
COVID-19 Vaccines: A Review of the Safety and Efficacy of Current Clinical Trials


1
Department of Medicine, Queen Mary Hospital, The University of Hong Kong, Hong Kong 999077, China
2
Department of Ophthalmology, The University of Hong Kong, Hong Kong 999077, China
*
Authors to whom correspondence should be addressed.
†
Co-first authors.
Pharmaceuticals 2021, 14(5), 406; https://0-doi-org.brum.beds.ac.uk/10.3390/ph14050406
Submission received: 25 March 2021
/
Revised: 12 April 2021
/
Accepted: 18 April 2021
/
Published: 25 April 2021
(This article belongs to the Special Issue Current Trends in RNA Virus Vaccines)
Abstract
:Various strategies have been designed to contain the COVID-19 pandemic. Among them, vaccine development is high on the agenda in spite of the unknown duration of the protection time. Various vaccines have been under clinical trials with promising results in different countries. The protective efficacy and the short-term and long-term side effects of the vaccines are of major concern. Therefore, comparing the protective efficacy and risks of vaccination is essential for the global control of COVID-19 through herd immunity. This study reviews the most recent data of 12 vaccines to evaluate their efficacy, safety profile and usage in various populations.

1. Introduction
The COVID-19 pandemic is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Up till February 2021 it had infected more than 110 million patients, causing 2.4 million deaths worldwide, according to data recorded by the World Health Organization (WHO) [1].
The prevention and control of the epidemic in 2020, other than treatment of symptomatic patients, has included monitoring of asymptomatic infections, follow-up and monitoring after cure and discharge, close contact tracking, high-risk population screening, and disinfection of the epidemic source, but the only way for the radical control of COVID-19 infections is by effective vaccination. Vaccines stimulate the body to produce specific antibodies, with anamnestic response when the body is exposed to this pathogen again.
During 2020, there has been extensive research to look into the use of vaccinations to prevent further transmission of SARS-CoV-2. Globally, several prospective vaccines have been produced and used by the public (Table 1). The protective efficacy and immunogenicity profile of each vaccine is also documented (Table 2).
There are currently two forms of messenger ribonucleic acid (mRNA) vaccines: non-replicating mRNA (NRM) vaccines and self-amplifying mRNA (SAM) vaccines. The constructed mRNA is formulated into a carrier—usually lipid nanoparticles—to protect them from degradation and promote cellular uptake [2]. After the carrier particles are ingested into the cell, mRNA is released, which is translated by the ribosome to produce the target protein (recognizable antigen) [3]. After the target protein is secreted by the cell, it is rec-ognized by the immune system and stimulates an immune response.
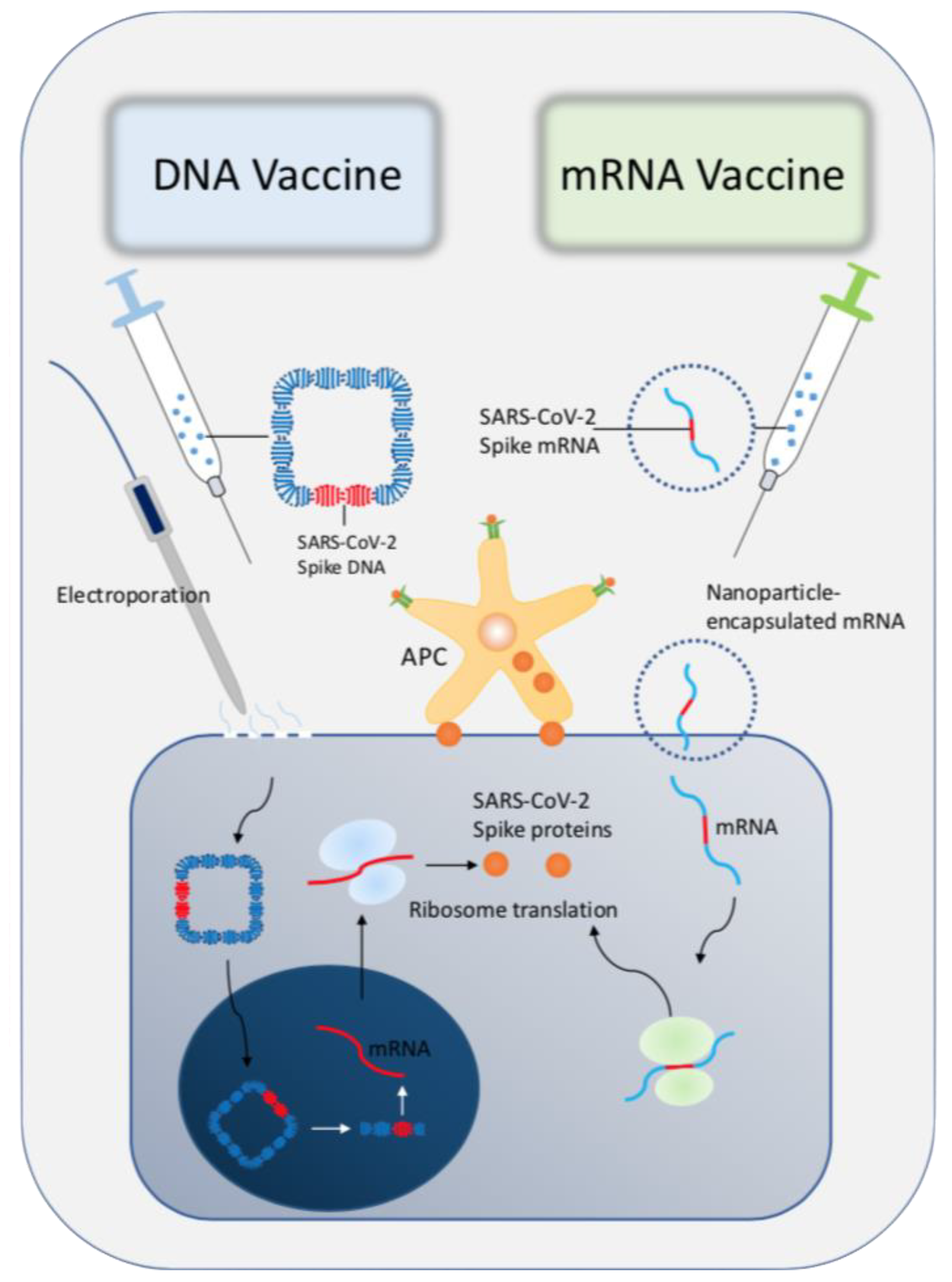
DNA vaccines, also known as nucleic acid vaccines or genetic vaccines, have also been studied. DNA vaccines are eukaryotic expression plasmid DNA (sometimes also RNA) that encode immunogens or immu-nogens4. It can enter animals through a certain route, and be transcribed and translated after being taken up by host cells. The antigen protein can stimulate the body to produce two kinds of non-specific and specific immune responses, thereby playing a role in immune protection [33,34]. The production process of mRNA is not complicated. The difficulty lies in the fact that mRNA is prone to folding and failure in the absence of protection [35]. Therefore, there is the shortcoming of extremely poor stability. It is questionable whether unstable mRNA is safe for the human body [36]. The comparison between DNA and RNA vaccines is shown in Figure 1.
As of 10 April 2021, the top five countries with vaccination programs are the United States (6.129 million), China (4.052 million), the European Union (2.66 million), the United Kingdom (1.82 million) and India (1.084 million) [37]. Although the implementation of vaccination is one of the important factors to achieve global herd immunity, there is no consensus concerning the superiority of one vaccine over the others in terms of protective efficacy and safety profile, even thigh previous reviews have commented on some of the vaccines [38,39].
To date, there are 86 vaccines under development in clinical phase trials. They are developed with different methods such as protein subunits, inactivated virus, DNA-based vaccine, RNA-based vaccine, viral vectors, and live-attenuated viruses. (see Table 3) [40]. However, many of them are currently in preclinical or phase 1 trials, or without publishing on academic journals at the time of writing. The inclusion criteria of this review are: (1) vaccines that has at least finished their phase 2 clinical trials; and (2) the clinical data of the trial has been published in academic journals and accessible on databases (PubMed, Embase, MedLine, Cochrane) at the time of writing. Exclusion criteria includes: (1) vaccines that are on preclinical phases at the time of writing. (2) vaccines that have not gone through at least phase 2 trials 3) vaccines that have phase 2 trials but have not published their data in academic journals nor accessible on databases (PubMed, Embase, Medline, Cochrane).
This study reviews 12 vaccines in production to evaluate their protective efficacy, safety profile and usage in high risk populations such as children, elderly and patients with co-morbidities.
2. BiONTech (BNT162b1 and BNT162b2)
The BiONTech trials focus on two candidates: BNT162b1 and BNT162b2. Both vaccines are lipid-based, nucleoside-modified mRNA vaccines that encode the trimerized receptor-binder (RBD) of the spike glycoprotein SARS-CoV-2. The RBD-IgG concentrations and SARS-CoV-2 neutralizing titres were measured after complete course of the vaccines. In the trial of BNT162b112, serum IgG geometric mean concentra-tion (GMC) of the recipient after first dose was comparable to the convalescent sera of COVID-19 patient. The trial showed a strong, dose-dependent vaccine-induced antibody response: the GMC of vaccine recipients is 8 times and 42 times the convalescent sera in the 10 μg and 30 μg group, respectively. A further increase to 100 μg showed no additional elevation of RBD IgG concentration, compared with 10 μg and 30 μg trials [4,5].
BNT162b1 induced functional CD4+ and CD8+ T cell responses in almost all recipients: 95.2% participants mounted RBD-specific CD4+ T cell responses. There is a positive correlation between RBD-binding IgG and SARS-CoV-2 neutralizing antibody titres [6]. Severe adverse events, such as grade 3 decrease of lymphocyte count and grade 2 neutropenia, were manageable. No clinical deteriorations were observed.
The overall serological responses of BNT162b2 and BNT162b1 were similar [7]: Phase 2/3 trial showed they conferred 94.6% (95% CI 89.7–97.3) protection against COVID-19 in persons older than 16 years of age [8]. Double dose vaccination further boosts the immune response in both younger and older adults, while the response was weaker in participants 65 to 85 years old. Exploration of dose elevations of vaccinations in the elderly should be conducted in future research.
Serious adverse events such as death from arteriosclerosis and cardiac arrest, paroxysmal ventricular arrhythmia were recorded. However, cardiovascular events occurred similarly in the placebo group, with two deaths due to haemorrhagic stroke and myocardial infarction, and two with unknown causes. It is uncertain whether the vaccine increases cardiovascular risk.
COVID-19 infections is associated with a higher inflammatory burden that can induce vascular inflammation, myocarditis and cardiac arrhythmias [17]. Vaccinations for other acute respiratory virus infection show the possibility of a transient increase in the risk of vascular events [18]. Some studies showed a 10-fold increase of acute myocardial infarction admission within the seven days for of testing positive for influenza B, and a 5-fold increase of risk with influenza A [41,42,43]. Another study suggests that binding of SARS-CoV-2 to ACE2 can cause acute myocardial and lung injury through the alteration in ACE2 signaling pathways [44]. The effect of vaccinations for patients with pre-existing cardiovascular diseases have to be further elucidated.
3. Moderna (mRNA1273)
mRNA1273 is manufactured by Moderna. It encodes stabilized prefusion S-2P antigen, consisting of the SARS-CoV-2 glycoprotein with a transmembrane anchor and an intact S1-S2 cleavage site [9]. A preliminary report showed the binding antibody IgG GMT to S-2P increased after vaccinations, with 100% serocon-version rates by day 15. Dose-response relationship was observed with higher dosage eliciting stronger IgG GMT. Both low dose (25 μg) and medium dose (100 μg) elicited CD4+ T cell responses by expression of Th1 cytokines.
The phase 1 clinical trial showed a dose-response relationship [45]. It also elicited a strong CD4+ cytokine response involving Th1 helper T cells. The higher dosage (100 μg) was chosen for phase 3 clinical trials. Robust neutralizing activity to the 614G variant was observed for the 100 μg dose, regardless of the patients’ age.
The phase 3 clinical trial showed 94.1% (95% CI 89.3–96.8; p < 0.001) protective efficacy in preventing COVID-19 illness [10]. The vaccine efficacy to prevent COVID-19 was consistent across subgroups stratified by age (18 to <65 years of age and ≥65 years), presence of risk for severe COVID-19, sex, and race and ethnic groups. The frequency of grade 3 adverse events in the placebo group (1.3%) was similar to that in the vaccine group (1.5%).
4. ChadOx1 nCoV-19 (AZD1222)
ChadOx1 nCoV-19 consists of replication-deficient simian adenovirus vector ChAdOx1, containing the full-length structural surface glycoprotein of SARS-CoV-2, with a tissue plasminogen activator leader sequence [12]. It expresses a codon-optimised coding sequence for the spike protein. Upon vaccination, antibodies against SARS-CoV-2 spike protein peaked by day 28 and remained elevated up to day 56 in participants receiving 1 dose. The median titre of the booster-dose group was more than five times higher than the single-dose group. Paracetamol was used to reduce local regional side effects such as fever and myalgia. Prophylactic paracetamol was prescribed in certain participants, but serological response was independent of prophylactic paracetamol prescription.
ChAdOx1 nCoV-19 appears to be better tolerated in older adults than in younger adults, and it provides similar immunogenicity across all age groups after a booster dose [13]. Serological response was independent of dosage and age after booster, with the IgG level being consistently higher than those without booster vaccinations. Median IgG titres peaked by day 42 in most groups who received two-dose vaccinations. A higher vaccine efficacy was observed when the participants first received a low-dose followed by a stand-ard-dose (90%, 95% CI 67.4–97.0, p = 0.01), compared with two standard-dose recipients (62.1%, 95% CI 41.0–75.7) [24].
In terms of safety profile, 13 serious adverse events occurred but none was considered related to either study vaccine as assessed by the investigators [13]. There was a reported case of hemolytic anemia and three cases of transverse myelitis. The independent neurological committee considered two of them were unlikely to be related to vaccination, and one of them was an idiopathic, short segment spinal cord demyelination [14].
Phase 3 trials are being performed in the United Kingdom, Brazil and the United States of America to assess the protective efficacy and safety [13].
Various thromboembolic events were reported after participants have received ChadOx1 nCoV-19 (AZD122) vaccinations. One of the reasons may be related to post-vaccination immune-mediated thrombo-cytopenia [46]. In a report including 28 patients after receiving AZD122 with thromboembolic events, all of them were tested positive for anti-platelet factor 4(PF4)-heparin antibodies, which clinically mimics auto-immune heparin-induced thrombocytopenia [47]. This was similarly observed in another study where five participants with thromboembolic events (100%) tested positive with high level of IgG anti-PF4-polyanion complexes, measured by enzyme linked immunoassay (ELISA) [48]. The adverse reaction may be related to the adenovirus-platelet-leukocyte complexes formed after vaccination, which are taken up by the liver by interaction [28] with membrane-associated heparan sulphate proteoglycan (MAHSP) [49,50]. MAHSP acts as a receptor for viral entry. Heparin can lead to dose-dependent inhibition of this reaction, leading to induction of anti-PF4/heparin antibodies [51]. Subsequently, heparin-induced thrombocytopenia and thrombophilia was observed in patients after receiving AZD122 vaccination.
5. Convidecia (Adenovirus Type-5 Vectored COVID-19 Vaccine)
Adenovirus type-5 (AD-5) vectored COVID-19 vaccine is a replication of defective Ad5-vectored vaccine expressing the spike glycoprotein SARS-CoV-2 [15]. It clones an optimized full-length spike gene based on Wuhan-Hu-1 with the tissue plasminogen activator signal peptide gene into an E1 and E3 deleted Ad-5 vector, and constructed the Ad-5 vectored COVID-19 vaccines using the Admax system. The vaccine demonstrated a dose-response relationship at day 28 after vaccination: the T-cell responses in the high dose group were significantly higher than that in the low-dose group (p < 0.0010), but not significant compared with that in the middle group. TNF-α expression from CD4+ T cells was significantly lower in the low dose group than in the high dose (p < 0.0001) and middle dose groups (p = 0.0032). TNF-α expression from CD8+ T cells was higher in the high-dose group than that in both the middle dose group (p = 0.016) and the low-dose group (p < 0.0001).
The phase two trial showed a higher dosage correlates with a higher seroconversion rate and higher GMTs of neutralizing antibody responses to pseudovirus [16]. The seroconversion rate in high-dose group was 59% (95% CI 52–65) and 47% (95% CI 39–56). The GMT were 61.4 (95% CI 53.0–71.0) in the high-dose group and 55.3 (95% CI 45.3–67.5) in the low dose group. Stratified analysis based on age showed older adults (>55 years) were associated with lower antibody responses in both dose groups post-vaccinations. A total of 25 grade 3 or above adverse events were documented, but they were self-limiting and resolved within 3 to 4 days without medications.
Phase 3 trial are being performed globally, with 40,000 participants. It is expected to be completed by January 2022 [17].
6. Gam-COVID-Vac (Recombinant Adenovirus Type 26 and Recombinant Adenovirus Type 5 Vaccine)
rAd26-S and rAD5-S are vaccines made by Russian manufacturer which carry the gene for SARS-CoV-2 full-length glycoprotein S. Phase 1/2 studies showed both rAd26-S and rAD5-S formulations were safe and well tolerated [18]. Patients receiving combined rAD26-S and rAD5-S were associated with a higher se-roconversion rate (100%) and neutralising antibody GMT (49.25) on day 28 [19]. Combined regimen was better than individual rAD26-S or rAD5-S injection. Increased CD4+ T cells, CD8+ T cells and IFN- γ secre-tion were observed in all vaccine recipients. No serious adverse events were reported.
The phase 3 study showed a protective efficacy of 91.6% (95% CI 85.6–95.2) against COVID-19 [19]. Immunogenicity was significantly higher in the vaccination arm: The RBD-specific IgG was detected in 98% participant samples, with a GMT of 8996 (95% CI 7610–10,635) and a seroconversion rate of 98.25%. Conversely, the RBD-specific IgG was detected in 15% participant samples with a GMT of 30.55 (95% CI 20.18–46.26) and a seroconversion rate of 14.91% (p < 0.0001 vs. the vaccination arm). Neutralising antibody follows a similar trend too: with GMT of 44.5 (95% CI 31.8–62.2) and seroconversion rate of 95.83% in the vaccination arm; compared with GMT of 1.6 (95% CI 1.12–2.19) and 7.14% seroconversion rate.
7. Covovax (NVAX-CoV2373)
NVAX-CoV2373 is a recombinant SARS-CoV-2 nanoparticle vaccine composed of trimeric full-length sARS-CoV-2 spike glycoproteins and Matrix-M1 adjuvant. The phase 1 study showed two-dose 5 μg regimen with adjuvant induced IgG GMT and neutralization responses that exceeded convalescent serum from most symptomatic COVID-19 patients [20]. The immunological outcomes in 5 μg and 25 μg vaccination groups were comparable. Second vaccinations with adjuvant resulted in GMT level four times greater than the convalescent plasma in symptomatic patients. Adjuvant regimens induced polyfunctional CD4+ T-cell responses that were reflected in IFN-γ, TNF-α and IL-2 production on spike protein stimulation. No serious adverse events were reported. Interim analysis showed the vaccine achieved protective efficacy of 86% against UK variant and 60% against South Africa variant [21]. The phase 3 trial showed a protective efficacy of 89.3% (95% CI 75.2–95.4) against B.1.1.7 UK variant, but only 49.4% (95% CI 6.1–72.8) against B.1.351 variant [22].
8. WIV04-Strain Inactivated SARS-CoV-2 Vaccine
The WIV-04 strain inactivated SARS-CoV-2 vaccine is designed by the Wuhan Institute of Biological Products Co Ltd. The WIV-04 strain was isolated and cultivated in a Verco cell line for propagation, and the supernatant of the infected cells was inactivated by β-propiolactone. Interim analysis of two randomised controlled trials showed a seroconversion rate of 100% in phase 1 trial and 85.7% in the phase 2 trial [10]. A lower-dosage injection was associated with a higher GMT of neutralizing antibody at day 14 after the third injection, compared with other dosage groups. Injection schedule on day 0 and 21 confer a higher GMT, compared with the schedule of day 0 and 14. Most patients started to generate antibody response after the second injection, and remained at high level 14 days after the third injection. The most common adverse reactions were injection site pain and fever, which were mild and self-limiting. The phase 3 study data was not available at the time of writing.
9. BBIBP-CorV
BBIBP-CorV is developed by the Beijing Institute of Biological Products. It is an inactivated vaccine developed from the strain 19nCoV-CDC-Tan-HB02 (HB02) [11]. The HB02 strain was purified and passaged in Vero cell lines to generate vaccine production by using a novel carrier in a basket reactor. In the phase 1 trial, a higher dosage (8 μg) was associated with a higher seroconversion rate by day 14, while seroconversion rates reached 100% in all three dosage cohorts on day 28. By day 28, the neutralizing antibody GMT was significantly higher in the high-dose group than the low-dose group (2 μg), with no significant difference between medium-dose (4 μg) and high-dose. Younger adults were associated with higher neutralizing anti-body GMT, compared with older adults (>60 years).
The phase 2 trial showed the immunization schedule of 4 μg on day 0 and 21 was associated with the highest neutralizing antibody GMT (282.7, 95% CI 221.2–361.4), compared with other immunization schedules. One grade 3 or above adverse event was documented due to self-limiting grade 3 fever (>38.5 °C).
A phase 3 study is currently underway in Abu Dhabi with 15,000 participants: 5000 participants receiving placebo, another 5000 receiving BBIBP-CorV, and the remaining 5000 receiving another inactivated vaccine manufacturer by Sinopharm [23].
10. Coronavac Vaccine
Coronavac is developed by Sinovac Life Sciences (Beijing China) as an inactivated vaccine created from Vero cells that have been inoculated with SARS-CoV-2 (CN02 strain) [24]. The phase 1 trial showed seroconversion rates of 88% and 100% and 8% in the 3 μg, 6 μg and placebo groups on day 28, respectively. The neutralising antibody GMT were 465.8 (95% CI 288.1–753.1), 1395.9 (95% CI, 955.2–2039.7) and 89.8 (95%CI 76.1–105.9) in the three groups, respectively. Higher dosage was associated with a better immunogenicity.
The phase 2 immunization schedule trial showed receiving vaccination on day 0 and 14 resulted in the most promising outcomes: seroconversion rates were 97%, 100% and 0% in the 3 μg, 6 μg and placebo groups on day 28, respectively. The neutralising antibody GMT were 44.1 (95% CI 37.2–52.2), 65.4 (95% CI 56.4–75.9) and 2.0 (95% CI 2.0–2.1) in the three groups, respectively. One case of serious adverse events related to acute hypersensitivity with presentation of urticaria 48 h after the first dose. It was managed with chlorphenamine and dexamethasone, and recovered within 3 days.
The phase 3 study data has not been published in medical journals. An online search of the phase 3 study in Brazil showed a 50.4% protective efficacy in preventing symptomatic infections, 78% protective efficacy in preventing mild cases requiring treatment and 100% prevention of severe cases [52]. Phase 3 studies in Turkey and Indonesia showed a protective efficacy of 83.5% and 65.3%, respectively [53,54].
11. Ad26.COV2.S
Ad26.COV2.S is developed by Johnson & Johnson. It is a recombinant, replication-incompetent adenovirus serotype 26 (Ad26) vector encoding a full-length and stabilized SARS-CoV-2 spike protein. Early animal studies showed promising efficacy with low-dose single-shot vaccination [25,26]. In the phase 1 clinical trial, binding and neutralizing antibodies were detected in 100% of vaccine recipients by 57 days after single vaccinations [27]. The geometric mean titres (GMT) of spike-specific binding antibodies and neutralizing antibodies ranged from 2432–5729 and 242–449, respectively. A booster immunization on day 57 increased binding antibody titres and neutralizing antibody titres by a mean of 2.56-fold (range 1.58–3.04) and 4.62-fold (range: 3.56–5.68), respectively. An interim study showed the titres remain stable until at least day 71 [28]. Strong immune responses were recorded as CD4+ T cells were detected in 76 to 83% of the young patients (aged 18–55 years), and 60 to 67% in older patients (aged greater than 65). Phase 3 data showed a 66.9% (95% CI 59.0–73.4) protective efficacy across all participant age groups, and 76.3% (95% CI, 61.6–86.0) in participants older than 60 years old [29]. In preventing severe or critical COVID-19, Ad26.COV2.S was associated with 76.7% efficacy at 14 days, and 85.4% at 28 days. Adverse reactions were recorded such as thromboembolic events (15 in vaccination arm and 10 in placebo arm) and tinnitus (6 vs. 0).
Subgroup analysis based on region showed a higher vaccine efficacy in N. America, compared with South Africa and Latin America. The protective efficacies were 74.4% (95% CI 65.0–81.6) at 14 days and 72.0% (95% CI 58.2–81.7) at 28 days; compared with 52.0% (95% CI 30.3–67.4) at day 14 and 64% (95% CI 41.2–87.7) in South Africa. The protective efficacies in Latin America were 64.7% (95% CI 54.1–73.0) and 61.0% (95% CI 46.9–71.8), respectively. This may be related to the difference in the prevalence of mutant strain of SARS-CoV-2 in different regions.
12. Covaxin (BBV 152)
BBV 152 is a whole-viron inactivated SARS-CoV-2 vaccine formulated with a toll-like receptor 7/8 agonist molecule (IMDG) adsorbed to alum (Algel) [30]. It is developed by Bharat Biotech from an isolated NIV-2020-770 strain of a patient with COVID-19 sequenced in India. Previous animal studies showed acceptable safety profiles, humoral and cell-mediated responses [31]. Phase 2 trials showed a good reactogenicity, safety profile, and enhanced humoral and cell-mediated immune responses when participants received a higher dose (6 μg) of Algel-IMDG formulation [32]. In the phase 2 trial, the GMT at day 56 was significantly higher in the 6 μg group (197.0, 95% CI 155.6–249.4) compared with the 3 μg group (100.9, 95% CI 74.7–137.4, p = 0.0041). Seroconversion rates were 92.9% (95% CI 88.2–96.2) in the 3 μg group, and 98.3% (95% CI 95.1–99.6) in the 6 μg group. The Algel-IMDG formulation elicited T-cell responses biased to a Th1 phenotype at day 42, with no significant difference in causing local or systemic adverse reactions between the 3 μg and the 6 μg groups. No serious adverse events were reported in the study. Protective efficacy was not reported.
13. Challenges
In view of the surging infections and promising efficacy in clinical trials of vaccines (Table 2), many countries have advocated vaccination programs for their citizens. However, questions have been raised concerning the efficacy against new variant strains. Experience in Manaus (Brazil) showed secondary immunity alone was not sufficient to arrest transmission [55], possibly due to new variant strains. The B.1.1.7 of the UK and South African 501Y.V2 variants are shown to cause alterations to the spike protein, which may affect immune recognition of antibodies derived from existing vaccines [56]. Further clinical trials are required to test for the efficacy of existing vaccines against mutant variants.
Another problem is the duration of the protective efficacy. It is likely that at least yearly boosters are necessary. Seasonal modification to annual vaccines to arrest the transmission of previous strains may also be considered. It is also doubtful whether circulating neutralizing antibody is protective against COVID-19 infection as animal studies showed robust viral infective activities in nasal turbinate. Reinfection is still potentially possible [57].
Also with the expansion of the vaccination programs in the general population, the relationship of certain side effects, such as the thrombotic events occurring after receiving ChadOx1 nCoV-19, with the vaccines has to be further determined.
The pathological correlation between incidence of cardiovascular adverse events and vaccination with in-activated or live-attenuated virus has to be elucidated. SARS-CoV-2 infection is associated with systemic inflammatory response causing cytokine releases and cytokine storm, resulting in vasculopathy and its complications [58]. Likewise, influenzae carries similar pathogenesis as SARS-CoV-2. However, the experience of influenzae vaccinations (inactivated virus) shows that vaccinations reduced major cardiovascular events significantly, and has become part of the routine care of patients with chronic cardiovascular conditions [59]. COVID-19 vaccinations do not follow the typical trend of influenzae. In general, attenuated patho-gens have the very rare potential to revert to its pathogenic form [60]. Further studies is required to determine whether vaccines with inactivated SARS-CoV-2 can reduce or induce cardiovascular events.
Diabetic patients are associated with a higher risk of inflammatory response and coagulopathy during an infection episode [61]. Close monitoring of inflammatory markers, tight glycemic controls and lifestyle modifications are recommended for diabetic COVID-19 care [62]. Acute complications after vaccinations can be monitored by measurement of prognostic inflammatory markers, such as serum ferritin, lactate dehydrogenase, C-reactive protein (CRP), erythrocyte sedimentation rate, D-dimer level, cardiac troponin and N-terminal pro-brain-type natriuretic peptide (NT-proBNP) [63,64,65,66]. These markers have close associations with the prognosis of COVID-19 infections. However, the interval and duration of monitoring has to be further studied. The relation between thrombotic events and vaccine using as adenovirus vector has been discussed in a previous section.
14. Conclusions
The COVID-19 vaccines in clinical trials have all shown promising immunogenicity with varying degree of protective efficacy, and an acceptable safety profile. A second dose immunization gives more robust immune response in all vaccines. The immunological outcome in the elderly is poorer than in the younger recipients. Further exploration on immunization schedule is required, such as more frequent vaccinations or higher dosage in each injection. Grade 3 or above side effects are not common in the clinical trials to date.
Author Contributions
Literature search, study designs, figures, data collections, data analysis, data interpretation and manuscript writing were done by Z.-P.Y., M.Y. and C.-L.L., Z.-P.Y. and M.Y. contributed equally to this work. All authors have read and agreed to the published version of the manuscript.
Funding
The authors did not receive funding for this project.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data generated during and/or analysed during the current study are available on electronic databases (PubMed, Embase, Medline, Google Scholar, Cochrane). All data generated or analysed during this study are included in this published article.
Conflicts of Interest
The authors Zhipeng Yan, Ming Yang and Ching-Lung Lai declare there is no conflict of interest.
References
- World Health Organization. Weekly Epidemiology Update 23 February 2021. WHO Situation Report. 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update---23-february-2021 (accessed on 25 March 2021).
- Bonam, S.R.; Kotla, N.G.; Bohara, R.A.; Rochev, Y.; Webster, T.J.; Bayry, J. Potential immuno-nanomedicine strategies to fight COVID-19 like pulmonary infections. Nano Today 2021, 36, 101051. [Google Scholar] [CrossRef] [PubMed]
- Pardi, N.; Hogan, M.J.; Weissman, D. Recent advances in mRNA vaccine technology. Curr. Opin. Immunol. 2020, 65, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Mulligan, M.J.; Lyke, K.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Raabe, V.; Bailey, R.; Swanson, K.A.; et al. Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults. Nature 2020, 586, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Sahin, U.; Muik, A.; Derhovanessian, E.; Vogler, I.; Kranz, L.M.; Vormehr, M.; Baum, A.; Pascal, K.; Quandt, J.; Maurus, D.; et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T-cell responses. Nature 2020, 586, 594–599. [Google Scholar] [CrossRef]
- Sette, A.; Moutaftsi, M.; Moyron-Quiroz, J.; McCausland, M.M.; Davies, D.H.; Johnston, R.J.; Peters, B.; Benhnia, M.R.-E.-I.; Hoffmann, J.; Su, H.-P.; et al. Selective CD4+ T Cell Help for Antibody Responses to a Large Viral Pathogen: Deterministic Linkage of Specificities. Immunnology 2008, 28, 847–858. [Google Scholar] [CrossRef] [Green Version]
- Walsh, E.E.; Frenck, R.W.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based Covid-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Jackson, L.A.; Anderson, E.J.; Rouphael, N.G. An mRNA Vaccine against SARS-CoV-2-Preliminary Report. N. Engl. J. Med. 2020, 383, 1920–1931. [Google Scholar] [CrossRef]
- Xia, S.; Duan, K.; Zhang, Y. Effect of an Inactivated Vaccine Against SARS-CoV-2 on Safety and Immuno-genicity Outcomes: Interim Analysis of 2 Randomized Clinical Trials. JAMA 2020, 324, 951–960. [Google Scholar] [CrossRef] [PubMed]
- Xia, S.; Zhang, Y.; Wang, Y. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: A randomised, double-blind, placebo-controlled, phase 1/2 trial. Lancet Infect. Dis. 2021, 21, 39–51. [Google Scholar] [CrossRef]
- Folegatti, P.M.; Ewer, K.J.; Aley, P.K. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: A preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet 2020, 396, 467–478. [Google Scholar] [CrossRef]
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J.; Flaxman, A.L.; Folegatti, P.M.; Owens, D.R.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G.; et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomised, controlled, phase 2/3 trial. Lancet 2020, 396, 1979–1993. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Zhu, F.C.; Li, Y.H.; Guan, X.H. Safety, tolerability, and immunogenicity of a recombinant adenovi-rus type-5 vectored COVID-19 vaccine: A dose-escalation, open-label, non-randomised, first-in-human trial. Lancet 2020, 395, 1845–1854. [Google Scholar] [CrossRef]
- Zhu, F.-C.; Guan, X.-H.; Li, Y.-H.; Huang, J.-Y.; Jiang, T.; Hou, L.-H.; Li, J.-X.; Yang, B.-F.; Wang, L.; Wang, W.-J.; et al. Immunogenicity and safety of a recombinant adenovirus type-5-vectored COVID-19 vaccine in healthy adults aged 18 years or older: A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet 2020, 396, 479–488. [Google Scholar] [CrossRef]
- ClinicalTrials.Gov. Phase III Trial of A COVID-19 Vaccine of Adenovirus Vector in Adults 18 Years Old and Above. Available online: https://clinicaltrials.gov/ct2/show/NCT04526990 (accessed on 18 March 2021).
- Logunov, D.Y.; Dolzhikova, I.V.; Zubkova, O.V. Safety and immunogenicity of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine in two formulations: Two open, non-randomised phase 1/2 studies from Russia. Lancet 2020, 396, 887–897. [Google Scholar] [CrossRef]
- Logunov, D.Y.; Dolzhikova, I.V.; Shcheblyakov, D.V. Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: An interim analysis of a randomised con-trolled phase 3 trial in Russia. Lancet 2021, 397, 671–681. [Google Scholar] [CrossRef]
- Keech, C.; Albert, G.; Cho, I. Phase 1-2 Trial of a SARS-CoV-2 Recombinant Spike Protein Nano-particle Vaccine. N. Engl. J. Med. 2020, 383, 2320–2332. [Google Scholar] [CrossRef]
- Mahase, E. Covid-19: Novavax vaccine efficacy is 86% against UK variant and 60% against South African variant. BMJ 2021, 372, n296. [Google Scholar] [CrossRef]
- Taylor, N.P. Novavax COVID-19 vaccine 90% efficacious in phase 3, but protection plummets against one variant. 2021. Available online: https://www.fiercebiotech.com/biotech/novavax-covid-19-vaccine-90-efficacious-phase-3-but-protection-plummets-against-one-variant (accessed on 9 April 2021).
- Chakraborty, S.; Mallajosyula, V.; Tato, C.M.; Tan, G.S.; Wang, T.T. SARS-CoV-2 vaccines in advanced clinical trials: Where do we stand? Adv. Drug Deliv. Rev. 2021, 172, 314–338. [Google Scholar] [CrossRef]
- Zhang, Y.; Zeng, G.; Pan, H. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18–59 years: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 181–192. [Google Scholar] [CrossRef]
- Anadolu Agency. Decision Based on Results of Country’s Phase III Trials That Put Estimated Vaccine Efficacy at 65.3%, Says Official. Available online: https://www.astrazeneca.com/media-centre/press-releases/2021/azd1222-us-phase-iii-primary-analysis-confirms-safety-and-efficacy.html (accessed on 18 March 2021).
- Mercado, N.B.; Zahn, R.; Wegmann, F. Single-shot Ad26 vaccine protects against SARS-CoV-2 in rhesus macaques. Nature 2020, 586, 583–588. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Chandrashekar, A.; Zahn, R.; Wegmann, F.; Yu, J.; Mercado, N.B.; McMahan, K.; Martinot, A.J.; Piedra-Mora, C.; Beecy, S.; et al. Low-Dose Ad26.COV2.S Protection Against SARS-CoV-2 Challenge in Rhesus Macaques. bioRxiv 2021. [Google Scholar] [CrossRef]
- Stephenson, K.E.; Le Gars, M.; Sadoff, J.; de Groot, A.M.; Heerwegh, D.; Truyers, C.; Atyeo, C.; Loos, C.; Chandrashekar, A.; McMahan, K.; et al. Immunogenicity of the Ad26.COV2.S Vaccine for COVID-19. JAMA 2021. [Google Scholar] [CrossRef]
- Sadoff, J.; Le Gars, M.; Shukarev, G.; Heerwegh, D.; Truyers, C.; De Groot, A.M.; Stoop, J.; Tete, S.; Van Damme, W.; Leroux-Roels, I.; et al. Interim Results of a Phase 1–2a Trial of Ad26.COV2.S Covid-19 Vaccine. New Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Yadav, P.D.; Ella, R.; Kumar, S.; Patil, D.R.; Mohandas, S.; Shete, A.M.; Vadrevu, K.M.; Bhati, G.; Sapkal, G.; Kaushal, H.; et al. Immunogenicity and protective efficacy of inactivated SARS-CoV-2 vaccine candidate, BBV152 in rhesus macaques. Nat. Commun. 2021, 12, 1–11. [Google Scholar] [CrossRef]
- Ella, R.; Vadrevu, K.M.; Jogdand, H.; Prasad, S.; Reddy, S.; Sarangi, V.; Ganneru, B.; Sapkal, G.; Yadav, P.; Abraham, P.; et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBV152: A double-blind, randomised, phase 1 trial. Lancet Infect. Dis. 2021, 21, 637–646. [Google Scholar] [CrossRef]
- Ella, R.; Vadrevu, K.M.; Jogdand, H.; Prasad, S.; Reddy, S.; Sarangi, V.; Ganneru, B.; Sapkal, G.; Yadav, P.; Abraham, P.; et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBV152: Interim results from a double-blind, random-ised, multicentre, phase 2 trial, and 3-month follow-up of a double-blind, randomised phase 1 trial. Lancet Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Porter, K.R.; Raviprakash, K. DNA Vaccine Delivery and Improved Immunogenicity. Curr. Issues Mol. Biol. 2017, 22, 129–138. [Google Scholar] [CrossRef]
- Li, L.; Petrovsky, N. Molecular mechanisms for enhanced DNA vaccine immunogenicity. Expert Rev. Vaccines 2016, 15, 313–329. [Google Scholar] [CrossRef] [Green Version]
- Suschak, J.J.; Williams, J.A.; Schmaljohn, C.S. Advancements in DNA vaccine vectors, non-mechanical delivery methods, and molecular adjuvants to increase immunogenicity. Hum. Vaccines Immunother. 2017, 13, 2837–2848. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.A. A Comparison of Plasmid DNA and mRNA as Vaccine Technologies. Vaccines 2019, 7, 37. [Google Scholar] [CrossRef] [Green Version]
- Ritchie, H.; Beltekian, D.; Mathieu, E.; Hasell, J.; Macdonald, B.; Giattino, C.; Appel, C.; Roser, M.; Yunits, B.; van Woerden, E.; et al. Statistics and Research: Coronavirus (COVID-19) Vaccinations. 2021. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 22 March 2021).
- Liu, X.; Liu, C.; Liu, G.; Luo, W.; Xia, N. COVID-19: Progress in diagnostics, therapy and vaccination. Theranostics 2020, 10, 7821–7835. [Google Scholar] [CrossRef] [PubMed]
- Karpinski, T.M.; Ozarowski, M.; Seremak-Mrozikiewicz, A.; Wolski, H.; Wlodkowic, D. The 2020 race to-wards SARS-CoV-2 specific vaccines. Theranostics 2021, 11, 1690–1702. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Solidarity Vaccines Trial Expert Group. Draft Landscape and Tracker of COVID-19 Candidate Vaccines; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Madjid, M.; Safavi-Naeini, P.; Solomon, S.D.; Vardeny, O. Potential Effects of Coronaviruses on the Cardiovascular System: A Review. JAMA Cardiol. 2020, 5, 831–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smeeth, L.; Thomas, S.L.; Hall, A.J.; Hubbard, R.; Farrington, P.; Vallance, P. Risk of Myocardial Infarction and Stroke after Acute Infection or Vaccination. New Engl. J. Med. 2004, 351, 2611–2618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwong, J.C.; Schwartz, K.L.; Campitelli, M.A. Acute Myocardial Infarction after Laboratory-Confirmed Influenza Infection. N. Engl. J. Med. 2018, 378, 345–353. [Google Scholar] [CrossRef]
- Soumya, R.S.; Unni, T.G.; Raghu, K.G. Impact of COVID-19 on the Cardiovascular System: A Review of Available Reports. Cardiovasc. Drugs Ther. 2020, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.J.; Rouphael, N.G.; Widge, A.T. Safety and Immunogenicity of SARS-CoV-2 mRNA-1273 Vaccine in Older Adults. N. Engl. J. Med. 2020, 383, 2427–2438. [Google Scholar] [CrossRef] [PubMed]
- Andreas Greinacher, T.T.; Theodore, E.; Warkentin, K.W.; Kyrle, P.; Eichinger., S. A Prothrombotic Thrombocytopenic Disorder Resembling Heparin-Induced Thrombocytopenia Following Coronavirus-19 Vaccination. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Schultz, N.H.; Sørvoll, I.H.; Michelsen, A.E.; Munthe, L.A.; Lund-Johansen, F.; Ahlen, M.T.; Wiedmann, M.; Aamodt, A.-E.; Skattør, T.H.; Tjønnfjord, G.E.; et al. Thrombosis and Thrombocytopenia after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Shayakhmetov, D.M.; Gaggar, A.; Ni, S.; Li, Z.-Y.; Lieber, A. Adenovirus Binding to Blood Factors Results in Liver Cell Infection and Hepatotoxicity. J. Virol. 2005, 79, 7478–7491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, A.H.; Mcvey, J.H.; Waddington, S.N.; Di Paolo, N.C.; Shayakhmetov, D.M. The Influence of Blood on In Vivo Adenovirus Bio-distribution and Transduction. Mol. Ther. 2007, 15, 1410–1416. [Google Scholar] [CrossRef] [PubMed]
- Summerford, C.; Samulski, R.J. Membrane-Associated Heparan Sulfate Proteoglycan Is a Receptor for Adeno-Associated Virus Type 2 Virions. J. Virol. 1998, 72, 1438–1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- News Reuters. UPDATE 2-China’s Sinovac Defends COVID-19 Vaccine after Disappointing Brazil Data. Available online: https://www.reuters.com/article/health-coronavirus-malaysia-idCNL1N2JO0O9 (accessed on 18 March 2021).
- Tavsan, S. Sinovac’s COVID-19 Shot is 83% Effective, Not 91%, Turkey Says. Nikkei Asia. Available online: https://asia.nikkei.com/Spotlight/Coronavirus/COVID-vaccines/Sinovac-s-COVID-19-shot-is-83-effective-not-91-Turkey-says (accessed on 9 April 2021).
- Nupus, H. Indonesia Approves China’s CoronaVac for Emergency Use. 2020. Available online: https://www.aa.com.tr/en/asia-pacific/indonesia-approves-china-s-coronavac-for-emergency-use/2105881 (accessed on 9 April 2021).
- U.S. Food and Drug Administration. FDA Briefing Document. In Proceedings of the Vaccines and Related Biological Products Advisory Committee Meeting, 11 December 2020; Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3747047 (accessed on 25 March 2021).
- Janssen Ad26.COV2.S. In Proceedings of the Vaccine for the Prevention of COVID-19. 26 February 2021. Available online: https://www.fda.gov/advisory-committees/advisory-committee-calendar/vaccines-and-related-biological-products-advisory-committee-february-26-2021-meeting-announcement (accessed on 25 March 2021).
- Buss, L.F.; Prete, C.A.; Abrahim, C.M.M. Three-quarters attack rate of SARS-CoV-2 in the Brazilian Amazon during a largely unmitigated epidemic. Science 2021, 371, 288–292. [Google Scholar] [CrossRef]
- Callaway, E. Could new COVID variants undermine vaccines? Labs scramble to find out. Nat. Cell Biol. 2021, 589, 177–178. [Google Scholar] [CrossRef]
- Zhou, D.; Chan, J.F.; Zhou, B. Robust SARS-CoV-2 infection in nasal turbinates after treatment with systemic neutralizing antibodies. Cell Host Microbe. 2021, 29, 551–563. [Google Scholar] [CrossRef]
- Clerkin, K.J.; Fried, J.A.; Raikhelkar, J.; Sayer, G.; Griffin, J.M.; Masoumi, A.; Jain, S.S.; Burkhoff, D.; Kumaraiah, D.; Rabbani, L.; et al. COVID-19 and Cardiovascular Disease. Circulation 2020, 141, 1648–1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, J.S.Y.; Tambyah, P.A.; Sia, C.-H. A Call for Vaccine Against COVID-19: Implications for Cardiovascular Morbidity and Healthcare Utilization. Cardiovasc. Drugs Ther. 2020, 34, 585–587. [Google Scholar] [CrossRef]
- World Health Organization. Module 2: Types of Vaccine and Adverse Reactions. Available online: https://vaccine-safety-training.org/live-attenuated-vaccines.html (accessed on 23 March 2021).
- Guo, W.; Li, M.; Dong, Y.; Zhou, H.; Zhang, Z.; Tian, C.; Qin, R.; Wang, H.; Shen, Y.; Du, K.; et al. Diabetes is a risk factor for the progression and prognosis of COVID-19. Diabetes/Metab. Res. Rev. 2020, 36, e3319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katulanda, P.; Dissanayake, H.A.; Ranathunga, I.; Ratnasamy, V.; Wijewickrama, P.S.A.; Yogendranathan, N.; Gamage, K.K.K.; De Silva, N.L.; Sumanatilleke, M.; Somasundaram, N.P.; et al. Prevention and management of COVID-19 among patients with diabetes: An appraisal of the literature. Diabetology 2020, 63, 1440–1452. [Google Scholar] [CrossRef]
- Chen, C.; Yan, J.T.; Zhou, N.; Zhao, J.P.; Wang, D.W. Analysis of myocardial injury in patients with COVID-19 and association between concomitant cardiovascular diseases and severity of COVID-19. Zhonghua Xin Xue Guan Bing Za Zhi 2020, 48, E008. [Google Scholar]
- Anderson, R.M.; Vegvari, C.; Truscott, J.; Collyer, B.S. Challenges in creating herd immunity to SARS-CoV-2 infection by mass vaccination. Lancet 2020, 396, 1614–1616. [Google Scholar] [CrossRef]
Figure 1.
Schematic graph of the comparison between DNA and mRNA vaccine in terms of mechanisms. DNA vaccine is a circle DNA which contains the spike gene of SARS-CoV-2. After electroporation, cell membrane permeation will be increased, allowing DNA enter into cytoplasm thereby reaching to the nuclear. Subsequently, DNA will be translated into mRNA, which will be further translated into SARS-CoV-2 spike proteins and express on cell membrane. Nanoparticle-encapsulated mRNA encoding SARS-CoV-2 antigen will be integrated into cytoplasm. The spike mRNA utilizes ribosome and bases to translate spike proteins, which express on the cell membrane. The membrane spike protein will be recognized by antigen presenting cell (APC) thereby activating immune reaction.
Figure 1.
Schematic graph of the comparison between DNA and mRNA vaccine in terms of mechanisms. DNA vaccine is a circle DNA which contains the spike gene of SARS-CoV-2. After electroporation, cell membrane permeation will be increased, allowing DNA enter into cytoplasm thereby reaching to the nuclear. Subsequently, DNA will be translated into mRNA, which will be further translated into SARS-CoV-2 spike proteins and express on cell membrane. Nanoparticle-encapsulated mRNA encoding SARS-CoV-2 antigen will be integrated into cytoplasm. The spike mRNA utilizes ribosome and bases to translate spike proteins, which express on the cell membrane. The membrane spike protein will be recognized by antigen presenting cell (APC) thereby activating immune reaction.

{kind=link}
{kind=link}
Table 1.
Summary of vaccine trials.
| Title [Reference] | Clinical Phase | Population Characteristics of the Latest Trial | Doses | Technology | Immunogenicity | Safety Profile |
|---|---|---|---|---|---|---|
| BNT162b1 [4,5,6] | 1–2 | 45 adults in 3 groups: 10 μg, 30 μg, 100 μg 12 vaccines: 3 placebo in each group | 2 injections, 21 days apart | Lipid nanoparticle nucleoside-modified mRNA vaccine, encoding the spike glycoprotein of SARS-CoV-2 | Dose-dependent antibody response | No serious adverse events |
| BNT162b2 [7,8] | 1–3 | 43,448 volunteers aged 16 or older in total: (1:1 ratio) 21,720 received vaccines 21,728 received placebo | 2 injections of 30 μg doses for phase 3, 21 days apart | Lipid nanoparticle nucleoside-modified mRNA vaccine, encoding the spike glycoprotein of SARS-CoV-2 | Similar dose-dependent response as BNT162b | No serious adverse events |
| mRNA-1273 [9,10,11] | 1–3 | 30,420 adults in total: (1:1 ratio) 15,210 received vaccines 15,210 received placebo | 2 injections of 100 μg doses, 28 days apart | Lipid nanoparticle capsule of four lipids, encoding the S-2P antigen. | 100% seroconversion rates by day 15 | Similar grade 3 adverse events in the placebo group (1.3%) and the vaccine group (1.5%) |
| ChAdOx1 nCoV-19 [12,13,14] | 1–3 | 23,848 adults randomised 1:1 ratio to receive ChAdOx1 nCoV-19 or placebo | 2 injections of 3.5–6.5 × 1010 viral particles per mL, 28 days apart | Chimpanzee adenovirus-vectored vaccine with SARS-CoV-2 spike glycoprotein | Median titre of booster-dose group is more than 5 times higher than the single-dose group. | - 13 serious adverse events - None considered related to the vaccine |
| Ad5-vectored COVID-19 [15,16,17] | 1 & 2 | 508 adults randomised 2:1:1 to receive vaccine at the dosage of 1 × 1011, 5 × 1010, or placebo | 1 injection | Replication defective Ad5-vectored vaccine expressing the spike glycoprotein of SARS-CoV-2 | Higher antibody GMT in high-dose group, compared with medium and low-dose groups. | - 25 grade 3 or above adverse events - All resolved within 3 to 4 days without medications |
| rAd26-S and rAd5-S [18,19] | 1–3 | 21,977 adults in total: 16,501 received vaccines 5476 received placebo | 2 injections of 1011 viral particles in 0.5 mL vaccine, 21 days apart | Replication of Ad5-vectored and Ad-26 vectored vaccine expressing the gene for SARS-CoV-2 full-length glycoprotein S | 100% seroconversion rate | No serious adverse events |
| NVX-CoV2373 [20,21,22] | 1–3 | 30,000 adults in total: Randomised in 2:1 ratio to receive vaccine and saline placebo | 2 injections of 5 mg protein with 50 mcg matrix-M adjuvant, 21 days apart. | Nanoparticle of trimeric full-length SARS-CoV-2 spike glycoproteins and Matrix-M1 adjuvant | IgG GMT and neutralization responses exceeding convalescent serum | No serious adverse events |
| WIV-04 strain inactivated vaccine [10] | 1–2 | 96 adults randomised 1:1:1:1 to receive low-dose, medium-dose, high-dose and aluminium hydroxide, respectively | Phase 1: 3 injections on day 0, 28 and 56 | Isolated from WIV-04 strain and cultivated in a Verco cell line, followed by serial inactivation | 100% seroconversion rates in phase 1 trial and 85.7% in the phase 2 | Mild injection site pain and fever (23.4%) |
| Phase 2: 2 injections on day 0 and 14, or day 0 and 21 | ||||||
| BBIBP-CorV [11,23] | 1–2 | 192 adults: 18–59 years (96 adults) ≥60 years (96 adults). 24 receiving vaccine of 2 μg, 4 μg or 8 μg on day 0 and 28; and 24 receiving placebo. | Phase 1: 2 injections separated 28 days | HB02-strain in Verco cell line, with serial inactivation | - Higher seroconversion with higher dosage (8 μg) by day 14, - Higher neutralizing antibody GMT in younger adults | One grade 3 adverse event: self-limiting fever (>38.5 °C) |
| Phase 2: Single-dose | ||||||
| Coronavac [24] | 1–3 | 13,000 adults randomised to receive vaccine or placebo (randomisation ratio not provided) | 2 injections, 28 days apart | Inactivated vaccine from Vero cell line with SARS-CoV-2 (CN02 strain) | -High seroconversion rates: 83% in the 3 μg group, 79% in the 6 μg group, and 4% in the placebo group | One case of serious hypersensitivity with urticaria, recovered 3 months after medical treatment. |
| Ad26.COV2.S [25,26,27,28,29] | 1–3 | 40,000 adults randomised to receive vaccination or placebo (randomisation ratio not provided) | 1 injection of 5 × 1010 virus particles | replication-incompetent adenovirus serotype 26 (Ad26) vector encoding full-length SARS-CoV-2 spike protein | 100% seroconversion day 57 | Comparable serious adverse events in vaccination group and placebo group. |
| BBV152 [30,31,32] | 1–2 | 380 participants (aged 12–65 years) randomised by 1:1 ratio to receive vaccines of either 3 μg or 6 μg. | 2 intramuscular injections on day 0 and day 28 | whole-virion inactivated SARS-CoV-2 vaccine formulated with a toll-like receptor 7/8 agonist molecule (IMDG) adsorbed to alum (Algel) | 92.9% (95% CI 88.2–96.2) seroconversion rate in the 3 μg group, and 98.3% (95% CI 95.1–99.6) in the 6 μg group. | Comparable local and systemic adverse event profile in the 3 μg (9.47%) and 6 μg (11.0%) groups. No reported serious adverse events. |
Table 2.
Efficacy and other immune responses of vaccines after completion of vaccinations.
| Title [Reference] | Protective Efficacy | Antigen-Specific IgG GMT Level | Neutralizing Antibody Responses | Cellular Responses |
|---|---|---|---|---|
| BNT162b1 [4,5,6] | Similar to BNT162b2 (actual figure not stated) | - 10 μg: 4813 U/mL - 30 μg: 27,873 U/mL - Increase dosage to 100 μg did not increase the IgG GMC. - Lower antigen-binding IgG in participants ≥65 years of age | Higher GMT compared to convalescent serum panel - 10 μg: 1.8-fold - 30 μg: 2.8-fold | -Functional CD4+ and CD8+ responses in all participants, predominantly Th1 helper responses. - The mean fraction of RBD-specific T cells was higher than convalescent plasma. |
| BNT162b2 [7,8] | 94.6% (95% CI 89.9–97.3) | - 10 μg: 5782 U/mL - 20 μg: 12,464 U/mL - 30 μg: 9136 U/mL - Lower antigen-binding IgG for ≥65 years of age | Higher GMT compared to convalescent serum panel 18–55 years: 1.7–4.6 times ≥65 years: 1.1–2.2 times | Not assessed |
| mRNA1273 [9,10,11] | 94.1% (95% CI 89.3–96.8; p < 0.001) | - 25 μg: 299,751 U/mL - 100 μg: 782,719 U/mL - 250 μg: 1,192,154 U/mL | Neutralizing PRNT80 generally at or above the value of convalescent serum | - The 25 μg, 100 μg groups elicited CD4+ T cell responses to Th1 cytokines. - Minimal Th2 response |
| ChadOx1 nCoV-19 [12,13,14] | Overall: 70.4% (95% CI 54.8–80.6) 2-standard dose: 62.1% (95% CI 41.0–75.7) Low dose + standard dose: 90.0% (95% CI 67.4–97.0) | - Antigen-specific antibody peaked at day 28 with 157 GMEU - Antigen specific IgG on day 28 decreased with increasing age: 18–55 years: 6439 U/mL; 56–69 years: 4553 U/mL; and ≥70 years: 3565 U/mL | 91% and 100% participants achieved PRNT80 responses in one-dose and booster-dose groups, respectively. | - The median SFCs PBPMC in the standard-dose groups: 18–55 years: 1187; 56–69 years: 797 ≥70 years: 977 No significant increase of PBPMC after the booster vaccination (p = 0.46 from paired Student’s t test of day 28 vs. day 42) |
| Ad5-vectored COVID-19 [15,16,17] | Not available at the time of writing | - High-dose: 1445.8 (95% CI 935.5–2234.5); - Medium-dose: 806 (95% CI 528.2–1229.9) - Low-dose: 615.8 (95% CI 405.4–935.5) - Seroconversions of 97%, 94% and 100% in the low-dose, medium-dose and high-dose groups, respectively. | - High-dose: 34.0 (95% CI 22.6–50.1); - Medium-dose: 16.2 (95% CI 10.4–25.2); - Low-dose: 14.5 (95% CI 9.6–12.8)) - 4-fold increase of anti-RBD IgG in 50%, 50% and 75% in the high-dose, medium-dose and low-dose groups, respectively. | - The mean SFCs PMPMC: Low-dose: 20.8 (95%CI 12.7–34.0); Medium-dose: 40.8 (95% CI 27.6–60.3) and High-dose: 58.0 (95% CI 39.1–85.9) T-cell responses in the high-dose group significantly higher than the low-dose group (p < 0.001) |
| rAd26-S and rAd5-S [18,19] | 91.6% (95% CI 85.6–95.2) | SARS-CoV-2 S1 subunit-specific IgG GMT was 53,006 with Gam-COVID-Vac and 51,200 with Gam-COVID-Vac-Lyo | 100% neutralizing antibody with GMT 49.25 and 45.95 by using Gam-COVID-Vac and 51,200 with Gam-COVID-Vac-Lyo, respectively. | - 100% increased formation of CD4+ and CD8+ cells, and increased IFN-γ - Median cell proliferation: In frozen formulation: CD4+: + 2.5% CD8+: +1.3% In lyophilised formulation: CD4+: +1.3% CD8+: +1.1% |
| NVX-CoV2373 [20,21,22] | 89.3% (95% CI 75.2–95.4) against B.1.1.7 UK variant, 49.4% (95% CI 6.1–72.8) against B.1.351 South Africa variant. | - GMEU increase by 8 (15,319 units in “5 μg + M1” and 20,429 units in “25 μg + M1”). - GMEU level higher than in convalescent serum after second dose | GMFRs 5 times greater with adjuvant (5.2 times in “5 μg + M1” and 6.3 times in “25 μg + M1”). Second dose with adjuvant resulted in GMT levels 4 times greater than those in symptomatic infections. | Stimulated Th1 phenotype response with increased IFN-γ, IL-2 and TNF- α. Minimal Th2 responses as measured by IL-5 and IL-13 cytokines. |
| WIV-04 strain inactivated vaccine [10] | Not available at the time of writing. | - Low-dose: 415 (95% CI 288–597); - Medium-dose: 349 (95% CI 258–472); - High-dose: 311 (95% CI 229–422) | Neutralizing antibody levels increased significantly 14 days after the second dose, and the third dose | Not assessed |
| BBIBP-CorV [11,23] | Not available at the time of writing. | In the 4 μg trial by 14 days after the second dose, the GMTs were: - 279.2 (95% CI 192.6–404.7) against 35C; - 234.8 (95% CI 122.2–450.8) against 56Y; - 181.0 (95% CI 105.9–309.5) against 834Y; - 304.4 (95% CI 202.1–485.6) against HN97; - 117.4 (95% CI 61.1–225.4) against F13; - 193.3 (95% CI 141.4–264.0) against HB01; - 210.7 (95% CI 120.3–369.1) against BJ01, - 146.8 (95% CI 93.8–230.0) against CQ01; - 218.5 (95% CI 125.3–380.8) against QD01; - 394.8 (95% CI 256.5–607.6) against passage 7 virus. | -In age group 18–59 years, neutralizing antibody GMT were: 2 μg: 22.6 (95% CI 18.9–27.0); 4 μg: 29.3 (95% CI 23.8–36.0); 8 μg: 36.7 (95% CI 29.8–45.2) -In the age group ≥60 years, neutralizing antibody GMT were: 2 μg: 13.4 (95% CI 9.4–19.0); 4 μg: 18.9 (95% CI 13.4–26.6); 8 μg: 23.7 (95% CI 19.0–29.6) | Not assessed |
| Coronavac [24] | Brazil: symptomatic prevention: 50.4% - mild cases prevention: 78% Severe cases prevention: 100% Turkey: 83.5% (confidence interval not reported) Indonesia: 65.3%. (confidence interval not reported) | 3 μg: 27.6 (95% CI 22.7–33.5) 6 μg: 34.5 (95% CI 28.5–41.8) Placebo: 2.3 (95% CI 2.0–2.5) | 3 μg: 5.6 (95% CI 3.6–8.7); 6 μg: 7.7 (95% CI 5.2–11.5); Placebo: 2.0 (95% CI 2.0–2.0) | The average IFN-γ positive spot-forming cells per 100,000 cells were: 3 μg group: 7.4 (95% CI 3.9–11.1); 6 μg group: 3.9 (95% CI 1.0–6.7); Placebo: 1.5 (95% CI 0.2–2.9) |
| Ad26.COV2.S [25,26,27,28,29] | Overall: 66.9% (95% CI 59.0–73.4) ≥60 years old 76.3% (95% CI, 61.6–86.0) | - Ranged from 2432 U/mL to 5729 U/mL. - The booster immunization on day 57 increased binding antibody titres 2.56-fold (range 1.58–3.04). | - The GMT of neutralizing antibody ranged from 242 to 449. - The booster immunization on day 57 increased neutralizing antibody titres by a mean of 4.62-fold (range: 3.56–5.68). | Stronger CD4+ cells response recorded in younger adults: 18–55 years:76 to 83% ≥65 years: 60 to 67% |
| BBV152 [30,31,32] | Not reported | - 3 μg: 100.9 (95% CI 74.1–137.4) - 6 μg: 197.0 (95% CI 155.6–249.4) (p = 0.0041) | The neutralizing IgG GMTs at day 56 were 10,413.9 (95% CI 9142.4–11,862.2) in the 3 μg group; and 9541.6 (95% CI 8245.9–11,041.0) in the 6 μg group at day 56. | Strongly biased to a Th1 cell response at day 42. Th2 response were detected at minimal level. |
GMC: Geometric Mean Concentration (U/mL); GMT: Geometric Mean Titre (U/mL); GMEU: Geometric Mean ELISA units (U/mL); GMFR: Geometric Mean Fold Rises (Times); RBD: Receptor-Binding Domain; PMPMC: Per Million Peripheral Mononuclear cells; PRNT80: Plaque Reduction Neutralizing Testing assay with detectable 80% live-virus neutralization.
Table 3.
Progress of existing 86 vaccines candidates in clinical trial as at 6th April 2021.
| Number | Vaccine Platform | Type of Candidate VACCINE | Usage | Developer | Clinical Status | Phase Trials Registration No. |
|---|---|---|---|---|---|---|
| 1 | Inactivated virus | CoronaVac; SARS-CoV-2 vaccine (inactivated) | 2 doses (day 0 + 14) Intramuscular | Sinovac Research and Development Co., Ltd. | Phase 4 | Phase ½: NCT04383574 NCT04352608 NCT04551547 |
| Phase 3: NCT04456595 NCT04508075 NCT04582344 NCT04617483 NCT04651790 NCT04800133 | ||||||
| Phase 4: NCT04756830 NCT04747821 NCT04775069 NCT04789356 NCT04754698 NCT04801888 | ||||||
| 2 | Inactivated virus | Inactivated SARS-CoV-2 vaccine (Vero cell) | 2 doses (day 0 + 21) Intramuscular | Sinopharm + China National Biotec Group Co + Wuhan Institute of Biological Products | Phase 3 | Phase ½: ChiCTR2000031809 |
| Phase 3: ChiCTR2000034780 ChiCTR2000039000 NCT04510207 NCT04612972 | ||||||
| 3 | Inactivated virus | Inactivated SARS-CoV-2 vaccine (Vero cell), vaccine name BBIBP-CorV | 2 doses (day 0 + 21) Intramuscular | Sinopharm + China National Biotec Group Co + Beijing Institute of Biological Products | Phase 3 | Phase 1/2: ChiCTR2000032459 |
| Phase 3: NCT04560881 NCT04510207 | ||||||
| 4 | Viral vector (Non-replicating) | ChAdOx1-S—(AZD1222) (Covishield) | 2 doses (day 0 + 28) Intramuscular | AstraZeneca + University of Oxford | Phase 4 | Phase 1: PACTR202005681895696 |
| Phase 1/2: PACTR202006922165132 NCT04568031 NCT04444674 NCT04324606 NCT04684446 ISRCTN15638344 NCT04760730 | ||||||
| Phase 2 NCT04686773 ISRCTN69254139 | ||||||
| Phase 3: ISRCTN89951424 NCT04516746 NCT04540393 NCT04536051 EUCTR2020–005226-28-DE NCT04800133 | ||||||
| Phase 4: NCT04760132 NCT04775069 | ||||||
| 5 | Viral vector (Non-replicating) | Recombinant novel coronavirus vaccine (Adenovirus type 5 vector) | 1 dose Day 0 Intramuscular | CanSino Biological Inc./Beijing Institute of Biotechnology | Phase 3 | Phase 1: ChiCTR2000030906 NCT04313127 NCT04568811 NCT04552366 |
| Phase 1/2: NCT04398147 | ||||||
| Phase 2: ChiCTR2000031781 NCT04566770 NCT04341389 | ||||||
| Phase 3: NCT04526990 NCT04540419 | ||||||
| 6 | Viral vector (Non-replicating) | Gam-COVID-Vac Adeno-based (rAd26-S + rAd5-S) | 2 doses (day 0 + 21) Intramuscular | Gamaleya Research Institute; Health Ministry of the Russian Federation | Phase 3 | Phase 1/2: NCT04436471 NCT04437875 NCT04713488 NCT04760730 |
| Phase 2: NCT04587219 | ||||||
| Phase 2/3: NCT04640233 | ||||||
| Phase 3: NCT04530396 NCT04564716 NCT04642339 NCT04656613 NCT04741061 | ||||||
| 7 | Viral vector (Non-replicating) | Ad26.COV2.S | 1–2 doses Day 0 or Day 0+ Day 56 Intramuscular | Janssen Pharmaceutical | Phase 3 | Phase 1: NCT04509947 |
| Phase 1/2: NCT04436276 | ||||||
| Phase 2: EUCTR2020-002584-63-DE NCT04535453 NCT04765384 | ||||||
| Phase 3: NCT04505722 NCT04614948 | ||||||
| 8 | Protein subunit | SARS-CoV-2 rS/Matrix M1-Adjuvant (Full length recombinant SARS CoV-2 glycoprotein nanoparticle vaccine adjuvanted with Matrix M) | 2 doses (day 0 + 21) Intramuscular | Novavax | Phase 3 | Phase 1/2: NCT04368988 |
| Phase 2: NCT04533399 | ||||||
| Phase 3: NCT04611802 EUCTR2020-004123-16-GB NCT04583995 | ||||||
| 9 | RNA based vaccine | mRNA -1273 mRNA-1283 | 2 doses (day 0 + 28) Intramuscular | Moderna + National Institute of Allergy and Infectious Diseases (NIAID) | Phase 4 | Phase 1: NCT04283461 NCT04813796 |
| Phase 1/2: NCT04677660 NCT04712110 | ||||||
| Phase 2: NCT04405076 NCT04761822 | ||||||
| Phase 2/3: NCT04649151 NCT04796896 | ||||||
| Phase 3: NCT04470427 NCT04811664 NCT04805125 NCT04806113 | ||||||
| Phase 4: NCT04760132 NCT04792567 | ||||||
| 10 | RNA based vaccine | BNT162b2 | 2 doses (day 0 + 21) Intramuscular | Pfizer/BioNTech + Fosun Pharma | Phase 4 | Phase 1: NCT04523571 ChiCTR2000034825 NCT04816643 |
| Phase 1/2: NCT04588480 NCT04380701 NCT04537949 EUCTR2020-003267-26-DE | ||||||
| Phase 2: NCT04649021 NCT04761822 | ||||||
| Phase 2/3: NCT04754594 | ||||||
| Phase 3: NCT04368728 NCT04713553 NCT04800133 NCT04805125 NCT04816669 | ||||||
| Phase 4: NCT04760132 EUCTR2021-000412-28-BE EUCTR2021-000412-28-BE NCT04780659 NCT04775069 | ||||||
| 11 | Protein subunit | Recombinant SARS-CoV-2 vaccine (CHO Cell) | 2–3 doses Day 0 + 28 or Day 0 + 28 + 56 Intramuscular | Anhui Zhifei Longcom Biopharmaceutical + Institute of Microbiology, Chinese Academy of Sciences | Phase 3 | Phase 1: NCT04445194 ChiCTR2000035691 NCT04636333 |
| Phase 1/2: NCT04550351 NCT04813562 | ||||||
| Phase 2: NCT04466085 | ||||||
| Phase 3: NCT04646590 | ||||||
| 12 | RNA based vaccine | CVnCoV Vaccine | 2 doses Day 0 + Day 28 Intramuscular | CureVac AG | Phase 3 | Phase 1: NCT04449276 |
| Phase 2: NCT04515147 PER-054-20 | ||||||
| Phase 2/3: NCT04652102 | ||||||
| Phase 3: NCT04674189 | ||||||
| 13 | Inactivated virus | SARS-CoV-2 vaccine (Vero cells) | 2 doses Day 0 + Day 28 Intramuscular | Institute of Medical Biology + Chinese Academy of Medical Sciences | Phase 3 | Phase 1/2: NCT04470609 NCT04412538 |
| Phase 3: NCT04659239 | ||||||
| 14 | Inactivated virus | QazCovid-in®—COVID-19 inactivated vaccine | 2 doses Day 0 + Day 21 Intramuscular | Research Institute for Biological Safety Problems, Rep of Kazakhstan | Phase 3 | Phase ½: NCT04530357 |
| Phase 3: NCT04691908 | ||||||
| 15 | DNA based vaccine | INO-4800 + electroporation | 2 doses Day 0 + Day 28 Intradermal | Inovio Pharmaceuticals + International Vaccine Institute + Advaccine (Suzhou) Biopharmaceutical Co., Ltd. | Phase 2/3 | Phase 1: NCT04336410 ChiCTR2000038152 |
| Phase 1/2: NCT04447781 | ||||||
| Phase 2: ChiCTR2000040146 | ||||||
| Phase 2/3: NCT04642638 | ||||||
| 16 | DNA based vaccine | AG0301-COVID19 | 2 doses Day 0 + Day 14 Intramuscular | AnGes + Takara Bio + Osaka University | Phase 2/3 | Phase 1/2: NCT04463472 NCT04527081 jRCT2051200085 |
| Phase 2/3: NCT04655625 | ||||||
| 17 | DNA based vaccine | nCov vaccine | 3 doses Day 0 + Day 28 + Day 56 Intradermal | Zydus Cadila | Phase 3 | Phase 1/2: CTRI/2020/07/026352 CTRI/2021/03/032051 |
| Phase 3: CTRI/2020/07/026352 | ||||||
| 18 | DNA based vaccine | GX-19N | 2 doses Day 0 + Day 28 Intramuscular | Genexine Consortium | Phase ½ | Phase 1/2: NCT04445389 NCT04715997 |
| 19 | Inactivated virus | Whole-Virion Inactivated SARS-CoV-2 Vaccine (BBV152) | 2 doses Day 0 + Day 14 Intramuscular | Bharat Biotech International Limited | Phase 3 | Phase 1/2: NCT04471519 CTRI/2020/07/026300 CTRI/2020/09/027674 |
| Phase 3: NCT04641481; CTRI/2020/11/028976 | ||||||
| 20 | Protein subunit | KBP-COVID-19 (RBD-based) | 2 doses Day 0 + Day 21 Intramuscular | Kentucky Bioprocessing Inc. | Phase 1/2 | Phase 1/2: NCT04473690 |
| 21 | Protein subunit | VAT00002: SARS-CoV-2 S protein with adjuvant | 2 doses Day 0 + Day 21 Intramuscular | Sanofi Pasteur + GSK | Phase 3 | Phase 1/2: NCT04537208 |
| Phase 2: NCT04762680 | ||||||
| Phase 3: PACTR202011523101903 | ||||||
| 22 | RNA based vaccine | ARCT-021 | 2 doses Day 0 + Day 21 Intramuscular | Arcturus Therapeutics | Phase 2 | Phase 1/2: NCT04480957 |
| Phase 2: NCT04668339 NCT04728347 | ||||||
| 23 | Virus like particle | RBD SARS-CoV-2 HBsAg VLP vaccine | 2 doses Day 0 + Day 28 Intramuscular | Serum Institute of India + Accelagen Pty + SpyBiotech | Phase 1/2 | Phase 1/2: ACTRN12620000817943 ACTRN12620001308987 |
| 24 | Inactivated virus | Inactivated SARS-CoV-2 vaccine (Vero cell) | 2–3 doses Detailed schedule not specified Intramuscular | Beijing Minhai Biotechnology Co | Phase 2 | Phase 1: NCT04758273 |
| Phase 2: NCT04756323 | ||||||
| 25 | Viral vector (Non-replicating) | GRAd-COV2 (Replication defective Simian Adenovirus (GRAd) encoding S) | 1 dose Day 0 Intramuscular | ReiThera + Leukocare + Univercells | Phase 2/3 | Phase 1: NCT04528641 |
| Phase 2/3: NCT04791423 | ||||||
| 26 | Viral vector (Non-replicating) | VXA-CoV2-1 Ad5 adjuvanted Oral Vaccine platform | 2 doses Day 0 + Day 28 Intramuscular | Vaxart | Phase 1 | Phase 1: NCT04563702 |
| 27 | Viral vector (Non-replicating) | MVA-SARS-2-S | 2 doses Day 0 + Day 28 Intramuscular | University of Munich (Ludwig-Maximilians) | Phase 1 | Phase 1: NCT04569383 |
| 28 | Protein subunit | SCB-2019 + AS03 or CpG 1018 adjuvant plus Alum adjuvant (Native like Trimeric subunit Spike Protein vaccine) | 2 doses Day 0 + Day 21 Intramuscular | Clover Biopharmaceuticals Inc./GSK/Dynavax | Phase 2/3 | Phase 1: NCT04405908 |
| Phase 2/3: NCT04672395 | ||||||
| 29 | Protein subunit | COVAX-19® Recombinant spike protein + adjuvant | 2 doses Day 0 + Day 21 Intramuscular | Vaxine Pty Ltd. | Phase 1 | Phase 1: NCT04453852 |
| 30 | Protein subunit | MVC-COV1901 (S-2P protein + CpG 1018) | 2 doses Day 0 + Day 28 Intramuscular | Medigen Vaccine Biologics + Dynavax + National Institute of Allergy and Infectious Diseases (NIAID) | Phase 2 | Phase 1: NCT04487210 |
| Phase 2: NCT04695652 | ||||||
| 31 | Protein subunit | FINLAY-FR1 anti-SARS-CoV-2 Vaccine (RBD + adjuvant) | 2 doses Day 0 + Day 28 Intramuscular | Instituto Finlay de Vacunas | Phase 1/2 | Phase 1: RPCEC00000338 |
| Phase 1/2: RPCEC00000332 | ||||||
| 32 | Protein subunit | FINLAY-FR-2 anti-SARS-CoV-2 Vaccine (RBD chemically conjugated to tetanus toxoid plus adjuvant) | 2 doses Day 0 + Day 28 Intramuscular | Instituto Finlay de Vacunas | Phase 3 | Phase 1: RPCEC00000340 |
| Phase 2: RPCEC00000347 | ||||||
| Phase 3: RPCEC00000354 | ||||||
| 33 | Protein subunit | EpiVacCorona (EpiVacCorona vaccine based on peptide antigens for the prevention of COVID-19) | 2 doses Day 0 + Day 21 Intramuscular | Federal Budgetary Research Institution State Research Center of Virology and Biotechnology “Vector” | Phase 3 | Phase 1/2: NCT04527575 |
| Phase 3: NCT04780035 | ||||||
| 34 | Protein subunit | RBD (baculovirus production expressed in Sf9 cells) Recombinant SARS-CoV-2 vaccine (Sf9 Cell) | 2 doses Day 0 + Day 21 Intramuscular | West China Hospital + Sichuan University | Phase 2 | Phase 1: ChiCTR2000037518 NCT04530656 |
| Phase 2: ChiCTR2000039994 NCT04640402 NCT04718467 | ||||||
| 35 | Protein subunit | IMP CoVac-1 (SARS-CoV-2 HLA-DR peptides) | 1 dose Day 0 Subcutaneous | University Hospital Tuebingen | Phase 1 | NCT04546841 |
| 36 | Protein subunit | UB-612 (Multitope peptide based S1-RBD-protein based vaccine) | 2 doses Day 0 + Day 28 Intramuscular | COVAXX + United Biomedical Inc | Phase 2/3 | Phase 1: NCT04545749 |
| Phase 2: NCT04773067 | ||||||
| Phase 2/3: NCT04683224 | ||||||
| 37 | Viral vector (Replicating) | DelNS1-2019-nCoV-RBD-OPT1 (Intranasal flu-based-RBD) | 2 doses Day 0 + Day 28 Intranasal | University of Hong Kong, Xiamen University and Beijing Wantai Biological Pharmacy | Phase 2 | Phase 1: ChiCTR2000037782 NCT04809389 |
| Phase 2: ChiCTR2000039715 | ||||||
| 38 | RNA based vaccine | LNP-nCoVsaRNA | 2 doses Day 0 + Day 28 Intranasal | Imperial College London | Phase 1 | Phase 1: ISRCTN17072692 |
| 39 | RNA based vaccine | SARS-CoV-2 mRNA vaccine (ARCoV) | 2 doses Day 0 + Day 28 Intranasal | Academy of Military Science (AMS), Walvax Biotechnology and Suzhou Abogen Biosciences | Phase 2 | Phase 1: ChiCTR2000034112 ChiCTR2000039212 |
| Phase 2: ChiCTR2100041855 | ||||||
| 40 | Virus like particle | Coronavirus-Like Particle COVID-19 (CoVLP) | 2 doses Day 0 + Day 21 Intranasal | Medicago Inc. | Phase 2/3 | Phase 1: NCT04450004 |
| Phase 2: NCT04662697 | ||||||
| Phase 2/3: NCT04636697 | ||||||
| 41 | Viral vector (Replicating) + APC | Covid-19/aAPC vaccine. The Covid-19/aAPC vaccine is prepared by applying lentivirus modification with immune modulatory genes and the viral minigenes to the artificial antigen presenting cells (aAPCs). | 3 doses Day 0 + Day 14 + Day 28 Subcutaneous | Shenzhen Geno-Immune Medical Institute | Phase 1 | Phase 1: NCT04299724 |
| 42 | Viral vector (Non-replicating) + APC | LV-SMENP-DC vaccine. Dendritic cells are modified with lentivirus vectors expressing Covid-19 minigene SMENP and immune modulatory genes. CTLs are activated by LV-DC presenting Covid-19 specific antigens. | 1 dose Day 0 Subcutaneous | Shenzhen Geno-Immune Medical Institute | Phase 1/2 | Phase 1/2: NCT04276896 |
| 43 | Protein subunit | AdimrSC-2f (Recombinant RBD +/− Aluminium) | No detail | Adimmune Corporation | Phase 1 | Phase 1: NCT04522089 |
| 44 | DNA based vaccine | Covigenix VAX-001—DNA vaccines + proteo-lipid vehicle (PLV) formulation | 2 doses Day 0 + Day 14 Intramuscular | Entos Pharmaceuticals Inc. | Phase 1 | NCT04591184 |
| 45 | DNA based vaccine | CORVax—Spike (S) Protein Plasmid DNA Vaccine | 2 doses Day 0 + Day 14 Intradermal | Providence Health & Services | Phase 1 | Phase 1: NCT04627675 |
| 46 | RNA based vaccine | ChulaCov19 mRNA vaccine | 2 doses Day 0 + Day 21 Intramuscular | Chulalongkorn University | Phase 1 | Phase 1: NCT04566276 |
| 47 | DNA based vaccine | bacTRL-Spike oral DNA vaccine | 1 dose Day 0 Oral | Symvivo Corporation | Phase 1 | NCT04334980 |
| 48 | Viral Vector (Non-replicating) | Human Adenovirus type 5: hAd5 S + N vaccine (S-fusion + N-ETSD) E2b-deleted Adeno | 1–2 doses Day 0 + day 21 Subcutaneous or Oral | Immunity Bio.Inc | Phase 1 | Phase 1: NCT04591717 NCT04710303 |
| 49 | Viral vector (Non-replicating) | COH04S1 (MVA-SARS-2-S)—Modified vaccinia ankara (sMVA) platform + synthetic SARS-CoV-2 | 2 doses Day 0 + Day 28 Intramuscular | City of Hope Medical Center + National Cancer Institute | Phase 1 | Phase 1: NCT04639466 |
| 50 | Viral vector (Replicating) | rVSV-SARS-CoV-2-S Vaccine | 1 dose Day 0 Intramuscular | Israel Institute for Biological Research | Phase 1/2 | Phase 1/2: NCT04608305 |
| 51 | Viral vector (Replicating) + APC | Dendritic cell vaccine AV-COVID-19. A vaccine consisting of autologous dendritic cells loaded with antigens from SARS-CoV-2, with or without GM-CSF | 1 dose Day 0 Intramuscular | Aivita Biomedical, Inc. National Institute of Health Research and Development, Ministry of Health Republic of Indonesia | Phase 1/2 | Phase 1: NCT04690387 NCT04685603 |
| Phase 1/2: NCT04386252 | ||||||
| 52 | Live attenuated virus | COVI-VAC | 1–2 doses Day 0 or Day 0 + 28 Intranasal | Codagenix/Serum Institute of India | Phase 1 | Phase 1: NCT04619628 |
| 53 | Protein subunit | CIGB-669 (RBD + AgnHB) | 3 doses Day 0 + 14 + 28 or Day 0 + 28 + 56 Intranasal | Center for Genetic Engineering and Biotechnology (CIGB) | Phase 1/2 | Phase 1/2: RPCEC00000345 |
| 54 | Protein subunit | CIGB-66 (RBD + aluminium hydroxide) | 3 doses Day 0 + 14 + 28 or Day 0 + 28 + 56 Intranasal | Center for Genetic Engineering and Biotechnology (CIGB) | Phase 3 | Phase 1/2: RPCEC00000346 |
| Phase 3 RPCEC00000359 | ||||||
| 55 | Inactivated Virus | VLA2001 | 2 doses Day 0 + Day 21 Intramuscular | Valneva, National Institute for Health Research, United Kingdom | Phase 1/2 | Phase 1/2: NCT04671017 |
| 56 | Protein subunit | BECOV2 | 2 doses Day 0 + Day 28 Intramuscular | Biological E. Limited | Phase 1/2 | Phase 1/2: CTRI/2020/11/029032 |
| 57 | Viral vector (Replicating) | AdCLD-CoV19 (adenovirus vector) | 1 dose Day 0 Intramuscular | Cellid Co., Ltd. | Phase 1/2 | Phase 1/2: NCT04666012 |
| 58 | DNA based vaccine | GLS-5310 | 2 doses Day 0 + Day 56 or Day 0 + Day 84 Intradermal | GeneOne Life Science, Inc. | Phase 1/2 | Phase 1/2: NCT04673149 |
| 59 | Protein subunit | Recombinant Sars-CoV-2 Spike protein, Aluminum adjuvanted | 2 doses Day 0 + 21 Intramuscular | Nanogen Pharmaceutical Biotechnology | Phase 1/2 | Phase 1/2: NCT04683484 |
| 60 | Protein subunit | Recombinant protein vaccine S-268019 (using Baculovirus expression vector system) | 2 doses Day 0 + 21 Intramuscular | Shionogi | Phase 1/2 | Phase 1/2: jRCT2051200092 |
| 61 | Viral vector (Non-replicating) | AdCOVID, Adenovirus-based platform expresses the receptor-binding domain (RBD) of the Sars-Cov-2 spike protein | 1 doses Day 0 Intranasal | Altimmune, Inc. | Phase 1 | Phase 1: NCT04679909 |
| 62 | Protein subunit | SARS-CoV-2-RBD-Fc fusion protein | Dosage and Schedule not specified Subcutaneous or intramuscular | University Medical Center Groningen + Akston Biosciences Inc. | Phase 1/2 | Phase 1/2: NCT04681092 |
| 63 | Inactivated Virus | ERUCOV-VAC, inactivated virus | 2 doses Day 0 + 21 Intramuscular | Erciyes University | Phase 2 | Phase 1: NCT04691947 |
| Phase 2: NCT04824391 | ||||||
| 64 | Protein subunit | COVAC-1 and COVAC-2 sub-unit vaccine (spike protein) + SWE adjuvant | 2 doses Day 0 + 28 Intramuscular | University of Saskatchewan | Phase 1/2 | Phase 1/2: NCT04702178 |
| 65 | Protein subunit | GBP510, a recombinant surface protein vaccine with adjuvant AS03 (aluminium hydroxide) | 2 doses Day 0 + 28 Intramuscular | SK Biosciences Co. Ltd. and CEPI | Phase 1/2 | Phase 1/2: NCT04742738 NCT04750343 |
| 66 | Protein subunit | Razi Cov Pars, recombinant spike protein | 3 doses Day 0 + 21 + 51 Intramuscular and intranasal | Razi Vaccine and Serum Research Institute | Phase 1 | Phase 1: IRCT20201214049709N1 |
| 67 | Inactivated Virus | COVID-19 inactivated vaccine | 2 doses Day 0 + 14 Intramuscular | Shifa Pharmed Industrial Co | Phase 2/3 | Phase 1: IRCT20201202049567N1 IRCT20201202049567N2 |
| 68 | Protein subunit | MF59 adjuvanted SARS-CoV-2 Sclamp vaccine | 2 doses Day 0 + 28 Intramuscular | The University of Queensland | Phase 1 | Phase 1: NCT04495933 |
| 69 | DNA based vaccine | COVIGEN | 2 doses Day 0 + 28 Intramuscular or intradermal | University of Sydney, Bionet Co., Ltd. Technovalia | Phase 1 | Phase 1: NCT04742842 |
| 70 | DNA based vaccine | COVID-eVax, a candidate plasmid DNA vaccine of the Spike protein | No detailed dosage schedule Intramuscular | Takis + Rottapharm Biotech | Phase 1/2 | Phase 1/2: NCT04788459 EUCTR2020-003734-20-IT |
| 71 | Viral vector (Non-replicating) | BBV154, Adenoviral vector COVID-19 vaccine | 1 dose Day 0 Intramuscular | Bharat Biotech International Limited | Phase 1 | Phase 1: NCT04751682 |
| 72 | RNA based vaccine | PTX-COVID19-B, mRNA vaccine | 2 doses Day 0 + 28 Intramuscular | Providence Therapeutics | Phase 1 | Phase 1: NCT04765436 |
| 73 | Viral vector (Replicating) | NDV-HXP-S, Newcastle disease virus (NDV) vector expressing the spike protein of SARS-CoV-2, with or without the adjuvant CpG 1018 | 2 doses Day 0 + 28 Intramuscular | Mahidol University; The Government Pharmaceutical Organization (GPO); Icahn School of Medicine at Mount Sinai | Phase 1/2 | Phase 1/2: NCT04764422 |
| 74 | RNA based vaccine | CoV2 SAM (LNP) vaccine. A self-amplifying mRNA (SAM) lipid nanoparticle (LNP) platform + Spike antigen | 2 doses Day 0 + 28 Intramuscular | GlaxoSmithKline | Phase 1 | Phase 1: NCT04758962 |
| 75 | Virus like particle | VBI-2902a. An enveloped virus-like particle (eVLP) of SARS-CoV-2 spike (S) glycoprotein and aluminum phosphate adjuvant. | 2 doses Day 0 + 28 Intramuscular | VBI Vaccines Inc. | Phase 1/2 | NCT04773665 |
| 76 | Protein subunit | SK SARS-CoV-2 recombinant surface antigen protein subunit (NBP2001) + adjuvanted with alum. | 2 doses Day 0 + 28 Intramuscular | SK Bioscience Co., Ltd. | Phase 1 | Phase 1: NCT04760743 |
| 77 | Viral vector (Non-replicating) | Chimpanzee Adenovirus serotype 68 (ChAd) and self-amplifying mRNA (SAM) vectors expressing spike alone, or spike plus additional SARS-CoV-2 T cell epitopes. | 2–3 doses Day 0 +14 + 28 or Day 0 + 28 + 56 or Day 0 + 112 Intramuscular | Gritstone Oncology | Phase 1 | Phase 1: NCT04776317 |
| 78 | RNA based vaccine | mRNA-1273.351. A lipid nanoparticle (LNP)-encapsulated mRNA-based vaccine that encodes for a full-length, prefusion stabilized S protein of the SARS-CoV-2 B.1.351 variant. | 3 doses Day 0 + 28 + 56 Intramuscular | Moderna + National Institute of Allergy and Infectious Diseases (NIAID) | Phase 1 | Phase 1: NCT04785144 |
| 79 | Protein subunit | SpFN (spike ferritin nanoparticle) uses spike proteins with a liposomal formulation QS21 (ALFQ) adjuvant. | 3 doses Day 0 + 28 + 120 Intramuscular | Walter Reed Army Institute of Research (WRAIR) | Phase 1 | Phase 1: NCT04784767 |
| 80 | Protein subunit | EuCorVac-19; A spike protein using the recombinant protein technology and with an adjuvant. | 2 doses Day 0 + 21 Intramuscular | POP Biotechnologies and EuBiologics Co.,Ltd | Phase 1/2 | Phase 1/2: NCT04783311 |
| 81 | Inactivated virus | Inactivated SARS-CoV-2 vaccine FAKHRAVAC (MIVAC) | 2 doses Day 0 + 21 Intramuscular | Organization of Defensive Innovation and Research | Phase 1 | Phase 1: IRCT20210206050259N1 |
| 82 | Live attenuated virus | MV-014-212, a live attenuated vaccine that expresses the spike (S) protein of SARS-CoV-2 | 2 doses Day 0 + 35 Intranasal | Meissa Vaccines, Inc. | Phase 1 | Phase 1: NCT04798001 |
| 83 | RNA based vaccine | MRT5500, an mRNA vaccine candidate | 2 doses Day 0 + 21 Intramuscular | Sanofi Pasteur and Translate Bio | Phase 1/2 | Phase 1/2: NCT04798027 |
| 84 | Virus like particle | SARS-CoV-2 VLP Vaccine | 1 doses Day 0 Subcutaneous | The Scientific and Technological Research Council of Turkey | Phase 1 | Phase 1: NCT04818281 |
| 85 | Protein subunit | ReCOV: Recombinant two-component spike and RBD protein COVID-19 vaccine (CHO cell). | 2 doses Day 0 + 21 Intramuscular | Jiangsu Rec-Biotechnology | Phase 1 | Phase 1: NCT04818801 |
| 86 | RNA based vaccine | DS-5670a, mRNA vaccine | 2 doses Day 0 + 21 Intramuscular | Daiichi Sankyo Co., Ltd. | Phase 1/2 | Phase 1/2: NCT04821674 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Yan, Z.-P.; Yang, M.; Lai, C.-L. COVID-19 Vaccines: A Review of the Safety and Efficacy of Current Clinical Trials. Pharmaceuticals 2021, 14, 406. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14050406
AMA Style
Yan Z-P, Yang M, Lai C-L. COVID-19 Vaccines: A Review of the Safety and Efficacy of Current Clinical Trials. Pharmaceuticals. 2021; 14(5):406. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14050406
Chicago/Turabian StyleYan, Zhi-Peng, Ming Yang, and Ching-Lung Lai. 2021. "COVID-19 Vaccines: A Review of the Safety and Efficacy of Current Clinical Trials" Pharmaceuticals 14, no. 5: 406. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14050406
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.