Left Ventricular Morphology and Function as a Determinant of Pulmonary Hypertension in Patients with Severe Aortic Stenosis: Cardiovascular Magnetic Resonance Imaging Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Transthoracic Echocardiography
2.3. Cardiac Magnetic Resonance Imaging Measurements
2.4. Feature Tracking Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Conflicts of Interest
References
- Carnero-Alcazar, M.; Reguillo-Lacruz, F.; Answers, A.; Villagran-Medinilla, E.; Maroto-Castellanos, L.C.; Rodriguez-Hernandez, J. Short- and mid-term results for aortic valve replacement in octogenarians. Interact. Cardiovasc. Thorac. Surg. 2010, 10, 549–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucon, A.; Oger, E.; Bedossa, M.; Boulmier, D.; Verhoye, J.P.; Eltchaninoff, H.; Iung, B.; Leguerrier, A.; Laskar, M.; Leprince, P.; et al. Prognostic implications of pulmonary hypertension in patients with severe aortic stenosis undergoing transcatheter aortic valve implantation: Study from the France 2 registry. Circ. Cardiovasc. Interv. 2014, 7, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Alushi, B.; Beckhoff, F.; Leistner, D.; Franz, M.; Reinthaler, M.; Stahli, B.E.; Morguet, A.; Figulla, H.R.; Doenst, T.; Maisano, F.; et al. Pulmonary hypertension in patients with severe aortic stenosis: Prognostic impact after transcatheter aortic valve replacement: Pulmonary hypertension in patients undergoing tavr. JACC Cardiovasc. Imaging 2019, 12, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Magne, J.; Donal, E.; O’Connor, K.; Dulgheru, R.; Rosca, M.; Pierard, L.A. Determinants and prognostic significance of exercise pulmonary hypertension in asymptomatic severe aortic stenosis. Circulation 2012, 126, 851–859. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, N.; Varadarajan, P.; Pai, R.G. Echocardiographic predictors of pulmonary hypertension in patients with severe aortic stenosis. Eur. J. Echocardiogr. J. Work. Group Echocardiogr. Eur. Soc. Cardiol. 2008, 9, 31–33. [Google Scholar] [CrossRef] [PubMed]
- Calin, A.; Rosca, M.; Beladan, C.C.; Enache, R.; Mateescu, A.D.; Ginghina, C.; Popescu, B.A. The left ventricle in aortic stenosis-imaging assessment and clinical implications. Cardiovasc. Ultrasound 2015, 13, 22. [Google Scholar] [CrossRef] [PubMed]
- Geva, T. Is mri the preferred method for evaluating right ventricular size and function in patients with congenital heart disease? Mri is the preferred method for evaluating right ventricular size and function in patients with congenital heart disease. Circ. Cardiovasc. Imaging 2014, 7, 190–197. [Google Scholar] [CrossRef]
- Rahman, Z.U.; Sethi, P.; Murtaza, G.; Virk, H.U.H.; Rai, A.; Mahmod, M.; Schoondyke, J.; Albalbissi, K. Feature tracking cardiac magnetic resonance imaging: A review of a novel non-invasive cardiac imaging technique. World J. Cardiol. 2017, 9, 312–319. [Google Scholar] [CrossRef]
- Bing, R.; Cavalcante, J.L.; Everett, R.J.; Clavel, M.A.; Newby, D.E.; Dweck, M.R. Imaging and impact of myocardial fibrosis in aortic stenosis. JACC Cardiovasc. Imaging 2019, 12, 283–296. [Google Scholar] [CrossRef]
- De Siqueira, M.E.; Pozo, E.; Fernandes, V.R.; Sengupta, P.P.; Modesto, K.; Gupta, S.S.; Barbeito-Caamano, C.; Narula, J.; Fuster, V.; Caixeta, A.; et al. Characterization and clinical significance of right ventricular mechanics in pulmonary hypertension evaluated with cardiovascular magnetic resonance feature tracking. J. Cardiovasc. Magn. Reson. Off. J. Soc. Cardiovasc. Magn. Reson. 2016, 18, 39. [Google Scholar] [CrossRef]
- Van Wolferen, S.A.; Marcus, J.T.; Boonstra, A.; Marques, K.M.; Bronzwaer, J.G.; Spreeuwenberg, M.D.; Postmus, P.E.; Vonk-Noordegraaf, A. Prognostic value of right ventricular mass, volume, and function in idiopathic pulmonary arterial hypertension. Eur. Heart J. 2007, 28, 1250–1257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swift, A.J.; Rajaram, S.; Campbell, M.J.; Hurdman, J.; Thomas, S.; Capener, D.; Elliot, C.; Condliffe, R.; Wild, J.M.; Kiely, D.G. Prognostic value of cardiovascular magnetic resonance imaging measurements corrected for age and sex in idiopathic pulmonary arterial hypertension. Circ. Cardiovasc. Imaging 2014, 7, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American society of echocardiography and the European Association of cardiovascular imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef] [PubMed]
- Galie, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 esc/ers guidelines for the diagnosis and treatment of pulmonary hypertension: The joint task force for the diagnosis and treatment of pulmonary hypertension of the European society of cardiology (esc) and the European respiratory society (ers): Endorsed by: Association for European paediatric and congenital cardiology (aepc), international society for heart and lung transplantation (ishlt). Eur. Heart J. 2016, 37, 67–119. [Google Scholar] [PubMed]
- Dweck, M.R.; Joshi, S.; Murigu, T.; Gulati, A.; Alpendurada, F.; Jabbour, A.; Maceira, A.; Roussin, I.; Northridge, D.B.; Kilner, P.J.; et al. Left ventricular remodeling and hypertrophy in patients with aortic stenosis: Insights from cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. Off. J. Soc. Cardiovasc. Magn. Reson. 2012, 14, 50. [Google Scholar] [CrossRef] [PubMed]
- Ahn, H.S.; Chang, S.A.; Kim, H.K.; Kim, S.J.; Lee, S.P.; Park, S.J.; Kim, Y.J.; Cho, G.Y.; Sohn, D.W.; Oh, J.K. Determinants of pulmonary hypertension development in moderate or severe aortic stenosis. Int. J. Cardiovasc. Imaging 2014, 30, 1519–1528. [Google Scholar] [CrossRef] [PubMed]
- Faggiano, P.; Antonini-Canterin, F.; Ribichini, F.; D’Aloia, A.; Ferrero, V.; Cervesato, E.; Pavan, D.; Burelli, C.; Nicolosi, G. Pulmonary artery hypertension in adult patients with symptomatic valvular aortic stenosis. Am. J. Cardiol. 2000, 85, 204–208. [Google Scholar] [CrossRef]
- Lancellotti, P.; Donal, E.; Magne, J.; O’Connor, K.; Moonen, M.L.; Cosyns, B.; Pierard, L.A. Impact of global left ventricular afterload on left ventricular function in asymptomatic severe aortic stenosis: A two-dimensional speckle-tracking study. Eur. J. Echocardiogr. J. Work. Group Echocardiogr. Eur. Soc. Cardiol. 2010, 11, 537–543. [Google Scholar] [CrossRef]
- Cramariuc, D.; Gerdts, E.; Davidsen, E.S.; Segadal, L.; Matre, K. Myocardial deformation in aortic valve stenosis: Relation to left ventricular geometry. Heart 2010, 96, 106–112. [Google Scholar] [CrossRef]
- Carasso, S.; Cohen, O.; Mutlak, D.; Adler, Z.; Lessick, J.; Aronson, D.; Reisner, S.A.; Rakowski, H.; Bolotin, G.; Agmon, Y. Relation of myocardial mechanics in severe aortic stenosis to left ventricular ejection fraction and response to aortic valve replacement. Am. J. Cardiol. 2011, 107, 1052–1057. [Google Scholar] [CrossRef]
- Lee, H.F.; Hsu, L.A.; Chan, Y.H.; Wang, C.L.; Chang, C.J.; Kuo, C.T. Prognostic value of global left ventricular strain for conservatively treated patients with symptomatic aortic stenosis. J. Cardiol. 2013, 62, 301–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajesh, G.N.; Thottian, J.J.; Subramaniam, G.; Desabandhu, V.; Sajeev, C.G.; Krishnan, M.N. Prevalence and prognostic significance of left ventricular myocardial late gadolinium enhancement in severe aortic stenosis. Indian Heart J. 2017, 69, 742–750. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Zeng, J.; Liu, D.; Yang, Q. Prognostic value of late gadolinium enhancement on CMR in patients with severe aortic valve disease: A systematic review and meta-analysis. Clin. Radiol. 2018, 73, 983.e7–983.e14. [Google Scholar] [CrossRef] [PubMed]
- Milan, A.; Magnino, C.; Veglio, F. Echocardiographic indexes for the non-invasive evaluation of pulmonary hemodynamics. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2010, 23, 225–239. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Overall (n = 30) | sPAP ≥ 45 mm Hg (n = 7) | sPAP < 45 mm Hg (n = 23) | p-value |
|---|---|---|---|---|
| Age, years | 70 (64–75) | 73 (60–75) | 70 (65–76) | 0.883 |
| Sex, male/female, n (%) | 16 (53.3)/14 (46.7) | 4 (57.1)/3 (42.9) | 12 (52.2)/11(47.8) | 1.0 |
| Arterial hypertension, n (%) | 25 (83.3) | 6 (85.7) | 19 (82.3) | 1.0 |
| Diabetes mellitus, n (%) | 2 (6.7) | 0 | 2 (6.7) | 1.0 |
| NYHA functional class 2–3, n (%) | 26 (86.7) | 6 (85.7) | 20 (87.0) | 1.0 |
| Body mass index, kg/m2 | 28.5 (25.0–32.30) | 27.0 (22.0–32.0) | 29.0 (25.0–33.0) | 0.349 |
| Glomerulal filtration rate, mL/min/1.73 2 | 83.5 (65.0–101.0) | 74.0 (58.0–83.0) | 87.0 (65.0–106.0) | 0.077 |
| Aortic valve area, cm2 | 0.85 (0.64–0.96) | 0.87 (0.75–0.95) | 0.8 (0.63–1.0) | 0.571 |
| Mean aortic gradient (mm Hg) | 43 (40–46) | 42 (40–45) | 43 (40–46) | 0.708 |
| sPAP, mm Hg | 37.5 (35.5–43.8) | 57.0 (49.0–63.0) | 36.0 (33.0–41.0) | <0.001 |
| LV end-diastolic diameter index, mm/m2 | 25.5 (22.8–29.3) | 30.0 (29.0–32.0) | 24.0 (22.0–27.0) | 0.003 |
| LV EF (%) | 55.0 (50.0–55.0) | 50.0 (40.0–55.0) | 55.0 (50.0–55.0) | 0.809 |
| Parameter | sPAP ≥ 45 mm Hg (n = 7) | sPAP < 45 mm Hg (n = 23) | p-value |
|---|---|---|---|
| LV EDV, mL | 289.0 (245.0–337.0) | 179.4 (159.0–200.4) | <0.001 |
| LV EDVi, mL/m² | 140 (120.0–160.0) | 90.0 (82.5–103.0) | <0.001 |
| LV ESV, mL | 109 (94–111) | 59 (50–84) | <0.001 |
| LV ESVi, mL/m² | 55 (55–60) | 32 (27–36) | <0.001 |
| LV MM, g | 235.0 (180.0–263.0) | 197.0 (141.1–306.0) | 0.54 |
| LV MMi, g/m2 | 121 (108–148) | 103 (82–140) | 0.26 |
| LV EF, % | 51.5 (42.2–64.3) | 61.5 (47.0–68.3) | 0.23 |
| LV GLS, % | −14.0 (−14.9–(−8.9)) | −21.1 (−23.4–(−17.8)) | 0.004 |
| LV GCS, % | −16.4 (−15.4–(−10.9)) | −32.0 (−36.1–(−20.8)) | 0.004 |
| LV fibrosis, % | 7.8 (5.6–8.0) | 1.3 (1.2–1.48) | 0.005 |
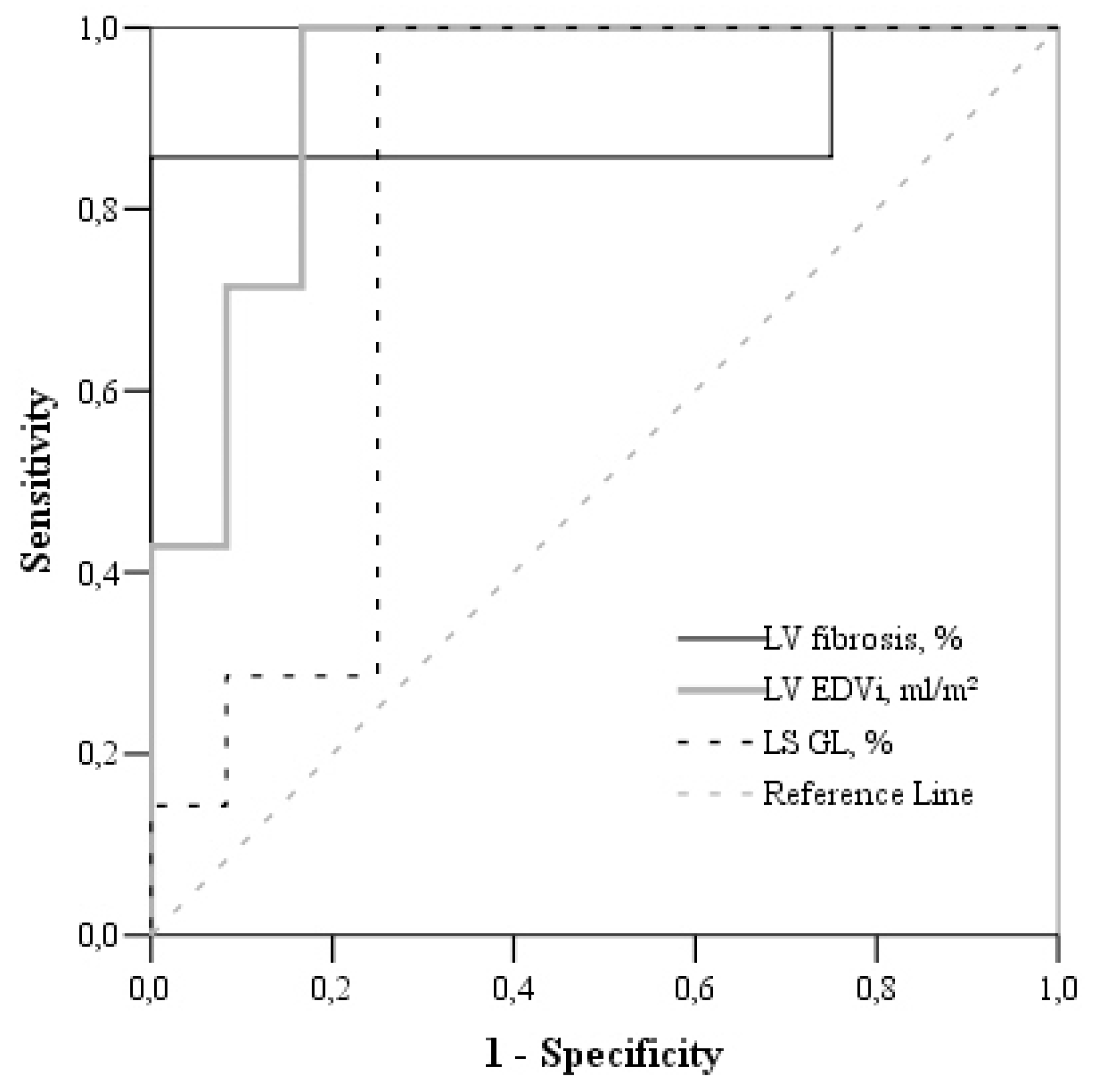
| Parameters/Threshold | Area under Curve (95% CI) | Sensitivity (%) | Specificity (%) |
|---|---|---|---|
| LV EDVi > 107.7 mL/m² | 95.7 (88.9–102) | 100 | 87 |
| LV LGS > −15.5% | 86.3 (73.0–99.7) | 100 | 82.6 |
| LV fibrosis > 5% | 89.3 (69.3–109.3) | 100 | 91.7 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gumauskiene, B.; Padervinskiene, L.; Vaskelyte, J.J.; Vaitiekiene, A.; Lapinskas, T.; Hoppenot, D.; Miliauskas, S.; Galnaitiene, G.; Simkus, P.; Ereminiene, E. Left Ventricular Morphology and Function as a Determinant of Pulmonary Hypertension in Patients with Severe Aortic Stenosis: Cardiovascular Magnetic Resonance Imaging Study. Medicina 2019, 55, 711. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55100711
Gumauskiene B, Padervinskiene L, Vaskelyte JJ, Vaitiekiene A, Lapinskas T, Hoppenot D, Miliauskas S, Galnaitiene G, Simkus P, Ereminiene E. Left Ventricular Morphology and Function as a Determinant of Pulmonary Hypertension in Patients with Severe Aortic Stenosis: Cardiovascular Magnetic Resonance Imaging Study. Medicina. 2019; 55(10):711. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55100711
Chicago/Turabian StyleGumauskiene, Birute, Lina Padervinskiene, Jolanta Justina Vaskelyte, Audrone Vaitiekiene, Tomas Lapinskas, Deimante Hoppenot, Skaidrius Miliauskas, Gryte Galnaitiene, Paulius Simkus, and Egle Ereminiene. 2019. "Left Ventricular Morphology and Function as a Determinant of Pulmonary Hypertension in Patients with Severe Aortic Stenosis: Cardiovascular Magnetic Resonance Imaging Study" Medicina 55, no. 10: 711. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55100711