
Lysergic Acid Diethylamide, Psilocybin and Dimethyltryptamine in Depression Treatment: A Systematic Review


Abstract
:1. Introduction
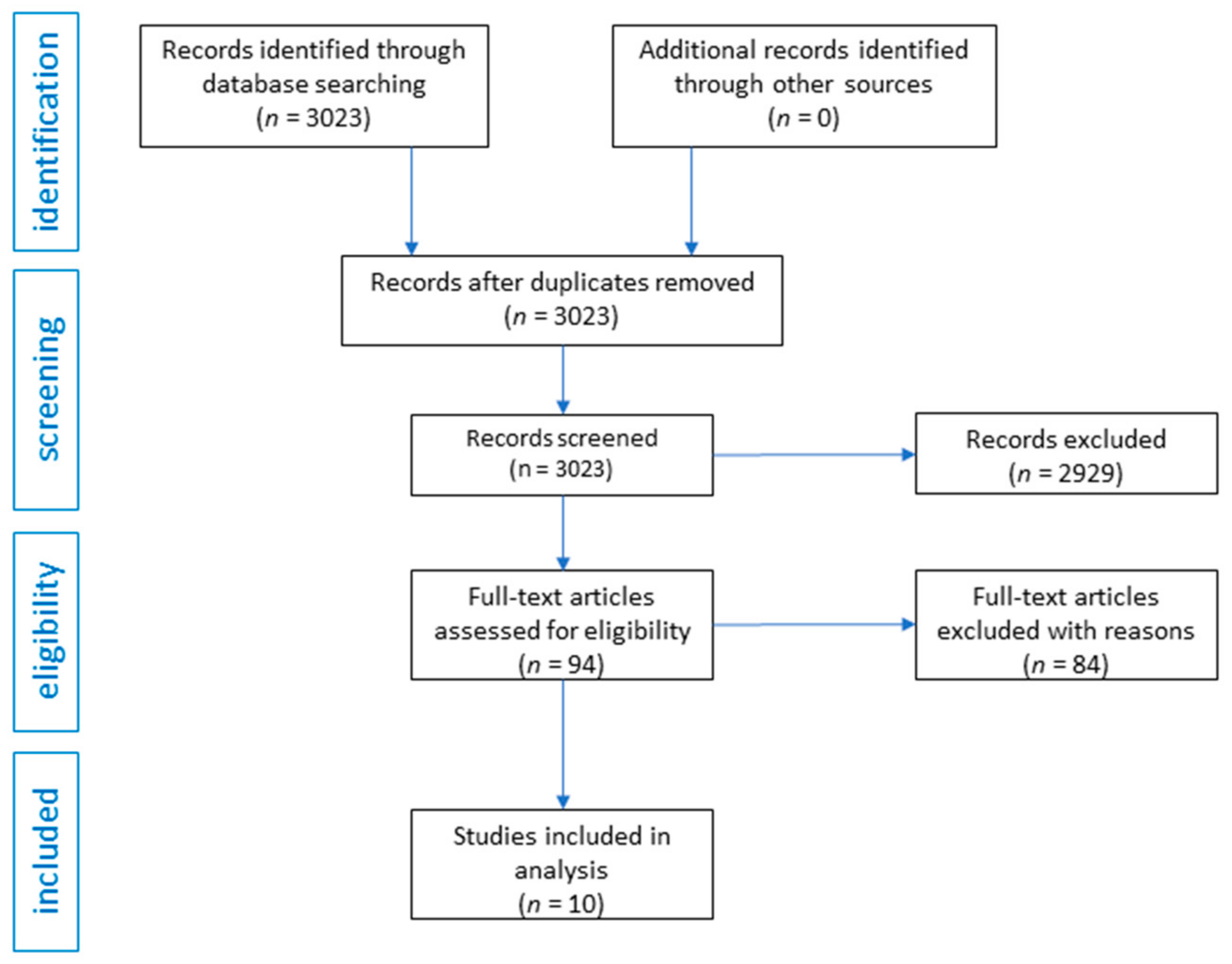
2. Material and Methods
3. Results
3.1. Primary Outcome
3.2. LSD
3.3. Psylocybin
3.4. DMT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miller, M.J.; Albarracin-Jordan, J.; Moore, C.; Capriles, J.M. Chemical evidence for the use of multiple psychotropic plants in a 1,000-year-old ritual bundle from South America. Proc. Natl. Acad. Sci. USA 2019, 116, 11207–11212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akers, B.P.; Ruiz, J.F.; Piper, A.; Ruck, C.A. Prehistoric Mural in Spain Depicting Neurotropic Psilocybe Mushrooms? Econ. Bot. 2011, 65, 121–128. [Google Scholar] [CrossRef]
- Libânio Osório Marta, R.F. Metabolism of lysergic acid diethylamide (LSD): An update. Drug Metab. Rev. 2019, 51, 378–387. [Google Scholar] [CrossRef]
- Dolder, P.; Matthias, E.; Rentsch, K.; Borgwardt, S.; Krähenbühl, S. The Pharmacology of d-Lysergic Acid Diethylamide (LSD); Department of Biomedicine, University Hospital Basel: Basel, Switzerland, 2017. [Google Scholar]
- Martín-Ruiz, R.; Puig, M.V.; Celada, P.; Shapiro, D.A.; Roth, B.L.; Mengod, G.; Artigas, F. Control of serotonergic function in medial prefrontal cortex by serotonin-2A receptors through a glutamate-dependent mechanism. J. Neurosci. 2001, 21, 9856–9866. [Google Scholar] [CrossRef] [Green Version]
- De Gregorio, D.; Comai, S.; Posa, L.; Gobbi, G. d-Lysergic Acid Diethylamide (LSD) as a Model of Psychosis: Mechanism of Action and Pharmacology. Int. J. Mol. Sci. 2016, 17, 1953. [Google Scholar] [CrossRef] [Green Version]
- Gasser, P.; Holstein, D.; Michel, Y.; Doblin, R.; Yazar-Klosinski, B.; Passie, T.; Brenneisen, R. Safety and efficacy of lysergic acid diethylamide-assisted psychotherapy for anxiety as-sociated with life-threatening diseases. J. Nerv. Ment. Dis. 2014, 202, 513–520. [Google Scholar] [CrossRef] [Green Version]
- Nichols, D.E.; Grob, C.S. Is LSD toxic? Forensic Sci. Int. 2018, 284, 41–145. [Google Scholar] [CrossRef]
- Daniel, J.; Haberman, M. Clinical potential of psilocybin as a treatment for mental health conditions. Ment. Health Clin. 2018, 7, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Studerus, E.; Kometer, M.; Hasler, F.; Vollenweider, F.X. Acute, subacute and long-term subjective effects of psilocybin in healthy humans: A pooled analysis of experimental studies. J. Psychopharmacol. 2011, 25, 434–1452. [Google Scholar] [CrossRef]
- Passie, T.; Seifert, J.; Schneider, U.; Emrich, H.M. The pharmacology of psilocybin. Addict. Biol. 2002, 7, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Barker, S.A. N, N-Dimethyltryptamine (DMT), an Endogenous Hallucinogen: Past, Present, and Future Research to Determine Its Role and Function. Front. Neurosci. 2018, 12, 536. [Google Scholar] [CrossRef] [Green Version]
- Cameron, L.P.; Olson, D.E. Dark Classics in Chemical Neuroscience: N, N-Dimethyltryptamine (DMT). ACS Chem. Neurosci. 2018, 9, 2344–2357. [Google Scholar] [CrossRef] [PubMed]
- Davis, A.K.; Barsuglia, J.P.; Lancelotta, R.; Grant, R.M.; Renn, E. The epidemiology of 5-methoxy- N, N-dimethyltryptamine (5-MeO-DMT) use: Benefits, consequences, patterns of use, subjective effects, and reasons for consumption. J. Psychopharmacol. 2018, 32, 779–792. [Google Scholar] [CrossRef]
- Simão, A.Y.; Gonçalves, J.; Duarte, A.P.; Barroso, M.; Cristóvão, A.C.; Gallardo, E. Toxicological Aspects and Determination of the Main Components of Ayahuasca: A Critical Review. Medicines 2019, 6, 106. [Google Scholar] [CrossRef] [Green Version]
- Dos Santos, R.G.; Hallak, J.E.C. Therapeutic use of serotoninergic hallucinogens: A review of the evidence and of the biological and psychological mechanisms. Neurosci. Biobehav. Rev. 2020, 108, 423–434. [Google Scholar] [CrossRef]
- Szafoni, S.; Więckiewicz, G.; Pudlo, R.; Gorczyca, P.; Piegza, M. Will MDMA-assisted psychotherapy become a breakthrough in treatment-resistant post-traumatic stress dis-order? A critical narrative review. Psychiatr. Pol. 2021, 228, 1–14. [Google Scholar] [CrossRef]
- Global Drugs Survey 2020 Key Findings Report, Executive Summary, Internet. Available online: https://www.globaldrugsurvey.com/wp-content/uploads/2021/01/GDS2020-Executive-Summary.pdf (accessed on 18 June 2021).
- Global Drugs Survey 2019 Key Findings Report, Executive Summary. Available online: https://www.globaldrugsurvey.com/gds-2019 (accessed on 18 June 2021).
- Psychedelic Therapy Could ‘Reset’ Depressed Brain. Available online: https://www.bbc.com/news/health-56373202 (accessed on 23 June 2021).
- Psychedelic Solution for Depression: British Drug Firm Starts Clinical Trials of New Treatment that Sends Patients on a Hallucinogenic Trip. Available online: https://www.dailymail.co.uk/sciencetech/article-9701763/British-firm-starts-trials-psychedelic-drug-treat-depression.html (accessed on 23 June 2021).
- Thomas, B.; Ciliska, D.; Dobbins, M.; Micucci, S. A Process for Systematically Reviewing the Literature: Providing the Research Evidence for Public Health Nursing Interventions. Worldviews Evid. Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of study quality for systematic reviews: A comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological research. J. Eval. Clin. Pract. 2010, 18, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Grob, C.S.; Danforth, A.L.; Chopra, G.S.; Marycie Hagerty, R.N.; McKay, C.R.; Halberstadt, A.L.; Greer, G.R. Pilot study of psilocybin treatment for anxiety in patients with advanced-stage cancer. Arch. Gen. Psychiatry 2011, 68, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, R.R.; Johnson, M.W.; Carducci, M.A.; Umbricht, A.; Richards, W.A.; Richards, B.D.; Cosimano, M.P.; Klinedinst, M.A. Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life-threatening cancer: A randomized double-blind trial. J. Psychopharmacol. 2016, 30, 1181–1197. [Google Scholar] [CrossRef]
- Carhart-Harris, R.L.; Bolstridge, M.; Rucker, J.; Day, C.M.; Erritzoe, D.; Kaelen, M.; Bloomfield, M.; Rickard, J.A.; Forbes, B.; Feilding, A.; et al. Psilocybin with psychological support for treatment-resistant depression: An open-label feasibility study. Lancet Psychiatry 2016, 3, 619–627. [Google Scholar] [CrossRef] [Green Version]
- Carhart-Harris, R.L.; Bolstridge, M.; Day, C.M.J.; Rucker, J.; Watts, R.; Erritzoe, D.E.; Kaelen, M.; Giribaldi, B.; Bloomfield, M.; Pilling, S.; et al. Psilocybin with psychological support for treatment-resistant depression: Six-month follow-up. Psychopharmacology 2018, 235, 399–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, S.; Bossis, A.; Guss, J.; Agin-Liebes, G.; Malone, T.; Cohen, B.; Mennenga, S.E.; Belser, A.; Kalliontzi, K.; Babb, J.; et al. Rapid and sustained symptom reduction following psilocybin treatment for anxiety and depres-sion in patients with life-threatening cancer: A randomized controlled trial. J. Psychopharmacol. 2016, 30, 1165–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, A.K.; Barrett, F.S.; May, D.G.; Cosimano, M.P.; Sepeda, N.D.; Johnson, M.W.; Finan, P.H.; Griffiths, R.R. Effects of Psilocybin-Assisted Therapy on Major Depressive Disorder: A Randomized Clinical Trial. JAMA Psychiatry 2021, 78, 481–489. [Google Scholar] [CrossRef]
- Palhano-Fontes, F.; Barreto, D.; Onias, H.; Andrade, K.C.; Novaes, M.M.; Pessoa, J.A.; Mota-Rolim, S.A.; Osório, F.L.; Sanches, R.; Dos Santos, R.G.; et al. Rapid antidepressant effects of the psychedelic ayahuasca in treatment-resistant depression: A randomized placebo-controlled trial. Psychol. Med. 2019, 49, 655–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osório Fde, L.; Sanches, R.F.; Macedo, L.R.; Santos, R.G.; Maia-de-Oliveira, J.P.; Wichert-Ana, L.; Araujo, D.B.; Riba, J.; Crippa, J.A.; Hallak, J.E. Antidepressant effects of a single dose of ayahuasca in patients with recurrent depression: A preliminary report. Braz. J. Psychiatry. 2015, 37, 13–20. [Google Scholar] [CrossRef] [Green Version]
- Sanches, R.F.; de Lima Osório, F.; Dos Santos, R.G.; Macedo, L.R.; Maia-de-Oliveira, J.P.; Wichert-Ana, L.; de Araujo, D.B.; Riba, J.; Crippa, J.A.; Hallak, J.E. Antidepressant Effects of a Single Dose of Ayahuasca in Patients with Recurrent Depression: A SPECT Study. J. Clin. Psychopharmacol. 2016, 36, 77–81. [Google Scholar] [CrossRef] [Green Version]
- Zeifman, R.J.; Singhal, N.; Dos Santos, R.G.; Sanches, R.F.; de Lima Osório, F.; Hallak, J.E.C.; Weissman, C.R. Rapid and sustained de-creases in suicidality following a single dose of ayahuasca among individuals with recurrent major depressive disorder: Results from an open-label trial. Psychopharmacology 2021, 238, 453–459. [Google Scholar] [CrossRef]
- Brito-da-Costa, A.M.; Dias-da-Silva, D.; Gomes, N.G.M.; Dinis-Oliveira, R.J.; Madureira-Carvalho, Á. Toxicokinetics and Toxicodynamics of Ayahuasca Alkaloids N,N-Dimethyltryptamine (DMT), Harmine, Harmaline and Tetrahydroharmine: Clinical and Forensic Impact. Pharmaceuticals 2020, 13, 334. [Google Scholar] [CrossRef]
- Rodrigues, A.V.; Almeida, F.J.; Vieira-Coelho, M.A. Dimethyltryptamine: Endogenous Role and Therapeutic Potential. J. Psychoact. Drugs 2019, 51, 299–310. [Google Scholar] [CrossRef]
- Espiard, M.L.; Lecardeur, L.; Abadie, P.; Halbecq, I.; Dollfus, S. Hallucinogen persisting perception disorder after psilocybin con-sumption: A case study. Eur. Psychiatry 2005, 20, 458–460. [Google Scholar] [CrossRef] [PubMed]
- Halpern, J.H.; Lerner, A.G.; Passie, T. A Review of Hallucinogen Persisting Perception Disorder (HPPD) and an Exploratory Study of Subjects Claiming Symptoms of HPPD. Curr. Top. Behav. Neurosci. 2018, 36, 333–360. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Year | Type of Study | Sample Size | Characteristic of Participants | Intervention | Results | Conclusions | QATQS Global Rating |
|---|---|---|---|---|---|---|---|---|
| Grob et al. [24] | 2011 | RCT | 12 | Subjects with depression and anxiety and advanced-stage cancer | Psylocybin in two sessions in several weeks interval (0.2 mg/kg) with 250 mg of niacin as a placebo As an efficacy measure BDI, STAI-S, STAI-T, Profile of Mood States (POMS) were used | BDI score were reduced at 6 months after treatment, STAI-T score reduction was observed at 1 and 3 months after treatment | Use of psilocybin combined with psychotherapy may provide an alternative treatment especially in the conditions with minimal response to conventional therapies, which needs to be investigated further in RCTs | 1 |
| Griffiths et al. [25] | 2016 | RCT | 51 | Subjects with depression or/and anxiety associated with life-threatening cancer | Psilocybin 22 or 30 mg/70 kg (high-dose) or placebo 1 or 3 mg/70 kg (low-dose) administered in controlled conditions in two sessions in 5 weeks interval. The effects were measured in GRID-HAM-D-17 scale and HAM-A assessed with the SIGH-A | Participants who get the high dose of psilocybin showed more significantly clinical response and symptom remission in GRID-HAM-D-17 and in HAM-A scale comparing to those patients who got low-dose therapy, those effects were sustained 6 months after treatment | Psilocybin decreases depressed mood as well as anxiety and also increase the quality of life in patients with a life-threatening cancer, the more various population of patients should be examined to evaluate the generality of psilocybin treatment | 1 |
| Carhart-Harris et al. [26] | 2016 | Non-RCT (open-label trial) | 12 | Subjects with treatment-resistant major depressive disorder (MDD) | Psylocybin 10 mg and 25 mg in two sessions with 7 days interval. Effects were assessed with QIDS-SR, Beck Depression Inventory (BDI), STAI, Snaith Hamilton Pleasure Scale (SHAPS), HAM-D, Montgomery-Asberg Depression Rating Scale and Global Assessment of Functioning (GAF) | BDI scores were reduced at 1 week, 3 and 6 months after treatment, STAI and SHAPS scores were reduced 1 week and 3 months after treatment, HAM-D and MADRS scores were reduced 1 week after treatment | Psilocybin is in need for further investigations in double-blind RCT as it seems to be effective in fighting drug-resistant MDD | 3 |
| Carhart-Harris et al. [27] | 2018 | Follow-up, Non-RCT (open-label trial) | 20 | Subjects with treatment-resistant major depressive disorder (MDD) | Psylocybin 10 mg and 25 mg in two sessions with 7 days interval. Effects were assessed with QIDS-SR (mainly) Beck Depression Inventory (BDI), STAI, Snaith Hamilton Pleasure Scale (SHAPS), HAM-D and Global Assessment of Functioning (GAF) | In 19 patients who completed all assesment time points, QIDS-SR16 scores were significantly reduced, BDI and STAI scores were reduced at 1 week, 3 and 6 months after treatment (p < 0.001), SHAPS scores were reduced at 1 week and 3 months after treatment (p < 0.001) and HAM-D and GAF scores were reduced 1 week after treatment (p < 0.001). No serious side-effects were observed during the treatment | Psilocybin is a promising tool in fighting unresponsive MDD and needs further investigations in double-blind RCT | 3 |
| Ross et al. [28] | 2016 | RCT | 29 | Subjects with depression and anxiety in life-threatening cancer | Psylocybin in two sessions (0.3 mg/kg) with a 7 days interval combined with psychotherapy and niacin (250 mg) as placebo. Efficacy was measured via STAI-T and STAI-S, HADS-A, HADS-D, HADS-T, BDI | Significant differences between study and control group, reductions on STAI-T, STAI-S, HADS-A( 58% vs. 14%), HADS-T, HADS-D and BDI (83% vs. 14%) in 1 day, 2, 6, and 7 weeks after first psylocybine session | In combination with psychotherapy in life-threatening illness psilocybin contributes to quick and sustained anti-depressant and anxiolytic effects | 2 |
| Davis et al. [29] | 2020 | RCT | 24 | Subjects with major depressive disorder (MDD) | Psilocybin 1 session 20 mg/70 kg, 2 session 30 mg/70 kg with supportive psychotherapy. Effects were evaluated in Hamilton Rating Scale for Depression (HAM-D) and in the Quick Inventory of Depressive Symptomatology-Self-Report (QIDS-SR) | After the session with psilocybin 71% of patients in 1 week and in 4 weeks showed more than 50% reduction in GRID-HAM score, 58% of participants in 1 week and 54% of participants in 4 weeks met the criteria of remission of depression; in QIDS-SR scale after psilocybin session the rapid, large decrease in mean depression score were observed which was remained 4 weeks after the treatment | Sessions with psilocybin-assisted therapy demonstrated large and sustained antidepressant effects among patients with MDD, however still further placebo-controlled studies are needed | 1 |
| Authors | Year | Type of Study | Sample Size | Characteristic of Participants | Intervention | Results | Conclusions | QATQS Global Rating |
|---|---|---|---|---|---|---|---|---|
| Palhano-Fontes et al. [30] | 2019 | RCT | 29 | Subjects with treatment-resistant major depressive disorder (MDD) | Patients received a single dose of either ayahuasca or placebo. Effects in depression severity were assessed with the Montgomery-Åsberg Depression Rating Scale (MADRS) and the Hamilton Depression Rating scale at baseline, and at 1 (D1), 2 (D2), and 7 (D7) days after dosing | Significant antidepressant effects of ayahuasca when compared with placebo at all-time points. MADRS scores were significantly lower in the ayahuasca group compared with placebo at D1 and D2 and at D7. Response rates were high for both groups at D1 and D2, and significantly higher in the ayahuasca group at D7 (64% vs. 27%). Remission rate showed a trend toward significance at D7 (36% vs. 7%) | This study brings new evidence supporting the safety and therapeutic value of ayahuasca, dosed within an appropriate setting, to help treat depression | 1 |
| Osório et al. [31] | 2015 | Non-RCT (open-label trial) | 6 | Subjects with current depressive episode | Patients received 120–200 mL of ayahuasca. Effects in depression severity were assessed with measured on the Hamilton Rating Scale for Depression (HAM-D), the Montgomery-Åsberg Depression Rating Scale (MADRS), and the Anxious-Depression subscale of the Brief Psychiatric Rating Scale (BPRS) | Statistically significant reductions of up to 82% in depressive scores were observed between baseline and 1, 7, and 21 days after ayahuasca administration | These results suggest that ayahuasca has fast-acting anxiolytic and antidepressant effects in patients with a depressive disorder | 3 |
| Sanches et al. [32] | 2016 | Non-RCT (open-label trial) | 17 | Subjects with recurrent depression episode | Patients receive ayahuasca (2.2 mL/kg) and were evaluated with the Hamilton Rating Scale for Depression, the Montgomery-Åsberg Depression Rating Scale, the Brief Psychiatric Rating Scale, the Young Mania Rating Scale, and the Clinician Administered Dissociative States Scale during acute ayahuasca effects and 1, 7, 14, and 21 days after drug intake | Increased psychoactivity (Clinician Administered Dissociative States Scale) and significant score decreases in depression-related scales (Hamilton Rating Scale for Depression, Montgomery-Åsberg Depression Rating Scale, Brief Psychiatric Rating Scale) from 80 min to day 21 | Results suggest that ayahuasca may have fast-acting and sustained antidepressive properties. These results should be replicated in randomized, double-blind, placebo-controlled trial. | 3 |
| Zeifman et al. [33] | 2020 | Non-RCT (open-label trial) | 17 | Subjects with major depressive disorder (MDD) | Patient received single dose of ayahuasca and were evaulated with The Montgomery-Åsberg Depression Rating Scale | Among individuals with suicidality at baseline (n = 15), there were significant acute (i.e., 40, 80, 140, and 180 min after administration) and post-acute (1, 7, 14, and 21 days after administration) decreases in suicidality following administration of ayahuasca | Ayahuasca could possibly lead to rapid and sustained reductions in suicidality among individuals with MDD Randomized, double-blind studies with larger sample sizes are needed to confirm this early finding | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Więckiewicz, G.; Stokłosa, I.; Piegza, M.; Gorczyca, P.; Pudlo, R. Lysergic Acid Diethylamide, Psilocybin and Dimethyltryptamine in Depression Treatment: A Systematic Review. Pharmaceuticals 2021, 14, 793. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14080793
Więckiewicz G, Stokłosa I, Piegza M, Gorczyca P, Pudlo R. Lysergic Acid Diethylamide, Psilocybin and Dimethyltryptamine in Depression Treatment: A Systematic Review. Pharmaceuticals. 2021; 14(8):793. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14080793
Chicago/Turabian StyleWięckiewicz, Gniewko, Iga Stokłosa, Magdalena Piegza, Piotr Gorczyca, and Robert Pudlo. 2021. "Lysergic Acid Diethylamide, Psilocybin and Dimethyltryptamine in Depression Treatment: A Systematic Review" Pharmaceuticals 14, no. 8: 793. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14080793