The Use of Selected Ion Flow Tube-Mass Spectrometry Technology to Identify Breath Volatile Organic Compounds for the Detection of Head and Neck Squamous Cell Carcinoma: A Pilot Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Recruitment
2.2. Breath Collection and Sampling
2.3. Breath Analysis
2.4. Statistical Analysis
3. Results
3.1. Demographics and Patient Characteristics
3.2. Breath VOCs Identified by SIM Scan
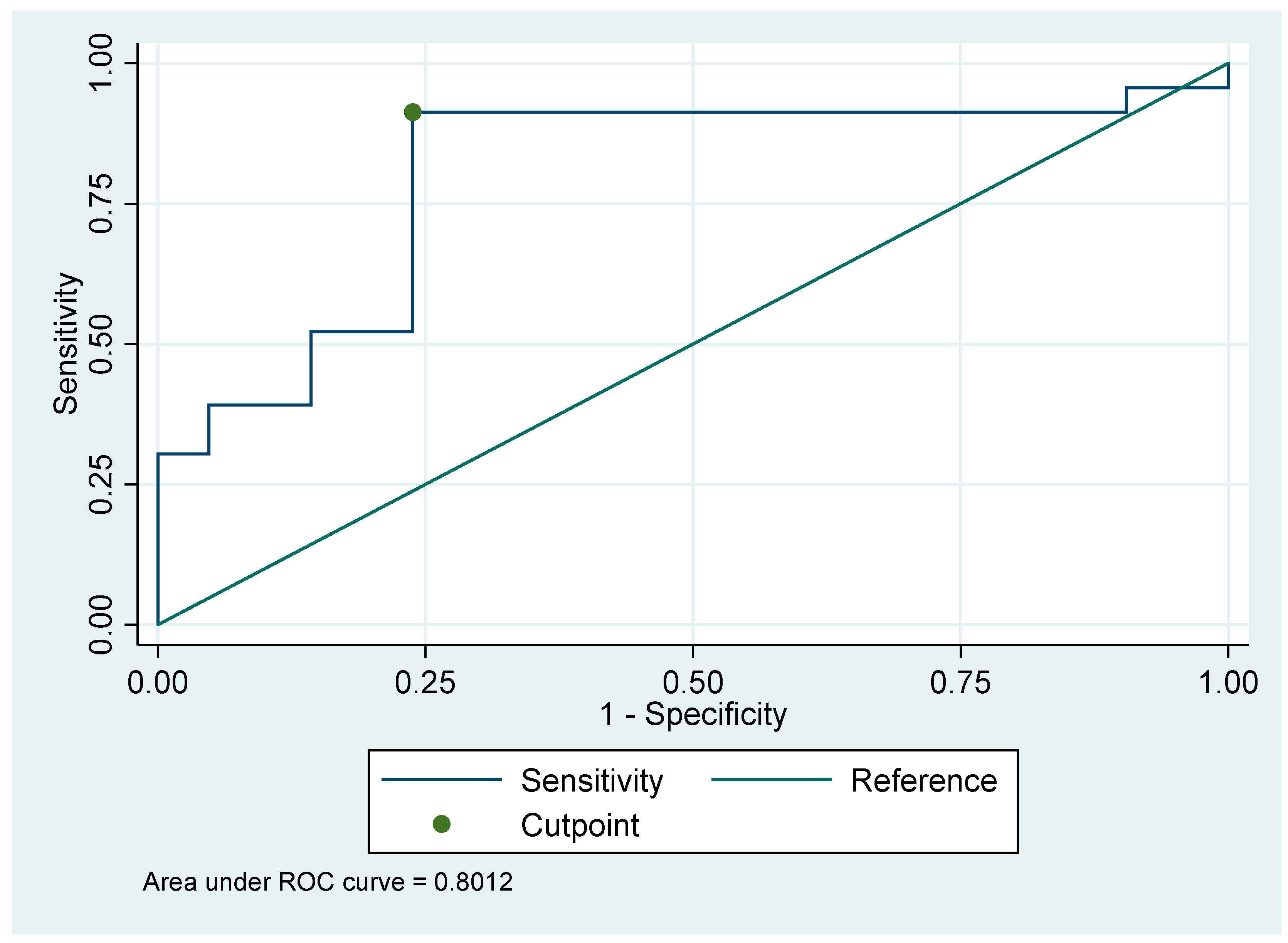
3.3. The Accuracy and Effectiveness of HCN as a Biomarker for HNSCC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerawala, C.J.; Bisase, B.; Lee, J. The use of examination under anaesthesia and panendoscopy in patients presenting with oral cavity and oropharyngeal squamous cell carcinoma. Ann. R. Coll. Surg. Engl. 2009, 91, 609–612. [Google Scholar] [CrossRef] [PubMed]
- Gruber, M.; Tisch, U.; Jeries, R.; Amal, H.; Hakim, M.; Ronen, O.; Marshak, T.; Zimmerman, D.; Israel, O.; Amiga, E. Analysis of exhaled breath for diagnosing head and neck squamous cell carcinoma: A feasibility study. Br. J. Cancer 2014, 111, 790–798. [Google Scholar] [CrossRef] [PubMed]
- Hakim, M.; Billan, S.; Tisch, U.; Peng, G.; Dvrokind, I.; Marom, O.; Abdah-Bortnyak, R.; Kuten, A.; Haick, H. Diagnosis of head-and-neck cancer from exhaled breath. Br. J. Cancer 2011, 104, 1649–1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atherton, J.; Spiller, R. The urea breath test for Helicobacter pylori. Gut 1994, 35, 723. [Google Scholar] [CrossRef] [PubMed]
- Mathew, T.; Pownraj, P.; Abdulla, S.; Pullithadathil, B. Technologies for clinical diagnosis using expired human breath analysis. Diagnostics 2015, 5, 27–60. [Google Scholar] [CrossRef]
- Amann, A.; de Lacy Costello, B.; Miekisch, W.; Schubert, J.; Buszewski, B.; Pleil, J.; Ratcliffe, N.; Risby, T. The human volatilome: Volatile organic compounds (VOCs) in exhaled breath, skin emanations, urine, feces and saliva. J. Breath Res. 2014, 8, 034001. [Google Scholar] [CrossRef] [PubMed]
- Garcia, R.A.; Morales, V.; Martin, S.; Vilches, E.; Toledano, A. Volatile organic compounds analysis in breath air in healthy volunteers and patients suffering epidermoid laryngeal carcinomas. Chromatographia 2014, 77, 501–509. [Google Scholar] [CrossRef]
- Leunis, N.; Boumans, M.L.; Kremer, B.; Din, S.; Stobberingh, E.; Kessels, A.G.; Kross, K.W. Application of an electronic nose in the diagnosis of head and neck cancer. Laryngoscope 2014, 124, 1377–1381. [Google Scholar] [CrossRef]
- Schmutzhard, J.; Rieder, J.; Deibl, M.; Schwentner, I.M.; Schmid, S.; Lirk, P.; Abraham, I.; Gunkel, A.R. Pilot study: Volatile organic compounds as a diagnostic marker for head and neck tumors. Head Neck 2008, 30, 743–749. [Google Scholar] [CrossRef]
- Van Hooren, M.R.; Leunis, N.; Brandsma, D.S.; Dingemans, A.-M.C.; Kremer, B.; Kross, K.W. Differentiating head and neck carcinoma from lung carcinoma with an electronic nose: A proof of concept study. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 3897–3903. [Google Scholar] [CrossRef] [PubMed]
- Van de Goor, R.; Leunis, N.; van Hooren, M.; Francisca, E.; Masclee, A.; Kremer, B.; Kross, K. Feasibility of electronic nose technology for discriminating between head and neck, bladder, and colon carcinomas. Eur. Arch. Oto-Rhino-Laryngol. 2017, 274, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Peng, Y.; Liu, Y.; Li, W.; Jin, Y.; Tang, Z.; Duan, Y. Investigation of potential breath biomarkers for the early diagnosis of breast cancer using gas chromatography—Mass spectrometry. Clin. Chim. Acta 2014, 436, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.; Cataneo, R.N.; Ditkoff, B.A.; Fisher, P.; Greenberg, J.; Gunawardena, R.; Kwon, C.S.; Rahbari-Oskoui, F.; Wong, C. Volatile markers of breast cancer in the breath. Breast J. 2003, 9, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.; Cataneo, R.N.; Ditkoff, B.A.; Fisher, P.; Greenberg, J.; Gunawardena, R.; Kwon, C.S.; Tietje, O.; Wong, C. Prediction of breast cancer using volatile biomarkers in the breath. Breast Cancer Res. Treat. 2006, 99, 19–21. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.; Cataneo, R.N.; Saunders, C.; Hope, P.; Schmitt, P.; Wai, J. Volatile biomarkers in the breath of women with breast cancer. J. Breath Res. 2010, 4, 026003. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Kumar, S.; Abbassi-Ghadi, N.; Španěl, P.; Smith, D.; Hanna, G.B. Selected ion flow tube mass spectrometry analysis of volatile metabolites in urine headspace for the profiling of gastro-esophageal cancer. Anal. Chem. 2013, 85, 3409–3416. [Google Scholar] [CrossRef]
- Machado, R.F.; Laskowski, D.; Deffenderfer, O.; Burch, T.; Zheng, S.; Mazzone, P.J.; Mekhail, T.; Jennings, C.; Stoller, J.K.; Pyle, J. Detection of lung cancer by sensor array analyses of exhaled breath. Am. J. Respir. Crit. Care Med. 2005, 171, 1286–1291. [Google Scholar] [CrossRef]
- Gordon, S.; Szidon, J.; Krotoszynski, B.; Gibbons, R.; O’Neill, H. Volatile organic compounds in exhaled air from patients with lung cancer. Clin. Chem. 1985, 31, 1278–1282. [Google Scholar]
- Chen, X.; Cao, M.; Li, Y.; Hu, W.; Wang, P.; Ying, K.; Pan, H. A study of an electronic nose for detection of lung cancer based on a virtual SAW gas sensors array and imaging recognition method. Meas. Sci. Technol. 2005, 16, 1535. [Google Scholar] [CrossRef]
- Phillips, M.; Cataneo, R.N.; Cheema, T.; Greenberg, J. Increased breath biomarkers of oxidative stress in diabetes mellitus. Clin. Chim. Acta 2004, 344, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Calenic, B.; Amann, A. Detection of volatile malodorous compounds in breath: Current analytical techniques and implications in human disease. Bioanalysis 2014, 6, 357–376. [Google Scholar] [CrossRef] [PubMed]
- Krilaviciute, A.; Heiss, J.A.; Leja, M.; Kupcinskas, J.; Haick, H.; Brenner, H. Detection of cancer through exhaled breath: A systematic review. Oncotarget 2015, 6, 38643. [Google Scholar] [CrossRef] [PubMed]
- Oakley-Girvan, I.; Davis, S.W. Breath based volatile organic compounds in the detection of breast, lung, and colorectal cancers: A systematic review. Cancer Biomark. 2018, 21, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.; Španěl, P. Selected ion flow tube mass spectrometry (SIFT-MS) for on-line trace gas analysis. Mass Spectrom. Rev. 2005, 24, 661–700. [Google Scholar] [CrossRef] [PubMed]
- Španěl, P.; Smith, D. Progress in SIFT-MS: Breath analysis and other applications. Mass Spectrom. Rev. 2011, 30, 236–267. [Google Scholar] [CrossRef] [PubMed]
- Buszewski, B.; Kęsy, M.; Ligor, T.; Amann, A. Human exhaled air analytics: Biomarkers of diseases. Biomed. Chromatogr. 2007, 21, 553–566. [Google Scholar] [CrossRef] [PubMed]
- Simeonova, F.P.; Fishbein, L. Hydrogen Cyanide and Cyanides: Human Health Aspects; World Health Organization Publications: Geneva, Switzerland, 2004. [Google Scholar]
- Španěl, P.; Dryahina, K.; Smith, D. Acetone, ammonia and hydrogen cyanide in exhaled breath of several volunteers aged 4–83 years. J. Breath Res. 2007, 1, 011001. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, S.; Dash, R.; Das, S.K.; Sarkar, D.; Fisher, P.B. Emerging strategies for the early detection and prevention of head and neck squamous cell cancer. J. Cell. Physiol. 2012, 227, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Enderby, B.; Smith, D.; Carroll, W.; Lenney, W. Hydrogen cyanide as a biomarker for Pseudomonas aeruginosa in the breath of children with cystic fibrosis. Pediatric Pulmonol. 2009, 44, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Panghal, M.; Kaushal, V.; Kadayan, S.; Yadav, J.P. Incidence and risk factors for infection in oral cancer patients undergoing different treatments protocols. BMC Oral Health 2012, 12, 22. [Google Scholar] [CrossRef] [PubMed]
- Joshi, P.; Dutta, S.; Chaturvedi, P.; Nair, S. Head and neck cancers in developing countries. Rambam Maimonides Med. J. 2014, 5. [Google Scholar] [CrossRef] [PubMed]
- Dragonieri, S.; Quaranta, V.N.; Carratu, P.; Ranieri, T.; Resta, O. Influence of age and gender on the profile of exhaled volatile organic compounds analyzed by an electronic nose. J. Bras. Pneumol. 2016, 42, 143–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| HNSCC associated VOCs 2,2-dimethylpropanoic acid ethanol undecane limonene 1-octene butanone acrylonitrile Colorectal Cancer associated VOCs isopentane (colorectal cancer) 2-methoxy-2-methyl butane 2-methylbutanoic acid decanal (colorectal cancer) N2 isopentane methylcyclohexane methylcyclopentane Breast cancer associated VOCs 2-propanol (breast cancer) isobutanoic acid (breast cancer) acetic acid (breast cancer) N2 2-methylundecanal tridecane longifolene cyclopropane 1,3-butadiene 1,4-benzoquinone Gastric cancer associated VOCs methyl n-propyl sulfide pentanal (gastric cancer) pentanoic acid furfural 4-methyloctanoic acid nonanal octanal | Lung Cancer associated VOCs 3-methylhexane methanol p-xylene methanol hexan-2-ol 1-propanol acetophenone benzoic acid cyclohexanone dodecane benzene 2-methylpentane 3-hexanone propanoic acid decane toluene 1,2,4-trimethylbenzene methylcyclopentane propylbenzene heptanal pentane hexanal acetone heptanal styrene decane isoprene formaldehyde isooctane furan N2 m-xylene 2,3-butanediol camphor ethane 3-methylbutanoic acid 3-methylhexane acetophenone methyl isobutyl ketone | Liver Disease associated VOCs dimethyl sulfide formic acid methyl mercaptan Infection associated VOCs ammonia hydrogen cyanide indole Halitosis isopropylamine trimethylamine 3-methylindole 1,5-diaminopentane Freon 113 acetoin 1,6-dihydrocarveol N2 1,1-dichloroethane Inflammatory bowel disease associated VOCs hydrogen sulfide dimethyl disulfide ammonia N2 butanoic acid Isobutanoic acid 1,4-diaminobutane |
| Factor | Level | Non-Cancer | HNSCC | p-Value |
|---|---|---|---|---|
| N | 21 | 23 | ||
| P16 status (positive) | - | 9 | ||
| Age, median (IQR) | 52 (41,60) | 61.5 (52.5,65.3) | 0.030 † | |
| Gender | F | 13 (62%) | 3 (13%) | <0.001 * |
| M | 8 (38%) | 20 (87%) | ||
| Height (cm), median (IQR) | 165.5 (162.4,172.0) | 172.0 (162.0,180.0) | 0.25 | |
| Weight (kg), median (IQR) | 75.0 (68.3,84.0) | 73.0 (61.0,93.0) | 0.91 | |
| Smoking Status | Never | 9 (43%) | 3 (13%) | 0.057 |
| Ex | 8 (38%) | 10 (43%) | ||
| Current | 4 (19%) | 10 (43%) | ||
| Smoking (pack years), median (IQR) | 1.0 (0.0,20.0) | 39.0 (25.0,52.0) | <0.001 § | |
| Alcohol intake (AUS standard drink)/week, median (IQR) | 1.0 (0.0,4.0) | 6.0 (0.0,21.0) | 0.019 § | |
| Hydrogen cyanide (74-90-8), median (IQR) | 1.1 (0.9,1.3) | 2.5 (1.6,4.4) | <0.001 § |
| Cancer Site | Number of Cases | Stage | |
|---|---|---|---|
| 1/11 | 111/1V | ||
| Oral Cavity | 4 | 3 | 1 |
| Oropharynx | 8 | 6 | 2 |
| Larynx | 8 | 4 | 4 |
| Hypopharynx | 3 | 1 | 2 |
| Cut-off Value | AUC | Sensitivity (%) | Specificity (%) | NPV (%) | PPV (%) |
|---|---|---|---|---|---|
| 1.25 | 0.801 | 91 | 76 | 88.6 | 80.4 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chandran, D.; Ooi, E.H.; Watson, D.I.; Kholmurodova, F.; Jaenisch, S.; Yazbeck, R. The Use of Selected Ion Flow Tube-Mass Spectrometry Technology to Identify Breath Volatile Organic Compounds for the Detection of Head and Neck Squamous Cell Carcinoma: A Pilot Study. Medicina 2019, 55, 306. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55060306
Chandran D, Ooi EH, Watson DI, Kholmurodova F, Jaenisch S, Yazbeck R. The Use of Selected Ion Flow Tube-Mass Spectrometry Technology to Identify Breath Volatile Organic Compounds for the Detection of Head and Neck Squamous Cell Carcinoma: A Pilot Study. Medicina. 2019; 55(6):306. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55060306
Chicago/Turabian StyleChandran, Dhinashini, Eng H. Ooi, David I Watson, Feruza Kholmurodova, Simone Jaenisch, and Roger Yazbeck. 2019. "The Use of Selected Ion Flow Tube-Mass Spectrometry Technology to Identify Breath Volatile Organic Compounds for the Detection of Head and Neck Squamous Cell Carcinoma: A Pilot Study" Medicina 55, no. 6: 306. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55060306