Surgical Site Infection after Breast Surgery: A Retrospective Analysis of 5-Year Postoperative Data from a Single Center in Poland

 , ,
, ,
Abstract
:1. Introduction
2. Methods
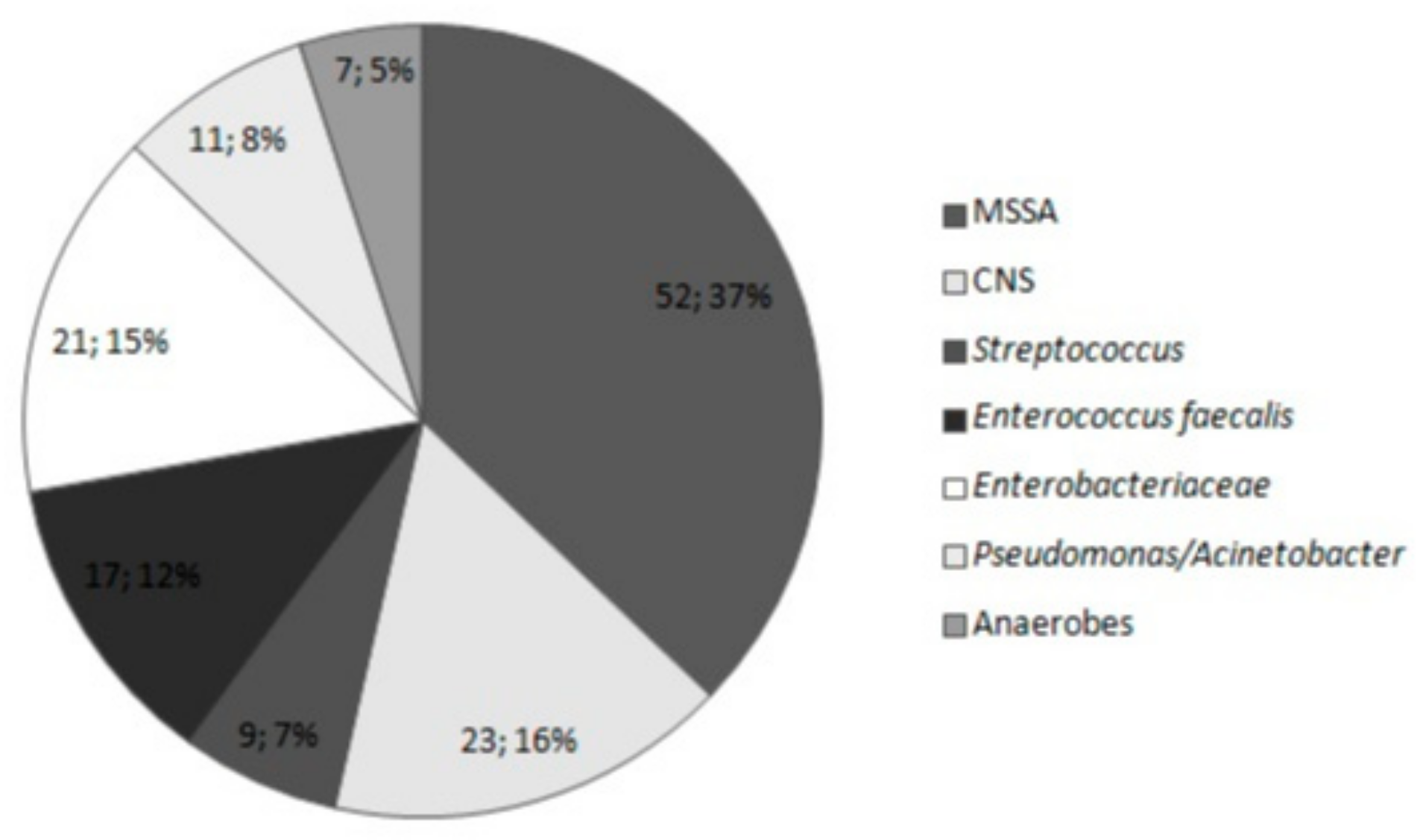
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bratzler, D.W.; Houck, P.M. Antimicrobial prophylaxis for surgery: An advisory statement from the national surgical infection prevention project. Clin. Infect. Dis. 2004, 38, 1706–1715. [Google Scholar] [CrossRef] [PubMed]
- Mangram, A.J.; Horan, T.C.; Pearson, M.L.; Silver, L.C.; Jarvis, W.R. Guideline for prevention of surgical site infection. Infect. Control Hosp. Epidemiol. 1999, 20, 247–280. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.H.; Anson, J. Peri-operative antibacterial prophylaxis. Pharm. J. 2004, 272, 743–745. [Google Scholar]
- Pałubicka, A.; Wekwejt, M.; Świeczko-Żurek, B.; Zieliński, J. Powikłania po rekonstrukcji piersi: Problem zakażeń i strategii prewencyjnej—Przegląd literaturowy. Chir. Plast. I Oparzenia 2017, 5, 89–97. [Google Scholar] [CrossRef]
- Ferlay, J.; Shin, H.; Bray, F.; Forman, D.; Mathers, C.; Parkin, D.M. Cancer Incidence and Mortality Worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, 359–386. [Google Scholar] [CrossRef] [PubMed]
- Gil-Londoño, J.C.; Nagles-Pelaez, J.A.; Maya-Salazar, W.A.; Madrid, J.; Maya-Restrepo, M.A.; Agudelo-Perez, R.A.; Ochoa, J. Surgical site infection after breast cancer surgery at 30 days. Infectio 2017, 21, 96–101. [Google Scholar] [CrossRef]
- Zhao, X.; Wu, X.; Dong, J.; Liu, Y.; Zheng, L.; Zhang, L. A Meta-analysis of Postoperative Complications of Tissue Expander/Implant Breast Reconstruction Using Acellular Dermal Matrix. Aesthetic Plast. Surg. 2015, 39, 892–901. [Google Scholar] [CrossRef] [PubMed]
- Olsen, M.A.; Lefta, M.; Dietz, J.R.; Brandt, K.E.; Aft, R.; Matthews, R.; Mayfield, J.; Fraser, V.J. Risk Factors for Surgical Site Infection after Major Breast Operation. J. Am. Coll. Surg. 2008, 207, 326–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Throckmorton, A.D.; Baddour, L.M.; Hoskin, T.L.; Boughey, J.C.; Degnim, A.C. Microbiology of surgical site infections complicating breast surgery. Surg. Infect. (Larchmt) 2010, 11, 355–359. [Google Scholar] [CrossRef] [PubMed]
- Franchelli, S.; Pesce, M.; Baldelli, I.; Marchese, A.; Santi, P.; De Maria, A. Analysis of clinical management of infected breast implants and of factors associated to successful breast pocket salvage in infections occurring after breast reconstruction. Int. J. Infect. Dis. 2018, 71, 67–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Blacam, C.; Ogunleye, A.A.; Momoh, A.O.; Colakoglu, S.; Tobias, A.M.; Sharma, R.; Houlihan, M.J.; Lee, B.T. High body mass index and smoking predict morbidity in breast cancer surgery: A multivariate analysis of 26,988 patients from the national surgical quality improvement program database. Ann. Surg. 2012, 255, 551–555. [Google Scholar] [CrossRef] [PubMed]
- Eck, D.L.; Koonce, S.L.; Goldberg, R.F.; Bagaria, S.; Gibson, T.; Bowers, S.P.; McLaughlin, S.A. Breast surgery outcomes as quality measures according to the NSQIP database. Ann. Surg. Oncol. 2012, 19, 3212–3217. [Google Scholar] [CrossRef] [PubMed]
- Davis, G.B.; Peric, M.; Chan, L.S.; Wong, A.K.; Sener, S.F. Identifying risk factors for surgical site infections in mastectomy patients using the National Surgical Quality Improvement Program database. Am. J. Surg. 2013, 205, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Crawford, C.B.; Clay, J.A.; Seydel, A.S.; Wernberg, J.A. Surgical Site Infections in Breast Surgery: The Use of Preoperative Antibiotics for Elective, Nonreconstructive Procedures. Int. J. Breast Cancer 2016, 2016, 1645192. [Google Scholar] [CrossRef] [PubMed]
- Vilar-Compte, D.; Jacquemin, B.; Robles-Vidal, C.; Volkow, P. Surgical site infections in breast surgery: Case-control study. World J. Surg. 2004, 28, 242–246. [Google Scholar]
- Ilonzo, N.; Tsang, A.; Tsantes, S.; Estabrook, A.; Thu Ma, A.M. Breast reconstruction after mastectomy: A ten-year analysis of trends and immediate postoperative outcomes. Breast 2017, 32, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Hanwright, P.; Davila, A.; Hirsch, E.M.; Khan, S.A.; Fine, N.A.; Bilimoria, K.Y.; Kim, J.Y. The differential effect of BMI on prosthetic versus autogenous breast reconstruction: A multivariate analysis of 12,986 patients. Breast 2013, 22, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Piper, M.L.; Roussel, L.O.; Koltz, P.F.; Wang, F.; Singh, K.; Chin, R.; Sbitany, H.; Langstein, H.N. Characterizing infections in prosthetic breast reconstruction: A validity assessment of national health databases. J. Plast. Reconstr. Aesthetic Surg. 2017, 70, 1345–1353. [Google Scholar] [CrossRef] [PubMed]
- Darragh, L.; Robb, A.; Hardie, C.M.; McDonald, S.; Valand, P.; O’Doboghue, J.M. Reducing implant loss rates in immediate breast reconstructions. Breast 2017, 31, 208–213. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Classic Breast Surgery (n = 865) | Breast-Conserving Surgery (n = 1002) | Breast Reconstruction via the TRAM Flap Method (n = 56) | Subcutaneous Amputation with Simultaneous Reconstruction (n = 206) | p Value | |
|---|---|---|---|---|---|
| All SSI | 46 (5.3%) | 48 (4.8%) | 8 (14.3%) | 30 (14.6%) | <0.001 |
| Early SSI | 34 (3.9%) | 31 (3.1%) | 4 (7.1%) | 17 (8.3%) | 0.004 |
| Late SSI | 12 (1.4%) | 17 (1.7%) | 4 (7.1%) | 13 (6.3%) | <0.001 |
| Classic Breast Surgery (n = 865) | Breast-Conserving Surgery (n = 1002) | Breast Reconstruction via the TRAM Flap Method (n = 56) | Subcutaneous Amputation with Simultaneous Reconstruction (n = 206) | p-Value | |
|---|---|---|---|---|---|
| MSSA | 22 (47.83%) | 16 (33.33%) | 3 (37.50%) | 11 (36.67%) | 0.529 |
| CNS | 7 (15.22%) | 10 (20.83%) | 0 (0.00%) | 6 (20.00%) | 0.499 |
| Streptococcus spp. | 3 (6.52%) | 4 (8.33%) | 1 (12.50%) | 1 (3.33%) | 0.763 |
| Enterococcus faecalis | 5 (10.87%) | 4 (8.33%) | 4 (50.00%) | 4 (13.33%) | 0.012 |
| Enterobacteriaceae | 13 (28.26%) | 7 (14.58%) | 0 (0.00%) | 1 (3.33%) | 0.016 |
| Pseudomonas/Acinetobacter | 6 (13.04%) | 3 (6.25%) | 1 (12.50%) | 1 (3.33%) | 0.428 |
| Anaerobes | 3 (6.52%) | 4 (8.33%) | 0 (0.00%) | 0 (0.00%) | 0.370 |
| Strains | ||||||||
|---|---|---|---|---|---|---|---|---|
| Staphylococcus aureus | Coagulase-negative Staphylococcus | Enterococcus faecalis | Streptococcus spp. | Enterobacteriaceae | Pseudomonas /Acinetobacter | Anaerobes | ||
| Number of Strains | 52 | 23 | 17 | 9 | 21 | 11 | 7 | |
| Antibiotics | PE | 0% | 0% | 100% | 100% | --------- | --------- | 100% |
| MET | 100% | 78% | --------- | --------- | --------- | --------- | --------- | |
| GE | 100% | 100% | --------- | --------- | --------- | --------- | --------- | |
| GE High | --------- | --------- | 100% | --------- | --------- | --------- | --------- | |
| S High | --------- | --------- | 100% | --------- | --------- | --------- | --------- | |
| TYG | --------- | --------- | 100% | 100% | --------- | --------- | --------- | |
| TEI | --------- | --------- | 100% | 100% | --------- | --------- | --------- | |
| AN | 100% | 100% | --------- | --------- | 100% | 100% | --------- | |
| E | 89% | 78% | nr | 89% | --------- | --------- | --------- | |
| CC | 89% | 78% | nr | --------- | --------- | --------- | 43% | |
| SXT | 100% | 91% | nr | --------- | 91% | 100% | --------- | |
| CIP | 98% | 91% | 87% | 100% | 96% | 100% | --------- | |
| VA | 100% | 100% | 100% | 100% | --------- | --------- | --------- | |
| LZD | 100% | 100% | 100% | 100% | --------- | --------- | --------- | |
| AM | 100% | 78% | 100% | 100% | 26% | --------- | 100% | |
| AMC | 100% | 78% | 100% | 100% | 26% | --------- | 100% | |
| CXM | 100% | 78% | nr | 100% | 96% | --------- | --------- | |
| CTX | 100% | 78% | nr | 100% | 96% | 88% | --------- | |
| CAZ | 100% | 78% | nr | 100% | 96% | 88% | --------- | |
| IPM | 100% | 78% | 100% | 100% | 100% | 100% | --------- | |
| MEM | 100% | 78% | 100% | 100% | 100% | 100% | --------- | |
| MTZ | --------- | --------- | --------- | --------- | --------- | --------- | 100% | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palubicka, A.; Jaworski, R.; Wekwejt, M.; Swieczko-Zurek, B.; Pikula, M.; Jaskiewicz, J.; Zielinski, J. Surgical Site Infection after Breast Surgery: A Retrospective Analysis of 5-Year Postoperative Data from a Single Center in Poland. Medicina 2019, 55, 512. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55090512
Palubicka A, Jaworski R, Wekwejt M, Swieczko-Zurek B, Pikula M, Jaskiewicz J, Zielinski J. Surgical Site Infection after Breast Surgery: A Retrospective Analysis of 5-Year Postoperative Data from a Single Center in Poland. Medicina. 2019; 55(9):512. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55090512
Chicago/Turabian StylePalubicka, Anna, Radoslaw Jaworski, Marcin Wekwejt, Beata Swieczko-Zurek, Michal Pikula, Janusz Jaskiewicz, and Jacek Zielinski. 2019. "Surgical Site Infection after Breast Surgery: A Retrospective Analysis of 5-Year Postoperative Data from a Single Center in Poland" Medicina 55, no. 9: 512. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55090512