Participation of Children with Spina Bifida: A Scoping Review Using the International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY) as a Reference Framework


Abstract
:1. Introduction
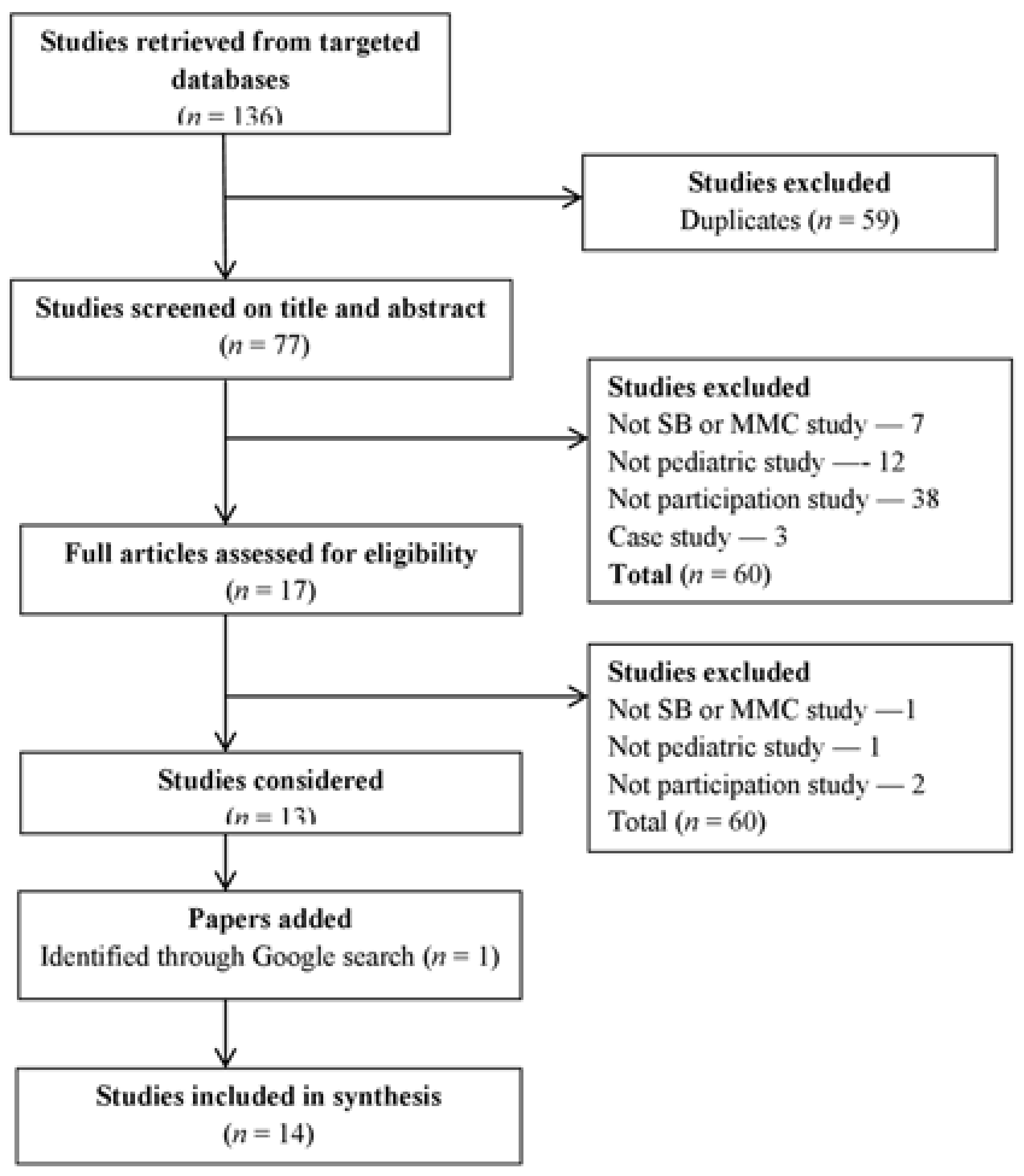
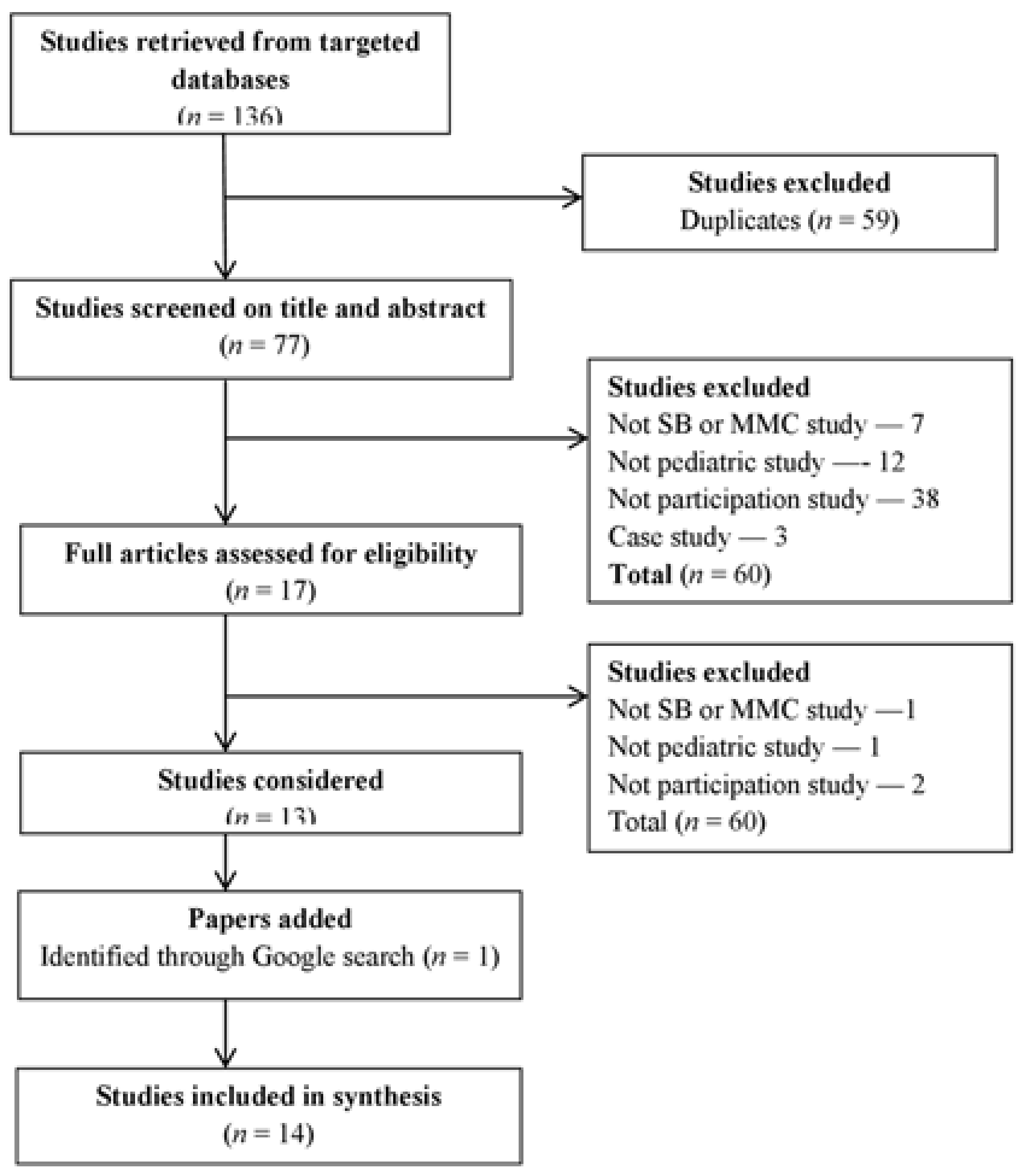
2. Materials and Methods
3. Results
3.1. Social Participation
3.2. Participating in Sports and Recreational Activities
3.3. Participating in School
3.4. Factors Influencing Participation
3.4.1. Body Function and Structures
3.4.2. Activity Limitations
3.4.3. Personal Factors
3.4.4. Environment
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001; 299p. [Google Scholar]
- Imms, C. Review of the Children’s Assessment of Participation and Enjoyment and the Preferences for Activity of Children. Phys. Occup. Ther. Pediatr. 2008, 28, 389–404. [Google Scholar] [CrossRef] [PubMed]
- Imms, C.; Adair, B.; Keen, D.; Ullenhag, A.; Rosenbaum, P.; Granlund, M. ‘Participation’: A systematic review of language, definitions, and constructs used in intervention research with children with disabilities. Dev. Med. Child Neurol. 2016, 58, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Powrie, B.; Kolehmainen, N.; Turpin, M.; Ziviani, J.; Copley, J. The meaning of leisure for children and young people with physical disabilities: A systematic evidence synthesis. Dev. Med. Child Neurol. 2015, 57, 993–1010. [Google Scholar] [CrossRef] [PubMed]
- King, G.; Willoughby, C.; Specht, J.A.; Brown, E. Social Support Processes and the Adaptation of Individuals with Chronic Disabilities. Qual. Health Res. 2006, 16, 902–925. [Google Scholar] [CrossRef] [PubMed]
- Liptak, G.S.; El Samra, A. Optimizing health care for children with spina bifida. Dev. Disabil. Res. Rev. 2010, 16, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Bowman, R.M.; Boshnjaku, V.; McLone, D.G. The changing incidence of myelomeningocele and its impact on pediatric neurosurgery: A review from the Children’s Memorial Hospital. Childs Nerv. Syst. 2009, 25, 801–806. [Google Scholar] [CrossRef] [PubMed]
- Oakeshott, P.; Hunt, G.M.; Kerry, S.; Strauss, D.J.; Shavelle, R.M.; Reynolds, R.J. Survival and mobility in open spina bifida: Comparison of results from the United States and the United Kingdom. Int. J. Disabil. Hum. Dev. 2008, 7, 101–106. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Pham, M.T.; Rajić, A.; Greig, J.D.; Sargeant, J.M.; Papadopoulos, A.; McEwen, S.A. A scoping review of scoping reviews: Advancing the approach and enhancing the consistency. Res. Synth. Methods 2014, 5, 371–385. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, L. The relationship between school environment and participation for students with disabilities. Pediatr. Rehabil. 2005, 8, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Coster, W. School Function Assessment: SFA: User’s Manual; Psychological Corp.: San Antonio, TX, USA, 1998. [Google Scholar]
- Law, M.; King, G.; Petrenchik, T.; Kertoy, M.; Anaby, D. The assessment of preschool children’s participation: Internal consistency and construct validity. Phys. Occup. Ther. Pediatr. 2012, 32, 272–287. [Google Scholar] [CrossRef] [PubMed]
- Fischer, N.; Church, P.; Lyons, J.; McPherson, A.C. A qualitative exploration of the experiences of children with spina bifida and their parents around incontinence and social participation: Incontinence in children with spina bifida. Child Care Health Dev. 2015, 41, 954–962. [Google Scholar] [CrossRef] [PubMed]
- Boudos, R.M.; Mukherjee, S. Barriers to community participation: Teens and young adults with spina bifida. J. Pediatr. Rehabil. Med. 2008, 1, 303–310. [Google Scholar] [PubMed]
- Flanagan, A.; Gorzkowski, M.; Altiok, H.; Hassani, S.; Ahn, K.W. Activity Level, Functional Health, and Quality of Life of Children with Myelomeningocele as Perceived by Parents. Clin. Orthop. Relat. Res. 2011, 469, 1230–1235. [Google Scholar] [CrossRef] [PubMed]
- Kelly, E.H.; Altiok, H.; Gorzkowski, J.A.; Abrams, J.R.; Vogel, L.C. How Does Participation of Youth With Spina Bifida Vary by Age? Clin. Orthop. Relat. Res. 2011, 469, 1236–1245. [Google Scholar] [CrossRef] [PubMed]
- Liptak, G.S.; Kennedy, J.A.; Dosa, N.P. Youth with Spina Bifida and Transitions: Health and Social Participation in a Nationally Represented Sample. J. Pediatr. 2010, 157, 584–588. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, A.; Kelly, E.H.; Vogel, L.C. Psychosocial outcomes of children and adolescents with early-onset spinal cord injury and those with spina bifida. Pediatr. Phys. Ther. 2013, 25, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Connor-Kuntz, F.J.; Dummer, G.M.; Paciorek, M.J. Physical education and sport participation of children and youth with spina bifida myelomeningocele. Adapt. Phys. Act. Q. 1995, 12, 228–238. [Google Scholar] [CrossRef]
- Marques, A.; Maldonado, I.; Peralta, M.; Santos, S. Exploring psychosocial correlates of physical activity among children and adolescents with spina bifida. Disabil. Health J. 2015, 8, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Peny-Dahlstrand, M.; Krumlinde-Sundholm, L.; Gosman-Hedstrom, G. Patterns of participation in school-related activities and settings in children with spina bifida. Disabil. Rehabil. 2013, 35, 1821–1827. [Google Scholar] [CrossRef] [PubMed]
- Bloemen, M.; Verschuren, O.; van Mechelen, C.; Borst, H.E.; de Leeuw, A.J.; van der Hoef, M.; de Groot, J.F. Personal and environmental factors to consider when aiming to improve participation in physical activity in children with Spina Bifida: A qualitative study. BMC Neurol. 2015, 15, 11. [Google Scholar] [CrossRef] [PubMed]
- Field, S.J.; Oates, R.K. Sport and recreation activities and opportunities for children with spina bifida and cystic fibrosis. J. Sci. Med. Sport 2001, 4, 71–76. [Google Scholar] [CrossRef]
- Anaby, D.; Hand, C.; Bradley, L.; DiRezze, B.; Forhan, M.; DiGiacomo, A.; Law, M. The effect of the environment on participation of children and youth with disabilities: A scoping review. Disabil. Rehabil. 2013, 35, 1589–1598. [Google Scholar] [CrossRef] [PubMed]
- WHO. United Nations Standard Rules on the Equalization of Opportunities for Persons with Disabilities. Available online: http://www.who.int/disabilities/policies/standard_rules/en/ (accessed on 13 September 2016).
- Imms, C. Children with cerebral palsy participate: A review of the literature. Disabil. Rehabil. 2008, 30, 1867–1884. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; King, G.; King, S.; Kertoy, M.; Hurley, P.; Rosenbaum, P.; Young, N.; Hanna, S. Patterns of participation in recreational and leisure activities among children with complex physical disabilities. Dev. Med. Child Neurol. 2006, 48, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Holmbeck, G.N.; Westhoven, V.C.; Phillips, W.S.; Bowers, R.; Gruse, C.; Nikolopoulos, T.; Totura, C.M.W.; Davison, K. A multimethod, multi-informant, and multidimensional perspective on psychosocial adjustment in preadolescents with spina bifida. J. Consult. Clin. Psychol. 2003, 71, 782–796. [Google Scholar] [CrossRef] [PubMed]
- Holmbeck, G.N.; Coakley, R.M.; Hommeyer, J.S.; Shapera, W.E.; Westhoven, V.C. Observed and perceived dyadic and systemic functioning in families of preadolescents with spina bifida. J. Pediatr. Psychol. 2002, 27, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Dennis, M.; Barnes, M.A. The cognitive phenotype of spina bifida meningomyelocele. Dev. Disabil. Res. Rev. 2010, 16, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Landry, S.H.; Taylor, H.B.; Swank, P.R.; Barnes, M.; Juranek, J. Longitudinal Mediators of Social Problem Solving in Spina Bifida and Typical Development. Rehabil. Psychol. 2013, 58, 196–205. [Google Scholar] [CrossRef] [PubMed]
- King, G.; Law, M.; King, S.; Rosenbaum, P.; Kertoy, M.K.; Young, N.L. A conceptual model of the factors affecting the recreation and leisure participation of children with disabilities. Phys. Occup. Ther. Pediatr. 2003, 23, 63–90. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| First Author (Year), Country | Sample N (N By Groups), Age | Design: Focus | Participation/Main Outcome Measure | Main Findings Related to Participation |
|---|---|---|---|---|
| Bloemen et al. (2015) [15], The Netherlands | Spina bifida (SB) N = 33 (8–18) (children); N = 42 (parent) | Qualitative, grounded theory: factors affecting physical activity | Physical activity for persons with disability (PAD) model: intention, attitude, self-efficacy, health condition, facilitators and barriers, intention, social influence. | Personal factors related to participation were: bowel and bladder care, competence in skills, sufficient fitness, medical events, and self-efficacy. Environmental ones were: support from other people, assistive devices for mobility and care, information related to possibilities for adapted sports and accessibility of sports facilities. |
| Fischer et al. (2015) [16], Canada | SB N = 11 (children) N = 10 (parents) | Qualitative, phenomenology: the experiences around continence issues, social participation, and peer relationships | Semi-structured interview (1) normal versus different; (2) independence, ownership and the road to continence; (3) peer relationships and acceptance | Children with SB that achieved bladder continence were more independent and participated in more social activities. |
| Marques et. al. (2015) [17], Portugal | SB N = 31 (10–17) | Quantitative, cross-sectional: psychosocial correlates of physical activity | Physical activity and psychosocial survey | Only 38.7% of the children participated in both organised and non-organised physical activity. Results did not support the relationship between participation in physical activities and psychosocial correlates. Only perception of competence (OR = 9.55, 1.06–85.99, p < 0.05) had the positive association with participation in non-organized physical activity |
| Flanagan et al. (2013) [18], USA | N = 137 (5–18) SB n = 54 Spinal cord injury (SCI) = 83 | Quantitative, cross-sectional: psychosocial outcomes (including community participation) of children and adolescents with early-onset SCI and SB | Children’s Assessment of Participation and Enjoyment (CAPE) | Children with SCI and SB had similar levels of participation with intensity score 2.1 for children with SB and 2.2 for children with SCI (out of a possible 7). Participants with SB participated in fewer activities (diversity score 23.9 out of possible 55) than those with paraplegic SCI (diversity score 23.9) |
| Peny-Dahlstrand et al. (2013) [19], Sweden | SB N = 50 (6–14) | Quantitative, population-based, cross-sectional cool participation, motor and process skills in task performance | Availability and Participation Scale (APS), School function assessment (SFA) | 89.6% of children showed a low level of active participation and involvement in school activities even though their frequency of participation was high. Motor and process skills were the most significant determinant of participation. |
| Kelly et al. (2011) [20], USA | SB N = 63 n = 19 (2–5) n = 21 (6–12) n = 23 (13–18) | Quantitative, cross-sectional: demographic and SB related factors affecting community participation | Assessment of Preschool Children’s Participation (APCP), CAPE | Adolescent’s participation in recreational, physical, and skill-based activities was lower compared to younger children. Social participation was positively associated with caregiver employment. Physical and skill-based activities were negatively related to the presence of a shunt and recent major medical issues. Bladder and bowel incontinence was a barrier to participation for children ages 6–12. |
| Liptak et al. (2010) [21], USA | SB N = 130 (13–17) | Quantitative, population-based, prospective: outcomes and factors affecting social participation | International Classification of Functioning, Disability and Health (ICF) based survey | 76% of adolescents with SB were competitively employed or attended school, 15% spend time with friends and were going on dates, and 30% had a driver’s license or learner’s permit. |
| Boudos et al. (2008) [22], USA | SB N = 101 (10–32) n = 31 (10–17) | Quantitative, cross-sectional: community participation and barriers to community participation | Medical conditions, function, psychosocial issues, activities, community participation survey | Only 30% of children with SB took part in an organised social activity at least once a week. The most frequent barriers identified were low motivation (38%), lack of information (25%) and time constraints (21%). |
| Field et al. (2001) [23], Australia | N = 166 SB = 97 cystic fibrosis (CF) = 69 | Quantitative, cross-sectional: sport and recreational activities | Sport and recreation facilities survey | 63% of parents of children with SB and 23% of parents of children with CF reported that their children had limited variety of opportunities for sport and recreation activities. |
| Connor-Kuntz et al. (1995) [24], USA | SB N = 133 (7–16) | Quantitative, cross-sectional: physical education and sport participation | Physical education and sports participation survey | One-third of children with SB did not have the opportunity to participate in physical education with their nondisabled peers. The lowest non-school sports participation was observed for children with SB who walked independently. |
| Measurement | Age Range/ Respondent | Purpose | Content | Scale/Items | Reliability | Validity |
|---|---|---|---|---|---|---|
| Assessment of Preschool Children’s Participation (APCP) [14] | 2 to 5 years and 11 months (children with/without disabilities) Parent | Participation | Activity in the areas of play, skill development, active physical recreation, and social | Diversity and intensity scores in 5 areas: play, skill development, active physical recreation, social activities, and total 45 drawings of everyday activities | * | ** |
| Availability and Participation Scale (APS) [19] | Elementary/high school (5–18 years (children with disabilities) Teacher | Participation, environment | School activities, school environment | 2 scales: availability (27 items), participation (29 items) | * | * |
| Children’s Assessment of Participation and Enjoyment (CAPE) [18,20] | 6–21 years (children with/without disabilities) Self-administered and interviewer-assisted version | Participation | Activity outside mandated school tasks | 2 domains: Informal (40 items) formal (15 items) 5 dimensions assessed for each domain: diversity, intensity, with whom, where, enjoyment, preference 5 activity types: recreational, active physical, social, skill-based, self-improvement | ** | ** |
| School function assessment (SFA) [19] | Elementary/primary school (5–12 years) School professionals | Activity, participation | School/related functional tasks | 3 parts: participation, task support, activity performance | ** | *** |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bakanienė, I.; Žiukienė, L.; Vasiliauskienė, V.; Prasauskienė, A. Participation of Children with Spina Bifida: A Scoping Review Using the International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY) as a Reference Framework. Medicina 2018, 54, 40. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina54030040
Bakanienė I, Žiukienė L, Vasiliauskienė V, Prasauskienė A. Participation of Children with Spina Bifida: A Scoping Review Using the International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY) as a Reference Framework. Medicina. 2018; 54(3):40. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina54030040
Chicago/Turabian StyleBakanienė, Indrė, Laura Žiukienė, Vaida Vasiliauskienė, and Audronė Prasauskienė. 2018. "Participation of Children with Spina Bifida: A Scoping Review Using the International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY) as a Reference Framework" Medicina 54, no. 3: 40. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina54030040