
Levetiracetam Therapeutic Drug Monitoring in a Large Cohort of Korean Epileptic Patients

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Demographic Characteristics and Descriptive Data
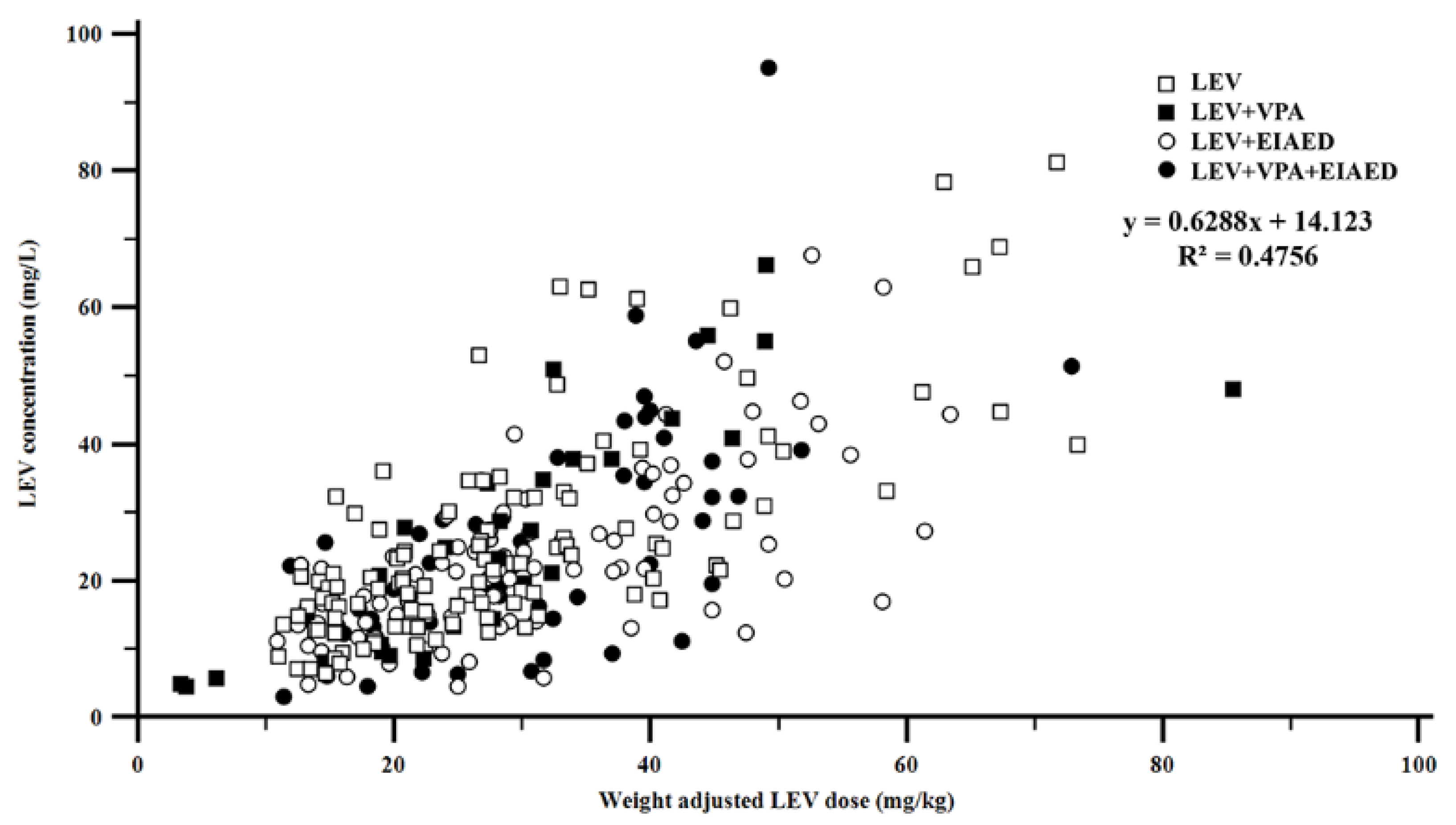
2.2. Levetiracetam Dosing and Serum Levetiracetam Concentrations
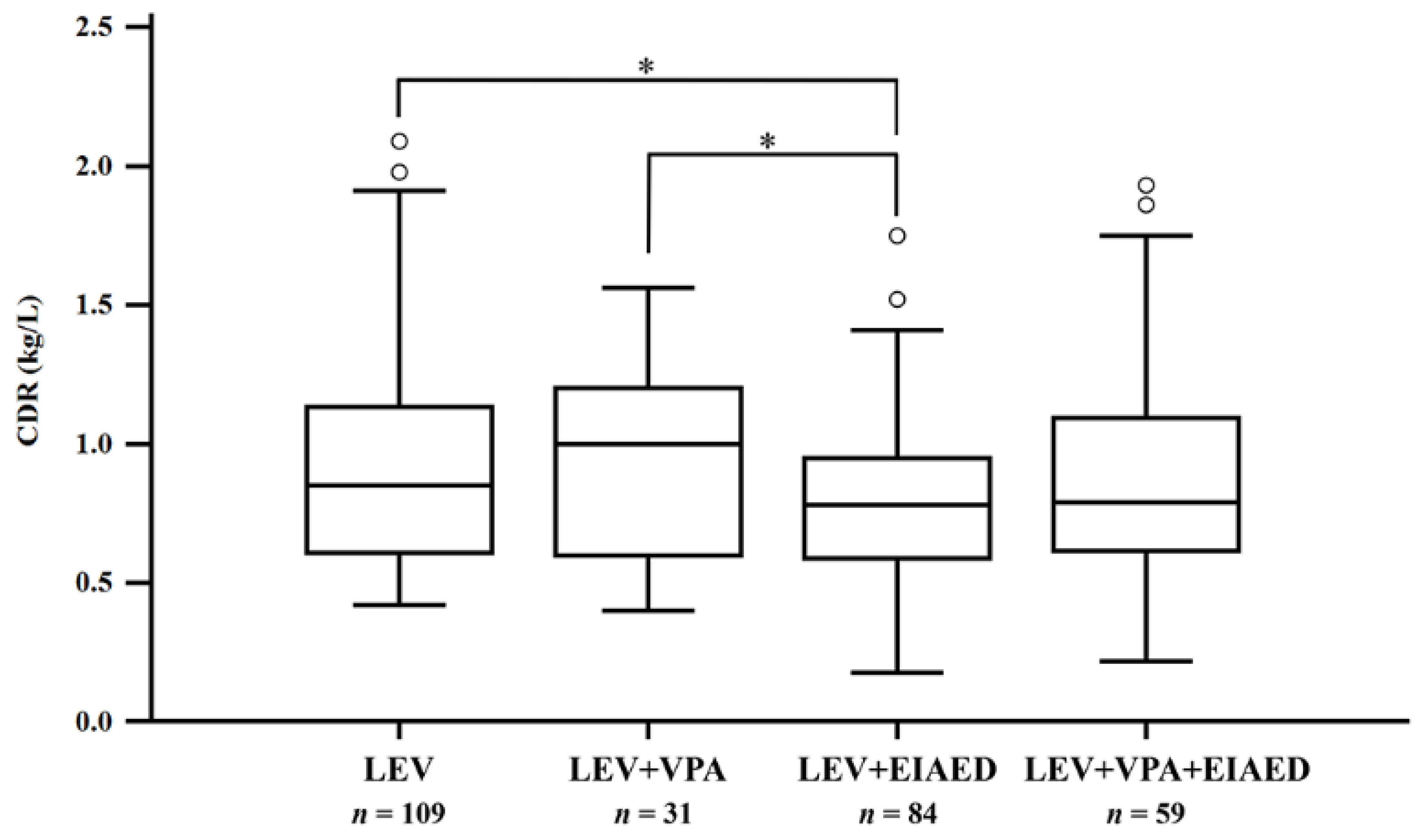
2.3. Comparison of Concentration-to-Dose Ratio between Concomitant Medication Groups
3. Discussion
4. Materials and Methods
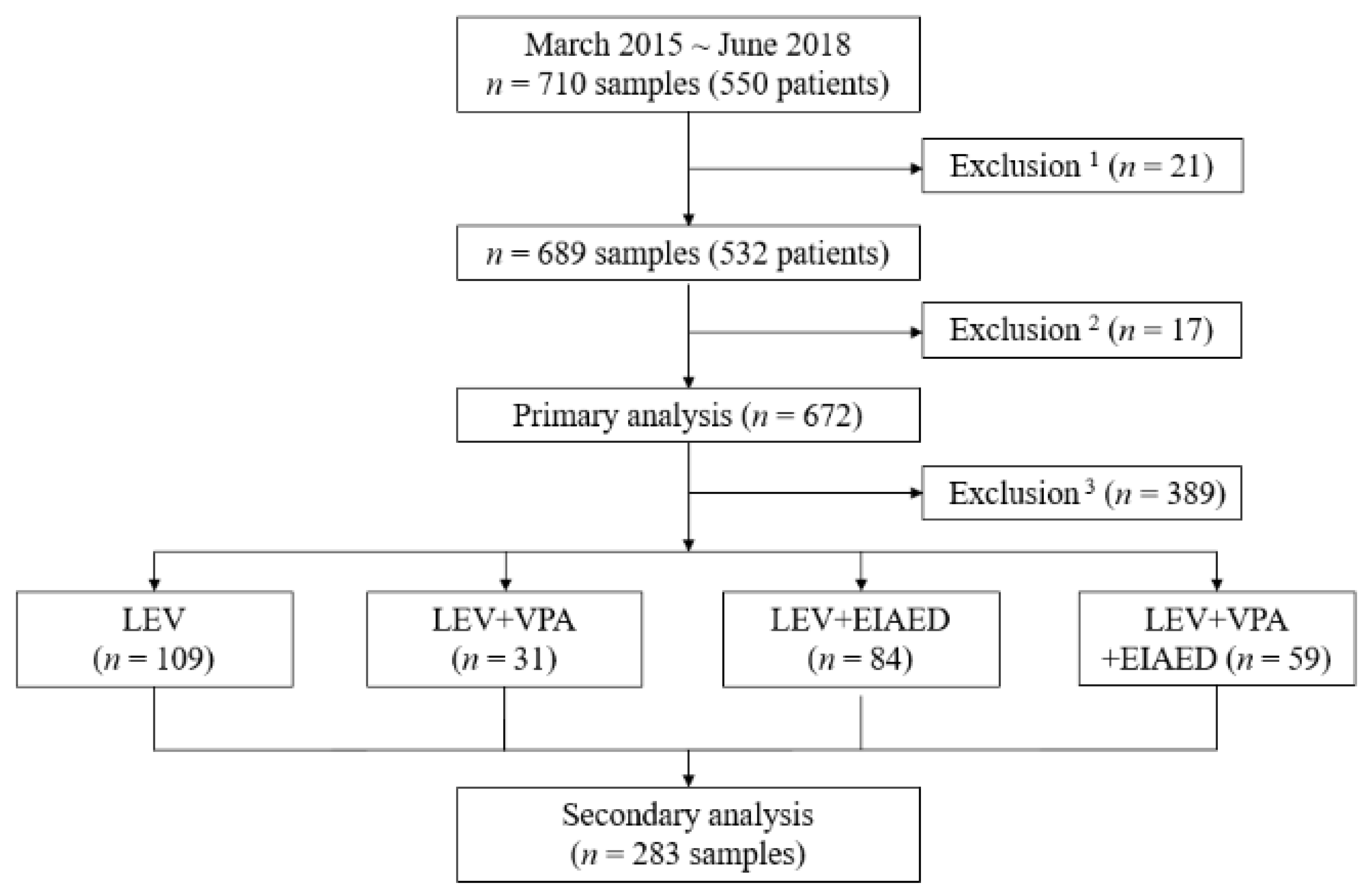
4.1. Study Subjects
4.2. Determination of Levetiracetam Concentration
4.3. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abou-Khalil, B. Levetiracetam in the treatment of epilepsy. Neuropsychiatr. Dis. Treat. 2008, 4, 507–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patsalos, P.N. Clinical pharmacokinetics of levetiracetam. Clin. Pharmacokinet. 2004, 43, 707–724. [Google Scholar] [CrossRef]
- Lancelin, F.; Franchon, E.; Kraoul, L.; Garciau, I.; Brovedani, S.; Tabaouti, K.; Landré, E.; Chassoux, F.; Paubel, P.; Piketty, M.L. Therapeutic drug monitoring of levetiracetam by high-performance liquid chromatography with photodiode array ultraviolet detection: Preliminary observations on correlation between plasma concentration and clinical response in patients with refractory epilepsy. Ther. Drug Monit. 2007, 29, 576–583. [Google Scholar] [CrossRef] [PubMed]
- May, T.W.; Rambeck, B.; Jürgens, U. Serum concentrations of Levetiracetam in epileptic patients: The influence of dose and co-medication. Ther. Drug Monit. 2003, 25, 690–699. [Google Scholar] [CrossRef]
- Jarvie, D.; Mahmoud, S.H. Therapeutic Drug Monitoring of Levetiracetam in Select Populations. J. Pharm. Pharm. Sci. A Publ. Can. Soc. Pharm. Sci. Soc. Can. Sci. Pharm. 2018, 21, 149s–176s. [Google Scholar] [CrossRef] [PubMed]
- Patsalos, P.N. Pharmacokinetic profile of levetiracetam: Toward ideal characteristics. Pharmacol. Ther. 2000, 85, 77–85. [Google Scholar] [CrossRef]
- Patsalos, P.N.; Berry, D.J.; Bourgeois, B.F.; Cloyd, J.C.; Glauser, T.A.; Johannessen, S.I.; Leppik, I.E.; Tomson, T.; Perucca, E. Antiepileptic drugs–best practice guidelines for therapeutic drug monitoring: A position paper by the subcommission on therapeutic drug monitoring, ILAE Commission on Therapeutic Strategies. Epilepsia 2008, 49, 1239–1276. [Google Scholar] [CrossRef] [PubMed]
- French, J.; Edrich, P.; Cramer, J.A. A systematic review of the safety profile of levetiracetam: A new antiepileptic drug. Epilepsy Res. 2001, 47, 77–90. [Google Scholar] [CrossRef]
- Nei, S.D.; Wittwer, E.D.; Kashani, K.B.; Frazee, E.N. Levetiracetam Pharmacokinetics in a Patient Receiving Continuous Venovenous Hemofiltration and Venoarterial Extracorporeal Membrane Oxygenation. Pharmacotherapy 2015, 35, e127–e130. [Google Scholar] [CrossRef]
- Rossetti, A.O.; Bromfield, E.B. Levetiracetam in the treatment of status epilepticus in adults: A study of 13 episodes. Eur. Neurol. 2005, 54, 34–38. [Google Scholar] [CrossRef]
- Perucca, E.; Gidal, B.E.; Baltès, E. Effects of antiepileptic comedication on levetiracetam pharmacokinetics: A pooled analysis of data from randomized adjunctive therapy trials. Epilepsy Res. 2003, 53, 47–56. [Google Scholar] [CrossRef]
- Gidal, B.E.; Baltès, E.; Otoul, C.; Perucca, E. Effect of levetiracetam on the pharmacokinetics of adjunctive antiepileptic drugs: A pooled analysis of data from randomized clinical trials. Epilepsy Res. 2005, 64, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Shorvon, S.D.; Löwenthal, A.; Janz, D.; Bielen, E.; Loiseau, P. Multicenter double-blind, randomized, placebo-controlled trial of levetiracetam as add-on therapy in patients with refractory partial seizures. European Levetiracetam Study Group. Epilepsia 2000, 41, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Contin, M.; Albani, F.; Riva, R.; Baruzzi, A. Levetiracetam therapeutic monitoring in patients with epilepsy: Effect of concomitant antiepileptic drugs. Ther. Drug Monit. 2004, 26, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, L.J.; Arif, H.; Buchsbaum, R.; Weintraub, D.; Lee, J.; Chang, J.T.; Resor, S.R., Jr.; Bazil, C.W. Effect of age and comedication on levetiracetam pharmacokinetics and tolerability. Epilepsia 2007, 48, 1351–1359. [Google Scholar] [CrossRef]
- Naik, G.S.; Kodagali, R.; Mathew, B.S.; Thomas, M.; Prabha, R.; Mathew, V.; Fleming, D.H. Therapeutic Drug Monitoring of Levetiracetam and Lamotrigine: Is There a Need? Ther. Drug Monit. 2015, 37, 437–444. [Google Scholar] [CrossRef]
- Pellock, J.M.; Glauser, T.A.; Bebin, E.M.; Fountain, N.B.; Ritter, F.J.; Coupez, R.M.; Shields, W.D. Pharmacokinetic study of levetiracetam in children. Epilepsia 2001, 42, 1574–1579. [Google Scholar] [CrossRef] [Green Version]
- Contin, M.; Mohamed, S.; Albani, F.; Riva, R.; Baruzzi, A. Levetiracetam clinical pharmacokinetics in elderly and very elderly patients with epilepsy. Epilepsy Res. 2012, 98, 130–134. [Google Scholar] [CrossRef]
- Sourbron, J.; Chan, H.; Wammes-van der Heijden, E.A.; Klarenbeek, P.; Wijnen, B.F.M.; de Haan, G.J.; van der Kuy, H.; Evers, S.; Majoie, M. Review on the relevance of therapeutic drug monitoring of levetiracetam. Seizure 2018, 62, 131–135. [Google Scholar] [CrossRef] [Green Version]
- Krasowski, M.D.; McMillin, G.A. Advances in anti-epileptic drug testing. Clin. Chim. Acta Int. J. Clin. Chem. 2014, 436, 224–236. [Google Scholar] [CrossRef]
- Johannessen Landmark, C.; Baftiu, A.; Tysse, I.; Valsø, B.; Larsson, P.G.; Rytter, E.; Johannessen, S.I. Pharmacokinetic variability of four newer antiepileptic drugs, lamotrigine, levetiracetam, oxcarbazepine, and topiramate: A comparison of the impact of age and comedication. Ther. Drug Monit. 2012, 34, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Krasowski, M.D. Therapeutic Drug Monitoring of the Newer Anti-Epilepsy Medications. Pharmaceuticals 2010, 3, 1909–1935. [Google Scholar] [CrossRef] [PubMed]
- Mathew, B.S.; Fleming, D.H.; Thomas, M.; Prabha, R.; Saravanakumar, K. An initial experience with therapeutic drug monitoring of levetiracetam as reported from a pediatric clinical setting in India. Neurol. India 2012, 60, 146–149. [Google Scholar] [CrossRef] [PubMed]
- Ito, S.; Yano, I.; Hashi, S.; Tsuda, M.; Sugimoto, M.; Yonezawa, A.; Ikeda, A.; Matsubara, K. Population Pharmacokinetic Modeling of Levetiracetam in Pediatric and Adult Patients With Epilepsy by Using Routinely Monitored Data. Ther. Drug Monit. 2016, 38, 371–378. [Google Scholar] [CrossRef]
- Otoul, C.; De Smedt, H.; Stockis, A. Lack of pharmacokinetic interaction of levetiracetam on carbamazepine, valproic acid, topiramate, and lamotrigine in children with epilepsy. Epilepsia 2007, 48, 2111–2115. [Google Scholar] [CrossRef]
- Toublanc, N.; Sargentini-Maier, M.L.; Lacroix, B.; Jacqmin, P.; Stockis, A. Retrospective population pharmacokinetic analysis of levetiracetam in children and adolescents with epilepsy: Dosing recommendations. Clin. Pharmacokinet. 2008, 47, 333–341. [Google Scholar] [CrossRef]
- Aldaz, A.; Alzueta, N.; Viteri, C. Influence of Comedication on Levetiracetam Pharmacokinetics. Ther. Drug Monit. 2018, 40, 130–134. [Google Scholar] [CrossRef]
- Dahlin, M.G.; Wide, K.; Ohman, I. Age and comedications influence levetiracetam pharmacokinetics in children. Pediatr. Neurol. 2010, 43, 231–235. [Google Scholar] [CrossRef]
- Stepanova, D.; Beran, R.G. Measurement of levetiracetam drug levels to assist with seizure control and monitoring of drug interactions with other anti-epileptic medications (AEMs). Seizure 2014, 23, 371–376. [Google Scholar] [CrossRef] [Green Version]
- Cotta, M.O.; Abdul-Aziz, M.H.; Frey, O.R.; Sime, F.B.; Roberts, J.A.; Roehr, A.C. What Are the Predictors for Achieving Therapeutic Levetiracetam Serum Concentrations in Adult Neurological Patients? Ther. Drug Monit. 2020, 42, 626–630. [Google Scholar] [CrossRef]
- Brandt, C.; Baumann, P.; Eckermann, G.; Hiemke, C.; May, T.W.; Rambeck, B.; Pohlmann-Eden, B. Therapeutic drug monitoring in epileptology and psychiatry. Nervenarzt 2008, 79, 167–174. [Google Scholar] [CrossRef]
- Johannessen, S.I.; Tomson, T. Pharmacokinetic variability of newer antiepileptic drugs: When is monitoring needed? Clin. Pharmacokinet. 2006, 45, 1061–1075. [Google Scholar] [CrossRef] [PubMed]
- Zaccara, G.; Perucca, E. Interactions between antiepileptic drugs, and between antiepileptic drugs and other drugs. Epileptic Disord. Int. Epilepsy J. Videotape 2014, 16, 409–431. [Google Scholar] [CrossRef]
- Ben-Menachem, E.; Falter, U. Efficacy and tolerability of levetiracetam 3000 mg/d in patients with refractory partial seizures: A multicenter, double-blind, responder-selected study evaluating monotherapy. European Levetiracetam Study Group. Epilepsia 2000, 41, 1276–1283. [Google Scholar] [CrossRef]
- Cereghino, J.J.; Biton, V.; Abou-Khalil, B.; Dreifuss, F.; Gauer, L.J.; Leppik, I. Levetiracetam for partial seizures: Results of a double-blind, randomized clinical trial. Neurology 2000, 55, 236–242. [Google Scholar] [CrossRef]
- Boon, P.; Chauvel, P.; Pohlmann-Eden, B.; Otoul, C.; Wroe, S. Dose-response effect of levetiracetam 1000 and 2000 mg/day in partial epilepsy. Epilepsy Res. 2002, 48, 77–89. [Google Scholar] [CrossRef]
- Weintraub, D.; Buchsbaum, R.; Spencer, H.; Hager, M.; Straka, T.; Salas-Humara, C.; Adams, D.J.; Bazil, C.W.; Resor, S.R.; Morrell, M.J.; et al. Tolerability of levetiracetam in 516 patients: Analysis by dose and serum concentration. Epilepsia 2004, 45 (Suppl. 3), 68. [Google Scholar]
- Hiemke, C.; Bergemann, N.; Clement, H.W.; Conca, A.; Deckert, J.; Domschke, K.; Eckermann, G.; Egberts, K.; Gerlach, M.; Greiner, C.; et al. Consensus Guidelines for Therapeutic Drug Monitoring in Neuropsychopharmacology: Update 2017. Pharmacopsychiatry 2018, 51, 9–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | 519 Patients 672 Samples |
|---|---|
| Patient Data | n = 519 |
| No. patients, male:female (%) | 275:244 (53.0:47.0) |
| Age, median (years) | 35 |
| Age range (Q25%–Q75%) | 2–88 (24–50) |
| Body weight, median (kg) | 63.0 |
| Body weight range (Q25%–Q75%) | 1.1–112.5 (53.3–73.0) |
| Number of measurements in single patient, n (%) | |
| Once | 424 (81.7) |
| Twice | 75 (14.5) |
| Three times or more | 20 (3.9) |
| Mean (range) | 1.3 (1–21) |
| Route of levetiracetam administration, n (%) | |
| PO | 491 (94.6) |
| IV | 26 (5.0) |
| PO and IV | 2 (0.4) |
| Requested department, n (%) | |
| Outpatient department | 404 (77.8) |
| Emergency department | 23 (4.4) |
| Inpatient | 92 (17.7) |
| Sample data | n = 672 |
| Sampling period (days) 1, n (%) | |
| <2 | 8 (1.2) |
| 2–7 (one week) | 20 (3.0) |
| 8–30 (one month) | 45 (6.7) |
| 31–365 (one year) | 115 (17.1) |
| >365 | 484 (72.0) |
| Characteristics | 519 Patients 672 Samples |
|---|---|
| Sample Data | n = 672 |
| LEV dose, median (mg/day) | 1500 |
| LEV dose, range (Q25%–Q75%) (mg/day) | 20–5000 (1000–2000) |
| LEV dose per body weight, median (mg/kg/day) | 25.5 |
| Range of LEV dose per body weight (Q25%–Q75%) | 3.03–133.0 (14.9–38.8) |
| LEV serum concentration, median (mg/L) | 17.3 |
| Range of LEV serum concentration (Q25%-Q75%) | 0.8–95.0 (8.5–28.3) |
| Sub-therapeutic level (<10 mg/L), n (%) | 201 (29.9) |
| Therapeutic level (10–40 mg/L), n (%) | 393 (58.5) |
| Supra-therapeutic level (>40 mg/L), n (%) | 78 (11.6) |
| Patient data | n = 519 |
| Number of co-prescribed drugs 1, n (%) | |
| Mean (median) | 2.08 (2) |
| Range (Q25%–Q75%) | 0–8 (1–3) |
| None | 101 (19.5) |
| One | 137 (26.4) |
| Two | 99 (19.1) |
| Three | 77 (14.8) |
| Four | 49 (9.4) |
| Five or more | 56 (10.8) |
| Group | Total | LEV (1) 1 | LEV + VPA (2) | LEV + EIAED (3) | LEV + VPA + EIAED (4) | p * | Paired Comparison ** |
|---|---|---|---|---|---|---|---|
| n | 283 | 109 | 31 | 84 | 59 | ||
| LEV concentration (mg/L) 2 | 21.6 (14.6–32.1) | 21.0 (15.6–32.1) | 23.1 (11.3–37.8) | 21.7 (14.4–28.0) | 22.2 (14.4–33.9) | 0.9335 | |
| LEV dose (mg/day) 2 | 2000 (1250–2000) | 1500 (1000–2000) | 2000 (1000–3000) | 2000 (1500–2500) | 2000 (1425–3000) | 0.0217 | (1)-(3), (1)-(4) |
| LEV dose/kg (mg/kg/day) 2 | 27.5 (19.9–38.4) | 26.7 (18.4–34.2) | 27.8 (19.0–33.6) | 28.4 (21.5–40.3) | 28.5 (21.4–39.5) | 0.2911 | |
| LEV CDR (kg/L) 2 | 0.81 (0.60–1.08) | 0.85 (0.61–1.13) | 1.00 (0.60–1.20) | 0.78 (0.59–0.95) | 0.79 (0.62–1.09) | 0.0406 | (1)-(3), (2)-(3) |
| Country | Patient (Sample) 1, n | Age, Years Median (Range) 1 | Dose, mg/Day Median (Range) 1 | LEV Conc, mg/L Median (Range) 1 | Proportion within TR | Proportion of Poly-AED | Concurrent Drugs 2 | Reference | Year |
|---|---|---|---|---|---|---|---|---|---|
| Korea | 519 (672) | 35 (2–88) | 1500 (20–5000) | 17.3 (0.8–95.0) | 58.5% | 80.5% | CBZ, PB, PHT, OXC | Our study | 2021 |
| India | 69 | 6 (1–16) | 800 (100–2000) | 14.7 (<1–53.8) | NR | 60.9% | CBZ, PB, PHT, OXC | [23] | 2012 |
| India | 330 (348) | NR (0.3–64) | NR | NR (2.4–44.9) | 56.9% | 63.5% | CBZ, PB, PHT, OXC | [16] | 2015 |
| Japan | 225 (583) | 38 (1–89) | 1200 (62.5–3000) | 12.5 (0.24–48.8) | NR | 90.2% | NS (CBZ, PHT, PB) | [24] | 2016 |
| Belgium | 94 | Mean 10.3 (4–16) | NR | NR | NR | None | NS (CBZ, VPA, TPM, LTG) | [25] | 2007 |
| Belgium | 228 (Pooled analysis) | 9.8 (3 months-18) | NR (20–60 mg/kg/day) | NR | NR | None | CBZ, PHT, PB, PRM | [26] | 2008 |
| Germany | 297 (363) | 33 (2–76) | 2500 (250–7000) | 14.2 (1.5–48.2) | NR | 94.9% | CBZ, OXC, PHT | [4] | 2003 |
| Italy | 590 (Pooled analysis) | 37 (14–70) | 2000 (1000–4000) | NR | NR | NR | NS (CBZ, PB, PHT, PRM) | [11] | 2003 |
| Italy 3 | 100 | NR | 2000 (1500–3000) 4 2000 (1312–2500) 4 | 10.4 (7.5–14.0) 4 14.7 (10.7–22.1) 4 | NR | 92.0% | CBZ, PB, PHT | [14] | 2004 |
| Italy 3 | 272 | NR (30–96) | 1750 (1000–2125) 4 1500 (1000–2000) 4 1000 (1000–1500) 4 | 12.7 (8.7–17.2) 4 15.1 (10.0–25.9) 4 23.0 (15.5–29.5) 4 | NR | 100% | CBZ, PB, PHT, OXC | [18] | 2012 |
| Spain 3 | 205 (330) | Mean 50.0 Mean 47.9 Mean 41.7 | Mean 1892 Mean 2560 Mean 2216 | Mean 20.1 Mean 17.3 Mean 20.5 | NR | 45.5% | CBZ, OXC, PB | [27] | 2018 |
| Sweden | 103 | Mean 10.2 (0–18) | NR | NR | NR | 90.3% | CBZ, ETX, PB, PHT, OXC | [28] | 2010 |
| Norway | 289 | Mean 34 (2–93) | NR | NR | NR | NR | CBZ, PB, PHT | [21] | 2012 |
| The USA 3 | 308 | Mean 25 (16–30) Mean 64 (55–88) | Mean 1990 (250–4625) Mean 1235 (125–4250) | Mean 16.2 (2.5–53.0) Mean 20.0 (3.5–85.3) | NR | 89.4% | CBZ, PB, PHT, PRM | [15] | 2007 |
| Australia | 52 | Mean 42 (19–69) | Mean 2919 (250–6000) | Mean 28 (2–100) | 61.5% | 55.8% | CBZ | [29] | 2014 |
| Australia | 130 | 71 | 1500 (250–4000) | 16.2 (9.8–26.1) 4 | 50.8% | NR | NR | [30] | 2020 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ha, C.; Lee, H.-S.; Joo, E.Y.; Shon, Y.-M.; Hong, S.B.; Seo, D.-W.; Lee, S.-Y. Levetiracetam Therapeutic Drug Monitoring in a Large Cohort of Korean Epileptic Patients. Pharmaceuticals 2021, 14, 826. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14080826
Ha C, Lee H-S, Joo EY, Shon Y-M, Hong SB, Seo D-W, Lee S-Y. Levetiracetam Therapeutic Drug Monitoring in a Large Cohort of Korean Epileptic Patients. Pharmaceuticals. 2021; 14(8):826. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14080826
Chicago/Turabian StyleHa, Changhee, Hyun-Seung Lee, Eun Yeon Joo, Young-Min Shon, Seung Bong Hong, Dae-Won Seo, and Soo-Youn Lee. 2021. "Levetiracetam Therapeutic Drug Monitoring in a Large Cohort of Korean Epileptic Patients" Pharmaceuticals 14, no. 8: 826. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14080826