Evaluation of the Salivary Level of Cortisol in Patients with Oral Lichen Planus: A Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
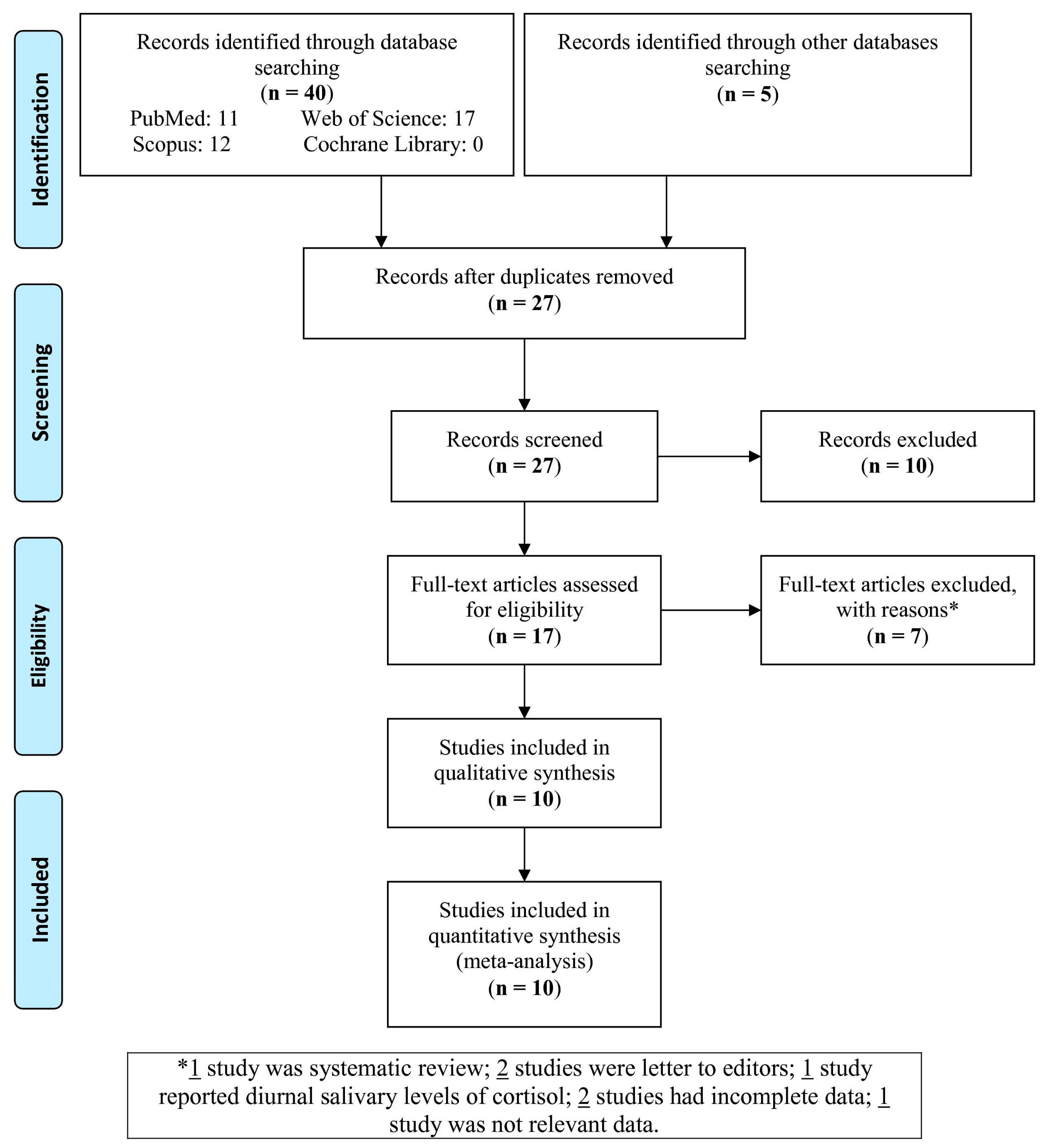
2.1. Protocol and Search Strategies
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Evaluation
2.5. Statistical Analyses
3. Results
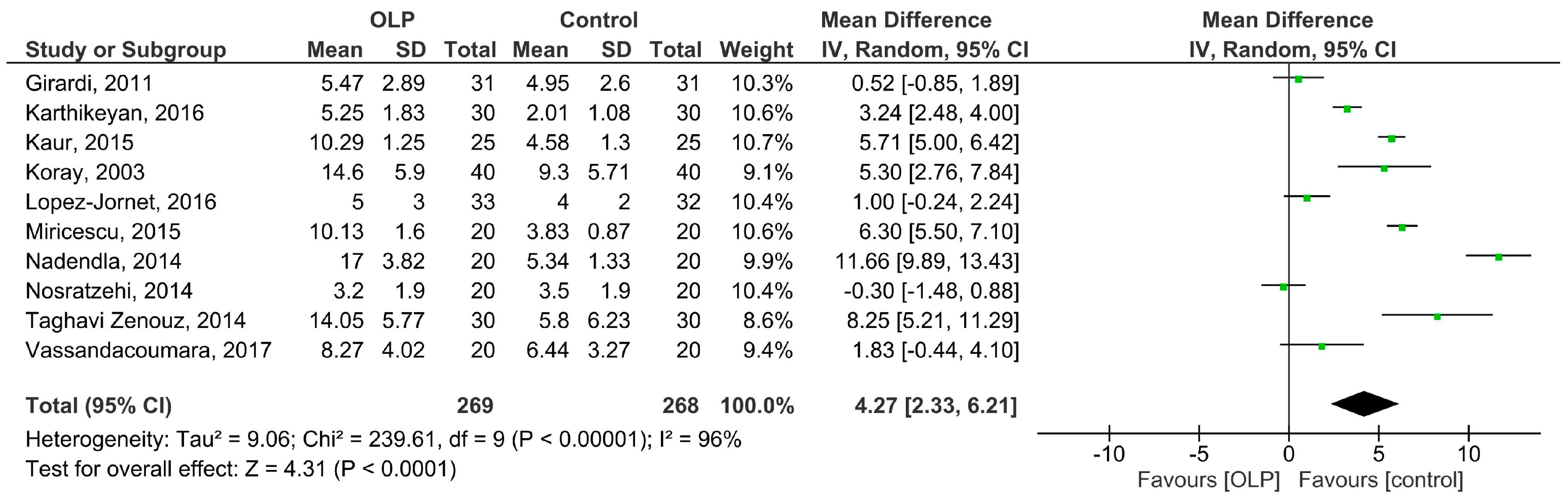
3.1. Meta-Analysis
3.1.1. Salivary Cortisol
3.1.2. Subgroup Analysis
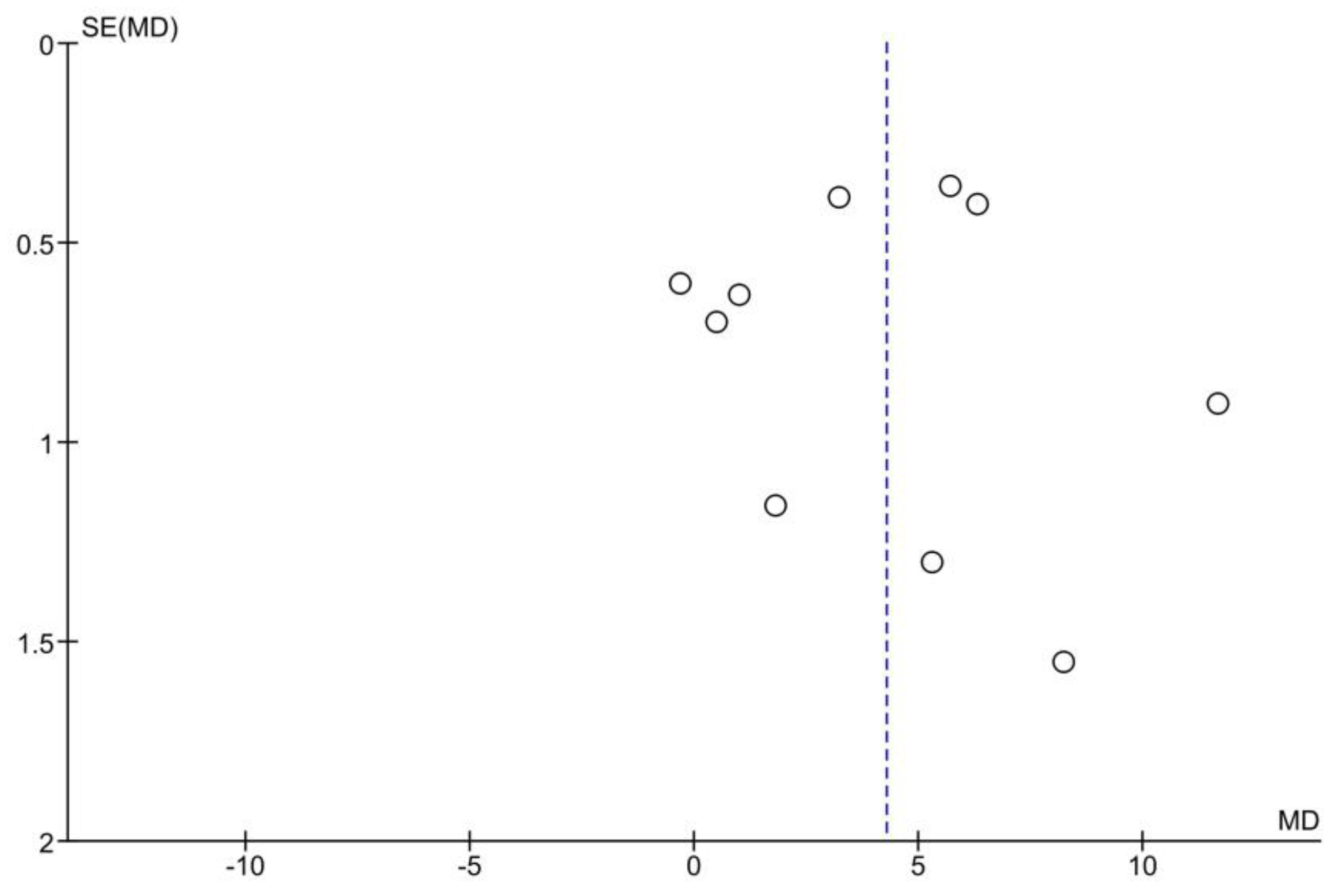
3.2. Publication Bias
3.3. Sensitivity Analysis
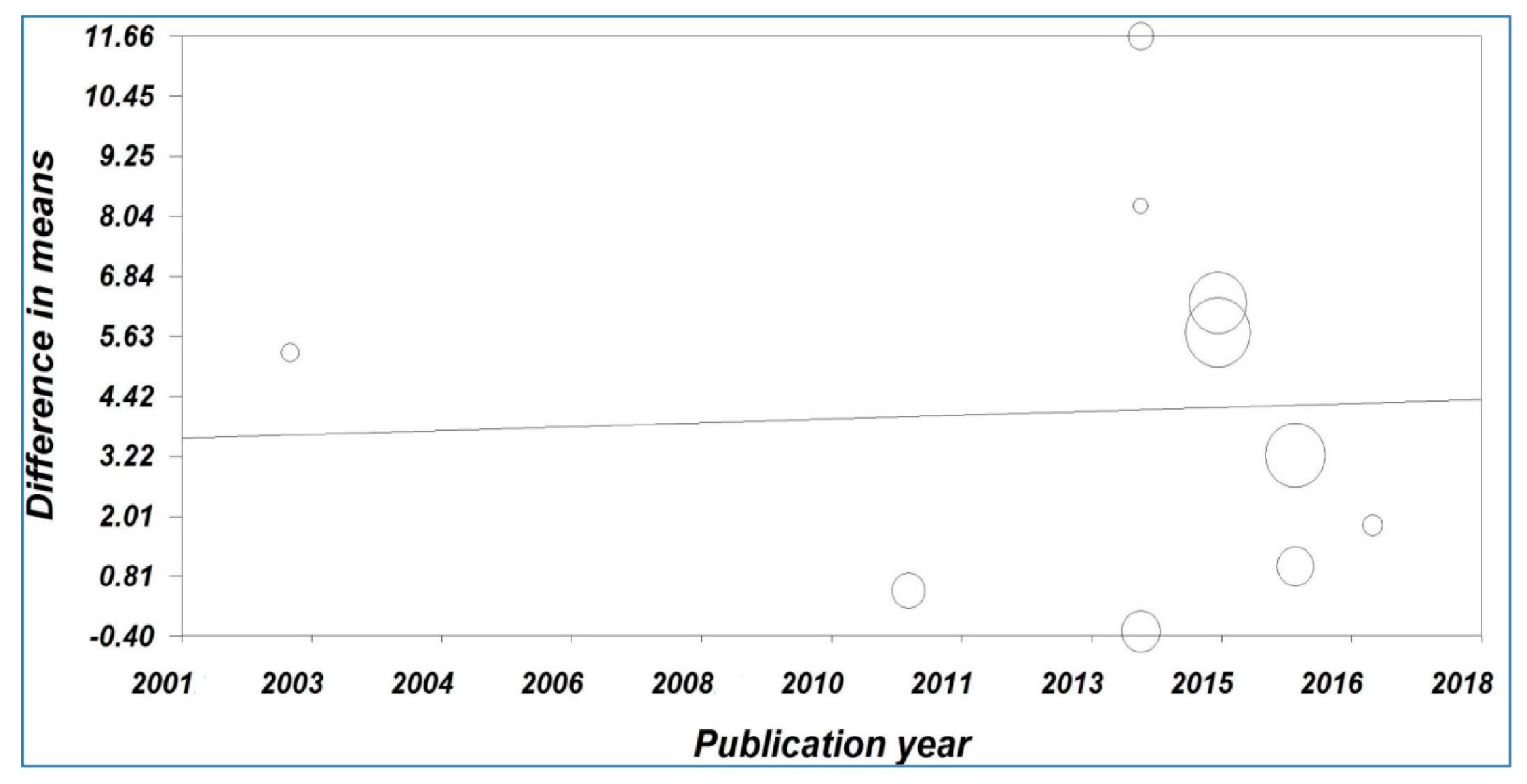
3.4. Meta-Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kaur, B.; Sunil, M.K.; Trivedi, A.; Singla, N.; Garg, S.; Goyal, N. Salivary Cortisol as a Diagnostic Marker in Oral Lichen Planus. J. Int. Oral Health 2015, 7, 43–48. [Google Scholar]
- Hazeldine, J.; Arlt, W.; Lord, J.M. Dehydroepiandrosterone as a regulator of immune cell function. J. Steroid Biochem. Mol. Biol. 2010, 120, 127–136. [Google Scholar] [CrossRef]
- Stojanovich, L. Stress autoimmunity. Autoimmun. Rev. 2010, 9, A271–A276. [Google Scholar] [CrossRef]
- Mozaffari, H.R.; Ramezani, M.; Mahmoudiahmadabadi, M.; Omidpanah, N.; Sadeghi, M. Salivary and serum levels of tumor necrosis factor-alpha in oral lichen planus: A systematic review and meta-analysis study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 124, e183–e189. [Google Scholar] [CrossRef]
- Mozaffari, H.R.; Sharifi, R.; Sadeghi, M. Interleukin-6 levels in the serum and saliva of patients with oral lichen planus compared with healthy controls: A meta-analysis study. Cent. Eur. J. Immunol. 2018, 43, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Mozaffari, H.R.; Sharifi, R.; Sadeghi, M. Prevalence of oral lichen planus in diabetes mellitus: A meta-analysis study. Acta Inform. Med. 2016, 24, 390–393. [Google Scholar] [CrossRef] [PubMed]
- Tvarijonaviciute, A.; Aznar-Cayuela, C.; Rubio, C.P.; Tecles, F.; Ceron, J.J.; López-Jornet, P. Salivary Antioxidant Status in Patients with Oral Lichen Planus: Correlation with Clinical Signs and Evolution during Treatment with Chamaemelum nobile. BioMed Res. Int. 2018, 2018, 5187549. [Google Scholar] [CrossRef] [PubMed]
- Girardi, C.; Luz, C.; Cherubini, K.; de Figueiredo, M.A.; Nunes, M.L.; Salum, F.G. Salivary cortisol and dehydroepiandrosterone (DHEA) levels, psychological factors in patients with oral lichen planus. Arch. Oral Biol. 2011, 56, 864–868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albanidou-Farmaki, E.; Poulopoulos, A.K.; Epivatianos, A.; Farmakis, K.; Karamouzis, M.; Antoniades, D. Increased anxiety level and high salivary and serum cortisol concentrations in patients with recurrent aphthous stomatitis. Tohoku J. Exp. Med. 2008, 214, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Ivanovski, K.; Nakova, M.; Warburton, G.; Pesevska, S.; Filipovska, A.; Nares, S.; Nunn, M.E.; Angelova, D.; Angelov, N. Psychological profile in oral lichen planus. J. Clin. Periodontol. 2005, 32, 1034–1040. [Google Scholar] [CrossRef]
- Mohamadi Hasel, K.; Besharat, M.A.; Abdolhoseini, A.; Alaei Nasab, S.; Niknam, S. Relationships of personality factors to perceived stress, depression, and oral lichen planus severity. Int. J. Behav. Med. 2013, 20, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Valter, K.; Boras, V.V.; Buljan, D.; Juras, D.V.; Susić, M.; Pandurić, D.G.; Verzak, Z. The influence of psychological state on oral lichen planus. Acta Clin. Croat. 2013, 52, 145–149. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Van der Waal, I. Potentially malignant disorders of the oral and oropharyngeal mucosa; terminology, classification and present concepts of management. Oral Oncol. 2009, 45, 317–323. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Robertson, J.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-Randomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2011; Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 12 January 2016).
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Nadendla, L.K.; Meduri, V.; Paramkusam, G.; Pachava, K.R. Association of salivary cortisol and anxiety levels in lichen planus patients. J. Clin. Diagn. Res. 2014, 8, ZC01–ZC03. [Google Scholar] [CrossRef] [PubMed]
- Karthikeyan, P.; Aswath, N. Stress as an etiologic co-factor in recurrent aphthous ulcers and oral lichen planus. J. Oral Sci. 2016, 58, 237–240. [Google Scholar] [CrossRef] [Green Version]
- Vassandacoumara, V.; Daniel, J.M. Correlation between salivary cortisol levels and Hospital Anxiety and Depression scores in oral lichen planus and recurrent aphthous stomatitis. Stomatol. Dis. Sci. 2017, 1, 103–108. [Google Scholar] [CrossRef]
- Koray, M.; Dülger, O.; Ak, G.; Horasanli, S.; Uçok, A.; Tanyeri, H.; Badur, S. The evaluation of anxiety and salivary cortisol levels in patients with oral lichen planus. Oral Dis. 2003, 9, 298–301. [Google Scholar] [CrossRef]
- Nosratzehi, T.; Arbabi-Kalati, F.; Salimi, S.; Honarmand, E. The Evaluation of Psychological Factor and Salivary Cortisol and IgA Levels in Patients with Oral Lichen Planus. Zahedan J. Res. Med. Sci. 2014, 16, 31–34. [Google Scholar]
- Taghavi Zenouz, A.; Mehdipour, M.; Dadashzadeh, H.; Rafieyan, S. Evaluation of relationship between salivary cortisol levels and stress intensity in oral lichen planus patients. Der. Pharm. Lett. 2014, 6, 459–461. [Google Scholar]
- Miricescu, D.; Totan, A.; Calenic, B.; Mocanu, B.; Greabu, M. Salivary and serum cortisol in patients with periodontal disease and oral lichen planus. Stomatol. Edu J. 2015, 2, 51–56. [Google Scholar]
- Lopez-Jornet, P.; Cayuela, C.A.; Tvarijonaviciute, A.; Parra-Perez, F.; Escribano, D.; Ceron, J. Oral lichen planus: Salival biomarkers cortisol, immunoglobulin A, adiponectin. J. Oral Pathol. Med. 2016, 45, 211–217. [Google Scholar] [CrossRef]
- Shetty, P.; Thopls, L.; Chatra, P.; Shenai Rao, P.; Bobu, S. An Association Between Serum Cortisol Levels In Erosive And Nonerosive Oral Lichen Planus Patients. Webmed Cent. Dent. 2010, 1, WMC0056. [Google Scholar]
- Chaudhary, S. Psychosocial stressors in oral lichen planus. Aust. Dent. J. 2004, 49, 192–195. [Google Scholar] [CrossRef]
- Rodstrom, P.O.; Jontell, M.; Hakebeg, M.; Berggren, U.; Lindstedt, G. Erosive lichen planus and salivary cortisol. J. Oral Pathol. Med. 2001, 30, 257–263. [Google Scholar] [CrossRef]
- Hampf, B.G.; Malmstrom, M.J.; Aalberg, V.A.; Hannula, J.A.; Vikkula, J. Psychiatric disturbance in patients with oral lichen planus. Oral Surg. Oral Med. Oral Pathol. 1987, 63, 429–432. [Google Scholar] [CrossRef]
- Shah, B.; Ashok, L.; Sujatha, G.P. Evaluation of salivary cortisol and psychological factors in patients with oral lichen planus. Indian J. Dent. Res. 2009, 20, 288–292. [Google Scholar] [CrossRef]
- McCartan, B.E.; Lamey, P.J.; Wallace, A.M. Salivary cortisol and anxiety in recurrent aphthous stomatitis. J. Oral Pathol. Med. 1996, 25, 357–359. [Google Scholar] [CrossRef]
- Nosratzehi, T. Oral Lichen Planus: An overview of potential risk factors, biomarkers and treatments. Asian Pac. J. Cancer Prev. 2018, 19, 1161–1167. [Google Scholar] [PubMed]
- Larsson, C.A.; Gullberg, B.; Råstam, L.; Lindblad, U. Salivary cortisol differs with age and sex and shows inverse associations with WHR in Swedish women: A cross-sectional study. BMC Endocr. Disord. 2009, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- Hanrahan, K.; McCarthy, A.M.; Kleiber, C.; Lutgendorf, S.; Tsalikian, E. Strategies for salivary cortisol collection and analysis in research with children. Appl. Nurs. Res. 2006, 19, 95–101. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| The First Author, Year | Country | Study Design | No. of OLP Patients/Controls | Mean Age of OLP Patients/Controls, Year | Male% of OLP Patients/Controls | Measurement Method (System) | Sampling Time (am) | OLP Forms | Score * |
|---|---|---|---|---|---|---|---|---|---|
| Koray, 2003 [21] | Turkey | CC | 40/40 | 35.2/34.6 | 40/45 | ELISA (Diagnostic System Laboratories, Inc, Webster, TX, USA) | 9–9:15 | NA | 7 |
| Girardi, 2011 [8] | Brazil | CC | 31/31 | 53.8/55.5 | 13/13 | Radioimmunoassay (Siemens Medical Solutions Diagnostics, Los Angeles, California, USA) | 8–10 | 55% combination of reticular and atrophic erosive, 25.8% reticular, 9.6% atrophic-erosive, and 9.6% combination of papular, reticular, and plaque | 7 |
| Nadendla, 2014 [18] | India | CC | 20/20 | Matched/Matched | Matched/Matched | ELISA (Diametra kit, Korea) | 9–9:15 | NA | 8 |
| Nosratzehi, 2014 [22] | Iran | CC | 20/20 | 45.8/42.8 | 35/Matched | ELISA | 9–10 | NA | 8 |
| Taghavi Zenouz, 2014 [23] | Iran | CC | 30/30 | 48.6/47.3 | 67/Matched | ELISA (DRG Salivary Cortisol—HS ELISA SLV 4635 DRG Instruments, GmbH, Germany) using Hyperion (USA) | 9–10 | NA | 7 |
| Kaur, 2015 [1] | India | CC | 25/25 | Matched/Matched | 36/Matched | ELISA | 9–10 | 52% reticular, 44% erosive, and 4% plaque | 7 |
| Miricescu, 2015 [24] | Romania | CC | 20/20 | NA/NA | 75/NA | ELISA | 9–10 | 100% keratosis and atrophic/erosive | 6 |
| Karthikeyan, 2016 [19] | India | CC | 30/30 | 39.9/NA | 43.3/50 | Electro chemiluminescence immunoassay (ECLIA) | before 10 | 76.7% reticular, 13.3% erosive, and 10% linear | 6 |
| Lopez-Jornet, 2016 [25] | Spain | CCS | 33/32 | 57/53 | 21.2/25 | Chemiluminescent enzyme immunoassay (Immulite; Siemens, Erlangen, Germany) | 10–12 | 75.7% reticular-papular and 24.3% atrophic-erosive | 7 |
| Vassandacoumara, 2017 [20] | India | CCS | 20/20 | 42.3/34.1 | 65/50 | Chemiluminescent immunoassay (ADVIA® Centaur™ System) | 8–9 | NA | 8 |
| No. of Studies | MD (95% CI) | P-Value | I2 | Ph | ||
|---|---|---|---|---|---|---|
| Area | India | 4 | 5.62 (2.67, 8.56) | 0.0002 | 97% | <0.00001 |
| Middle East | 3 | 4.28 (−1.13, 9.70) | 0.12 | 95% | <0.00001 | |
| Europe | 2 | 3.67 (−1.52, 8.87) | 0.17 | 98% | <0.00001 | |
| Method | ELISA | 6 | 5.33 (2.72, 7.93) | <0.0001 | 97% | <0.00001 |
| Others | 3 | 1.93 (−0.01, 3.87) | 0.05 | 83% | 0.002 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopez-Jornet, P.; Zavattaro, E.; Mozaffari, H.R.; Ramezani, M.; Sadeghi, M. Evaluation of the Salivary Level of Cortisol in Patients with Oral Lichen Planus: A Meta-Analysis. Medicina 2019, 55, 213. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55050213
Lopez-Jornet P, Zavattaro E, Mozaffari HR, Ramezani M, Sadeghi M. Evaluation of the Salivary Level of Cortisol in Patients with Oral Lichen Planus: A Meta-Analysis. Medicina. 2019; 55(5):213. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55050213
Chicago/Turabian StyleLopez-Jornet, Pia, Elisa Zavattaro, Hamid Reza Mozaffari, Mazaher Ramezani, and Masoud Sadeghi. 2019. "Evaluation of the Salivary Level of Cortisol in Patients with Oral Lichen Planus: A Meta-Analysis" Medicina 55, no. 5: 213. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55050213