
Considerations to Be Taken When Carrying Out Medicinal Plant Research—What We Learn from an Insight into the IC50 Values, Bioavailability and Clinical Efficacy of Exemplary Anti-Inflammatory Herbal Components

Abstract
:1. Introduction
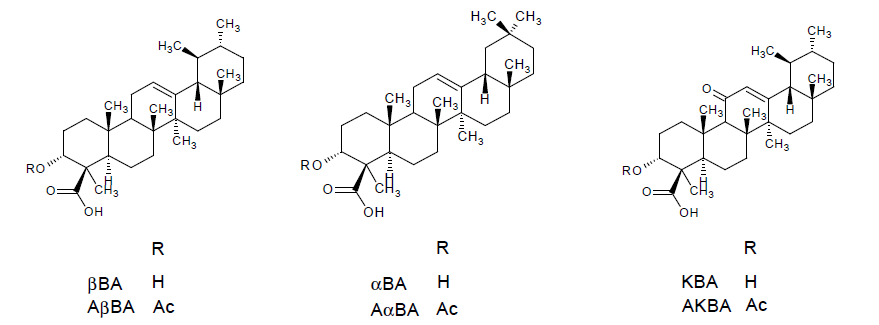
2. Frankincense Extracts: In Vitro IC50 Values, Bioavailability and Clinical Efficacy
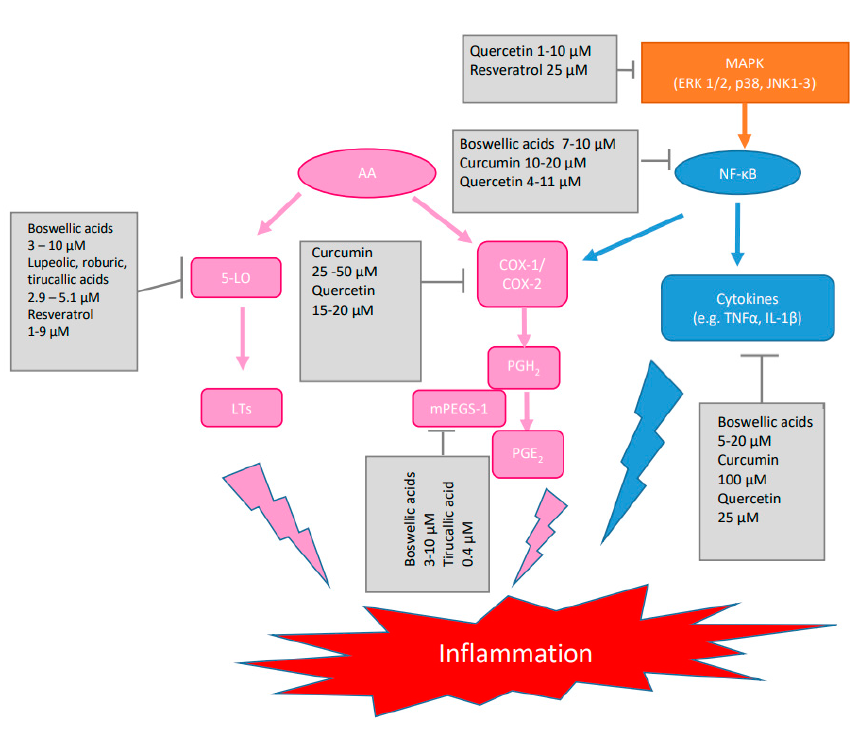
2.1. In Vitro IC50 Values
2.2. Oral Bioavailability in Human
2.3. Clinical Trials

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | Study Design | Dosage | Observations | References |
|---|---|---|---|---|
| Osteoarthritis knee | Pilot, randomized, double-blind, placebo-controlled on 48 newly diagnosed or untreated osteoarthritis patients | Self-administration of two tablets à 169.33 mg Boswellia serrata extract enriched in AKBA and βBA (AKBA 53.27 mg, βBA 20.83 mg, KBA 7.11 mg, AβBA 6.06 mg) for 120 days | ↓ pain and stiffness ↑ motility of knee joints ↓ hs-CRP | [41] |
| Osteoarthritis knee | Pilot, randomized, double-blind, placebo-controlled on 60 patients with mild to moderate osteoarthritis | Aflapin 100 mg per day for 30 days (Aflapin contains Boswellia serrata extract enriched in AKBA with non-volatile oil of Boswellia serrata) | Clinically and statistically significant improvement in pain scores and physical function scores already after 5 days of treatment by ↓ 5-LO and ↓ TNFα | [42] |
| Osteoarthritis knee | randomized, double-blind, placebo-controlled on 60 patients with mild to moderate symptoms | Aflapin 100 mg per day compared to 100 mg 5-Loxin per day for 90 days | Clinically and statistically significant improvement in pain scores and physical functional scores 7 days after start of treatment ↓ TNFα induced cartilage degrading synovial fluid matrix metalloproteinase-3 and ↓ TNFα induced intercellular adhesion molecule (ICAM)-1 expression Aflapin better than 5-Loxin | [43] |
| Osteoarthritis knee | randomized, double-blind, placebo-controlled on 75 patients with mild to moderate symptoms | 100 mg or 250 mg 5-Loxin (Boswellia serrata extract enriched with 30% AKBA) for 90 days | dose dependant clinically and statistically significant improvement in pain scores and physical functional scores 7 days after start of treatment ↓ TNFα induced synovial fluid matrix metalloproteinase-3 | [44] |
| Osteoarthritis knee | randomized, double-blind, placebo-controlled on 30 patients | 3 × 333 mg WokVel™ per day for 8 weeks (Boswellia serrata oleogum resin with a minimum of 65% organic acids or a minimum of 40% total boswellic acids) | ↓ knee pain, ↑ knee flexion, ↑ walking distance and ability to climb stairs. After withdrawal of treatment symptoms returned | [45] |
| Morbus Crohn | randomized double-blind, verum-controlled parallel group on 83 patients | ↓ Crohn’s Disease Activity Index (CDAI) by 90 in the H15 group and by 53 score points after therapy with mesalazine. Difference not statistically significant | [49] | |
| Collagenous Colitis | randomized, double-blind, placebo-controlled multicenter trial on 25 patients | 3 × 400 mg Boswellia serrata resin extract (H15™) per day for 6 weeks | Proportion of patients in clinical remission was higher in the Boswellia group compared to placebo group (63.6% vs. 26.7%). No significant difference in histology or quality of life | [50] |
| Bronchial asthma | double-blind, placebo-controlled on 40 patients | 3 × 300 mg Boswellia serrata oleogum resin extract (S-compound™) per day for 6 weeks | Improvement of disease reflected in disappearance of physical symptoms and different signs as well as decrease in eosinophilic count in 70% of the Boswellia group compared to 27% of the placebo group. | [52] |
| Brain tumors | Prospective pilot, randomized, placebo-controlled double-blind study on 44 patients | 3 × 4 × H15 (350 mg Boswellia serrata extract) starting with the first day of radiotherapy | reduction >75% of cerebral edema in 60% of the patients receiving Boswellia compared to 26% of patients in placebo group | [22] |
2.4. Conclusions
- possible role of boswellic acids with too high IC50 values that are not achieved in vivo in providing therapeutic effects
- pharmacokinetic properties of other promising frankincense ingredients i.e., tirucallic, lupeolic and roburic acid
- the influence of other extract ingredients on the pharmacological activity and efficacy
- effect of the pharmacological assays applied and experimental conditions on the outcoming results with regard to pharmacological activity and bioavailability
- the need for more well designed and high quality clinical trials to better underline positive/negative effects already observed
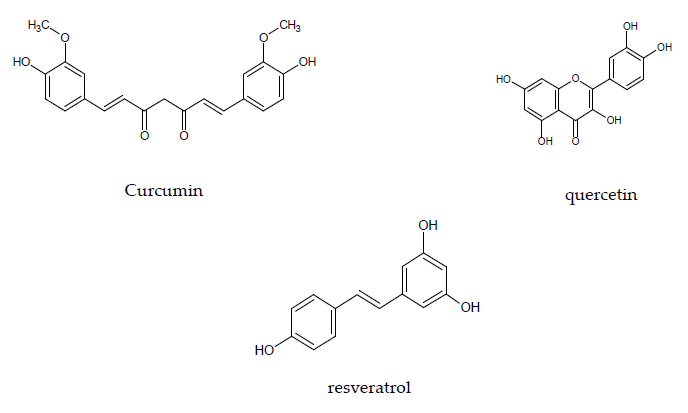
3. Curcumin: In Vitro IC50 Values, Bioavailability and Clinical Efficacy
3.1. In Vitro IC50 Values
3.2. Oral Bioavailability in Human
3.3. Clinical Efficacy
| Disease | No. of Clinical Trials and Patients Included in the Meta-Analysis/Systematic Review | Formulation | Observations | References |
|---|---|---|---|---|
| Primary knee osteoarthritis | Ten RCTs on 1287 participants | Formulations of turmeric or curcumin extract with increased bioavailability as adjunct or mono-therapy compared to placebo for up to maximal 8 months | ↓ pain and ↑ function with reduced incidence of adverse events compared to NSAIDs | [67] |
| Osteoarthritis knee | 16 RCTs on 1810 participants mostly from Asia | All forms of turmeric extracts compared to placebo or actives e.g., NSAID for up to 12 weeks (one study 16 weeks) | ↓ pain and ↑ function compared to placebo and similar to NSAIDs with improved safety profile | [68] |
| Ulcerative colitis (UC) and Crohn’s disease (CD) | 6 RCTs on a total of 374 patients with active mild to moderate UC and one RCT on 30 patients with mild to moderate CD | All forms of curcumin formulations compared to placebo for up to 6 months | Promising results. Two studies with low oral doses reported no significant differences and four with higher doses or better bioavailable curcumin reported significant reduction in clinical symptoms and higher remission rates | [70] |
3.4. Conclusions
- contrasting juxtaposition of achievable plasma concentrations and effective concentrations in vitro for the most targets identified
- possible accumulation of curcumin in plasma following repeated oral administration over long periods of time
- possible accumulation of curcumin in cells, which might lead to effective local concentrations
- possible activation of curcumin conjugates by intracellular glucoronidases or sulfatases
4. Quercetin and Resveratrol: Further Actives with a Lot of Unresolved Questions
4.1. In Vitro Activity
4.2. Oral Bioavailability in Human
4.3. Clinical Efficacy
4.4. Conclusions
- the role of quercetin and resveratrol conjugates as well as the respective parent compounds in the mediation of the pharmacological effects
- possible activation of metabolites by glucuronidases and/or sulfatases in the tissues
- achievable tissue concentrations of the active substances
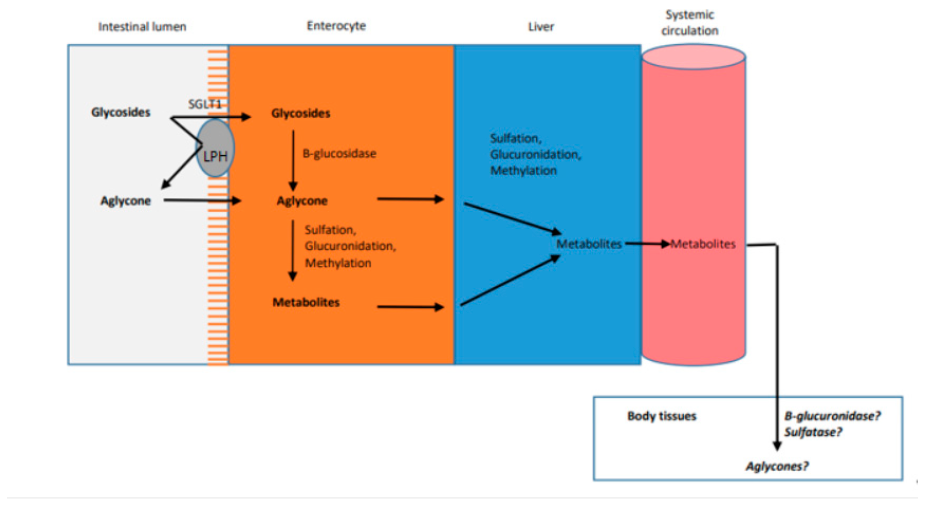
5. Is Tissue Distribution a Better Surrogate Than Plasma Levels?
5.1. What We Know about the Tissue Distribution of Boswellic Acids, Curcumin, Quercetin and Resveratrol
5.2. The Role of Protein-Facilitated Uptake into Tissues
5.3. Role of Tissue β-Glucuronidases and Sulfatases
5.4. Further Examples for the Relevance of Tissue Concentration
5.5. Methods to Determine the Tissue-to-Plasma Ratio
Distribution Dialysis
5.6. Conclusions
6. The Challenges of Complex Multi-Component Herbal Mixtures
6.1. Identification of Combinatory Compounds Attributing to Pharmacological Activity
6.2. Pharmacokinetics of Multicomponent Complex Herbal Mixtures
6.3. Conclusions
7. Other Influence Factors to Be Considered
7.1. Physiological Relevance of In Vitro Assays
7.2. Physiological Relevance of In Vitro Absorption Studies in Cell-Line Based Models
7.3. Future Perspectives
8. Final Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Germolec, D.R.; Shipkowski, K.A.; Frawley, R.P.; Evans, E. Markers of Inflammation. Methods Mol. Biol. 2018, 1803, 57–79. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- Patil, K.R.; Mahajan, U.B.; Unger, B.S.; Goyal, S.N.; Belemkar, S.; Surana, S.J.; Ojha, S.; Patil, C.R. Animal Models of Inflammation for Screening of Anti-inflammatory Drugs: Implications for the Discovery and Development of Phytopharmaceuticals. Int. J. Mol. Sci. 2019, 20, 4367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuerst, R.; Zuendorf, I. Plant derived anti-inflammatory compounds: Hopes and disappointments regarding the translation of preclinical knowledge into clinical progress. Mediators Inflamm. 2014, 2014, 146832. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Zhou, F.; Lu, M.; Ji, W.; Niu, F.; Zha, W.; Wu, X.; Hao, H.; Wang, G. Pharmacokinetics-Pharmacology Disconnection of Herbal Medicines and its Potential Solutions with Cellular Pharmacokinetic-Pharmacodynamic Strategy. Curr. Drug Metab. 2012, 13, 558–576. [Google Scholar] [CrossRef] [PubMed]
- Efferth, T.; Oesch, F. Anti-inflammatory and anti-cancer activities of frankincense: Targets, treatments and toxicities. Semin. Cancer Biol. 2020. [Google Scholar] [CrossRef]
- Herrmann, A.; König, S.; Lechtenberg, M.; Sehlbach, M.; Vakhrushev, S.Y.; Peter-Katalinic, J.; Hensel, A. Proteoglycans from Boswellia serrata Roxb. and B. carterii Birdw. and identfication of a proteolytic plant basic secretory protein. Glycobiology 2019, 22, 1424–1439. [Google Scholar] [CrossRef] [Green Version]
- Ammon, H.P.T. Boswellic Acids and Their Role in Chronic Inflammatory Diseases. Adv. Exp. Med. Biol. 2016, 928, 291–327. [Google Scholar] [CrossRef]
- Roy, N.K.; Parama, D.; Banik, K.; Bordoloi, D.; Devi, A.K.; Thakur, K.K.; Padmavathi, G.; Shakibaei, M.; Fan, L.; Sethi, G.; et al. An Update on Pharmacological Potential of Boswellic Acids against Chronic Diseases. Int. J. Mol. Sci. 2019, 20, 4101. [Google Scholar] [CrossRef] [Green Version]
- Koeberle, A.; Henkel, A.; Verhoff, M.; Tausch, L.; König, S.; Fischer, D.; Kather, N.; Seitz, S.; Paul, M.; Jauch, J.; et al. Triterpene Acids from Frankincense and Semi-Synthetic Derivatives That Inhibit 5-Lipoxygenase and Cathepsin G. Molecules 2018, 23, 506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simoneit, U. Anti-Inflammatory Actions of Boswellic Acids: Identification and Critical Evaluation of Molecular Targets and Signaling Pathways. Ph.D. Thesis, Eberhard Karls University, Tuebingen, Germany, 24 April 2009. [Google Scholar]
- Verhoff, M.; Seitz, S.; Paul, M.; Noha, S.M.; Jauch, J.; Schuster, D.; Werz, O. Tetra- and Pentacyclic Triterpene Acids from the Ancient Anti-inflammatory Remedy Frankincense as Inhibitors of Microsomal Prostaglandin E2Synthase-1. J. Nat. Prod. 2014, 77, 1445–1451. [Google Scholar] [CrossRef]
- Takada, Y.; Ichikawa, H.; Badmaev, V.; Aggarwal, B.B. Acetyl-11-keto-beta-boswellic acid potentiates apoptosis, inibits invasion and abolishes osteoclastogenesis by suppressing NF-kappa B and NF-kappa B regulated gene expression. J. Immunol. 2006, 176, 3127–3140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syrovets, T.; Büchele, B.; Krauss, C.; Laumonier, Y.; Simmet, T. Acetylboswellic acids inhibt lipopolysaccharide-mediated TNF-alpha induction in monocytes by direct interaction with IkappaB kinase. J. Immunol. 2005, 174, 498–506. [Google Scholar] [CrossRef]
- Ammon, H.P.T. Boswellic Acids and Their Role in Chronic Inflammatory Diseases. In Anti-Inflammatory Nutraceuticals and Chronic Diseases. Advances in Experimental Medicine and Biology 928, 1st ed.; Gupta, S.C., Prasad, S., Aggarwal, B.B., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 291–326. [Google Scholar]
- Moussaieff, A.; Shohami, E.; Kashman, Y.; Fride, E.; Schmitz, M.L.; Renner, F.; Fiebich, B.L.; Munoz, E.; Ben-Neriah, Y.; Mechoulam, R. Incensole Acetate, a novel anti-inflammatory compound isoalted from Boswellia resin, inhibits nuclear factor-κB activation. Mol. Pharmacol. 2007, 72, 1657–1664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chevrier, M.R.; Ryan, A.E.; Lee, D.Y.W.; Zhongze, M.; Wu-Yan, Z.; Via, C.S. Boswellia carterii Extract Inhibits TH1 Cytokines and Promotes TH2 Cytokines In Vitro. Clin. Diagn. Lab. Immunol. 2005, 12, 575–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siemoneit, U.; Pergola, C.; Jazzar, B.; Northoff, H.; Skarke, C.; Jauch, J.; Werz, O. On the Interference of Boswellic Acids with 5-lipoxygenase: Mechanistic Studies In Vitro and Pharmcological Relevance. Eur. J. Pharmacol. 2009, 606, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Furtado, N.A.J.C.; Pirson, L.; Edelberg, H.; Miranda, L.M.; Loira-Pastoriza, C.; Preat, V.; Larondelle, Y.; André, C.M. Pentacyclic Triterpene Bioavailability: An Overview of In Vitro and In Vivo Studies. Molecules 2017, 22, 400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerbeth, K.; Meins, J.; Kirste, S.; Momm, F.; Schubert-Zsilavecz, M.; Abdel-Tawab, M. Determination of major boswellic acids in plasma by high-pressure liquid chromatography/mass spectrometry. J. Pharm. Biomed. Anal. 2011, 56, 998–1005. [Google Scholar] [CrossRef] [PubMed]
- Sterk, V.; Büchele, B.; Simmet, T. Effect of Food Intake on the Bioavailability of Boswellic Acids from a Herbal Preparation in Healthy Volunteers. Planta Med. 2004, 70, 1155–1160. [Google Scholar] [CrossRef] [PubMed]
- Kirste, S.; Treier, M.; Wehrle, S.J.; Becker, G.; Abdel-Tawab, M.; Gerbeth, K.; Hug, M.J.; Lubrich, B.; Grosu, A.L.; Momm, F. Boswellia serrata acts on cerebral edema in patients irradiated for brain tumors. Cancer 2011, 117, 3788–3795. [Google Scholar] [CrossRef] [PubMed]
- Buechele, B.; Simmet, T. Analysis of 12 different pentacyclic triterpene acids from frankincense in plasma by high-performance liquid chromatography and photodiode array detection. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2003, 795, 355–362. [Google Scholar] [CrossRef]
- Sharma, T.; Jana, S. Investigation of Molecular Properties that Influence the Permeability and Oral Bioavailability of Major β-Boswellic Acids. Eur. J. Drug Metab. Pharmacokinet. 2019, 45, 243–255. [Google Scholar] [CrossRef] [PubMed]
- Yee, S. In Vitro Permeability across Caco-2 Cells (Colonic) Can Predict In Vivo (Small Intestinal) Absorption in Man: Fact or Myth. Pharm. Res. 1997, 14, 763–766. [Google Scholar] [CrossRef]
- Kruger, P.; Daneshfar, R.; Eckert, G.P.; Klein, J.; Volmer, D.A.; Bahr, U.; Müller, W.E.; Karas, M.; Schubert-Zsilavecz, M.; Abdel-Tawab, M. Metabolism of Boswellic Acids In Vitro and In Vivo. Drug Metab. Dispos. 2008, 36, 1135–1142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerbeth, K.; Hüsch, J.; Fricker, G.; Werz, O.; Schubert-Zsilavecz, M.; Abdel-Tawab, M. In Vitro metabolism, permeation, and brain availability of six major boswellic acids from Boswellia serrata gum resins. Fitoterapia 2013, 84, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Du, Z.; Liu, Z.; Ning, Z.; Liu, Y.; Song, Z.; Wang, C.; Lu, A. Prospects ob boswellic acids as potential pharmaceutics. Planta Med. 2015, 81, 259–271. [Google Scholar]
- Siemoneit, U.; Koeberle, A.; Rossi, A.; Dehm, F.; Verhoff, M.; Reckel, S.; Maier, T.J.; Jauch, J.; Northoff, H.; Bernhard, F.; et al. Inhibition of microsomal prostaglandin E2 synthase-1 as a molecular basis for the anti-inflammatory actions of boswellic acids from frankincense. Br. J. Pharmacol. 2010, 162, 147–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poeckel, D.; Werz, O. Boswellic acids: Biological actions and moelcular targets. Curr. Med. Chem. 2006, 13, 3359–3369. [Google Scholar] [CrossRef]
- Koeberle, A.; Werz, O. Inhibitors of the microsomal prostaglandin E(2) synthase-1 as alternative to non-steroidal anti-inflammatory drugs (NSAIDs): A critical review. Curr. Med. Chem. 2009, 16, 4274–4296. [Google Scholar] [CrossRef]
- Skarke, C.; Kucka, K.; Tausch, L.; Werz, O.; Rossmanith, T.; Barrett, J.S.; Harder, S.; Holtmeier, W.; Schwarz, J.A. Increased bioavailability of 11-keto-beta-boswellic acid following single oral dose frankincense extract administration after a standardized meal in healthy male volunteers: Modeling and simulation considerations for evaluating drug exposures. J. Clin. Pharmacol. 2012, 52, 1592–1600. [Google Scholar]
- Sharma, A.; Gupta, N.K.; Dixit, V.K. Complexation with phosphatidyl choline as a strategy for absorption enhancement of boswellic acid. Drug Deliv. 2010, 17, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Hüsch, J.; Gerbeth, K.; Fricker, G.; Setzer, C.; Zirkel, J.; Rebmann, H.; Schubert-Zsilavecz, M.; Abdel-Tawab, M. Effect of Phospholipid-Based Formulations of Boswellia serrata Extract on the Solubility, Permeability, and Absorption of the Individual Boswellic Acid Constituents Present. J. Nat. Prod. 2012, 75, 1675–1682. [Google Scholar] [CrossRef]
- Hüsch, J.; Bohnet, J.; Fricker, G.; Skarke, C.; Artaria, C.; Appendino, G.; Schubert-Zsilavecz, M.; Abdel-Tawab, M. Enhanced absorption of boswellic acids by a lecithin delivery form (Phytosome®) of Boswellia extract. Fitoterapia 2013, 84, 89–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sengupta, K.; Kolla, J.N.; Krishnaraju, A.V.; Yalamanchili, N.; Rao, C.V.; Golakoti, T.; Raychaudhuri, S.; Raychaudhuri, S.P. Cellular and molecular mechanisms of anti-inflammatory effect of Aflapin: A novel Boswellia serrata extract. Mol. Cell. Biochem. 2011, 354, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Bairwa, K.; Jachak, S.M. Development and optimisation of 3-Acetyl-11-keto-β-boswellic acid loaded poly-lactic-co-glycolic acid-nanoparticles with enhanced oral bioavailability and In Vivo anti-inflammatory activity in rats. J. Pharm. Pharmacol. 2015, 67, 1188–1197. [Google Scholar] [CrossRef] [PubMed]
- Mehta, M.; Satijy, S.; Nanda, A.; Garg, M. Nanotechnolgies for boswellic acids. Am. J. Drug Discov. Dev. 2014, 4, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Meins, J.; Behnam, D.; Abdel-Tawab, M. Enhanced absorption of boswellic acids by a micellar solubilized delivery form of Boswellia extract. NFS J. 2018, 11, 12–16. [Google Scholar] [CrossRef]
- Yu, G.; Xiang, W.; Zhang, T.; Zeng, L.; Yang, K.; Li, J. Effectiveness of Boswellia and Boswellia extract for osteoarthritis patients: A systematic review and meta-analysis. BMC Complement. Med. Ther. 2020, 20, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Majeed, M.; Majeed, S.; Narayanan, N.K.; Nagabhushanam, K. A pilot, randomized, double-blind, placebo-controlled trial to assess the safety and efficacy of a novel Boswellia serrata extract in the management of osteoarthritis of the knee. Phytother. Res. 2019, 33, 1457–1468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vishal, A.A.; Mishra, A.; Raychaudhuri, S.P. A Double Blind, Randomized, Placebo Controlled Clinical Study Evaluates the Early Efficacy of Aflapin® in Subjects with Osteoarthritis of Knee. Int. J. Med. Sci. 2011, 8, 615–622. [Google Scholar] [CrossRef] [Green Version]
- Sengupta, K.; Krishnarju, A.V.; Vishal, A.A.; Mishra, A.; Trimurtulu, G.; Sharma, K.V.S.; Raychaudhuri, S.K.; Raychaudhuri, S.P. Comparative efficacy and tolerability of 5-Loxin and Aflapin against osteoarthritis of the knee: A double blind randomized, placebo controlled clinical study. Int. J. Med. Sci. 2010, 7, 366–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sengupta, K.; Alluri, K.V.; Satish, A.R.; Mishra, S.; Golakoti, T.; Sarma, K.V.; Dey, D.; Raychaudhuri, S.P. A double-blind randomized placebo controlled clinical study of the efficacy of and safety of 5-Loxin for treatment of osteoarthritis of the knee. Arthritis Res. Ther. 2008, 10, R85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimmatkar, N.; Thawani, V.; Hingorani, L.; Khiyani, R. Efficacy and tolerability of Boswellia serrata extract in treatment of osteoarthritis of knee: A randomized double blind placebo controlled trial. Phytomedicine 2003, 10, 3–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sander, O.; Herborn, G.; Rau, R. Is H15 (extract of Boswellia serrata “incense”) an efficient supplementation to established drug therapy of rhemuamtoid arthritis? Results of a double-blind pilot trial. Z. Rheumatol. 1998, 57, 11–16. [Google Scholar] [CrossRef]
- Gupta, I.; Parihar, A.; Malhotra, P.; Singh, G.B.; Lüdtke, R.; Safayhi, H.; Ammon, H.P. Effects of Boswellia serrata gum resin in patients with ulcerative colitis. Eur. J. Med. Res. 1997, 2, 37–43. [Google Scholar]
- Gupta, I.; Parihar, A.; Malhotra, P.; Singh, G.B.; Lüdtke, R.; Safayhi, H.; Ammon, H.P.T. Effects of Boswellia serrata gum resin in patients with chronic colitis. Planta Med. 2001, 67, 391–395. [Google Scholar] [CrossRef]
- Gerhardt, H.; Seifert, F.; Buvari, P.; Vogelsang, H.; Repges, R. Therapy of active Crohn Disease with Boswellis serrata extract H15. Z. Gastroenterol. 2001, 39, 11–17. [Google Scholar] [CrossRef]
- Madisch, A.; Miehlke, S.; Eichele, O.; Mrwa, J.; Bethke, B.; Kuhlisch, E.; Bästlein, E.; Wilhelms, G.; Morgner, A.; Wigginghaus, B.; et al. Boswellia serrata extract for the treatment of collagenous colitis. A double-blind, randomized, placebo-controlled, multicenter trial. Int. J. Color. Dis. 2007, 22, 1445–1451. [Google Scholar] [CrossRef]
- Parian, A.; Limketkai, B.N. Dietary supplement therapies for inflammatory bowel disease: Crohn’s disease and ulcerative colitis. Curr. Pharm. Dis. 2016, 22, 180–188. [Google Scholar] [CrossRef]
- Gupta, I.; Gupta, V.; Parihar, A.; Gupta, S.; Lüdtke, R.; Safayhi, H.; Ammon, H.P. Effects of Boswellia serrata gum resin in patients with bronchial asthma: Results of a double-blind, placebo-controlled, 6-week clinical study. Eur. J. Med. Res. 1998, 3, 511–514. [Google Scholar]
- Streffer, J.; Bitzer, M.; Schabet, M.; Dichgans, J.; Weller, M. Response of radiochemotherapy-associated cerebral edema to a phytotherapeutic agent, H15. Neurology 2001, 56, 1219–1221. [Google Scholar] [CrossRef] [Green Version]
- Boeker, D.K.; Winking, M. The role of boswellic acids in therapy of malignant glioma. Dt. Aerztebl. 1997, 94, 1197–1199. [Google Scholar]
- Adiwidjaja, J.; McLachlan, A.J.; Boddy, A.V. Curcumin as a clinically promising anti-cancer agent: Pharmacokientics and drug interactions. Expert Opin. Drug Metab. Toxicol. 2017, 13, 953–972. [Google Scholar] [CrossRef] [PubMed]
- Fadus, M.C.; Lau, C.; Bikhchandani, J.; Lynch, H.T. Curcumin: An age-old anti-inflammatory and anti-neoplastic agent. J. Tradit. Complement. Med. 2017, 7, 339–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunnumakkara, A.B.; Bordoloi, D.; Padmavathi, G.; Monisha, J.; Roy, N.K.; Prasad, S.; Aggarwal, B.B. Curcumin, the golden nutraceuticaö: Multitargeting for multiple chronic diseases. Br. J. Pharmacol. 2017, 174, 1325–1348. [Google Scholar] [CrossRef] [Green Version]
- Koeberle, A.; Werz, O. Multi-target approach for natural products in inflammation. Drug Discov. Today 2014, 19, 1871–1882. [Google Scholar] [CrossRef] [PubMed]
- Mallo, N.; Lamas, J.; Sueiro, R.A.; Leiro, J.M. Molecular Targets Implicated in the Antiparasitic and Anti-Inflammatory Activity of the Phytochemical Curcumin in Trichomoniasis. Molecules 2020, 25, 5321. [Google Scholar] [CrossRef] [PubMed]
- Koeberle, A.; Northoff, H.; Werz, O. Curcumin blocks prostaglandin E2 biosynthesis through direct inhibition of the microsomal prostaglandin E2 synthase-1. Mol. Cancer Ther. 2009, 8, 2348–2355. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, B.B.; Sung, B. Pharmacological basis for the role of curcumin in chronic diseases: An age-old spice with modern targets. Trends Pharmacol. Sci. 2009, 30, 85–94. [Google Scholar] [CrossRef]
- Cheng, A.L.; Hsu, C.H.; Lin, J.K.; Hsu, M.M.; Ho, Y.F.; Shen, T.S.; Ko, J.Y.; Lin, J.T.; Lin, B.R.; Ming-Shiang, W.; et al. Phase I clinical trial of curcumin, a chemopreventive agent, in patients with high-risk or pre-malignant lesions. Anticancer Res. 2001, 21, 2895–2900. [Google Scholar]
- Vareed, S.K.; Kakarala, M.; Ruffin, M.T.; Crowell, J.A.; Normolle, D.P.; Djuric, Z.; Brenner, D.E. Pharmacokinetics of Curcumin Conjugate Metabolites in Healthy Human Subjects. Cancer Epidemiol. Bimarkers Prev. 2008, 17, 1411–1417. [Google Scholar] [CrossRef] [Green Version]
- Hoehle, S.I.; Pfeiffer, E.; Metzler, M. Glucuronidation of curcuminoids by human microsomal and recombinant UDP-glucuronosyltransferases. Mol. Nutr. Food Res. 2007, 51, 932–938. [Google Scholar] [CrossRef] [PubMed]
- Shoba, G.; Joy, D.; Joseph, T.; Majeed, M.; Rajendran, R.; Srinivas, P.S.S.R. Influence of Piperine on the Pharmacokinetics of Curcumin in Animals and Human Volunteers. Planta Med. 1998, 64, 353–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamwal, R. Bioavailable curcumin formulations: A review of pharmacokinetic studies in healthy volunteers. J. Integr. Med. 2018, 16, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Paultre, K.; Cade, W.; Hernandez, D.; Reynolds, J.; Greif, D.; Best, T.M. Therapeutic effects of turmeric or curcumin extract on pain and function for individuals with knee osteoarthritis: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000935. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Singh, A.; Jones, G.; Winzenberg, T.; Ding, C.; Chopra, A.; Das, S.; Danda, D.; Laslett, L.; Antony, B. Efficacy and Safety of Turmeric Extracts for the Treatment of Knee Osteoarthritis: A Systematic Review and Meta-analysis of Randomised Controlled Trials. Curr. Rheumatol. Rep. 2021, 23, 1–11. [Google Scholar] [CrossRef]
- Chandran, B.; Goel, A. A randomized, pilot study to access the efficacy and safety of curcumin in patients with active rheumatoid arthritis. Phytother. Res. 2012, 26, 1719–1725. [Google Scholar] [CrossRef]
- Goulart, R.D.A.; Barbalho, S.M.; Lima, V.M.; De Souza, G.A.; Matias, J.N.; Araújo, A.C.; Rubira, C.J.; Buchaim, R.L.; Buchaim, D.V.; De Carvalho, A.C.A.; et al. Effects of the Use of Curcumin on Ulcerative Colitis and Crohn’s Disease: A Systematic Review. J. Med. Food 2020. [Google Scholar] [CrossRef]
- Zheng, T.; Wang, X.; Chen, Z.; He, A.; Zheng, Z.; Liu, G. Efficacy of adjuvant curcumin therapy in ulcerative colitis: A meta-analysis of randomized controlled trials. J. Gastroenterol. Hepatol. 2019, 35, 722–729. [Google Scholar] [CrossRef]
- Coelho, M.R.; Romi, M.D.; Ferreira, D.M.T.P.; Zaltman, C.; Soares-Mota, M. The Use of Curcumin as a Complementary Therapy in Ulcerative Colitis: A Systematic Review of Randomized Controlled Clinical Trials. Nutrients 2020, 12, 2296. [Google Scholar] [CrossRef]
- Chandan, S.; Mohan, B.P.; Chandan, O.C.; Ahmad, R.; Tummala, H.; Singh, S.; Dhawan, P.; Singh, A.B. Su1871: Curcumin Use in Ulcerative Colitis—Is It Ready for Prime Time? A Systematic Review and Meta-Analysis of Clinical Trials. Gastroenterology 2019, 156, 53–58. [Google Scholar] [CrossRef]
- Sharma, R.A.; Ireson, C.R.; Verschoyle, R.D.; Hill, K.A.; Williams, M.L.; Leuratti, M.M.; Marnett, L.J.; Steward, W.P.; Gescher, A. Effects of dietary curcumin on glutathione S-transferase and malodialdehyde-DNA adducts in rat liver and colon mucosa. Clin. Cancer Res. 2001, 7, 1452–1458. [Google Scholar] [PubMed]
- Yang, Z.; Liu, W.; Zhou, X.; Zhu, X.; Suo, F.; Yao, S. The effectiveness and safety of curcumin as a complementary therapy in inflammatory bowel disease. Medicine 2020, 99, e22916. [Google Scholar] [CrossRef] [PubMed]
- Tabrizi, R.; Vakili, S.; Akbari, M.; Mirhosseini, N.; Lankarani, K.B.; Rahimi, M.; Mobini, M.; Jafarnejad, S.; Vahedpoor, Z.; Asemi, Z. The effects of curcumin-containing supplements on biomarkers of inflammation and oxidative stress: A systematic review and meta-analysis of randomized controlled trials. Phytother. Res. 2019, 33, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.A.; Euden, S.A.; Platton, S.L.; Cooke, D.N.; Shafayat, A.; Hewitt, H.R.; Marczylo, T.H.; Morgan, B.; Hemingway, D.; Plummer, S.M.; et al. Phase I clinical trial of oral curcumin: Biomarkers of systemic activity and compliance. Clin. Cancer 2004, 10, 6847–6854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Yao, J.; Han, C.; Yang, J.; Chaudhry, M.T.; Wang, S.; Liu, H.; Yin, Y. Quercetin, Inflammation and Immunity. Nutrients 2016, 8, 167. [Google Scholar] [CrossRef]
- Ribeiro, D.; Freitas, M.; Tomé, S.M.; Silva, A.M.S.; Laufer, S.; Lima, J.L.F.C.; Fernandes, E. Flavonoids Inhibit COX-1 and COX-2 Enzymes and Cytokine/Chemokine Production in Human Whole Blood. Inflammation 2014, 38, 858–870. [Google Scholar] [CrossRef] [PubMed]
- Dabeek, W.M.; Marra, M.V. Dietary quercetin and kaempferol: Bioavailability and potential cardiovasular-related bioactivity in humans. Nutrients 2019, 11, 2288. [Google Scholar] [CrossRef] [Green Version]
- Pannu, N.; Bhatnagar, A. Resveratrol: From enhanced biosynthesis and bioavailability to multitargeting chronic diseases. Biomed. Pharmacother. 2019, 109, 2237–2251. [Google Scholar] [CrossRef]
- Wang, P.; Sang, S. Metabolism and pharmacokinetics of resveratrol and pterostilbene. BioFactors 2018, 44, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Walle, T. Bioavailability of resveratrol. Ann. N. Y. Acad. Sci. 2011, 1215, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Brown, V.A.; Patel, K.R.; Viskaduraki, M.; Crowell, J.A.; Perloff, M.; Booth, T.D.; Vasilinin, G.; Sen, A.; Schinas, A.M.; Piccirilli, G.; et al. Repeat Dose Study of the Cancer Chemopreventive Agent Resveratrol in Healthy Volunteers: Safety, Pharmacokinetics, and Effect on the Insulin-like Growth Factor Axis. Cancer Res. 2010, 70, 9003–9011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, S.; Mukai, Y. Modulation of Chronic Inflammation by Quercetin: The Beneficial Effects on Obesity. J. Inflamm. Res. 2020, 13, 421–431. [Google Scholar] [CrossRef] [PubMed]
- Gualdoni, G.A.; Kovarik, J.J.; Hofer, J.; Dose, F.; Pignitter, M.; Doberer, D.; Steinberger, P.; Somoza, V.; Wolzt, M.; Zlabinger, G.J. Resveratrol enhances TNF-α production in human monocytes upon bacterial stimulation. Biochim. Biophys. Acta Gen. Subj. 2014, 1840, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Espinoza, J.L.; Trung, L.Q.; Inaoka, P.T.; Yamada, K.; An, D.T.; Mizuno, S.; Nakao, S.; Takami, A. The Repeated Administration of Resveratrol Has Measurable Effects on Circulating T-Cell Subsets in Humans. Oxid. Med. Cell. Longev. 2017, 2017, 1–10. [Google Scholar] [CrossRef]
- Shi, G.; Hua, M.; Xu, Q.; Ren, T. Resveratrol improves treatment outcome and laboratory parameters in patients with Takayasu arthritis: A randomized double-blind and placebo-controlled clinical trial. Immunobiology 2017, 222, 164–168. [Google Scholar] [CrossRef]
- Samsami-Kor, M.; Daryani, N.E.; Asl, P.R.; Hekmatdoost, A. Anti-Inflammatory Effects of Resveratrol in Patients with Ulcerative Colitis: A Randomized, Double-Blind, Placebo-controlled Pilot Study. Arch. Med. Res. 2015, 46, 280–285. [Google Scholar] [CrossRef]
- Singh, A.P.; Singh, R.; Verma, S.S.; Rai, V.; Kaschula, C.H.; Maiti, P.; Gupta, S.C. Health benefits of resveratrol: Evidence from clinical studies. Med. Res. Rev. 2019, 39, 1851–1891. [Google Scholar] [CrossRef]
- Yoshino, J.; Conte, C.; Fontana, L.; Mittendorfer, B.; Imai, S.I.; Schechtman, K.B.; Gu, C.; Kunz, I.; Fanelli, F.R.; Patterson, B.W.; et al. Resveratrol Supplementation Does Not Improve Metabolic Function in Nonobese Women with Normal Glucose Tolerance. Cell Metab. 2012, 16, 658–664. [Google Scholar] [CrossRef] [Green Version]
- Ramírez-Garza, S.L.; Laveriano-Santos, E.P.; Marhuenda-Muñoz, M.; Storniolo, C.E.; Tresserra-Rimbau, A.; Vallverdú-Queralt, A.; Lamuela-Raventós, R.M. Health Effects of Resveratrol: Results from Human Intervention Trials. Nutrients 2018, 10, 1892. [Google Scholar] [CrossRef] [Green Version]
- López-Yerena, A.; Perez, M.; Vallverdú-Queralt, A.; Escribano-Ferrer, E. Insights into the Binding of Dietary Phenolic Compounds to Human Serum Albumin and Food-Drug Interactions. Pharmaceutics 2020, 12, 1123. [Google Scholar] [CrossRef] [PubMed]
- Batiha, G.E.S.; Beshbishy, A.M.; Ikram, M.; Mulla, Z.S.; El-Hack, M.E.A.; Taha, A.E.; Algammal, A.M.; Elewa, Y.H.A. The Pharmacological Activity, Biochemical Properties, and Pharmacokinetics of the Major Natural Polyphenolic Flavonoid: Quercetin. Foods 2020, 9, 374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paulke, A.; Eckert, G.P.; Schubert-Zsilavecz, M. Isoquercetin provides better bioavailability than quercetin: Comparison of quercetin metabolites in body tissue and brain sections after six-day administraiton of isoquercetin and quercetin. Pharmazie 2012, 67, 991–996. [Google Scholar] [PubMed]
- El-Mohsen, M.A.; Bayele, H.; Kuhnle, G.; Gibson, G.; Debnam, E.; Srai, S.K.; Rice-Evans, C.; Spencer, J.P.E. Distribution of [H]trans-resveratrol in rat tissues following oral administration. Br. J. Nutr. 2006, 96, 62–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Yu, X.; Zhang, L.; Wang, L.; Peng, Z.; Chen, Y. The pharmacokinetics and tissue distribution of curcumin and its metabolites in mice. Biomed. Chromatogr. 2018, 32, e4267. [Google Scholar] [CrossRef] [PubMed]
- Bangphumi, K.; Kittiviriyakul, C.; Towiwat, P.; Rojsitthisak, P.; Khemawoot, P. Pharmacokinetics of Curcumin Diethyl Disuccinate, a Prodrug of Curcumin, in Wistar Rats. Eur. J. Drug Metab. Pharmacokinet. 2015, 41, 777–785. [Google Scholar] [CrossRef]
- Begum, A.N.; Jones, M.R.; Lim, G.P.; Morihara, T.; Kim, P.; Heath, D.D.; Rock, C.L.; Pruitt, M.A.; Yang, F.; Hudspeth, B.; et al. Curcumin Structure-Function, Bioavailability, and Efficacy in Models of Neuroinflammation and Alzheimer’s Disease. J. Pharmacol. Exp. Ther. 2008, 326, 196–208. [Google Scholar] [CrossRef] [Green Version]
- Cas, M.D.; Ghidoni, R. Dietary Curcumin: Correlation between Bioavailability and Health Potential. Nutrients 2019, 11, 2147. [Google Scholar] [CrossRef] [Green Version]
- Bowman, C.M.; Benet, L.Z. An exaination of protein binding and protein-facilitated uptake relating to in vitro-in vivo extrapolation. Eur. J. Pharm. Sci. 2018, 123, 502–514. [Google Scholar] [CrossRef]
- Poulin, P.; Haddad, S. Albumin and uptake of drugs in cells: Additional validation excercises of a recently published equation that quantifies the albumin-facilitated uptake mechanism(s) in physiologically based pharmacokinetic and pharmacodynamic modeling research. J. Pharm. Sci. 2015, 104, 4448–4458. [Google Scholar] [CrossRef]
- Poulin, P.; Burczynski, F.J.; Haddad, S. The role of extracellular binding proteins in the cellular uptake of drugs: Impact on quantitative in-vitro-in-vivo extrapolations of toxicity and efficacy in physiologically based pharmacokinetic-pharmacodynamic research. J. Phar. Sci. 2016, 105, 497–508. [Google Scholar] [CrossRef] [Green Version]
- Giacomini, K.M.; Huang, S.M.; Twedie, D.J.; Benet, L.Z.; Brouwer, K.I.; Chu, X.; Dahlin, A.; Evers, R.; Fischer, V.; Hillgren, K.M.; et al. Membrane transporters in drug development. Nat. Rev. Drug Discov. 2010, 9, 215–236. [Google Scholar] [PubMed]
- Neves, A.R.; Lucio, M.; Lima, J.L.; Reis, S. Resveratrol in Medicinal Chemistry: A Critical Review of its Pharmacokinetics, Drug-Delivery, and Membrane Interactions. Curr. Med. Chem. 2012, 19, 1663–1681. [Google Scholar] [CrossRef]
- Wanat, K. Biological barriers, and the influence of protein binding on the passage of drugs across them. Mol. Biol. Rep. 2020, 47, 3221–3231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, H.; Mizojiri, K. Drug-preotein binding and blood-brain barrier permeability. J. Pharmacol. Ther. 1999, 288, 912–918. [Google Scholar]
- Heymans, M.; Sevin, E.; Gosselet, F.; Lundquist, S.; Culot, M. Mimicking brain tissue binding in an in vitro model of the blood-brain barrier illustrates differences between in vitro and in vivo methods for assessing the rate of brain penetration. Eur. J. Pharm. Biopharm. 2018, 127, 453–461. [Google Scholar] [CrossRef]
- Böhmdorfer, M.; Szakmary, A.; Schiestl, R.H.; Vaquero, J.; Riha, J.; Brenner, S.; Thalhammer, T.; Szekeres, T.; Jäger, W. Involvement of UDP-Glucuronyltransferases and sulfotansferases in the excretion and tissue distribution of resveratrol in mice. Nutrients 2017, 9, 1347. [Google Scholar] [CrossRef] [Green Version]
- Kunihiro, A.G.; Brickey, J.A.; Frye, J.B.; Luis, P.B.; Schneider, C.; Funk, J.L. Curcumin, but not curcumin-glucuronide, inhibits Smad signaling in TGFβ-dependent bone metastatic breast cancer cells and is enriched in bone compared to other tissues. J. Nutr. Biochem. 2019, 63, 150–156. [Google Scholar] [CrossRef]
- Shimoi, K.; Nakayama, T. Glucuronidase Deconjugation in Inflammation. Methods Enzymol. 2005, 400, 263–272. [Google Scholar] [CrossRef]
- O’Leary, K.A.; Day, A.J.; Needs, P.W.; Sly, W.S.; O’Brien, N.M.; Williamson, G. Flavonoid glucuronides are substrates for human liver beta-glucuronidase. FEBS Lett. 2001, 503, 103–106. [Google Scholar] [CrossRef] [Green Version]
- Bieger, J.; Cermak, R.; Blank, R.; De Boer, V.C.J.; Hollman, P.C.H.; Kamphues, J.; Wolffram, S. Tissue Distribution of Quercetin in Pigs after Long-Term Dietary Supplementation. J. Nutr. 2008, 138, 1417–1420. [Google Scholar] [CrossRef]
- Ishisaka, A.; Kawabata, K.; Miki, S.; Shiba, Y.; Minekawa, S.; Nishikawa, T.; Mukai, R.; Terao, J.; Kawai, Y. Mitochondrial Dysfunction Leads to Deconjugation of Quercetin Glucuronides in Inflammatory Macrophages. PLoS ONE 2013, 8, e80843. [Google Scholar] [CrossRef] [Green Version]
- Galindo, P.; Rodríguez-Gómez, I.; González-Manzano, S.; Dueñas, M.; Jiménez, R.; Menéndez, C.; Vargas, F.; Tamargo, J.; Santos-Buelga, C.; Perez-Vizcaino, F.; et al. Glucuronidated Quercetin Lowers Blood Pressure in Spontaneously Hypertensive Rats via Deconjugation. PLoS ONE 2012, 7, e32673. [Google Scholar] [CrossRef] [Green Version]
- Menéndez, C.; Dueñas, M.; Galindo, P.; González-Menzano, S.; Jiménez, R.; Moreno, L.; Zarzuelo, M.J.; Rodriguez-Gómez, I.; Duarte, J.; Santos-Buelga, C.; et al. Vascular deconjugation of quercetin glucuronide: The flavonoid paradox revealed? Mol. Nutr. Food Res. 2011, 55, 1780–1790. [Google Scholar] [CrossRef] [PubMed]
- Slominski, A.T.; Semak, I.; Fischer, T.W.; Kim, T.K.; Kleszcynski, K.; Hardeland, R.; Reiter, R.J. Metabolism of melatonin in the skin: Why is it important? Exp. Dermatol. 2017, 26, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Slominski, A.T.; Zmijewski, M.A.; Semak, I.; Kim, T.-K.; Janjetovic, Z.; Slominski, R.M.; Zmijewski, J.W. Melatonin, mitochondria, and the skin. Cell. Mol. Life Sci. 2017, 74, 3913–3925. [Google Scholar] [CrossRef] [PubMed]
- Slominski, A.T.; Chaiprasongsuk, A.; Janjetovic, Z.; Kim, T.-K.; Stefan, J.; Slominski, R.M.; Hanumanthu, V.S.; Raman, C.; Qayyum, S.; Song, Y.; et al. Photoprotective Properties of Vitamin D and Lumisterol Hydroxyderivatives. Cell Biophys. 2020, 78, 165–180. [Google Scholar] [CrossRef] [PubMed]
- Slominski, A.T.; Li, W.; Kim, T.K.; Semak, I.; Wang, J.; Zjawiony, J.K.; Tuckey, R.C. Novel activities of CYP11A1 and their potential physiological significance. J. Steroid Biochem. Mol. Biol. 2015, 151, 25–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bickel, M.H.; Gerny, R. Drug distribution as a function of binding competetion. Experiments with the distribution dialysis technique. J. Pharm. Pharmacol. 1980, 32, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Clausen, J.; Bickel, M.H. Prediction of drug distribution in distribution dialysis and in vivo from binding to tissues and blood. J. Pharm. Sci. 1993, 82, 345–349. [Google Scholar] [CrossRef]
- Rizk, M.L.; Zou, L.; Savic, R.M.; E Dooley, K. Importance of Drug Pharmacokinetics at the Site of Action. Clin. Transl. Sci. 2017, 10, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Holt, K.; Ye, M.; Nagar, S.; Korzekwa, K. Prediction of tissue-plasma partition coefficients using microsomal partitioning: Incorporation into physiolgically based pharmacokientic models and steady-state volume of distribution predictions. Drug Met. Dispos. 2019, 47, 1050–1060. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.S.; Chang, J.H.; Flores, M.; Brecht, E. Evaluation of a competetive equilibrium dialysis approach for assessing the impact of protein binding on clearance prediction. J. Pharm. Sci. 2021, 110, 536–542. [Google Scholar] [CrossRef]
- Long, F.; Yang, H.; Xu, Y.; Hao, H.; Li, P. A strategy for the identification of combinatorial bioactive compounds contributing to the holistic effect of herbal medicines. Sci. Rep. 2015, 5, 12361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, P.; Yang, H.; Long, F.; Hao, H.P.; Xu, X.; Liu, Y.; Shi, X.W.; Zhang, D.D.; Zheng, H.C.; Wen, Q.Y.; et al. Bioactive Equivalence of Combinatorial Components Identified in Screening of an Herbal Medicine. Pharm. Res. 2014, 31, 1788–1800. [Google Scholar] [CrossRef] [Green Version]
- Zhuo, R.; Liu, H.; Liu, N.; Wang, Y. Ligand Fishing: A Remarkable Strategy for Discovering Bioactive Compounds from Complex Mixture of Natural Products. Molecules 2016, 21, 1516. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Liang, H.; Cao, H.; Zhang, B.; Li, J.; Wang, W.; Qin, S.; Wang, Y.; Xuan, L.; Lai, L.; et al. Efficient ligand siecovery from natural herbs by integrating virtual screening, affinity mass spectrometry and targeted metabolomics. Analyst 2019, 144, 2881–2890. [Google Scholar] [CrossRef]
- Heinrich, M.; Lardos, A.; Leonti, M.; Weckerle, C.; Willcox, M.; Applequist, W.; Ladio, A.; Long, C.L.; Mukherjee, P.; Stafford, G. Best practice in research: Consensus Statement on Ethnopharmacological Field Studies—ConSEFS. J. Ethnopharmacol. 2018, 211, 329–339. [Google Scholar] [CrossRef] [Green Version]
- Heinrich, M.; Appendino, G.; Efferth, T.; Fürst, R.; Izzo, A.A.; Kayser, O.; Pezzuto, J.M.; Viljoen, A. Best practice in research: Overcoming common challenges in phytopharmacological research. J. Ethnopharmacol. 2020, 246, 112230. [Google Scholar] [CrossRef]
- Lan, K.; Xie, G.; Jia, W. Towards Polypharmacokinetics: Pharmacokinetics of Multicomponent Drugs and Herbal Medicines Using a Metabolomics Approach. Evid. Based Complement. Altern. Med. 2013, 2013, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Lan, K.; Jia, W. An integrated metabolomics and pharmacokinetics strategy for multi-component drugs evaluation. Curr. Drug Met. 2010, 11, 105–114. [Google Scholar]
- Plumb, R.S.; Stumpf, C.L.; Granger, J.H.; Catro-Perez, J.; Haselden, J.N.; Dear, G.J. Use of liquid chromatography/time-offlight mass spectrometry and multivariate statistical analysis shows promise for the detection of drug metabolites in biological fluids. Rapid Commun. Mass Spectrom. 2003, 17, 2632–2638. [Google Scholar] [CrossRef]
- Wang, X.J.; Ren, J.L.; Zhang, A.H.; Sun, H.; Yan, G.L.; Han, Y.; Liu, L. Novel applications of masspectrometry-based metabolomics in herbal medicines and its active ingredients: Current evidence. Mass Spectrom. Rev. 2019, 38, 380–402. [Google Scholar] [CrossRef] [PubMed]
- Guijas, C.; Montenegro-Burke, J.R.; Warth, B.; E Spilker, M.; Siuzdak, G. Metabolomics activity screening for identifying metabolites that modulate phenotype. Nat. Biotechnol. 2018, 36, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Xie, G.; Wang, S.; Zhang, H.; Zhao, A.; Liu, J.; Ma, Y.; Lan, K.; Ni, Y.; Liu, C.; Liu, P.; et al. Poly-pharmacokinetic Study of a Multicomponent Herbal Medicine in Healthy Chinese Volunteers. Clin. Pharmacol. Ther. 2018, 103, 692–702. [Google Scholar] [CrossRef] [PubMed]
- Markus, J.; Landry, T.; Stevens, Z.; Scott, H.; Llanos, P.; Debatis, M.; Armento, A.; Klausner, M.; Ayehunie, S. Human small intestinal organotypic culture model for drug permeation, inflammation, and toxicity assays. Vitr. Cell. Dev. Biol. Anim. 2021, 57, 160–173. [Google Scholar] [CrossRef]
- Srinivasan, B.; Kolli, A.R.; Esch, M.B.; Abaci, H.E.; Shuler, M.L.; Hickman, J.J. TEER Measurement Techniques for In Vitro Barrier Model Systems. J. Lab. Autom. 2015, 20, 107–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, J.; Ahluwalia, A. Advances and Current Challenges in Intestinal in vitro Model Engineering: A Digest. Front. Bioeng. Biotechnol. 2019, 7, 144. [Google Scholar] [CrossRef] [Green Version]
- Summerfield, S.G.; Read, K.; Begley, D.J.; Obradovic, T.; Hidalgo, I.J.; Coggon, S.; Lewis, A.V.; Porter, R.A.; Jeffrey, P. Central Nervous System Drug Disposition: The Relationship between in Situ Brain Permeability and Brain Free Fraction. J. Pharmacol. Exp. Ther. 2007, 322, 205–213. [Google Scholar] [CrossRef] [Green Version]
- Nam, K.H.; Smith, A.C.T.; Lone, S.; Kwon, S.; Kim, D.H. Biomimetic three-dimensional models for advanced high-throughput drug screening. J. Lab. Autom. 2015, 20, 201–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]






| Dosage of Boswellia Extract | Concentrations of Boswellic Acids in Plasma [µM] | Ref. | |||||
|---|---|---|---|---|---|---|---|
| KBA | AKBA | βBA | AβBA | αBA | AαBA | ||
| 3 × 4 capsules à 350 mg/day for 1 week (n = 14) (in total: KBA 63.6 mg, AKBA 80,4 mg, βBA 2236.8 mg, AβBA 228 mg, αBA 969.6 mg, AαBA 73.2 mg) | 0.01–0.52 | 0–0.03 | 0.19–26.20 | 0.26–12.31 | 0.08–10.59 | 0.14–5.99 | [20] |
| 3 × 282 mg/day—fasted state | 0.17 [0.05–0.52] | 0.01 [0.002–0.08] | 0.4 [0.10–3.9] | ND | ND | ND | [21] |
| 3 × 282 mg/day—fed state (n = 12) (in total: KBA 48.12 mg, AKBA 28.71 mg, βBA 143.4 mg, AβBA 82.71 mg, αBA 103.71 mg, AαBA 26.25 mg) | 0.48 [0.21–0.9] | 0.06 [0.03–0.52] | 2.5 [0.91–4.7] | ND in most subjects | 0.69 [0.1–2.9] | 0.24 [0.09–0.8] | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdel-Tawab, M. Considerations to Be Taken When Carrying Out Medicinal Plant Research—What We Learn from an Insight into the IC50 Values, Bioavailability and Clinical Efficacy of Exemplary Anti-Inflammatory Herbal Components. Pharmaceuticals 2021, 14, 437. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14050437
Abdel-Tawab M. Considerations to Be Taken When Carrying Out Medicinal Plant Research—What We Learn from an Insight into the IC50 Values, Bioavailability and Clinical Efficacy of Exemplary Anti-Inflammatory Herbal Components. Pharmaceuticals. 2021; 14(5):437. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14050437
Chicago/Turabian StyleAbdel-Tawab, Mona. 2021. "Considerations to Be Taken When Carrying Out Medicinal Plant Research—What We Learn from an Insight into the IC50 Values, Bioavailability and Clinical Efficacy of Exemplary Anti-Inflammatory Herbal Components" Pharmaceuticals 14, no. 5: 437. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14050437