Serum and Salivary IgA, IgG, and IgM Levels in Oral Lichen Planus: A Systematic Review and Meta-Analysis of Case-Control Studies

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
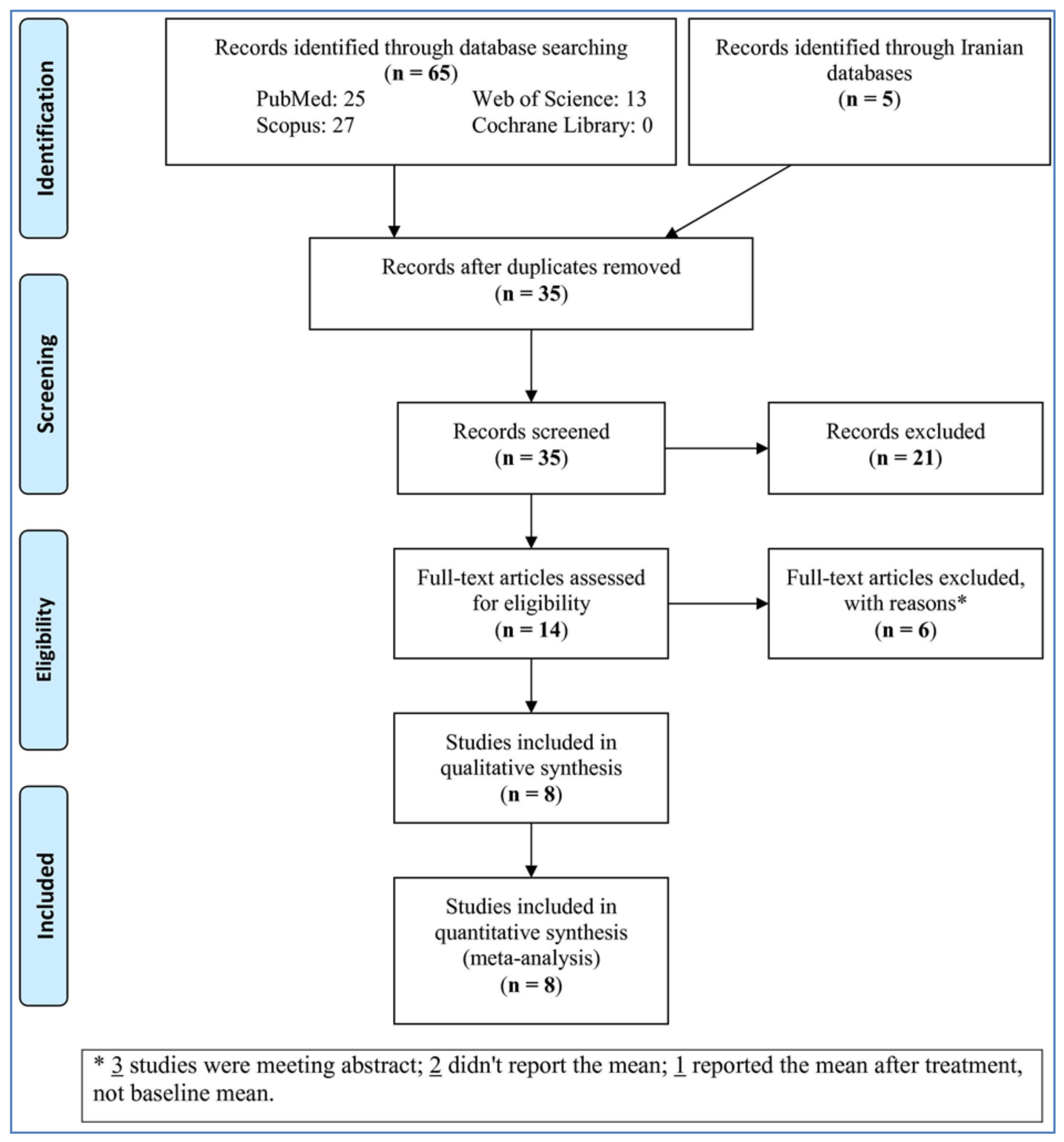
3. Search Strategies
4. Study Selection
5. Data Extraction
6. Quality Evaluation
7. Statistical Analyses
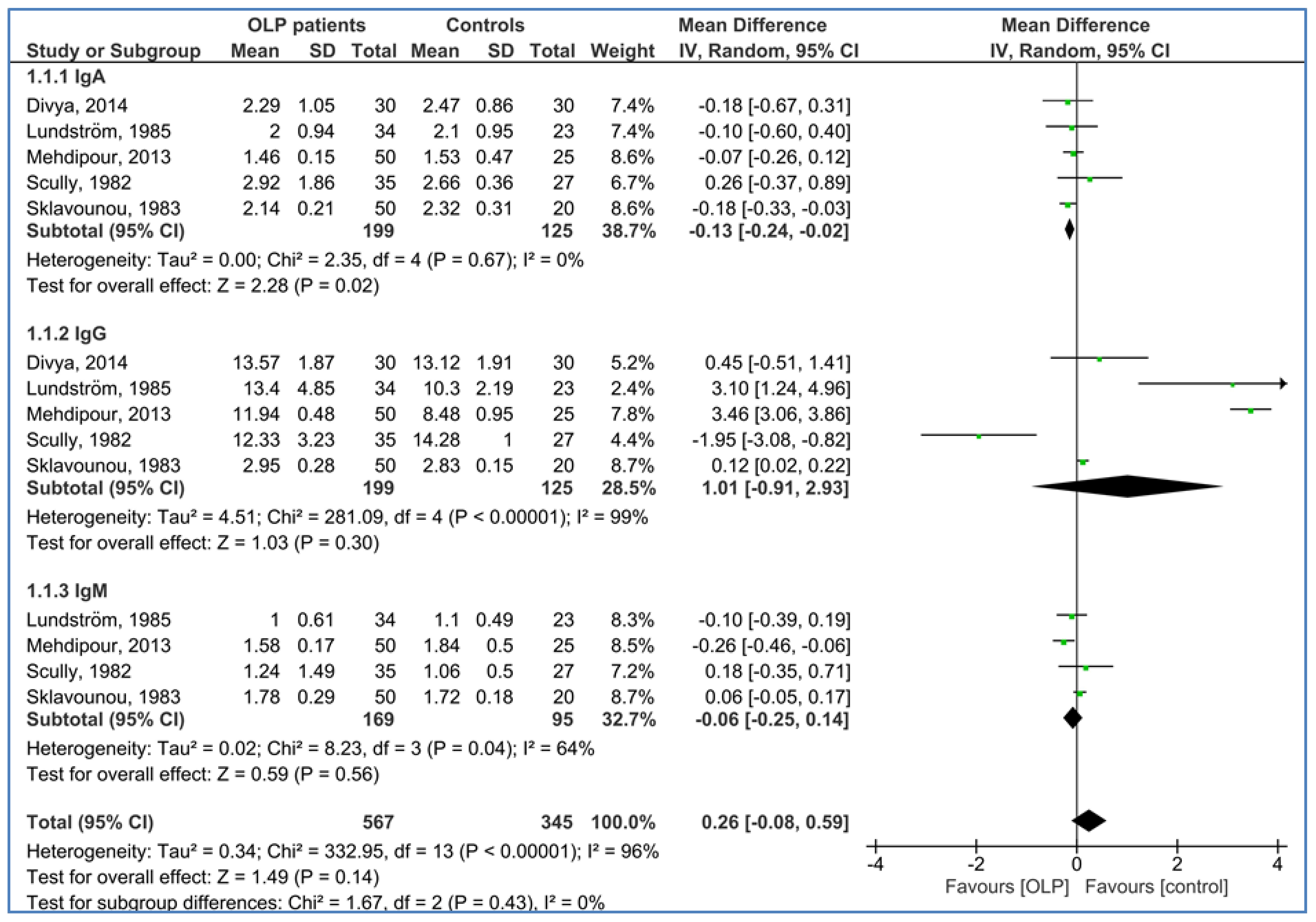
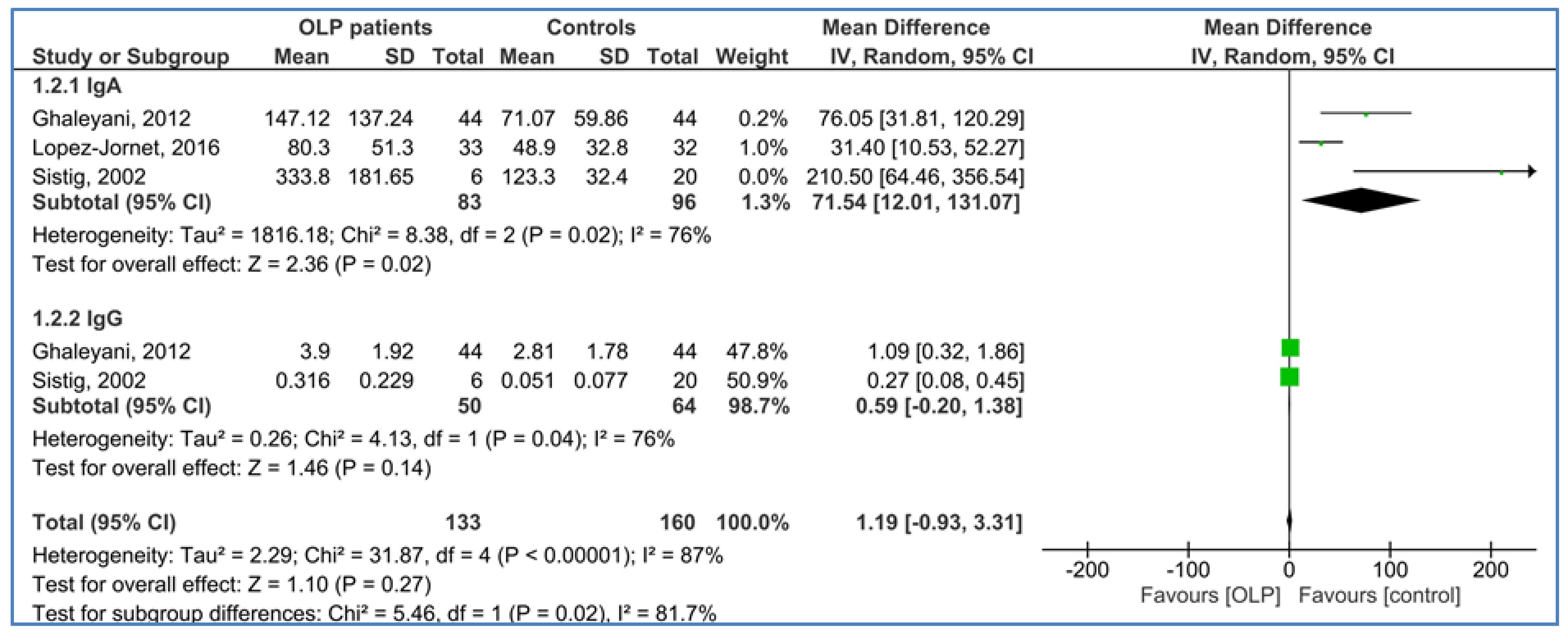
8. Results
9. Quality Assessment
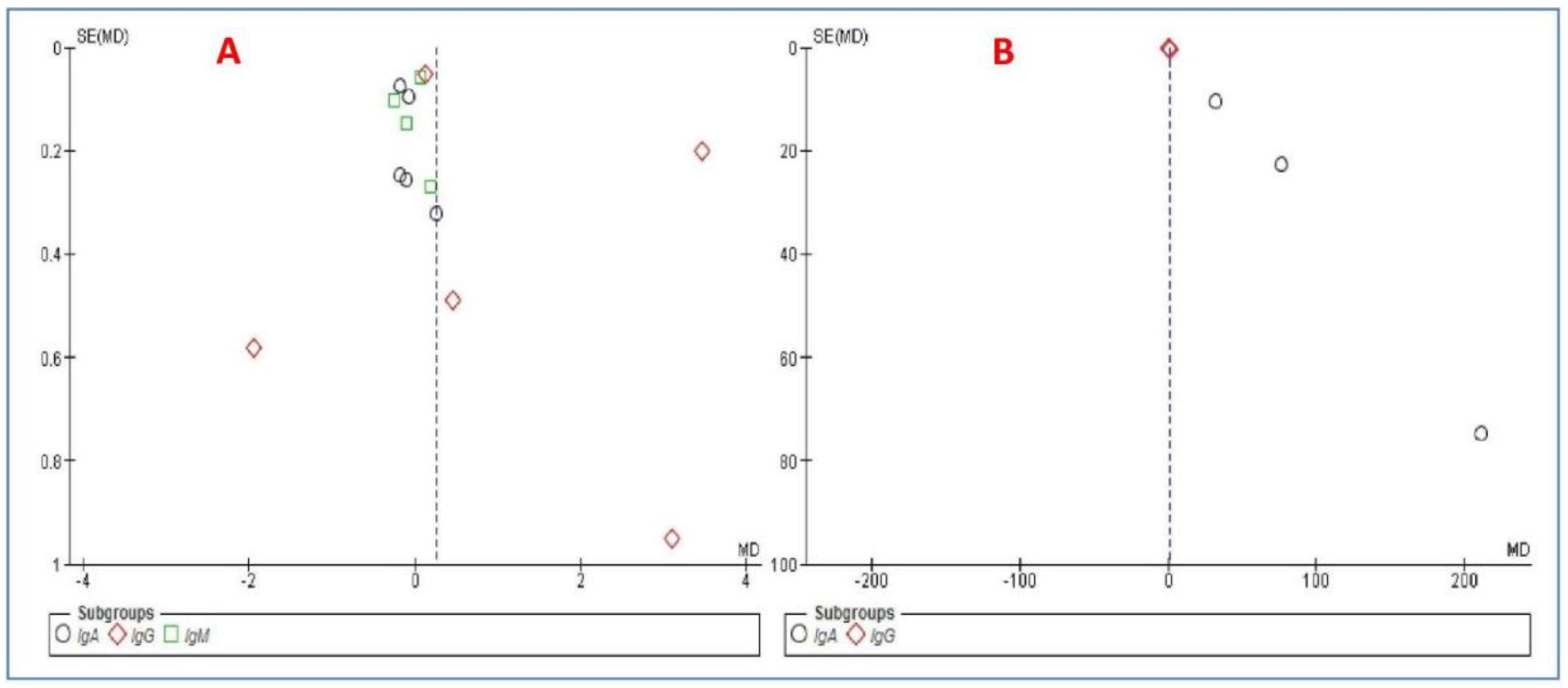
10. Publication Bias
11. Discussion
12. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mozaffari, H.R.; Sharifi, R.; Sadeghi, M. Prevalence of Oral Lichen Planus in Diabetes Mellitus: A Meta-Analysis Study. Acta. Inform. Med. 2016, 24, 390–393. [Google Scholar] [CrossRef] [PubMed]
- Carrozzo, M.; Thorpe, R. Oral lichen planus: A review. Minerva Stomatol. 2009, 58, 519–537. [Google Scholar]
- Lucchese, A.; Dolci, A.; Minervini, G.; Salerno, C.; Di Stasio, D.; Minervini, G.; Laino, L.; Silvestre, F.; Serpico, R. Vulvovaginal gingival lichen planus: Report of two cases and review of the literature. Oral Implantol. 2016, 9, 54–60. [Google Scholar]
- Van der Waal, I. Potentially malignant disorders of the oral and oropharyngeal mucosa; terminology, classification and present concepts of management. Oral Oncol. 2009, 45, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Kilian, M.; Ellegard, B.; Mestecky, J. Distribution of immunoglobulin isotypes including IgA subclasses in adult, juvenile and rapidly progressive periodontitis. J. Clin. Periodontol. 1989, 16, 179–184. [Google Scholar] [CrossRef]
- Macpherson, A.J.; McCoy, K.D.; Johansen, F.E.; Brandtzaeg, P. The immune geography of IgA induction and function. Mucosal Immunol. 2008, 1, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Mantis, N.J.; Rol, N.; Corthesy, B. Secretory IgA’s complex roles in immunity and mucosal homeostasis in the gut. Mucosal Immunol. 2011, 4, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Lux, A.; Aschermann, S.; Biburger, M.; Nimmerjahn, F. The pro and anti-inflammatory activities of immunoglobulin G. Ann. Rheum. Dis. 2010, 69, i92–i96. [Google Scholar] [CrossRef] [PubMed]
- Larsen, K.R.; Johansen, J.D.; Reibel, J.; Zachariae, C.; Rosing, K.; Pedersen, A.M.L. Oral symptoms and salivary findings in oral lichen planus, oral lichenoid lesions and stomatitis. BMC Oral Health 2017, 17, 103. [Google Scholar] [CrossRef] [Green Version]
- Lopez-Jornet, P.; Cayuela, C.A.; Tvarijonaviciute, A.; Parra-Perez, F.; Escribano, D.; Ceron, J. Oral lichen planus: Salival biomarkers cortisol, immunoglobulin A, adiponectin. J. Oral Pathol. Med. 2016, 45, 211–217. [Google Scholar] [CrossRef]
- Shi, H.; Guo, X.; Zhang, Q.; Wu, H.; Du, H.; Liu, L.; Wang, C.; Xia, Y.; Liu, X.; Li, C.; et al. Serum Immunoglobulin M Concentration Varies with Triglyceride Levels in an Adult Population: Tianjin Chronic Low-Grade Systemic Inflammation and Health (TCLSIHealth) Cohort Study. PLoS ONE 2015, 10, e0124255. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Robertson, J.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-Randomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2011; Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 12 January 2016).
- Ghaleyani, P.; Sardari, F.; Akbari, M. Salivary IgA and IgG in oral lichen planus and oral lichenoid reactions diseases. Adv. Biomed. Res. 2012, 1, 73. [Google Scholar] [PubMed]
- Mehdipour, M.; Eslami, H.; Taghavi Zenooz, A.; Babaloo, Z. Comparative evaluation of IgG, IgM and IgA serum levels in patients with lichen planus referring to Tabriz Faculty of Dentistry. J. Isfahan Dent. Sch. 2013, 9, 232–241. [Google Scholar]
- Scully, C. Serum IgG, IgA, IgM, IgD and IgE in lichen planus: No evidence for a humoral immunodeficiency. Clin. Exp. Dermatol. 1982, 7, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Sklavounou, A.D.; Laskaris, G.; Angelopoulos, A.P. Serum immunoglobulins and complement (C’3) in oral lichen planus. Oral Surg. Oral Med. Oral Pathol. 1983, 55, 47–51. [Google Scholar] [CrossRef]
- Sistig, S.; Vucićević-Boras, V.; Lukac, J.; Kusić, Z. Salivary IgA and IgG subclasses in oral mucosal diseases. Oral Dis. 2002, 8, 282–286. [Google Scholar] [CrossRef]
- Lundström, I.M. Serum immunoglobulins and autoantibodies in patients with oral lichen planus. Int. J. Oral Surg. 1985, 14, 259–268. [Google Scholar] [CrossRef]
- Divya, V.C.; Sathasivasubramanian, S. Estimation of serum and salivary immunoglobulin G and immunoglobulin A in oral pre-cancer: A study in oral submucous fibrosis and oral lichen planus. J. Nat. Sci. Biol. Med. 2014, 5, 90–94. [Google Scholar] [CrossRef]
- Mancini, G.; Carbonara, A.O.; Heremans, J.F. Immunochemical Quantitation of Antigens by Single Radial Immunodiffusion. Immunochemistry. 1965, 2, 235–254. [Google Scholar] [CrossRef]
- Mozaffari, H.R.; Sharifi, R.; Sadeghi, M. Interleukin-6 levels in the serum and saliva of patients with oral lichen planus compared with healthy controls: A meta-analysis study. Cent. Eur. J. Immunol. 2018, 43, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Mozaffari, H.R.; Ramezani, M.; Mahmoudiahmadabadi, M.; Omidpanah, N.; Sadeghi, M. Salivary and serum levels of tumor necrosis factor-alpha in oral lichen planus: A systematic review and meta-analysis study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 124, e183–e189. [Google Scholar] [CrossRef] [PubMed]
- Sato, K. Enzyme-linked immunosorbent assay of SIgA in whole saliva of healthy subjects and patients with oral diseases. Bull. Tokyo Med. Dent. Univ. 1991, 38, 9–18. [Google Scholar]
- Rutherfurd-Markwich, K.; Starck, C.; Dolson, D.K.; Ali, A. Salivary diagnostic markers in males and females during rest and exercise. J. Int. Soc. Sports Nutr. 2017, 14, 27. [Google Scholar] [CrossRef] [PubMed]
- Braathen, G.; Ingildsen, V.; Twetman, S.; Ericson, D.; Jørgensen, M.R. Presence of Lactobacillus reuteri in saliva coincide with higher salivary IgA in young adults after intake of probiotic lozenges. Benef. Microbes. 2017, 8, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Galvão-Moreira, L.V.; de Andrade, C.M.; de Oliveira, J.F.F.; Bomfim, M.R.Q.; Figueiredo, P.M.S.; Branco-de-Almeida, L.S. Sex differences in salivary parameters of caries susceptibility in healthy individuals. Oral Health Prev. Dent. 2018, 16, 71–77. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author (year) | Country | Number of Patients/Mean Age (year)/Male% | Number of Controls/Mean Age (year)/Male% | IgA | IgG | IgM | Method |
|---|---|---|---|---|---|---|---|
| Scully, 1982 [16] | Scotland | 35 42 years 48.6% | 27 40 years 48.1% | Serum | Serum | Serum | Modified single radial immunodiffusion [21] |
| Sklavounou, 1983 [17] | Greece | 50 53 years 40% | 20 46.4 years 50% | Serum | Serum | Serum | The single radial immunodiffusion [21] |
| Lundström, 1985 [19] | Sweden | 34 55.9 years 20.6% | 23 56.4 years 26.1% | Serum | Serum | Serum | IgG (immunochemical turbidimetric) and IgA and IgM (electroimmuno Assay) |
| Sistig, 2002 [18] | Croatia | 65 4 years 33.3% | 20 37 years 50% | Saliva | Saliva | - | IgG (ELISA) and IgA (radial immunodiffusion) |
| Ghaleyani, 2012 [14] | Iran | 44 45.6 years 34.1% | 44 44.8 years 38.6% | Saliva | Saliva | - | IgA (Human IgA Saliva Diametra kit, the binding Site, Italy), and IgG (radial immunodiffusion) |
| Mehdipour, 2013 [15] | Iran | 50 40 years 48% | 25 37 years 48% | Serum | Serum | Serum | Autoanalyzer (Abbot- alcion, USA) and Pars Azmon kits |
| Divya, 2014 [20] | India | 30 matched matched | 30 matched matched | Serum | Serum | - | Dade Behring BN ProSpec Nephelometer (Sri Ramachandra University). |
| Lopez-Jornet, 2016 [10] | Spain | 33 57 years 21.2% | 32 53 years 25% | Saliva | - | - | ELISA kit (Bethyl, Montgomery, TX, USA) |
| First Author (Year) | Selection | Comparability * | Outcome | Total Score | Quality | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Case Definition Adequate | Representativeness of the Cases | Selection of Controls | Definition of Controls | Main Factor | Additional Factor | Ascertainment of Exposure | Same Method of Ascertainment for Cases and Controls | Non-Response Rate | |||
| Scully, 1982 [16] | * | * | - | * | * | * | * | * | - | 7 | Good |
| Sklavounou, 1983 [17] | * | * | - | * | * | - | * | * | - | 6 | Fair |
| Lundström, 1985 [19] | * | * | - | * | * | * | * | * | - | 7 | Good |
| Sistig, 2002 [18] | * | * | - | * | - | - | * | * | - | 5 | Fair |
| Ghaleyani, 2012 [14] | * | * | - | * | * | * | * | * | - | 7 | Good |
| Mehdipour, 2013 [15] | * | * | - | * | * | * | * | * | - | 7 | Good |
| Divya, 2014 [20] | * | * | * | * | * | * | * | * | - | 8 | Good |
| Lopez-Jornet, 2016 [10] | * | * | - | * | * | * | * | * | - | 7 | Good |
| Mean Score | 6.75 | ||||||||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mozaffari, H.R.; Zavattaro, E.; Abdolahnejad, A.; Lopez-Jornet, P.; Omidpanah, N.; Sharifi, R.; Sadeghi, M.; Shooriabi, M.; Safaei, M. Serum and Salivary IgA, IgG, and IgM Levels in Oral Lichen Planus: A Systematic Review and Meta-Analysis of Case-Control Studies. Medicina 2018, 54, 99. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina54060099
Mozaffari HR, Zavattaro E, Abdolahnejad A, Lopez-Jornet P, Omidpanah N, Sharifi R, Sadeghi M, Shooriabi M, Safaei M. Serum and Salivary IgA, IgG, and IgM Levels in Oral Lichen Planus: A Systematic Review and Meta-Analysis of Case-Control Studies. Medicina. 2018; 54(6):99. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina54060099
Chicago/Turabian StyleMozaffari, Hamid Reza, Elisa Zavattaro, Abas Abdolahnejad, Pia Lopez-Jornet, Neda Omidpanah, Roohollah Sharifi, Masoud Sadeghi, Mohammad Shooriabi, and Mohsen Safaei. 2018. "Serum and Salivary IgA, IgG, and IgM Levels in Oral Lichen Planus: A Systematic Review and Meta-Analysis of Case-Control Studies" Medicina 54, no. 6: 99. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina54060099