
Evaluation of the Expression Profile of Irinotecan-Induced Diarrhea in Patients with Colorectal Cancer


Abstract
:1. Introduction
2. Results
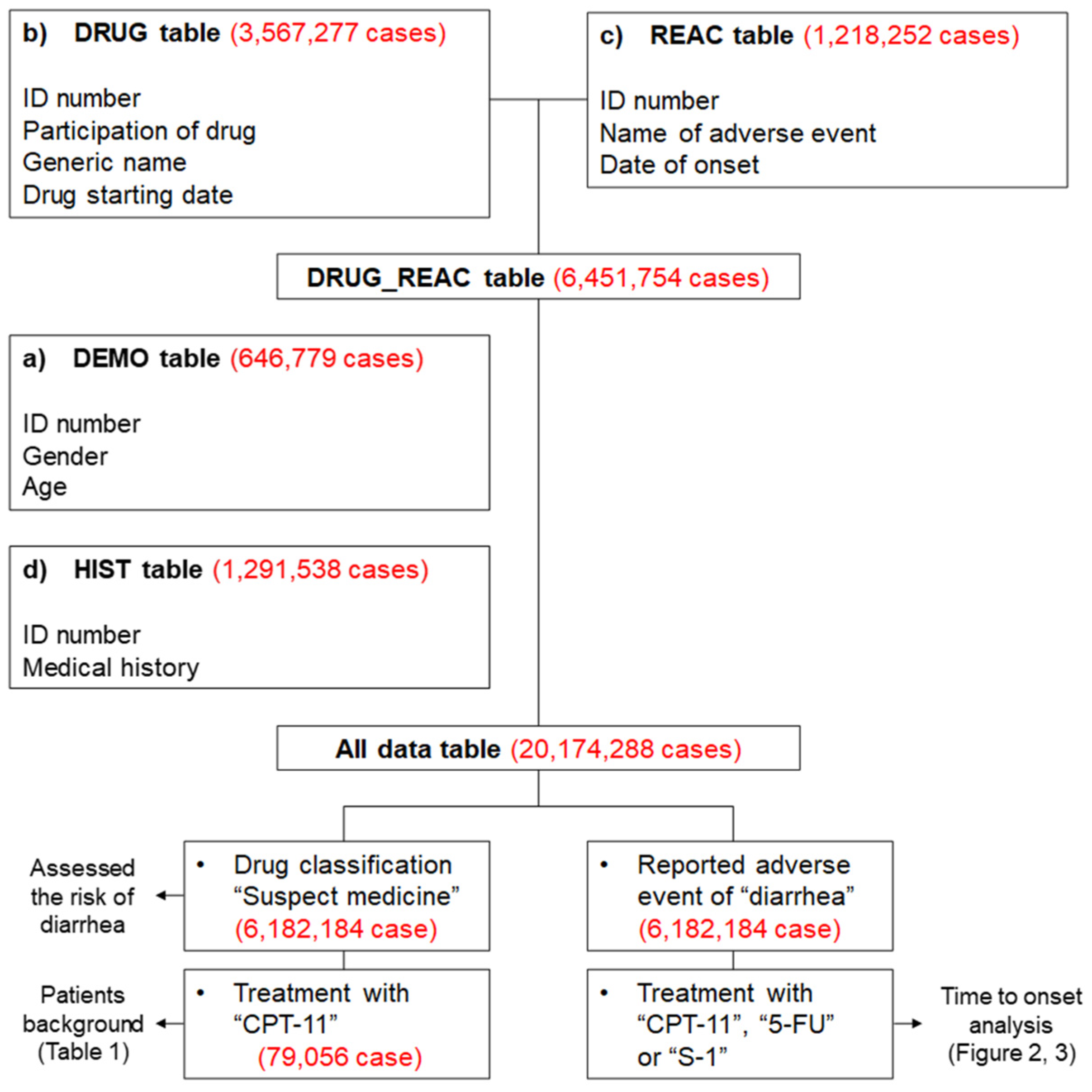
2.1. Presentation of Data
2.2. Diarrhea and Patient Background
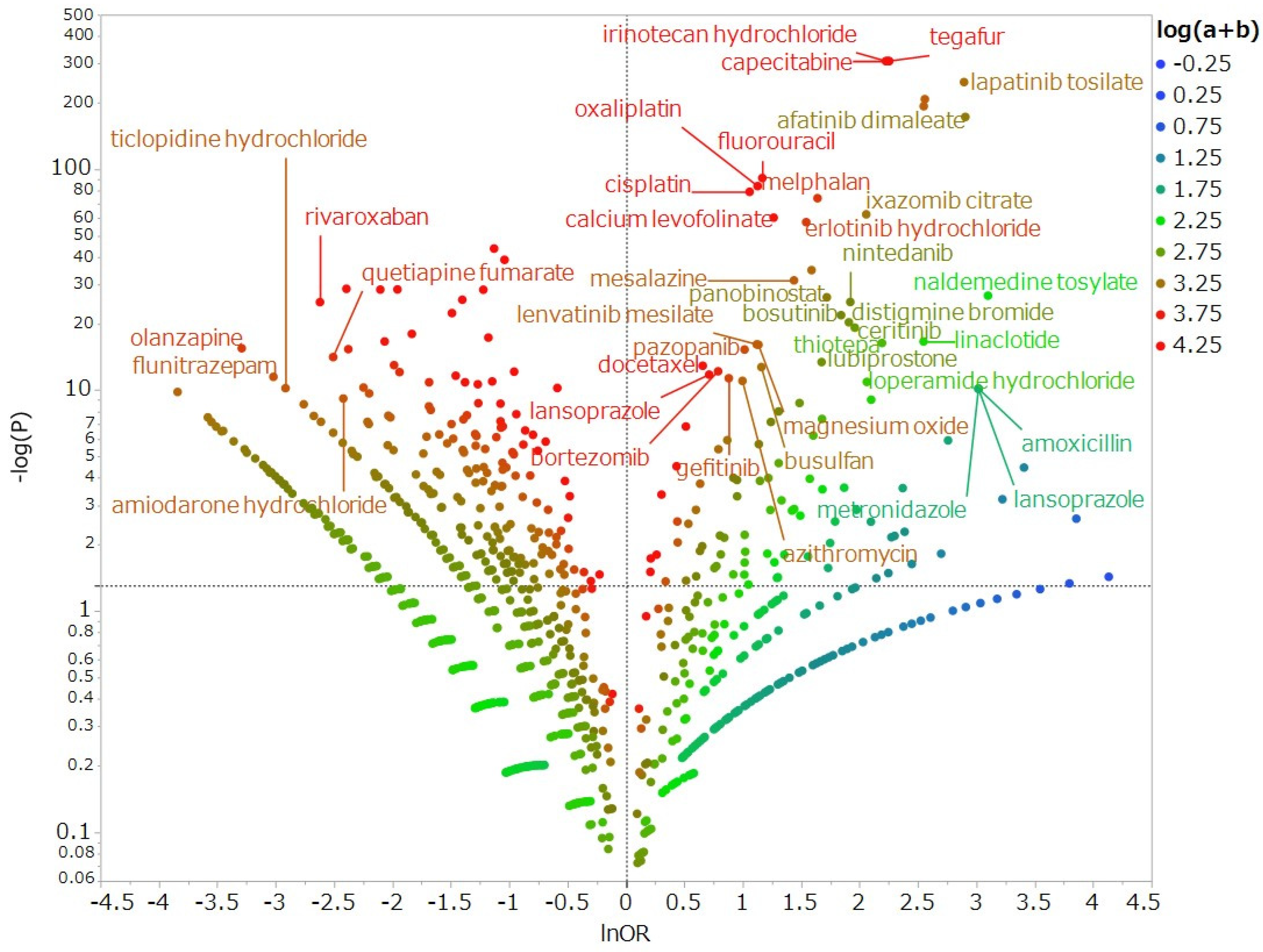
2.3. Diarrhea-Inducing Medications
2.4. Diarrhea as a Result of Drug–Drug Interaction
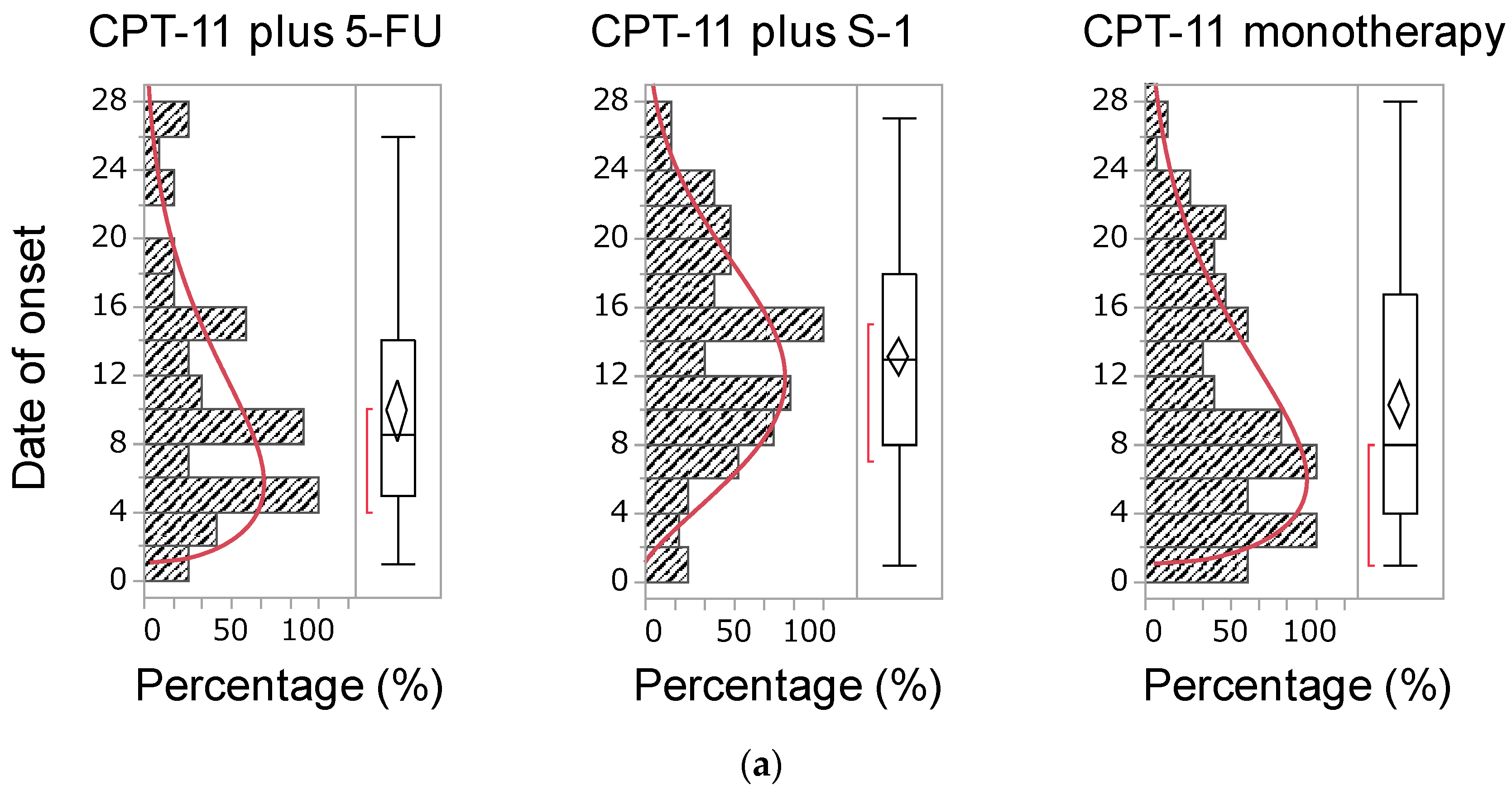
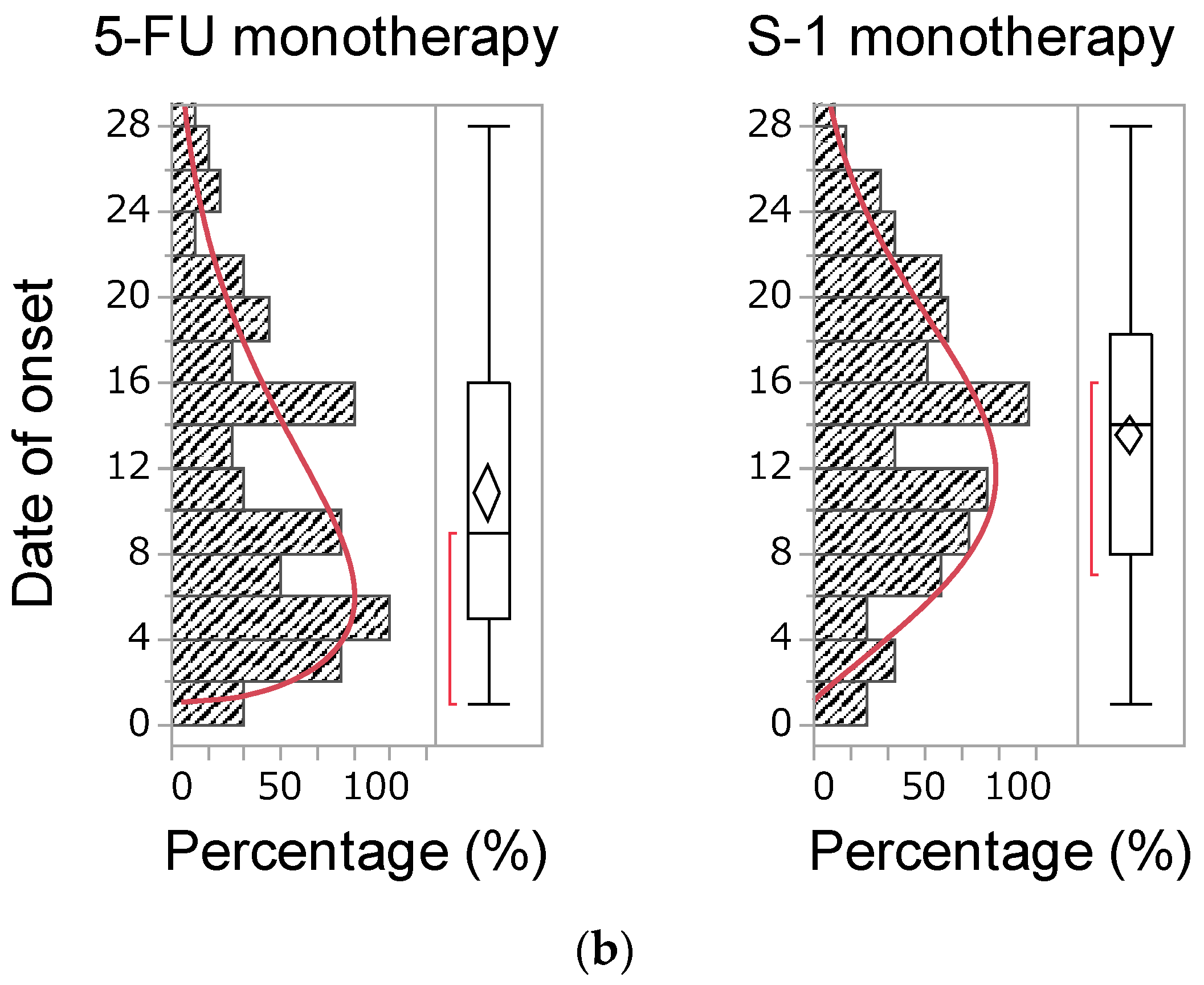
2.5. Time of Onset of Diarrhea
3. Discussion
3.1. Diarrhea as a Result of Drug–Drug Interaction
3.2. Time of Onset of Diarrhea
3.3. Limitations
4. Materials and Methods
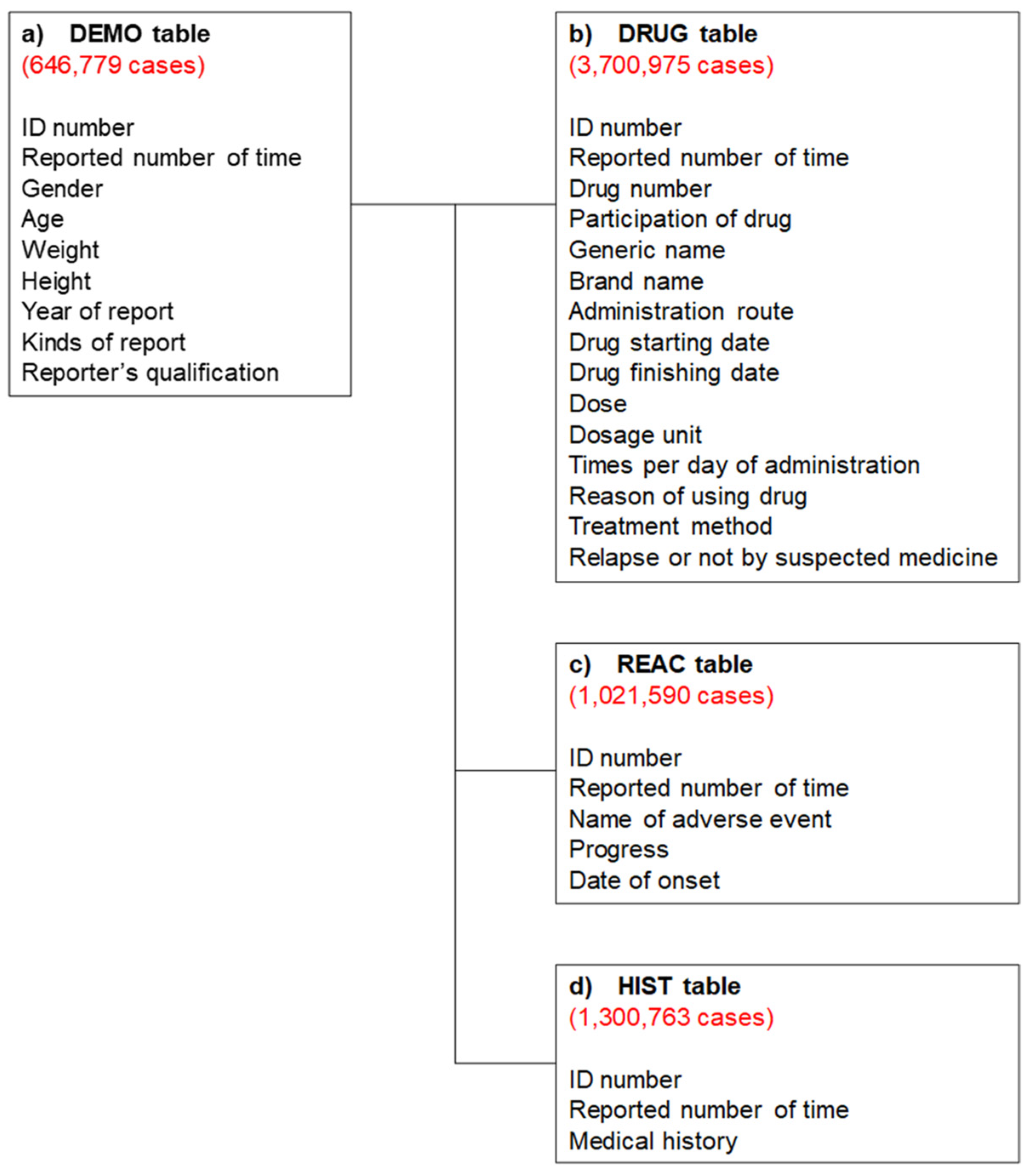
4.1. Database Information
4.2. Production of a Data Analysis Table
4.3. Analyzed Drugs and Adverse Event Terms
4.4. Relationship Between Suspected Medicines and Diarrhea
4.5. Onset Time of Diarrhea
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feely, J.; Soerjomataram, I.; Ervik, M.; Dikshit, R.; Eser, S.; Mathers, C. GLOBOCAN 2012 v1.1, Cancer Incidence and Mortality Worldwide: IARS Cancer Base No. 11 [Internet]; International Agency for Research on Cancer: Lyon, France, 2014. [Google Scholar]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Arain, M.A.; Chen, Y.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Farkas, L.; et al. Colon Cancer, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology Colon Cancer. J. Natl. Compr. Cancer Netw. 2021, 19, 329–359. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/020571s048lbl.pdf (accessed on 18 April 2021).
- Available online: https://dailymed.nlm.nih.gov/dailymed/drugInfo/camptosar (accessed on 18 April 2021).
- Saliba, F.; Hagipantelli, R.; Misset, J.L.; Bastian, G.; Vassal, G.; Bonnay, M.; Herait, P.; Cote, C.; Mahjoubi, M.; Mignard, D.; et al. Pathophysiology and therapy of irinotec-an-induced delayed-onset diarrhea in patients with advanced colorectal cancer: A prospective assessment. J. Clin. Oncol. 1998, 16, 2745–2751. [Google Scholar] [CrossRef] [PubMed]
- Hyatt, J.L.; Tsurkan, L.; Morton, C.L.; Yoon, K.J.; Harel, M.; Brumshtein, B.; Silman, I.; Sussman, J.L.; Wadkins, R.M.; Potter, P.M. Inhibition of acetylcholinesterase by the anticancer prodrug CPT-11. Chem. Interact. 2005, 157–158, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.info.pmda.go.jp/go/pack/4240404A1040_1_14/?view=frame&style=SGML&lang=ja (accessed on 18 April 2021).
- Longley, D.B.; Harkin, D.P.; Johnston, P.G. 5-Fluorouracil: Mechanisms of action and clinical strategies. Nat. Rev. Cancer 2003, 3, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Yasui, H.; Goto, A.; Arai, T.; Ura, T.; Hamaguchi, T.; Muro, K.; Shimada, Y.; Shirao, K. Phase I study of irinotecan and S-1 combination therapy in patients with metastatic gastric cancer. Int. J. Clin. Oncol. 2003, 8, 374–380. [Google Scholar] [CrossRef]
- Shirasaka, T.; Shimamato, Y.; Ohshimo, H.; Yamaguchi, M.; Kato, T.; Yonekura, K.; Fukushima, M. Development of a novel form of an oral 5-fluorouracil derivative (S-1) di-rected to the potentiation of the tumor selective cytotoxicity of 5-fluorouracil by two biochemical modulators. Anticancer Drugs 1996, 7, 548–557. [Google Scholar] [CrossRef]
- Peeters, M.; Price, T.J.; Cervantes, A.; Sobrero, A.F.; Ducreux, M.; Hotko, Y. Randomized phase III study of panitumumab with fluorouracil, leucovorin, and irinotecan (FOLFIRI) compared with FOLFIRI alone as second-line treatment in pa-tients with metastatic colorectal cancer. J. Clin. Oncol. 2010, 28, 4706–4713. [Google Scholar] [CrossRef]
- Yamada, Y.; Yamaguchi, T.; Matsumoto, H.; Ichikawa, Y.; Goto, A.; Kato, K.; Hamaguchi, T.; Shimada, Y. Phase II study of oral S-1 with irinotecan and bevacizumab (SIRB) as first-line therapy for patients with metastatic colorectal cancer. Investig. New Drugs 2011, 30, 1690–1696. [Google Scholar] [CrossRef]
- Yamada, Y.; Denda, T.; Gamoh, M.; Iwanaga, I.; Yuki, S.; Shimodaira, H.; Nakamura, M.; Yamaguchi, T.; Ohori, H.; Kobayashi, K.; et al. S-1 and irinotecan plus bevacizumab versus mFOLFOX6 or CapeOX plus bevacizumab as first-line treatment in patients with metastatic colorectal cancer (TRI-COLORE): A randomized, open-label, phase III, noninferiority trial. Ann. Oncol. 2018, 29, 624–631. [Google Scholar] [CrossRef]
- Yamada, M.; Handa, J. 2. Comparison of the Onset Time Profile among the Interferon Formulations in Adverse Drug Reaction of Suicide- or Diabetes-Related. Jpn. J. Pharmacoepidemiol. Yakuzai Ekigaku 2014, 19, 23–30. [Google Scholar] [CrossRef]
- Benson, A.B., III; Ajani, J.A.; Catalano, R.B.; Engelking, C.; Kornblau, S.M.; Martenson, J.A., Jr.; McCallum, R.; Mitchell, E.P.; O’Dorisio, T.M.; Vokes, E.E.; et al. Recommended Guidelines for the Treatment of Cancer Treatment-Induced Diarrhea. J. Clin. Oncol. 2004, 22, 2918–2926. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.ema.europa.eu/en/documents/product-information/teysuno-epar-product-information_en.pdf (accessed on 18 April 2021).
- Sasaki, Y.; Shimada, Y.; Ohtsu, A.; Ono, K.; Saijo, N. Simultaneous administration of CPT-11 and fluorouracil: Alteration of the pharma-cokinetics of CPT-11 and SN-38 in patients with advanced colorectal cancer. J. Natl. Cancer. Inst. 1994, 86, 1096–1098. [Google Scholar] [CrossRef] [Green Version]
- Maroun, J.A.; Anthony, L.B.; Blais, N.; Burkes, R.; Dowden, S.D.; Dranitsaris, G.; Samson, B.; Shah, A.; Thirlwell, M.P.; Vincent, M.D.; et al. Prevention and management of chemotherapy-induced diarrhea in patients with colorectal cancer: A consensus statement by the Canadian Working Group on Chemotherapy-Induced Diarrhea. Curr. Oncol. 2007, 14, 13–20. [Google Scholar] [CrossRef] [Green Version]
- Falcone, A.; Di Paolo, A.; Masi, G.; Allegrini, G.; Danesi, R.; Lencioni, M.; Pfanner, E.; Comis, S.; Del Tacca, M.; Conte, P. Sequence Effect of Irinotecan and Fluorouracil Treatment on Pharmacokinetics and Toxicity in Chemotherapy-Naive Metastatic Colorectal Cancer Patients. J. Clin. Oncol. 2001, 19, 3456–3462. [Google Scholar] [CrossRef] [PubMed]
- Maeda, R. JADER from Pharmacovigilance Point of View. Jpn. J. Pharmacoepidemiol. Yakuzai Ekigaku 2014, 19, 51–56. [Google Scholar] [CrossRef]
- Post-marketing Data Science Advisory Group. Leap toward much better safety measures in Japan. PMDRS 2014, 45, 98–105. [Google Scholar]
- Pariente, A.; Avillach, P.; Salvo, F.; Thiessard, F.; Miremont-Salamé, G.; Fourrier-Reglat, A.; Haramburu, F.; Bégaud, B.; Moore, N. Effect of Competition Bias in singnal generation. Drug Saf. 2012, 35, 855–864. [Google Scholar] [CrossRef] [PubMed]
- Avillach, P.; Salvo, F.; Thiessard, F.; Miremont-Salamé, G.; Fourrier-Réglat, A.; Haramburu, F.; Begaud, B.; Moore, N.; Pariente, A.; on behalf of l’Association des Centres Régionaux de Pharmacovigilance. Pilot evaluation of an automated method to decrease false-positive signals induced by co-prescriptions in spontaneous reporting databases. Pharmacoepidemiol. Drug Saf. 2013, 23, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.pmda.go.jp/files/000147250.pdf (accessed on 18 April 2021).
- Available online: https://www.pmda.go.jp/safety/info-services/drugs/adr-info/suspected-adr/0003.html (accessed on 18 April 2021).
- The International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Hu-man Use (ICH). Medical Dictionary for Regulatory Activities. Available online: http://www.meddra.org/ (accessed on 18 April 2021).
- Watanabe, H.; Matsushita, Y.; Watanabe, A.; Maeda, T.; Nukui, K.; Ogawa, Y.; Sawa, J.; Maeda, H. Early detection of important safety information. Jpn. J. Biomet. 2004, 25, 37–60. [Google Scholar] [CrossRef]
- Ohyama, K.; Sugiura, M. Evaluation of the Association between Topical Prostaglandin F2α Analogs and Asthma Using the JADER Database: Comparison with β-Blockers. Yakugaku Zasshi 2018, 138, 559–564. [Google Scholar] [CrossRef] [Green Version]
- Rothman, K.J.; Lanes, S.; Sacks, S.T. The reporting odds ratio and its advantages over the proportional reporting ratio. Pharmacoepidemiol. Drug Saf. 2004, 13, 519–523. [Google Scholar] [CrossRef] [PubMed]
- van Puijenbroek, E.P.; Bate, A.; Leufkens, H.G.; Lindquist, M.; Orre, R.; Egberts, A.C. A comparison of measures of dispropor-tionality for signal detection in spontaneous reporting systems for adverse drug reactions. Pharmacoepidemiol. Drug Saf. 2002, 11, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.J.; Wang, S.-J.; Tsai, C.-A.; Lin, C.-J. Selection of differentially expressed genes in microarray data analysis. Pharm. J. 2006, 7, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, H.; Uchida, M.; Suzuki, S.; Suga, Y.; Uesawa, Y.; Nakagawa, T.; Takase, H. Analyses of Respiratory Depres-sion Associated with Opioids in Cancer Patients Based on the Japanese Adverse Drug Event Report Database. Biol. Pharm. Bull. 2019, 42, 1185–1191. [Google Scholar] [CrossRef] [Green Version]
- Noguchi, Y.; Tachi, T.; Teramachi, H. Subset Analysis for Screening Drug–Drug Interaction Signal Using Pharmacovigilance Database. Pharmaceutics 2020, 12, 762. [Google Scholar] [CrossRef] [PubMed]
- Sauzet, O.; Carvajal, A.; Escudero, A.; Molokhia, M.; Cornelius, V.R. Illustration of the Weibull Shape Parameter Signal Detec-tion Tool Using Electronic Healthcare Record Data. Drug. Saf. 2013, 36, 995–1006. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Diarrhea | Non-Diarrhea | p-Value | ||
|---|---|---|---|---|---|
| n | (%) | n | (%) | ||
| Sex (Male/Female) * | 534/347 | (60.6/39.4) | 3,674/2,149 | (63.1/36.9) | 0.016 |
| Age ** | 872 | 65.6 ± 0.42 | 5,732 | 64.7 ± 0.16 | 0.076 |
| Drug | Reporting Times | Odds Ratio | (95% CI) |
|---|---|---|---|
| CPT-11 monotherapy | 11,589 | 9.258 | (8.633–9.928) |
| 5-FU monotherapy | 15,118 | 3.211 | (2.918–3.534) |
| Tegafur, Gimeracil, Oteracil Potassium (S-1) monotherapy | 12,697 | 9.511 | (8.900–10.164) |
| CPT-11 plus 5-FU | 1,993 | 6,199 | (5,260–7,306) |
| CPT-11 plus S-1 | 866 | 25,695 | (22,042–29,854) |
| Regimen | Signal for CPT-11 | Signal for S-1 | ||
|---|---|---|---|---|
| N | ROR (95% CI) | N | ROR (95% CI) | |
| patients group using CPT-11 | – | – | 1690 | 2.042 (1.825–2.284) |
| patients group using S-1 | 1690 | 1.989 (1.780–2.222) | – | – |
| Regimen | Signal for CPT-11 | Signal for 5-FU | ||
|---|---|---|---|---|
| N | ROR (95% CI) | N | ROR (95% CI) | |
| patients group using CPT-11 | – | – | 3813 | 0.442 (0.398–0.491) |
| patients group using 5-FU | 3813 | 2.091 (1.858–2.353) | – | – |
| Regimen | n | Time of Onset (Day) | Regimen | n | Time of Onset (Day) | p-Value * | ||
|---|---|---|---|---|---|---|---|---|
| Median | Range | Median | Range | |||||
| CPT-11 plus S-1 | 117 | 14.0 | 1–27 | CPT-11 plus 5-FU | 36 | 8.5 | 1–26 | 0.005 |
| CPT-11 monotherapy | 112 | 8.0 | 1–28 | CPT-11 plus 5-FU | 36 | 8.5 | 1–26 | 0.911 |
| CPT-11 monotherapy | 112 | 8.0 | 1–28 | CPT-11 plus S-1 | 117 | 14.0 | 1–27 | <0.005 |
| 5-FU monotherapy | 91 | 9.0 | 1–28 | S-1 monotherapy | 223 | 14.0 | 1–28 | <0.005 |
| Regimen | n | Shape Parameter: β | |
|---|---|---|---|
| β | 95% CI | ||
| CPT-11 plus 5-FU | 36 | 1.554 | 1.179–1.978 |
| CPT-11 plus S-1 | 117 | 2.208 | 1.891–2.551 |
| CPT-11 monotherapy | 112 | 1.461 | 1.251–1.690 |
| 5-FU monotherapy | 91 | 1.511 | 1.265–1.782 |
| S-1 monotherapy | 223 | 2.075 | 1.855–2.309 |
| Diarrhea | Non-Diarrhea | |
|---|---|---|
| Reports with the suspected medicine | a | c |
| All other reports | b | d |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okunaka, M.; Kano, D.; Matsui, R.; Kawasaki, T.; Uesawa, Y. Evaluation of the Expression Profile of Irinotecan-Induced Diarrhea in Patients with Colorectal Cancer. Pharmaceuticals 2021, 14, 377. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14040377
Okunaka M, Kano D, Matsui R, Kawasaki T, Uesawa Y. Evaluation of the Expression Profile of Irinotecan-Induced Diarrhea in Patients with Colorectal Cancer. Pharmaceuticals. 2021; 14(4):377. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14040377
Chicago/Turabian StyleOkunaka, Mashiro, Daisuke Kano, Reiko Matsui, Toshikatsu Kawasaki, and Yoshihiro Uesawa. 2021. "Evaluation of the Expression Profile of Irinotecan-Induced Diarrhea in Patients with Colorectal Cancer" Pharmaceuticals 14, no. 4: 377. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14040377