Adrenomedullin Is a Diagnostic and Prognostic Biomarker for Acute Intracerebral Hemorrhage

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Issues
2.2. Patients and Volunteers
2.3. Variables of the Study
2.4. Determination of AM Levels
2.5. Determination of NOx Levels
2.6. Statistical Analysis
3. Results
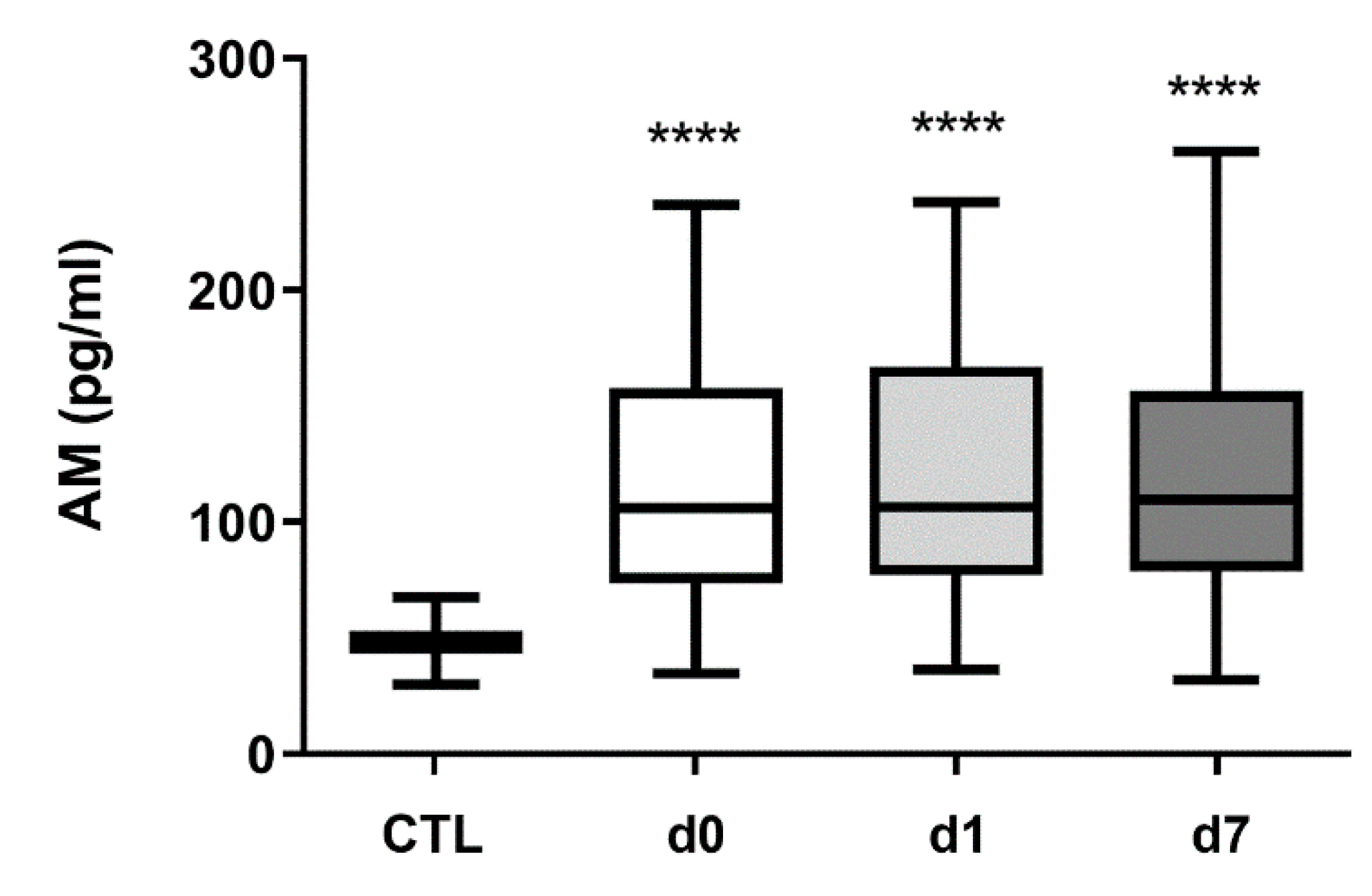
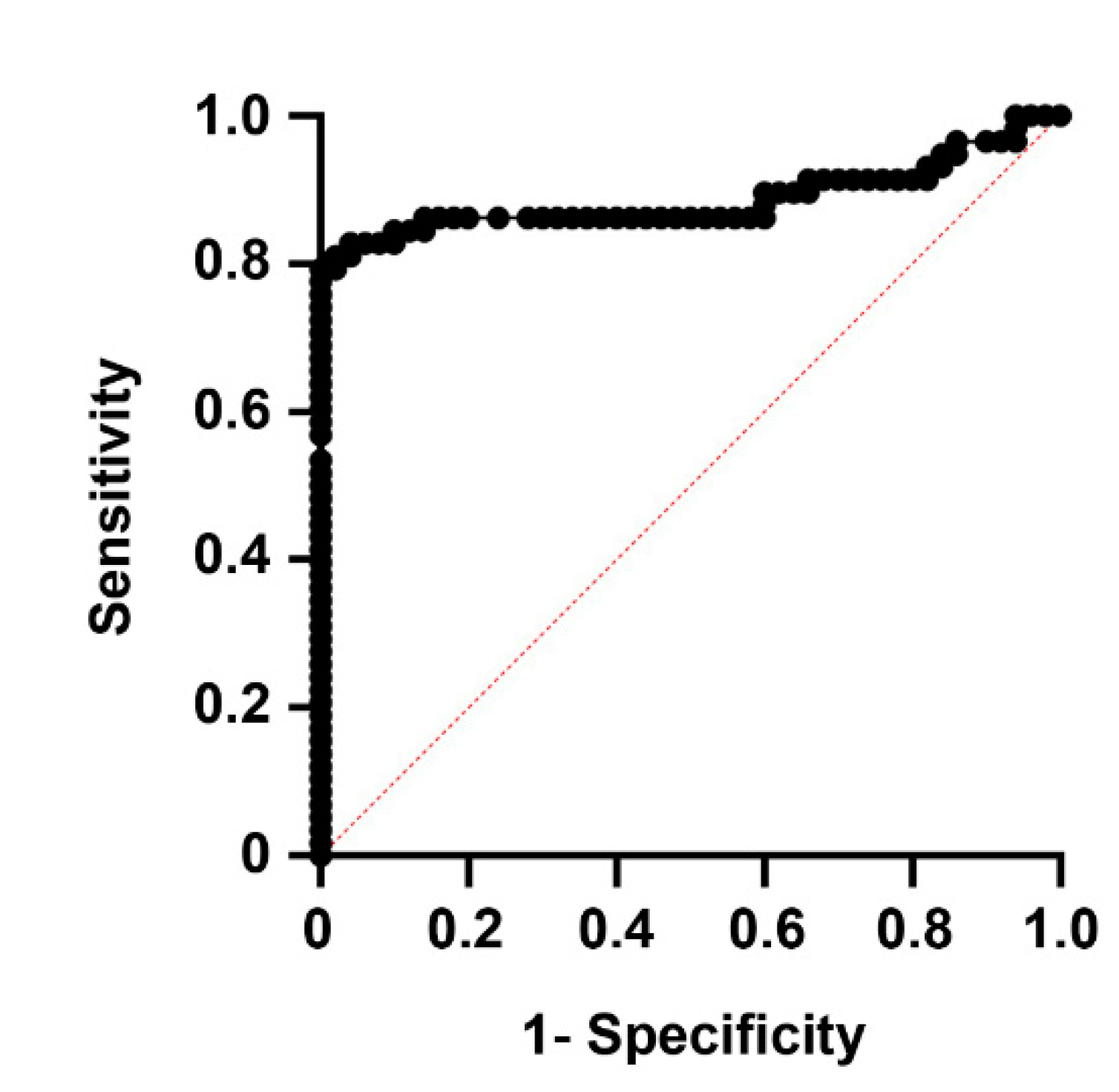
3.1. Serum AM Levels Are Higher in Intracerebral Hemorrhage Patients Than in Healthy Controls
3.2. The Temporal Pattern of AM Levels Predicts Prognosis and Patient Dependency
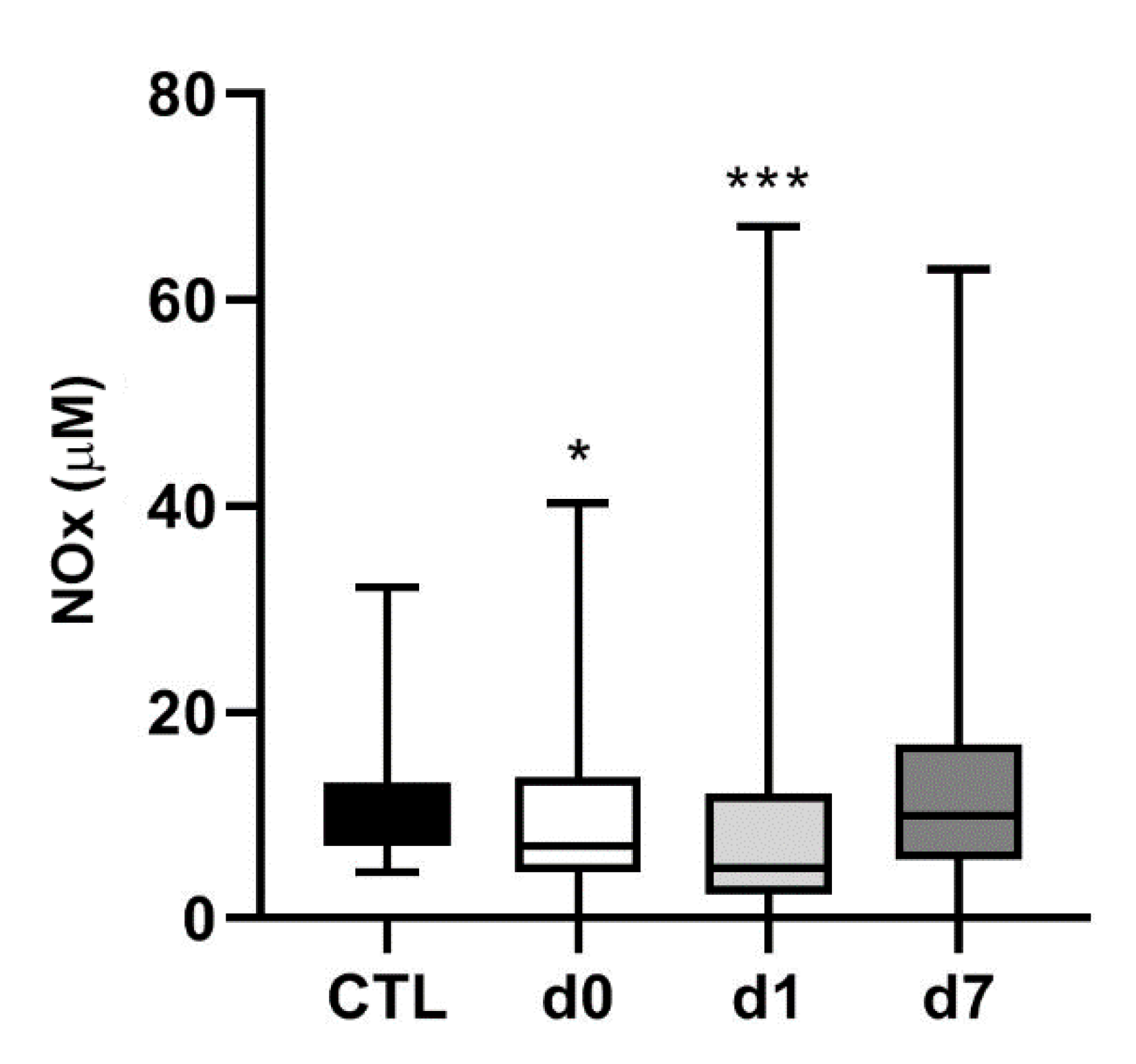
3.3. NOx Levels Are Lower in Hemorrhagic Stroke Patients Than in Healthy Controls
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. The Top 10 Causes of Death. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 10 June 2021).
- Feigin, V.L.; Nguyen, G.; Cercy, K.; Johnson, C.O.; Alam, T.; Parmar, P.G.; Abajobir, A.A.; Abate, K.H.; Abd-Allah, F.; Abejie, A.N.; et al. Global, Regional, and Country-Specific Lifetime Risks of Stroke, 1990 and 2016. N. Engl. J. Med. 2018, 379, 2429–2437. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef] [PubMed]
- Katan, M.; Luft, A. Global Burden of Stroke. Semin. Neurol. 2018, 38, 208–211. [Google Scholar] [CrossRef] [Green Version]
- Amarenco, P.; Bogousslavsky, J.; Caplan, L.R.; Donnan, G.A.; Hennerici, M.G. Classification of stroke subtypes. Cerebrovasc. Dis. 2009, 27, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Boehme, A.K.; Esenwa, C.; Elkind, M.S. Stroke Risk Factors, Genetics, and Prevention. Circ. Res. 2017, 120, 472–495. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, G.; Debette, S. Genetic Risk Factors for Ischemic and Hemorrhagic Stroke. Curr. Cardiol. Rep. 2016, 18, 124. [Google Scholar] [CrossRef] [Green Version]
- Poorthuis, M.H.; Algra, A.M.; Algra, A.; Kappelle, L.J.; Klijn, C.J. Female- and Male-Specific Risk Factors for Stroke: A Systematic Review and Meta-analysis. JAMA Neurol. 2017, 74, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Morotti, A.; Goldstein, J.N. Diagnosis and Management of Acute Intracerebral Hemorrhage. Emerg. Med. Clin. N. Am. 2016, 34, 883–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitago, T.; Ratan, R.R. Rehabilitation following hemorrhagic stroke: Building the case for stroke-subtype specific recovery therapies. F1000Research 2017, 6, 2044. [Google Scholar] [CrossRef] [Green Version]
- Turnbull, M.T.; Zubair, A.C.; Meschia, J.F.; Freeman, W.D. Mesenchymal stem cells for hemorrhagic stroke: Status of preclinical and clinical research. NPJ Regen. Med. 2019, 4, 10. [Google Scholar] [CrossRef]
- Bonnard, T.; Gauberti, M.; de Martinez, L.S.; Campos, F.; Vivien, D. Recent Advances in Nanomedicine for Ischemic and Hemorrhagic Stroke. Stroke 2019, 50, 1318–1324. [Google Scholar] [CrossRef]
- Simpkins, A.N.; Janowski, M.; Oz, H.S.; Roberts, J.; Bix, G.; Dore, S.; Stowe, A.M. Biomarker Application for Precision Medicine in Stroke. Transl. Stroke Res. 2020, 11, 615–627. [Google Scholar] [CrossRef] [Green Version]
- Makris, K.; Haliassos, A.; Chondrogianni, M.; Tsivgoulis, G. Blood biomarkers in ischemic stroke: Potential role and challenges in clinical practice and research. Crit. Rev. Clin. Lab. Sci. 2018, 55, 294–328. [Google Scholar] [CrossRef] [PubMed]
- Serrano, J.; Uttenthal, L.O.; Martinez, A.; Fernandez, A.P.; Martinez de Velasco, J.; Alonso, D.; Bentura, M.L.; Santacana, M.; Gallardo, J.R.; Martínez-Murillo, R.; et al. Distribution of adrenomedullin-like immunoreactivity in the rat central nervous system by light and electron microscopy. Brain Res. 2000, 853, 245–268. [Google Scholar] [CrossRef] [Green Version]
- Lopez, J.; Martinez, A. Cell and molecular biology of the multifunctional peptide, adrenomedullin. Int. Rev. Cytol. 2002, 221, 1–92. [Google Scholar] [CrossRef] [PubMed]
- Garayoa, M.; Martinez, A.; Lee, S.; Pio, R.; An, W.G.; Neckers, L.; Trepel, J.; Montuenga, L.M.; Ryan, H.; Johnson, R.; et al. Hypoxia-inducible factor-1 (HIF-1) up-regulates adrenomedullin expression in human tumor cell lines during oxygen deprivation: A possible promotion mechanism of carcinogenesis. Mol. Endocrinol. 2000, 14, 848–862. [Google Scholar] [CrossRef]
- Nishida, H.; Horio, T.; Suzuki, Y.; Iwashima, Y.; Kamide, K.; Kangawa, K.; Kawano, Y. Plasma adrenomedullin as an independent predictor of future cardiovascular events in high-risk patients: Comparison with C-reactive protein and adiponectin. Peptides 2008, 29, 599–605. [Google Scholar] [CrossRef]
- Serrano, J.; Alonso, D.; Encinas, J.M.; Lopez, J.C.; Fernandez, A.P.; Castro-Blanco, S.; Fernández-Vizarra, P.; Richart, A.; Bentura, M.L.; Santacana, M.; et al. Adrenomedullin expression is up-regulated by ischemia-reperfusion in the cerebral cortex of the adult rat. Neuroscience 2002, 109, 717–731. [Google Scholar] [CrossRef]
- Serrano, J.; Fernandez, A.P.; Sanchez, J.; Rodrigo, J.; Martinez, A. Adrenomedullin expression is up-regulated by acute hypobaric hypoxia in the cerebral cortex of the adult rat. Brain Pathol. 2008, 18, 434–442. [Google Scholar] [CrossRef] [Green Version]
- Robertson, C.L.; Minamino, N.; Ruppel, R.A.; Kangawa, K.; Wisniewski, S.R.; Tsuji, T.; Janesko, K.L.; Ohta, H.; Adelson, P.D.; Marion, D.W.; et al. Increased adrenomedullin in cerebrospinal fluid after traumatic brain injury in infants and children. J. Neurotrauma 2001, 18, 861–868. [Google Scholar] [CrossRef]
- Chen, T.J.; Fu, Q.Y.; Wu, W.Q. Plasma levels of adrenomedullin in patients with traumatic brain injury: Potential contribution to prognosis. Peptides 2014, 56, 146–150. [Google Scholar] [CrossRef]
- Hurtado, O.; Serrano, J.; Sobrado, M.; Fernandez, A.P.; Lizasoain, I.; Martinez-Murillo, R.; Moro, M.A.; Martinez, A. Lack of adrenomedullin, but not complement factor H, results in larger infarct size and more extensive brain damage in a focal ischemia model. Neuroscience 2010, 171, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Somay, G.; Halac, G.U.; Uslu, E.; Aydin, S. Plasma adrenomedullin in acute ischemic stroke. Neurosciences 2007, 12, 351–353. [Google Scholar] [PubMed]
- Serrano-Ponz, M.; Rodrigo-Gasque, C.; Siles, E.; Martinez-Lara, E.; Ochoa-Callejero, L.; Martinez, A. Temporal profiles of blood pressure, circulating nitric oxide, and adrenomedullin as predictors of clinical outcome in acute ischemic stroke patients. Mol. Med. Rep. 2016, 13, 3724–3734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.L.; Lin, H.Y.; Xu, J.W.; Jiang, F.F.; Yang, M.; Wang, J.H.; Huang, X.-Q. Blood levels of adrenomedullin on admission predict outcomes after acute intracerebral hemorrhage. Peptides 2014, 54, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Kikumoto, K.; Kubo, A.; Hayashi, Y.; Minamino, N.; Inoue, S.; Dohi, K.; Kitamura, K.; Kangawa, K.; Matsuo, H.; Furuya, H. Increased plasma concentration of adrenomedullin in patients with subarachnoid hemorrhage. Anesth. Analg. 1998, 87, 859–863. [Google Scholar] [CrossRef] [PubMed]
- Kubo, Y.; Ogasawara, K.; Kakino, S.; Kashimura, H.; Yoshida, K.; Ogawa, A. Cerebrospinal fluid adrenomedullin concentration correlates with hyponatremia and delayed ischemic neurological deficits after subarachnoid hemorrhage. Cerebrovasc. Dis. 2008, 25, 164–169. [Google Scholar] [CrossRef]
- Kubo, Y.; Koji, T.; Kashimura, H.; Otawara, Y.; Ogawa, A.; Ogasawara, K. Adrenomedullin concentration in the cerebrospinal fluid is related to appetite loss and delayed ischemic neurological deficits after subarachnoid hemorrhage. Neurol. Res. 2013, 35, 713–718. [Google Scholar] [CrossRef]
- Weimar, C.; Konig, I.R.; Kraywinkel, K.; Ziegler, A.; Diener, H.C. Age and National Institutes of Health Stroke Scale Score within 6 hours after onset are accurate predictors of outcome after cerebral ischemia: Development and external validation of prognostic models. Stroke 2004, 35, 158–162. [Google Scholar] [CrossRef]
- Koennecke, H.C.; Belz, W.; Berfelde, D.; Endres, M.; Fitzek, S.; Hamilton, F.; Kreitsch, P.; Mackert, B.-M.; Nabavi, D.G.; Nolte, C.H.; et al. Factors influencing in-hospital mortality and morbidity in patients treated on a stroke unit. Neurology 2011, 77, 965–972. [Google Scholar] [CrossRef]
- Kothari, R.U.; Brott, T.; Broderick, J.P.; Barsan, W.G.; Sauerbeck, L.R.; Zuccarello, M.; Khoury, J. The ABCs of measuring intracerebral hemorrhage volumes. Stroke 1996, 27, 1304–1305. [Google Scholar] [CrossRef] [PubMed]
- Dowlatshahi, D.; Demchuk, A.M.; Flaherty, M.L.; Ali, M.; Lyden, P.L.; Smith, E.E. Defining hematoma expansion in intracerebral hemorrhage: Relationship with patient outcomes. Neurology 2011, 76, 1238–1244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pio, R.; Martinez, A.; Unsworth, E.J.; Kowalak, J.A.; Bengoechea, J.A.; Zipfel, P.F.; Elsasser, T.H.; Cuttitta, F. Complement factor H is a serum-binding protein for adrenomedullin, and the resulting complex modulates the bioactivities of both partners. J. Biol. Chem. 2001, 276, 12292–12300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez, A.; Elsasser, T.H.; Bhathena, S.J.; Pio, R.; Buchanan, T.A.; Macri, C.J.; Cuttitta, F. Is adrenomedullin a causal agent in some cases of type 2 diabetes? Peptides 1999, 20, 1471–1478. [Google Scholar] [CrossRef]
- Yin, J.; Mutiso, F.; Tian, L. Joint hypothesis testing of the area under the receiver operating characteristic curve and the Youden index. Pharm. Stat. 2021. [Google Scholar] [CrossRef] [PubMed]
- Iring, A.; Jin, Y.J.; Albarran-Juarez, J.; Siragusa, M.; Wang, S.; Dancs, P.T.; Nakayama, A.; Tonack, S.; Chen, M.; Künne, C.; et al. Shear stress-induced endothelial adrenomedullin signaling regulates vascular tone and blood pressure. J. Clin. Investig. 2019, 129, 2775–2791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larrayoz, I.M.; Ferrero, H.; Martisova, E.; Gil-Bea, F.J.; Ramirez, M.J.; Martinez, A. Adrenomedullin Contributes to Age-Related Memory Loss in Mice and Is Elevated in Aging Human Brains. Front. Mol. Neurosci. 2017, 10, 384. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Yan, J.; Greer, J.M.; Read, S.J.; Henderson, R.D.; Rose, S.E.; Coulthard, A.; A McCombe, P. Correlation of adrenomedullin gene expression in peripheral blood leukocytes with severity of ischemic stroke. Int. J. Neurosci. 2014, 124, 271–280. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Tang, B.; Yin, C.G.; Chen, Y.; Meng, Q.L.; Jiang, L.; Wang, W.-P.; Niu, G.-Z. Plasma adrenomedullin levels are associated with long-term outcomes of acute ischemic stroke. Peptides 2014, 52, 44–48. [Google Scholar] [CrossRef]
- Chiu, D.; Peterson, L.; Elkind, M.S.V.; Rosand, J.; Gerber, L.M.; Silverstein, M.D. Comparison of outcomes after intracerebral hemorrhage and ischemic stroke. J. Stroke Cerebrovasc. Dis. 2010, 19, 225–229. [Google Scholar] [CrossRef]
- Li, F.J.; Zheng, S.R.; Wang, D.M. Adrenomedullin: An important participant in neurological diseases. Neural Regen. Res. 2020, 15, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Yue, T.L.; Barone, F.C.; White, R.F.; Clark, R.K.; Willette, R.N.; Sulpizio, A.C.; Aiyar, N.V.; Ruffolo, R.R.; Feuerstein, G.Z. Discovery of adrenomedullin in rat ischemic cortex and evidence for its role in exacerbating focal brain ischemic damage. Proc. Natl. Acad. Sci. USA 1995, 92, 11480–11484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dogan, A.; Suzuki, Y.; Koketsu, N.; Osuka, K.; Saito, K.; Takayasu, M.; Shibuya, M.; Yoshida, J. Intravenous infusion of adrenomedullin and increase in regional cerebral blood flow and prevention of ischemic brain injury after middle cerebral artery occlusion in rats. J. Cereb. Blood Flow Metab. 1997, 17, 19–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, K.; Takayasu, M.; Noda, A.; Hara, M.; Takagi, T.; Suzuki, Y.; Noda, A.; Hara, M.; Yoshia, J. Adrenomedullin reduces ischemic brain injury after transient middle cerebral artery occlusion in rats. Acta Neurochir. 2001, 143, 1157–1161. [Google Scholar] [CrossRef] [PubMed]
- Xia, C.F.; Yin, H.; Borlongan, C.V.; Chao, J.; Chao, L. Postischemic infusion of adrenomedullin protects against ischemic stroke by inhibiting apoptosis and promoting angiogenesis. Exp. Neurol. 2006, 197, 521–530. [Google Scholar] [CrossRef]
- Ochoa-Callejero, L.; Pozo-Rodrigalvarez, A.; Martinez-Murillo, R.; Martinez, A. Lack of adrenomedullin in mouse endothelial cells results in defective angiogenesis, enhanced vascular permeability, less metastasis, and less brain damage. Sci. Rep. 2016, 6, 33495. [Google Scholar] [CrossRef]
- Martinez, A.; Weaver, C.; Lopez, J.; Bhathena, S.J.; Elsasser, T.H.; Miller, M.J.; Moody, T.W.; Unsworth, E.J.; Cuttitta, F. Regulation of insulin secretion and blood glucose metabolism by adrenomedullin. Endocrinology 1996, 137, 2626–2632. [Google Scholar] [CrossRef] [Green Version]
- Martinez, A.; Miller, M.J.; Unsworth, E.J.; Siegfried, J.M.; Cuttitta, F. Expression of adrenomedullin in normal human lung and in pulmonary tumors. Endocrinology 1995, 136, 4099–4105. [Google Scholar] [CrossRef]
- Ouafik, L.; Sauze, S.; Boudouresque, F.; Chinot, O.; Delfino, C.; Fina, F.; Vuaroqueaux, V.; Dussert, C.; Palmari, J.; Dufour, H.; et al. Neutralization of adrenomedullin inhibits the growth of human glioblastoma cell lines in vitro and suppresses tumor xenograft growth in vivo. Am. J. Pathol. 2002, 160, 1279–1292. [Google Scholar] [CrossRef] [Green Version]
- Kaafarani, I.; Fernandez-Sauze, S.; Berenguer, C.; Chinot, O.; Delfino, C.; Dussert, C.; Metellus, P.; Boudouresque, F.; Mabrouk, K.; Grisoli, F.; et al. Targeting adrenomedullin receptors with systemic delivery of neutralizing antibodies inhibits tumor angiogenesis and suppresses growth of human tumor xenografts in mice. FASEB J. 2009, 23, 3424–3435. [Google Scholar] [CrossRef]
- Ishikawa, T.; Chen, J.; Wang, J.; Okada, F.; Sugiyama, T.; Kobayashi, T.; Shindo, M.; Higashino, F.; Katoh, H.; Asaka, M.; et al. Adrenomedullin antagonist suppresses in vivo growth of human pancreatic cancer cells in SCID mice by suppressing angiogenesis. Oncogene 2003, 22, 1238–1242. [Google Scholar] [CrossRef] [Green Version]
- Ramachandran, V.; Arumugam, T.; Hwang, R.F.; Greenson, J.K.; Simeone, D.M.; Logsdon, C.D. Adrenomedullin is expressed in pancreatic cancer and stimulates cell proliferation and invasion in an autocrine manner via the adrenomedullin receptor, ADMR. Cancer Res. 2007, 67, 2666–2675. [Google Scholar] [CrossRef] [Green Version]
- Martinez, A.; Julian, M.; Bregonzio, C.; Notari, L.; Moody, T.W.; Cuttitta, F. Identification of vasoactive nonpeptidic positive and negative modulators of adrenomedullin using a neutralizing antibody-based screening strategy. Endocrinology 2004, 145, 3858–3865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paspalj, D.; Nikic, P.; Savic, M.; Djuric, D.; Simanic, I.; Zivkovic, V.; Jeremic, N.; Srejovic, I.; Jakovljevic, V. Redox status in acute ischemic stroke: Correlation with clinical outcome. Mol. Cell. Biochem. 2015, 406, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Waheed, S.; Kalsekar, A.G.; Kamal, A.K.; Bryan, N.S.; Mian, A.I. Association of Plasma Levels of Nitric Oxide Oxidative Metabolites with Acute Stroke in Patients Presenting to the Emergency Department of a Low-Middle Income Country. Emerg. Med. Int. 2019, 9206948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terpolilli, N.A.; Feiler, S.; Dienel, A.; Muller, F.; Heumos, N.; Friedrich, B.; Stover, J.; Thal, S.; Schöller, K.; Plesnila, N. Nitric oxide inhalation reduces brain damage, prevents mortality, and improves neurological outcome after subarachnoid hemorrhage by resolving early pial microvasospasms. J. Cereb. Blood Flow Metab. 2016, 36, 2096–2107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenz, I.J.; Plesnila, N.; Terpolilli, N.A. Role of endothelial nitric oxide synthase for early brain injury after subarachnoid hemorrhage in mice. J. Cereb. Blood Flow Metab. 2020. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hemorrhagic Patients | Healthy Volunteers | p Value | ||
|---|---|---|---|---|
| Age [years], median (Q1–Q3) | 81 (72.2–87) | 46.5 (40–54) | <0.001 | |
| Sex [males], (%) | 38 (59.4%) | 31 (62.0%) | 0.91 | |
| Risk factors | ||||
| Arterial hypertension | 49 (76.6%) | |||
| Diabetes mellitus | 15 (23.4%) | |||
| Dyslipidemia | 20 (21.9%) | |||
| Atrial fibrillation | 18 (28.1%) | |||
| Stroke | 16 (25.0%) | |||
| Ischemic heart disease | 8 (12.5%) | |||
| Cognitive impairment | 8 (31.2%) | |||
| Smoking | 17 (26. 6%) | |||
| Previous treatment | ||||
| Antihypertensives | 45 (70.3%) | |||
| Anti-aggregants | 19 (29.7%) | |||
| Anticoagulants | 20 (31.8%) | |||
| Statins | 21 (32.8%) | |||
| Hematoma localization | ||||
| Supratentorial | 41 (64.1%) | |||
| Infratentorial | 6 (9.4%) | |||
| Lobar | 14 (21.8%) | |||
| Mixed | 3 (4.7%) | |||
| Rankin scale | ||||
| Basal | 0–1–2 | 54 (84.4%) | ||
| 3–4 | 10 (15.6%) | |||
| 5–6 | 0 (0.0%) | |||
| 3 months | 0–1–2 | 28 (43.7%) | ||
| 3–4 | 12 (18.7%) | |||
| 5–6 | 24 (37.5%) | |||
| NIHSS, median (Q1–Q3) | ||||
| Basal | 7.5 (2–16) | |||
| Hospital discharge | 5 (2–6.7) | |||
| Hematoma at d0 (cm3) | 4.5 (1–13.9) | |||
| Hematoma at d1 (cm3) | 4.6 (1–15.0) | |||
| AM at d0 (pg/mL), median (Q1–Q3) | 105.8 (74.6–157.8) | 47.7 (43.3–52.8) | <0.0001 | |
| AM at d1 (pg/mL), median (Q1–Q3) | 106.4 (79.3–166.4) | |||
| AM at d7 (pg/mL), median (Q1–Q3) | 109.7 (79.2–154.4) | |||
| NOx at d0 (µM), median (Q1–Q3) | 7.0 (4.6–12.9) | 9.1 (7.1–12.1) | 0.04 | |
| NOx at d1 (µM), median (Q1–Q3) | 4.8 (2.4–11.5) | |||
| NOx at d7 (µM), median (Q1–Q3) | 9.9 (5.9–16.3) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Julián-Villaverde, F.J.; Ochoa-Callejero, L.; Siles, E.; Martínez-Lara, E.; Martínez, A. Adrenomedullin Is a Diagnostic and Prognostic Biomarker for Acute Intracerebral Hemorrhage. Curr. Issues Mol. Biol. 2021, 43, 324-334. https://0-doi-org.brum.beds.ac.uk/10.3390/cimb43010027
Julián-Villaverde FJ, Ochoa-Callejero L, Siles E, Martínez-Lara E, Martínez A. Adrenomedullin Is a Diagnostic and Prognostic Biomarker for Acute Intracerebral Hemorrhage. Current Issues in Molecular Biology. 2021; 43(1):324-334. https://0-doi-org.brum.beds.ac.uk/10.3390/cimb43010027
Chicago/Turabian StyleJulián-Villaverde, Francisco J., Laura Ochoa-Callejero, Eva Siles, Esther Martínez-Lara, and Alfredo Martínez. 2021. "Adrenomedullin Is a Diagnostic and Prognostic Biomarker for Acute Intracerebral Hemorrhage" Current Issues in Molecular Biology 43, no. 1: 324-334. https://0-doi-org.brum.beds.ac.uk/10.3390/cimb43010027