NSAIDs and Acute Pancreatitis: A Systematic Review

{kind=link}
Abstract
:1. Introduction
2. Literature Search
3. NSAIDs as Inducers of Acute Pancreatitis
4. The Prophylactic Use of NSAIDs for Preventing Post-ERCP Acute Pancreatitis
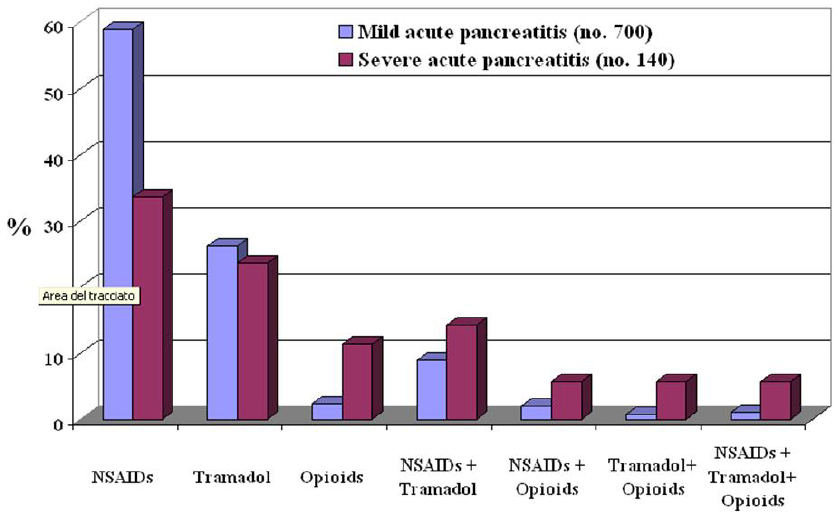
5. NSAIDs for Treating Pain in Acute Pancreatitis

6. Conclusions
References and Notes
- Ebbehoj, N.; Friis, J.; Svendsen, L.B.; Bulow, S.; Madsen, P. Indomethacin treatment of acute pancreatitis. A controlled double-blind trial. Scand. J. Gastroenterol. 1985, 20, 798–800. [Google Scholar] [CrossRef] [PubMed]
- Jakobs, R.; Adamek, M.U.; von Bubnoff, A.C.; Riemann, J.F. Buprenorphine or procaine for pain relief in acute pancreatitis. A prospective randomized study. Scand. J. Gastroenterol. 2000, 35, 1319–1323. [Google Scholar] [CrossRef] [PubMed]
- Stevens, M.; Esler, R.; Asher, G. Transdermal fentanyl for the management of acute pancreatitis pain. Appl. Nurs. Res. 2002, 15, 102–110. [Google Scholar]
- Kahl, S.; Zimmermann, S.; Pross, M.; Schulz, H.U.; Schmidt, U.; Malfertheiner, P. Procaine hydrochloride fails to relieve pain in patients with acute pancreatitis. Digestion 2004, 69, 5–9. [Google Scholar]
- Mennecier, D.; Ceppa, F.; Sinayoko, L.; Corberand, D.; Harnois, F.; Thiolet, C.; Farret, O. Acute pancreatitis after treatment by celecoxib. Gastroenterol. Clin. Biol. 2007, 31, 668–669. [Google Scholar]
- Heluwaert, F.; Pofelski, J.; Germain, E.; Roblin, X. Piroxicam and acute pancreatitis. Gastroenterol. Clin. Biol. 2006, 30, 635–636. [Google Scholar]
- Mete, D.; Milon, A.; Belon, G.; Gatina, J.H. Acute pancreatitis and ketoprofen. Gastroenterol. Clin. Biol. 2001, 25, 721–722. [Google Scholar] [PubMed]
- Maroy, B. Benign acute pancreatitis probably due to taking ketoprofen. Therapie 1998, 53, 602–603. [Google Scholar]
- Flamenbaum, M.; Abergel, A.; Marcato, N.; Zenut, M.; Kemeny, J.L.; Cassan, P. Regressive fulminant hepatitis, acute pancreatitis and renal insufficiency after taking ketoprofen. Gastroenterol. Clin. Biol. 1998, 22, 975–976. [Google Scholar] [PubMed]
- Aygencel, G.; Akbuga, B.; Keles, A. Acute pancreatitis following naproxen intake. Eur. J. Emerg. Med. 2006, 13, 372. [Google Scholar]
- Mahjoub, W.; Jarboui, S.; Ben Moussa, M.; Abdesselem, M.M.; Zaouche, A. Indomethacin-induced pancreatitis: A second case report. JOP 2006, 7, 321–323. [Google Scholar]
- Memis, D.; Akalin, E.; Yucel, T. Indomethacin-induced pancreatitis: A case report. JOP 2005, 6, 344–347. [Google Scholar]
- Nind, G.; Selby, W. Acute pancreatitis: A rare complication of celecoxib. Intern. Med. J. 2002, 32, 624–625. [Google Scholar]
- Amaravadi, R.K.; Jacobson, B.C.; Solomon, D.H.; Fischer, M.A. Acute pancreatitis associated with rofecoxib. Am. J. Gastroenterol. 2002, 97, 1077–1078. [Google Scholar]
- Baciewicz, A.M.; Sokos, D.R.; King, T.J. Acute pancreatitis associated with celecoxib. Ann. Intern. Med. 2000, 132, 680. [Google Scholar]
- Carrillo-Jimenez, R.; Nurnberger, M. Celecoxib-induced acute pancreatitis and hepatitis: A case report. Arch. Intern. Med. 2000, 160, 553–554. [Google Scholar]
- Castiella, A.; Lopez, P.; Bujanda, L.; Arenas, J.I. Possible association of acute pancreatitis with naproxen. J. Clin. Gastroenterol. 1995, 21, 258. [Google Scholar]
- Murray, B.; Carter, R.; Imrie, C.; Evans, S.; O'Suilleabhain, C. Diclofenac reduces the incidence of acute pancreatitis after endoscopic retrograde cholangiopancreatography. Gastroenterology 2003, 124, 1786–1791. [Google Scholar]
- Kim, K.H.; Kim, T.N.; Jang, B.I. A case of acute pancreatitis caused by 5-aminosalicylic acid suppositories in a patient with ulcerative colitis. Korean J. Gastroenterol. 2007, 50, 379–383. [Google Scholar]
- Montano Loza, A.; Garcia Correa, J.; Gonzalez Ojeda, A.; Fuentes Orozco, C.; Davalos Cobian, C.; Rodriguez Lomeli, X. Prevention of hyperamilasemia and pancreatitis after endoscopic retrograde cholangiopancreatography with rectal administration of indomethacin. Rev. Gastroenterol. Mex. 2006, 71, 262–267. [Google Scholar]
- Vlasov, A.I.; Berezin, V.A.; Gerasimenko, A.V.; Mosina, L.M.; Saushev, I.V. Dimephosphon in complex therapy of acute edematous pancreatitis. Vestn. Khir. Im. I. I. Grek. 2003, 162, 81–84. [Google Scholar]
- Bulychev, V.F.; Vakhrushev, Ia.M. Therapy of patients with chronic pancreatitis of alcoholic etiology by dalagrin and laser therapy of the blood. Klin. Med. (Mosk) 2000, 78, 43–45. [Google Scholar]
- Schworer, H.; Ramadori, G. Acute pancreatitis--adverse effect of 5-aminosalicylic acid (mesalazine) in various galenic dosage forms. Dtsch. Med. Wochenschr. 2000, 125, 1328–1330. [Google Scholar]
- Glintborg, B. Pancreatitis in a patient with Crohn disease treated with mesalazine and azathioprine. Ugeskr. Laeger. 2000, 162, 4553–4554. [Google Scholar]
- Miyasaka, Y.; Ono, K.; Nagayama, K.; Murakami, T.; Noguchi, O.; Uchihara, M.; Izumi, N.; Miyake, S.; Kubota, K.; Enomoto, N.; Tanaka, Y.; Marumo, F.; Sato, C. A case of pancreatic pleural effusion and ascites treated successfully with conservative measures including octreotide and nafamostat mesilate. Nippon Shokakibyo Gakkai Zasshi 1996, 93, 937–941. [Google Scholar]
- Skomarovskii, A.T.; Zemskov, V.S.; Skomarovskii, A.A. Use of dalargin in the treatment of acute cholecystopancreatitis complicated by obstructive jaundice. Klin. Khir. 1996, 8, 13–14. [Google Scholar]
- Zheng, M.H.; Xia, H.H.; Chen, Y.P. Rectal administration of NSAIDs in the prevention of post-ERCP pancreatitis: A complementary meta-analysis. Gut 2008, 57, 1632–1633. [Google Scholar]
- Lankisch, P.G. Indomethacin may reduce the incidence and severity of acute pancreatitis after ERCP. Am. J. Gastroenterol. 2008, 103, 244. [Google Scholar]
- Bai, Y.; Duowu, Z.; Zhaoshen, L. Is indomethacin a new hope for post-ERCP pancreatitis? Am. J. Gastroenterol. 2007, 102, 2103. [Google Scholar] [PubMed]
- Wagh, M.S.; Sherman, S. Indomethacin for post-ERCP pancreatitis prophylaxis: Another attempt at the Holy Grail. Am. J. Gastroenterol. 2007, 102, 984–986. [Google Scholar]
- Antonopoulos, S.; Mikros, S.; Kokkoris, S.; Protopsaltis, J.; Filioti, K.; Karamanolis, D.; Giannoulis, G. A case of acute pancreatitis possibly associated with combined salicylate and simvastatin treatment. JOP 2005, 6, 264–268. [Google Scholar]
- Boix, E.; Lopez, P.; Perez-Mateo, M.; Pico, A. Lanreotide autogel is a therapeutic option for patients who develop acute pancreatitis after somatostatin analog treatment. J. Endocrinol. Invest. 2004, 27, 613–614. [Google Scholar]
- Machala, W.; Wachowicz, N.; Komorowska, A.; Gaszynski, W. The use of drotrecogin alfa (activated) in severe sepsis during acute pancreatitis - two case studies. Med. Sci. Monit. 2004, 10, CS31–CS36. [Google Scholar]
- Oiofinlade, O. Diclofenac reduces the incidence of acute pancreatitis after endoscopic retrograde cholangiopancreatography. Gastroenterology 2004, 126, 632. [Google Scholar]
- O'Connor, A.S.; Navab, F.; Germain, M.J.; Freeman, J.K.; Mulhern, J.G.; O'Shea, M.H.; Lipkowitz, G.S.; Madden, R.L.; Braden, G.L. Pancreatitis and duodenitis from sarcoidosis, successful therapy with mycophenolate mofetil. Dig. Dis. Sci. 2003, 48, 2191–2194. [Google Scholar]
- Toubanakis, C.; Batziou, E.; Sipsas, N.; Galanopoulos, G.; Tzivras, M.; Archimandritis, A. Acute pancreatitis after long-term therapy with mesalazine, and hyperamylasaemia associated with azathioprine in a patient with ulcerative colitis. Eur. J. Gastroenterol. Hepatol. 2003, 15, 933–934. [Google Scholar]
- Freeman, M.L. Prevention of post-ERCP pancreatitis: Pharmacologic solution or patient selection and pancreatic stents? Gastroenterology 2003, 124, 1977–1980. [Google Scholar] [CrossRef] [PubMed]
- Famularo, G.; Bizzarri, C.; Nicotra, G.C. Acute pancreatitis caused by ketorolac tromethamine. J. Clin. Gastroenterol. 2002, 34, 283–284. [Google Scholar]
- Yang, C.C.; Deng, J.F.; Lin, T.J. Pancytopenia, hyperglycemia, shock, coma, rhabdomyolysis, and pancreatitis associated with acetaminophen poisoning. Vet. Hum. Toxicol. 2001, 43, 344–347. [Google Scholar] [PubMed]
- Adachi, E.; Okazaki, K.; Matsushima, Y.; Seno, H.; Uchida, K.; Nakase, H.; Kawanami, C.; Nakamura, T.; Chiba, T. Acute pancreatitis secondary to 5-aminosalicylic acid therapy in a patient with ulcerative colitis. Int. J. Pancreatol. 1999, 25, 217–221. [Google Scholar]
- Fernandez, J.; Sala, M.; Panes, J.; Feu, F.; Navarro, S.; Teres, J. Acute pancreatitis after long-term 5-aminosalicylic acid therapy. Am. J. Gastroenterol. 1997, 92, 2302–2303. [Google Scholar]
- Debongnie, J.C.; Dekoninck, X. Sulfasalazine, 5-ASA and acute pancreatitis in Crohn's disease. J. Clin. Gastroenterol. 1994, 19, 348–349. [Google Scholar]
- Choi, C.W.; Kang, D.H.; Kim, G.H.; Eum, J.S.; Lee, S.M.; Song, G.A.; Kim, D.U.; Kim, I.D.; Cho, M. Nafamostat mesylate in the prevention of post-ERCP pancreatitis and risk factors for post-ERCP pancreatitis. Gastrointest. Endosc. 2009, 69, e11–e18. [Google Scholar]
- Chen, C.; Xu, S.; Wang, W.X.; Ding, Y.M.; Yu, K.H.; Wang, B.; Chen, X.Y. Rosiglitazone attenuates the severity of sodium taurocholate-induced acute pancreatitis and pancreatitis-associated lung injury. Arch. Med. Res. 2009, 40, 79–88. [Google Scholar]
- Xiping, Z.; Jie, Z.; Qin, X.; Guanghua, F.; Yang, C.; Tongfa, J.; Qi, X. Influence of baicalin and octreotide on NF-kappaB and p-selectin expression in liver and kidney of rats with severe acute pancreatitis. Inflammation 2009, 32, 1–11. [Google Scholar]
- Sha, H.; Ma, Q.; Jha, R.K.; Xu, F.; Wang, L.; Wang, Z.; Zhao, Y.; Fan, F. Resveratrol ameliorates hepatic injury via the mitochondrial pathway in rats with severe acute pancreatitis. Eur. J. Pharmacol. 2008, 601, 136–142. [Google Scholar]
- Xiping, Z.; Hua, T.; Hanqing, C.; Li, C.; Zhiwei, W.; Keyi, W.; Wei, Y.; Yun, L.; Qingyu, L.; Qing, H.; Fei, W. The protecting effects and mechanisms of Baicalin and Octreotide on heart injury in rats with SAP. Mediators Inflamm. 2007, 2007, 19469. [Google Scholar] [PubMed]
- Barkay, O.; Niv, E.; Santo, E.; Bruck, R.; Hallak, A.; Konikoff, F.M. Low-dose heparin for the prevention of post-ERCP pancreatitis: A randomized placebo-controlled trial. Surg. Endosc. 2008, 22, 1971–1976. [Google Scholar]
- Wang, L.; Ma, Q.; Chen, X.; Sha, H.; Ma, Z. Effects of resveratrol on calcium regulation in rats with severe acute pancreatitis. Eur. J. Pharmacol. 2008, 580, 271–276. [Google Scholar]
- Cheng, B.Q.; Liu, C.T.; Li, W.J.; Fan, W.; Zhong, N.; Zhang, Y.; Jia, X.Q.; Zhang, S.Z. Ethyl pyruvate improves survival and ameliorates distant organ injury in rats with severe acute pancreatitis. Pancreas 2007, 35, 256–261. [Google Scholar]
- Szabolcs, A.; Tiszlavicz, L.; Kaszaki, J.; Posa, A.; Berko, A.; Varga, I.S.; Boros, I.; Szuts, V.; Lonovics, J.; Takacs, T. Zerumbone exerts a beneficial effect on inflammatory parameters of cholecystokinin octapeptide-induced experimental pancreatitis but fails to improve histology. Pancreas 2007, 35, 249–255. [Google Scholar]
- Zhang, X.P.; Zhang, L.; Yang, P.; Zhang, R.P.; Cheng, Q.H. Protective effects of baicalin and octreotide on multiple organ injury in severe acute pancreatitis. Dig. Dis. Sci. 2008, 53, 581–591. [Google Scholar]
- Seo, S.W.; Jung, W.S.; Piao, T.G.; Hong, S.H.; Yun, K.J.; Park, R.K.; Shin, M.K.; Song, H.J.; Park, S.J. Selective cyclooxygenase-2 inhibitor ameliorates cholecystokinin-octapeptide-induced acute pancreatitis in rats. World J. Gastroenterol. 2007, 13, 2298–2304. [Google Scholar]
- Xue, D.; Zhang, W.; Zhang, Y.; Wang, H.; Zheng, B.; Shi, X. Adjusting effects of baicalin for nuclear factor-kappaB and tumor necrosis factor-alpha on rats with caerulein-induced acute pancreatitis. Mediat. Inflamm. 2006, 5, 26295. [Google Scholar]
- Zhao, H.; Lu, H.G.; Shi, Y.B.; Zhao, L.M.; Bai, C.; Wang, X. Role of enteral nutrition supplemented with ebselen and EHEC in pancreatitis-associated multiple organ dysfunction in rats. Inflamm. Res. 2006, 55, 423–429. [Google Scholar]
- Kalyoncu, N.I.; Alhan, E.; Ercin, C.; Kural, B.V. Effects of dual inhibitor of cyclooxygenase and 5-lipoxygenase on acute necrotizing pancreatitis in rats. Hepatogastroenterology 2006, 53, 597–602. [Google Scholar]
- Shapiro, H.; Singer, P.; Halpern, Z.; Bruck, R. Polyphenols in the treatment of inflammatory bowel disease and acute pancreatitis. Gut 2007, 56, 426–435. [Google Scholar]
- de Almeida, J.L.; Jukemura, J.; Coelho, A.M.; Patzina, R.A.; Machado, M.C.; da Cunha, J.E. Inhibition of cyclooxygenase-2 in experimental severe acute pancreatitis. Clinics (Sao Paulo) 2006, 61, 301–306. [Google Scholar] [PubMed]
- Alsfasser, G.; Warshaw, A.L.; Thayer, S.P.; Antoniu, B.; Laposata, M.; Lewandrowski, K.B.; Fernandez-del Castillo, C. Decreased inflammation and improved survival with recombinant human activated protein C treatment in experimental acute pancreatitis. Arch. Surg. 2006, 141, 670–676. [Google Scholar]
- Lefter, L.P.; Dajbog, E.; Scripcariu, V.; Dragomir, C. Safety and efficacy of conservative management in acute severe pancreatitis. Chirurgia (Bucur.) 2006, 101, 135–139. [Google Scholar] [PubMed]
- Cosen-Binker, L.I.; Binker, M.G.; Cosen, R.; Negri, G.; Tiscornia, O. Influence of nitric oxide-donating nonsteroidal anti-inflammatory drugs on the evolution of acute pancreatitis. Shock 2006, 25, 190–203. [Google Scholar]
- Letoha, T.; Kusz, E.; Papai, G.; Szabolcs, A.; Kaszaki, J.; Varga, I.; Takacs, T.; Penke, B.; Duda, E. In vitro and in vivo nuclear factor-kappaB inhibitory effects of the cell-penetrating penetratin peptide. Mol. Pharmacol. 2006, 69, 2027–2036. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.H.; Ma, Q.Y.; Wang, L.C.; Sha, H.C.; Wu, S.L.; Zhang, M. Effect of resveratrol on peritoneal macrophages in rats with severe acute pancreatitis. Inflamm. Res. 2005, 54, 522–527. [Google Scholar]
- Lau, H.Y.; Bhatia, M. The effect of CP96, 345 on the expression of tachykinins and neurokinin receptors in acute pancreatitis. J. Pathol. 2006, 208, 364–371. [Google Scholar]
- Reding, T.; Bimmler, D.; Perren, A.; Sun, L.K.; Fortunato, F.; Storni, F.; Graf, R. A selective COX-2 inhibitor suppresses chronic pancreatitis in an animal model (WBN/Kob rats): Significant reduction of macrophage infiltration and fibrosis. Gut 2006, 55, 1165–1173. [Google Scholar]
- Zhao, Y.F.; Zhai, W.L.; Zhang, S.J.; Chen, X.P. Protection effect of triptolide to liver injury in rats with severe acute pancreatitis. Hepatobiliary Pancreat. Dis. Int. 2005, 4, 604–608. [Google Scholar]
- Alhan, E.; Kalyoncu, N.I.; Ercin, C.; Kural, B.V. Effects of the celecoxib on the acute necrotizing pancreatitis in rats. Inflammation 2004, 28, 303–309. [Google Scholar]
- Huang, J.; Moochhala, S.M.; Moore, P.K.; Bhatia, M. Flurbiprofen and HCT1026 protect mice against acute pancreatitis-associated lung injury. Shock 2005, 24, 182–187. [Google Scholar]
- Ma, Z.H.; Ma, Q.Y. Resveratrol: A medical drug for acute pancreatitis. World J. Gastroenterol. 2005, 11, 3171–3174. [Google Scholar]
- Madanick, R.D.; O'Loughlin, C.J.; Barkin, J.S. Diclofenac reduces the incidence of acute pancreatitis after endoscopic retrograde cholangiopancreatography. Dig. Dis. Sci. 2005, 50, 879–881. [Google Scholar]
- O'Brien, G.; Shields, C.J.; Winter, D.C.; Dillon, J.P.; Kirwan, W.O.; Redmond, H.P. Cyclooxygenase-2 plays a central role in the genesis of pancreatitis and associated lung injury. Hepatobiliary Pancreat. Dis. Int. 2005, 4, 126–128. [Google Scholar]
- Meng, Y.; Zhang, M.; Xu, J.; Liu, X.M.; Ma, Q.Y. Effect of resveratrol on microcirculation disorder and lung injury following severe acute pancreatitis in rats. World J. Gastroenterol. 2005, 11, 433–435. [Google Scholar]
- Yang, R.; Uchiyama, T.; Alber, S.M.; Han, X.; Watkins, S.K.; Delude, R.L.; Fink, M.P. Ethyl pyruvate ameliorates distant organ injury in a murine model of acute necrotizing pancreatitis. Crit. Care Med. 2004, 32, 1453–1459. [Google Scholar]
- Slogoff, M.I.; Ethridge, R.T.; Rajaraman, S.; Evers, B.M. COX-2 inhibition results in alterations in nuclear factor (NF)-kappaB activation but not cytokine production in acute pancreatitis. J. Gastrointest. Surg. 2004, 8, 511–519. [Google Scholar]
- Warzecha, Z.; Dembinski, A.; Ceranowicz, P.; Konturek, S.; Tomaszewska, R.; Stachura, J.; Nakamura, T.; Konturek, P.C. Inhibition of cyclooxygenase-2 reduces the protective effect of hepatocyte growth factor in experimental pancreatitis. Eur. J. Pharmacol. 2004, 486, 107–119. [Google Scholar]
- Foitzik, T.; Hotz, H.G.; Hotz, B.; Wittig, F.; Buhr, H.J. Selective inhibition of cyclooxygenase-2 (COX-2) reduces prostaglandin E2 production and attenuates systemic disease sequelae in experimental pancreatitis. Hepatogastroenterology 2003, 50, 1159–1162. [Google Scholar]
- Mentes, A.; Batur, Y.; Bayol, U. Salycylate--induced pancreatic injury in the cat: A preliminary study. Rom. J. Gastroenterol. 2002, 11, 309–312. [Google Scholar]
- Gukovsky, I.; Reyes, C.N.; Vaquero, E.C.; Gukovskaya, A.S.; Pandol, S.J. Curcumin ameliorates ethanol and nonethanol experimental pancreatitis. Am. J. Physiol. Gastrointest. Liver Physiol. 2003, 284, G85–G95. [Google Scholar]
- Hirata, M.; Hayashi, I.; Yoshimura, K.; Ishii, K.; Soma, K.; Ohwada, T.; Kakita, A.; Majima, M. Blockade of bradykinin B(2) receptor suppresses acute pancreatitis induced by obstruction of the pancreaticobiliary duct in rats. Br. J. Pharmacol. 2002, 135, 29–36. [Google Scholar]
- Su, S.B.; Motoo, Y.; Xie, M.J.; Taga, H.; Sawabu, N. Antifibrotic effect of the herbal medicine Saiko-keishi-to (TJ-10) on chronic pancreatitis in the WBN/Kob rat. Pancreas 2001, 22, 8–17. [Google Scholar]
- Su, S.B.; Motoo, Y.; Xie, M.J.; Sakai, J.; Taga, H.; Sawabu, N. Expression of pancreatitis-associated protein (PAP) in rat spontaneous chronic pancreatitis: Effect of herbal medicine Saiko-keishi-to (TJ-10). Pancreas 1999, 19, 239–247. [Google Scholar]
- Andersen, V.; Sonne, J.; Larsen, S. Antipyrine, oxazepam, and indocyanine green clearance in patients with chronic pancreatitis and healthy subjects. Scand. J. Gastroenterol. 1999, 34, 813–817. [Google Scholar] [CrossRef] [PubMed]
- Griesbacher, T.; Lembeck, F. Effects of the bradykinin antagonist, HOE 140, in experimental acute pancreatitis. Br. J. Pharmacol. 1992, 107, 356–360. [Google Scholar] [PubMed]
- Henry, D.; Lim, L.L.; Garcia Rodriguez, L.A.; Perez Gutthann, S.; Carson, J.L.; Griffin, M.; Savage, R.; Logan, R.; Moride, Y.; Hawkey, C.; Hill, S.; Fries, J.T. Variability in risk of gastrointestinal complications with individual non-steroidal anti-inflammatory drugs: Results of a collaborative meta-analysis. Br. Med. J. 1996, 312, 1563–1566. [Google Scholar]
- Dai, H.F.; Wang, X.W.; Zhao, K. Role of nonsteroidal anti-inflammatory drugs in the prevention of post-ERCP pancreatitis: A meta-analysis. Hepatobiliary Pancreat. Dis. Int. 2009, 8, 11–16. [Google Scholar]
- Elmunzer, B.J.; Waljee, A.K.; Elta, G.H.; Taylor, J.R.; Fehmi, S.M.; Higgins, P.D. A meta-analysis of rectal NSAIDs in the prevention of post-ERCP pancreatitis. Gut 2008, 57, 1262–1267. [Google Scholar]
- Cheon, Y.K.; Cho, K.B.; Watkins, J.L.; McHenry, L.; Fogel, E.L.; Sherman, S.; Schmidt, S.; Lazzell-Pannell, L.; Lehman, G.A. Efficacy of diclofenac in the prevention of post-ERCP pancreatitis in predominantly high-risk patients: A randomized double-blind prospective trial. Gastrointest. Endosc. 2007, 66, 1126–1132. [Google Scholar]
- Montano Loza, A.; Rodriguez Lomeli, X.; Garcia Correa, J.E.; Davalos Cobian, C.; Cervantes Guevara, G.; Medrano Munoz, F.; Fuentes Orozco, C.; Gonzalez Ojeda, A. Effect of the administration of rectal indomethacin on amylase serum levels after endoscopic retrograde cholangiopancreatography, and its impact on the development of secondary pancreatitis episodes. Rev. Esp. Enferm. Dig. 2007, 99, 330–335. [Google Scholar]
- Khoshbaten, M.; Khorram, H.; Madad, L.; Ehsani Ardakani, M.J.; Farzin, H.; Zali, M.R. Role of diclofenac in reducing post-endoscopic retrograde cholangiopancreatography pancreatitis. J. Gastroenterol. Hepatol. 2008, 23, e11–e16. [Google Scholar]
- Sotoudehmanesh, R.; Khatibian, M.; Kolahdoozan, S.; Ainechi, S.; Malboosbaf, R.; Nouraie, M. Indomethacin may reduce the incidence and severity of acute pancreatitis after ERCP. Am. J. Gastroenterol. 2007, 102, 978–983. [Google Scholar]
- Peiro, A.M.; Martinez, J.; Martinez, E.; de Madaria, E.; Llorens, P.; Horga, J.F.; Perez-Mateo, M. Efficacy and tolerance of metamizole versus morphine for acute pancreatitis pain. Pancreatology 2008, 8, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, H.T.; Jacobsen, J.; Norgaard, M.; Pedersen, L.; Johnsen, S.P.; Baron, J.A. Newer cyclo-oxygenase-2 selective inhibitors, other non-steroidal anti-inflammatory drugs and the risk of acute pancreatitis. Aliment. Pharmacol. Ther. 2006, 24, 111–116. [Google Scholar]
- Jick, H.; Derby, L.E.; Garcia Rodriguez, L.A.; Jick, S.S.; Dean, A.D. Nonsteroidal antiinflammatory drugs and certain rare, serious adverse events: A cohort study. Pharmacotherapy 1993, 13, 212–217. [Google Scholar]
- Blomgren, K.B.; Sundström, A.; Steineck, G.; Genell, S.; Sjöstedt, S.; Wiholm, B.E. A Swedish case-control network for studies of drug-induced morbidity: Acute pancreatitis. Eur. J. Clin. Pharmacol. 2002, 58, 275–283. [Google Scholar]
- Ibáñez, L.; Laporte, J.R.; Carné, X. Adverse drug reactions leading to hospital admission. Drug Saf. 1991, 6, 450–459. [Google Scholar]
- Motola, D.; Vaccheri, A.; Silvani, M.C.; Poluzzi, E.; Bottoni, A.; De Ponti, F.; Montanaro, N. Pattern of NSAID use in the Italian general population: A questionnaire-based survey. Eur. J. Clin. Pharmacol. 2004, 60, 731–738. [Google Scholar]
- Pezzilli, R.; Romboli, E.; Campana, D.; Corinaldesi, R. Mechanisms involved in the onset of post-ERCP pancreatitis. J.O.P. 2002, 3, 162–168. [Google Scholar]
- Kunz, D.; Bank, U.; Ittenson, A.; Schulz, H.U.; Sokolowski, A. Alteration of immunological functions in acute pancreatitis. Eur. J. Clin. Chem. Clin. Biochem. 1993, 31, A35–A36. [Google Scholar]
- Kiviniemi, H.; Juvonen, T.; Makela, J. Acute phase response in patients with uncomplicated endoscopic retrograde cholangiopancreatography. H.P.B. Surg. 1994, 8, 129–131. [Google Scholar]
- Oezcueruemez-Porsch, M.; Kunz, D.; Hardt, P.D.; Fadgyas, T.; Kress, O.; Schulz, H.U.; Schnell-Kretschmer, H.; Temme, H.; Westphal, S.; Luley, C.; Kloer, H.U. Diagnostic relevance of interleukin pattern, acute-phase proteins, and procalcitoninin early phase of post-ERCP pancreatitis. Dig. Dis. Sci. 1998, 43, 1763–1769. [Google Scholar] [PubMed]
- Kaw, M.; Singh, S. Serum lipase, C-reactive protein, and interleukin-6 levels in ERCP-induced pancreatitis. Gastrointest. Endosc. 2001, 54, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, J.A.; Barve, S.; Joshi-Barve, S.; Talwalker, R.; Gates, L.K. Cytokine production by CAPAN-1 and CAPAN-2 cell lines. Dig. Dis. Sci. 2000, 45, 927–932. [Google Scholar]
- Pezzilli, R.; Gabbrielli, A.; Morselli-Labate, A.M.; D'Alessio, P.; Barakat, B.; Costamagna, G.; Dibenedetti, F.; Massa, M.; Merlini, G.; Melzi d'Eril, G.M. Does gabexate mesilate affect serum concentrations of acute phase proteins after endoscopic retrograde cholangiopancreatography examination? Hepatogastroenterology 2003, 50, 851–855. [Google Scholar] [PubMed]
- Deviere, J.; Le Moine, O.; Van Laethem, J.L.; Eisendrath, P.; Ghilain, A.; Severs, N.; Cohard, M. Interleukin 10 reduces the incidence of pancreatitis after therapeutic endoscopic retrograde cholangiopancreatography. Gastroenterology 2001, 120, 498–505. [Google Scholar]
- Sherman, S.; Cheng, C.L.; Costamagna, G.; Binmoeller, K.F.; Puespoek, A.; Aithal, G.P.; Kozarek, R.A.; Chen, Y.K.; Van Steenbergen, W.; Tenner, S.; Freeman, M.; Monroe, P.; Geffner, M.; Deviere, J. Interleukin-10 ERCP Study Group. Efficacy of recombinant human interleukin-10 in prevention of post-endoscopic retrograde cholangiopancreatography pancreatitis in subjects with increased risk. Pancreas 2009, 38, 267–274. [Google Scholar] [PubMed]
- Gross, V.; Leser, H.G.; Heinisch, A.; Schölmerich, J. Inflammatory mediators and cytokines. New aspects of pathophysiology and assessment of severity of acute pancreatitis? Hepatogastroenterology 1993, 40, 522–530. [Google Scholar] [PubMed]
- Makela, A.; Kuusi, T.; Schroeder, T. Inhibition of serum phospholipase A2 in acute pancreatitis by pharamacologic agents in vitro. Scand. J. Clin. Lab. Invest. 1997, 57, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.M.; Anderson, K.E. Clinical phamacokinetics of diclofenac. Therapeutic insights and pitfalls. Clin. Pharamakokinet. 1997, 33, 184–213. [Google Scholar] [CrossRef]
- Pezzilli, R. Pharmacotherapy for acute pancreatitis. Expert Opin. Pharmacother. 2009, 10, 2999–3014. [Google Scholar]
- Liddle, R.A.; Nathan, J.D. Neurogenic inflammation and pancreatitis. Pancreatology 2004, 4, 551–559. [Google Scholar]
- Ferreira, S.H.; Vane, J.R. New aspects of the mode of action of nonsteroidal anti-inflammatory drugs. Annu. Rev. Pharmacol. 1974, 53, 57–73. [Google Scholar]
- Swift, J.Q.; Garry, M.G.; Roszkowski, M.T.; Hargreaves, K.M. Effect of flurbiprofen on tissue levels of immunoreactive bradykinin and acute post-operative pain. J. Oral. Maxillofac. Surg. 1993, 51, 112–116. [Google Scholar]
- Cashman, J.N. The mechanisms of action of NSAIDs in analgesia. Drugs 1996, 5, 13–23. [Google Scholar]
- Malmberg, A.B.; Yaksh, T.L. Hyperalgesia mediated by spinal glutamate or substance P receptor blocked by spinal cyclooxygenase inhibition. Science 1992, 257, 1276–1279. [Google Scholar]
- Pezzilli, R.; Uomo, G.; Gabbrielli, A.; Zerbi, A.; Frulloni, L.; De Rai, P.; Castoldi, L.; Cavallini, G.; Di Carlo, V. ProInf-AISP Study Group. A prospective multicentre survey on the treatment of acute pancreatitis in Italy. Dig. Liver Dis. 2007, 39, 838–846. [Google Scholar] [CrossRef] [PubMed]
© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Pezzilli, R.; Morselli-Labate, A.M.; Corinaldesi, R. NSAIDs and Acute Pancreatitis: A Systematic Review. Pharmaceuticals 2010, 3, 558-571. https://0-doi-org.brum.beds.ac.uk/10.3390/ph3030558
Pezzilli R, Morselli-Labate AM, Corinaldesi R. NSAIDs and Acute Pancreatitis: A Systematic Review. Pharmaceuticals. 2010; 3(3):558-571. https://0-doi-org.brum.beds.ac.uk/10.3390/ph3030558
Chicago/Turabian StylePezzilli, Raffaele, Antonio Maria Morselli-Labate, and Roberto Corinaldesi. 2010. "NSAIDs and Acute Pancreatitis: A Systematic Review" Pharmaceuticals 3, no. 3: 558-571. https://0-doi-org.brum.beds.ac.uk/10.3390/ph3030558