
In Vitro Time-Kill of Common Ocular Pathogens with Besifloxacin Alone and in Combination with Benzalkonium Chloride

1
Clinical Microbiology, Royal University Hospital, Saskatoon, SK S7N 0W8, Canada
2
Bausch + Lomb, Rochester, NY 14609, USA
*
Author to whom correspondence should be addressed.
Pharmaceuticals 2021, 14(6), 517; https://0-doi-org.brum.beds.ac.uk/10.3390/ph14060517
Submission received: 30 April 2021
/
Revised: 17 May 2021
/
Accepted: 20 May 2021
/
Published: 27 May 2021
(This article belongs to the Special Issue Mechanisms of Antibiotic Action and Resistance)
Abstract
:Background: Besifloxacin ophthalmic suspension 0.6% (w/v%) contains benzalkonium chloride (BAK) as a preservative. We evaluated the in vitro time-kill activity of besifloxacin, alone and in combination with BAK, against common bacteria implicated in ophthalmic infections. Methods: The activity of besifloxacin (100 µg/mL), BAK (10, 15, 20, and 100 µg/mL), and combinations of besifloxacin and BAK were evaluated against isolates of Staphylococcus epidermidis (n = 4), Staphylococcus aureus (n = 3), Haemophilus influenzae (n = 2), and Pseudomonas aeruginosa (n = 2) in time-kill experiments of 180 min duration. With the exception of one S. aureus isolate, all of the staphylococcal isolates were methicillin- and/or ciprofloxacin-resistant; one P. aeruginosa isolate was ciprofloxacin-resistant. The reductions in the viable colony counts (log10 CFU/mL) were plotted against time, and the differences among the time–kill curves were evaluated using an analysis of variance. Areas-under-the-killing-curve (AUKCs) were also computed. Results: Besifloxacin alone demonstrated ≥3-log killing of P. aeruginosa (<5 min) and H. influenzae (<120 min), and approached 3-log kills of S. aureus. BAK alone demonstrated concentration-dependent killing of S. epidermidis, S. aureus and H. influenzae, and at 100 µg/mL produced ≥3-log kills in <5 min against these species. The addition of BAK (10, 15, and 20 µg/mL) to besifloxacin increased the rate of killing compared to besifloxacin alone, with earlier 3-log kills of all species except P. aeruginosa and a variable impact on S. aureus. The greatest reductions in AUKC were observed among H. influenzae (8-fold) and S. epidermidis (≥5-fold). Similar results were found when the isolates were evaluated individually by their resistance phenotype. Conclusions: In addition to confirming the activity of 100 µg/mL BAK as a preservative in the bottle, these data suggest that BAK may help besifloxacin to achieve faster time-kills on-eye in the immediate timeframe post-instillation before extensive dilution against bacterial species implicated in ophthalmic infections, including drug-resistant S. epidermidis. Greater killing activity may help prevent resistance development and/or help treat resistant organisms.
1. Introduction
Fluoroquinolones are broad-spectrum, bactericidal antibiotics that inhibit DNA synthesis through dual actions on the bacterial enzymes DNA gyrase (topoisomerase II) and topoisomerase IV [1]. Besifloxacin is a chlorinated fluoroquinolone introduced into clinical practice in the US in 2009, and is available worldwide including in Canada, Australia, and several Latin American, Middle Eastern, African, and Asian countries. Unlike other fluoroquinolones, besifloxacin was developed and formulated solely for topical ocular administration and is indicated in the US for the treatment of bacterial conjunctivitis [2]. Studies have shown that the minimum inhibitory concentration (MIC) values for besifloxacin against Gram-positive pathogens are consistently lower, by at least two to three dilutions, than those for moxifloxacin and gatifloxacin against the same isolates [3,4,5], and that besifloxacin was also the most rapidly bactericidal [6]. Besifloxacin ophthalmic suspension 0.6% (Besivance®, Bausch + Lomb) has been studied clinically for the treatment of bacterial conjunctivitis [7,8,9,10,11,12,13,14] and other potential uses [15,16,17,18,19].
The marketed formulation of besifloxacin includes the drug at a concentration of 6 mg/mL (0.6%) and the preservative benzalkonium chloride (BAK) at a concentration of 100 µg/mL (0.01%) [2]. The quaternary ammonium compound BAK is the most widely used preservative in ophthalmic medications and has been shown to have antimicrobial activity of its own. BAK is a detergent preservative and interacts with lipid components of the bacterial cell membrane leading to membrane destabilization, release of cell contents, and ultimately cell death [20]. BAK has demonstrated significant in vitro antimicrobial activity against common Gram-positive cocci such as Staphylococcus aureus and Staphylococcus epidermidis, but much less so on Gram-negative rods such as Pseudomonas aeruginosa [21,22]. In vehicle-controlled clinical conjunctivitis studies, 0.6% besifloxacin ophthalmic suspension containing 0.01% BAK was statistically superior to vehicle alone with respect to both clinical and microbiological resolution at almost every follow up visit; however, a percentage of subjects using only vehicle, which contained BAK, also achieved successful outcomes [7,8,10]. While bacterial conjunctivitis is typically self-resolving given enough time [23], these findings suggest that BAK may contribute to microbial resolution in vehicle-treated subjects and may enhance microbial resolution with besifloxacin in the marketed formulation.
Our laboratory (JB) previously found MIC values of ≤3.1 µg/mL when BAK was tested against isolates of methicillin-susceptible S. aureus (MSSA) [24], methicillin-resistant S. aureus (MRSA) [24,25], and coagulase-negative staphylococci (CoNS) [24]. Additionally, when gatifloxacin or moxifloxacin was tested in vitro in combination with varying concentrations of BAK against these pathogens, the MIC values were multiple-fold lower (all ≤0.008 µg/mL) compared to the MIC values for the fluoroquinolone agents alone [24,25].
MIC data are useful in comparing the potency of antibacterial agents to one another against a specific pathogenic organism. However, given concerns about increasing bacterial resistance and mutant bacteria selection, the potential of a drug or combination of drugs to completely eradicate an organism, which is referred to as kill data, can provide information that is perhaps more relevant. In the current study, in vitro time-kill studies were performed to compare the activity of besifloxacin alone, BAK alone at increasing concentrations, and the combination of besifloxacin and BAK against common ophthalmic Gram-positive and Gram-negative pathogens implicated in ocular infections, including isolates with varying antibacterial resistance profiles.
2. Results
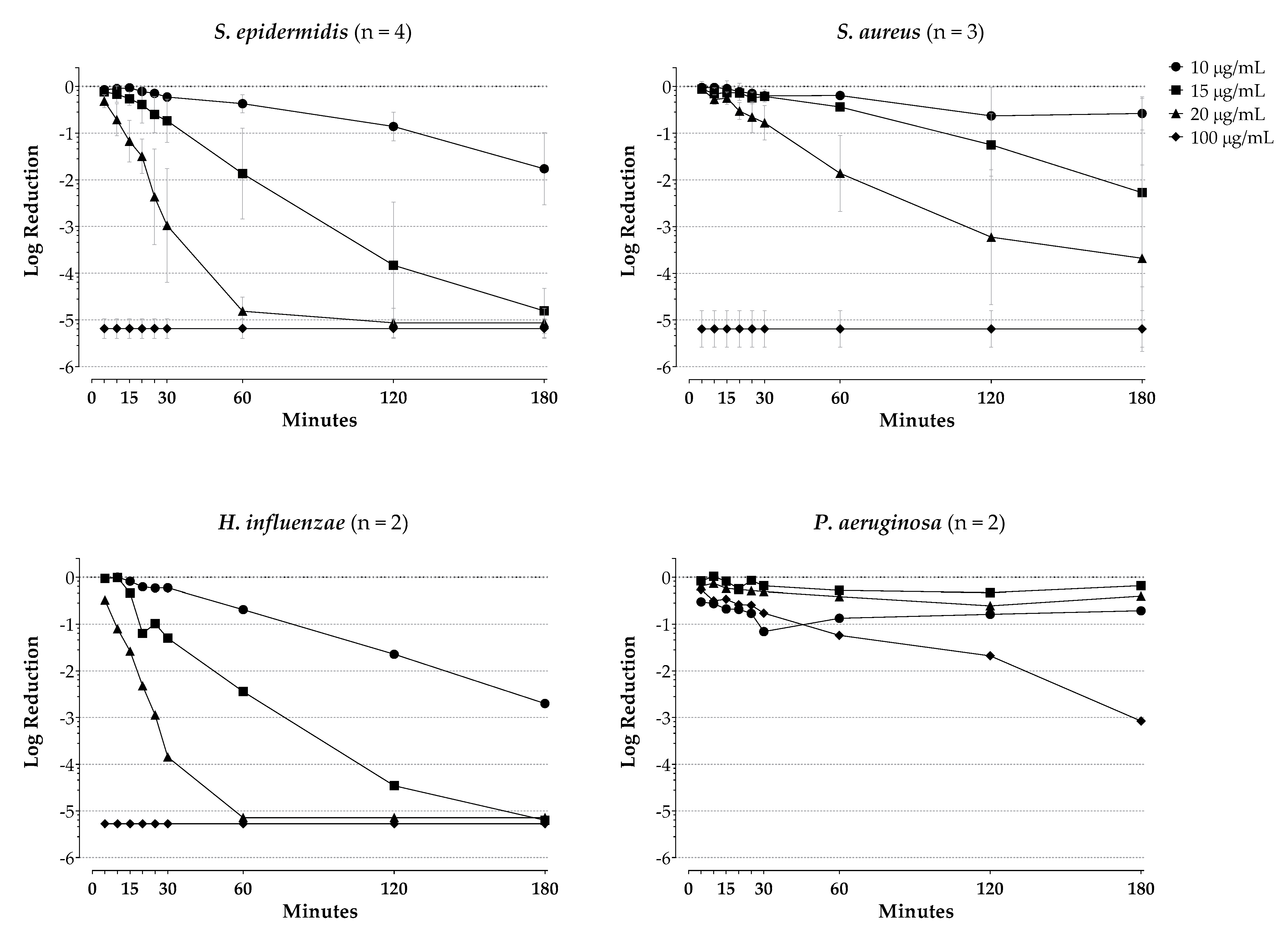
Figure 1 presents the log reductions in viable cell counts (CFU/mL) of S. epidermidis, S. aureus, H. influenzae, and P. aeruginosa following incubation with BAK alone over 180 min. BAK demonstrated concentration-dependent killing of S. epidermidis, H. influenzae, and S. aureus. At the highest concentration tested (100 µg/mL), BAK produced a >5-log kill within 5 min against S. epidermidis, S. aureus, and H. influenzae. As expected, BAK did not demonstrate robust killing activity against P. aeruginosa, although a ≥3-log kill was seen with the highest concentration of BAK, but only after 180 min incubation.
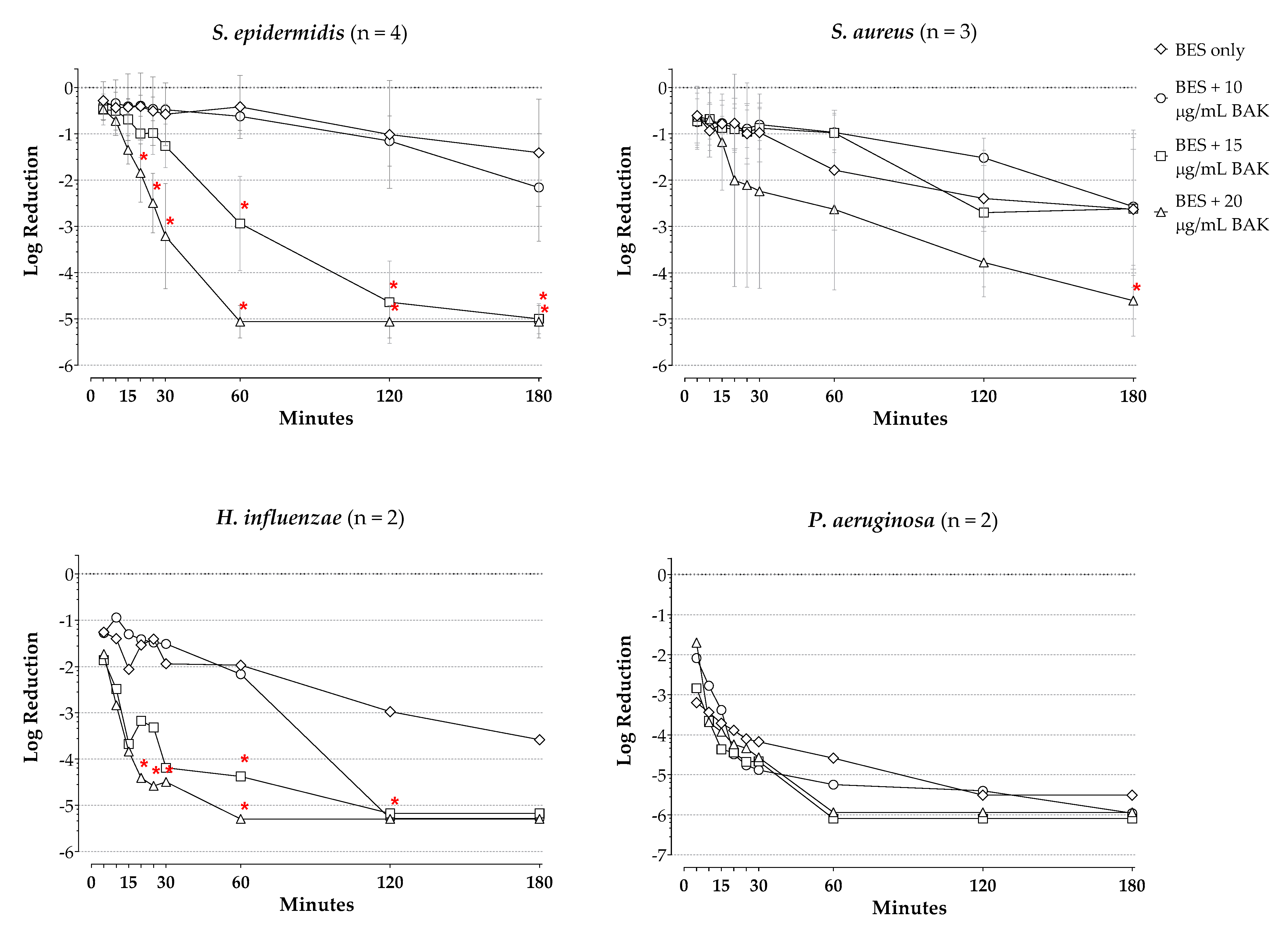
Figure 2 presents log reductions in viable counts for besifloxacin alone at 100 µg/mL and in combination with increasing concentrations of BAK (10 µg/mL, 15 µg/mL, 20 µg/mL) for each species (average of isolates thereof) tested over 180 min. The corresponding log reductions at the final timepoint are presented in Table 1. Results of the ANOVA of kill curves, excluding those with BAK at 100 µg/mL, indicated a significant effect of test agent (i.e., besifloxacin and/or BAK) on kill curves for S. epidermidis, H. influenzae, and P. aeruginosa (p ≤ 0.0092), as well as a significant effect of time and interaction of time with test agent for all four species (p ≤ 0.0157).
With 100 µg/mL besifloxacin alone, a 0.3-log reduction was seen in viable S. epidermidis organisms following 5 min of drug exposure, increasing to a 1.4-log reduction at 180 min of drug exposure (Figure 2). While the addition of BAK at 10 µg/mL provided no additional killing of S. epidermidis organisms, the addition of BAK at 15 µg/mL and BAK at 20 µg/mL increased the killing, resulting in 3-log reductions in viable S. epidermidis organisms by about 60 min for the combination of besifloxacin and 15 µg/mL BAK, and in less than 30 min for the combination of besifloxacin and 20 µg/mL BAK. The addition of BAK at 15 and at 20 µg/mL to besifloxacin significantly increased the bacterial killing of S. epidermidis compared to that with besifloxacin alone at the timepoints 60 min and 20 min onward, respectively (p ≤ 0.003). The corresponding AUKC for the combination of besifloxacin and BAK at 15 µg/mL and besifloxacin and 20 µg/mL BAK were decreased 2.5- and 5.6-fold from the AUKC for besifloxacin alone. Comparison of kill curves for BAK alone compared to besifloxacin alone showed a significant difference at the timepoints 60 min and 20 min onward for BAK at 15 and BAK at 20 µg/mL, respectively (p ≤ 0.049, data not shown), with greater activity for BAK at these concentrations vs besifloxacin alone at these timepoints.
Against S. aureus, 100 µg/mL besifloxacin alone produced a 0.6-log reduction in viable organisms after 5 min of drug exposure, increasing to a 2.6-log reduction after 180 min of drug exposure. While the addition of BAK at 10 µg/mL or at 15 µg/mL to besifloxacin had no effect on log reductions of viable S. aureus organisms compared to those observed with besifloxacin alone, the addition of BAK at 20 µg/mL to besifloxacin produced a 3-log reduction in viable S. aureus organisms by roughly 80 min and a significantly increased bacterial kill at the 180 min timepoint on the kill curve for the combination compared to besifloxacin alone (p = 0.0358). The corresponding AUKC for the combination was also decreased 1.6-fold from that with besifloxacin alone. Comparison of the kill curve of 100 µg/mL besifloxacin alone to kill curves of BAK alone showed a significant difference to that of BAK at 10 µg/mL at the 180 min timepoint (p = 0.0275; data not shown), with significantly greater activity of besifloxacin alone vs BAK at 10 µg/mL.
Against H. influenzae, besifloxacin alone at 100 µg/mL produced a 1.3-log reduction in viable counts by 5 min of exposure, increasing to a 3.0-log reduction by 120 min of exposure. The addition of BAK at 15 µg/mL or 20 µg/mL to besifloxacin resulted in 3-log reductions in viable H. influenzae organisms in just over 10 min for both combinations. Furthermore, the addition of 15 µg/mL BAK to besifloxacin produced significantly increased bacterial killing of H. influenzae at the 60-min timepoint (p = 0.0320), while the addition of 20 µg/mL BAK to besifloxacin produced significantly increased bacterial killing of H. influenzae at timepoints from 20 min to 120 min compared to besifloxacin alone (p ≤ 0.0412). The AUKC for besifloxacin combined with 15 µg/mL BAK or combined with 20 µg/mL BAK were decreased 4.4- and 8.2-fold from that with besifloxacin alone. Comparison of the kill curve of 100 µg/mL besifloxacin alone to the kill curves of BAK alone showed a significant difference to that of BAK at 20 µg/mL at the 60-min timepoint (p = 0.0024; data not shown), with greater killing activity for BAK.
A 3.2-log reduction in viable cell counts of P. aeruginosa was observed with 100 µg/mL besifloxacin as early as 5 min of exposure, increasing to a 5.5-log reduction at 180 min. No significant increases in the reduction of viable cell counts of P. aeruginosa were observed with the addition of BAK at any concentration to besifloxacin compared to besifloxacin alone at any timepoint. Likewise, the AUKCs for besifloxacin in combination with BAK at 10 µg/mL, 15 µg/mL, and 20 µg/mL were not reduced compared to that of besifloxacin alone. Notably, 100 µg/mL besifloxacin alone was significantly more active than BAK alone at 10 µg/mL, 15 µg/mL, and 20 µg/mL at all timepoints of the kill curve (p ≤ 0.0400; data not shown), and besifloxacin’s AUKC was reduced by approximately 9-fold from those with BAK alone at those concentrations.
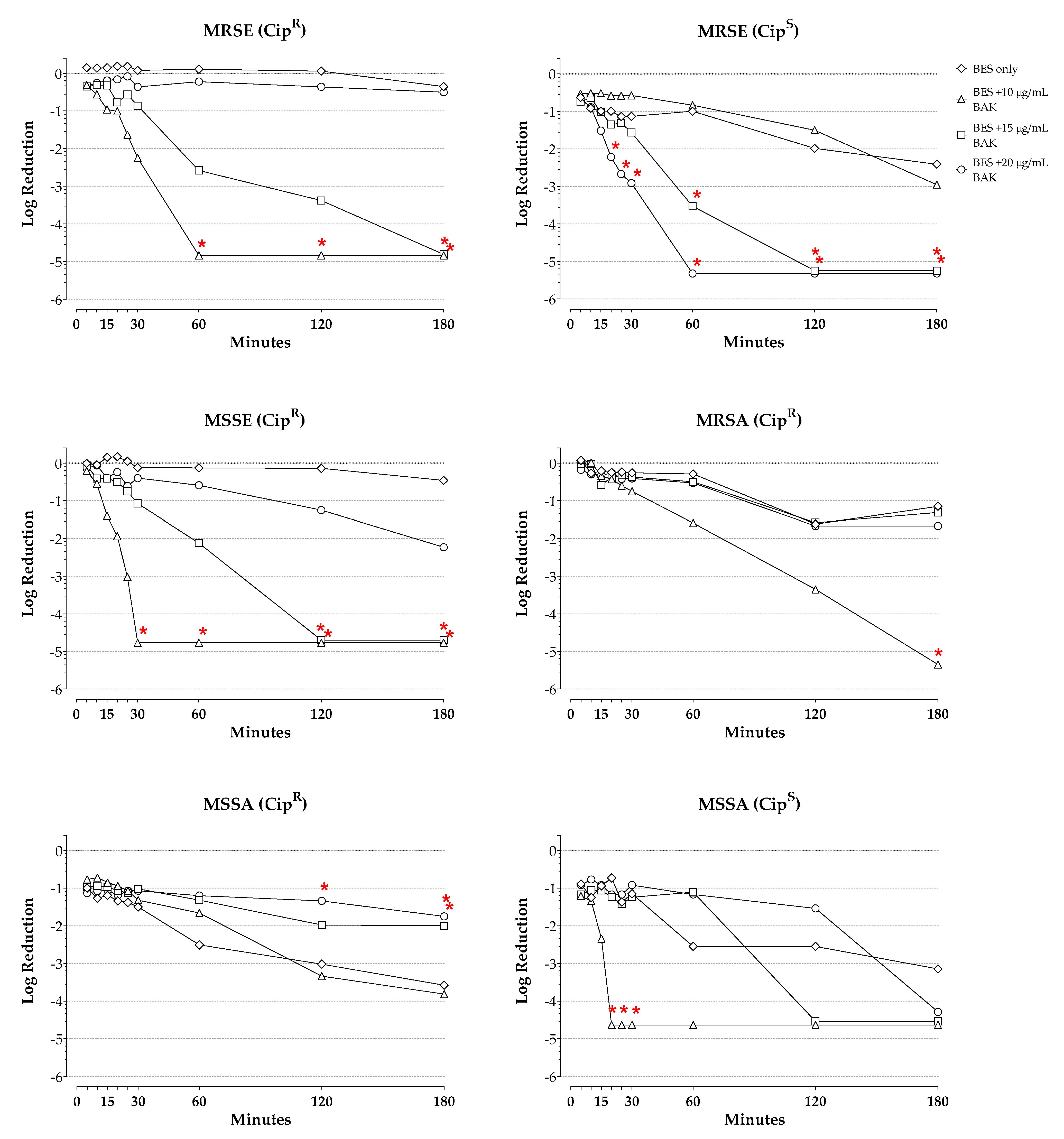
Figure 3 presents the log reductions in viable cell counts over time for besifloxacin alone and in combination with increasing concentrations of BAK for S. epidermidis and S. aureus isolates categorized by their methicillin and/or ciprofloxacin resistance profile. Corresponding log reductions at the final timepoint are presented in Table 1. Results of the ANOVA for the kill curves for these individual isolates indicated a significant effect of test agent and time for these isolates regardless of the isolate resistance profile (p ≤ 0.0003 for all).
With besifloxacin alone, a 0.2-log kill was observed of the CipR MRSE isolate at 5 min drug exposure, which increased to a 0.4-log kill by 180 min, whereas more robust bacterial killing was observed of the two CipS MRSE isolates, with a 0.6-log kill observed at 5 min drug exposure, which increased to a 2.4-log kill by 180 min. The addition of BAK at 15 µg/mL or 20 µg/mL led to increased bacterial killing regardless of the ciprofloxacin resistance-phenotype. Thus, the combination of besifloxacin with BAK at 15 µg/mL or at 20 µg/mL, respectively, resulted in 3-log kills of the CipR MRSE isolate by about 90 and 45 min, and of the CipS MRSE isolates by about 50 and 30 min of combined drug exposure. Furthermore, the combination of BAK and besifloxacin was significantly more active than besifloxacin alone against the CipR MRSE isolate at the 180-min timepoint for BAK at 15 µg/mL; at the 60-min timepoint and onward for BAK at 20 µg/mL (p ≤ 0.0092); against the CipS MRSE isolates at the 60-min timepoints and onward for BAK at 15 µg/mL; and at the 20-min timepoint and onward for BAK at 20 µg/mL (p ≤ 0.0046). Minimal killing (<0.1-log kill) was observed with besifloxacin alone against the CipR MSSE isolate, increasing to 0.5 log units by 180 min. The addition of BAK to besifloxacin led to increased killing of this isolate, with 3-log kills achieved at approximately 80 min exposure for the combination of besifloxacin with 15 µg/mL BAK, and at 25 min for the combination of besifloxacin with 20 µg/mL BAK. Significant differences in the bacterial killing compared to besifloxacin alone were also found against this isolate at the 120-min timepoint and onward for BAK at 15 µg/mL, and at the 30-min timepoint and onward for BAK at 20 µg/mL (p ≤ 0.0110). The corresponding AUKCs for these S. epidermidis isolates were decreased by 2.2- to 2.7-fold with BAK at 15 µg/mL, and by 4.7- to 6.0-fold with BAK at 20 µg/mL from those with besifloxacin alone.
Besifloxacin alone at 100 µg/mL produced a minimal (<0.1 log) reduction in viable organisms of the CipR MRSA isolate after 5 min of exposure, increasing to a 1.2-log reduction by 180 min of drug exposure. Besifloxacin alone demonstrated greater activity against the MSSA isolates, with 1.0- and 0.9-log reductions at 5 min for the CipR and CipS MSSA isolates, respectively, increasing to 3-log reductions at 120 and 180 min. As was the case for the analysis of the kill curves for the three S. aureus isolates combined, the addition of BAK at 10 or 15 µg/mL to besifloxacin did not increase the log reductions in viable cells of the individual isolates at any timepoint. However, the addition of BAK at 20 µg/mL to besifloxacin increased the killing rate, with a 3-log reduction in viable cells observed at approximately 100 min for the CipR MRSA isolate, and by 20 min for the CipS MSSA isolate. A significantly increased bacterial kill was achieved for the combination of besifloxacin and BAK at 20 µg/mL compared to besifloxacin alone for the CipR MRSA isolate at 180 min (p = 0.0003) and the CipS MSSA isolate at 20, 25, and 30 min (p ≤ 0.0422). Notably, a reduction in the bacterial killing of the CipR MSSA isolate was observed when BAK at 10 or 15 µg/mL was added to besifloxacin, with significant differences observed at 120 min for the combination of besifloxacin and 10 µg/mL BAK, and at 180 min for both combinations compared to besifloxacin alone (p ≤ 0.0427). The AUKC for besifloxacin combined with 20 µg/mL BAK was decreased 1.7-fold for the CipR MRSA isolate and 3.7-fold for the CipS MSSA isolate from that with besifloxacin alone.
One of the P. aeruginosa isolates was ciprofloxacin-resistant, whereas the other was ciprofloxacin sensitive. The evaluation of kill curves for these individual isolates demonstrated a 1.0-log reduction in the viable counts of the CipR P. aeruginosa isolate, increasing to a 3-log reduction at 30 min, and a 5.4-log reduction in the viable counts of the CipS P. aeruginosa isolate already at 5 min of exposure. The addition of BAK to besifloxacin appeared to increase the bacterial killing rate of the CipR P. aeruginosa isolate slightly, helping to achieve 3-log reductions in viable cells by approximately 10 min through the addition of BAK at 15 µg/mL or at 20 µg/mL to besifloxacin, and by 20 min through the addition of BAK at 10 µg/mL to besifloxacin. However, no statistically significant increases were noted over besifloxacin alone at any of the added BAK concentrations. Likewise, the AUKCs for besifloxacin in combination with BAK at 10 µg/mL, 15 µg/mL, and 20 µg/mL were not reduced compared to that of besifloxacin alone.
3. Discussion
Bacterial resistance to antibacterial agents and/or the development of resistance is an ongoing concern in all fields of medicine, including ophthalmology. While MICs are useful in the evaluation of the relative potencies of antibiotics, an MIC only measures the degree of growth inhibition at a given drug concentration. Despite a low MIC and an organism labeled as “susceptible,” it is possible for mutant organisms to survive and/or develop, especially when the bacterial load is large. In vitro bacterial time-kill experiments, however, provide data regarding the rapidity and extent of killing by antibiotics, both of which may be important clinically, and are likely to be more relevant in the context of understanding the potential or lack of potential for resistance development. Indeed, as famously expressed by Charles Nightingale (Hartford Hospital, Hartford, CT) and subsequently adapted by others [26,27] “dead bugs don’t mutate.”
In this in vitro time-kill study, BAK alone demonstrated concentration-dependent killing of three of the four common ocular bacterial pathogens tested. For S. epidermidis, H. influenzae and S. aureus, the rate and extent of the organism killing were greater with increasing concentrations of BAK, and at the highest BAK concentration tested (100 µg/mL), these organisms were killed completely within the first 5 min of drug exposure. However, as is consistent with prior reports [28,29,30], BAK alone had poor activity against P. aeruginosa. In contrast, besifloxacin alone at 100 µg/mL demonstrated killing of all four of these common pathogenic species, including P. aeruginosa. Besifloxacin’s bacterial killing was greatest against P. aeruginosa, despite one of the isolates tested being ciprofloxacin-resistant, with a mean log kill of >3 after only 5 min of exposure, increasing to 5.5-log kills (the maximum possible) by 120 min, followed by H. influenzae, with a mean log kill of 1.3 after only 5 min of drug exposure, increasing to 3.6-log reductions after 180 min. Bacterial killing was also observed against S. epidermidis and S. aureus, with mean log reductions of 0.3 and 0.6, respectively, after 5 min, increasing to log kills of 1.4 and 2.6 at 180 min.
The objective of this study was to evaluate the effect of added BAK on the in vitro bacterial killing of besifloxacin. Against S. epidermidis and H. influenzae isolates, the addition of BAK to besifloxacin increased the rate of bacterial killing compared to besifloxacin alone in proportion to the concentration of the BAK added, whereas the addition of BAK had a variable impact against S. aureus in which increased bacterial killing was only found with the addition of 20 µg/mL BAK, and only in two of the three isolates tested. In general, 3-log kills were achieved faster through the addition of BAK to besifloxacin compared to besifloxacin alone, and statistically significant increased killing was even found at specific timepoints in the time–kill curves, particularly for the concentration of BAK at 20 µg/mL in combination with besifloxacin compared to besifloxacin alone. All of the S. epidermidis isolates tested in this study were methicillin- and/or ciprofloxacin-resistant, and these findings were likewise observed for S. epidermidis strains when kill curves were analyzed according to the isolate(s) resistance profile. Corresponding reductions in the AUKC were also observed with the addition of BAK to besifloxacin in most instances, again signifying greater and/or faster killing with the combination of besifloxacin and BAK of these three common pathogenic species. However, as expected, there was no significant impact of BAK on the killing effect of besifloxacin against P. aeruginosa, despite the appearance of slightly increased killing of the CipR isolate.
Our findings expand on prior studies demonstrating increased killing effects when relatively high concentrations of BAK are added to a fluoroquinolone. Haas et al. [6] performed in vitro time-kill experiments evaluating besifloxacin, moxifloxacin, and gatifloxacin against S. aureus, S. epidermidis, and H. influenzae, with and without BAK. Regardless of the bacterial species, viable cell counts were reduced to the lowest level of detection within the first 5 min when evaluating the fluoroquinolones combined with BAK at 50 or 100 µg/mL. Consistent with our results, concentration-dependent killing was observed at BAK concentrations <50 µg/mL. However, the authors failed to observe increased killing for BAK at concentrations <50 µg/mL in combination with besifloxacin, likely due to the concentration of besifloxacin tested, namely 0.24 µg/mL, which was much lower than that tested in our study [6]. In another in vitro study evaluating the kill rates of commercial formulations, 0.3% gatifloxacin ophthalmic suspension (formulated with BAK 50 µg/mL) was found to eradicate S. aureus and CoNS more rapidly than the 0.5% moxifloxacin ophthalmic solution, which does not contain BAK [31].
Clearly, the data presented here are in vitro findings, and the time-kill data reflect the continued exposure of the bacterial inoculum to a particular concentration of besifloxacin alone or in combination with different concentrations of BAK for several hours, whereas with clinical administration to the ocular surface, natural physiologic processes lead to a rapid dilution of both besifloxacin and BAK in the tear film. In the current in vitro study, the concentration of besifloxacin tested, namely 100 µg/mL, is 60-fold lower than that in the instilled drop (0.6% or 6 mg/mL). Proksch et al. reported a besifloxacin maximum tear concentration of 610 µg/g at 10 min following a single drop administration to healthy volunteers, which decreased to approximately 50 μg/g at 8 h, 10 μg/g at 12 h, and still more than 1 μg/g at 24 h [32]. Thus, a 100 µg/mL concentration of besifloxacin is a reasonable estimate of the on-eye concentration of besifloxacin that is clinically achievable and sustained for a significant time following instillation of a drop; the in vitro findings herein for besifloxacin alone are therefore reassuring and confirm the expected clinical activity of besifloxacin. In contrast, the highest concentration of BAK tested in vitro, also 100 µg/mL, is the same as that in the bottle, and represents undiluted BAK. It follows that the log reduction findings for the 100 µg/mL BAK concentration are relevant only to bactericidal activity in the bottle and are supportive of the intended use of BAK as a preservative in the bottle. However, the findings for BAK at the lower concentrations of 10 µg/mL, 15 µg/mL, and 20 µg/mL, representing 10-, 6.7-, and 5-fold dilutions, respectively, may roughly represent the concentrations of BAK achieved on-eye, especially in the immediate time frame after the drop instillation. The testing of BAK at lower concentrations was not reasonable given the reported MIC of BAK of ≤3.1 µg/mL against strains of methicillin-sensitive and -resistant S. aureus and CoNS, along with reporting by Friedlaender et al. of a 16-fold dilution of BAK in tears (to only 3.2 µg/mL) as early as 1 min after the instillation of another fluoroquinolone formulation containing 0.005% (50 µg/mL) BAK [33].
However, even as the BAK concentrations are diluted rapidly during the first few minutes after instillation, the expected increased killing effects observed with BAK in combination with besifloxacin in this immediate time frame post-instillation compared to besifloxacin alone could very well be clinically meaningful, especially against S. epidermidis, some S. aureus, and H. influenzae organisms, and may help minimize the potential for microbial resistance development in these species, given that the greater and/or faster the killing of a pathogenic bacteria is, the smaller the risk of resistance development. Moreover, an increased rate of kill may also help mitigate infection with isolates which are already resistant. While little antibacterial resistance has been reported among H. influenzae in ocular infections to date, in vitro resistance has been reported among CoNS and S. aureus [5,34,35,36,37], and MRSA has become a growing concern in ophthalmic infections [38,39,40,41,42,43]. In this context, it is notable that the addition of BAK at 20 µg/mL to besifloxacin was especially impactful with regards to the achievement of 3-log kills of CipR and CipS MRSE as well as CipR MSSE by approximately 30 min. Similarly, the addition of BAK at 20 µg/mL to besifloxacin decreased the time of exposure needed to achieve the 3-log killing of the CipR MRSA isolate compared to besifloxacin alone. However, the addition of BAK did not increase the bacterial killing rate of the one CipR methicillin-sensitive S. aureus isolate tested in this study. In fact, BAK appeared to paradoxically decrease the bacterial kill rate of that isolate when added at concentrations of either 10 and 15 µg/mL. The reason for this finding is unclear and warrants further investigation.
The limitations of this study include the lack of timepoints between 0 and 5 min of drug exposure, the small number of isolates tested, and the inability of time-kill experiments to accurately reflect the changing concentrations of either besifloxacin and BAK on-eye following the instillation of a drop of besifloxacin ophthalmic suspension 0.6%. However, in general, the findings of this in vitro study do suggest that the inclusion of BAK at 0.01% in the besifloxacin formulation could enhance the bacterial killing with besifloxacin in the immediate period post-instillation on-eye, in particular that of S. epidermidis and S. aureus with varying resistance profiles, and that of H. influenzae, thereby aiding in the prevention of antibiotic resistance development and/or the treatment of already drug-resistant isolates. Finally, the MICs of besifloxacin for the isolates tested were not known, nor would they have been interpretable given the current absence of established CLSI breakpoints for besifloxacin. Nevertheless, microbiological studies to date indicate that the MIC of besifloxacin is normally within one to two dilutions of that of moxifloxacin against methicillin-sensitive S. aureus and methicillin-sensitive CoNS, and three dilutions lower than that of moxifloxacin against methicillin-resistant staphylococci [5]. Thus, the concentration of besifloxacin tested in this study, 100 µg/mL, is likely to be several-fold higher than the 4X MIC typically used as the lower limit in time-kill studies. More importantly, the concentration studied was selected based on the known/expected concentrations of besifloxacin on-eye following the instillation of 0.6% besifloxacin ophthalmic solution.
In conclusion, the addition of BAK to besifloxacin led to rapid eradication of common ocular pathogens under in vitro conditions. While the clinical significance of enhanced antibacterial killing with the addition of BAK cannot be determined with certainty, these data support the inclusion of BAK in the besifloxacin formulation and in other topical ophthalmic fluoroquinolone formulations. Beyond its use as a preservative in the bottle, BAK may contribute to the killing of bacterial pathogens immediately post-instillation and thereby help to suppress antibiotic resistance development and/or aid in the eradication of bacterial strains that are already resistant.
4. Methods
Clinical, non-duplicate ocular isolates of four bacterial species were collected at the Clinical Microbiology Laboratory of the Royal University Hospital, Saskatoon, Saskatchewan, Canada, including S. epidermidis (4 isolates), S. aureus (3 isolates), P. aeruginosa (2 isolates), and Haemophilus influenzae (2 isolates). The staphylococcal isolates had varying drug resistance phenotypes: three of the S. epidermidis isolates and one S. aureus isolate were oxacillin-resistant (i.e., methicillin-resistant; MRSE and MRSA, respectively), and two S. epidermidis and two S. aureus isolates (including the oxacillin-resistant one) were ciprofloxacin-resistant (CipR). The respective MICs for ciprofloxacin and moxifloxacin against staphylococcal isolates were 64 and 16 µg/mL for CipR MRSE, ≤0.063 and ≤0.031 µg/mL for ciprofloxacin-sensitive (CipS) MRSE, 32 and 16 µg/mL for CipR MSSE, ≥64 and ≥16 µg/mL for CipR MRSA, 8 and 0.25 µg/mL CipR MSSA, and 0.125 and 0.031 µg/mL for CipS MSSA. Additionally, one P. aeruginosa isolate was ciprofloxacin resistant.
Institutional review board approval was not required as this was a laboratory study. The isolates were obtained from specimens submitted during standard care, and no patient-specific information was collected or recorded for these isolates for the purposes of the study.
Besifloxacin and BAK were obtained from Bausch & Lomb Incorporated (Rochester, NY). Methods for culture preparation and time-kill studies were described previously [44,45,46]. Briefly, S. epidermidis, P. aeruginosa, and S. aureus isolates were grown overnight on Tryptic Soy Agar (TSA) plates containing 5% sheep blood, whereas the H. influenzae isolates were grown on TSA plates containing 5% defibrinated sheep blood (chocolate plates). On the following day, an inoculum of each isolate was transferred to test tubes containing growth media appropriate to the species (i.e., S. epidermidis, S. aureus, and P. aeruginosa were transferred to Mueller–Hinton Broth and H. influenzae isolates were transferred to Haemophilus Test Media) and incubated for 2 h at 35–37 °C (in ambient air for staphylococci and P. aeruginosa, or in 5% CO2 for H. influenzae) in order to ensure that the bacterial isolates were in the growth phase.
For the time-kill experiments, isolate cultures were evaluated spectrophotometrically and diluted as necessary to achieve final cell densities of 104–105 cells/mL, and antimicrobial agents were added to the culture tubes to achieve final concentrations of 10, 15, 20, or 100 µg/mL BAK, 100 µg/mL besifloxacin, or combinations of besifloxacin (100 µg/mL) and BAK (10, 15, 20, or 100 µg/mL). Following 5, 10, 15, 20, 25, 30, 60, 120, and 180 min of exposure, triplicate sample aliquots were removed, serially diluted, and plated on appropriate drug-free agar medium. After incubation overnight at 35–37 °C (in 5% CO2 or ambient air, based on the species) viable colonies were enumerated.
The rate and extent of the bacterial killing were determined by plotting the reduction in viable colony counts (log10 CFU/mL) against time. Differences in time-kill curves were evaluated using two-way analysis of variance (ANOVA) followed by the Dunnett’s multiple comparisons test. A p value of <0.05 was considered significant. Additionally, areas-under-the-killing-curve (AUKC) over 180 min were computed using the trapezoid rule and a fixed baseline of −5.2 log units, and fold-reductions in the AUKC were calculated. Data were plotted and analyzed using GraphPad Prism version 6.07 for Windows (GraphPad Software, La Jolla, CA, USA).
Author Contributions
J.B. provided all of the in vitro data, and together with H.D. analyzed and interpreted the data. Both authors contributed to the writing and revision of the manuscript, and have read and agreed to the submitted version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by Bausch & Lomb Incorporated.
Institutional Review Board Statement
Institutional review board approval was not applicable as this laboratory study neither involved humans or animals.
Informed Consent Statement
Not applicable for studies not involving humans.
Data Availability Statement
The data presented in this study are available in this article, “In Vitro Time-Kill of Common Ocular Pathogens with Besifloxacin Alone and in Combination with Benzalkonium Chloride”.
Acknowledgments
The authors acknowledge the writing and editing assistance of Churchill Communications (Maplewood, NJ, USA), funded by Bausch + Lomb, a division of Bausch Health US, LLC (Rochester, NY, USA).
Conflicts of Interest
J. Blondeau has received unrestricted investigator-initiated grants from Bausch + Lomb. H. DeCory is an employee of Bausch Health US, LLC.
References
- Davis, S.L.; Neuhauser, M.M.; McKinnon, P.S. Quinolones. Antimicrobe. Available online: http://www.antimicrobe.org/d17.asp#t4 (accessed on 2 June 2020).
- Besivance® Prescribing Information; Bausch + Lomb: Bridgewater, NJ, USA, 2020.
- Haas, W.; Pillar, C.M.; Zurenko, G.E.; Lee, J.C.; Brunner, L.S.; Morris, T.W. Besifloxacin, a Novel Fluoroquinolone, Has Broad-Spectrum In Vitro Activity against Aerobic and Anaerobic Bacteria. Antimicrob. Agents Chemother. 2009, 53, 3552–3560. [Google Scholar] [CrossRef] [Green Version]
- Miller, D.; Chang, J.; Flynn, H.W.; Alfonso, E.C. Comparative In Vitro Susceptibility of Besifloxacin and Seven Comparators Against Ciprofloxacin- and Methicillin-Susceptible/Nonsusceptible Staphylococci. J. Ocul. Pharmacol. Ther. 2013, 29, 339–344. [Google Scholar] [CrossRef]
- Asbell, P.A.; Sanfilippo, C.M.; Sahm, D.F.; DeCory, H.H. Trends in Antibiotic Resistance Among Ocular Microorganisms in the United States From 2009 to 2018. JAMA. Ophthalmol. 2020, 138, 439–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haas, W.; Pillar, C.M.; Hesje, C.K.; Sanfilippo, C.M.; Morris, T.W. In Vitro Time-Kill Experiments with Besifloxacin, Moxifloxacin and Gatifloxacin in the Absence and Presence of Benzalkonium Chloride. J. Antimicrob. Chemother. 2011, 66, 840–844. [Google Scholar] [CrossRef] [Green Version]
- Karpecki, P.; DePaolis, M.; Hunter, J.A.; White, E.M.; Rigel, L.; Brunner, L.S.; Usner, D.W.; Paterno, M.R.; Comstock, T.L. Besifloxacin Ophthalmic Suspension 0.6% in Patients with Bacterial Conjunctivitis: A Multicenter, Prospective, Randomized, Double-Masked, Vehicle-Controlled, 5-Day Efficacy and Safety Study. Clin. Ther. 2009, 31, 514–526. [Google Scholar] [CrossRef]
- Tepedino, M.E.; Heller, W.H.; Usner, D.W.; Brunner, L.S.; Morris, T.W.; Haas, W.; Paterno, M.R.; Comstock, T.L. Phase III Efficacy and Safety Study of Besifloxacin Ophthalmic Suspension 0.6% in the Treatment of Bacterial Conjunctivitis. Curr. Med. Res. Opin. 2009, 25, 1159–1169. [Google Scholar] [CrossRef]
- McDonald, M.B.; Protzko, E.E.; Brunner, L.S.; Morris, T.W.; Haas, W.; Paterno, M.R.; Comstock, T.L.; Usner, D.W. Efficacy and Safety of Besifloxacin Ophthalmic Suspension 0.6% Compared with Moxifloxacin Ophthalmic Solution 0.5% for Treating Bacterial Conjunctivitis. Ophthalmology 2009, 116, 1615–1623. [Google Scholar] [CrossRef] [PubMed]
- DeLeon, J.; Silverstein, B.E.; Allaire, C.; Gearinger, L.S.; Bateman, K.M.; Morris, T.W.; Comstock, T.L. Besifloxacin Ophthalmic Suspension 0.6% Administered Twice Daily for 3 Days in the Treatment of Bacterial Conjunctivitis in Adults and Children. Clin. Drug Investig. 2012, 32, 303–317. [Google Scholar] [CrossRef]
- Sanfilippo, C.M.; Allaire, C.M.; DeCory, H.H. Besifloxacin Ophthalmic Suspension 0.6% Compared with Gatifloxacin Ophthalmic Solution 0.3% for the Treatment of Bacterial Conjunctivitis in Neonates. Drugs R D 2017, 17, 167–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garg, P.; Mathur, U.; Sony, P.; Tandon, R.; Morris, T.W.; Comstock, T.L. Clinical and Antibacterial Efficacy and Safety of Besifloxacin Ophthalmic Suspension Compared with Moxifloxacin Ophthalmic Solution. Asia Pac. J. Ophthalmol. (Phila). 2015, 4, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, B.E.; Allaire, C.; Bateman, K.M.; Gearinger, L.S.; Morris, T.W.; Comstock, T.L. Efficacy and Tolerability of Besifloxacin Ophthalmic Suspension 0.6% Administered Twice Daily for 3 Days in the Treatment of Bacterial Conjunctivitis: A Multicenter, Randomized, Double-Masked, Vehicle-Controlled, Parallel-Group Study in Adults and Children. Clin. Ther. 2011, 33, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, B.E.; Morris, T.W.; Gearinger, L.S.; DeCory, H.H.; Comstock, T.L. Besifloxacin Ophthalmic Suspension 0.6% in the Treatment of Bacterial Conjunctivitis Patients with Pseudomonas aeruginosa Infections. Clin. Ophthalmol. 2012, 6, 1987–1996. [Google Scholar] [CrossRef] [Green Version]
- Bucci, J.F.; Evans, R.E.; Amico, L.M.; Morris, T.W.; Fluet, A.T.; Sanfilippo, C.M.; DeCory, H.H.; Comstock, T.L. Antibacterial Efficacy of Prophylactic Besifloxacin 0.6% and Moxifloxacin 0.5% in Patients Undergoing Cataract Surgery. Clin. Ophthalmol. 2015, 9, 843–852. [Google Scholar] [CrossRef] [Green Version]
- John, G. A Comparative Study in the Clinical and Microbial Efficacy of Topical Besifloxacin Ophthalmic Suspension 0.6% with Erythromycin Ophthalmic Ointment 0.5% for Management of Acute Blepharitis. Investig. Ophthalmol. Vis. Sci. 2012, 53, 6263. [Google Scholar]
- Kissling, R.F.; Sanfilippo, C.M.; DeCory, H.H. Comparative In Vitro Activity of Antibiotics Frequently Used in the Management of Staphylococcal Blepharitis. In Proceedings of the Association for Research in Vision and Ophthalmology Annual Meeting (ARVO), Digital, 7 May 2021. [Google Scholar]
- Tu, Y.; Boschert, B.; Schwab, J.; Wagner, R.; DeRespinis, P.; Guo, S. Management of Congenital Nasolacrimal Duct Obstruction with Infection in Infants using Besifloxacin-A Prospective Study. Investig. Ophthalmol. Vis. Sci. 2015, 56, 4870. [Google Scholar]
- Tu, Y.; Boschert, K.; Schwab, J.V.; Wagner, R.S.; Derespinis, P.; Guo, S. Comparison of Besifloxacin and Polymyxin–trimethoprim in Treating Congenital Nasolacrimal Duct Obstruction with Infection in Children. In Proceedings of the American Society of Cataract and Refractive Surgery Annual Symposium and Congress (ASCRS), San Diego, CA, USA, 17 April 2015. [Google Scholar]
- Freeman, P.D.; Kahook, M.Y. Preservatives in Topical Ophthalmic Medications: Historical and Clinical Perspectives. Expert Rev. Ophthalmol. 2009, 4, 59–64. [Google Scholar] [CrossRef]
- Saji, M.; Usuki, R.; Ibaraki, N.; Hayama, N.; Osono, E.; Ohkuni, H. Studies of Antibacterial Activity of Benzalkonium Chloride as Preservative for Ophthalmic Solutions Against Gram-positive Cocci and Negative Rods. Jpn. J. Pharm. Health Care Sci. 2003, 29, 341–345. [Google Scholar] [CrossRef] [Green Version]
- Block, S.S. (Ed.) Disinfection, Sterilization and Preservation, 4th ed.; Lea & Febiger: Philadelphia, PA, USA, 1991; p. 633. [Google Scholar]
- Sheikh, A.; Hurwitz, B.; Van Schayck, C.P.; McLean, S.; Nurmatov, U. Antibiotics Versus Placebo for Acute Bacterial Conjunctivitis. Cochrane Database Syst. Rev. 2012, 9, CD001211. [Google Scholar] [CrossRef] [Green Version]
- Hesje, C.K.; Borsos, S.D.; Blondeau, J.M. Benzalkonium Chloride Enhances Antibacterial Activity of Gatifloxacin and Reduces its Propensity to Select for Fluoroquinolone-Resistant Strains. J. Ocul. Pharmacol. Ther. 2009, 25, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Blondeau, J.; Borsos, S.; Hesje, C. Antimicrobial Efficacy of Gatifloxacin and Moxifloxacin with and without Benzalkonium Chloride Compared with Ciprofloxacin and Levofloxacin Against Methicillin-resistant Staphylococcus aureus. J. Chemother. 2007, 19, 146–151. [Google Scholar] [CrossRef]
- Stratton, C.W. Dead Bugs Don’t Mutate: Susceptibility Issues in the Emergence of Bacterial Resistance. Emerg. Infect. Dis. 2003, 9, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Dean, N.C. Encouraging News from the Antibiotic Resistance Front. Chest 2003, 124, 423–424. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, R.P.; Kowalski, B.R.; Romanowski, E.G.; Mah, F.S.; Thompson, P.P.; Gordon, Y.J. The In vitro Impact of Moxifloxacin and Gatifloxacin Concentration (0.5% vs. 0.3%) and the Addition of Benzalkonium Chloride on Antibacterial Efficacy. Am. J. Ophthalmol. 2006, 142, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Hatt, J.K.; Weigand, M.R.; Krishnan, R.; Pavlostathis, S.G.; Konstantinidis, K.T. Genomic and Transcriptomic Insights into How Bacteria Withstand High Concentrations of Benzalkonium Chloride Biocides. Appl. Environ. Microbiol. 2018, 84, e00197-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambert, R.; Joynson, J.; Forbes, B. The Relationships and Susceptibilities of Some Industrial, Laboratory and Clinical Isolates of Pseudomonas Aeruginosa to Some Antibiotics and Biocides. J. Appl. Microbiol. 2001, 91, 972–984. [Google Scholar] [CrossRef] [Green Version]
- Hyon, J.Y.; Eser, I.; O’Brien, T.P. Kill Rates of Preserved and Preservative-Free Topical 8-Methoxy Fluoroquinolones Against Various Strains of Staphylococcus. J. Cataract. Refract. Surg. 2009, 35, 1609–1613. [Google Scholar] [CrossRef]
- Proksch, J.W.; Granvil, C.P.; Siou-Mermet, R.; Comstock, T.L.; Paterno, M.R.; Ward, K.W. Ocular Pharmacokinetics of Besifloxacin Following Topical Administration to Rabbits, Monkeys, and Humans. J. Ocul. Pharmacol. Ther. 2009, 25, 335–344. [Google Scholar] [CrossRef]
- Friedlaender, M.H.; Breshears, D.; Amoozgar, B.; Sheardown, H.; Senchyna, M. The Dilution of Benzalkonium Chloride (BAK) in the Tear Film. Adv. Ther. 2006, 23, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Asbell, P.A.; Colby, K.A.; Deng, S.; McDonnell, P.; Meisler, D.M.; Raizman, M.B.; Sheppard, J.D.; Sahm, D.F. Ocular TRUST: Nationwide Antimicrobial Susceptibility Patterns in Ocular Isolates. Am. J. Ophthalmol. 2008, 145, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Oydanich, M.; Dingle, T.; Hamula, C.L.; Ghisa, C.; Asbell, P. Retrospective Report of Antimicrobial Susceptibility Observed in Bacterial Pathogens Isolated from Ocular Samples at Mount Sinai Hospital, 2010 to 2015. Antimicrob. Resist. Infect. Control. 2017, 6, 29. [Google Scholar] [CrossRef] [Green Version]
- Miller, D. Update on the Epidemiology and Antibiotic Resistance of Ocular Infections. Middle East Afr. J. Ophthalmol. 2017, 24, 30–42. [Google Scholar]
- Gentile, R.C.; Shukla, S.; Shah, M.; Ritterband, D.C.; Engelbert, M.; Davis, A.; Hu, D.-N. Microbiological Spectrum and Antibiotic Sensitivity in Endophthalmitis: A 25-year review. Ophthalmology 2014, 121, 1634–1642. [Google Scholar] [CrossRef] [PubMed]
- Teweldemedhin, M.; Gebreyesus, H.; Atsbaha, A.H.; Asgedom, S.W.; Saravanan, M. Bacterial Profile of Ocular Infections: A Systematic Review. BMC. Ophthalmol. 2017, 17, 212. [Google Scholar] [CrossRef] [Green Version]
- Vola, M.M.; Moriyama, A.S.; Lisboa, R.; Hirai, F.E.; Bispo, P.J.M.; Höfling-Lima, A.L. Prevalence and Antibiotic Susceptibility of Methicillin-Resistant Staphylococcus Aureus in Ocular Infections. Arq. Bras. Oftalmol. 2013, 76, 350–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amato, M.; Pershing, S.; Walvick, M.; Tanaka, S. Trends in Ophthalmic Manifestations of Methicillin-Resistant Staphylococcus Aureus (MRSA) in a Northern California Pediatric Population. J. AAPOS. 2013, 17, 243–247. [Google Scholar] [CrossRef]
- Asbell, P.A.; Sahm, D.F.; Shaw, M.; Draghi, D.C.; Brown, N.P. Increasing Prevalence of Methicillin Resistance in Serious Ocular Infections Caused by Staphylococcus Aureus in the United States: 2000 to 2005. J. Cataract Refract. Surg. 2008, 34, 814–818. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.-Y.; Chu, H.-S.; Wang, I.-J.; Chen, W.-L.; Hu, F.-R. Microbial Keratitis in Taiwan: A 20-Year Update. Am. J. Ophthalmol. 2019, 205, 74–81. [Google Scholar] [CrossRef]
- Chang, V.S.; Dhaliwal, D.K.; Raju, L.; Kowalski, R.P. Antibiotic Resistance in the Treatment of Staphylococcus aureus Keratitis. Cornea 2015, 34, 698–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blondeau, J.M.; Hansen, G.T.; Metzler, K.L.; Borsos, S.; Chau, J. Optimal Killing of Streptococcus Pneumoniae by Gemifloxacin, Levofloxacin and Moxifloxacin. Round Table Ser. R. Soc. Med. 2002, 76, 15–26. [Google Scholar]
- Blondeau, J.; Blondeau, L.; Hesje, C.; Borsos, S. Application of Two Methods to Determine Killing of Streptococcus pneumoniae by Various Fluoroquinolones. J. Chemother. 2006, 18, 366–372. [Google Scholar] [CrossRef]
- Blondeau, J.; Borsos, S.; Blondeau, L.; Blondeau, B. In Vitro Killing of Escherichia Coli, Staphylococcus Pseudintermedius and Pseudomonas Aeruginosa by Enrofloxacin in Combination with its Active Metabolite Ciprofloxacin Using Clinically Relevant Drug Concentrations in the Dog and Cat. Vet. Microbiol. 2012, 155, 284–290. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Log reductions in viable cells over time with increasing concentrations of BAK alone. Starting (0 min) viable cell densities for each isolate were ~105 CFU/mL. Each plot point represents the mean (±SD) (S. epidermidis and S. aureus) or average (H. influenzae and P. aeruginosa) for the isolates tested of each species.
Figure 1.
Log reductions in viable cells over time with increasing concentrations of BAK alone. Starting (0 min) viable cell densities for each isolate were ~105 CFU/mL. Each plot point represents the mean (±SD) (S. epidermidis and S. aureus) or average (H. influenzae and P. aeruginosa) for the isolates tested of each species.
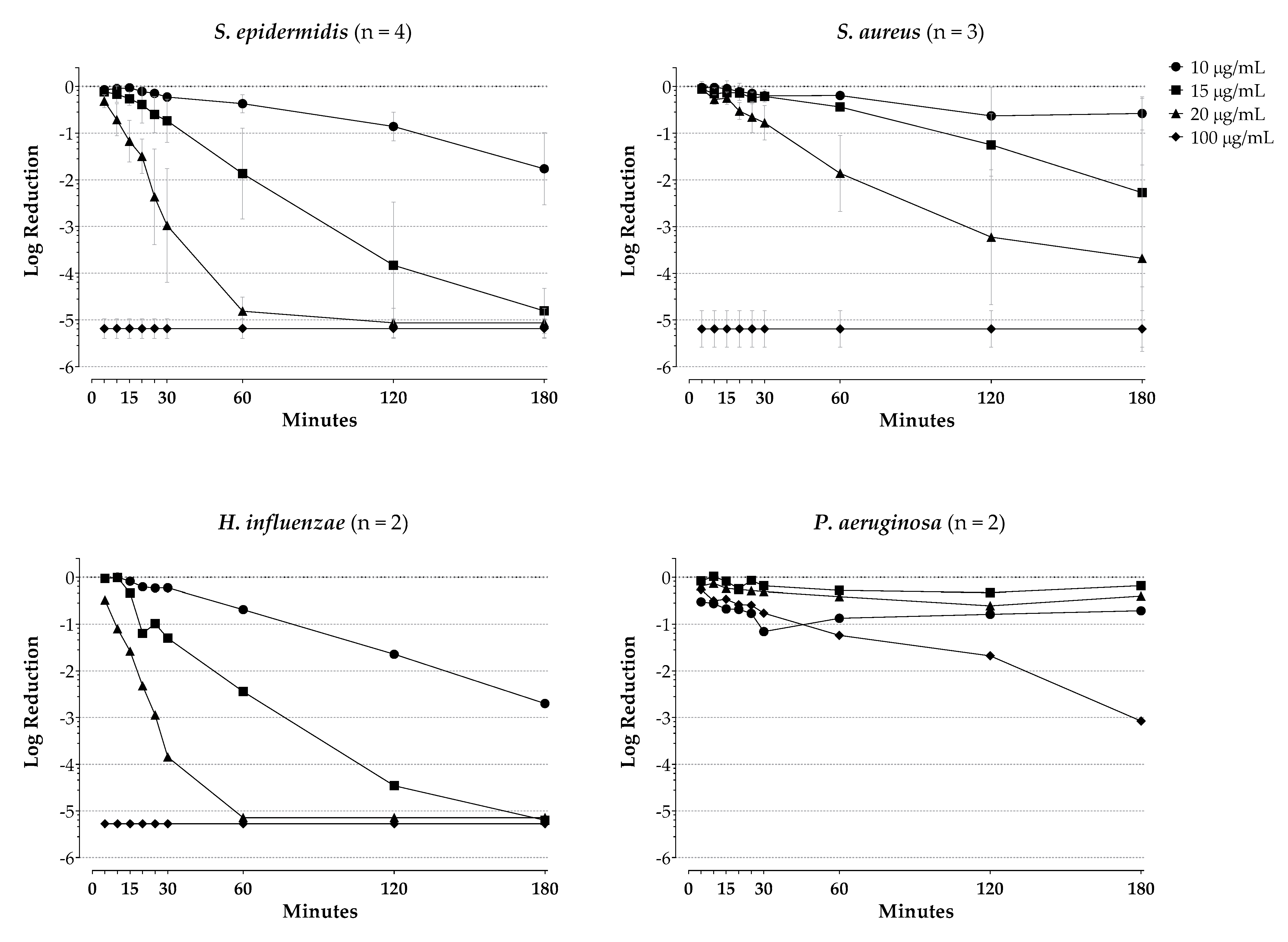
Figure 2.
Log reductions in viable cells over time with 100 µg/mL besifloxacin alone or combined with increasing amounts of BAK. Starting (0 min) viable cell densities for each isolate were ~105 CFU/mL. Each plot point represents the mean (±SD) (S. epidermidis and S. aureus) or average (H. influenzae and P. aeruginosa) for the isolates tested of each species. * p < 0.05 compared with besifloxacin. BES = besifloxacin, BAK = benzalkonium chloride.
Figure 2.
Log reductions in viable cells over time with 100 µg/mL besifloxacin alone or combined with increasing amounts of BAK. Starting (0 min) viable cell densities for each isolate were ~105 CFU/mL. Each plot point represents the mean (±SD) (S. epidermidis and S. aureus) or average (H. influenzae and P. aeruginosa) for the isolates tested of each species. * p < 0.05 compared with besifloxacin. BES = besifloxacin, BAK = benzalkonium chloride.
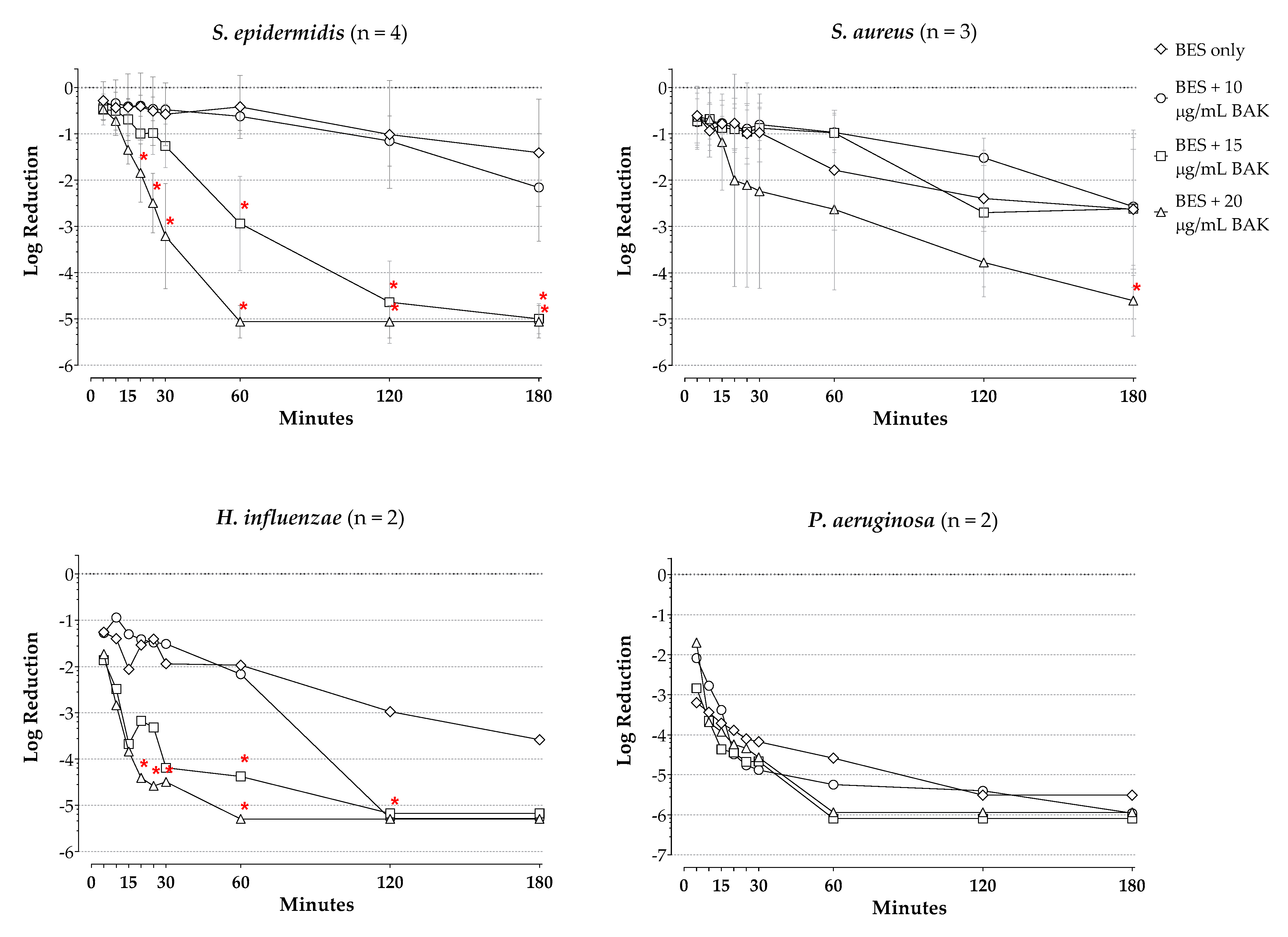
Figure 3.
Log reductions in viable organisms over time with 100 µg/mL besifloxacin alone or combined with increasing amounts of BAK for S. epidermidis and S. aureus isolates by resistance profile. Starting (0 min) viable cell densities for each isolate were ~105 CFU/mL. All of the plots represent one tested isolate, with the exception of MRSE (CipS), which represents the average of two tested isolates. * p < 0.05 compared with besifloxacin. BES = besifloxacin, BAK = benzalkonium chloride, MRSE = methicillin-resistant S. epidermidis, MSSE = methicillin-sensitive S. epidermidis, MRSA = methicillin-resistant S. aureus, MSSA = methicillin-sensitive S. aureus, CipR = ciprofloxacin-resistant, CipS = ciprofloxacin-sensitive.
Figure 3.
Log reductions in viable organisms over time with 100 µg/mL besifloxacin alone or combined with increasing amounts of BAK for S. epidermidis and S. aureus isolates by resistance profile. Starting (0 min) viable cell densities for each isolate were ~105 CFU/mL. All of the plots represent one tested isolate, with the exception of MRSE (CipS), which represents the average of two tested isolates. * p < 0.05 compared with besifloxacin. BES = besifloxacin, BAK = benzalkonium chloride, MRSE = methicillin-resistant S. epidermidis, MSSE = methicillin-sensitive S. epidermidis, MRSA = methicillin-resistant S. aureus, MSSA = methicillin-sensitive S. aureus, CipR = ciprofloxacin-resistant, CipS = ciprofloxacin-sensitive.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Bacterial kill after 180 min for besifloxacin alone and besifloxacin in combination with BAK.
Table 1.
Bacterial kill after 180 min for besifloxacin alone and besifloxacin in combination with BAK.
| BES (100 µg/mL) | BES a + BAK (10 µg/mL) | BES a + BAK (15 µg/mL) | BES a + BAK (20 µg/mL) | |
|---|---|---|---|---|
| S. epidermidis, n = 4 | ||||
| Mean Δlog CFU/mL | −1.41 | −2.16 | −5.00 | −5.06 |
| Mean Difference (95% CI) | 0.753 (−0.306, 1.81) | 3.59 (2.53, 4.65) | 3.66 (2.60, 4.71) | |
| p-value b | NS | <0.0001 | <0.0001 | |
| CipR MRSE, n = 1 | ||||
| Δlog CFU/mL | −0.350 | −0.500 | −4.81 | −4.81 |
| Mean Difference (95% CI) | 0.150 (−3.43, 3.73) | 4.46 (0.876, 8.04) | 4.49 (0.906, 8.07) | |
| p-value b | NS | 0.0092 | 0.0086 | |
| CipS MRSE, n = 2 | ||||
| Mean Δlog CFU/mL | −2.41 | −2.96 | −5.24 | −5.32 |
| Mean Difference (95% CI) | 0.545 (−0.463, 1.55) | 2.83 (1.82, 3.84) | 2.91 (1.90, 3.92) | |
| p-value b | NS | <0.0001 | <0.0001 | |
| CipR MSSE, n = 1 | ||||
| Δlog CFU/mL | −0.460 | −2.23 | −4.70 | −4.77 |
| Mean Difference (95% CI) | 1.77 (−1.71, 5.25) | 4.24 (0.765, 7.72) | 4.31 (0.835, 7.79) | |
| p-value b | NS | 0.0110 | 0.0095 | |
| S. aureus, n = 3 | ||||
| Mean Δlog CFU/mL | −2.63 | −2.57 | −2.62 | −4.60 |
| Mean Difference (95% CI) | −0.0567 (−1.81, 1.70) | −0.0100 (−1.77, 1.75) | 1.98 (0.221, 3.73) | |
| p-value b | NS | NS | 0.0196 | |
| CipR MRSA, n = 1 | ||||
| Δlog CFU/mL | −1.15 | −1.67 | −1.31 | −5.35 |
| Mean Difference (95% CI) | 0.520 (−1.96, 3.00) | 0.160 (−2.32, 2.64) | 4.20 (1.72, 6.68) | |
| p-value b | NS | NS | 0.0003 | |
| CipR MSSA, n = 1 | ||||
| Δlog CFU/mL | −3.58 | −1.75 | −2.00 | −3.82 |
| Mean Difference (95% CI) | −1.83 (−3.37, −0.29) | −1.58 (−3.12, −0.04) | 0.024 (−1.30, 1.78) | |
| p-value b | 0.0141 | 0.0427 | NS | |
| CipS MSSA, n = 1 | ||||
| Δlog CFU/mL | −3.15 | −4.29 | −4.54 | −4.64 |
| Mean Difference (95% CI) | 1.14 (−2.05, 4.33) | 1.39 (−1.80, 4.58) | 1.49 (−1.70, 4.68) | |
| p-value b | NS | NS | NS | |
| H. influenzae, n = 2 | ||||
| Mean Δlog CFU/mL | −3.58 | −5.29 | −5.18 | −5.30 |
| Mean Difference (95% CI) | 1.71 (−0.380, 3.79) | 1.60 (−0.490, 3.68) | 1.72 (−0.370, 3.80) | |
| p-value b | NS | NS | NS | |
| P. aeruginosa, n = 2 | ||||
| Mean Δlog CFU/mL | −5.51 | −5.96 | −6.10 | −5.94 |
| Mean Difference (95% CI) | 0.450 (−2.27, 3.17) | 0.585 (−2.13, 3.30) | 0.430 (−2.29, 3.15) | |
| p-value b | NS | NS | NS | |
| CipR P. aeruginosa, n = 1 | ||||
| Δlog CFU/mL | −5.63 | −5.93 | −5.99 | −5.97 |
| Mean Difference (95% CI) | 0.300 (−2.86, 3.46) | 0.360 (−2.80, 3.52) | 0.340 (−2.82, 3.50) | |
| p-value b | NS | NS | NS | |
| CipS P. aeruginosa, n = 1 | ||||
| Δlog CFU/mL | −5.39 | −5.99 | −6.20 | −5.91 |
| Mean Difference (95% CI) | 0.600 (−1.77, 2.97) | 0.810 (−1.56, 3.18) | 0.520 (−1.85, 2.89) | |
| p-value b | NS | NS | NS |
BES, besifloxacin; BAK, benzalkonium chloride; CFU/mL, colony forming units per mL; CI, confidence interval; NS, not significant; CipR, ciprofloxacin-resistant; CipS, ciprofloxacin sensitive; MRSE, methicillin-resistant S. epidermidis; MSSE, methicillin-sensitive S. epidermidis; MRSA, methicillin-resistant S. aureus; MSSA, methicillin-sensitive S. aureus. a 100 µg/mL. b p value from Dunnett’s multiple comparisons test. The respective MICs for ciprofloxacin and moxifloxacin against staphylococcal isolates were 64 and 16 µg/mL for CipR MRSE, ≤0.063 and ≤0.031 µg/mL for CipS MRSE, 32 and 16 µg/mL for CipR MSSE, ≥64 and ≥16 µg/mL for CipR MRSA, 8 and 0.25 µg/mL CipR MSSA, and 0.125 and 0.031 µg/mL for CipS MSSA.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Blondeau, J.; DeCory, H. In Vitro Time-Kill of Common Ocular Pathogens with Besifloxacin Alone and in Combination with Benzalkonium Chloride. Pharmaceuticals 2021, 14, 517. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14060517
AMA Style
Blondeau J, DeCory H. In Vitro Time-Kill of Common Ocular Pathogens with Besifloxacin Alone and in Combination with Benzalkonium Chloride. Pharmaceuticals. 2021; 14(6):517. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14060517
Chicago/Turabian StyleBlondeau, Joseph, and Heleen DeCory. 2021. "In Vitro Time-Kill of Common Ocular Pathogens with Besifloxacin Alone and in Combination with Benzalkonium Chloride" Pharmaceuticals 14, no. 6: 517. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14060517
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.