Association between the Vicious Cycle of Diabetes-Associated Complications and Glycemic Control among the Elderly: A Systematic Review



Abstract
:1. Introduction
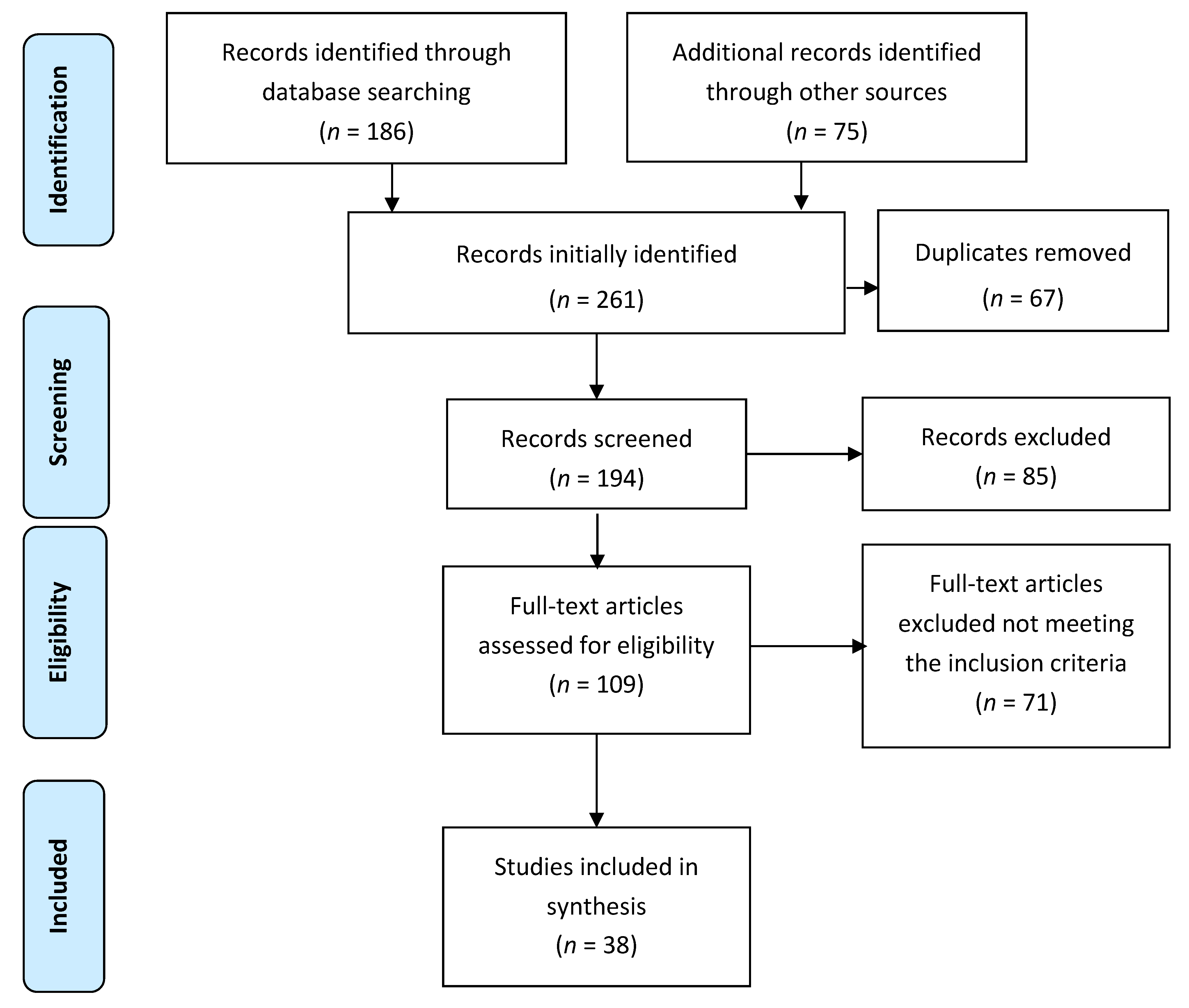
2. Methods
2.1. Search Methods
2.2. Data Extraction (Selection and Coding)
2.3. Risk of Bias (Quality) Assessment
2.4. Strategy for Data Synthesis
3. Results
3.1. Characteristics of Selected Studies
3.2. Study Evaluation Criteria
4. Discussion
4.1. Interrelationship between Diabetes-Associated Complications and Clinical Outcomes
4.1.1. Depression
4.1.2. Impaired Cognition
4.2. Poor Physical Functioning
4.2.1. Frailty
4.2.2. Pain
4.3. Malnutrition
4.4. Poor Self-Care
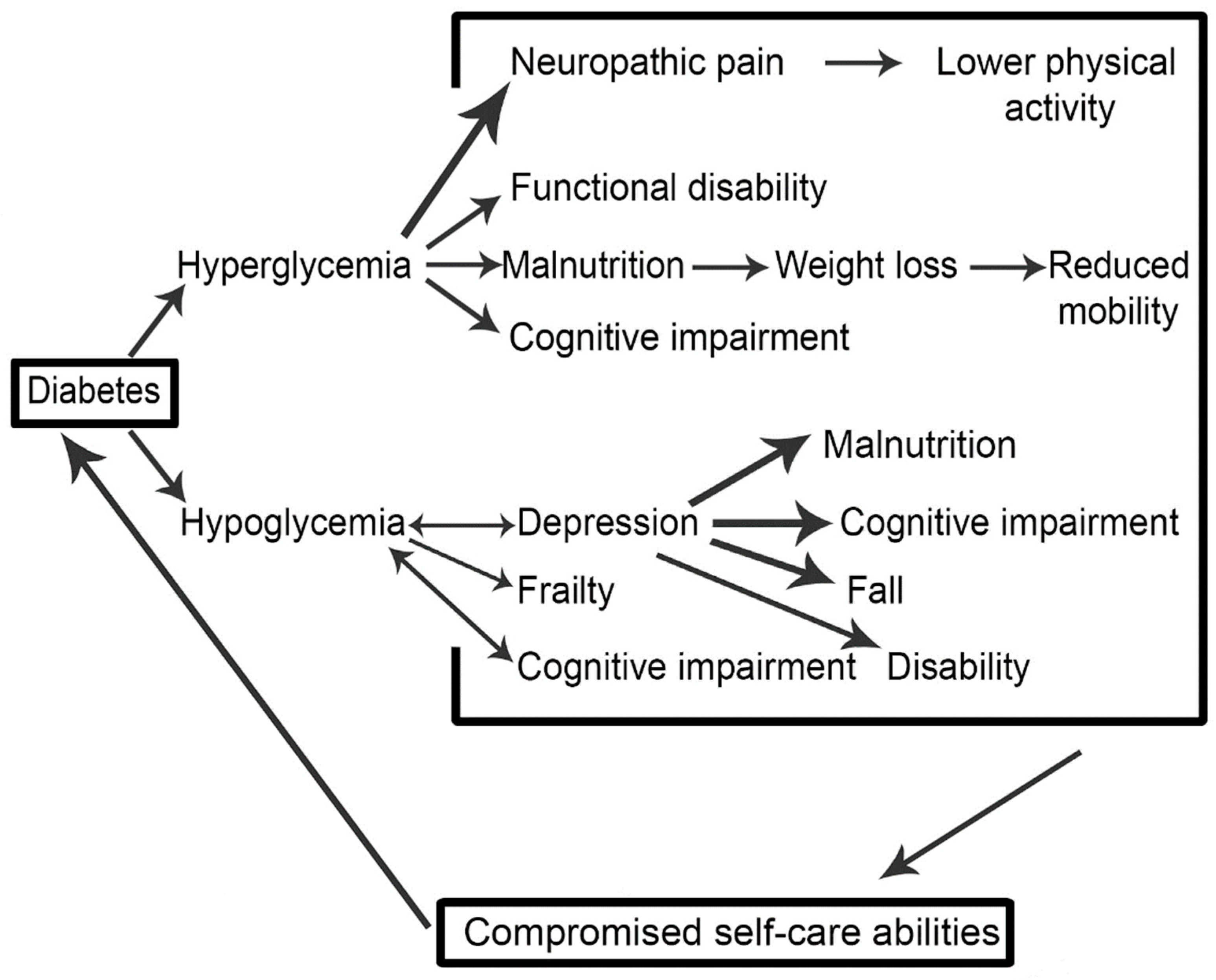
4.5. A Schema of the Vicious Cycle of Diabetes-Associated Complications (DAC) and Their Outcomes
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Diabetes (Key Facts). Available online: http://www.who.int/mediacentre/factsheets/fs312/en/ (accessed on 30 June 2016).
- Samaras, K.; Sachdev, P.S. Diabetes and the elderly brain: Sweet memories? Ther. Adv. Endocrinol. Metab. 2012, 3, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Bourdel Marchasson, I.; Doucet, J.; Bauduceau, B.; Berrut, G.; Blickle, J.F.; Brocker, P.; Constans, T.; Fagot Campagna, A.; Kaloustian, E.; Lassmann Vague, V.; et al. Key priorities in managing glucose control in older people with diabetes. J. Nutr. Health Aging 2009, 13, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Araki, A.; Ito, H. Diabetes mellitus and geriatric syndromes. Geriatr. Gerontol. Int. 2009, 9, 105–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Awad, N.; Gagnon, M.; Messier, C. The relationship between impaired glucose tolerance, type 2 diabetes, and cognitive function. J. Clin. Exp. Neuropsychol. 2004, 26, 1044–1080. [Google Scholar] [CrossRef] [PubMed]
- Black, S.A.; Markides, K.S.; Ray, L.A. Depression predicts increased incidence of adverse health outcomes in older Mexican Americans with type 2 diabetes. Diabetes Care 2003, 26, 2822–2828. [Google Scholar] [CrossRef] [PubMed]
- Chou, K.L.; Chi, I. Functional disability related to diabetes mellitus in older Hong Kong Chinese adults. Gerontology 2005, 51, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Ciechanowski, P.S.; Katon, W.J.; Russo, J.E.; Hirsch, I.B. The relationship of depressive symptoms to symptom reporting, self-care and glucose control in diabetes. Gen. Hosp. Psychiatry 2003, 25, 246–252. [Google Scholar] [CrossRef]
- International Diabetes Federation. International Diabetes Federation Managing Older People with Type 2 Diabetes Global Guidelines; International Diabetes Federation: Brussels, Belgium, 2013. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Kmet, L.M.; Lee, R.C.; Cook, L.S. Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields. Available online: http://0-www-biomedcentral-com.brum.beds.ac.uk/content/supplementary/1471-2393-14-52-s2.pdf (accessed on 30 June 2016).
- Blazer, D.G.; Moody-Ayers, S.; Craft-Morgan, J.; Burchett, B. Depression in diabetes and obesity: Racial/ethnic/gender issues in older adults. J. Psychosom. Res. 2002, 53, 913–916. [Google Scholar] [CrossRef]
- Munshi, M.; Grande, L.; Hayes, M.; Ayres, D.; Suhl, E.; Capelson, R.; Lin, S.; Milberg, W.; Weinger, K. Cognitive dysfunction is associated with poor diabetes control in older adults. Diabetes Care 2006, 29, 1794–1799. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, K.; Haan, M.; Blackwell, T.; Cherkasova, E.; Whitmer, R.A.; West, N. Metabolic syndrome and cognitive decline in elderly Latinos: Findings from the Sacramento Area Latino Study of Aging study. J. Am. Geriatr. Soc. 2007, 55, 758–762. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, K.; Falvey, C.M.; Hamilton, N.; Harris, T.B.; Simonsick, E.M.; Strotmeyer, E.S.; Shorr, R.I.; Metti, A.; Schwartz, A.V.; Health, A.B.C.S. Association between hypoglycemia and dementia in a biracial cohort of older adults with diabetes mellitus. JAMA Intern. Med. 2013, 173, 1300–1306. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, K.; Falvey, C.; Hamilton, N.; Schwartz, A.V.; Simonsick, E.M.; Satterfield, S.; Cauley, J.A.; Rosano, C.; Launer, L.J.; Strotmeyer, E.S.; et al. Diabetes, glucose control, and 9-year cognitive decline among older adults without dementia. Arch. Neurol. 2012, 69, 1170–1175. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.S.; Burcham, J.; Cheng, H. Diabetes mellitus is associated with an increased risk of falls in elderly residents of a long-rerm care facility. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 1157–1162. [Google Scholar] [CrossRef] [PubMed]
- Nelson, J.M.; Dufraux, K.; Cook, P.F. The relationship between glycemic control and falls in older adults. J. Am. Geriatr. Soc. 2007, 55, 2041–2044. [Google Scholar] [CrossRef] [PubMed]
- Kalyani, R.R.; Saudek, C.D.; Brancati, F.L.; Selvin, E. Association of diabetes, comorbidities, and A1C with functional disability in older adults: Results from the National Health and Nutrition Examination Survey (NHANES), 1999–2006. Diabetes Care 2010, 33, 1055–1060. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.K.; Jones, R.N.; Milberg, W.P.; Tennstedt, S.; Talbot, L.; Morris, J.N.; Lipsitz, L.A. Effect of blood pressure and diabetes mellitus on cognitive and physical functions in older adults: A longitudinal analysis of the advanced cognitive training for independent and vital elderly cohort. J. Am. Geriatr. Soc. 2005, 53, 1154–1161. [Google Scholar] [CrossRef] [PubMed]
- Lin, E.H.; Katon, W.; Von Korff, M.; Rutter, C.; Simon, G.E.; Oliver, M.; Ciechanowski, P.; Ludman, E.J.; Bush, T.; Young, B. Relationship of depression and diabetes self-care, medication adherence, and preventive care. Diabetes Care 2004, 27, 2154–2160. [Google Scholar] [CrossRef] [PubMed]
- Dhamoon, M.S.; Moon, Y.P.; Paik, M.C.; Sacco, R.L.; Elkind, M.S. Diabetes predicts long-term disability in an elderly urban cohort: The Northern Manhattan Study. Ann. Epidemiol. 2014, 24, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Egede, L.E.; Osborn, C.Y. Role of motivation in the relationship between depression, self-care, and glycemic control in adults with type 2 diabetes. Diabetes Educ. 2010, 36, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Krein, S.L.; Heisler, M.; Piette, J.D.; Makki, F.; Kerr, E.A. The effect of chronic pain on diabetes patients’ self-management. Diabetes Care 2005, 28, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, A.V.; Hillier, T.A.; Sellmeyer, D.E.; Resnick, H.E.; Gregg, E.; Ensrud, K.E.; Schreiner, P.J.; Margolis, K.L.; Cauley, J.A.; Nevitt, M.C.; et al. Older women with diabetes have a higher risk of falls: A prospective study. Diabetes Care 2002, 25, 1749–1754. [Google Scholar] [CrossRef] [PubMed]
- Galer, B.S.; Gianas, A.; Jensen, M.P. Painful diabetic polyneuropathy: Epidemiology, pain description, and quality of life. Diabetes Res. Clin. Pract. 2000, 47, 123–128. [Google Scholar] [CrossRef]
- Maraldi, C.; Volpato, S.; Penninx, B.W.; Yaffe, K.; Simonsick, E.M.; Strotmeyer, E.S.; Cesari, M.; Kritchevsky, S.B.; Perry, S.; Ayonayon, H.N.; et al. Diabetes mellitus, glycemic control, and incident depressive symptoms among 70- to 79-year-old persons: The health, aging, and body composition study. Arch. Intern. Med. 2007, 167, 1137–1144. [Google Scholar] [CrossRef] [PubMed]
- Marden, J.R.; Mayeda, E.R.; Tchetgen, E.J.T.; Kawachi, I.; Glymour, M.M. High Hemoglobin A1c and Diabetes Predict Memory Decline in the Health and Retirement Study. Alzheimer Dis. Assoc. Disord. 2017, 31, 48. [Google Scholar] [CrossRef] [PubMed]
- Turnbull, P.; Sinclair, A. Evaluation of nutritional status and its relationship with functional status in older citizens with diabetes mellitus using the Mini Nutritional Assessment (MNA) tool. A preliminary investigation. J. Nutr. Health Aging 2002, 6, 185–189. [Google Scholar] [PubMed]
- Sinclair, A.J.; Conroy, S.P.; Bayer, A.J. Impact of diabetes on physical function in older people. Diabetes Care 2008, 31, 233–235. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, A.J.; Girling, A.J.; Bayer, A.J. Cognitive dysfunction in older subjects with diabetes mellitus: Impact on diabetes self-management and use of care services. Diabetes Res. Clin. Pract. 2000, 50, 203–212. [Google Scholar] [CrossRef]
- Davies, M.; Brophy, S.; Williams, R.; Taylor, A. The prevalence, severity, and impact of painful diabetic peripheral neuropathy in type 2 diabetes. Diabetes Care 2006, 29, 1518–1522. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Wang, J.; Zheng, P.; Haardorfer, R.; Kegler, M.C.; Zhu, Y.; Fu, H. Effects of self-care, self-efficacy, social support on glycemic control in adults with type 2 diabetes. BMC Fam. Pract. 2013, 14, 66. [Google Scholar] [CrossRef] [PubMed]
- Fung, A.C.; Tse, G.; Cheng, H.L.; Lau, E.S.; Luk, A.; Osaki, R.; So, T.T.; Wong, R.Y.; Tsoh, J.; Chow, E. Depressive symptoms and glycemic control in Hong Kong Chinese elderly patients with type 2 diabetes mellitus. Front. Endocrinol. 2018, 9, 261. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, R.E.; Andrew, M.K.; Fallah, N.; Rockwood, K. Comparison of the prognostic importance of diagnosed diabetes, co-morbidity and frailty in older people. Diabet. Med. 2010, 27, 603–606. [Google Scholar] [CrossRef] [PubMed]
- Thiel, D.M.; Al Sayah, F.; Vallance, J.K.; Johnson, S.T.; Johnson, J.A. Association between physical activity and health-related quality of life in adults with type 2 diabetes. Can. J. Diabetes 2017, 41, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Meneilly, G.S.; Berard, L.D.; Cheng, A.Y.; Lin, P.J.; MacCallum, L.; Tsuyuki, R.T.; Yale, J.-F.; Nasseri, N.; Richard, J.-F.; Goldin, L. Insights into the current management of older adults with type 2 diabetes in the Ontario primary care setting. Can. J. Diabetes 2018, 42, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Ulger, Z.; Halil, M.; Kalan, I.; Yavuz, B.B.; Cankurtaran, M.; Gungor, E.; Ariogul, S. Comprehensive assessment of malnutrition risk and related factors in a large group of community-dwelling older adults. Clin. Nutr. 2010, 29, 507–511. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, Z.G.; Uzunlulu, M.; Caklili, O.T.; Mutlu, H.H.; Oguz, A. Malnutrition rate among hospitalized patients with type 2 diabetes mellitus. Prog. Nutr. 2018, 20, 183–188. [Google Scholar]
- Pijpers, E.; Ferreira, I.; de Jongh, R.T.; Deeg, D.J.; Lips, P.; Stehouwer, C.D.; Nieuwenhuijzen Kruseman, A.C. Older individuals with diabetes have an increased risk of recurrent falls: Analysis of potential mediating factors: The Longitudinal Ageing Study Amsterdam. Age Ageing 2012, 41, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Vischer, U.M.; Perrenoud, L.; Genet, C.; Ardigo, S.; Registe-Rameau, Y.; Herrmann, F.R. The high prevalence of malnutrition in elderly diabetic patients: Implications for anti-diabetic drug treatments. Diabet. Med. 2010, 27, 918–924. [Google Scholar] [CrossRef] [PubMed]
- Pai, Y.-W.; Lin, C.-H.; Lee, I.-T.; Chang, M.-H. Variability of fasting plasma glucose and the risk of painful diabetic peripheral neuropathy in patients with type 2 diabetes. Diabetes Metab. 2018, 44, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Tabesh, M.; Shaw, J.E.; Zimmet, P.Z.; Söderberg, S.; Koye, D.N.; Kowlessur, S.; Timol, M.; Joonas, N.; Sorefan, A.; Gayan, P. Association between type 2 diabetes mellitus and disability: What is the contribution of diabetes risk factors and diabetes complications? J. Diabetes 2018, 10, 744–752. [Google Scholar] [CrossRef] [PubMed]
- Tharek, Z.; Ramli, A.S.; Whitford, D.L.; Ismail, Z.; Zulkifli, M.M.; Sharoni, S.K.A.; Shafie, A.A.; Jayaraman, T. Relationship between self-efficacy, self-care behaviour and glycaemic control among patients with type 2 diabetes mellitus in the Malaysian primary care setting. BMC Fam. Pract. 2018, 19, 39. [Google Scholar] [CrossRef] [PubMed]
- Aro, A.-K.; Karjalainen, M.; Tiihonen, M.; Kautiainen, H.; Saltevo, J.; Haanpää, M.; Mäntyselkä, P. Glycemic control and health-related quality of life among older home-dwelling primary care patients with diabetes. Prim. Care Diabetes 2017, 11, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Zuberi, S.I.; Syed, E.U.; Bhatti, J.A. Association of depression with treatment outcomes in Type 2 Diabetes Mellitus: A cross-sectional study from Karachi, Pakistan. BMC Psychiatry 2011, 11, 27. [Google Scholar] [CrossRef] [PubMed]
- Weinger, K.; Beverly, E.A.; Smaldone, A. Diabetes self-care and the older adult. West. J. Nurs. Res. 2014, 36, 1272–1298. [Google Scholar] [CrossRef] [PubMed]
- Pasquier, F.; Boulogne, A.; Leys, D.; Fontaine, P. Diabetes mellitus and dementia. Diabetes Metab. 2006, 32, 403–414. [Google Scholar] [CrossRef]
- Wu, J.H.; Haan, M.N.; Liang, J.; Ghosh, D.; Gonzalez, H.M.; Herman, W.H. Impact of antidiabetic medications on physical and cognitive functioning of older Mexican Americans with diabetes mellitus: A population-based cohort study. Ann. Epidemiol. 2003, 13, 369–376. [Google Scholar] [CrossRef]
- Goodpaster, B.H.; Park, S.W.; Harris, T.B.; Kritchevsky, S.B.; Nevitt, M.; Schwartz, A.V.; Simonsick, E.M.; Tylavsky, F.A.; Visser, M.; Newman, A.B. The loss of skeletal muscle strength, mass, and quality in older adults: The health, aging and body composition study. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Mathur, S.; Zammitt, N.N.; Frier, B.M. Optimal glycaemic control in elderly people with type 2 diabetes: What does the evidence say? Drug Saf. 2015, 38, 17–32. [Google Scholar] [CrossRef] [PubMed]
- Marchettini, P.; Lacerenza, M.; Mauri, E.; Marangoni, C. Painful peripheral neuropathies. Curr. Neuropharmacol. 2006, 4, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Schmader, K.E. Epidemiology and impact on quality of life of postherpetic neuralgia and painful diabetic neuropathy. Clin. J. Pain 2002, 18, 350–354. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Koirala, J.; Khardori, R.; Khardori, N. Infections in diabetes mellitus and hyperglycemia. Infect. Dis. Clin. N. Am. 2007, 21, 617–638. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.V.; Guralnik, J.M.; Dansie, E.J.; Turk, D.C. Prevalence and impact of pain among older adults in the United States: Findings from the 2011 National Health and Aging Trends Study. Pain 2013, 154, 2649–2657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinger, K.; Butler, H.A.; Welch, G.W.; La Greca, A.M. Measuring diabetes self-care: A psychometric analysis of the Self-Care Inventory-Revised with adults. Diabetes Care 2005, 28, 1346–1352. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Sr. No. | Inclusion Criteria |
|---|---|
| 1 | Studies on diabetes-associated complications published during the period from 1 January 2000 to 22 September 2018. |
| 2 | All original research articles describing the association between diabetes, diabetes-associated complications, and glycemic control in the elderly, available in the scientific literature. |
| 3 | Studies conducted in elderly (≥60 years) diabetic patients. |
| 4 | Studies having quality evaluation scores of >66%. |
| Exclusion criteria | |
| 1 | Studies published in a language other than English. |
| 2 | Studies without clear inclusion and exclusion criteria. |
| 3 | Studies without clearly stated outcomes. |
| (First Author) (Year) (Country) | Main Objective | Design | Setting | Type of Diabetes | Sample Demographics | Main Results |
|---|---|---|---|---|---|---|
| Blazer, D.G. (1986–1997) (US) [12] | Assessment of association between depression, obesity and diabetes. | Observational, cross-sectional and longitudinal survey | House hold survey | Not specified | N = 4162 Age ≥ 65 years | In the controlled and uncontrolled analyses, functional impairment (p < 0.001), female gender (p < 0.05), cognitive impairment (p < 0.01), and lower education were found to be associated with depression, diabetes, and high BMI (p < 0.05). The frequency of comorbidity between depression and diabetes was 2.6%. |
| Black, S.A. (1995–2001) (US) [6] | Assessment of impact of diabetes and depression on poor health outcomes in diabetes patients. | Longitudinal survey | In-home face-to-face interviews | T2DM | N = 2830 Age ≥65 years | Significant relationship was seen between depression and diabetes. About 24% of the patients had minor depression, 9% of the patients had major depression, and 47% of the patients had diabetes with minimum levels of depression. |
| Chiechanowski, P.S. (1999) (US) [8] | Assessment of association between diabetes, depression, PF, self-care, and HbA1c levels. Moreover, assessment of intensity of depression and HbA1c levels in patients with T1DM as compared the patients with T2DM. | Cross-sectional observational study | Tertiary care specialty clinic | T1DM, T2DM | N = 276 T1DM patients N = 199 T2DM patients Mean age of the relevant group = 48.8 ± 15.9 years | A significant association was seen between depression, glycemic control (p < 0.0001), HbA1c levels (p < 0.0001), PF (p < 0.01), and adherence to self-care behavior (p < 0.0001). Similarly, a significantly greater number (66.7%) of T1DM patients with HbA1c levels >8 were found to be depressed than T2DM depressed patients (37.5%) (p = 0.02). |
| Zuberi, S.I. (2008–2009) (Pakistan) [46] | Assessment of association between depression, self-care, and diabetes. | Cross-sectional study | Tertiary care hospital | T2DM | N = 286 diabetes patients Age = 31–60 years | Depression in male diabetes patients was lesser than female diabetes patients by the values; 39.2 and 60.8 respectively (p = 0.03). Moreover, HbA1c levels were significantly higher in depressed patients than in non-depressed diabetes patients (8.5% vs. 7.7%, p < 0.001). |
| Munshi, M. (2005) (US) [13] | Assessment of the association between cognitive dysfunction and glycemic control. | Cross-sectional study | Geriatric diabetic clinic | Not specified | N = 60 Age ≥ 70 years | Results showed that 34% of diabetes patients had low scores of CIB, whereas 38% of the patients had low CDT scores. Both the tests CIB (r = −0.37, p < 0.004) and CDT (r = −0.38, p < 0.004) had an inverse correlation with HbA1c levels. Furthermore, 33% of the patients were depressed, and 33% of the patients had history of falls, whereas 39% of the patients had poor IADL scores. |
| Yaffe, K.Y. (1998–1999) (US) [14] | To investigate the association between metabolic syndrome and cognitive function, and effect of inflammation on this association. | Longitudinal cohort study | Sacramento area and the surrounding California counties | Hyperglycemia associated with metabolic syndrome | N = 1624 Age ≥ 60 years | Rate of cognitive decline was found to be greater in patients with metabolic syndrome having hyperglycemia. Low scores of DelRec (p = 0.02) proved the finding. Similarly, low 3MS scores (p = 0.03) in the patients with inflammation, showed the impact of inflammation on cognitive decline. |
| Yaffe, K. (1997–2006) (US) [16] | Association between diabetes and cognitive decline and impact of glycemic control on cognitive function. | Prospective cohort study | Community clinics | Not specified | N = 3069 Age = 70–79 years | Participants with DM showed decline in cognitive function, and had low scores of cognitive status, i.e., 3MS (p = 0.001) and DSS (p = 0.001). Likewise, a significant association was also observed between HbA1c levels and cognitive decline, which was shown by low 3MS (p = 0.003) and DSS (p = 0.04) scores in the diabetes patients. |
| Yaffe, K. (1997–2008) (US) [15] | Assessment of association between hypoglycemia and dementia. | Prospective study | General population | Not specified | N = 783 Age = 70–79 years | Results indicated that 7.8% of diabetes patients had incidence of hypoglycemia, whereas 18.9% of the patients suffered from dementia. The incidence of dementia was double in patients facing hypoglycemia (p < 0.001). In the same way, the patients having dementia were at a higher risk of developing hypoglycemia (p < 0.001). |
| Turnbull, P.J. (2002) (UK) [29] | Assessment of nutritional status in diabetes patients and its impact on PF. | Case control study | General community | Not specified | N = 35 diabetes patients N = 35 non-diabetes patients Age > 65 years | Diabetes patients scored significantly lower on MNA (p < 0.01). These scores had significant correlation with BI (p < 0.01). |
| Vischer, U.M. (2010) (Switzerland) [41] | Assessment of prevalence of malnutrition elderly. | Prospective study | The Geneva Geriatric Hospital | Not specified | N = 146 Age > 65 years | Low scores of MNA indicated high prevalence of malnutrition in 77.1% of the diabetes patients. Moreover, in these patients, MNA scores were significantly associated with HbA1c levels (p = 0.0014). |
| Hubbard, R.E. (Canada) (2010) [35] | Comparison of prognostic value of frailty and number and severity of co-morbidities in older diabetes patients. | Longitudinal prospective cohort study | General community in five Canadian regions | Not specified | N = 2305 Age ≥ 70 years | There was a strong relationship between diabetes and medium-term mortality HR = 1.42 (CI 95% = 1.2–1.69). Frail diabetes patients had 2.62 times (CI 95% = 1.36–5.06) greater tendency of having diabetes complications than non-diabetes patients of same age. Moreover, the diabetes patients had more co-morbidities than non-diabetes patients (p < 0.005). |
| Maurer, M.S. (2005) (US) [17] | To investigate the association between diabetes and the risk of falls in the elderly. | Prospective cohort study | A long-term care facility | Not specified | N = 139 Age ≥ 60 years | The incidence rate for falls in diabetic patients as compared to non-diabetic patients was 70% and 30% respectively (p < 0.001). |
| Nelson, J.M. (2007) (US) [18] | Assessment of association between glycemic control and risk of falls in frail and non-frail elderly diabetes patients. | Retrospective, case-control study | A health maintenance organization | Not specified | N = 111 Age ≥ 75 years | Risk of falls increased in the patients with HbA1c levels ≤7 (p = 0.01). |
| Kalyani, R.R. (2010) (US) [19] | Assessment of the association between diabetes and functional disability in older adults, and the impact of HbA1c levels and other comorbidities on this association. | Cross-sectional, retrospective study | General community non, institutionalized population | Not specified | N = 6097 civilians Age ≥ 60 years | The prevalence of disability in GPA of the patients was found to be 73.6%, in LEM 52.2% and in IADL 43.6%. In addition, diabetes was associated with increased chances of disability by 2–3 times (p < 0.05). CVD and poor glycemic control had up to 85% more chance of diabetes-associated disabilities. |
| Kuo, H.K. (2005) (US) [20] | Assessment of the impact of BP and DM on physical and cognitive function. | Longitudinal prospective study | Independent living older subjects in six field sites in the US | Not specified | N = 2802 Age = 65–94 years | In terms of PF, patients with stage 1 (p = 0.03) and stage 2 (p = 0.007) hypertension showed a faster reduction in PF; similarly, those with DM also showed a decline in PF (p = 0.005), specifically in IADL. With respect to cognitive function, BP showed negative impact on memory (p = 0.008), stage 1 (p = 0.03), and stage 2 (p = 0.005) hypertension resulted in a reduction in reasoning; however, DM was a cause of a reduction in cognitive function DSS (p = 0.02). |
| Sinclair, A.J. (2008) (UK) [30] | Assessment of the nature of functional deterioration in older diabetes patients. | Case control study | General community | Not specified | N = 403 cases N = 403 controls Age ≥ 65 years | Diabetes patients had a greater number of comorbidities than non-diabetic patients (p < 0.0001) and they had a greater risk of severe functional deterioration (p < 0.001). |
| Lin, E.H. (2004) (US) [21] | Assessment of association between self-care of diabetes medication adherence, preventative services, and depression. | Cross-sectional and longitudinal retrospective survey | Primary care clinics | T2DM | N = 4500 Mean age of the relevant group = 63 ± 13.4 years. | Results show that 19.5% (p < 0.005) of the patients were non-adherent to the therapy, while 12% of the patients had major depression, which had an association with lower PF (p < 0.0001). Moreover, the depressed patients also had poor self-care activities (p < 0.0001). |
| Chou, K.L. & Chi, I. (1996) (China) [7] | Assessment of association between diabetes and disability, and the impact of diabetes complications on this association. | Cross-sectional study | Non-institutionalized population (general community) | Not specified | N = 2003 Age ≥ 60 years | Diabetic patients had a greater risk of poor performance of ADLs and IADLs than non-diabetic patients, and their inability to perform self-care was 3.5 times greater than non-diabetic patients (p < 0.01). |
| Dhamoon, M.S. (1993–2001) (US) [22] | To evaluate that diabetes acts as a long-term predictor of disability. | Prospective cohort study | General community | Not specified | N = 3298 Mean age of the relevant group = 69.2 years | Annual decline (p < 0.0001) in PF was found in the patients. |
| Egede, L.E. & Osborn, C.Y. (2008) (US) [23] | To evaluate the impact of depression on glycemic control and self-care. | Cross-sectional study | Internal medicine clinic | T2DM | N = 126 Mean age of the relevant group = 62.7 ± 11.8 years | Depression was negatively associated with social support (p = 0.002) and self-care activities (p = 0.004). Self-care of diabetes was partially associated with glycemic control (p = 0.08). |
| Gao, J. (2011) (China) [33] | To assess the impact of social support, self-efficacy, and self-care on glycemic control. | Cross-sectional study | Primary healthcare center | T2DM | N = 222 Age = 44–80 years | Self-care directly affected the glycemic control (p = 0.007); however, social support (p = 0.009), self-efficacy (p < 0.001), and PPC had an indirect effect on glycemic control. |
| Krein, S.L. (1998–1999) (US) [24] | Assessment of the association between chronic pain and diabetes self -management. | Cross-sectional study | Healthcare center | Not specified | N = 993 Age = 64 ± 10 years | Diabetes patients with chronic pain showed poor diabetes self-management and self-care (p = 0.002); similarly, those with severe or very severe chronic pain also reported poor self-management (p = 0.003) of diabetes. |
| Maraldi, C. (2001–2007) (US) [27] | Assessment of association between diabetes and depression. | Prospective cohort study | General community | Not specified | N = 2522 Age = 70–79 years | Diabetic patients had increased risk of depressed mood (p = 0.02) and recurrent depressed mood (p < 0.001) than non-diabetic patients. |
| Pijpers, E. (2009–2012) (Netherlands) [40] | Investigation of association between the risks of intermittent falls along with factors associated with it, and diabetes. | Longitudinal cohort study | General community | Not specified | N = 1145 Age ≥65 years | About 30% of the patients with diabetes had intermittent falls with an incidence rate of 129.7 per 1000 persons/year whereas, 19.4% of the subjects without diabetes had an incidence rate of intermittent falls recorded as 77.4 per 1000 persons/year HR = 1.67 (CI 95% = 1.11–2.51). Moreover, numerous physical and mental factors associated with diabetes, increased the risk of falls in diabetes patients by 47% HR = 1.3 (CI 95% = 0.79–2.11). |
| Schwartz, A.V. (1988–1994) (US) [25] | To assess the association between diabetes and risk of falls in older female diabetes patients. | Prospective cohort study | General community | Not specified | N = 9249 Age ≥ 67 years | Women with diabetes had more falls during follow-up (p <0.01). Diabetes and insulin use was associated with increased risk of falling among the patients i.e., more than once a year. |
| Sinclair, A.J. (2000) (UK) [31] | Assessment of linkage between impaired cognition self-care abilities among diabetes patients. | Case control study | General community | Not specified | N = 396 cases N = 393 controls Age ≥ 65 years | Diabetes patients having MMSE scores <23 had low levels of self-care (p < 0.001) and monitoring (p < 0.001). Association between low MMSE scores and higher hospitalization (p = 0.001), lower ADL (p < 0.001) and need of help in personal care (p = 0.001) was also seen. |
| Ulger, Z. (2002–2004) (Turkey) [38] | Assessment of malnutrition and factors associated with it in elderly. | Cross-sectional | Out-patient clinic | Not specified | N = 2327 Age ≥ 65 years | According to the results, 28% of the patients had poor MNA scores, which were mostly affected by depression (p = 0.0001), physical dependence (p = 0.0001), fasting plasma glucose level (p = 0.005), hematocrit (p = 0.005), ESR (p = 0.03), albumin (p = 0.002), bone mineral density (p = 0.007), and chronic diseases including diabetes (p = 0.820). The ratio of diabetes patients with and without the risk of malnutrition was 23.7%:24.2%. |
| Davies, M. (2006) (UK) [32] | Assessment of PDPN together with its severity and impact. | Cross-sectional descriptive study | General community | T2DM | N = 595 Mean age of relevant group = 67.1 ± 11.5 years | During the first phase of the study, 63.8% of the patients identified with pain. In the second phase, PDPN was found in about 19% of the patients. Furthermore, 36.8% of the patients suffered from non-neuropathic pain, and 7.4% of the patients had mixed pain. The prevalence of PDPN among the patients was 26.4%, and about 80% of those with PDPN reported moderate to severe pain, impairing their quality of life OR = 1.7 (CI 95% = 0.4–2.9%). |
| Galer, B.S. (1999) (US) [26] | Assessment of the nature and scope of PDN. | Cross-sectional study | Patients enrolled in a clinical trial | Not specified | N = 105 Age ≥ 60 years | Around 96% of the patients felt pain associated with neuropathy on their feet. Over half (53%) of the patients felt consistent pain which had become severe since the onset of PDN. |
| Thiel, D.M. (2011–2013) (Canada) [36] | To assess the association of compliance between physical activity recommendations and HRQoL in T2DM patients. | Prospective cohort study | Diabetes clinics, Public advertisement, primary care centers | T2DM | N = 1948 Mean Age = 64.5± 10.8 years | Results showed that 78.6% of the patients did not conform to the physical activity recommendations, while patients meeting the recommendations showed high scores of PF (p < 0.001), role physical (p = 0.001), body pain (p = 0.001), and physical component summary (p < 0.001) compared to the patients not meeting the required criteria. |
| Tabesh M. (2015) (Mauritius) [43] | Assessment of association between T2DM and physical functional disability. Moreover, determination of the degree of the association between related risk factors and diabetes. | Cross-sectional study | General community | T2DM | N = 3692 Mean Age = 62.1 ± 8.0 | Diabetes was found to have significant association with increased risk of disability, OR = 1.76 (CI 95% = 1.34–2.08), among the study participants, having 13.2% of the prevalence of disability. Significant associations between diabetes and disability was seen among African Creoles OR = 2.03 (CI 95% = 1.16–3.56); whereas obesity highlighted the association between diabetes and disability, with an increased risk in South Asians and African Creoles of 26.3% and 12.1% respectively. The overall results showed a 67% increased risk of disability associated with diabetes. |
| Pai, Y.-W. (2013) (Taiwan) [42] | Assessment of the association between variation in fasting plasma glucose levels and PDPN among the T2DM patients. | Retrospective, case control study | Tertiary care hospital setting | T2DM | N = 2773 (enrolled) N = 626 (randomly selected from total) Age = 72.9 ± 10.5 years | The results showed that variation in fasting plasma glucose was significantly associated with PDPN OR = 4.08 (CI 95% = 1.60–10.42) in the third and fourth quartile, as compared to the first quartile OR = 5.49 (CI 95% = 2.14–14.06). |
| Yildirim, G.Z. (2014–2015) (Turkey) [39] | Assessment of nutritional status of the T2DM hospitalized patients, and highlighting the risk factors of malnutrition among such patients. | Cross-sectional study | Training and research hospital facility | T2DM | N = 104 Age = 65.08 ± 12.57 | Results showed that the rate of malnutrition among the patients was 7.7%, whereas 18.3% patients were at risk of malnutrition. The risk factors of malnutrition among the patients were BMI <25 kg/m2, OR = 4.565 (CI 95% = 1.47–14.13), and duration of diabetes (15–20 years) OR = 5.535 (CI 95% = 1.15–26.6), (>20 years) OR = 7.147 (CI 95% = 1.59–31.96). |
| Tharek, Z. (2014–2015) (Malaysia) [44] | Assessment of the extent of self- efficacy, self-care behavior, and glycemic control and association between self-care behavior and glycemic control. Moreover, assessment of the factors associated with glycemic control among the T2DM patients. | Cross-sectional study | Primary Care Clinics | T2DM | N = 340 Age = 58.34 ± 11.86 | Results showed the mean ± (SD) scores of self-efficacy 7.33 ± (2.25) and self-care behavior was 3.76 ± (1.87); whereas, a positive association existed between these factors r = 0.538 (p < 0.001). An inverse relation was found between self-efficacy and HbA1c, r = −0.41 (p < 0.001). Moreover, high self-efficacy has a significant association with good glycemic state, b = −0.398 (CI 95% = −0.024, −0.014), (p < 0.001) |
| Meneilly, G.S. (2015–2016) (Canada) [37] | Assessment of the status of management of T2DM of the elderly at the primary care clinics. | Cross-sectional study | Primary care clinics | T2DM | N = 833 Age ≥ 65 Years | Results showed that 53% participants had a HbA1c level ≤7%, the percentage of assessment for frailty, cognitive impairment, and depression was 11%, 16%, and 19% respectively; whereas, 88% and 83% assessments were of eye and foot examination respectively. Significant numbers of patients had cognitive impairment (p < 0.0001) and frailty (p < 0.0001), and a history of falls (p = 0.0007). |
| Aro, A.-K. (2015) (Finland) [45] | Assessment of HRQoL and the association between functional capability and glycemic control among the diabetes patients. | Cross-sectional study | Community-based study | Not specified | N = 172 Age > 65 Years | The EQ-5D scores for good glycemic control was 0.78, and for intermediate and poor glycemic control, it was 0.74 and 0.7 respectively (p = 0.037), HbA1c was significantly associated with poor HRQoL, r = 0.16 (CI95% = 0.01–0.31). Similarly, various domains of self-care (p = 0.031), mobility (p = 0.002), and IADL (p = 0.008) were compromised by poor glycemic control. |
| Fung, A.C.H. (2013) (China) [34] | Assessment of the association between depression and cardiac and metabolic risk factors, along with health condition among elderly T2DM patients. | Cross-sectional study | Diabetes center in a hospital setting | T2DM | N = 325 Age ≥ 65 Years | Depression was observed among 13% of the patients, with a positive history of co-morbidities OR = 2.84, (CI 95% = 1.35–6.00) (p = 0.006). The depressed patients had a longer duration of disease (mean disease duration ± (SD), 15.1 ± (9.1) versus 11.6 ± (8.1) years, (p = 0.02), a high frequency of hypoglycemic events (17 versus 6%) (p = 0.003), and poor target achievement (0 versus 16%) (p = 0.004). |
| Marden, J.R. (2006–2012) (USA) [28] | Assessment of association between diabetes, HbA1c and impaired memory among the patients with T2DM. | Prospective cohort Study Case control study (Little doubtful) | General community (noninstitutionalized population) | T2DM | N = 8888 Diabetics = 1837 Non Diabetics = 7051 Age = 67.4 ± 8.8 | Diabetes was found to be significantly associated with a reduction of memory at a 10% faster rate (β = −0.04) per decade (CI 95% -0.06–0.01), an inverse relation was seen between HbA1c and memory loss with a 0.05 SD decline in memory score per decade (CI 95% = 0.08–0.03). |
| Study Name (Reference) | [12] | [38] | [8] | [22] | [13] | [6] | [14] | [16] | [35] | [29] |
| 1. Question/objective sufficiently described? | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 2 |
| 2. Study design evident and appropriate? | 2 | 2 | 2 | 2 | 0 | 1 | 2 | 2 | 1 | 2 |
| 3. Method of subject/comparison group selection or source of information/input variables described and appropriate? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| 4. Subject characteristics sufficiently described? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 1 |
| 5. If interventional and random allocation was possible, was it described? | NA | NA | NA | NA | NA | NA | NA | NA | NA | 1 |
| 6. If interventional and blinding of investigators was possible, was it reported? | NA | NA | NA | NA | NA | NA | NA | NA | NA | 0 |
| 7. If interventional and blinding of subjects was possible, was it reported? | NA | NA | NA | NA | NA | NA | NA | NA | NA | 0 |
| 8. Outcome and exposure measure(s) well-defined and robust to measurement/misclassification bias? Means of assessment reported? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| 9. Sample size appropriate? | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 1 |
| 10. Analytic methods described/justified and appropriate? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| 11. Is some estimate of variance reported for the main results? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| 12. Controlled for confounding factors? | 2 | NA | 1 | 0 | NA | NA | 0 | 0 | NA | 2 |
| 13. Results reported in sufficient detail? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| 14. Conclusions supported by the results? | 2 | 1 | 1 | 1 | 2 | 2 | 0 | 1 | 0 | 2 |
| Total points | 22 | 19 | 20 | 18 | 17 | 19 | 18 | 19 | 16 | 21 |
| Max points possible | 22 | 20 | 22 | 22 | 20 | 20 | 22 | 22 | 20 | 28 |
| Summary score, in percentage | 100% | 95% | 91% | 82% | 85% | 95% | 82% | 86% | 80% | 75% |
| Study Name (Reference) | [32] | [26] | [21] | [17] | [18] | [41] | [7] | [23] | [19] | [46] |
| 1. Question/objective sufficiently described? | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 |
| 2. Study design evident and appropriate? | 2 | 2 | 0 | 2 | 2 | 1 | 2 | 0 | 2 | 2 |
| 3. Method of subject/comparison group selection or source of information/input variables described and appropriate? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 1 |
| 4. Subject characteristics sufficiently described? | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| 5. If interventional and random allocation was possible, was it described? | NA | NA | NA | NA | NA | 2 | NA | NA | NA | NA |
| 6. If interventional and blinding of investigators was possible, was it reported? | NA | NA | NA | NA | NA | 0 | NA | NA | NA | NA |
| 7. If interventional and blinding of subjects was possible, was it reported? | NA | NA | NA | NA | NA | 0 | NA | NA | NA | NA |
| 8. Outcome and exposure measure (s) well-defined and robust to measurement/ misclassification bias? Means of assessment reported? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| 9. Sample size appropriate? | 2 | 1 | 2 | 1 | 2 | 1 | 2 | 1 | 2 | 2 |
| 10. Analytic methods described/justified and appropriate? | 2 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| 11. Is some estimate of variance reported for the main results? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| 12. Controlled for confounding? | NA | NA | NA | 1 | 1 | NA | NA | NA | 1 | 1 |
| 13. Results reported in sufficient detail? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 |
| 14. Conclusions supported by the results? | 2 | 1 | 2 | 1 | 1 | 1 | 2 | 1 | 2 | 2 |
| Total points | 20 | 16 | 17 | 19 | 20 | 18 | 20 | 15 | 20 | 20 |
| Max points possible | 20 | 20 | 20 | 22 | 22 | 26 | 20 | 20 | 22 | 22 |
| Summary score, in percentage | 100% | 80% | 85% | 86% | 91% | 69% | 100% | 75% | 91% | 91% |
| Study Name (Reference) | [33] | [24] | [27] | [40] | [25] | [31] | [15] | [30] | [20] | |
| 1. Question/objective sufficiently described? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | |
| 2. Study design evident and appropriate? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | |
| 3. Method of subject/comparison group selection or source of information/input variables described and appropriate? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | |
| 4. Subject characteristics sufficiently described? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | |
| 5. If interventional and random allocation was possible, was it described? | NA | NA | NA | NA | NA | 0 | NA | NA | NA | |
| 6. If interventional and blinding of investigators was possible, was it reported? | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| 7. If interventional and blinding of subjects was possible, was it reported? | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| 8. Outcome and exposure measure (s) well-defined and robust to measurement/ misclassification bias? Means of assessment reported? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | |
| 9. Sample size appropriate? | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | |
| 10. Analytic methods described/justified and appropriate? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | |
| 11. Is some estimate of variance reported for the main results? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | |
| 12. Controlled for confounding? | NA | NA | NA | NA | NA | NA | 1 | NA | NA | |
| 13. Results reported in sufficient detail? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | |
| 14. Conclusions supported by the results? | 2 | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 1 | |
| Total points | 19 | 20 | 20 | 19 | 20 | 19 | 21 | 18 | 19 | |
| Max points possible | 20 | 20 | 20 | 20 | 20 | 22 | 22 | 20 | 20 | |
| Summary score, in percentage | 95% | 100% | 100% | 95% | 100% | 86% | 95% | 90% | 95% | |
| Study Name (Reference) | [36] | [43] | [39] | [42] | [44] | [37] | [45] | [34] | [28] | |
| 1. Question/objective sufficiently described? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | |
| 2. Study design evident and appropriate? | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | |
| 3. Method of subject/comparison group selection or source of information/input variables described and appropriate? | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | |
| 4. Subject characteristics sufficiently described? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | |
| 5. If interventional and random allocation was possible, was it described? | NA | NA | NA | 2 | NA | NA | NA | NA | 0 | |
| 6. If interventional and blinding of investigators was possible, was it reported? | NA | NA | NA | 0 | NA | NA | NA | NA | 0 | |
| 7. If interventional and blinding of subjects was possible, was it reported? | NA | NA | NA | 0 | NA | NA | NA | NA | 0 | |
| 8. Outcome and exposure measure (s) well-defined and robust to measurement/ misclassification bias? Means of assessment reported? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | |
| 9. Sample size appropriate? | 2 | 2 | 1 | 2 | 2 | 2 | 1 | 2 | 2 | |
| 10. Analytic methods described/justified and appropriate? | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | |
| 11. Is some estimate of variance reported for the main results? | 2 | 2 | 1 | 2 | 2 | 0 | 2 | 2 | 2 | |
| 12. Controlled for confounding? | NA | NA | NA | 2 | 1 | NA | NA | 2 | 2 | |
| 13. Results reported in sufficient detail? | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | |
| 14. Conclusions supported by the results? | 2 | 2 | 1 | 1 | 1 | 2 | 1 | 2 | 2 | |
| Total points | 20 | 20 | 15 | 23 | 20 | 17 | 18 | 22 | 22 | |
| Max points possible | 20 | 20 | 20 | 28 | 22 | 20 | 20 | 22 | 28 | |
| Summary score, in percentage | 100% | 100% | 75% | 82% | 90% | 85% | 90% | 100% | 78.6% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Atif, M.; Saleem, Q.; Babar, Z.-U.-D.; Scahill, S. Association between the Vicious Cycle of Diabetes-Associated Complications and Glycemic Control among the Elderly: A Systematic Review. Medicina 2018, 54, 73. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina54050073
Atif M, Saleem Q, Babar Z-U-D, Scahill S. Association between the Vicious Cycle of Diabetes-Associated Complications and Glycemic Control among the Elderly: A Systematic Review. Medicina. 2018; 54(5):73. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina54050073
Chicago/Turabian StyleAtif, Muhammad, Quratulain Saleem, Zaheer-Ud-Din Babar, and Shane Scahill. 2018. "Association between the Vicious Cycle of Diabetes-Associated Complications and Glycemic Control among the Elderly: A Systematic Review" Medicina 54, no. 5: 73. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina54050073