Physiological Gait versus Gait in VR on Multidirectional Treadmill—Comparative Analysis

 ,
,  ,
,
Abstract
:1. Introduction
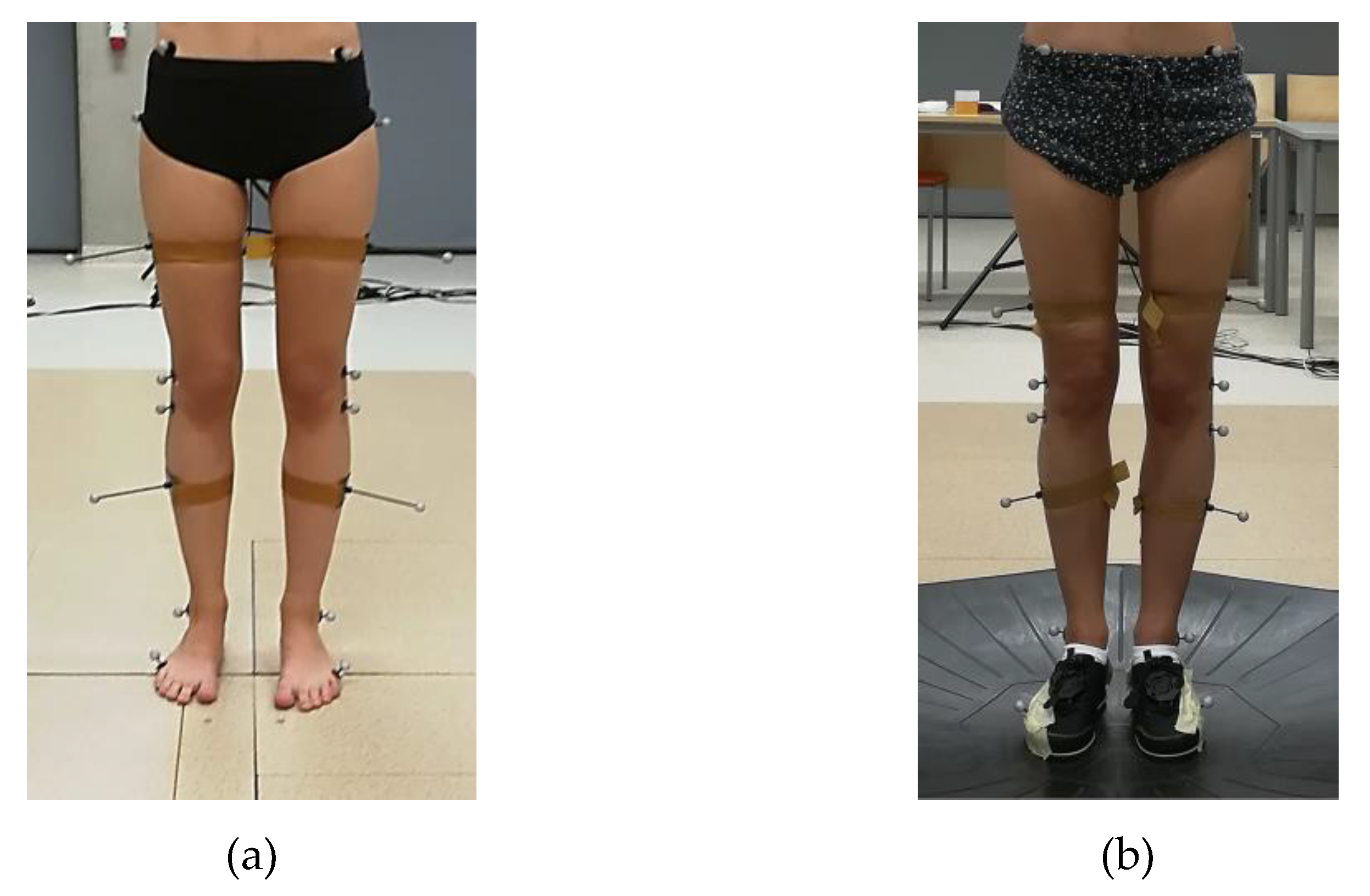
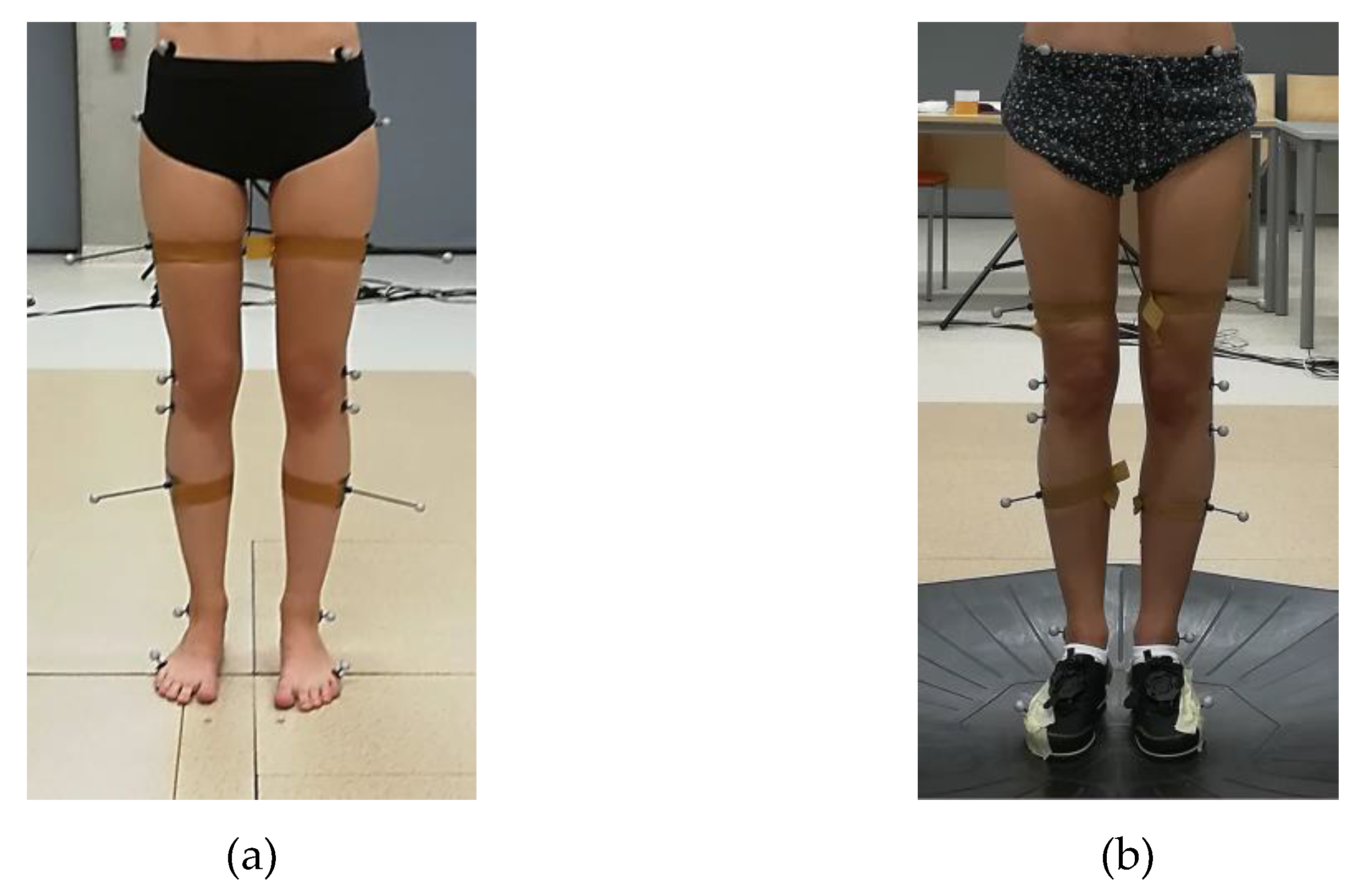
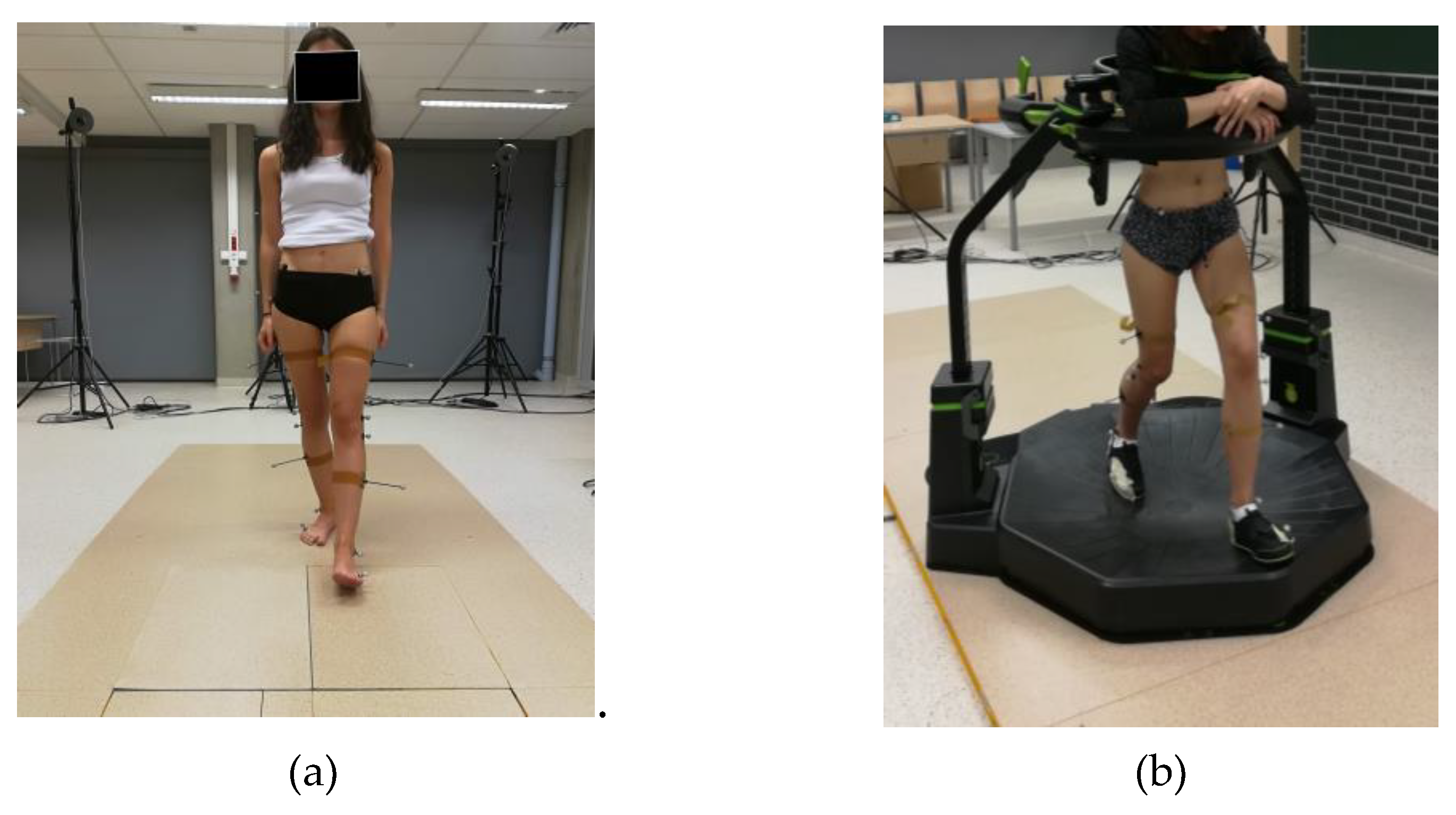
2. Materials and Methods
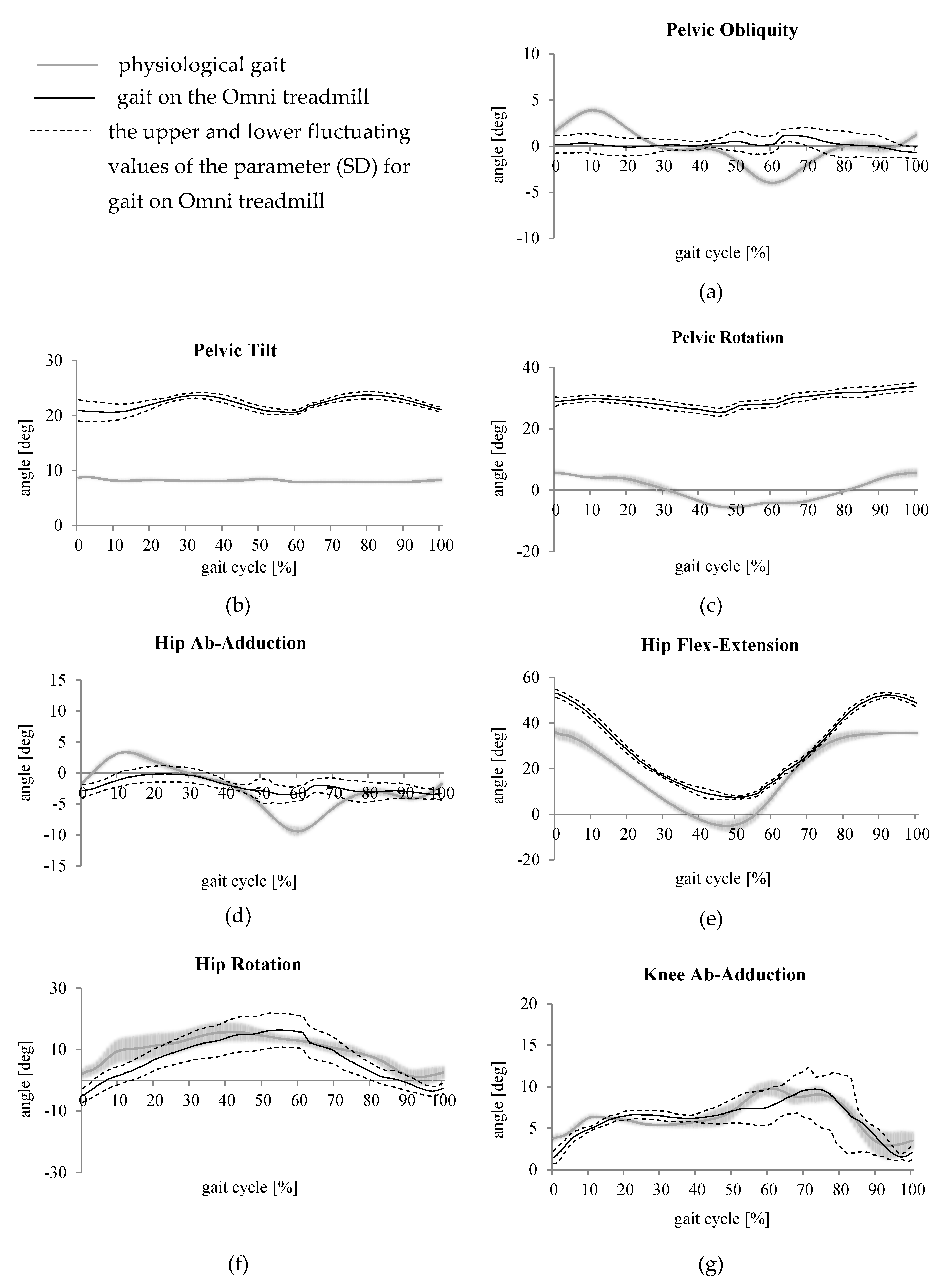
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mellecker, R.; McManus, A. Active video games and physical activity recommendations: A comparison of the Gamercize Stepper, XBOX Kinect and XaviX J-Mat. J. Sci. Med. Sport 2014, 17, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Naugle, K.E.; Naugle, K.M.; Wikstrom, E.A. Cardiovascular and Affective Outcomes of Active Gaming: Using the Nintendo Wii as a Cardiovascular Training Tool. J. Strength Cond. Res. 2014, 28, 443–451. [Google Scholar] [CrossRef] [PubMed]
- O’Donovan, C.; Hussey, J. Active video games as a form of exercise and the effect of gaming experience: A preliminary study in healthy young adults. Physiotherapy 2012, 98, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Polechoński, J.; Mynarski, W.; Garbaciak, W.; Fredyk, A.; Rozpara, M.; Nawrocka, A. Energy Expenditure and Intensity of Interactive Video Dance Games according to Health Recommendations. Cent. Eur. J. Sport Sci. Med. 2018, 24, 35–43. [Google Scholar] [CrossRef]
- Sween, J.; Wallington, S.F.; Sheppard, V.; Taylor, T.; Llanos, A.A.; Adams-Campbell, L.L. The Role of Exergaming in Improving Physical Activity: A Review. J. Phys. Act. Health 2014, 11, 864–870. [Google Scholar] [CrossRef] [Green Version]
- González González, C.; Gómez Río, N.; Navarro-Adelantado, V. Exploring the Benefits of Using Gamification and Videogames for Physical Exercise: A Review of State of Art. Int. J. Interact. Multimed. Artif. Intell. 2018. [Google Scholar] [CrossRef]
- Kraft, A.J.; Russell, W.D.; Bowman, A.T.; Selsor, C.W.; Foster, G.D. Heart Rate and Perceived Exertion During Self-Selected Intensities for Exergaming Compared to Traditional Exercise in College-Age Participants. J. Strength Cond. Res. 2011, 25, 1736–1742. [Google Scholar] [CrossRef]
- Lyons, E.J.; Tate, D.F.; Komoski, S.E.; Carr, P.M.; Ward, D.S. Novel Approaches to Obesity Prevention: Effects of Game Enjoyment and Game Type on Energy Expenditure in Active Video Games. J. Diabetes Sci. Technol. 2012, 6, 839–848. [Google Scholar] [CrossRef] [Green Version]
- Kafri, M.; Myslinski, M.J.; Gade, V.K.; Deutsch, J.E. Energy Expenditure and Exercise Intensity of Interactive Video Gaming in Individuals Poststroke. Neurorehabilit. Neural Repair 2014, 28, 56–65. [Google Scholar] [CrossRef]
- Palacios-Ceña, D.; Ortiz-Gutiérrez, R.; Buesa-Estellez, A.; Río, F.G.D.; Cachon-Perez, J.M.; Martínez-Piedrola, R.; Velarde-Garcia, J.F.; La Cuerda, R.C.D. Multiple sclerosis patients’ experiences in relation to the impact of the kinect virtual home-exercise programme: A qualitative study. Eur. J. Phys. Rehabil. Med. 2016, 52, 347–355. [Google Scholar]
- Staiano, A.E.; Flynn, R. Therapeutic Uses of Active Videogames: A Systematic Review. Games Health J. 2014, 3, 351–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carvalho, B.; Neves, A.; Soares, G.; Lins, A.; Soares, M.M.; Rebelo, F. Virtual Reality Devices Applied to Digital Games. In Around the Patient Bed; Informa: London, UK, 2016; pp. 125–141. [Google Scholar]
- Matsangidou, M.; Ang, C.S.; Mauger, A.R.; Intarasirisawat, J.; Otkhmezuri, B.; Avraamides, M.N. Is your virtual self as sensational as your real? Virtual Reality: The effect of body consciousness on the experience of exercise sensations. Psychol. Sport Exerc. 2019, 41, 218–224. [Google Scholar] [CrossRef]
- de Melo, G.E.L.; Kleiner, A.F.R.; Lopes, J.B.P.; Dumont, A.J.L.; Lazzari, R.D.; Galli, M.; Oliveira, C.S. Effect of virtual reality training on walking distance and physical fitness in individuals with Parkinson’s disease. Neuro Rehabil. 2018, 42, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Lange, B.; George, S.; Deutsch, E.J.; Saposnik, G.; Crotty, M.; Laver, E.K. Virtual reality for stroke rehabilitation. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef]
- Lee, H.C.; Huang, C.L.; Ho, S.H.; Sung, W.H. The Effect of a Virtual Reality Game Intervention on Balance for Patients with Stroke: A Randomized Controlled Trial. Games Health J. 2017, 6, 303–311. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Ceurstemont, S. Optical illusions help you explore a virtual world on foot. New Sci. 2013, 218, 22. [Google Scholar] [CrossRef]
- Frissen, I.; Campos, J.L.; Sreenivasa, M.; Ernst, M.O. Enabling Unconstrained Omnidirectional Walking Through Virtual Environments: An Overview of the CyberWalk Project. In Hum. Walk. Virtual Environ: Perception, Technology, and Applications; Steinicke, F., Visell, Y., Campos, J., Lécuyer, A., Eds.; Springer International Publishing: Basel, Switzerland, 2013; Chapter 6; pp. 113–144. [Google Scholar]
- Giphart, J.E.; Chou, Y.-H.; Kim, D.H.; Bortnyk, C.T.; Wagenaar, R.C. Effects of Virtual Reality Immersion and Walking Speed on Coordination of Arm and Leg Movements. Presence Teleoperators Virtual Environ. 2007, 16, 399–413. [Google Scholar] [CrossRef]
- Nabiyouni, M.; Saktheeswaran, A.; Bowman, D.A.; Karanth, A. Comparing the Performance of Natural, Semi-Natural, and Non-Natural Locomotion Techniques in Virtual Reality. In Proceedings of the 2015 IEEE Symposium on 3D User Interfaces (3DUI), Arles, France, 23–24 March 2015; pp. 3–10. [Google Scholar]
- Vaughan, C.L.; Davis, B.L.; O’Connor, J.C. Dynamics of Human Gait; Kiboho Publishers: Cape Town, South Africa, 1999. [Google Scholar]
- Omni by Virtuix—The leading and most popular VR motion platform. Virtuix Omni n.d. Available online: https://www.virtuix.com/ (accessed on 5 August 2019).
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H.; et al. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion—Part I: Ankle, hip, and spine. J. Biomech. 2002, 35, 543–548. [Google Scholar] [CrossRef]
- Michnik, R.; Nowakowska, K.; Jurkojć, J.; Jochymczyk-Woźniak, K.; Kopyta, I. Motor functions assessment method based on energy changes in gait cycle. Acta Bioeng. Biomech. 2017, 19, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Jochymczyk-Woźniak, K.; Nowakowska, K.; Michnik, R.; Gzik, M.; Wodarski, P.; Janoska, P. Three-Dimensional Children Gait Pattern-Reference Data for Healthy Children Aged Between 7 and 17. In Information Technologies in Medicine 6th International Conference, ITIB 2018, Kamień Śląski, Poland, 18–20 June 2018; Piętka, E., Badura, P., Kawa, J., Wieclawek, W., Eds.; Springer International Publishing: Basel, Switzerland, 2019; pp. 589–601. [Google Scholar]
- Leszczewska, J.; Czaprowski, D.; Pawłowska, P.; Oponowicz, A. Inter-Examiner, Within-Session and Between-Session Repeatability of Kinematic Gait Parameters Among Adult Subjects. Hum. Mov. 2012, 13, 337–343. [Google Scholar] [CrossRef]
- Franz, J.R.; Kram, R. Advanced age and the mechanics of uphill walking: A joint-level, inverse dynamic analysis. Gait Posture 2014, 39, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Ehlen, K.A.; Reiser, R.F.; Browning, R.C. Energetics and Biomechanics of Inclined Treadmill Walking in Obese Adults. Med. Sci. Sports Exerc. 2011, 43, 1251–1259. [Google Scholar] [CrossRef] [PubMed]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1081. [Google Scholar] [CrossRef] [PubMed]
- Hootman, J.M.; Macera, C.A.; Ainsworth, B.E.; Addy, C.L.; Martin, M.; Blair, S.N. Epidemiology of musculoskeletal injuries among sedentary and physically active adults. Med. Sci. Sports Exerc. 2002, 34, 838–844. [Google Scholar] [CrossRef] [PubMed]
- Browning, R.C.; Baker, E.A.; Herron, J.A.; Kram, R. Effects of obesity and sex on the energetic cost and preferred speed of walking. J. Appl. Physiol. 2006, 100, 390–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hills, A.P.; Byrne, N.M.; Wearing, S.; Armstrong, T. Validation of the intensity of walking for pleasure in obese adults. Prev. Med. 2006, 42, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Lelas, J.L.; Merriman, G.J.; Riley, O.P.; Kerrigan, D. Predicting peak kinematic and kinetic parameters from gait speed. Gait Posture 2003, 17, 106–112. [Google Scholar] [CrossRef]
- Winter, D.A. Kinematic and kinetic patterns in human gait: Variability and compensating effects. Hum. Mov. Sci. 1984, 3, 51–76. [Google Scholar] [CrossRef]
- Polechoński, J.; Mynarski, W.; Nawrocka, A. Applicability of pedometry and accelerometry in the calculation of energy expenditure during walking and Nordic walking among women in relation to their exercise heart rate. J. Phys. Ther. Sci. 2015, 27, 3525–3527. [Google Scholar] [CrossRef]
- Chwała, W.; Klimek, A.; Mirek, W. Changes in Energy Cost and Total External Work of Muscles in Elite Race Walkers Walking at Different Speeds. J. Hum. Kinet. 2014, 44, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Williams, K.R.; Cavanagh, P.R. A model for the calculation of mechanical power during distance running. J. Biomech. 1983, 16, 115–128. [Google Scholar] [CrossRef]
- Petrovic, M.; Maganaris, C.; Bowling, F.; Boulton, A.; Reeves, N. Vertical displacement of the centre of mass during walking in people with diabetes and diabetic neuropathy does not explain their higher metabolic cost of walking. J. Biomech. 2019, 83, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Dejaeger, D.; Willems, P.; Heglund, N. The energy cost of walking in children. Pflügers Archiv. Eur. J. Physiol. 2001, 441, 538–543. [Google Scholar] [CrossRef] [PubMed]
- Dziuba, A.K.; Tylkowska, M.; Jaroszczuk, S. Index of mechanical work in gait of children with cerebral palsy. Acta Bioeng. Biomech. 2014, 16, 77–87. [Google Scholar] [PubMed]
- McDowell, B.; Cosgrove, A.; Baker, R. Estimating mechanical cost in subjects with myelomeningocele. Gait Posture 2002, 15, 25–31. [Google Scholar] [CrossRef]
- Van de Walle, P.; Desloovere, K.; Truijen, S.; Gosselink, R.; Aerts, P.; Hallemans, A. Age-related changes in mechanical and metabolic energy during typical gait. Gait Posture 2010, 31, 495–501. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Physiological Gait Δep [J kg−1] | Gait on the Omni Treadmill ΔEp [J kg−1] | Physiological Gait Δek [J kg−1] | Gait on the Omni Treadmill Δek [J kg−1] | Physiological Gait Δec [J kg−1] | Gait on the Omni Treadmill Δec [J kg−1] | Physiological Gait Δsacrum [M] | Gait on the Omni Treadmill Δsacrum [M] | |
|---|---|---|---|---|---|---|---|---|
| Person 1 | 0.348 | 0.202 | 0.358 | 0.006 | 0.551 | 0.208 | 0.033 | 0.007 |
| Person 2 | 0.601 | 0.244 | 0.104 | 0.021 | 0.704 | 0.265 | 0.058 | 0.021 |
| Person 3 | 0.421 | 0.154 | 0.174 | 0.016 | 0.595 | 0.17 | 0.038 | 0.012 |
| Person 4 | 0.303 | 0.12 | 0.114 | 0.011 | 0.416 | 0.132 | 0.029 | 0.008 |
| Person 5 | 0.442 | 0.244 | 0.172 | 0.018 | 0.614 | 0.262 | 0.042 | 0.018 |
| Person 6 | 0.449 | 0.081 | 0.129 | 0.014 | 0.578 | 0.095 | 0.04 | 0.005 |
| Person 7 | 0.358 | 0.177 | 0.177 | 0.033 | 0.535 | 0.209 | 0.034 | 0.013 |
| Person 8 | 0.454 | 0.315 | 0.084 | 0.018 | 0.538 | 0.327 | 0.04 | 0.025 |
| Person 9 | 0.427 | 0.251 | 0.146 | 0.018 | 0.573 | 0.269 | 0.031 | 0.02 |
| Person 10 | 0.364 | 0.284 | 0.088 | 0.023 | 0.452 | 0.288 | 0.033 | 0.024 |
| Mean | 0.417 | 0.207 | 0.155 | 0.018 | 0.556 | 0.222 | 0.038 | 0.015 |
| SD | 0.082 | 0.074 | 0.08 | 0.007 | 0.081 | 0.073 | 0.008 | 0.007 |
| Range of Motion (Min,Max) | |||
|---|---|---|---|
| Normative Values [27] | Physiological Gait | Gait on the Omni Treadmill | |
| Registration System | Vicon | BTS Smart | BTS Smart |
| Age [years] | 18–40 | 20–24 | 20–24 |
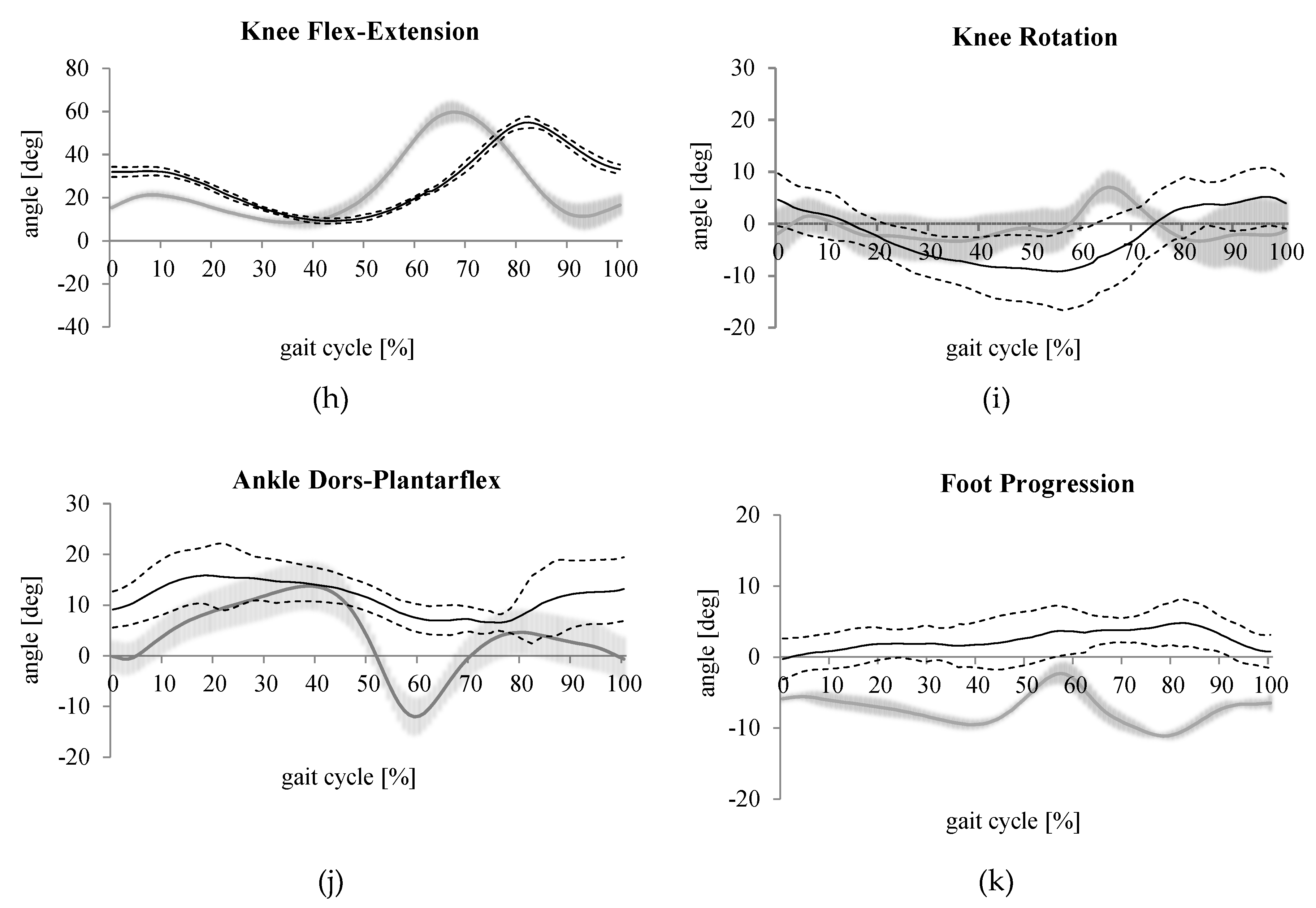
| Ankle dorsal-plantar flexion [deg] | 25.5 | 25.8 (−12,13.7) | 9.3 (6.6,15.9) |
| Foot progression [deg] | 15.7 | 13.5 (−11.1,−2.3) | 5.1 (−0.3,4.8) |
| Knee flexion-extension [deg] | 56.7 | 51.3 (8.4,59.7) | 45.7 (9.2,54.9) |
| Knee adduction-abduction [deg] | 13.4 | 6.9 (2.9,9.8) | 8.7 (1.4,9.7) |
| Knee rotation [deg] | 16 | 10.4 (−3.4,7.1) | 14.4 (−9.2,5.2) |
| Hip flexion-extension [deg] | 43.3 | 41 (−5.2,35.8) | 45. 6 (7.4,53) |
| Hip adduction-abduction [deg] | 11.6 | 12.8 (−9.4,3.4) | 3.4 (−3.5,−0.1) |
| Hip rotation [deg] | 13 | 14.7 (1,15.7) | 21.3 (−4.9,16.4) |
| Pelvic tilt [deg] | 2.8 | 0.9 (7.9,8.8) | 3.1 (20.6,23.8) |
| Pelvic obliquity [deg] | 8.4 | 7.9 (−4,3.9) | 1.9 (−0.7,1.2) |
| Pelvic rotation [deg] | 9.2 | 11.3 (−5.7,5.7) | 8.5 (1,1.7) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jochymczyk-Woźniak, K.; Nowakowska, K.; Polechoński, J.; Sładczyk, S.; Michnik, R. Physiological Gait versus Gait in VR on Multidirectional Treadmill—Comparative Analysis. Medicina 2019, 55, 517. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55090517
Jochymczyk-Woźniak K, Nowakowska K, Polechoński J, Sładczyk S, Michnik R. Physiological Gait versus Gait in VR on Multidirectional Treadmill—Comparative Analysis. Medicina. 2019; 55(9):517. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55090517
Chicago/Turabian StyleJochymczyk-Woźniak, Katarzyna, Katarzyna Nowakowska, Jacek Polechoński, Sandra Sładczyk, and Robert Michnik. 2019. "Physiological Gait versus Gait in VR on Multidirectional Treadmill—Comparative Analysis" Medicina 55, no. 9: 517. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55090517