Ventilator-Associated Pneumonia due to Drug-Resistant Acinetobacter baumannii: Risk Factors and Mortality Relation with Resistance Profiles, and Independent Predictors of In-Hospital Mortality

Abstract
:1. Introduction
2. Materials and Methods
Statistics
3. Results
3.1. Associations between the VAP Pathogen A.baumannii Drug Resistance Profile and Risk Factors for VAP
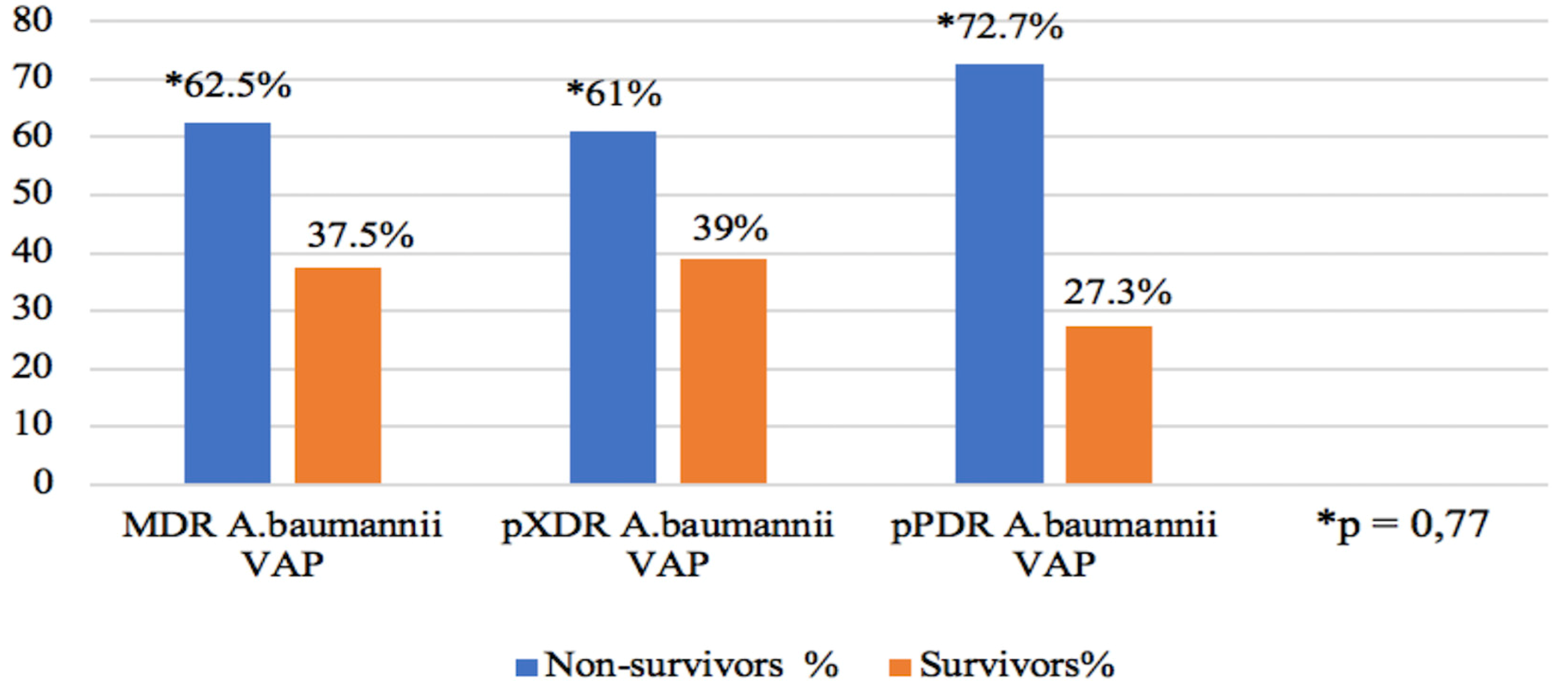
3.2. The Relationship between A.baumannii Drug Resistance Profile and Mortality
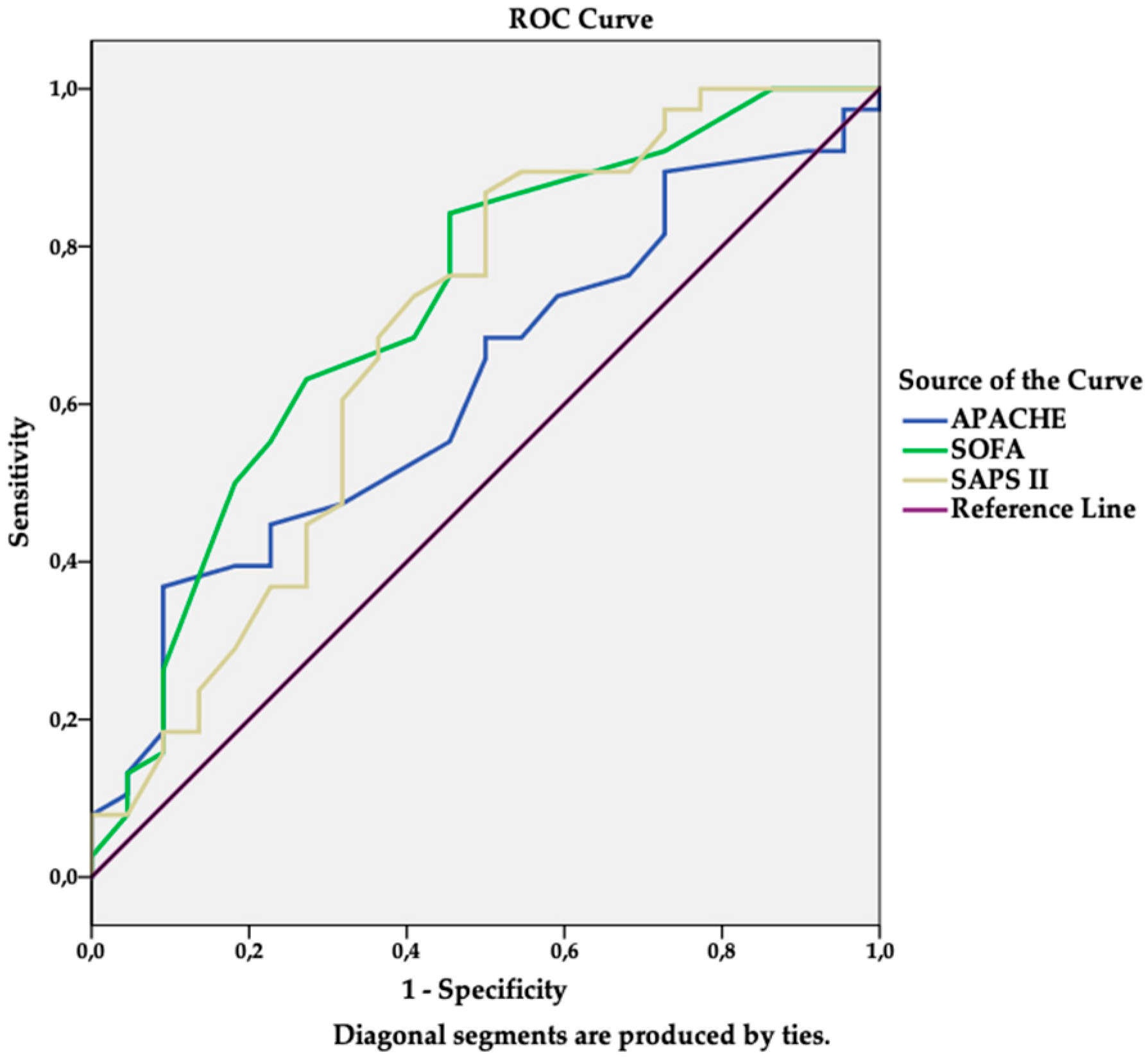
3.3. Predictors of In-Hospital Mortality
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am. J. Respir. Crit. Care Med. 2005, 171, 388–416. [Google Scholar] [CrossRef]
- Ozgur, E.; Horasan, E.; Karaca, K.; Ersoz, G.; Atis, S.N.; Kaya, A. Ventilator-associated pneumonia due to extensive drug-resistant Acinetobacter baumannii: Risk factors, clinical features, and outcomes. Am. J. Infect. Control 2014, 42, 206–208. [Google Scholar] [CrossRef]
- Li, Y.J.; Pan, C.Z.; Fang, C.Q.; Zhao, Z.X.; Chen, H.L.; Guo, P.H.; Zhao, Z.W. Pneumonia caused by extensive drug-resistant Acinetobacter baumannii among hospitalized patients: Genetic relationships, risk factors and mortality. BMC Infect. Dis. 2017, 17, 371. [Google Scholar] [CrossRef] [PubMed]
- Guillamet, C.V.; Kollef, M.H. Acinetobacter pneumonia: Improving outcomes with early identification and appropriate therapy. Clin. Infect. Dis. 2018, 67, 1455–1462. [Google Scholar] [CrossRef] [PubMed]
- Niederman, M.S.; Kollef, M.H. The road forward in the management of Acinetobacter infections in ICU. Intensive Care Med. 2015, 41, 2207–2209. [Google Scholar] [CrossRef] [PubMed]
- Koulenti, D.; Tsigou, E.; Rello, J. Nosocomial pneumonia in 27 ICUs in Europe: Perspectives from the EU-VAP/CAP study. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 1999–2006. [Google Scholar] [CrossRef] [PubMed]
- Hurley, J.C. Word-wide variation in incidence of Acinetobacter associated ventilator-associated pneumonia. BMC Infect. Dis. 2016, 16, 577. [Google Scholar] [CrossRef] [PubMed]
- Kanafani, A.Z.; Kanj, S.S. Acinetobacter Infection: Treatment and Prevention. 2018. Available online: https://www.uptodate.com/contents/acinetobacter-infection-treatment-and-prevention (accessed on 24 November 2018).
- Camp, C.; Tatum, O.L. A review of Acinetobacter baumannii as a highly successful pathogen in times of war. Lab. Med. 2010, 41, 649–657. [Google Scholar] [CrossRef]
- Rello, J.; Kalwaje Eshwara, K.; Lagunes, L.; Alves, J.; Wunderic, R.G.; Conway-Morris, A.; Rojas, J.N.; Alp, E.; Zhang, Z. A global priority list of the TOp TEn resistant Microorganisms (TOTEM) study at intensive care: A prioritization exercise based on multi-criteria decision analysis. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Montero, A.; Corbella, X.; Ariza, J. Clinical relevance of Acinetobacter baumannii ventilator-associated pneumonia. Crit. Care Med. 2003, 31, 2557–2558. [Google Scholar] [CrossRef]
- Garnacho-Montero, J.; Gutierrez-Pizarraya, A.; Diaz-Martin, A.; Cisneros-Herreros, J.M.; Cano, M.E.; Gato, E.; Ruiz de Alegría, C.; Fernández-Cuenca, F.; Vila, J.; Martínez-Martínez, L.; et al. Acinetobacter baumannii in critically ill patients: Molecular epidemiology, clinical features and predictors of mortality. Enferm. Infecc. Microbiol. Clin. 2016, 34, 551–558. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. European Antibiotic Awareness Day (EAAD) Summary of the Latest Data on Antibiotic Resistance in the European Union; EARS-Net Surveillance Data 2015; ECDC: Stockholm, Sweden, 2016. Available online: https://ecdc.europa.eu/sites/portal/files/documents/antibiotics-EARS-Net-summary-2016_0.pdf (accessed on 24 November 2018).
- Tacconelli, E.; Magrini, N. Global Priority List of Antibiotic-Resistant Bacteria to Guide Research, Discovery, and Development of New Antibiotics. Available online: http://www.who.int/medicines/publications/global-priority-list-antibiotic-resistant-bacteria/en/ (accessed on 24 November 2018).
- Surveillance of Healthcare-Associated Infections in Intensive Care Units. Annual Epidemiological Report for 2015 [Hospitalinių Infekcijų Epidemiologinės Priežiūros Padidintos Rizikos Skyriuose 2015 m. ataskaita]. Available online: http://www.hi.lt/news/1043/998/Hospitaliniu-infekciju-epidemiologines-prieziuros-padidintos-rizikos-skyriuose-2015-m-ataskaita.html (accessed on 24 November 2018).
- Surveillance of Healthcare-Associated Infections in Intensive Care Units. Annual epidemiological report for 2017 [Hospitalinių infekcijų epidemiologinės priežiūros padidintos rizikos skyriuose 2017 m. ataskaita]. Available online: http://www.hi.lt/uploads/pdf/hospitalines/duomenu ataskaitos/RITS 2017 ataskaita SF GALUTINIS (002).pdf (accessed on 10 December 2018).
- European Centre for Disease Prevention and Control. Surveillance of Antimicrobial Resistance in Europe 2017. Available online: https://ecdc.europa.eu/sites/portal/files/documents/AMR-surveillance-EARS-Net-2017.pdf (accessed on 10 December 2018).
- Garnacho-Montero, J.; Ortiz-Leyba, C.; Jimenez-Jimenez, F.J.; Barrero-Almodovar, A.E.; Garcia-Gamendia, J.L.; Bernabeu-Wittell, M.; Gallego-Lara, S.L.; Madrazo-Osuna, J. Treatment of multidrug-resistant Acinetobacter baumannii ventilator-associated pneumonia (VAP) with intravenous colistin: A comparission with imipenem-susceptible VAP. Clin. Infect. Dis. 2003, 36, 1111–1118. [Google Scholar] [CrossRef] [PubMed]
- Inchai, J.; Liwsrisakun, C.; Theerakittikul, T.; Chaiwarith, R.; Khositsakulchai, W.; Pothirat, C. Risk factors of multidrug-resistant, extensively drug-resistant and pandrug-resistant Acinetobacter baumannii ventilator-associated pneumonia in a Medical Intensive Care Unit of University Hospital in Thailand. J. Infect. Chemother. 2015, 21, 570–574. [Google Scholar] [CrossRef] [PubMed]
- Dellinger, R.P.; Levy, M.M.; Rhodes, A.; Annane, D.; Gerlach, H.; Opal, S.M.; Sevransky, J.E.; Sprung, C.L.; Douglas, I.S.; Jaeschke, R.; et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2012. Crit. Care Med. 2013, 41, 580–637. [Google Scholar] [PubMed]
- European Committee on Antimicrobial Susceptibility Testing (EUCAST). EUCAST Breakpoints Tables for Interpretation of MICs and Zone Diametres, Version 2.0. 2015. Available online: http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/Breakpoint_table_v_2.0_120221.pdf (accessed on 10 December 2018).
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug- resistant, extensively drug resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed]
- Inchai, J.; Pothirat, C.; Bumroongkit, C.; Limsukon, A.; Khositsakulchai, W.; Liwsrisakun, C. Prognostic factors associated with mortality of drug-resistant Acinetobacter baumannii ventilator-associated pneumonia. J. Intensive Care 2015, 3, 9. [Google Scholar] [CrossRef] [PubMed]
- Sengul, A.; Sengul, E.; Baris, S.A.; Hayirloglu, N. Factors associated with mortality in ventilator associated pneumonia of multidrug resistant acinetobacter baumannii. Eur. Respir. J. 2013, 42, P2747. [Google Scholar]
- Larsson, J.; Itenov, T.S.; Bestle, M.H. Risk prediction models for mortality in patients with ventilator-associated pneumonia: A systematic review and meta-analysis. J. Crit. Care 2017, 37, 112–118. [Google Scholar] [CrossRef]
- Karakuzu, Z.; Iscimen, R.; Akalin, H.; Girgin, N.K.; Kahveci, F.; Sinirtas, M. Prognostic risk factors in ventilator-associated pneumonia. Med. Sci. Monit. 2018, 24, 1321–1328. [Google Scholar] [CrossRef]
- Tsioutis, C.; Kristosakis, E.I.; Karageorgos, S.A.; Stratakou, S.; Psarologakis, C.; Kokkini, S.; Gikas, A. Clinical epidemiology, treatment and prognostic factors of extensively drug-resistant Acinetobacter baumannii ventilator-associated pneumonia in critically ill patients. Int. J. Antimicrob. Agents 2016, 48, 492–497. [Google Scholar] [CrossRef]
- Marik, P.E.; Corwin, H.L. Efficacy of red blood cell transfusion in the critically ill: A systematic review of the literature. Crit. Care Med. 2008, 36, 2667–2674. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Sakr, Y.; Sprung, C.; Harboe, S.; Damas, P. Sepsis occurrence in acutely ill patients (SOAP) investigators. Are blood transfusions associated with greater mortality rates? Results of the Sepsis Occurrence in Acutely Ill Patients study. Anesthesiology 2008, 108, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Jaschinski, U.; Wittebole, X.; Lefrant, J.L.; Jakob, S.M.; Almekhlafi, G.A.; Pellis, T.; Tripathy, S.; Rubatto Birri, P.N.; Sakr, Y.; et al. Worldwide audit of blood transfusion practise in critically ill patients. Crit. Care 2018, 22, 102. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | All Cases n = 60 | Drug Resistance Profiles of VAP Pathogen A. baumannii | p Value | ||
|---|---|---|---|---|---|
| MDR n = 8 | XDR n = 41 | pPDR n = 11 | |||
| Gender, n (%) | |||||
| Female | 29 (48.3) | 6 (75) | 18 (43.9) | 5 (45.5) | 0.201 |
| Male | 31 (51.7) | 2 (25) | 23 (56.1) | 6 (54.5) | |
| Age (years), mean (SD) | 63.95 (15) | 60 (18.4) | 65.37 (15.3) | 61.55 (11.1) | 0.555 |
| Reintubation, n (%) | 19 (31.7) | 3 (37.5) | 13 (31.7) | 3 (27.3) | 0.894 |
| Surgical intervention, n (%) | 23 (38.3) | 4 (50) | 16 (39) | 3 (27.3) | 0.593 |
| Tracheostomy prior VAP, n (%) | 8 (13.3) | 0 (0) | 5 (12.2) | 3 (27.3) | 0.209 |
| Severity score on ICU admission: | |||||
| APACHE II, median (IQR) | 19 (13–27.5) | 18 (13.3–31.5) | 18 (12-24) | 23 (18–30) | 0.189 |
| SAPS II, mean (SD) | 47.95 (13) | 42.6 (13.8) | 48.7(12.8) | 49 (13.5) | 0.048 |
| SOFA, mean (SD) | 11.5 (4.3) | 11.8 (4.3) | 11.5 (4.6) | 11.36 (3) | 0.981 |
| Admission type, n (%) | |||||
| Surgery | 17 (28.3) | 2 (25) | 10 (24.4) | 5 (45.5) | 0.186 |
| Medical | 29 (48.3) | 5 (62.5) | 18 (43.9) | 6 (54.5) | |
| Trauma | 14 (23.3) | 1 (12.5) | 13 (31.7) | 0 (0) | |
| Coma (GCS <9), n (%) | 8 (13.3) | 2 (25.0) | 4 (9.8) | 2 (18.2) | 0.445 |
| Chronic disease, n (%) | 43 (71.7) | 7 (87.5) | 29 (70.7) | 7 (63.6) | 0.508 |
| Sepsis status on ICU admission, n (%) | |||||
| Sepsis | 54 (90) | 8 (100) | 36 (87.8) | 10 (90.9) | 0.572 |
| Shock | 20 (33.3) | 2 (25) | 16 (39) | 2 (18.2) | 0.371 |
| RBC transfusion prior to VAP, n (%) | 36 (60) | 4 (50) | 24 (58.5) | 8 (72.7) | 0.573 |
| Antibiotic treatment prior to VAP (days), median (IQR) | 13 (7–18) | 10.5 (5.3–13.8) | 13 (7.5–20) | 14 (6–19) | 0.475 |
| Antibiotic treatment prior to VAP (class), n (%) | |||||
| Cephalosporin | 46 (76.7) | 5 (62.5) | 32 (78) | 9 (76.7) | 0.576 |
| Penicillin ± BLI | 34 (56.7) | 3 (37.5) | 23 (56.1) | 6 (54.5) | 0.626 |
| Quinolone | 6 (10) | 0 (0) | 5 (12.2) | 1 (9.1) | 0.572 |
| Aminoglycoside | 3 (5) | 1 (12.5) | 1 (2.4) | 1 (9.1) | 0.387 |
| Carbapenem | 18 (30) | 4 (50) | 12 (29.3) | 2 (18.2) | 0.036 |
| Other | 8 (13.3) | 1 (12.5) | 4 (9.8) | 3 (27.3) | 0.315 |
| LOS (days), median (IQR) | |||||
| Hospital prior to ICU | 1 (0–3.8) | 0 (0–0.8) | 1 (0–3.5) | 2 (0–10) | 0.036 |
| ICU prior to MV | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–1) | 0.406 |
| ICU prior to VAP | 9 (6–13) | 9.5 (5.3–13.5) | 9 (6–13) | 8 (5–16) | 0.974 |
| Hospital prior to MV | 0 (0–2.7) | 0 (0–0) | 0 (0–2) | 3 (0–6) | 0.013 |
| Hospital prior to VAP | 11.5 (6–16.5) | 10 (6–13.5) | 12 (6–16) | 14 (8–22) | 0.424 |
| MV prior to VAP (days), median (IQR) | 8.50 (5–14) | 10.5 (5–13.3) | 8 (5.5–14) | 7 (2–11) | 0.845 |
| Variable | Survivors (n = 22) | Non-Survivors (n = 38) | p Value |
|---|---|---|---|
| Gender, n (%) | |||
| Female | 6 (20.7) | 23 (79.3) | 0.017 |
| Male | 16 (51.6) | 15 (48.4) | |
| Age (years), mean (SD) | 60.77 (16) | 65.79 (14.3) | 0.214 |
| Severity score on ICU admission, mean (SD) | |||
| APACHE II | 17.64 (7.1) | 21.63 (9.1) | 0.082 |
| SOFA | 9.41 (4.3) | 12.71 (3.8) | 0.003 |
| SAPS II | 41.73 (15.2) | 51.55 (10.1) | 0.011 |
| Sepsis status on ICU admission, n (%) | |||
| Sepsis | 19 (35.2) | 35 (64.8) | 0.659 |
| Shock | 9 (45) | 11 (55) | 0.401 |
| Chronic diseases, n (%) | 12 (27.9) | 31 (72.1) | 0.038 |
| Coma GCS <9, n (%) | 4 (50) | 4 (50) | 0.449 |
| Admission type, n (%) | |||
| Surgery | 6 (35.3) | 11 (64.7) | 0.981 |
| Internal disease | 11 (37.9) | 18 (62.1) | |
| Trauma | 5 (35.7) | 9 (64.3) | |
| Reintubation, n (%) | 8 (42.1) | 11 (57.9) | 0.577 |
| Surgical intervention, n (%) | 6 (26.1) | 17 (73.9) | 0.271 |
| Tracheostomy prior to VAP, n (%) | 1 (12.5) | 7 (87.5) | 0.238 |
| RBC transfusion prior to VAP, n (%) | 9 (25) | 27 (75) | 0.03 |
| RBC (units), median (IQR) | 0 (0–2.3) | 2 (0–5) | 0.044 |
| LOS (days), median (IQR) | |||
| Hospital prior to ICU | 0.5 (0–3.5) | 1 (0–4) | 0.568 |
| ICU prior to MV | 0 (0–0.3) | 0 (0–0.25) | 0.876 |
| ICU prior to VAP | 8 (5.8–11) | 9.5 (5.8–15) | 0.442 |
| Hospital prior to MV | 0 (0–1.3) | 0.5 (0–4) | 0.341 |
| Hospital prior to VAP | 9.5 (6–14) | 13 (7.5–20) | 0.126 |
| MV prior to VAP (days), median (IQR) | 9 (5–11.5) | 8 (5–15.3) | 0.729 |
| Antibiotic treatment prior to VAP (days), median (IQR) | 10 (6–14.8) | 14 (7.8–20) | 0.164 |
| Independent Variable | Odds Ratio | 95% CI | p Value |
|---|---|---|---|
| Gender (female) | 5.26 | 1.21–22.83 | 0.027 |
| SOFA score on ICU admission | 1.28 | 1.06–1.53 | 0.008 |
| RBC transfusion | 5.97 | 1.41–25.27 | 0.015 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Čiginskienė, A.; Dambrauskienė, A.; Rello, J.; Adukauskienė, D. Ventilator-Associated Pneumonia due to Drug-Resistant Acinetobacter baumannii: Risk Factors and Mortality Relation with Resistance Profiles, and Independent Predictors of In-Hospital Mortality. Medicina 2019, 55, 49. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020049
Čiginskienė A, Dambrauskienė A, Rello J, Adukauskienė D. Ventilator-Associated Pneumonia due to Drug-Resistant Acinetobacter baumannii: Risk Factors and Mortality Relation with Resistance Profiles, and Independent Predictors of In-Hospital Mortality. Medicina. 2019; 55(2):49. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020049
Chicago/Turabian StyleČiginskienė, Aušra, Asta Dambrauskienė, Jordi Rello, and Dalia Adukauskienė. 2019. "Ventilator-Associated Pneumonia due to Drug-Resistant Acinetobacter baumannii: Risk Factors and Mortality Relation with Resistance Profiles, and Independent Predictors of In-Hospital Mortality" Medicina 55, no. 2: 49. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55020049