
Safety, Tolerability, Pharmacokinetics, and Pharmacodynamics of Cholic Acid (MT921) after a Subcutaneous Injection in the Submental Area to Humans

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. Subjects
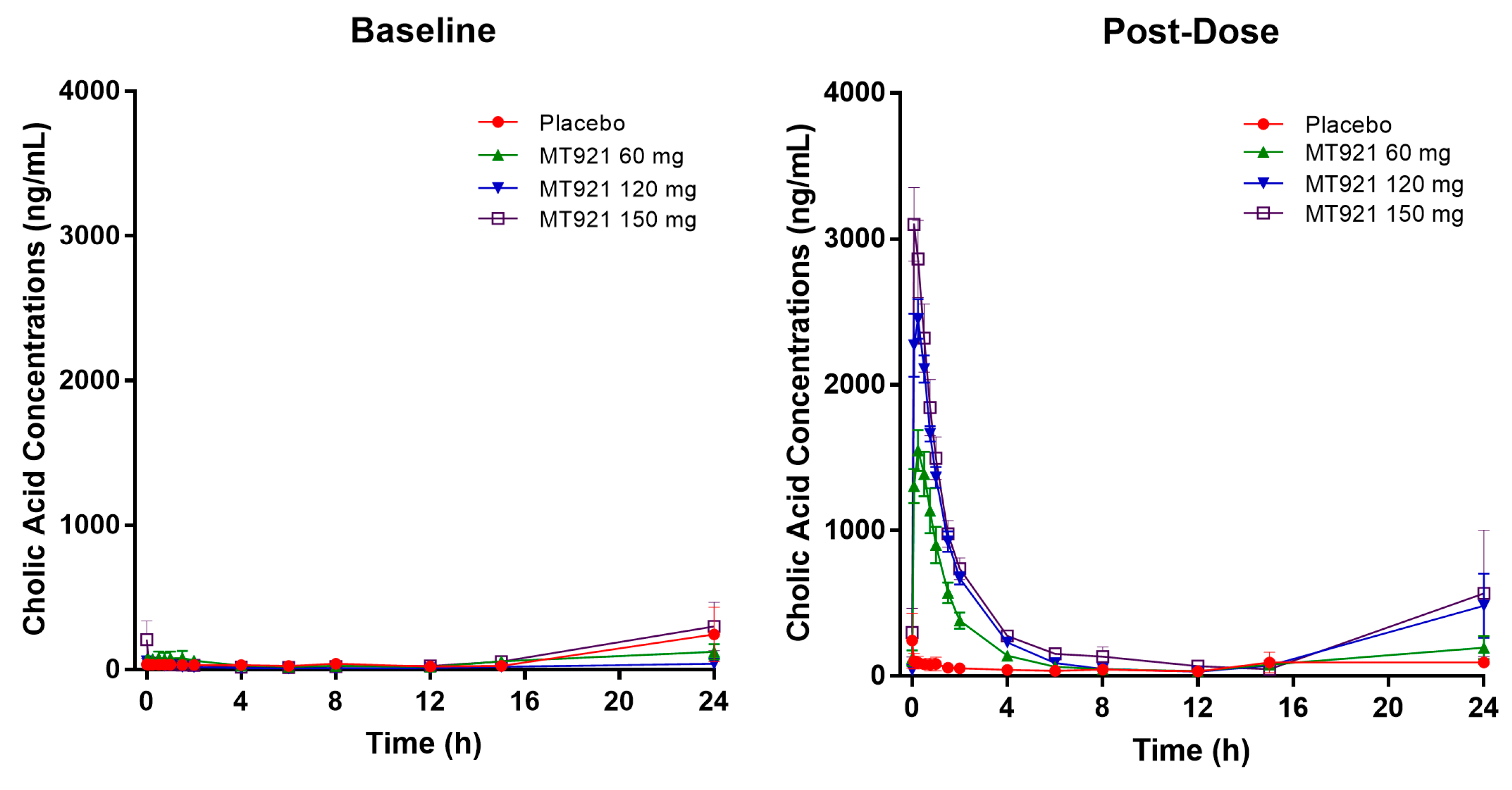
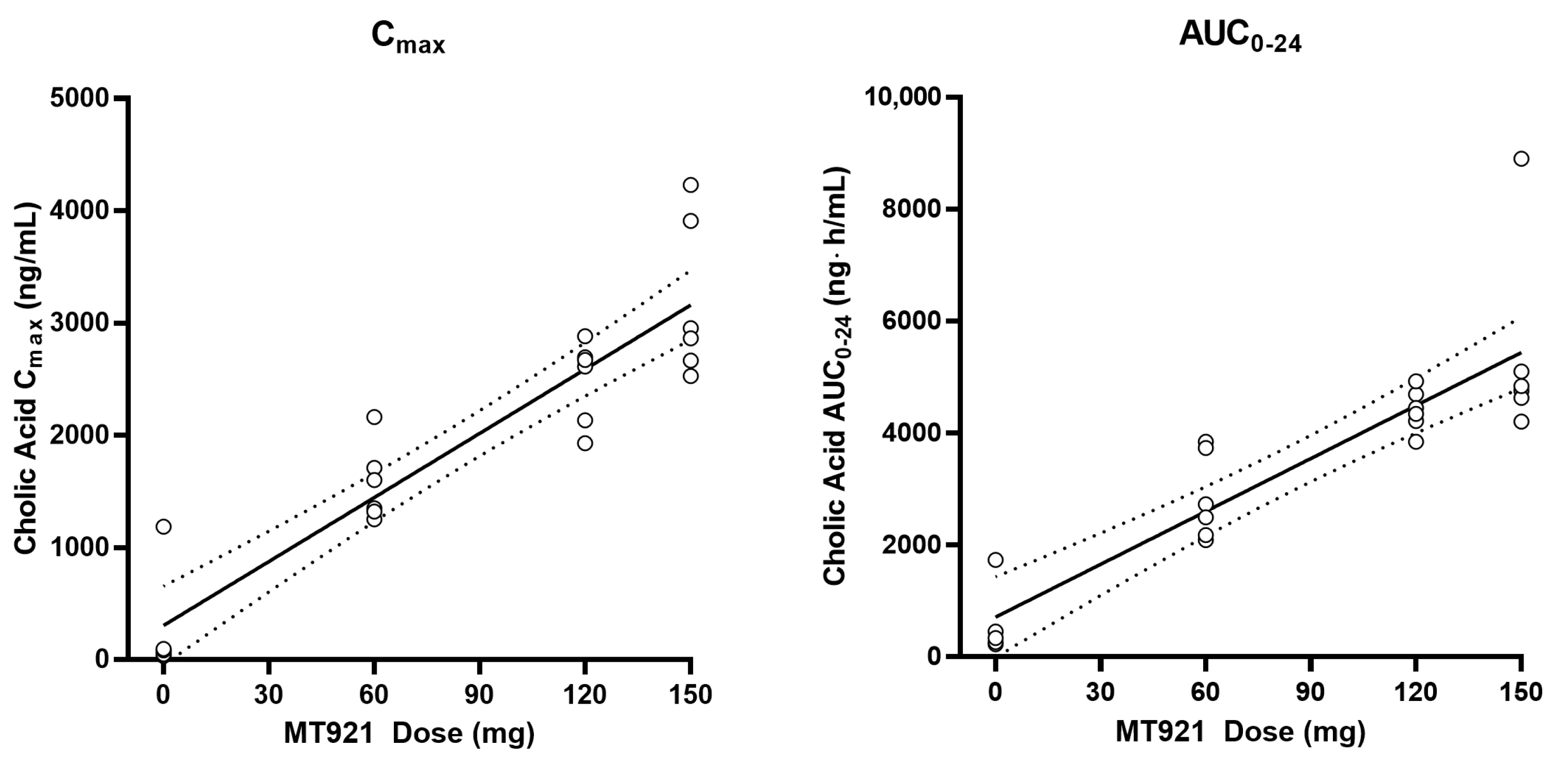
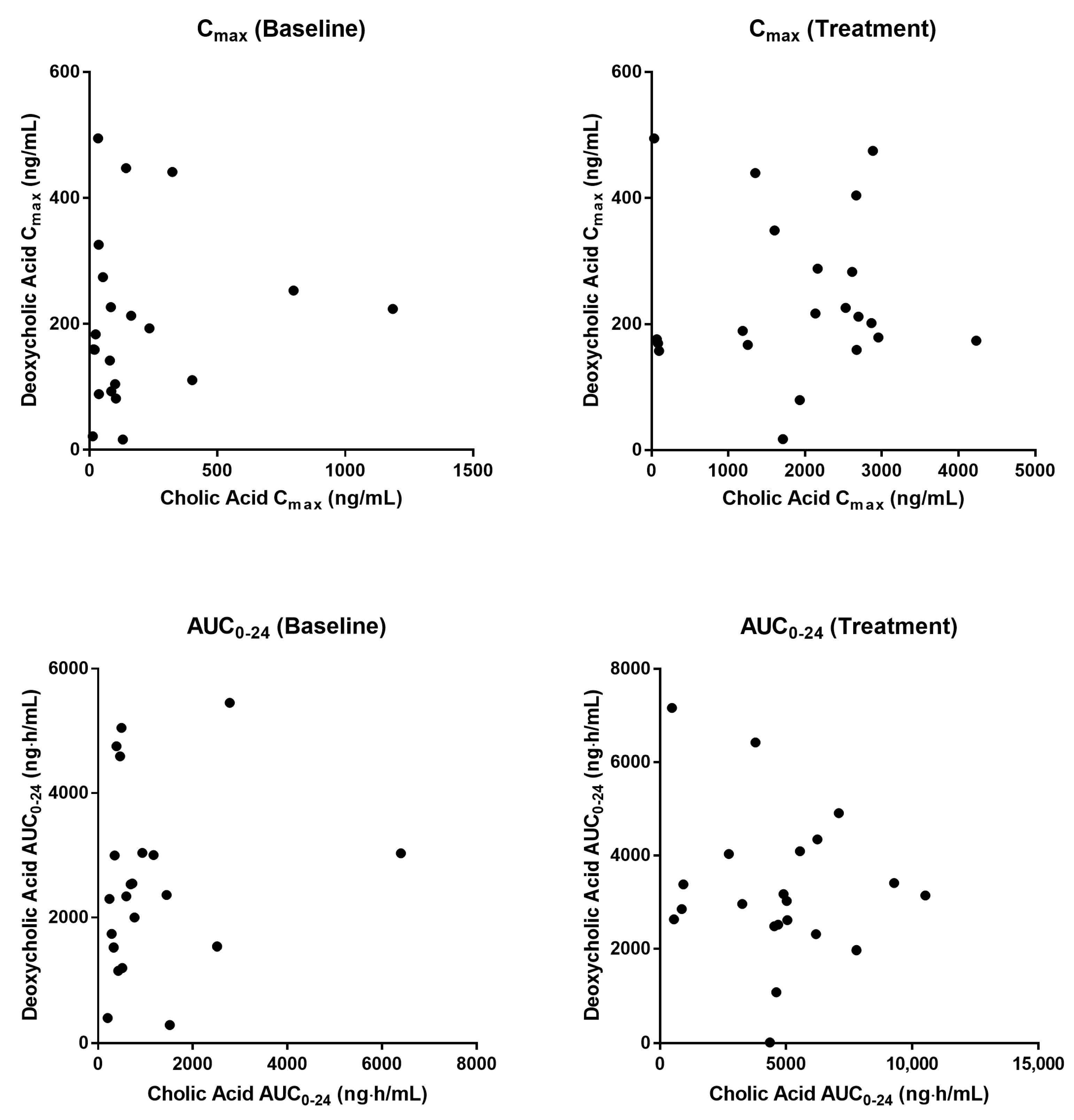
2.2. Pharmacokinetics of Cholic Acid and Deoxycholic Acid
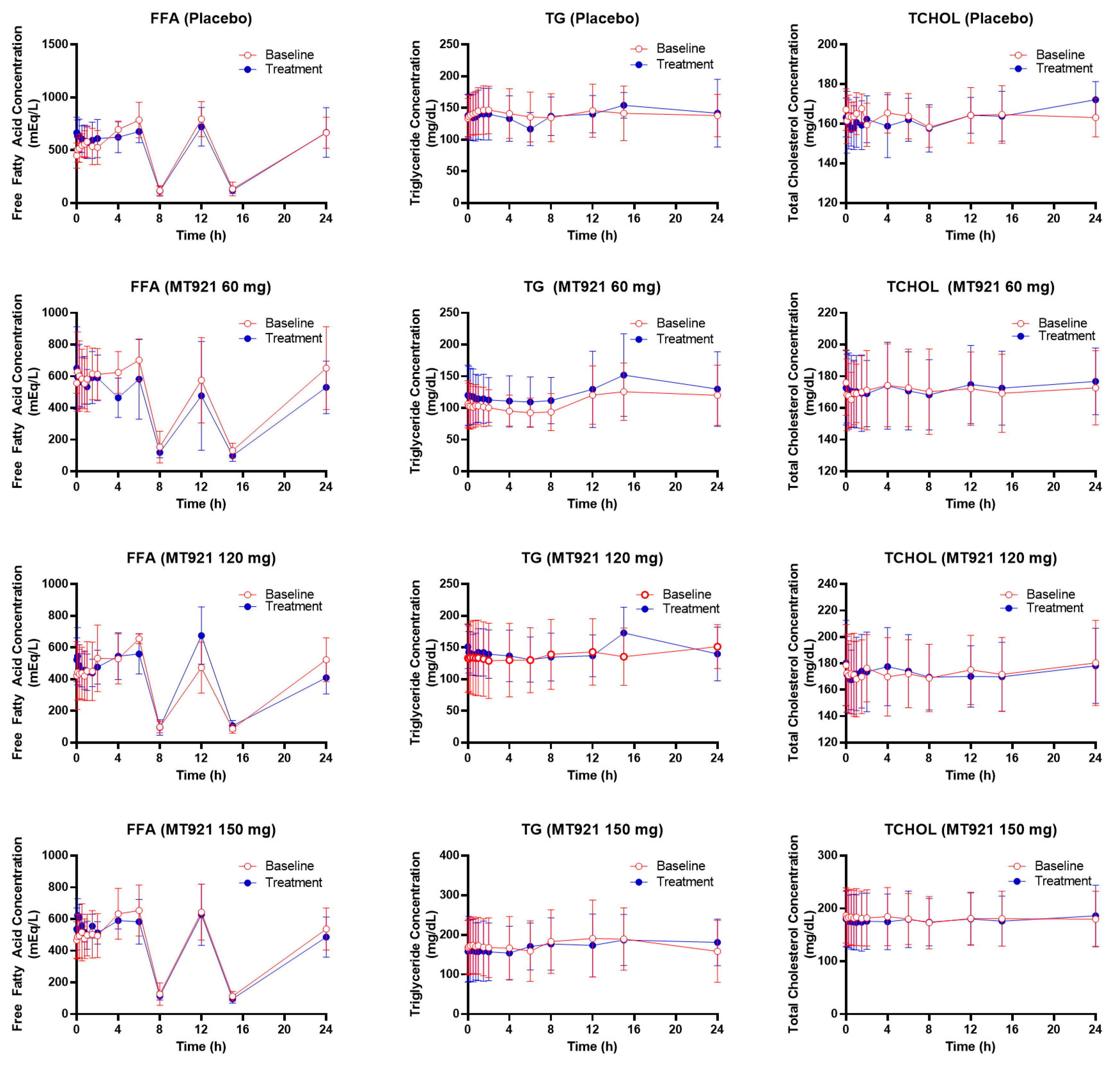
2.3. Pharmacodynamics
2.4. Safety and Tolerability
3. Discussion
4. Materials and Methods
4.1. Subjects
4.2. Study Design
4.3. Determination of Plasma Concentrations of Cholic Acid and Deoxycholic Acid
4.4. Pharmacokinetic/Pharmacodynamic Analysis
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ellenbogen, R.; Karlin, J.V. Visual criteria for success in restoring the youthful neck. Plast. Reconstr. Surg. 1980, 66, 826–837. [Google Scholar] [CrossRef]
- Raveendran, S.S.; Anthony, D.J.; Ion, L. An anatomic basis for volumetric evaluation of the neck. Aesthetic Surg. J. 2012, 32, 685–691. [Google Scholar] [CrossRef] [Green Version]
- Baumann, L.; Shridharani, S.M.; Humphrey, S.; Gallagher, C.J. Personal (Self) Perceptions of Submental Fat Among Adults in the United States. Dermatol. Surg. Off. Publ. Am. Soc. Dermatol. Surg. 2019, 45, 124–130. [Google Scholar] [CrossRef]
- 2019 Consumer Survey on Cosmetic Dermatologic Procedures: American Society for Dermatologic Surgery. 2019. Available online: https://www.asds.net/medical-professionals/practice-resources/asds-consumer-survey-on-cosmetic-dermatologic-procedures (accessed on 16 October 2019).
- 2018 Plastic Surgery Statistics Report: American Society of Plastic Surgeons. Available online: https://www.plasticsurgery.org/news/plastic-surgery-statistics (accessed on 16 October 2019).
- Koehler, J. Complications of neck liposuction and submentoplasty. Oral Maxillofac. Surg. Clin. N. Am. 2009, 21, 43–52. [Google Scholar] [CrossRef]
- KYBELLA (Deoxycholic Acid) Injection: Highlights of Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/206333s001lbl.pdf (accessed on 16 October 2019).
- Jones, D.H.; Carruthers, J.; Joseph, J.H.; Callender, V.D.; Walker, P.; Lee, D.R.; Subramanian, M.; Lizzul, P.F.; Gross, T.M. REFINE-1, a Multicenter, Randomized, Double-Blind, Placebo-Controlled, Phase 3 Trial With ATX-101, an Injectable Drug for Submental Fat Reduction. Dermatol. Surg. Off. Publ. Am. Soc. Dermatol. Surg. 2016, 42, 38–49. [Google Scholar] [CrossRef]
- Humphrey, S.; Sykes, J.; Kantor, J.; Bertucci, V.; Walker, P.; Lee, D.R.; Lizzul, P.F.; Gross, T.M.; Beddingfield, F.C., III. ATX-101 for reduction of submental fat: A phase III randomized controlled trial. J. Am. Acad. Dermatol. 2016, 75, 788–797.e7. [Google Scholar] [CrossRef] [Green Version]
- Chiang, J.Y. Bile acid metabolism and signaling. Compr. Physiol. 2013, 3, 1191–1212. [Google Scholar] [PubMed] [Green Version]
- CHOLBAM (Cholic Acid) Capsules: Highlights of Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/205750lbl.pdf (accessed on 7 October 2019).
- Vyvoda, O.S.; Coleman, R.; Holdsworth, G. Effects of different bile salts upon the composition and morphology of a liver plasma membrane preparation. Deoxycholate is more membrane damaging than cholate and its conjugates. Biochim. Biophys. Acta 1977, 465, 68–76. [Google Scholar] [CrossRef]
- Ryu, H.J.; Moon, H.K.; Lee, J.; Yang, G.H.; Yang, S.Y.; Yun, H.Y. Evaluation for Potential Drug-Drug Interaction of MT921 Using In Vitro Studies and Physiologically-Based Pharmacokinetic Models. Pharmaceuticals 2021, 14, 654. [Google Scholar] [CrossRef]
- Einarsson, K.; Reihner, E.; Ewerth, S.; Bjorkhem, I. Serum concentrations of unconjugated and conjugated cholic acid in portal venous and systemic venous blood of fasting man. Scand. J. Clin. Lab. Investig. 1989, 49, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Yang, J.; Xiang, D.; Li, G.; Liu, D.; Zhang, C. Circadian rhythms and bile acid homeostasis: A comprehensive review. Chronobiol. Int. 2020, 37, 618–628. [Google Scholar] [CrossRef] [PubMed]
- Al-Khaifi, A.; Straniero, S.; Voronova, V.; Chernikova, D.; Sokolov, V.; Kumar, C.; Angelin, B.; Rudling, M. Asynchronous rhythms of circulating conjugated and unconjugated bile acids in the modulation of human metabolism. J. Intern. Med. 2018, 284, 546–559. [Google Scholar] [CrossRef] [PubMed]
- Chiang, J.Y. Bile acids: Regulation of synthesis. J. Lipid Res. 2009, 50, 1955–1966. [Google Scholar] [CrossRef] [Green Version]
- Walker, P.; Fellmann, J.; Lizzul, P.F. A phase I safety and pharmacokinetic study of ATX-101: Injectable, synthetic deoxycholic acid for submental contouring. J. Drugs Dermatol. 2015, 14, 279–287. [Google Scholar]
- Angelin, B.; Bjorkhem, I. Postprandial serum bile acids in healthy man. Evidence for differences in absorptive pattern between individual bile acids. Gut 1977, 18, 606–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, D.W.; Setchell, K.D. Bile acid biosynthesis. Biochemistry 1992, 31, 4737–4749. [Google Scholar] [CrossRef]
- LaRusso, N.F.; Szczepanik, P.A.; Hofmann, A.F. Effect of deoxycholic acid ingestion on bile acid metabolism and biliary lipid secretion in normal subjects. Gastroenterology 1977, 72, 132–140. [Google Scholar] [CrossRef]
- Carulli, N.; Ponz de Leon, M.; Zironi, F.; Iori, R.; Loria, P. Bile acid feeding and hepatic sterol metabolism: Effect of deoxycholic acid. Gastroenterology 1980, 79, 637–641. [Google Scholar] [CrossRef]
- Cunha, K.S.; Lima, F.; Cardoso, R.M. Efficacy and safety of injectable deoxycholic acid for submental fat reduction: A systematic review and meta-analysis of randomized controlled trials. Expert Rev. Clin. Pharmacol. 2021, 14, 383–397. [Google Scholar] [CrossRef]
- Farina, G.A.; Cherubini, K.; de Figueiredo, M.A.Z.; Salum, F.G. Deoxycholic acid in the submental fat reduction: A review of properties, adverse effects, and complications. J. Cosmet. Dermatol. 2020, 19, 2497–2504. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.P.; Vandenhende, F.R.; DeSante, K.A.; Farid, N.A.; Welch, P.A.; Callaghan, J.T.; Forgue, S.T. Confidence interval criteria for assessment of dose proportionality. Pharm. Res. 2000, 17, 1278–1283. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Placebo (N = 6) | 60 mg (N = 6) | 120 mg (N = 6) | 150 mg (N = 6) | Total (N = 24) | |
|---|---|---|---|---|---|
| Age (years) | 26.7 ± 3.7 | 34.7 ± 12.0 | 32.7 ± 11.4 | 27.8 ± 4.4 | 30.5 ± 8.9 |
| Height (cm) | 172.5 ± 5.3 | 172.8 ± 5.7 | 175.7 ± 5.5 | 172.0 ± 4.0 | 173.3 ± 5.0 |
| Weight (kg) | 83.57 ± 6.65 | 81.30 ± 10.38 | 81.92 ± 8.14 | 83.23 ± 5.88 | 82.50 ± 7.47 |
| BMI (kg/m2) | 28.05 ± 1.10 | 27.11 ± 2.11 | 26.48 ± 1.18 | 28.12 ± 1.39 | 27.44 ± 1.56 |
| Analyte | Parameter | Placebo (N = 6) | 60 mg (N = 6) | 120 mg (N = 6) | 150 mg (N = 6) |
|---|---|---|---|---|---|
| Cholic Acid | Tmax (h) | 0.04 (0–15) | 0.25 (0.08–0.5) | 0.25 (0.08–0.25) | 0.08 (0.08–0.25) |
| Cmax (ng/mL) | 319 ± 451 | 1568 ± 342 | 2488 ± 370 | 3193 ± 703 | |
| Baseline adjusted Cmax (ng/mL) | 70 ± 156 | 1413 ± 291 | 2400 ± 342 | 2769 ± 663 | |
| AUC0-24 (ng∙h/mL) | 1618 ± 1501 | 4262 ± 1185 | 7071 ± 2505 | 8344 ± 6851 | |
| Baseline adjusted AUC0-24 (ng∙h/mL) | −67 ± 2141 | 2887 ± 1108 | 6582 ± 2344 | 6319 ± 4498 | |
| Deoxycholic Acid | Tmax (h) | 8 (0–12) | 24 (0.25–24) | 24 (24–24) | 24 (0.08–24) |
| Cmax (ng/mL) | 237 ± 144 | 252 ± 164 | 237 ± 135 | 237 ± 96 | |
| Baseline adjusted Cmax (ng/mL) | −35 ± 46 | 57 ± 147 | 64 ± 205 | 62 ± 53 | |
| AUC0-24 (ng∙h/mL) | 4009 ± 1844 | 3383 ± 2329 | 2701 ± 1077 | 3065 ± 1062 | |
| Baseline adjusted AUC0-24 (ng∙h/mL) | 869 ± 922 | 586 ± 1220 | 424 ± 917 | 970 ± 798 |
| Analyte | Parameter | Placebo (N = 6) | MT921 60 mg (N = 6) | MT921 120 mg (N = 6) | MT921 150 mg (N = 6) |
|---|---|---|---|---|---|
| Free Fatty Acid | Emax (mEq/L) | 844.50 ± 126.98 | 832.00 ± 287.24 | 738.67 ± 158.42 | 732.17 ± 132.42 |
| AUEC (mEq∙h/L) | 11,010.61 ± 2183.47 | 8846.40 ± 2277.39 | 8739.81 ± 1093.95 | 9255.14 ± 1385.66 | |
| Baseline adjusted Emax (mEq/L) | 2.00 ± 132.58 | 31.17 ± 217.58 | 41.67 ± 161.63 | −36.50 ± 197.70 | |
| Baseline adjusted AUEC (mEq∙h/L) | −487.36 ± 1314.18 | −1799.47 ± 2301.01 | 106.26 ± 1158.29 | −532.02 ± 2078.38 | |
| Triglyceride | Emax (mg/dL) | 167.67 ± 39.50 | 153.83 ± 65.63 | 178.00 ± 40.8 | 200.50 ± 67.64 |
| AUEC (mg∙h/dL) | 3381.84 ± 704.86 | 3069.19 ± 1217.15 | 3508.22 ± 857.22 | 4201.19 ± 1576.94 | |
| Baseline adjusted Emax (mg/dL) | 10.17 ± 25.79 | 22.67 ± 27.62 | 15.17 ± 17.37 | −11.17 ± 30.11 | |
| Baseline adjusted AUEC (mg∙h/dL) | 10.51 ± 271.19 | 390.99 ± 469.07 | 181.05 ± 430.11 | −28.40 ± 402.08 | |
| Total Cholesterol | Emax (mg/dL) | 174.50 ± 10.69 | 181.50 ± 24.80 | 184.00 ± 29.71 | 190.33 ± 57.99 |
| AUEC (mg∙h/dL) | 3929.37 ± 249.66 | 4146.27 ± 548.96 | 4144.37 ± 629.21 | 4279.70 ± 1219.62 | |
| Baseline adjusted Emax (mg/dL) | 1.50 ± 10.56 | 1.67 ± 7.89 | −1.50 ± 4.85 | −0.33 ± 10.25 | |
| Baseline adjusted AUEC (mg∙h/dL) | 10.07 ± 94.89 | 36.32 ± 241.13 | −18.95 ± 90.91 | −42.69 ± 156.79 |
| Adverse Event | Placebo | MT921 60 mg | MT921 120 mg | MT921 150 mg |
|---|---|---|---|---|
| Injection Site Bruising | - | [2] 5.5 (5–6) | [5] 18 (6–20) | [2] 14 (8–20) |
| Injection Site Erythema | - | [1] 1 (1–1) | [1] 2 (2–2) | [3] 2 (2–2) |
| Injection Site Hypoesthesia | - | [1] 9 (9–9) | [1] 62 (62–62) | - |
| Injection Site Nodule | - | [1] 17 (17–17) | - | - |
| Injection Site Edema | [1] 3 (3–3) | [6] 5 (4–5) | [6] 16.5 (6–36) | [6] 23 (8–27) |
| Injection Site Pain | - | [6] 1.5 (1–4) | [6] 11 (1–36) | [6] 20 (8–23) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, H.; Park, J.-W.; Kim, D.-H.; Seo, S.-H.; Kim, K.-A.; Lee, W.-S.; Park, J.-Y. Safety, Tolerability, Pharmacokinetics, and Pharmacodynamics of Cholic Acid (MT921) after a Subcutaneous Injection in the Submental Area to Humans. Pharmaceuticals 2021, 14, 830. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14080830
Chung H, Park J-W, Kim D-H, Seo S-H, Kim K-A, Lee W-S, Park J-Y. Safety, Tolerability, Pharmacokinetics, and Pharmacodynamics of Cholic Acid (MT921) after a Subcutaneous Injection in the Submental Area to Humans. Pharmaceuticals. 2021; 14(8):830. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14080830
Chicago/Turabian StyleChung, Hyewon, Jin-Woo Park, Dai-Hyun Kim, Soo-Hong Seo, Kyoung-Ah Kim, Woo-Shun Lee, and Ji-Young Park. 2021. "Safety, Tolerability, Pharmacokinetics, and Pharmacodynamics of Cholic Acid (MT921) after a Subcutaneous Injection in the Submental Area to Humans" Pharmaceuticals 14, no. 8: 830. https://0-doi-org.brum.beds.ac.uk/10.3390/ph14080830