The Relationship between the Soluble Receptor for Advanced Glycation End Products and Oxidative Stress in Patients with Palmoplantar Warts


 , ,
, ,
Abstract
:1. Introduction
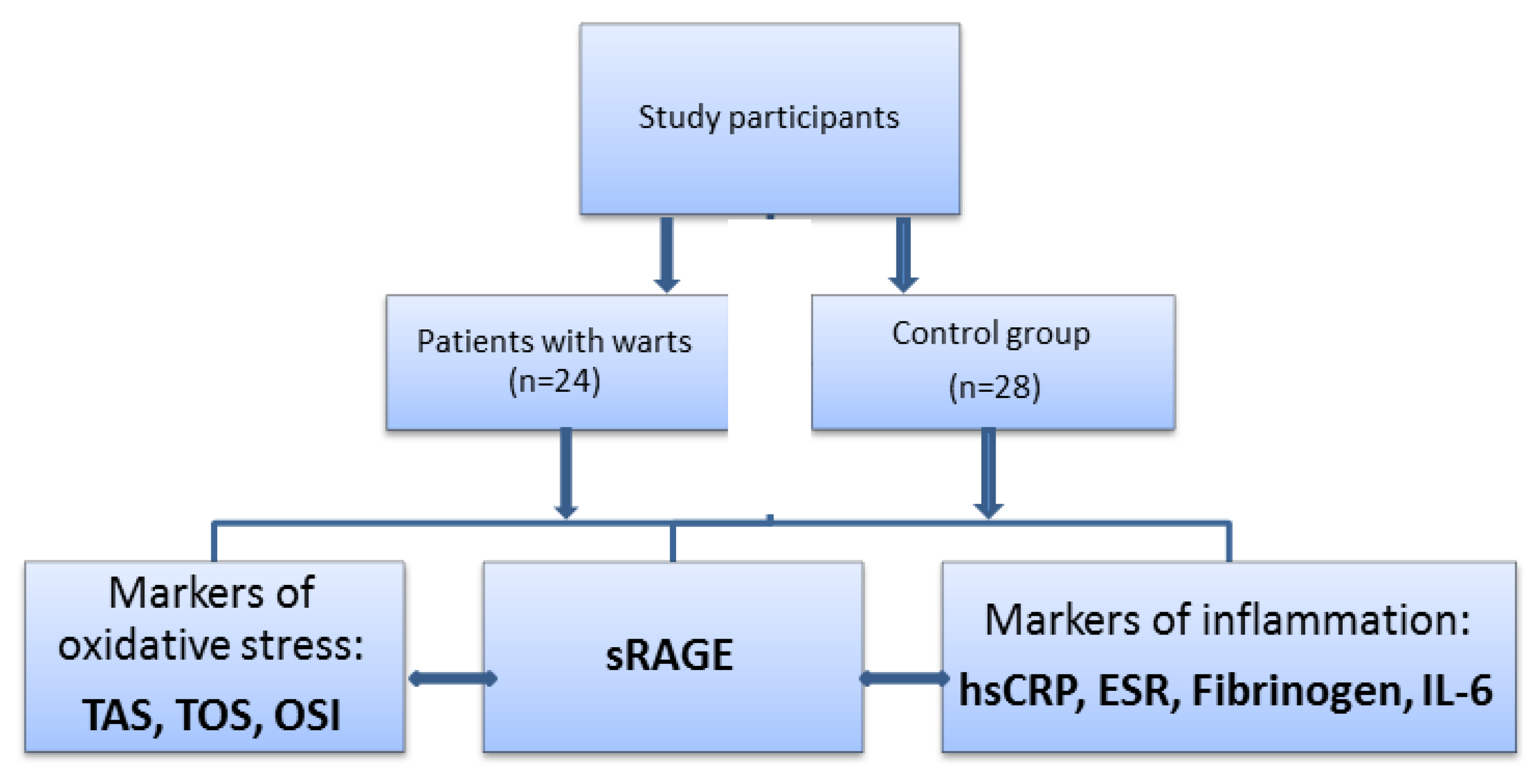
2. Materials and Methods
2.1. Study Participants
2.2. Laboratory Tests
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kirnbauer, R.; Androphy, E.J. Human papilloma virus infections. In Fitzpatrick’s Dermatology in General Medicine, 8th ed.; Goldsmith, L.A., Katz, S.I., Eds.; Mc. Graw-Hill Medical: New York, NY, USA, 2012; Volume 1, pp. 2421–2433. [Google Scholar]
- Doorbar, J.; Egawa, N.; Griffin, H.; Kranjec, C.; Murakami, I. Human papillomavirus molecular biology and disease association. Rev. Med. Virol. 2015, 25 (Suppl. S1), 2–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harden, M.E.; Munger, K. Human papillomavirus molecular biology. Mutat. Res. Rev. Mutat. Res. 2017, 772, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Bruggink, S.C.; de Koning, M.N.; Gussekloo, J.; Egberts, P.F.; Ter Schegget, J.; Feltkamp, M.C.; Bavinck, J.N.; Quint, W.G.; Assendelft, W.J.; Eekhof, J.A. Cutaneous wart-associated HPV types: Prevalence and relation with patient characteristics. J. Clin. Virol. 2012, 55, 250–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cubie, H.A. Diseases associated with human papillomavirus infection. Virology 2013, 445, 21–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witchey, D.J.; Witchey, N.B.; Roth-Kauffman, M.M.; Kauffman, M.K. Plantar warts: Epidemiology, pathophysiology, and clinical management. J. Am. Osteopath. Assoc. 2018, 118, 92–105. [Google Scholar] [CrossRef] [PubMed]
- Olia, J.B.H.; Ansari, M.H.K.; Yaghmaei, P.; Ayatollahi, H.; Khalkhali, H.R. Evaluation of oxidative stress marker in patients with papilloma virus infection. Ann. TMPH 2017, 10, 1518–1523. [Google Scholar]
- Nicolae, I.; Tampa, M.; Mitran, C.; Ene, C.D.; Mitran, M.; Matei, C.; Musetescu, A.; Pituru, S.; Pop, C.S.; Georgescu, S.R. Gamma-Glutamyl Transpeptidase Alteration As A Biomarker Of Oxidative Stress in Patients with Human Papillomavirus Lesions Following Topical Treatment with Sinecatechins. Farmacia 2017, 65, 617–623. [Google Scholar]
- Georgescu, S.R.; Mitran, C.I.; Mitran, M.I.; Caruntu, C.; Sarbu, M.I.; Matei, C.; Nicolae, I.; Tocut, S.M.; Popa, M.I.; Tampa, M. New Insights in the Pathogenesis of HPV Infection and the Associated Carcinogenic Processes: The Role of Chronic Inflammation and Oxidative Stress. J. Immunol. Res. 2018, 2018, 5315816. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, J.C.; Calonje, E. Cutaneous manifestations of human papillomaviruses: A review. Acta Dermatovenerol. Alp. Pannonica Adriat. 2011, 20, 145–154. [Google Scholar]
- Chow, L.T.; Broker, T.R. Human papillomavirus infections: Warts or cancer? Cold Spring Harb. Perspect. Biol. 2013, 5, a012997. [Google Scholar] [CrossRef]
- Choi, Y.J.; Park, J.S. Clinical significance of human papillomavirus genotyping. J. Gynecol. Oncol. 2016, 27, e21. [Google Scholar] [CrossRef] [PubMed]
- Moerman-Herzog, A.; Nakagawa, M. Early defensive mechanisms against human papillomavirus infection. Clin. Vaccine Immunol. 2015, 22, 850–857. [Google Scholar] [CrossRef] [PubMed]
- Santilli, F.; Vazzana, N.; Bucciarelli, L.G.; Davì, G. Soluble forms of RAGE in human diseases: Clinical and therapeutical implications. Curr. Med. Chem. 2009, 16, 940–952. [Google Scholar] [CrossRef] [PubMed]
- Tang, D.; Kang, R.; Coyne, C.B.; Zeh, H.J.; Lotze, M.T. PAMPs and DAMPs: Signal 0s that spur autophagy and immunity. Immunol. Rev. 2012, 249, 158–175. [Google Scholar] [CrossRef]
- Abeck, D.; Fölster-Holst, R. Quadrivalent human papillomavirus vaccination: A promising treatment for recalcitrant cutaneous warts in children. Acta Derm. Venereol. 2015, 95, 1017–1019. [Google Scholar] [CrossRef]
- Iwamura, M.; Yamamoto, Y.; Kitayama, Y.; Higuchi, K.; Fujimura, T.; Hase, T.; Yamamoto, H. Epidermal expression of receptor for advanced glycation end products (RAGE) is related to inflammation and apoptosis in human skin. Exp. Dermatol. 2016, 25, 235–237. [Google Scholar] [CrossRef]
- Papagrigoraki, A.; Maurelli, M.; Del Giglio, M.; Gisondi, P.; Girolomoni, G. Advanced Glycation End Products in the Pathogenesis of Psoriasis. Int. J. Mol. Sci. 2017, 18, 2471. [Google Scholar] [CrossRef]
- Pranal, T.; Pereira, B.; Berthelin, P.; Roszyk, L.; Godet, T.; Chabanne, R.; Eisenmann, N.; Lautrette, A.; Belville, C.; Blondonnet, R. Clinical and Biological Predictors of Plasma Levels of Soluble RAGE in Critically Ill Patients: Secondary Analysis of a Prospective Multicenter Observational Study. Dis. Markers 2018, 2018, 7849675. [Google Scholar] [CrossRef]
- Georgescu, S.R.; Ene, C.D.; Tampa, M.; Matei, C.; Benea, V.; Nicolae, I. Oxidative stress-related markers and alopecia areata through latex turbidimetric immunoassay method. Mater. Plast. 2016, 53, 522–526. [Google Scholar]
- Bongarzone, S.; Savickas, V.; Luzi, F.; Gee, A.D. Targeting the receptor for advanced glycation endproducts (RAGE): A medicinal chemistry perspective. J. Med. Chem. 2017, 60, 7213–7232. [Google Scholar] [CrossRef]
- Khan, M.I.; Su, Y.K.; Zou, J.; Yang, L.W.; Chou, R.H.; Yu, C. S100B as an antagonist to block the interaction between S100A1 and the RAGE V domain. PLoS ONE 2018, 13, e0190545. [Google Scholar] [CrossRef] [PubMed]
- Fishman, S.L.; Sonmez, H.; Basman, C.; Singh, V.; Poretsky, L. The role of advanced glycation end-products in the development of coronary artery disease in patients with and without diabetes mellitus: A review. Mol. Med. 2018, 24, 59. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.M.; Yan, S.D.; Yan, S.F.; Stern, D.M. The biology of the receptor for advanced glycation end products and its ligands. Biochim. Biophys. Acta 2000, 1498, 99–111. [Google Scholar] [CrossRef] [Green Version]
- van Zoelen, M.A.; Achouiti, A.; van der Poll, T. The role of receptor for advanced glycation endproducts (RAGE) in infection. Crit. Care 2011, 15, 208. [Google Scholar] [CrossRef]
- Bierhaus, A.; Humpert, P.M.; Morcos, M.; Wendt, T.; Chavakis, T.; Arnold, B.; Stern, D.M.; Nawroth, P.P. Understanding RAGE, the receptor for advanced glycation end products. J. Mol. Med. 2005, 83, 876–886. [Google Scholar] [CrossRef]
- Jensen, L.J.; Flyvbjerg, A.; Bjerre, M. Soluble receptor for advanced glycation end product: A biomarker for acute coronary syndrome. BioMed Res. Int. 2015, 2015, 815942. [Google Scholar] [CrossRef]
- Meerwaldt, R.; Links, T.; Zeebregts, C.; Tio, R.; Hillebrands, J.L.; Smit, A. The clinical relevance of assessing advanced glycation endproducts accumulation in diabetes. Cardiovasc. Diabetol. 2008, 7, 29. [Google Scholar] [CrossRef]
- Manigrasso, M.B.; Pan, J.; Rai, V.; Zhang, J.; Reverdatto, S.; Quadri, N.; DeVita, R.J.; Ramasamy, R.; Shekhtman, A.; Schmidt, A.M. Small molecule inhibition of ligand-stimulated RAGE-DIAPH1 signal transduction. Sci. Rep. 2016, 6, 22450. [Google Scholar] [CrossRef]
- Maruthur, N.M.; Li, M.; Halushka, M.K.; Astor, B.C.; Pankow, J.S.; Boerwinkle, E.; Coresh, J.; Selvin, E.; Kao, W.H. Genetics of plasma soluble receptor for advanced glycation end-products and cardiovascular outcomes in a community-based population: Results from the Atherosclerosis Risk in Communities Study. PLoS ONE 2015, 10, e0128452. [Google Scholar] [CrossRef]
- Vazzana, N.; Santilli, F.; Cuccurullo, C.; Davì, G. Soluble forms of RAGE in internal medicine. Intern. Emerg. Med. 2009, 4, 389–401. [Google Scholar] [CrossRef]
- Ardans, J.A.; Eonou, A.P.; Martins, J.M.; Zhou, M.; Wahl, L.M. Oxidized low-density and high-density lipoproteins regulate the production of matrix metalloproteinase-1 and -9 by activated monocytes. J. Leukoc. Biol. 2002, 71, 1012–1018. [Google Scholar] [PubMed]
- Yan, S.F.; Ramasamy, R.; Schmidt, A.M. Soluble RAGE: Therapy and biomarker in unraveling the RAGE axis in chronic disease and aging. Biochem. Pharmacol. 2010, 79, 1379–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massaccesi, L.; Bonomelli, B.; Marazzi, M.G.; Drago, L.; Romanelli, M.M.C.; Erba, D.; Papini, N.; Barassi, A.; Goi, G.; Galliera, E. Plasmatic Soluble Receptor for Advanced Glycation End Products as a New Oxidative Stress Biomarker in Patients with Prosthetic-Joint-Associated Infections? Dis. Markers 2017, 2017, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsumoto, H.; Matsumoto, N.; Ogura, H.; Shimazaki, J.; Yamakawa, K.; Yamamoto, K.; Shimazu, T. The clinical significance of circulating soluble RAGE in patients with severe sepsis. J. Trauma Acute Care Surg. 2015, 78, 1086–1093. [Google Scholar] [CrossRef] [PubMed]
- Reis, J.S.; Veloso, C.A.; Volpe, C.M.; Fernandes, J.S.; Borges, E.A.; Isoni, C.A.; Dos Anjos, P.M.; Nogueira-Machado, J.A. Soluble RAGE and malondialdehyde in type 1 diabetes patients without chronic complications during the course of the disease. Diabete Vasc. Dis. Res. 2012, 9, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Gkogkolou, P.; Böhm, M. Advanced glycation end products: Key players in skin aging? Dermatoendocrinology 2012, 4, 259–270. [Google Scholar] [CrossRef]
- Kasperska-Zajac, A.; Damasiewicz-Bodzek, A.; Tyrpień-Golder, K.; Zamlyński, J.; Grzanka, A. Circulating soluble receptor for advanced glycation end products is decreased and inversely associated with acute phase response in chronic spontaneous urticaria. Inflamm. Res. 2016, 65, 343–346. [Google Scholar] [CrossRef]
- Giuliano, A.R.; Siegel, E.M.; Roe, D.J.; Ferreira, S.; Baggio, M.L.; Galan, L.; Duarte-Franco, E.; Villa, L.L.; Rohan, T.E.; Marshall, J.R.; et al. Dietary intake and risk of persistent human papillomavirus (HPV) infection: The Ludwig-McGill HPV Natural History Study. J. Infect. Dis. 2003, 188, 1508–1516. [Google Scholar] [CrossRef]
- Briganti, S.; Picardo, M. Antioxidant activity, lipid peroxidation and skin diseases. What’s new. J. Eur. Acad. Dermatol. Venereol. 2003, 17, 663–669. [Google Scholar] [CrossRef]
- Erturan, I.; Kumbul Doğuç, D.; Korkmaz, S.; Büyükbayram, H.İ.; Yıldırım, M.; Kocabey Uzun, S. Evaluation of oxidative stress in patients with recalcitrant warts. J. Eur. Acad. Dermatol. Venereol. 2019, 33, jdv.15746. [Google Scholar] [CrossRef]
- Tampa, M.; Nicolae, I.L.; Ene, C.D.; Sarbu, I.; Matei, C.L.; Georgescu, S.R. Vitamin C and thiobarbituric acid reactive substances (TBARS) in psoriasis vulgaris related to psoriasis area severity index (PASI). Rev. Chim. 2017, 68, 43–47. [Google Scholar]
- Hudson, B.I.; Moon, Y.P.; Kalea, A.Z.; Khatri, M.; Marquez, C.; Schmidt, A.M.; Paik, M.C.; Yoshita, M.; Sacco, R.L.; DeCarli, C.; et al. Association of serum soluble receptor for advanced glycation end-products with subclinical cerebrovascular disease: The Northern Manhattan Study (NOMAS). Atherosclerosis 2011, 216, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Mitran, M.I.; Mitran, C.I.; Sarbu, M.I.; Matei, C.; Nicolae, I.; Caruntu, A.; Tocut, S.M.; Popa, M.I.; Caruntu, C.; Georgescu, S.R. Mediators of Inflammation–A Potential Source of Biomarkers in Oral Squamous Cell Carcinoma. J. Immunol. Res. 2018, 2018, 1061780. [Google Scholar]
- McNair, E.D.; Wells, C.R.; Mabood Qureshi, A.; Basran, R.; Pearce, C.; Orvold, J.; Devilliers, J.; Prasad, K. Modulation of high sensitivity C-reactive protein by soluble receptor for advanced glycation end products. Mol. Cell. Biochem. 2010, 341, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Sasmaz, S.; Arican, O.; Kurutas, E.B. Oxidative stress in patients with nongenital warts. Mediat. Inflamm. 2005, 2005, 233–236. [Google Scholar] [CrossRef] [PubMed]
- Yonchuk, J.G.; Silverman, E.K.; Bowler, R.P.; Agustí, A.; Lomas, D.A.; Miller, B.E.; Tal-Singer, R.; Mayer, R.J. Circulating soluble receptor for advanced glycation end products (sRAGE) as a biomarker of emphysema and the RAGE axis in the lung. Am. J. Respir. Crit. Care Med. 2015, 192, 785–792. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | Patients with Warts n = 24 | Controls n = 28 | p Value |
|---|---|---|---|
| sRAGE (pg/mL) | 1036.50 ± 207.60 | 1215.32 ± 266.12 | <0.05 * |
| Markers of oxidative stress | |||
| TAS (µmol Trolox Eq/L). | 1.85 ± 0.12 | 2.03 ± 0.14 | <0.01 * |
| TOS (µmol H2O2 Eq/L) | 3.17 ± 0.27 | 2.93 ± 0.22 | <0.01 * |
| OSI (arbitrary units) | 1.72 ± 0.22 | 1.45 ± 0.17 | <0.01 * |
| Markers of inflammation | |||
| hs-CRP (mg/dL) | 0.19 ± 0.14 | 0.06 ± 0.02 | <0.01 * |
| ESR (mm/h) | 5.20 ± 3.30 | 3.80 ± 2.10 | >0.05 |
| Fibrinogen (mg/dL) | 183.5 ± 59.10 | 179.6 ± 64.70 | >0.05 |
| IL-6 (pg/mL) | 7.62 ± 2.60 | 7.08 ± 2.40 | >0.05 |
| Parameter | Patients with Warts | p Value | ||
|---|---|---|---|---|
| <5 (n = 11) | 5–10 (n = 8) | >10 (n = 5) | ||
| sRAGE (pg/mL) | 1029.45 ± 237.52 | 10,562.5 ± 204.47 | 1020.4 ± 179.90 | 0.9 |
| Markers of oxidative stress | ||||
| TAS (µmol Trolox Eq/L). | 1.83 ± 0.12 | 1.85 ± 0.11 | 1.89 ± 0.17 | 0.58 |
| TOS (µmol H2O2 Eq/L) | 3.23 ± 0.35 | 3.10 ± 0.21 | 3.17 ± 0.24 | 0.62 |
| OSI (arbitrary units) | 1.77 ± 0.23 | 1.68 ± 0.15 | 1.70 ± 0.30 | 0.52 |
| Markers of inflammation | ||||
| hs-CRP (mg/dL) | 0.19 ± 0.16 | 0.20 ± 0.16 | 0.19 ± 0.11 | 0.9 |
| ESR (mm/h) | 6.00 ± 3.58 | 4.50 ± 3.11 | 4.60 ± 3.13 | 0.8 |
| Fibrinogen (mg/dL) | 171.72 ± 53.20 | 191.37 ± 57.58 | 206.4 ± 78.00 | 0.6 |
| IL-6 (pg/mL) | 7.93 ± 2.72 | 7.49 ± 2.63 | 7.16 ± 2.93 | 0.9 |
| Parameter | Patients with Warts | p Value | ||
|---|---|---|---|---|
| <1 (n = 6) | 1–6 (n = 10) | >6 (n = 8) | ||
| sRAGE (pg/mL) | 1061.00 ± 278.63 | 1090.50 ± 207.13 | 950.62 ± 133.72 | 0.26 |
| Markers of oxidative stress | ||||
| TAS (µmol Trolox Eq/L). | 1.86 ± 0.12 | 1.88 ± 0.14 | 1.82 ± 0.12 | 0.49 |
| TOS (µmol H2O2 Eq/L) | 3.13 ± 0.20 | 3.16 ± 0.33 | 3.22 ± 0.30 | 0.91 |
| OSI (arbitrary units) | 1.69 ± 0.10 | 1.70 ± 0.27 | 1.78 ± 0.22 | 0.79 |
| Markers of inflammation | ||||
| hs-CRP (mg/dL) | 0.20 ± 0.13 | 0.21 ± 0.16 | 0.19 ± 0.16 | 0.82 |
| ESR (mm/h) | 7.17 ± 3.87 | 4.00 ± 2.45 | 5.25 ± 3.41 | 0.23 |
| Fibrinogen (mg/dL) | 182.33 ± 67.45 | 185.20 ± 55.23 | 188.25 ± 65.53 | 0.87 |
| IL-6 (pg/mL) | 6.92 ± 3.16 | 8.12 ± 2.24 | 7.53 ± 2.89 | 0.92 |
| Parameter | Rho | p Value |
|---|---|---|
| TAS | 0.43 | <0.05 * |
| TOS | −0.90 | <0.01 * |
| OSI | −0.86 | <0.01 * |
| hs-CRP | 0.11 | >0.05 |
| ESR | −0.10 | >0.05 |
| Fibrinogen | 0.04 | >0.05 |
| IL-6 | −0.14 | >0.05 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitran, C.I.; Nicolae, I.; Tampa, M.; Mitran, M.I.; Caruntu, C.; Sarbu, M.I.; Ene, C.D.; Matei, C.; Ionescu, A.C.; Georgescu, S.R.; et al. The Relationship between the Soluble Receptor for Advanced Glycation End Products and Oxidative Stress in Patients with Palmoplantar Warts. Medicina 2019, 55, 706. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55100706
Mitran CI, Nicolae I, Tampa M, Mitran MI, Caruntu C, Sarbu MI, Ene CD, Matei C, Ionescu AC, Georgescu SR, et al. The Relationship between the Soluble Receptor for Advanced Glycation End Products and Oxidative Stress in Patients with Palmoplantar Warts. Medicina. 2019; 55(10):706. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55100706
Chicago/Turabian StyleMitran, Cristina Iulia, Ilinca Nicolae, Mircea Tampa, Madalina Irina Mitran, Constantin Caruntu, Maria Isabela Sarbu, Corina Daniela Ene, Clara Matei, Antoniu Cringu Ionescu, Simona Roxana Georgescu, and et al. 2019. "The Relationship between the Soluble Receptor for Advanced Glycation End Products and Oxidative Stress in Patients with Palmoplantar Warts" Medicina 55, no. 10: 706. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55100706