Impact of the Allergic Asthma on Foot Health-Related Quality of Life and Depression: A Novel Case-Control Research

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Methods
2.1. Design and Sample
2.2. Procedure
2.3. Ethics Considerations
2.4. Sample size Calculation
2.5. Statistical Analyses
3. Results
3.1. Descriptive Data
3.2. Outcome Measurements
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Busse, W.W.; Lemanske, R.F. Asthma. N. Eng. J. Med. 2001, 344, 350–362. [Google Scholar] [CrossRef] [PubMed]
- Global Asthma Network. The Global Asthma Report. Available online: http://www.globalasthmareport.org/Global%20Asthma%20Report%202018.pdf (accessed on 10 January 2019).
- Ciprandi, G.; Schiavetti, I.; Rindone, E.; Ricciardolo, F.L.M. The impact of anxiety and depression on outpatients with asthma. Ann. Allergy Asthma Immunol. 2015, 115, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.H.; Zhao, H.S.; Zhang, F.R.; Gao, Y.; Shen, P.; Chen, R.C.; Zhang, G.J. The Relationship between depression and asthma: A meta-analysis of prospective studies. PLoS ONE 2015, 10, e0132424. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Xu, J.; Yang, X. Asthma and risk of cardiovascular disease or all-cause mortality: A meta-analysis. Ann. Saudi Med. 2017, 37, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Ali, Z.; Ulrik, C.S. Obesity and asthma: A coincidence or a causal relationship? A systematic review. Respir. Med. 2013, 107, 1287–1300. [Google Scholar] [CrossRef] [Green Version]
- Lunardi, A.C.; Marques da Silva, C.C.B.; Rodrigues Mendes, F.A.; Marques, A.P.; Stelmach, R.; Fernandes Carvalho, C.R. Musculoskeletal dysfunction and pain in adults with asthma. J. Asthma 2011, 48, 105–110. [Google Scholar] [CrossRef] [PubMed]
- López-López, D.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Palomo-López, P.; Rodríguez-Sanz, D.; Brandariz-Pereira, J.M.; Calvo-Lobo, C. Evaluation of foot health related quality of life in individuals with foot problems by gender: A cross-sectional comparative analysis study. BMJ Open 2018, 8, e023980. [Google Scholar] [CrossRef] [PubMed]
- López-López, D.; Grela-Fariña, M.; Losa-Iglesias, M.; Calvo-Lobo, C.; Rodríguez-Sanz, D.; Palomo-López, P.; Becerro-de-Bengoa-Vallejo, R. Clinical aspects of foot health in individuals with alzheimer’s disease. Int. J. Environ. Res. Public Health 2018, 15, 286. [Google Scholar] [CrossRef]
- Palomo-López, P.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Rodríguez-Sanz, D.; Calvo-Lobo, C.; López-López, D. Footwear used by older people and a history of hyperkeratotic lesions on the foot: A prospective observational study. Medicine 2017, 96, e6623. [Google Scholar] [CrossRef] [PubMed]
- Pita-Fernandez, S.; Gonzalez-Martin, C.; Seoane-Pillado, T.; Pertega-Diaz, S.; Perez-Garcia, S.; Lopez-Calvino, B. Podiatric medical abnormalities in a random population sample 40 years or older in Spain. J. Am. Pod. Med. Assoc. 2014, 104, 574–582. [Google Scholar]
- Rodríguez-Sanz, D.; Barbeito-Fernández, D.; Losa-Iglesias, M.E.; Saleta-Canosa, J.L.; López-López, D.; Tovaruela-Carrión, N.; Becerro-de-Bengoa-Vallejo, R. Foot health and quality of life among university students: Cross-sectional study. Sao Paulo Med. J. 2018, 136, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Welch, V.; Jull, J.; Petkovic, J.; Armstrong, R.; Boyer, Y.; Cuervo, L.G.; Edwards, S.J.L.; Lydiatt, A.; Gough, D.; Grimshaw, J.; et al. Protocol for the development of a CONSORT-equity guideline to improve reporting of health equity in randomized trials. Implement. Sci. 2015, 10, 146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irwig, L.; Groeneveld, H.; Becklake, M. Relationship of lung function loss to level of initial function: Correcting for measurement error using the reliability coefficient. J. Epidemiol. Community Health 1988, 42, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Debouche, S.; Pitance, L.; Robert, A.; Liistro, G.; Reychler, G. Reliability and reproducibility of chest wall expansion measurement in young healthy adults. J. Manipulative Physiol. Ther. 2016, 39, 443–449. [Google Scholar] [CrossRef] [PubMed]
- 2018 GINA Report: Global Strategy for Asthma Management and Prevention—Global Initiative for Asthma. Available online: https://ginasthma.org/2018-gina-report-global-strategy-for-asthma-management-and-prevention/ (accessed on 3 November 2018).
- Sirera-Vercher, M.J.; Sáez-Zamora, P.; Sanz-Amaro, M.D. Traducción y adaptación transcultural al castellano y al valenciano del Foot Health Status Questionnaire. Rev. Esp. Cir. Ortop. Traumatol. 2010, 54, 211–219. [Google Scholar] [CrossRef]
- Cuesta-Vargas, A.; Bennett, P.; Jimenez-Cebrian, A.M.; Labajos-Manzanares, M.T. The psychometric properties of the Spanish version of the Foot Health Status Questionnaire. Qual. Life Res. 2013, 22, 1739–1743. [Google Scholar] [CrossRef] [PubMed]
- Bennett, P.J.; Patterson, C.; Wearing, S.; Baglioni, T. Development and validation of a questionnaire designed to measure foot-health status. J. Am. Podiatr. Med. Assoc. 1998, 88, 419–428. [Google Scholar] [CrossRef]
- Palomo-López, P.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Rodríguez-Sanz, D.; Calvo-Lobo, C.; López-López, D. Impact of plantar fasciitis on the quality of life of male and female patients according to the Foot Health Status Questionnaire. J. Pain Res. 2018, 11, 875–880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palomo López, P.; Rodríguez-Sanz, D.; Becerro de Bengoa Vallejo, R.; Losa-Iglesias, M.E.; Guerrero Martín, J.; Calvo Lobo, C.; López-López, D. Clinical aspects of foot health and their influence on quality of life among breast cancer survivors: A case-control study. Cancer Manag. Res. 2017, 9, 545–551. [Google Scholar] [CrossRef]
- Palomo-López, P.; Losa-Iglesias, M.E.; Becerro-de-Bengoa-Vallejo, R.; López-López, D.; Rodríguez-Sanz, D.; Romero-Morales, C.; Calvo-Lobo, C. Specific foot health-related quality-of-life impairment in patients with type II versus type I diabetes. Int. Wound J. 2019, 16, 47–51. [Google Scholar] [CrossRef]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Bonilla, J.; Bernal, G.; Santos, A.; Santos, D. A revised Spanish version of the beck depression inventory: Psychometric properties with a Puerto Rican sample of college students. J. Clin. Psychol. 2004, 60, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Bonicatto, S.; Dew, A.M.; Soria, J.J. Analysis of the psychometric properties of the Spanish version of the beck depression inventory in Argentina. Psychiatry Res. 1998, 79, 277–285. [Google Scholar] [CrossRef]
- Valdés, C.; Morales-Reyes, I.; Pérez, J.C.; Medellín, A.; Rojas, G.; Krause, M. Psychometric properties of a spanish version of the Beck depression inventory IA. Rev. Med. Chil. 2017, 145, 1005–1012. [Google Scholar] [CrossRef]
- Barrick, B.J.; Jalan, S.; Tollefson, M.M.; Milbrandt, T.A.; Larson, A.N.; Rank, M.A.; Lohse, C.M.; Davis, D.M.R. Associations of self-reported allergic diseases and musculoskeletal problems in children. Ann. Allergy Asthma Immunol. 2017, 119, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Ekici, A.; Ekici, M.; Kara, T.; Keles, H.; Kocyigit, P. Negative mood and quality of life in patients with asthma. Qual. Life Res. 2006, 15, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Siroux, V.; Boudier, A.; Anto, J.M.; Cazzoletti, L.; Accordini, S.; Alonso, J.; Cerveri, I.; Corsico, A.; Gulsvik, A.; Jarvis, D.; et al. Quality-of-life and asthma-severity in general population asthmatics: Results of the ECRHS II study. Allergy 2008, 63, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Geraldo José Cunha, Â.; Zbonik Mendes, A.; Dias Wanderley de Carvalho, F.; Aparecida Ribeiro de Paula, M.; Gonçalves Brasil, T. The impact of asthma on quality of life and anxiety: A pilot study. J. Asthma 2018, 10, 1–6. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Descriptive Data | Total Group (n = 152) | Asthma (n = 76) | Healthy (n = 76) | p-Value | |
|---|---|---|---|---|---|
| Age (years) | 37.00 ± 16.00 (18–65) | 36.00 ± 16.50 (20–65) | 38.00 ± 16.75 (18–65) | 0.368† | |
| Weight (kg) | 69.00 ± 20.65 (44–120) | 69.50 ± 22.00 (44–120) | 69.00 ± 18.75 (45-106) | 0.900† | |
| Height (m) | 1.65± 0.14 (1.43–1.97) | 1.67 ± 0.15 (1.50–1.97) | 1.64 ± 0.13 (1.43–1.87) | 0.361† | |
| BMI (kg/m2) | 24.44 ± 5.73 (17.21–39.18) | 24.06 ± 6.18 (17.21–39.18) | 24.57 ± 5.41 (17.30–34.72) | 0.531† | |
| Sex | Male | 58 (38.1%) | 31 (40.8%) | 27 (35.5%) | 0.617‡ |
| Female | 94 (61.9%) | 45 (59.2%) | 49 (64.5%) | ||
| Outcome Measurements | Total Group (n = 152) | Asthma (n = 76) | Healthy (n = 76) | p-Value (Asthma vs. Healthy) | |
|---|---|---|---|---|---|
| FHSQ foot pain | 87.50 ± 15.63 (0–100) | 87.50 ± 21.25 (16.88–100) | 87.50 ± 17.97 (0–100) | 0.485† | |
| FHSQ foot function | 93.75 ± 18.75 (6.25–100) | 93.75 ± 17.19 (25–100) | 93.75 ± 18.75 (6.25–100) | 0.997† | |
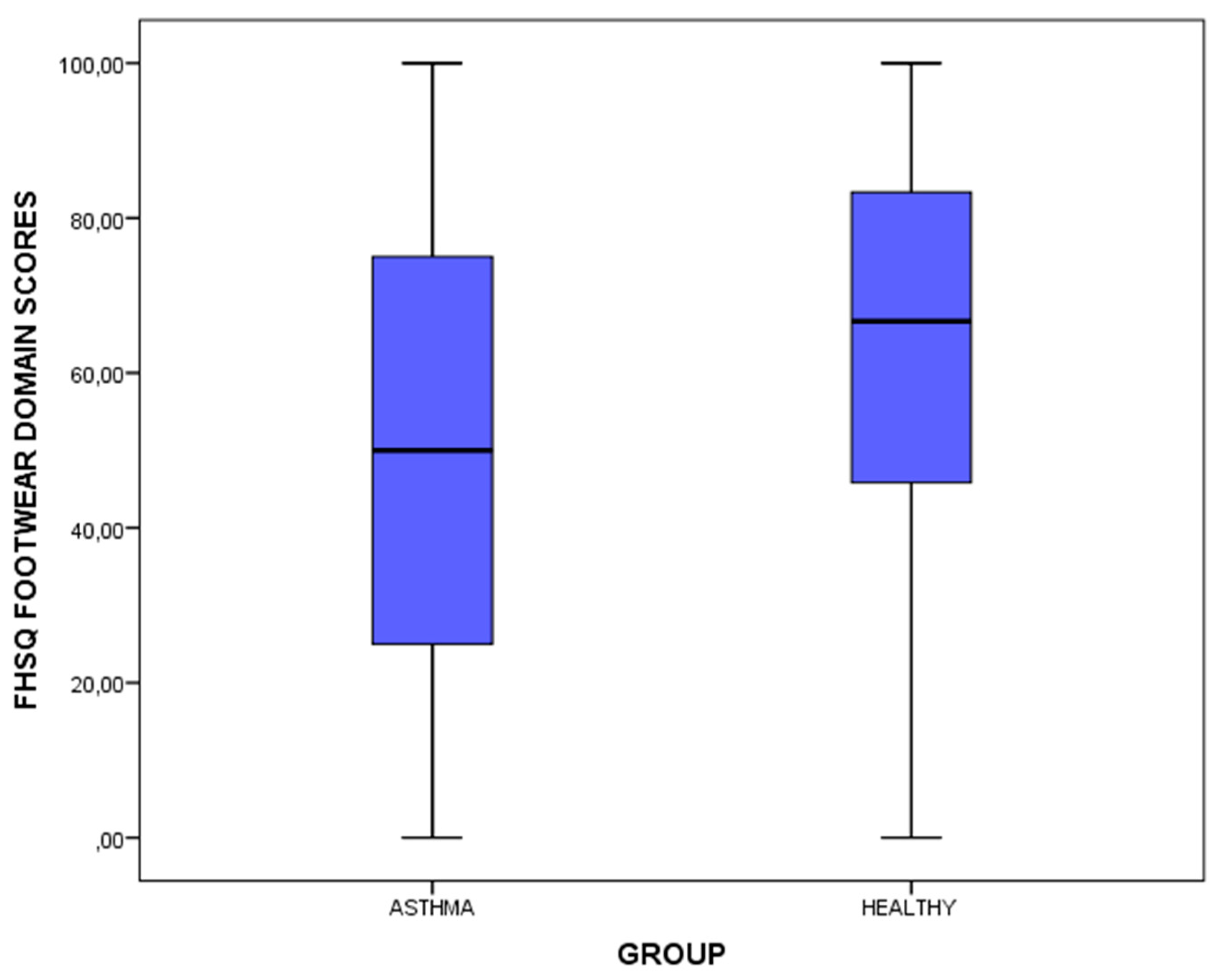
| FHSQ footwear | 58.33 ± 41.67 (0–100) | 50.00 ± 50.00 (0–100) | 66.56 ± 39.58 (0–100) | 0.003† | |
| FHSQ general foot health | 72.50 ± 35.00 (0–100) | 60.00 ± 35.00 (12.5–100) | 76.25 ± 42.50 (0–100) | 0.107† | |
| FHSQ general health | 70.00 ± 40.00 (10–100) | 70.00 ± 30.00 (20–100) | 70.00 ± 40.00 (10–100) | 0.383† | |
| FHSQ physical activity | 94.44 ± 16.67 (22.22–100) | 94.44 ± 16.67 (44.44–100) | 94.44 ± 16.67 (22.22–100) | 0.529† | |
| FHSQ social capacity | 100.00 ± 25.00 (0–100) | 100.00 ± 25.00 (25–100) | 100.00 ± 25.00 (0–100) | 0.356† | |
| FHSQ vigour | 56.25 ± 31.25 (12.5–100) | 56.25 ± 31.25 (12.5–100) | 56.25 ± 31.25 (12.5–100) | 0.626† | |
| BDI scores | 4.00 ± 7.00 (0–25) | 4.00 ± 6.00 (0–24) | 3.00 ± 7.00 (0–25) | 0.439† | |
| BDI category* | no depression | 124 (81.6%) | 62 (81.6%) | 62 (81.6%) | 0.928‡ |
| Mild | 17 (11.2%) | 8 (10.5%) | 9 (11.8%) | ||
| Moderate | 11 (7.2%) | 6 (7.9%) | 5 (6.6%) | ||
| Severe | 0 (0%) | 0 (0%) | 0 (0%) | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-López, D.; Painceira-Villar, R.; García-Paz, V.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Rodríguez-Sanz, D.; Calvo-Lobo, C. Impact of the Allergic Asthma on Foot Health-Related Quality of Life and Depression: A Novel Case-Control Research. Medicina 2019, 55, 124. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55050124
López-López D, Painceira-Villar R, García-Paz V, Becerro-de-Bengoa-Vallejo R, Losa-Iglesias ME, Rodríguez-Sanz D, Calvo-Lobo C. Impact of the Allergic Asthma on Foot Health-Related Quality of Life and Depression: A Novel Case-Control Research. Medicina. 2019; 55(5):124. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55050124
Chicago/Turabian StyleLópez-López, Daniel, Roi Painceira-Villar, Vanesa García-Paz, Ricardo Becerro-de-Bengoa-Vallejo, Marta Elena Losa-Iglesias, David Rodríguez-Sanz, and César Calvo-Lobo. 2019. "Impact of the Allergic Asthma on Foot Health-Related Quality of Life and Depression: A Novel Case-Control Research" Medicina 55, no. 5: 124. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55050124