef]
- Nannini, D.R.; Kim, H.; Fan, F.; Gao, X. Genetic Risk Score Is Associated with Vertical Cup-to-Disc Ratio and Improves Prediction of Primary Open-Angle Glaucoma in Latinos. Ophthalmology 2018, 125, 815–821. [Google Scholar] [CrossRef]
- Fan, B.J.; Bailey, J.C.; Igo, R.P.; Kang, J.H.; Boumenna, T.; Brilliant, M.H.; Budenz, D.L.; Fingert, J.H.; Gaasterland, T.; Gaasterland, D.; et al. Association of a Primary Open-Angle Glaucoma Genetic Risk Score With Earlier Age at Diagnosis. JAMA Ophthalmol. 2019. [Google Scholar] [CrossRef]
- Mabuchi, F.; Mabuchi, N.; Sakurada, Y.; Yoneyama, S.; Kashiwagi, K.; Iijima, H.; Yamagata, Z.; Takamoto, M.; Aihara, M.; Iwata, T.; et al. Genetic Variants Associated With the Onset and Progression of Primary Open-Angle Glaucoma. Am. J. Ophthalmol. 2020, 215, 135–140. [Google Scholar] [CrossRef]
- Sakurada, Y.; Yoneyama, S.; Sugiyama, A.; Tanabe, N.; Kikushima, W.; Mabuchi, F.; Kume, A.; Kubota, T.; Iijima, H. Prevalence and Genetic Characteristics of Geographic Atrophy among Elderly Japanese with Age-Related Macular Degeneration. PLoS ONE 2016, 11, e0149978. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Baseline Characteristics | Total | AMD (n = 129) | PCV(n = 132) | p-value |
|---|---|---|---|---|
| Age (years) | 74.8 ± 8.3 | 77.1 ± 8.1 | 72.5 ± 7.8 | 3.84 × 10−6 |
| Male gender | 188 (72%) | 86 (66.7%) | 102 (77.3%) | 0.056 |
| Baseline logMAR BCVA | 0.42 ± 0.37 | 0.50 ± 0.38 | 0.35 ± 0.34 | 1.2610−4 |
| ARMS2 A69S(rs10490924) T allele frequency | 63.2% | 68.2% | 58.3% | 0.019 |
| CFH I62V(rs800292) G allele frequency | 75.3% | 77.9% | 72.7% | 0.17 |
| C2-CFB-SKIV2L(rs429608) G allele frequency | 91.8% | 94.6% | 89.0% | 0.02 |
| C3 (rs2241394) G allele frequency | 94.3% | 94.6% | 89.4% | 0.03 |
| CETP (rs3764261) A allele frequency | 19.7% | 19.0% | 20.5% | 0.67 |
| ADAMTS9 (rs6795735) T allele frequency | 86.8% | 86.8% | 86.7% | 0.98 |
| Genetic Variants | Exudative AMD Risk Allele Frequency | Controls Risk Allele Frequency | Odds Ratio | 95% CI |
|---|---|---|---|---|
| ARMS2 A69S (rs10490924) T allele (risk allele) (T:G) | 0.632 (330:192) | 0.384 (132:212) | 2.76 | 2.06–3.66 |
| CFH I62V (rs800292) G allele (risk allele) (G:A) | 0.753 (393:129) | 0.599(206:138) | 2.04 | 1.52–2.74 |
| C3 (rs2241394) G allele (risk allele) (G:C) | 0.961 (492:30) | 0.901 (310:34) | 1.80 | 1.08–3.00 |
| ADAMTS9 (rs6795735) T allele (risk allele) (T:C) | 0.885 (453:69) | 0.791 (272:72) | 1.74 | 1.21–2.50 |
| SKIV2L-C2-CFB (rs429608) G allele (risk allele) (G:A) | 0.936 (479:43) | 0.884 (304:40) | 1.47 | 0.93–2.33 |
| CETP (rs3764261) A allele (risk allele) (A:T) | 0.197 (103:419) | 0.198 (68:286) | 0.97 | 0.69–1.36 |
| Variable | β-Coefficient | P Value |
|---|---|---|
| Age | 0.0034 | 0.096 |
| Male gender | 0.012 | 0.75 |
| Baseline VA | 0.614 | 3.0 × 10−31 |
| PRS involving ARMS2, CFH, C3, and ADAMTS9 | 0.041 | 0.046 |
| Variables | Requiring Retreatment (n = 175) | Without Retreatment (n = 86) | p-Value | Hazard Ratio | 95% CI |
|---|---|---|---|---|---|
| Age (year) | 76.0 ± 7.9 | 72.3 ± 8.6 | 2.3 × 10−3 | 1.07 | 1.03–1.11 |
| Male gender (%) | 126 (72.0%) | 62 (72.1%) | 0.99 | 1.32 | 0.71–2.49 |
| Baseline logMAR BCVA | 0.41 ± 0.37 | 0.44 ± 0.37 | 0.52 | 0.59 | 0.28–1.27 |
| PRS involving ARMS2 and CFH | 3.9 ± 0.75 | 3.5 ± 0.78 | 1.6 × 10−4 | 2.09 | 1.45–3.03 |
| Variable | β-Coefficient | p Value |
|---|---|---|
| Age | 0.021 | 0.17 |
| Male gender | 0.27 | 0.33 |
| Baseline VA | –0.86 | 0.011 |
| PRS involving ARMS2 and CFH | 0.75 | 2.42 × 10−6 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shijo, T.; Sakurada, Y.; Yoneyama, S.; Kikushima, W.; Sugiyama, A.; Matsubara, M.; Fukuda, Y.; Mabuchi, F.; Kashiwagi, K. Association between Polygenic Risk Score and One-Year Outcomes Following As-Needed Aflibercept Therapy for Exudative Age-Related Macular Degeneration. Pharmaceuticals 2020, 13, 257. https://0-doi-org.brum.beds.ac.uk/10.3390/ph13090257
Shijo T, Sakurada Y, Yoneyama S, Kikushima W, Sugiyama A, Matsubara M, Fukuda Y, Mabuchi F, Kashiwagi K. Association between Polygenic Risk Score and One-Year Outcomes Following As-Needed Aflibercept Therapy for Exudative Age-Related Macular Degeneration. Pharmaceuticals. 2020; 13(9):257. https://0-doi-org.brum.beds.ac.uk/10.3390/ph13090257
Chicago/Turabian StyleShijo, Taiyo, Yoichi Sakurada, Seigo Yoneyama, Wataru Kikushima, Atsushi Sugiyama, Mio Matsubara, Yoshiko Fukuda, Fumihiko Mabuchi, and Kenji Kashiwagi. 2020. "Association between Polygenic Risk Score and One-Year Outcomes Following As-Needed Aflibercept Therapy for Exudative Age-Related Macular Degeneration" Pharmaceuticals 13, no. 9: 257. https://0-doi-org.brum.beds.ac.uk/10.3390/ph13090257